
Abstract
Objective
Unicompartmental knee arthroplasty (UKA) offers potential advantages over total knee arthroplasty, but evidence regarding its efficacy in patients aged over 75 years remains limited. This comparative study evaluates clinical outcomes following UKA in patients aged ≥75 years and compares mobile-bearing (MB) versus fixed-bearing (FB) prostheses in this population.
Methods
We conducted a retrospective cohort study of 189 consecutive patients aged ≥75 years who underwent UKA for medial compartment osteoarthritis (June 2021-December 2022). The cohort comprised 118 MB and 71 FB prostheses. Demographic data, perioperative complications, and patient-reported outcome measures (Knee Society Score [KSS], Oxford Knee Score [OKS], Visual Analogue Scale [VAS] for pain, and Forgotten Joint Score-12 [FJS-12]) were collected preoperatively and at minimum 12-month follow-up. Wilcoxon signed-rank and Mann-Whitney U tests were used for within- and between-group comparisons, respectively.
Results
Mean follow-up was 25 months (range, 12-36 months), with no losses or deaths. Significant improvements occurred across all outcomes. Median KSS clinical score improved from 30.00 to 91.00 (P < 0.001); KSS functional from 25.00 to 70.00 (P < 0.001); OKS from 40.00 to 18.00 (P < 0.001); and VAS pain from 6.00 to 1.00 (P < 0.001). One patient (0.5%) experienced a minor cardiac event; no revisions, infections, or bearing complications occurred. No significant differences were observed between MB and FB groups for any outcome measure, including FJS-12 (median 100 both groups; P = 0.359).
Conclusion
UKA provides significant, clinically meaningful improvements in pain and function for patients aged ≥75 years with medial compartment osteoarthritis, with low complication rates and excellent joint awareness. Both MB and FB prostheses yield equivalent outcomes. Advanced age alone should not contraindicate UKA.
1. Introduction
Knee osteoarthritis (KOA) represents a leading cause of functional disability among elderly populations worldwide, with prevalence increasing proportionally with population aging.1,2 In China, the rapidly growing cohort of individuals aged 75 years and older poses particular challenges for orthopedic management, as this demographic exhibits both a high osteoarthritis burden and reduced physiological reserve.3,4 Elderly patients frequently present with complex comorbidities affecting cardiovascular, respiratory, and neurological systems that may destabilize during the perioperative period, necessitating surgical approaches that minimize physiological insult while optimizing functional recovery. 5 When conservative measures exhaust their therapeutic utility, the selection of a procedure that balances definitive joint reconstruction with reduced tissue trauma and accelerated rehabilitation assumes paramount importance.
Total knee arthroplasty (TKA) has historically constituted the conventional surgical approach for advanced KOA with varus deformity, demonstrating reliable long-term outcomes across diverse patient populations. 6 However, a substantial proportion of patients presenting with medial compartment osteoarthritis demonstrate intact cruciate ligaments and preserved lateral compartments, rendering them suitable candidates for joint-preserving alternatives. Unicompartmental knee arthroplasty (UKA) has emerged as a compelling treatment modality, offering advantages such as preservation of the cruciate ligaments, maintenance of native knee kinematics, reduced soft-tissue disruption, and accelerated postoperative recovery compared with TKA.7,8 Contemporary evidence from randomized controlled trials and registry analyses has substantiated these benefits, demonstrating shorter hospitalization periods, more rapid return to functional activities, and enhanced patient-reported outcomes following UKA in appropriately selected patients.9-12
Within the domain of Unicompartmental arthroplasty, two principal prosthetic design philosophies have evolved: mobile-bearing (MB) and fixed-bearing (FB) implants, each embodying distinct biomechanical principles and surgical requirements. 13 Mobile-bearing designs feature a freely mobile polyethylene insert that optimizes articular conformity and, theoretically, reduces polyethylene wear, while fixed-bearing designs provide inherent stability and eliminate the risk of bearing dislocation. The comparative performance of these designs has generated substantial scholarly discourse, with systematic reviews yielding heterogeneous conclusions regarding clinical outcomes, survivorship, and complication profiles.14-16 Some investigators have reported superior clinical outcomes with FB prostheses, while others have demonstrated enhanced alignment correction with MB designs. 17 Patient satisfaction comparisons have yielded similarly divergent results, with some studies reporting superior satisfaction with MB prostheses and others failing to detect significant differences.18,19
Despite the expanding evidence base supporting UKA utilization, a critical knowledge gap persists regarding the specific applicability and comparative effectiveness of MB versus FB prostheses in the very elderly population aged 75 years and older. Existing comparative studies have predominantly enrolled younger, higher-demand patient cohorts, leaving the unique considerations of geriatric patients inadequately addressed. This demographic omission is particularly significant given the distinct physiological characteristics, functional expectations, and risk-benefit calculus governing surgical decision-making in octogenarians and beyond. Very elderly patients may derive differential benefits from specific prosthetic designs based on factors including activity level, bone quality, ligamentous integrity, and the relative importance of minimizing perioperative complications versus achieving optimal long-term kinematic performance. Furthermore, the limited existing data on UKA outcomes in advanced-age populations rarely distinguish between bearing designs, precluding evidence-based guidance for surgeons managing this growing patient demographic.
The present comparative study addresses this evidence gap by systematically evaluating the clinical outcomes of UKA specifically in patients aged over 75 years, with particular emphasis on comparative analysis between MB and FB prosthetic designs. By focusing exclusively on the very elderly population and providing direct comparison between contemporary MB and FB implants, this investigation aims to generate clinically actionable evidence to inform prosthesis selection, perioperative management strategies, and patient counseling. The findings have potential significance for optimizing surgical approaches to medial compartment osteoarthritis in geriatric patients, potentially contributing to improved functional outcomes, reduced complication rates, and enhanced quality of life in the fastest-growing segment of the arthroplasty candidate population. We hypothesize that both bearing designs will demonstrate significant clinical improvement, and we sought to determine whether any clinically meaningful differences exist between MB and FB prostheses in this elderly cohort.
2. Methods
2.1. Study Design and Patient Population
This retrospective comparative cohort study included 189 consecutive patients aged 75 years or older who underwent UKA for medial compartment knee osteoarthritis at our institution between June 1, 2021, and December 31, 2022. All surgeries were performed during this 19-month period, with patient enrollment continuing until the target sample size was achieved. The study was conducted in Fengfeng General Hospital of North China Medical and Health Group, Handan Orthopedic Hospital, Handan, China. This study sought to answer the following primary research question: In patients aged 75 years and older with medial compartment osteoarthritis, do clinical outcomes differ between mobile-bearing (MB) and fixed-bearing (FB) unicompartmental knee arthroplasty (UKA)? The study was designed to compare clinical outcomes between mobile-bearing and fixed-bearing prostheses. The cohort comprised 45 male and 144 female patients, with 118 patients receiving mobile-bearing (MB) prostheses and 71 patients receiving FB prostheses. All patients underwent unilateral UKA. Of the 189 procedures, 102 (54.0%) were performed on the left knee and 87 (46.0%) on the right knee. No bilateral procedures were included in this study.
2.2. Inclusion and Exclusion Criteria
2.2.1. Inclusion Criteria
Patients were considered eligible for inclusion if they met the following criteria: 1 confirmed diagnosis of medial compartment knee osteoarthritis with Kellgren-Lawrence grade III or IV, with predominant pain localized to the medial compartment; 2 preoperative knee range of motion ≥90°, flexion contracture ≤15°, and varus deformity ≤15°; 3 functionally intact anterior and posterior cruciate ligaments as assessed clinically and by preoperative imaging; and 4 availability of complete preoperative and minimum 12-month postoperative clinical data.
2.2.2. Exclusion Criteria
Exclusion criteria were: 1 significant patellofemoral joint osteoarthritis characterized by groove-like changes or bone loss on axial radiographs; 2 prior knee surgery including high tibial osteotomy, arthroscopic procedures, or open reduction internal fixation; 3 inflammatory arthropathy or crystal arthropathy; 4 neurological deficits affecting lower limb function, including sequelae of cerebrovascular accidents with residual weakness; 5 cervical or lumbar spine pathology with radicular symptoms (e.g., radiating pain, numbness, or weakness in a dermatomal distribution) that could mimic or confound knee-related pain, as determined by clinical examination. Patients with isolated axial back pain without radicular symptoms were not excluded; and 6 contraindications to UKA identified on advanced imaging, including anterior cruciate ligament insufficiency or lateral compartment bone loss.
2.3. Preoperative Evaluation
All patients underwent standardized preoperative imaging, including weight-bearing anteroposterior and lateral knee radiographs, patellofemoral axial views, and full-length lower-limb alignment films. Magnetic resonance imaging was performed selectively when clinical examination or radiographs raised suspicion of cruciate ligament insufficiency, osteonecrosis, or occult lateral compartment disease that might contraindicate UKA.
2.4. Surgical Technique and Prosthesis Selection
All procedures were performed by experienced arthroplasty surgeons utilizing a standardized minimally invasive approach. Under regional or general anesthesia, the patient was positioned supine with a tourniquet applied to the proximal thigh. A midline skin incision of approximately 8-10 cm was made, followed by a medial parapatellar capsular approach. The quadriceps tendon was not incised, and the patella was retracted laterally without eversion. Anterior tibial osteophytes were excised to facilitate exposure. The medial compartment was inspected to confirm cartilage loss confined to the medial femoral condyle and medial tibial plateau with an intact anterior cruciate ligament and preserved lateral compartment.
Tibial preparation was performed first using extramedullary guides, followed by femoral preparation using intramedullary or extramedullary guides according to the specific prosthesis system. For mobile-bearing (Oxford, Zimmer Biomet) prostheses, particular attention was paid to achieving balanced flexion-extension gaps and restoring medial collateral ligament tension to prevent bearing dislocation. For fixed-bearing prostheses, 1-2 mm of laxity in extension and 2-3 mm of laxity in flexion were accepted. Trial components were inserted, and range of motion, ligamentous balance, and component stability were assessed. Final components were cemented in place. After cement hardening, the wound was irrigated, and closure was performed in layers.
The choice between mobile-bearing and fixed-bearing prostheses was determined by surgeon preference, patient anatomy, and intraoperative assessment of ligamentous balance. Both groups underwent identical postoperative rehabilitation protocols emphasizing early range of motion, immediate weight-bearing as tolerated, and progressive strengthening exercises.
The higher proportion of MB prostheses (118 vs. 71) reflected surgeon preference during the study period, as the senior authors had greater experience with the Oxford mobile-bearing system. MB prostheses were preferentially selected for patients with well-preserved ligamentous balance and minimal varus deformity, while FB prostheses were more commonly used in cases with mild residual laxity or when concerns about bearing dislocation risk existed.
2.5. Data Collection and Outcome Measures
2.5.1. Demographic and Clinical Data
Demographic and clinical data collected included age, sex, height, weight, body mass index (BMI), and length of hospital stay. Perioperative complications were documented, including cardiovascular events, thromboembolic phenomena, wound complications, and prosthesis-related issues such as dislocation, loosening, or infection requiring reoperation.
2.5.2. Functional Outcome Measures
Functional outcomes were assessed using validated instruments administered preoperatively and at each postoperative follow-up visit.
2.5.2.1. Knee Society Score (KSS)
The Knee Society Score comprises separate clinical (100 points) and functional (100 points) subscales. Higher scores indicate better knee function. The clinical subscale assesses pain (50 points), range of motion (25 points), and stability (25 points). The functional subscale assesses walking distance (50 points) and stair climbing ability (50 points).
2.5.2.2. Oxford Knee Score (OKS)
The Oxford Knee Score comprises 12 items assessing pain (5 items) and functional limitations (7 items). Each item is scored from 1 (best) to 5 (worst), yielding a total score of 12 to 60 points, with lower scores indicating better outcomes. The OKS is specifically validated for knee arthroplasty patients.
2.5.2.3. Visual Analogue Scale (VAS)
The Visual Analogue Scale for pain required patients to rate their average knee pain over the past week on a 0 to 10 scale, where 0 indicates no pain and 10 represents the worst imaginable pain. This single-item measure has well-established reliability and validity.
2.5.2.4. Forgotten Joint Score-12 (FJS-12)
The Forgotten Joint Score-12 comprises 12 questions assessing the patient’s ability to forget about their artificial joint during daily activities (e.g., walking, sitting, lying in bed, standing, performing household chores). Each item is scored from 1 (never) to 5 (mostly), and scores are transformed to a 0-100 scale using the formula: (100 - [sum of scores - 12]/48 × 100). Higher scores indicate a greater degree of forgetting the joint and thus superior outcomes.
2.6. Follow-Up Assessment
Patients were routinely evaluated at 6 weeks, 3 months, 6 months, and annually thereafter at our outpatient clinic. For patients unable to attend in-person follow-up due to mobility limitations or distance, assessments were conducted via telephone interview using the same validated outcome measures (KSS, OKS, VAS, FJS-12). For this analysis, the most recent follow-up data were utilized, with a minimum follow-up duration of 12 months postoperatively. With a mean follow-up of 25 months (range, 12-36 months), this study reports short-term to mid-term clinical outcomes following UKA. Long-term outcomes (beyond 5 years) were not assessed and remain an important direction for future research.
2.7. Statistical Analysis
Statistical analyses were performed using SPSS version 25.0 (IBM Corp., Armonk, NY, USA). Continuous variables were assessed for normality using the Shapiro-Wilk test and are presented as mean ± standard deviation for normally distributed data or median with interquartile range (IQR) for non-normally distributed data. Categorical variables are presented as frequencies and percentages.
For within-group comparisons of preoperative and postoperative scores, paired-sample t-tests were employed for normally distributed data, while Wilcoxon signed-rank tests were used for non-normally distributed data. For between-group comparisons (MB versus FB prostheses), independent-samples t-tests or Mann-Whitney U tests were applied based on the data distribution. These comparative analyses were performed to evaluate whether any clinically meaningful differences existed between the two bearing designs. Statistical significance was set at P < 0.05 for all analyses.
2.8. Ethical Approval
This study was conducted in accordance with the Declaration of Helsinki and received approval from the Institutional Review Board of the authors’ affiliated institution (Approval Number: 2021-056-FHMUS). All procedures performed were part of routine clinical care. Informed consent was waived due to the retrospective nature of the study.
3. Results
3.1. Patient Flow and Baseline Characteristics
A total of 347 patients aged 75 years or older who underwent UKA for medial compartment osteoarthritis were assessed for eligibility during the study period from June 2021 to December 2022. Following application of inclusion and exclusion criteria, 158 patients were excluded: 64 patients had prior knee surgery, 52 patients exhibited significant patellofemoral osteoarthritis, and 42 patients had incomplete clinical data. The remaining 189 patients were included in the final analysis, comprising 118 patients who received MB prostheses and 71 patients who received FB prostheses. All 189 patients completed a minimum of 12-month follow-up, with no patients lost to follow-up or deceased during the study period. The patient selection process is illustrated in Figure 1. Patient selection flowchart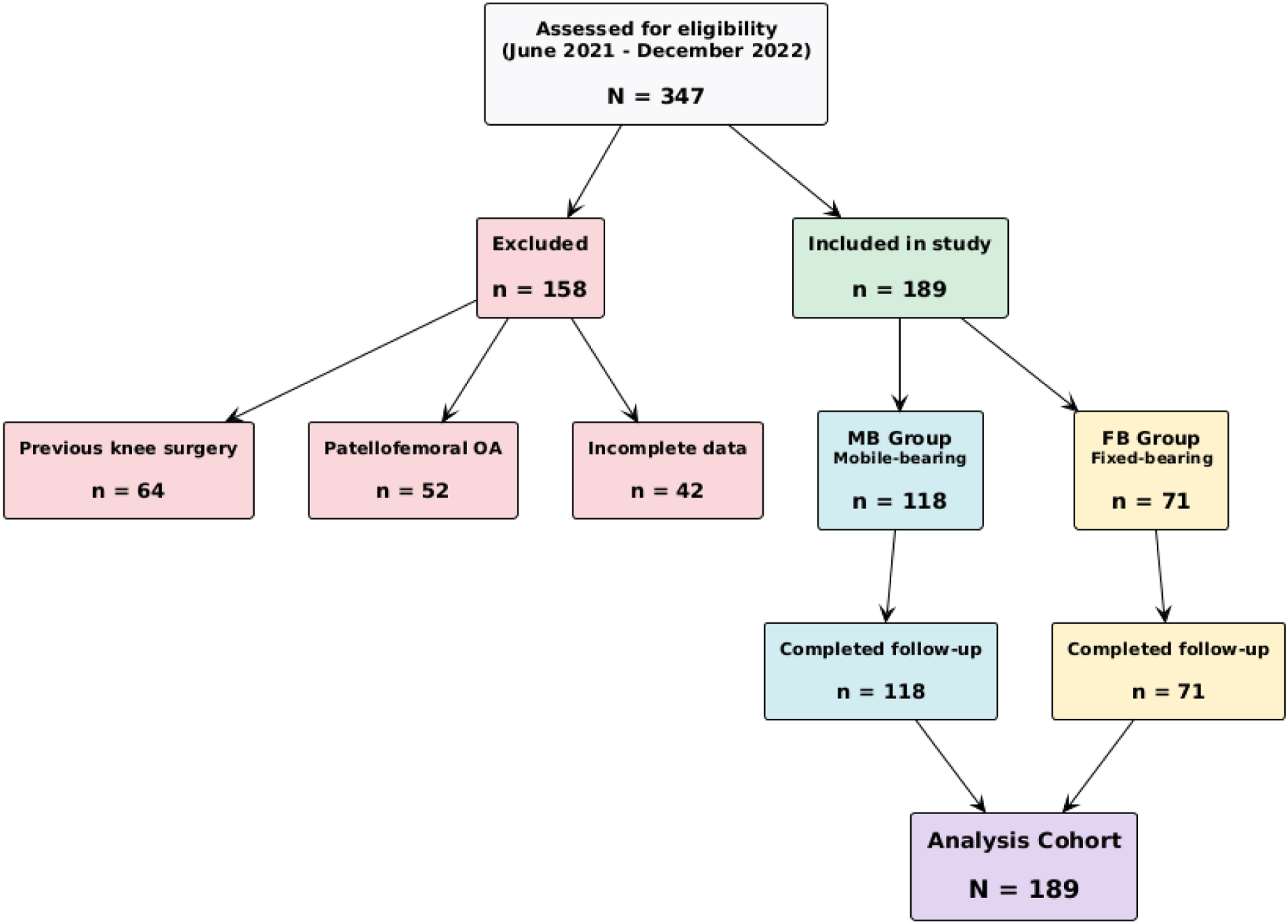
Patient Demographics and Baseline Characteristics
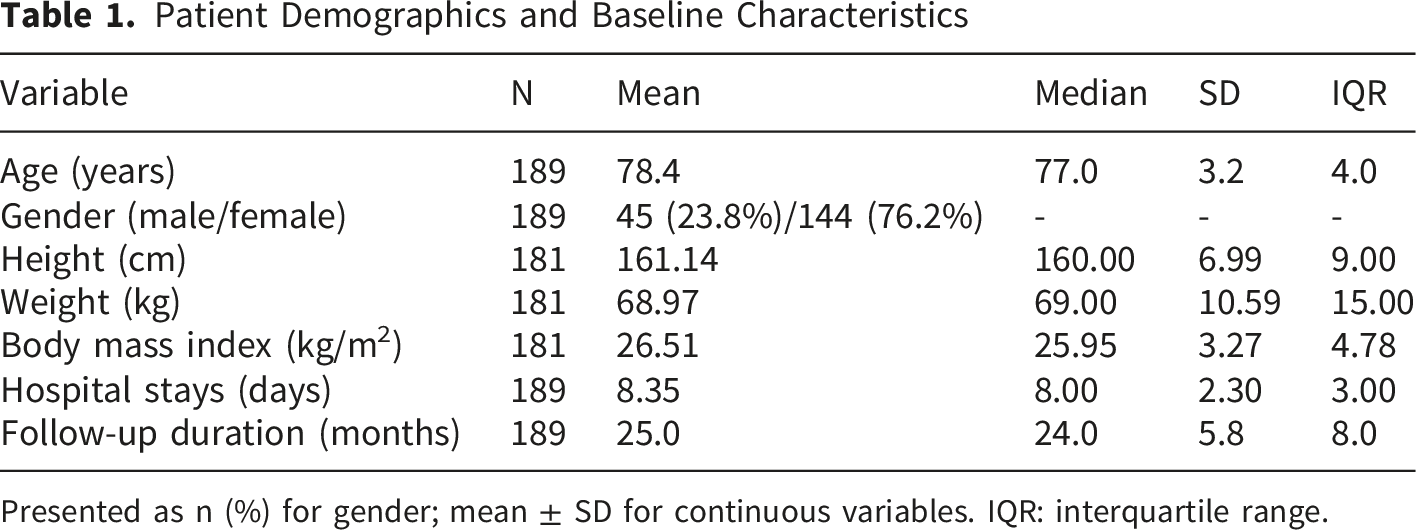
Presented as n (%) for gender; mean ± SD for continuous variables. IQR: interquartile range.
3.2. Perioperative Complications
Perioperative complications were assessed during the first 12 postoperative days. No mortalities occurred in either group. One patient (0.5%) in the mobile-bearing group experienced a postoperative cardiac event that resolved with conservative management, and the patient was discharged without sequelae. There were no instances of prosthetic dislocation, component loosening, surgical site infection, revision surgery, thromboembolic events, blood glucose fluctuations, gastrointestinal disturbances, or urinary retention in either group. Both mobile-bearing and fixed-bearing prostheses demonstrated excellent safety profiles with no between-group differences in complication rates.
3.3. Postoperative Functional Recovery
All patients achieved 90° of knee flexion within the first postoperative week (mean flexion at discharge: 94.3° ± 4.2°) and 120° of flexion by three months postoperatively (mean flexion at 3 months: 123.7° ± 5.1°). All patients successfully completed straight leg raise exercises without quadriceps lag by postoperative day 3, indicating early recovery of quadriceps function and extensor mechanism integrity. All patients were ambulatory with assistive devices by postoperative day 1 and progressed to independent ambulation prior to hospital discharge.
3.4. Overall Clinical Outcomes
Significant improvements were observed across all patient-reported outcome measures following UKA. Figure 2 visually demonstrates the magnitude of improvement from preoperative to postoperative assessment for all four outcome measures, with each showing marked enhancement following surgical intervention. Preoperative versus postoperative clinical outcome scores. Bar chart showing significant improvements in all four patient-reported outcome measures following UKA in N = 189 patients aged over 75 years. Data are presented as mean scores with standard deviation error bars. Lower OKS and VAS scores indicate better function and less pain, respectively. All comparisons were statistically significant using two-tailed Wilcoxon signed-rank tests (exact P values: KSS Clinical <0.001, KSS Functional <0.001, OKS <0.001, VAS <0.001)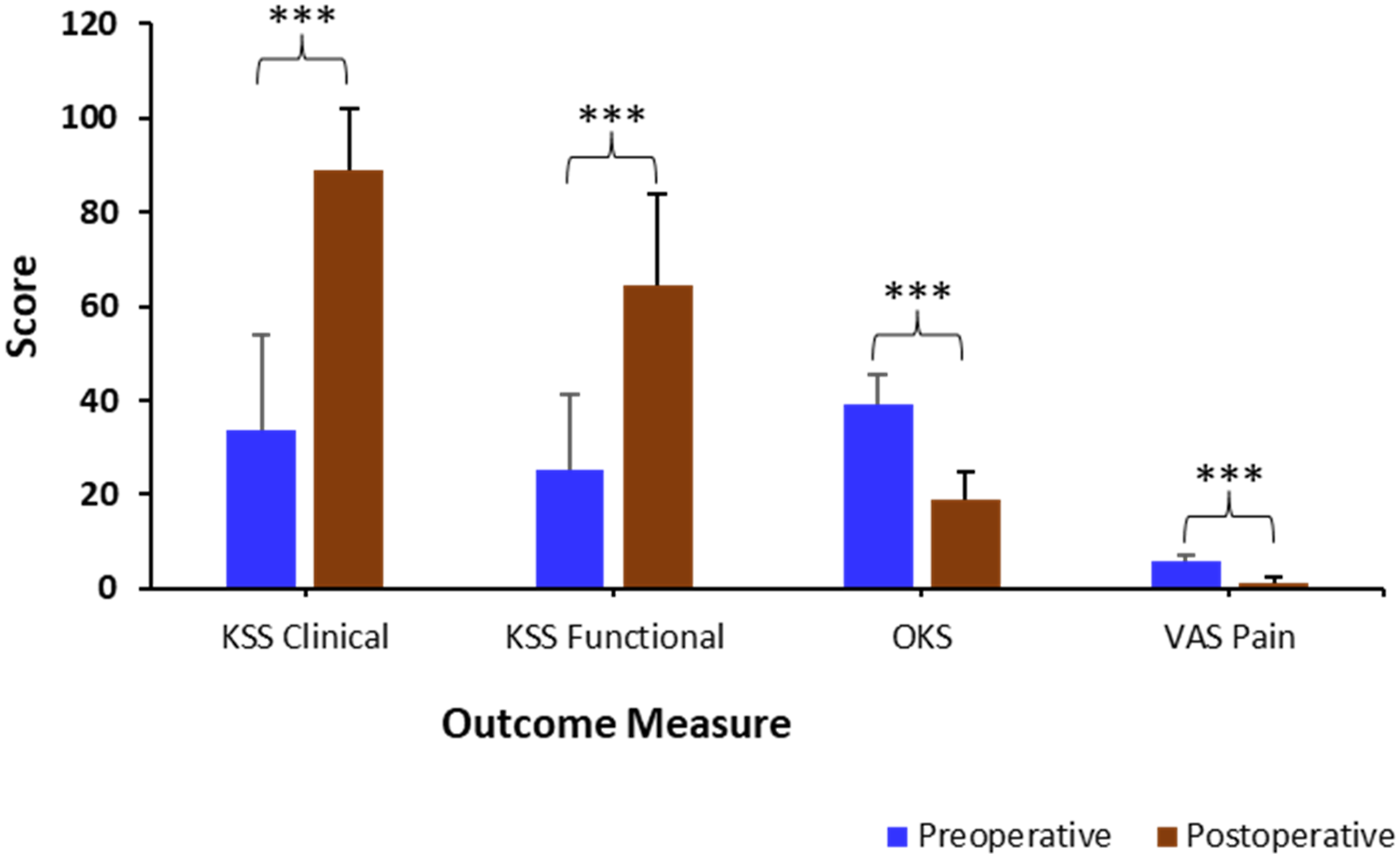
Comparison of Preoperative and Postoperative Clinical Outcomes for all Patients (N=189)
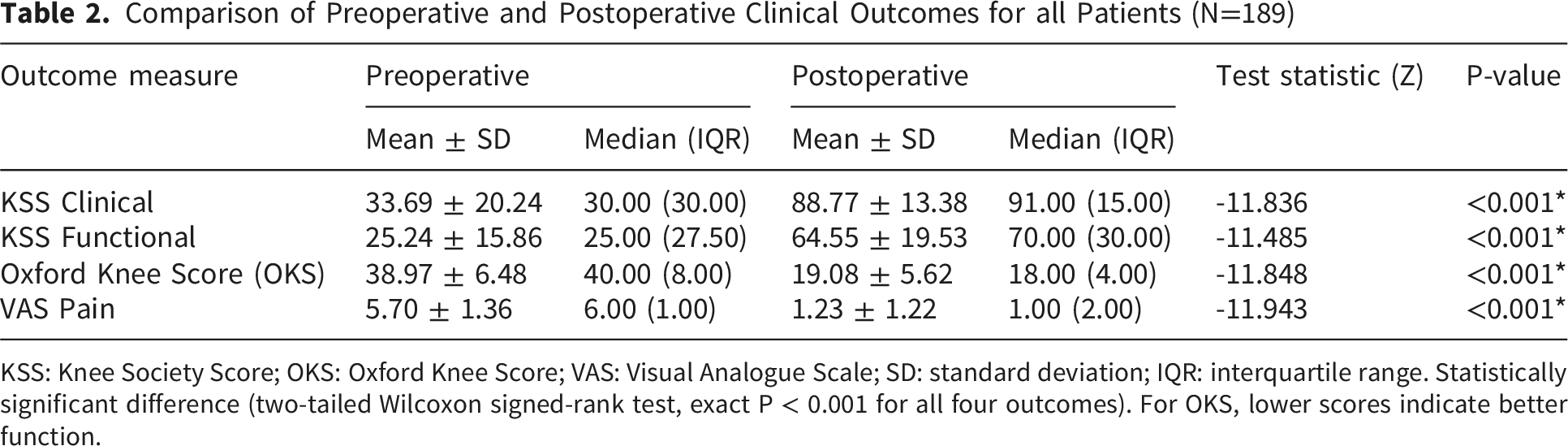
KSS: Knee Society Score; OKS: Oxford Knee Score; VAS: Visual Analogue Scale; SD: standard deviation; IQR: interquartile range. Statistically significant difference (two-tailed Wilcoxon signed-rank test, exact P < 0.001 for all four outcomes). For OKS, lower scores indicate better function.
3.5. Comparison of Mobile-Bearing and Fixed-Bearing Prostheses
3.5.1. Preoperative Comparability
Comparison of Clinical Outcomes Between Mobile-Bearing and Fixed-Bearing UKA
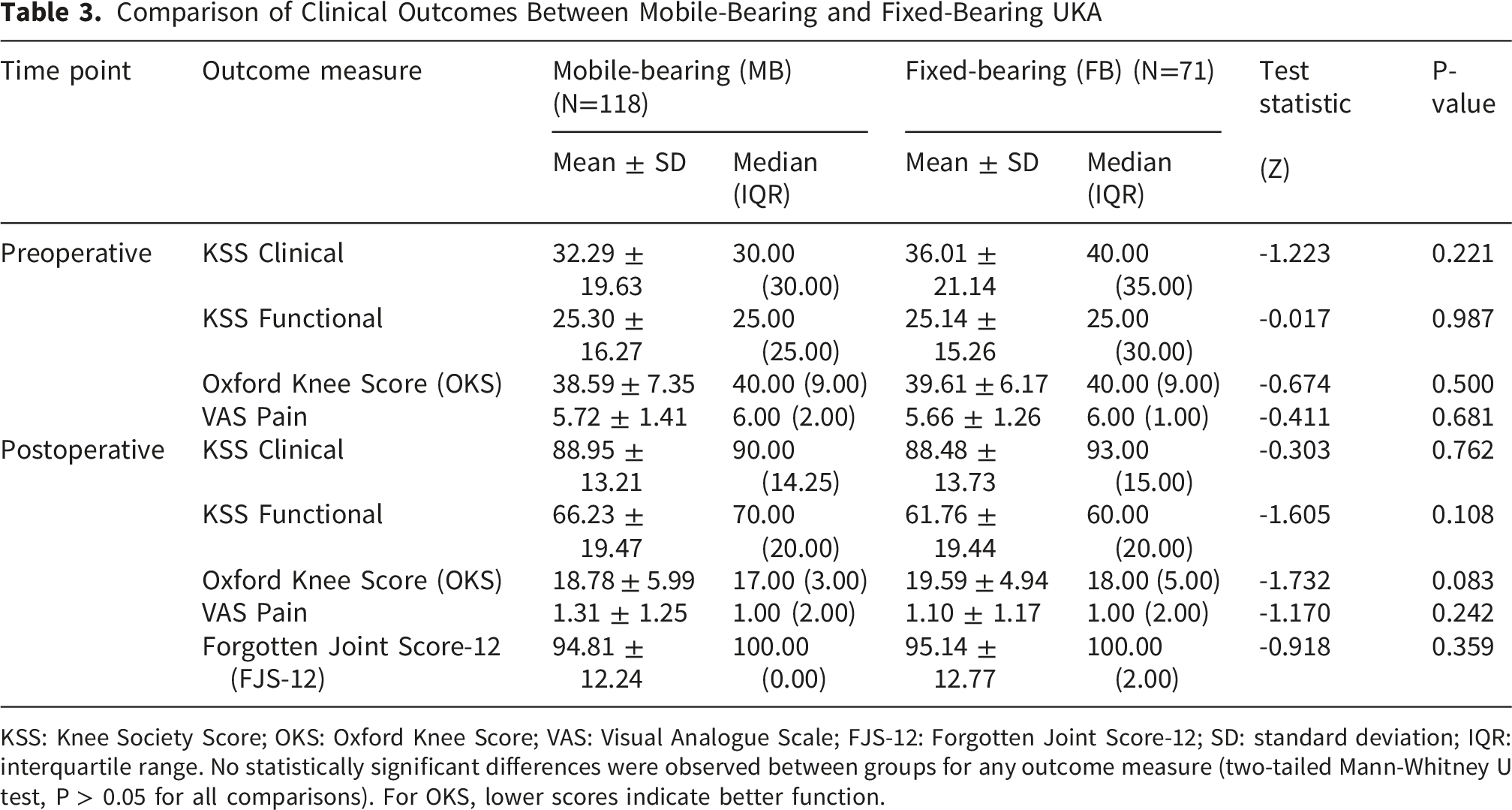
KSS: Knee Society Score; OKS: Oxford Knee Score; VAS: Visual Analogue Scale; FJS-12: Forgotten Joint Score-12; SD: standard deviation; IQR: interquartile range. No statistically significant differences were observed between groups for any outcome measure (two-tailed Mann-Whitney U test, P > 0.05 for all comparisons). For OKS, lower scores indicate better function.
3.5.2. Postoperative Outcomes
Both prosthesis types demonstrated significant improvements from preoperative baseline (all P < 0.001 within each group; within-group comparisons not shown in tables). However, comparison of postoperative outcomes between the MB and FB groups revealed no statistically significant differences in any of the measured parameters, including KSS clinical scores, KSS functional scores, OKS, VAS pain scores, or FJS-12 scores (Table 3).
Notably, the median Forgotten Joint Score (FJS-12) was 100 in both groups, with minimal interquartile ranges (MB: IQR 0.00; FB: IQR 2.00), indicating that patients in both cohorts achieved excellent joint forgetfulness postoperatively (Table 3). This ceiling effect suggests near-complete absence of joint awareness in this elderly population.
4. Discussion
This comparative study demonstrates that UKA provides significant clinical improvement in patients aged over 75 years with medial compartment osteoarthritis, with substantial enhancements observed across all patient-reported outcome measures, including KSS, OKS, and VAS for pain. Notably, these improvements exceeded established minimal clinically important differences, confirming not only statistical significance but also meaningful functional benefit for this elderly cohort. Furthermore, a comparative analysis of MB and FB prostheses revealed no statistically significant differences in any postoperative outcome measure, including the Forgotten Joint Score-12 (FJS-12), which showed excellent joint awareness outcomes with median scores of 100 in both groups. This comparative study was designed to answer whether clinical outcomes differ between MB and FB UKA in patients aged 75 years and older. The answer is that neither bearing design is superior to the other in this population. These findings suggest that both bearing designs are equally effective in this population, and that advanced age alone should not constitute a contraindication to UKA. This study was not designed to prioritize one outcome measure over another; rather, we assessed multiple validated instruments to provide a comprehensive comparison of MB versus FB prostheses.
The comparable outcomes between MB and FB prostheses observed in our elderly cohort align with several previous investigations, while contrasting with others, reflecting the ongoing debate regarding optimal bearing design in Unicompartmental arthroplasty. Kim et al 19 similarly reported no significant differences in KSS, WOMAC, or Tegner activity scores between MB and FB prostheses at a minimum 5-year follow-up in a cohort of 115 patients, although they observed superior FJS scores in the MB group. Our findings extend these observations to the very elderly population, demonstrating equivalent functional outcomes and, importantly, equivalent joint forgetfulness as measured by FJS-12.
However, our results differ from the meta-analysis by Huang et al 14 , which analyzed 1,861 patients with 1,996 knees and suggested that FB UKA achieved better clinical outcomes than MB designs, while MB prostheses demonstrated superior lower limb force line correction and reduced polyethylene wear. This discrepancy may reflect differences in study populations: the meta-analysis included predominantly younger patients with higher functional demands, whereas our cohort comprised exclusively patients aged over 75 years, whose activity levels and biomechanical requirements may differ substantially. Similarly, Bhattacharya et al 18 reported higher satisfaction rates with MB prostheses (93.9%) compared to FB designs (83.5%) in their series of 115 patients with a minimum three-year follow-up, a finding not replicated in our elderly population, where satisfaction, as reflected by FJS-12 scores, was equally high across both groups.
The excellent safety profile observed in our cohort, with only one minor cardiac event and no major complications, revisions, or infections, is consistent with previous studies examining UKA outcomes in elderly populations.15,16 These findings support the notion that UKA, when performed with appropriate patient selection and meticulous surgical technique, carries an acceptable risk even in patients of advanced age with potential comorbidities. The absence of bearing-related complications in both MB and FB groups further suggests that both designs can be safely implanted in elderly patients when surgical principles are respected.
The biomechanical differences between MB and FB prostheses warrant consideration in interpreting our results. MB designs require restoration of medial collateral ligament (MCL) tension to achieve balanced flexion-extension gaps and prevent bearing dislocation, a technically demanding aspect of the procedure that may influence outcomes in less experienced hands. FB designs, by contrast, accommodate 1-2 mm of laxity in extension and 2-3 mm in flexion, preserving some physiologic ligamentous laxity without dislocation risk. 17 Despite these design-specific technical requirements, our findings suggest that both approaches can yield equivalent clinical results in elderly patients when performed by experienced surgeons adhering to principles of minimally invasive technique.
The rapid functional recovery observed in our cohort, with all patients achieving 90° flexion within 1 week and 120° by 3 months, underscores the advantages of the minimally invasive approach. The 8-10 cm incision, quadriceps-sparing exposure, and avoidance of patellar eversion or dislocation facilitate early rehabilitation and may contribute to the low complication rates observed.11,12 These technical factors may be particularly relevant in elderly patients, for whom prolonged immobilization or delayed recovery carries a heightened risk of medical decompensation, muscle wasting, and functional decline.
Our findings carry several important implications for clinical practice. First, the substantial and clinically meaningful improvements observed across all outcome measures support the continued use of UKA in appropriately selected patients aged 75 years or older, challenging any residual notion that advanced age limits the benefits of joint arthroplasty. Second, the equivalent performance of MB and FB prostheses suggests that surgeon preference, familiarity, and intraoperative assessment of ligamentous balance may reasonably guide prosthesis selection without compromising patient outcomes. Third, the excellent safety profile, including the absence of bearing-related complications in either group, provides reassurance that both designs can be reliably implanted in elderly patients when surgical indications and techniques are appropriately observed.
The high FJS-12 scores observed (median 100 in both groups) are particularly noteworthy, as the ability to “forget” the artificial joint during daily activities represents a sophisticated measure of successful arthroplasty outcome. That elderly patients achieve this level of joint awareness, comparable to or exceeding that reported in younger populations 19 , suggests that UKA can restore not only objective functional capacity but also a subjective sense of normalcy in this age group.
4.1. Limitations and Future Directions
This comparative study has several limitations that warrant acknowledgement. First, the sample size of 189 patients, while adequate for detecting large treatment effects, may be insufficient to identify small but clinically meaningful differences between MB and FB prostheses, particularly for rare complications. Second, the mean follow-up duration of 25 months, although meeting minimum standards for early outcome assessment, precludes analysis of long-term implant survivorship, polyethylene wear, or late complications. Third, the retrospective design introduces potential selection bias, as prosthesis selection was not randomized but determined by surgeon preference and intraoperative findings. Fourth, the absence of radiographic outcome measures, including lower limb alignment correction and component positioning, limits our ability to correlate functional outcomes with mechanical factors that may influence long-term performance. Fifth, the single-center design may limit generalizability to other practice settings with different patient populations or surgical techniques. Sixth, the uneven distribution between MB (n=118) and FB (n=71) groups reflects surgeon preference rather than randomization, which may introduce selection bias. Surgeons preferentially selected MB prostheses based on greater familiarity with the Oxford system and for patients with better ligamentous balance. This imbalance is an inherent limitation of the retrospective design. Seventh, the lack of a comparative TKA group precludes direct comparison of UKA versus TKA outcomes in this elderly population, although extensive literature already addresses this comparison.7,8 Eighth, no a priori sample size calculation or power analysis was performed, as this was a retrospective study of consecutive patients. Therefore, the study may have been underpowered to detect small but clinically meaningful differences between MB and FB prostheses.
Future research should address these limitations through prospective, multicenter randomized controlled trials comparing MB and FB UKA specifically in elderly populations, with standardized surgical techniques, comprehensive radiographic assessment, and extended follow-up of at least five to ten years. Such studies should incorporate patient-reported outcome measures validated in geriatric populations, comprehensive reporting of complications, and cost-effectiveness analyses to inform healthcare resource allocation. Additionally, investigation of patient-specific factors, such as bone quality, activity level, and comorbidity burden, that may predict differential responses to bearing designs could enable more personalized prosthesis selection. Comparative effectiveness research examining UKA versus TKA in the very elderly, using large registry databases with propensity score matching, would further clarify the optimal surgical approach for this growing patient demographic.
5. Conclusion
This comparative study demonstrates that Unicompartmental knee arthroplasty provides significant, clinically meaningful improvements in pain and function for patients aged 75 years or older with medial compartment osteoarthritis. Both mobile-bearing and fixed-bearing prostheses yield excellent outcomes, with no significant differences in any patient-reported outcome measure, including the Forgotten Joint Score-12. Complication rates are low, recovery is rapid, and patients achieve high levels of joint awareness postoperatively. These findings support the continued use of UKA in appropriately selected elderly patients and confirm that advanced age alone should not constitute a contraindication to this joint-preserving procedure. Surgeons may reasonably select either bearing design based on personal preference and intraoperative assessment, with confidence that elderly patients can achieve satisfactory clinical outcomes.
Footnotes
Acknowledgements
The authors gratefully acknowledge the support and collaboration of their research colleagues, including the medical, nursing, and laboratory staff who contributed to the successful completion of this study. We are especially indebted to the participants for their willingness to take part in this research.
Ethical Consideration
This study was conducted in accordance with the Declaration of Helsinki and received approval from the Institutional Review Board (Approval number: 2021-056-FHMUS) of the authors’ affiliated institutions. All procedures performed were part of routine clinical care, and informed consent was waived due to the study’s retrospective nature.
Consent to Participate
Written informed consent was obtained from all participants before enrollment in the study. Participants were informed about the purpose, procedures, potential risks, and benefits of the study, and their right to withdraw at any time without affecting their medical care.
Consent for Publication
Consent for publication was obtained from all patients included in the study.
Authors’ Contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article:This work was supported by the Natural Science Foundation of Hebei Province [grant numbers H2021206093 and H2021206505]; the Research Foundation of Hebei Provincial Health Commission [grant number 20210068]; and the Research Foundation of Hebei Provincial Administration of Traditional Chinese Medicine [grant number 2019128]. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data generated or analyzed during this study are included this published article.
Trial Registration
The Institutional Review Board Approval number: 2021-056-FHMUS.
Grant Number
Grant numbers: H2021206093, H2021206505, 20210068 and 2019128.