
Abstract
Purpose
Sleep disorder is a frequent postoperative complication after total hip arthroplasty (THA). This study aimed to characterize sleep disorder phenotypes, identify associated risk factors, and explore the relationships between sleep disturbance patterns and clinical outcomes in elderly patients aged ≥70 years.
Materials and Methods
A single-center retrospective analysis included 892 primary THA patients between January 2021 and December 2024. Sleep disorders were assessed via a validated 12-item questionnaire and diagnosed according to the International Classification of Sleep Disorders, 2nd Edition. Visual analog scale (VAS) pain scores and length of hospital stay (LOS) were extracted and stratified by different groups. All patients finished a minimum 6-month postoperative follow-up.
Results
78.3% of patients had postoperative sleep disturbances (median 6 weeks, range 4-8 weeks). Primary insomnias (72.1%) dominated, with adjustment sleep disorder (41.5%) most common; secondary insomnias (27.9%) linked to comorbidities (19.7%) and drugs (8.2%). Elderly patients had 83.5% incidence and 3.2-fold higher risk of persistent disturbances versus non-elderly patients (p<0.001). Patients with sleep maintenance difficulties or non-restorative sleep tended to present with higher VAS (p<0.001) and longer LOS (p<0.001) significantly.
Discussion
Pain (38.6%), psychological stress (29.4%), and intrinsic factors (16.2%) were most commonly associated with sleep disturbances. Elderly patients were more vulnerable to comorbidity-related and environmental sleep disruptors. Differences in clinical indicators were observed between patients receiving personalized perioperative management and those under routine care.
Conclusions
Adjustment sleep disorder is the most common postoperative sleep phenotype in THA patients. Pain, psychological factors, and intrinsic characteristics are key drivers. In addition, patients with difficulty in staying asleep and non-restorative sleep are associated with higher pain scores and prolonged LOS. Elderly patients are high-risk for persistent sleep disturbances and inferior recovery outcomes. These findings suggest potential directions for patient-centered perioperative management, while relevant associations need further verification.
Keywords
Introduction
Total hip arthroplasty (THA) is the gold standard surgery for end-stage hip pathologies, like avascular necrosis (AVN), osteoarthritis (OA), and rheumatoid arthritis. It is capable of relieving pain and recovering joint function effectively. 1 Postoperative sleep disturbance is a common complication that impairs quality of life and rehabilitation. Similar to total knee arthroplasty counterparts, THA patients frequently report sleep disturbances.2,3 Insufficient sleep reduces pain tolerance, fosters daytime fatigue, and disrupts emotional regulation, all of which delay recovery and are potentially correlated with a spectrum of perioperative adverse events, including wound complications and deep vein thrombosis. 4 A bidirectional interaction between sleep and pain is prominent among THA patients. 5
As enhanced recovery after surgery (ERAS) protocols have been widely applied in joint surgery, sleep management has emerged as a crucial role of perioperative care. 6 However, studies focusing specifically on THA-related sleep disturbance remain limited. The International Classification of Sleep Disorders, 2nd Edition (ICSD-2) offers a standardized framework, categorizing sleep disorders into 8 major classes: insomnias, sleep-related breathing disorders, and hypersomnias. 7 For total knee arthroplasty patients, adjustment insomnia and pain-related sleep disruption dominate, 8 but THA differs markedly: surgical approach, pain patterns (hip pain often radiates to the groin or thigh, unlike localized knee pain), and rehabilitation paradigms. These factors could reshape the sleep disorder landscape.
THA patients face unique sleep-related challenges. To minimize hip dislocation risk, they must avoid hip flexion beyond 90 degrees adduction and internal rotation for 4-6 weeks postoperatively. 9 This prolonged positional constraint breeds discomfort and pressure-related pain during sleep, especially in elderly patients with diminished tissue elasticity. Nocturnal pain is also aggravated in THA recipients: nighttime reduction of anti-inflammatory cortisol and elevation of pro-inflammatory cytokines jointly intensify pain perception. 5
Elderly patients (≥70 years) stand out as a distinct high-risk group for postoperative sleep disorders.6,10 The sleep-pain interaction is more obvious in this population, which can be explained by age-related changes in sleep structure, higher comorbidity burden (chronic obstructive pulmonary disease, heart failure) and greater sensitivity to environmental interference. 10 However, few studies have proposed targeted interventions, leaving a critical gap in clinical practice.
This study aimed to: (1) classify postoperative sleep disorders in THA patients using ICSD-2 criteria; (2) identify factors associated with sleep disturbances; (3) analyze associations between sleep disorder subtypes, age, and key recovery outcomes [visual analog scale (VAS) pain scores, length of hospital stay (LOS)]; and (4) propose personalized intervention strategies for elderly THA patients.
Materials and Methods
This single-center retrospective observational cohort study was reported in compliance with the STROBE Guidelines and approved by the Institutional Review Board. Eligible patients underwent primary THA between January 2021 and December 2024 for AVN and OA. This time frame was selected to ensure the consistency of perioperative ERAS protocols and nursing practices, thereby minimizing confounding bias from systematic clinical changes. Inclusion criteria mandated complete medical records, sleep questionnaire completion (during hospitalization or follow-up), and a minimum 6-month follow-up (range, 6-12 months). Exclusion criteria included preoperatively diagnosed chronic sleep disorders, chronic pain conditions, neurological/psychiatric conditions (e.g., schizophrenia, severe depression, and perioperative medication use), incomplete data, and revision THA.
Patient data were collected from inpatient medical records, outpatient follow-up files, and a specialized “sleep-related” questionnaire administered to all patients with sleep disturbances. The diagnosis of sleep disorders was performed using subjective tools; compared with objective testing methods such as polysomnography (PSG), subjective assessment more effectively reflects patients’ real experiences and subjective perceptions of their sleep status.11,12 It does not indicate higher accuracy, but better captures patient-centered sleep status.
Sleep disorder assessment combined a 12-item subjective questionnaire and ICSD-2 criteria.7,13 This 12-item questionnaire was adapted from Medical Outcomes Study Sleep Scale, with minor revisions tailored to the clinical characteristics of perioperative THA patients. The revised scale was reviewed by a panel of sleep medicine and psychology experts to ensure content validity, and was further validated in our orthopedic inpatient cohort with excellent internal consistency (Cronbach’s α > 0.93). 7 The full item list is provided in Supplementary Materials. The questionnaire evaluated five domains: (1) Sleep quality: Rated on a 10-cm VAS (0 = worst sleep quality, 10 = best sleep quality); (2) Disruptive factors: Patients selected the primary sleep disruptor. Options are like: pain, anxiety/depression, intrinsic conditions (e.g., COPD, HF), ward noise, nursing care, treatments, light stimulation, and positional discomfort; (3) Specific forms: Presence of difficulty falling asleep, difficulty staying asleep, early awakening, or non-restorative sleep (defined as occurring ≥3 days weekly); (4) Sleep quantity/efficiency: Bedtime, wake time, total sleep hours, sleep efficiency; (5) Daytime impact: Daytime sleepiness and functional impairment (VAS 0-10).
In our study, Sleep medicine and psychology specialists performed systematic assessments of patients’ sleep and psychological status, and final diagnoses were determined based on ICSD-2 criteria. The detailed classification framework is presented in Supplementary Table 1. The study mainly focused on insomnia, the most prevalent sleep disorder among orthopedic patients, which was divided into primary and secondary subtypes. 8 Any diagnostic disagreements were resolved through group discussion; if consensus could not be reached, a third reviewer was consulted for a final decision.
All THA procedures were performed via a posterior lateral approach by a single team of orthopedic surgeons. Standard cementless femoral stems and acetabular components (Waldemar Link, Germany) were used, with ceramic-on-ceramic or metal-on-polyethylene bearing surfaces. Drainage tubes were removed within 24-48 hours postoperatively.
Postoperative management adhered to ERAS principles: (1) Prophylactic antibiotics for 24 hours (cefotaxime, 1g intravenously three times daily); (2) Anticoagulant therapy began within 12h after surgery and continued for 35 days [rivaroxaban, 10mg daily, or low-molecular-weight heparin 2850 IU daily for body weight <90kg, 5700 IU daily for body weight >90kg]; (3) Early mobilization, patients ambulated with walkers or crutches within 24-48 hours, transitioning to unassisted walking as tolerated (typically 4-6 weeks); (4) Physical therapy, daily functional exercises (hip flexion, abduction, extension), each movement repeated 10-15 times per set, 2 sets daily.1,14 All postoperative clinical and rehabilitation protocols, including pain assessment, functional exercise guidance, and ward environment management, were uniformly implemented by the interdisciplinary care team to ensure consistency of nursing practice.
Among elderly patients (≥70 years), a subgroup received personalized perioperative interventions following a standard clinical protocol. Eligible participants for this group were aged ≥70 years undergoing primary THA with complete baseline and follow-up data, and presented with perioperative sleep disturbance or high-risk features including multiple comorbidities, preoperative sleep impairment or severe postoperative pain. Patients with revision THA, severe cognitive dysfunction, pre-existing chronic sleep disorders or incomplete data were excluded.
Personalized interventions included a multimodal analgesic regimen (extended-release nonsteroidal anti-inflammatory drugs + nocturnal acetaminophen), sleep-friendly environmental modifications (soundproof curtains, clustered nursing care to reduce nighttime disruptions, dimmed evening lighting), sleep hygiene education, and targeted positional guidance for THA-specific restrictions. The control group received routine ERAS-based perioperative management as standard care, without additional sleep-targeted interventions, optimized multimodal analgesia or structured sleep-friendly ward environment adjustments. Treatment allocation was performed sequentially based on clinical admission order to minimize selection bias, and all interventions were delivered by a dedicated interdisciplinary team blinded to outcome assessment.
Key postoperative outcomes were extracted from medical records, including the VAS pain score, LOS, sleep disturbance duration, and persistent sleep disorder. Specifically, VAS pain scores were assessed serially at discharge, 2 weeks, 6 weeks, and 3 months postoperatively, with the 2-week assessment representing the acute recovery phase; serial assessments were used to reflect longitudinal pain recovery trends. Nocturnal pain was rated separately for episodes of nighttime awakenings (0-10 scale, 0 = no pain, 10 = worst pain). LOS was defined as the total hospital stay, calculated from the time of admission to discharge. Sleep disturbance duration was defined as the time from surgery to symptom resolution. Resolution was set as a sleep quality VAS score ≥7, a validated cutoff for arthroplasty patients.7,11,13 Persistent sleep disorder was defined as sleep disturbance lasting over 8 weeks, following standard definitions from prior research on elderly orthopedic patients.10,11,13 This endpoint was the primary outcome for elderly subgroup analysis. Additional sleep-related outcomes were derived from questionnaire responses and medical documentation.
Statistical analyses were performed using SAS 9.2 (SAS Institute Inc., Cary, NC, USA). Categorical variables were presented as counts and percentages, compared via Chi-square test. Continuous variables were tested for normality with the Shapiro-Wilk test; normally distributed data were reported as mean ± standard deviation (SD), non-normally distributed data were reported as median [interquartile range (IQR)]. Differences in continuous outcomes across sleep disorder subtypes and age groups were analyzed via one-way analysis of variance or Kruskal-Wallis test, with Tukey’s test for post-hoc comparisons. Multivariate logistic regression was used to identify independent factors associated with persistent sleep disorders, adjusting for key confounders including gender, body mass index (BMI), comorbidities, preoperative pain score, and preoperative sleep quality. The odds ratio (OR) and 95% confidence interval (CI) were calculated. Note: Odds ratios derived from multivariate logistic regression are presented here, as this is the standard output for this statistical model. Pearson correlation analysis examined relationships between VAS pain scores and sleep quality indices. Statistical significance was set at p<0.05.
The authors have independently reviewed, revised, and confirmed the accuracy, academic rigor, and consistency of the language content, and assume full responsibility for the final version of the manuscript.
Results
Baseline Clinical Characteristics
Baseline Clinical Characteristics of Patients (n=892)
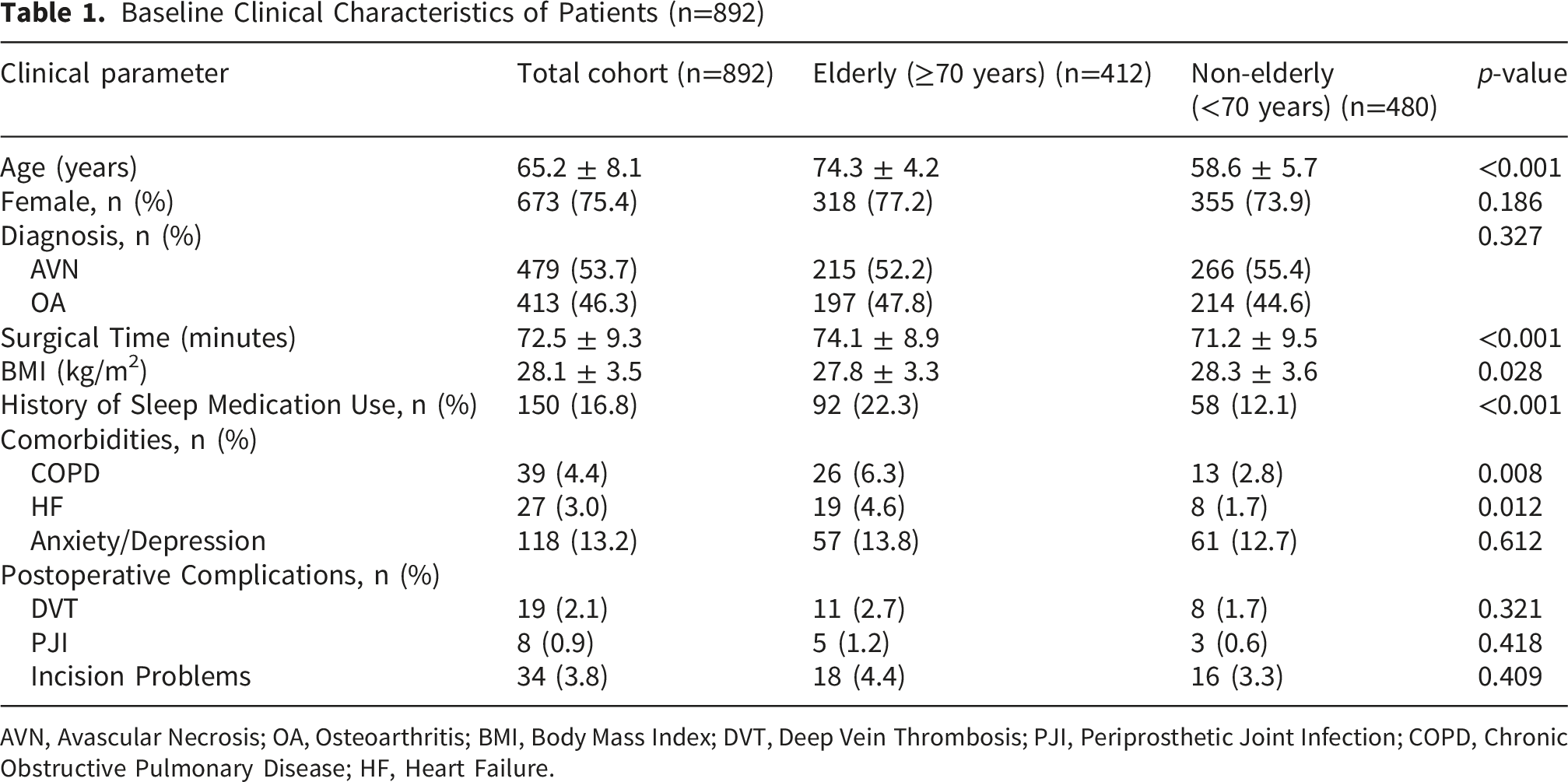
AVN, Avascular Necrosis; OA, Osteoarthritis; BMI, Body Mass Index; DVT, Deep Vein Thrombosis; PJI, Periprosthetic Joint Infection; COPD, Chronic Obstructive Pulmonary Disease; HF, Heart Failure.
Elderly patients had higher comorbidity rates [COPD: 6.3% versus (vs.) 2.8%; HF: 4.6% vs. 1.7%], higher preoperative sleep medication use (22.3% vs. 12.1%), and similar mental health comorbidity rates (anxiety/depression: 13.8% vs. 12.7%) compared to non-elderly patients.
Prevalence and Subtypes of Postoperative Sleep Disorders
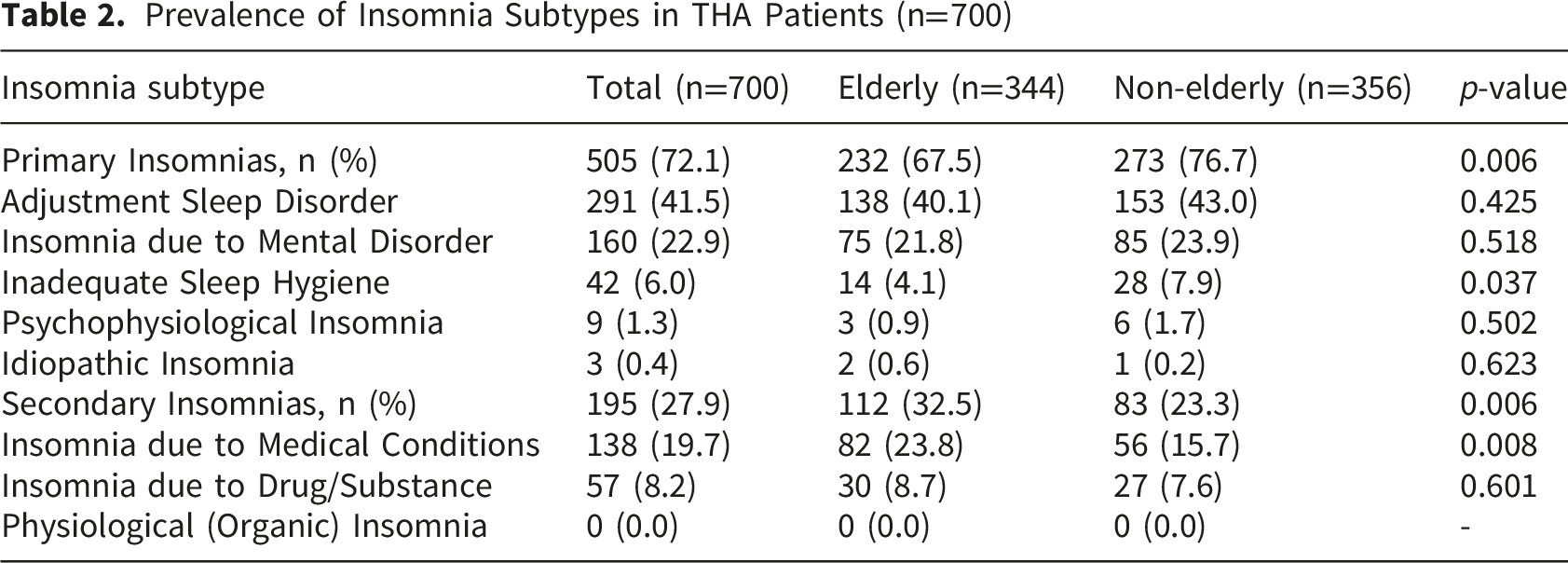
Prevalence of Insomnia Subtypes in THA Patients (n=700)
Factors Contributing to Postoperative Sleep Disorders
Factors Contributing to Postoperative Sleep Disorders (n=700)
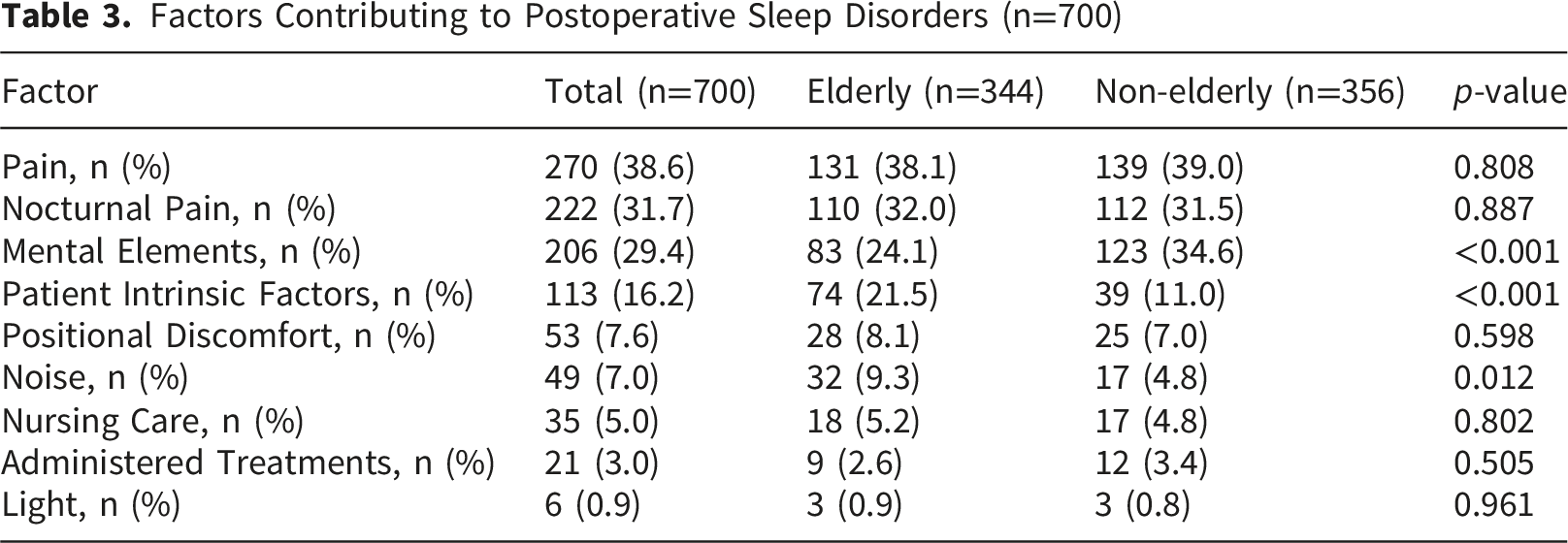
Elderly patients had a unique disruptor profile: more intrinsic factors (21.5% vs. 11.0%) and environmental noise (9.3% vs. 4.8%) compared to non-elderly patients.
Association Between Sleep Disorder Forms and Postoperative Outcomes
Comparisons Among Varied Forms of Insomnias (n=700)
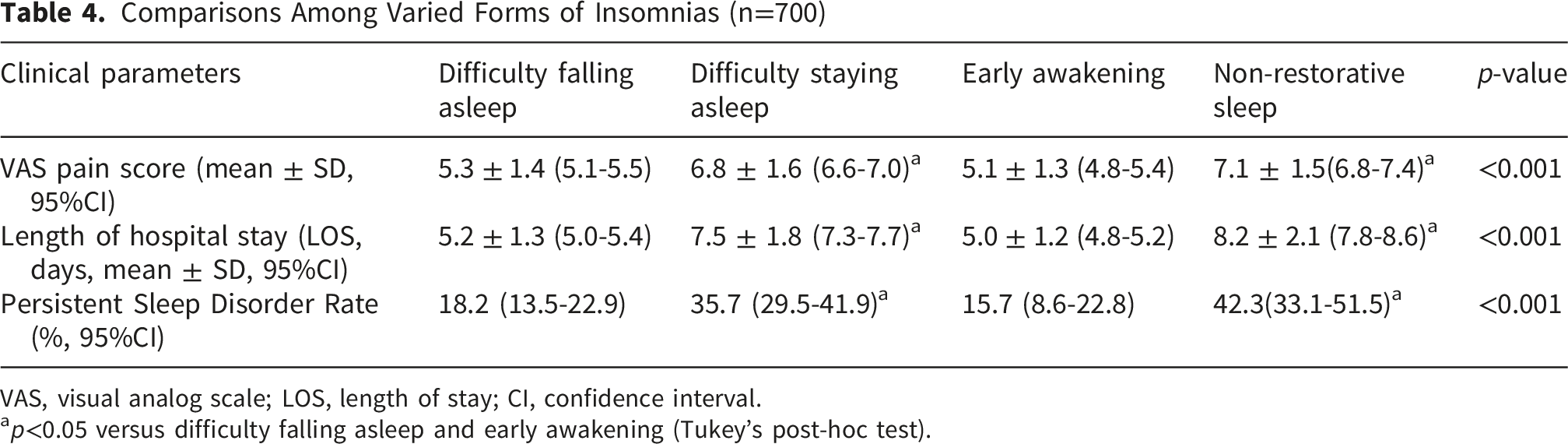
VAS, visual analog scale; LOS, length of stay; CI, confidence interval.
ap<0.05 versus difficulty falling asleep and early awakening (Tukey’s post-hoc test).
Comparison Between Different Perioperative Management Patterns (Elderly Subgroup Analysis)
A post-hoc analysis was conducted among 148 elderly patients. Statistically significant differences were detected between the personalized management group and the standard care group: the former had a lower rate of persistent sleep disorders (31.1% vs. 53.6%, p<0.001) and a shorter LOS (6.8 ± 1.5 days vs. 7.9 ± 1.8 days, p=0.002).
Discussion
This retrospective study explored postoperative sleep disturbance after THA, with a particular focus on elderly patients aged 70 years and older. Previous studies have reported high prevalence of sleep disturbances after total joint arthroplasty, but most focused on either THA or TKA without dedicated elderly subgroup analysis, and few used standardized ICSD-2 criteria to classify insomnia phenotypes in detail. Few large-sample studies have further analyzed the correlations between sleep subtypes, pain, hospitalization and persistent sleep disturbance.
Compared with previous literature, the present study has several novel strengths: First, this study used ICSD-2 standardized criteria to clarify the phenotypic distribution of postoperative insomnia, providing a clear classification for clinical identification. Second, this study enrolled a large sample of elderly patients and confirmed that advanced age is a strong independent risk factor for persistent sleep disturbance, which has not been fully emphasized in previous studies. Third, this study linked specific sleep subtypes (sleep maintenance difficulty, non-restorative sleep) to worse clinical outcomes, which reflect notable clinical correlations. Fourth, this study analyzed clinical characteristics among patients receiving age-specific sleep management schemes tailored to sleep disruptors in elderly THA patients, filling the gap of evidence-based sleep management strategies for this vulnerable population. Key findings emerged: Adjustment sleep disorder dominates as the most common subtype; Pain (notably nocturnal), psychological stressors, and intrinsic patient characteristics were closely associated with poor sleep, with elderly patients more affected by comorbidities and environmental noise; Sleep maintenance difficulties and non-restorative sleep correlate with inferior recovery outcomes, an association amplified in elderly patients; Distinctions in persistent sleep disturbance and postoperative indicators were noted between patients with different management patterns.14,15
The overall prevalence of postoperative sleep disturbance was high, with elderly patients demonstrating significantly greater vulnerability.2,5 Elderly patients exhibited a higher proportion of secondary insomnias, largely due to comorbidities (COPD, HF), reflecting age-related physiological changes and heightened comorbidity burdens. 10 This suggests that aging itself alters sleep architecture and increases vulnerability to internal and external disruptors, which clinicians should consider during risk stratification.
The finding that elderly patients have a 3.2-fold higher risk of persistent sleep disorders demands attention. Older patients often have reduced physiological reserve, less effective pain modulation, and higher sensitivity to environmental changes, all of which extend sleep disturbance beyond the acute postoperative phase. This suggests elderly patients require intensified perioperative care for associated risk factors that perpetuate sleep disturbance.16,17 Clinically, early attention to sleep-related issues is recommended for this population at admission.
Pain was the most common factor associated with sleep disruptors across all groups, aligning with biological mechanisms: circadian fluctuations reduce nighttime pain tolerance, as cortisol levels decline (diminishing anti-inflammatory effects) and pro-inflammatory cytokines surge (amplifying pain perception), but elderly patients present a unique profile.5,14,15 Mental stressors were more prominent in non-elderly patients, while elderly patients were more vulnerable to intrinsic factors and environmental noise. This pattern may be attributed to age-related declines in respiratory function and sensory acuity. 10 These factors compound the THA-specific challenge of positional discomfort, making sleep continuity particularly difficult to maintain. These differences imply that management priorities should vary by age group: psychological support may be more relevant for younger patients, while comorbidity control and environmental adjustment deserve more attention for the elderly.
Positional discomfort related to postoperative activity restrictions was a common cause of sleep disturbance. Relevant guidance on sleeping positions can be adopted in routine clinical care. Positional discomfort affects elderly and non-elderly patients equally. This underscores the need for interventions targeting this issue, such as pressure-relief cushions and alternative sleep position training, which are especially critical for elderly patients with fragile tissue elasticity. 18 This is a unique, surgery-specific target that can be addressed with simple, low-cost supportive tools in routine ward care.
Sleep maintenance difficulties and non-restorative sleep were closely linked to unfavorable perioperative profiles, including: higher pain scores, longer LOS, and elevated persistent sleep disorder rates. This pattern is amplified in elderly patients. These sleep subtypes reflect severely fragmented sleep and impaired restorative function, rather than mild onset insomnia. Patients with these sleep patterns tend to have prolonged recovery, so early attention to their sleep status is recommended clinically.
These findings highlight a bidirectional association between sleep and recovery: poor sleep was associated with worse pain and delayed rehabilitation, while unaddressed pain and functional limitations further disrupt sleep.5,16,18 For elderly patients, breaking this cycle is uniquely challenging. Different perioperative management approaches were correlated with varied recovery profiles.17,19 These associations indicate that sleep status is closely linked to rehabilitation progress and hospital stay duration.
Based on the observed associations and previous evidence,3,6,9,10 we put forward targeted perioperative management suggestions for elderly total hip arthroplasty (THA) patients: perioperative analgesia optimization involving multimodal analgesia (extended-release nonsteroidal anti-inflammatory drugs + nocturnal acetaminophen + local nerve blocks) to target nocturnal pain, while steering clear of high-dose opioids to avoid sedation and confusion that can worsen sleep19,20; comorbidity management through collaboration with internal medicine specialists to optimize preoperative and postoperative care for comorbidities such as COPD and HF, including adjusting HF medications to reduce nocturnal dyspnea and prescribing bronchodilators for COPD patients to improve sleep-related breathing 10 ; sleep-friendly environmental adjustments encompassing noise reduction (soundproof curtains, silent alarms), clustered nursing care to minimize nighttime disruptions, dimmed evening lighting, and provision of earplugs and eye masks for patients sensitive to environmental stimuli17,20; and positional support involving pressure-relief cushions, instruction on alternative sleep positions (e.g., side-lying with a pillow between knees) to alleviate discomfort from hip restrictions, and adjustment of rehabilitation protocols to gradually expand positional flexibility. 18
Clinical and Rehabilitation Implications for Perioperative Management
This study provides evidence-based nursing implications for managing postoperative sleep disorders in THA patients, especially elderly cohorts, and optimizing perioperative nursing care. First, individualized pain assessment and management are essential: the care team should conduct regular nocturnal pain assessments (at least every 4 hours) for THA patients, especially those with VAS pain scores ≥4, and collaborate with physicians to adjust analgesic regimens timely (e.g., adding nocturnal acetaminophen) such measures may serve as clinical references for managing pain-related sleep disturbance, and these suggestions are in line with ERAS principles. Second, targeted psychological nursing is essential for patients with anxiety/depression: the care team can provide preoperative psychological counseling, guide patients to use relaxation techniques (e.g., deep breathing, progressive muscle relaxation) during hospitalization, and manage sleep issues caused by psychological stress. Third, sleep-friendly ward environment optimization should be implemented: the care team can adopt clustered nursing care to minimize nighttime disruptions (e.g., concentrate vital sign monitoring, medication administration), install soundproof curtains to reduce noise, and dim evening lighting to create a better sleeping environment, especially for elderly patients sensitive to environmental stimuli. Fourth, elderly-specific nursing support is needed: for patients aged ≥70 years, the care team can provide positional guidance (e.g., side-lying with a pillow between knees) to reduce THA-specific positional discomfort, and assist with early functional exercise under the premise of safety to shorten hospital stay and reduce sleep disturbance caused by prolonged hospitalization. Finally, preoperative sleep health education should be integrated into routine nursing: the care team can educate patients on sleep hygiene knowledge (e.g., avoiding caffeine before bedtime, maintaining a regular sleep schedule) preoperatively to improve patients’ sleep self-management ability.
This study has several limitations. First, sleep assessment was based on subjective questionnaires rather than objective tools such as PSG, which may overestimate or underestimate disturbances compared to objective measures. Second, this is a single-center retrospective study performed by a single surgical team with unified implant selection and standardized institutional protocols, and all participants were exclusively enrolled from Chinese patients, which limits the generalizability of our findings and rehabilitation recommendations to other regions, ethnic groups and medical centers. Third, the intervention analysis was performed in a post-hoc non-randomized manner, without clear group allocation or prospective control, which may introduce selection bias and treatment allocation bias. All observed relationships should be interpreted as associations rather than definite causality. Fourth, Long-term sleep outcomes were not assessed, and the current follow-up duration may not fully reflect prolonged sleep outcomes. Although we adjusted for major confounders including preoperative pain and preoperative sleep quality in the regression model, residual confounding cannot be completely ruled out. Fifth, although the definitions of sleep disturbance resolution and persistent sleep disorder were based on validated thresholds from previous literature, they still relied on subjective VAS assessment without strict objective instrumental validation. The non-randomized post-hoc comparison between personalized intervention and standard care cannot confirm definite intervention efficacy. These findings remain hypothesis-generating and are intended to guide future prospective trials, rather than supporting immediate widespread clinical implementation. Despite these limitations, this study provides real-world evidence regarding postoperative sleep disorders in elderly THA patients.
Conclusions
Postoperative sleep disorders are highly prevalent in elderly patients undergoing THA, with advanced age constituting a major risk factor for persistent sleep disturbance. Adjustment sleep disorder is the most common subtype, while sleep maintenance difficulty and non-restorative sleep are associated with worse pain outcomes and longer hospital stays. Pain, psychological factors, comorbidities, and environmental disruptions represent key contributors to sleep disturbance. Distinctions in sleep status and rehabilitation indicators were observed between patients receiving different perioperative management plans. Routine risk screening and targeted sleep care are recommended for this patient group. All above associations require further verification in prospective studies.
Supplemental Material
Supplemental Material - Postoperative Sleep Disorders in Elderly THA Patients: Phenotypes, Risk Factors, and Perioperative Rehabilitation Strategies: A Single-Center Retrospective Observational Study
Supplemental Material for Sleep Disorders in Elderly THA Patients: Phenotypes, Risk Factors, and Perioperative Rehabilitation Strategies: A Single-Center Retrospective Observational Study by Jinqiang Chen, Bin Ma, Kunpeng Fu, Hui Zhang, Yang Yu, Xiaoli Zhang and Zhenhu Wang in Geriatric Orthopaedic Surgery & Rehabilitation.
Footnotes
Acknowledgments
We thank the patients who participated in this study, and the nursing and medical staff for their invaluable assistance.
Ethical Considerations
The study was approved by the Institutional Review Board of the Hospital of 82nd Group Army PLA (formerly 252 Hospital of Chinese PLA) (Approval No.: Orth-C-2025-12).
Consent to Participate
Informed consent was waived due to the retrospective design of this study. The study was conducted in accordance with the Declaration of Helsinki.
Author Contributions
ZHW conceptualized the study. HZ, YY and XLZ collected data. JQC, BM, KPF and ZHW performed surgeries and contributed to manuscript preparation. JQC and BM wrote the manuscript and assisted with formatting and study overview. YY provided statistical consultation. JQC and BM contributed to manuscript preparation. All authors reviewed and edited the manuscript and approved the final version.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The raw clinical data generated and analyzed during this study are not publicly available due to patient privacy protection and institutional data management regulations. Qualified researchers may request access to the corresponding author for reasonable academic purposes after formal application.
Reporting Guidelines Compliance
This retrospective observational cohort study was conducted in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Guidelines. The completed STROBE Checklist for Cohort Studies is available as a supplementary file.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.