
Abstract
Background
Postoperative pulmonary complications (PPCs) are common surgical complications and have a significant cost impact. However, the incidence, risk factors, and cost burden of US health care associated with PPCs after spine fusion surgery have not been comprehensively analyzed through large national databases.
Methods
A retrospective analysis utilized the Nationwide Inpatient Sample (NIS) database from 2010 to 2019. Adult patients (≥18 years) undergoing spinal fusion were identified via ICD-9-CM/ICD-10-CM procedural codes. PPCs—defined as pneumonia, acute respiratory failure (ARF), pulmonary embolism, or pulmonary edema—were identified by diagnostic codes. Multivariate and stratified logistic regression analyses examined overall and subtype-specific risk factors.
Results
Among 812,609 patients, 17,121 (2.11%) developed PPCs, including 9,591 (1.18%) with ARF, 7,376 (0.91%) with pneumonia, 2,159 (0.27%) with pulmonary embolism, and 553 (0.07%) with pulmonary edema. The overall PPCs’ rate increased from 2014 to 2019, driven primarily by rising ARF incidence. Patients with PPCs had longer hospital stays (9 vs. 3 days), higher total charges ($197,994 vs. $85,233), and greater in-hospital mortality (5.82% vs. 0.08%, all P < 0.001). Multivariate analysis identified advanced age (≥75: OR = 1.86), multiple comorbidities (OR = 10.98), pulmonary circulation disorders (OR = 11.38), continuous trauma ventilation (OR = 13.34), and septicemia (OR = 14.34) as high-risk factors. Stratified analyses revealed distinct risk profiles: impaired pulmonary reserve and frailty were associated with pneumonia and ARF; venous thromboembolism risk factors with pulmonary embolism; and cardiac, renal, and fluid-related disorders with pulmonary edema. Protective factors included female sex (OR = 0.70), elective admission (OR = 0.32), lumbar fusion (OR = 0.76), and private insurance (OR = 0.89).
Conclusion
PPCs after spinal fusion are increasing, primarily due to rising ARF rates. These complications exhibit clinically distinct risk profiles that support subtype-specific assessment and individualized prevention strategies targeting pulmonary reserve, thromboembolic risk, and cardiopulmonary vulnerability.
Keywords
1. Introduction
An increasing trend in spinal fusion surgeries has been observed due to the increasing demand from the aging population and the development of novel spinal fixation devices. 1 Between 1990 and 2014, there was an overall 118% increase in spine fusion surgeries across the US. 1 A comprehensive understanding of the major complications after spinal fusion surgery is essential for assessing the potential healthcare burden. Postoperative pulmonary complications (PPCs), mainly including acute respiratory failure (ARF), pneumonia, pulmonary edema, and pulmonary embolism, 2 are some of the most common and serious complications after spinal fusion. 3 The reported incidence of PPCs following spinal fusion ranges from 0.40% to 13.90%,4-11 which varies among different studies, mainly depending on the patient population and the range of pulmonary complications.2,10,11 Patients with PPCs have also significantly strained healthcare resources by extending hospital stays and escalating medical expenses.12-14 Additionally, PPCs have an adverse impact on patients and family members, as they are associated with progressive functional impairment, higher mortality, and other complications like sepsis, myocardial infarction, and postoperative delirium.4,15,16
Identifying whether patients have high risks of PPCs is crucial to optimizing postoperative outcomes and reducing complications. Previous studies have reported several risk factors for PPCs, among which older age is the most frequently acknowledged.55,10,17,18 Other risk factors, including pre-existing pulmonary conditions, the nature and location of surgical procedures, revision surgeries, and thoracoplasty, have also been identified.10,11,17,19 However, these results could be biased due to the dominance of data from large academic medical centers, which may restrict the prevalence estimates and the generalizability of the findings across the United States. Up to now, few studies on PPCs after spinal fusion have been based on large-scale national database analysis. Thus, this research aimed to investigate the trends and relevant risk factors of PPCs after spinal fusion by utilizing a national database from the United States.
We hypothesized that PPCs after spinal fusion surgery would not represent a single homogeneous outcome, but rather a group of clinically distinct complications with partially different risk profiles. Specifically, we expected that pneumonia and acute respiratory failure would be more strongly associated with impaired pulmonary reserve, frailty, infection, aspiration risk, and postoperative ventilatory support; pulmonary embolism would be more closely related to immobility, venous thromboembolism, coagulopathy, and pulmonary vascular disease; and pulmonary edema would be more closely associated with cardiac, renal, and fluid-related disorders. Therefore, in addition to evaluating PPCs as a composite endpoint, we further examined individual pulmonary complications, including pneumonia, acute respiratory failure, pulmonary embolism, and pulmonary edema.
2. Methods
2.1. Data Source
The Nationwide Inpatient Sample (NIS), a component of the Healthcare Cost and Utilization Project (HCUP) under the U.S. Agency for Healthcare Research and Quality, served as the data source for this investigation. As the largest publicly accessible national database for inpatient care, the NIS compiles a 20% stratified sample of annual discharges across a spectrum of over 1000 U.S. hospitals, encompassing general, short-term, non-federal, and specialized medical centers.1,19 This comprehensive dataset is instrumental for estimating trends in disease occurrence, procedure prevalence, and outcomes associated with surgical interventions within the United States. This study was conducted from July 2024 to July 2025.
2.2. Definition of Cases and Associated Indices
This study collected data from the NIS database spanning the years 2010 to 2019. The diagnosis and procedure information were described via the International Classification of Diseases, Ninth or Tenth Revision, and Clinical Modification (ICD-9-CM or ICD-10-CM).
Inclusion criteria were: (1) age ≥18 years and (2) spinal fusion surgery performed during hospitalization, as identified by the ICD-9-CM or ICD-10-CM procedural codes. Patients diagnosed with postoperative pulmonary complications were defined by the ICD-9-CM or ICD-10-CM diagnostic codes of pneumonia, acute respiratory failure, pulmonary embolism, or pulmonary edema.
Exclusion criteria included: (1) missing data; (2) intravertebral malignancy; (3) intravertebral abscess; (4) osteomyelitis; or (5) various thoracic traumas.
The entire flow used to extract the data is shown in Figure 1, and all the ICD-9-CM or ICD-10-CM codes used are shown in Supplemental Table 1. Flow diagram of patient selection
Variables Used in Binary Logistic Regression Analysis
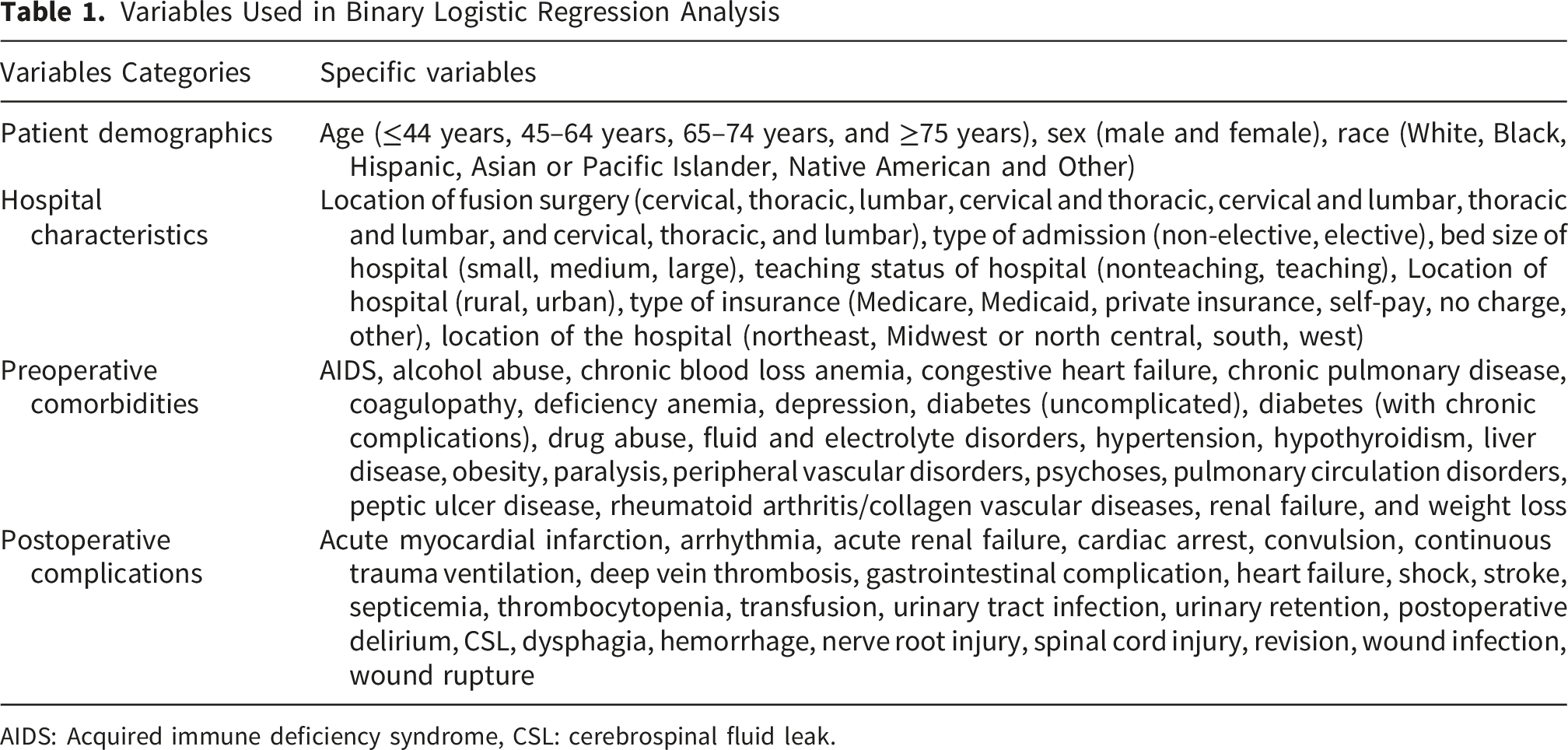
AIDS: Acquired immune deficiency syndrome, CSL: cerebrospinal fluid leak.
2.3. Statistical Methods
Data analysis was conducted using Statistical Package for the Social Sciences (SPSS) 27.0 statistical software (IBM Corporation, Armonk, New York, USA) and R version 4.0.3 (R Foundation for Statistical Computing, Vienna, Austria)/RStudio version 1.4.1717 (RStudio, Inc., Boston, MA, USA). Frequency distributions were calculated to summarize the characteristics of PPCs in these patients with spine fusion.
Because PPCs include clinically heterogeneous events, additional stratified logistic regression analyses were performed for each individual pulmonary complication (pneumonia, acute respiratory failure, pulmonary embolism, and pulmonary edema) to explore whether different preoperative comorbidities and postoperative adverse events were associated with distinct pulmonary outcomes. Postoperative complications were interpreted as co-occurring in-hospital events rather than causal predictors, as the NIS database does not provide the exact temporal sequence of each diagnosis during hospitalization.
Continuous variables were assessed using the T-test, while categorical variables were evaluated with the Chi-square test or Fisher’s exact test. Covariates—including baseline characteristics, preoperative comorbidities, and postoperative complications—that demonstrated a significant association (P < 0.05) in univariate analysis were subsequently entered into separate multivariate logistic regression models. No adjustment was made for multiple comparisons. The odds ratio (OR) and the corresponding 95% confidence interval (CI) from the logistic regression models were computed and extracted utilizing SPSS software. Given the substantial sample size, statistical significance of multivariate analysis was stringently set at an alpha level of P ≤ 0.001, aligning with thresholds established in prior NIS researches. 20
3. Results
3.1. PPCs Trends
Patient Characteristics and Outcomes After Spinal Fusion Surgery (2010-2019)
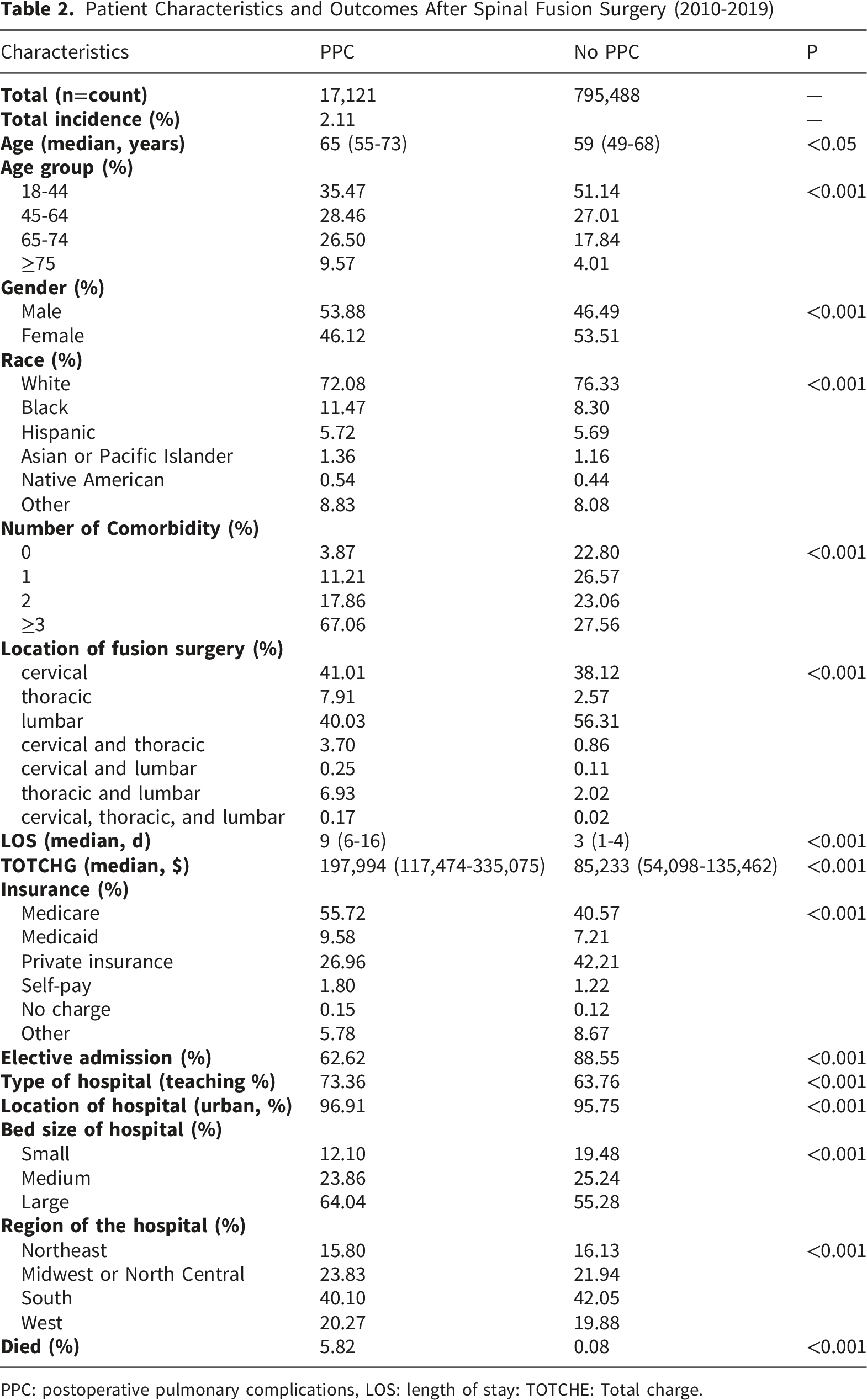
PPC: postoperative pulmonary complications, LOS: length of stay: TOTCHE: Total charge.
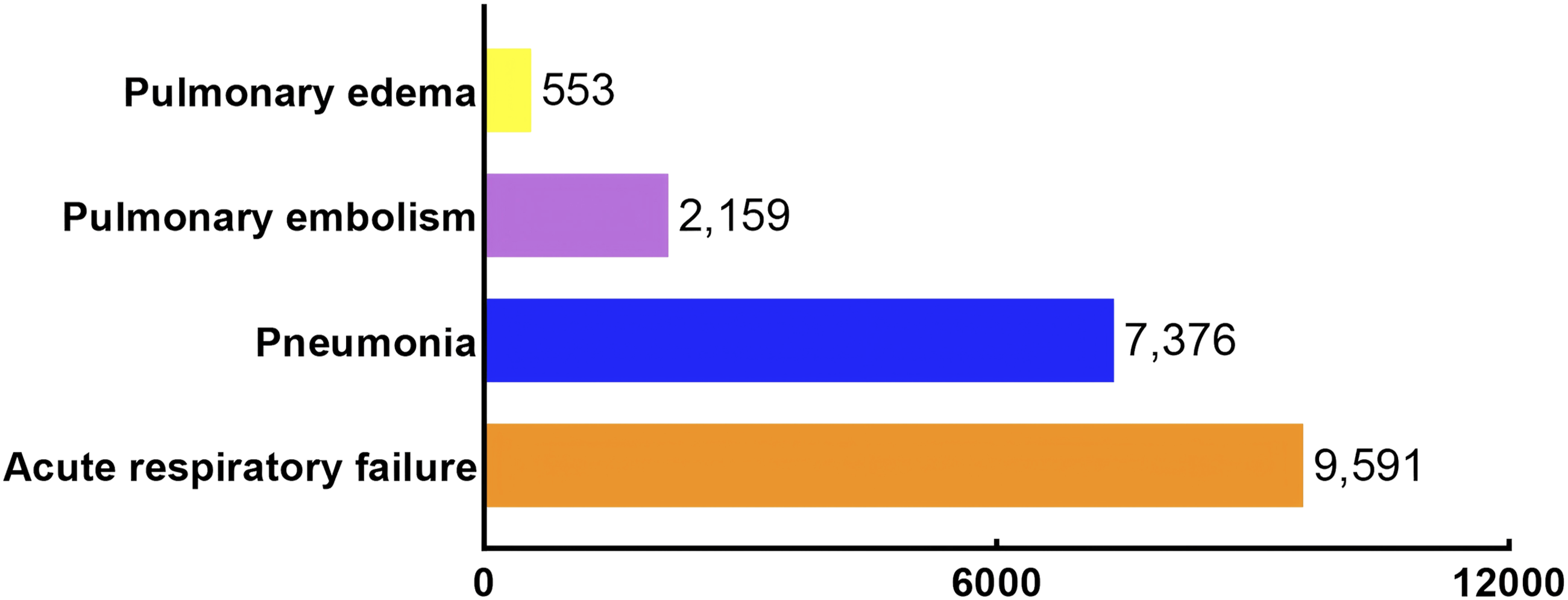
The distribution of the overall numbers of various pulmonary complications from 2010 to 2019
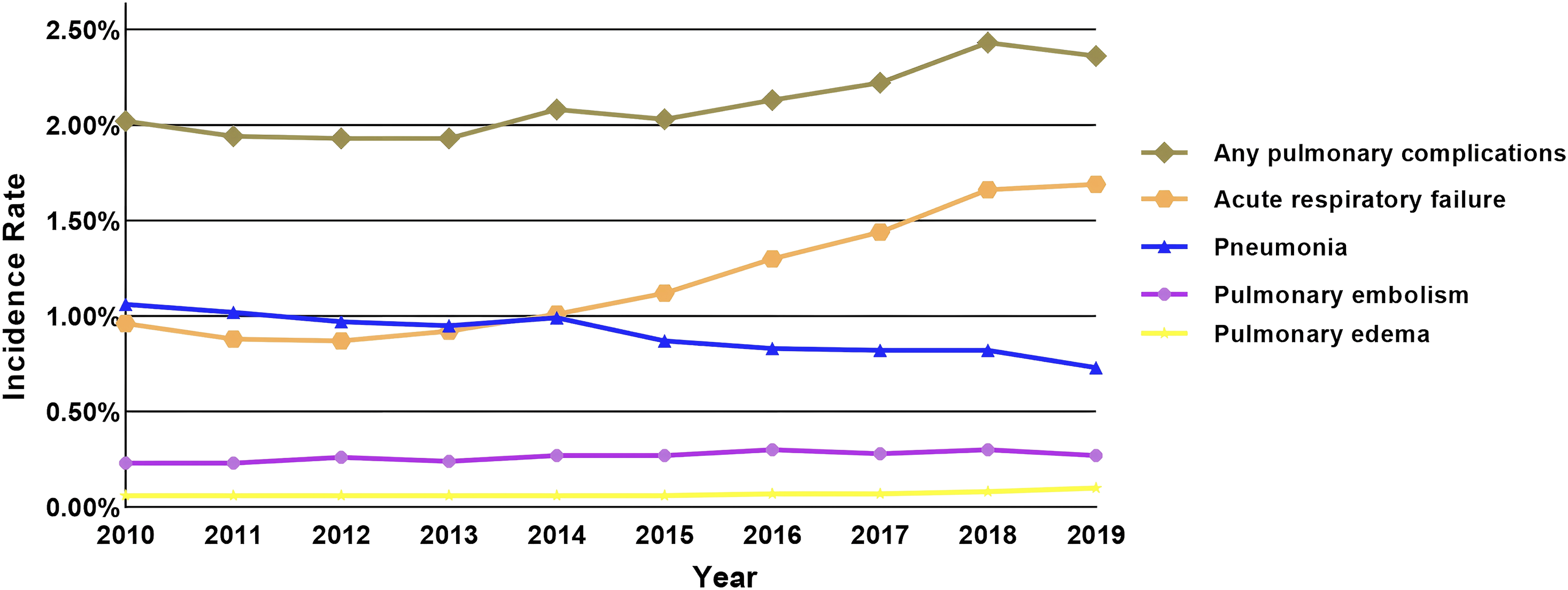
Annual incidence of pulmonary complications. The annual incidence of acute respiratory failure, pneumonia, pulmonary embolism, pulmonary edema after spinal fusion surgery from 2010 to 2019 is shown above. The pooled incidence of any of the aforementioned complications is shown above by the graph labeled “Any Pulmonary Complication”
3.2. Patient Cohort
The majority of patients who underwent spine fusion were male, White Americans, treated at teaching or urban hospitals located in the southern region of the country, and primarily used Medicare (Table 2). Compared with patients without PPCs, those with PPCs tended to be older (65 years vs. 59 years), had higher rates of thoracic fusion surgery (7.91% vs. 2.57%) and comorbidities (≥3, 67.06% vs. 27.56%), and were less likely to be elective admissions (62.62% vs. 88.55%). They also had higher total charges (197,994 $ vs. 85,233 $, p < 0.001) and mortality rates (5.82% vs. 0.08%, p < 0.001), whereas patients without pulmonary complications were more dependent on private insurance as a private payer (42.21 vs. 26.96, p<0.001). With respect to race, African Americans (11.47% vs. 8.30%), Hispanics (5.72% vs. 5.69%), Asians (1.36% vs. 1.16%), and Native Americans (0.54% vs. 0.44%) had higher rates of PPCs. Interestingly, patients with PPCs were more likely to have used large bed size hospitals (64.04% vs. 55.28%, p<0.001), and pulmonary complications were also less likely to occur in patients with lumbar fusion (40.03% vs. 56.31%).
3.3. Risk Factors
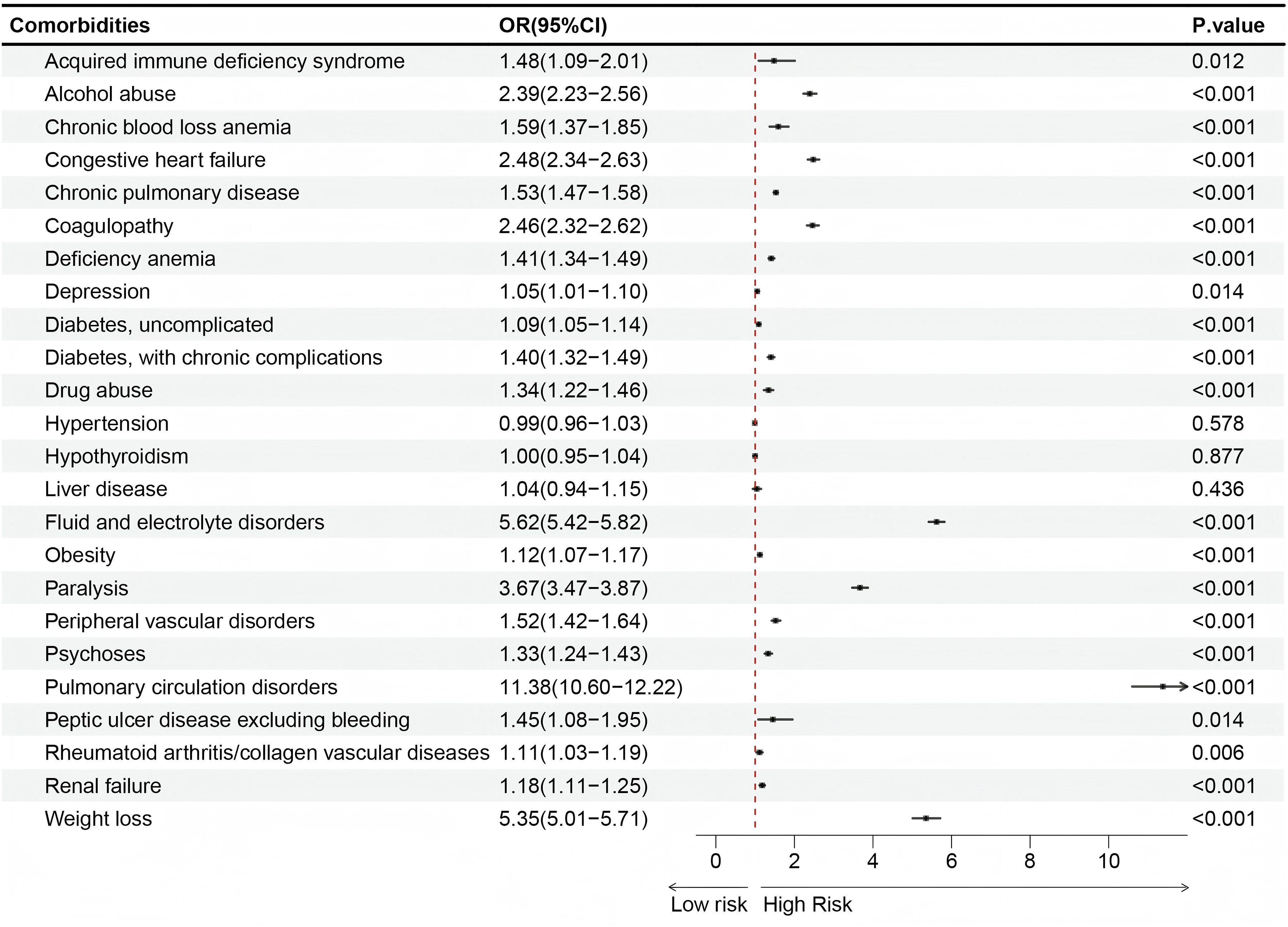
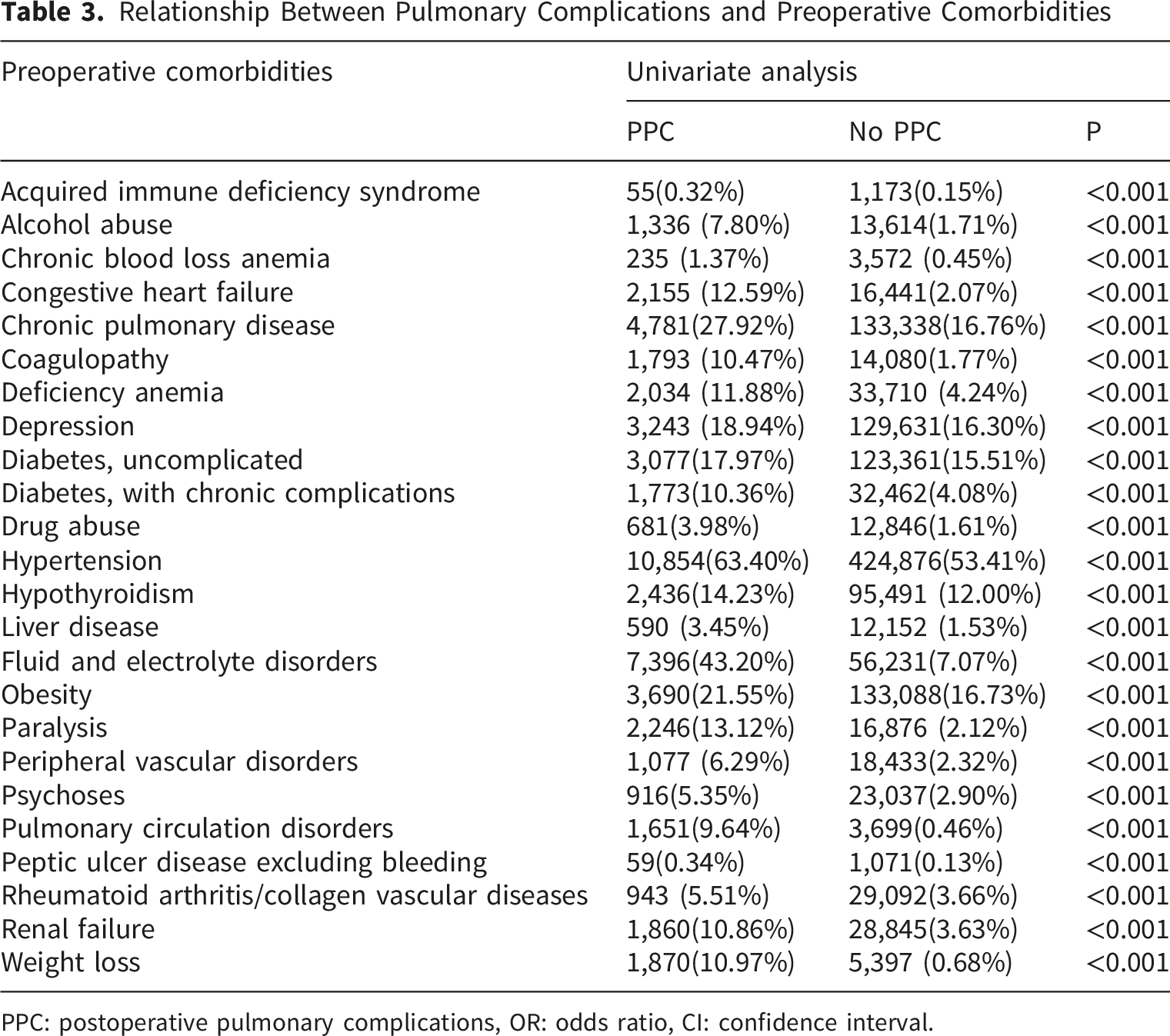
The results of multivariate regression analyses indicate that the risk of PPCs (Figure 4 ; Figure 5, based on the comorbidities presented in Table 3) increased with advanced age (≥75, OR = 1.86, CI = 1.74-1.99), multiple comorbidities (OR = 10.98, CI = 10.14-11.90), thoracic (OR = 1.83, CI = 1.72-1.95) or multilocation surgery (OR = 4.52, CI = 2.95-6.92), misuse of alcohol (OR = 2.39, CI = 2.23-2.56), drug abuse (OR = 1.34, CI = 1.22-1.46), deficiency anemia (OR = 1.41, CI = 1.34-1.49), chronic hemorrhagic anemia (OR = 1.59, CI = 1.37-1.85), congestive heart failure (OR = 2.48, CI = 2.34-2.63), coagulopathy (OR = 2.46, CI = 2.32-2.62), diabetes with chronic complications (OR = 1.40, CI = 1.32-1.49), fluid or electrolyte disorders (OR = 5.62, CI = 5.42-5.82), paralysis (OR = 3.67, CI = 3.47-3.87), psychoses (OR = 1.33, CI = 1.24-1.43), renal failure (OR = 1.18, CI = 1.11-1.25), pulmonary vascular disorders (OR = 11.38, CI = 10.60-12.22), peripheral vascular disorders (OR = 1.52, 1.42-1.64), chronic pulmonary disease (OR = 1.53, CI = 1.47-1.58), and weight reduction (OR = 5.35, CI = 5.01-5.71). In contrast, female (OR = 0.70, CI = 0.68-0.73), lumbar fusion (OR = 0.76, CI = 0.73-0.79), private insurance (OR = 0.89, CI = 0.85-0.93), and elective admission (OR = 0.32, CI = 0.31-0.33) were protective factors for PPCs. Multivariate analysis of characteristics of patients with no PPCs and PPCs Multivariate analysis of between different comorbidities and postoperative pulmonary complications Relationship Between Pulmonary Complications and Preoperative Comorbidities PPC: postoperative pulmonary complications, OR: odds ratio, CI: confidence interval.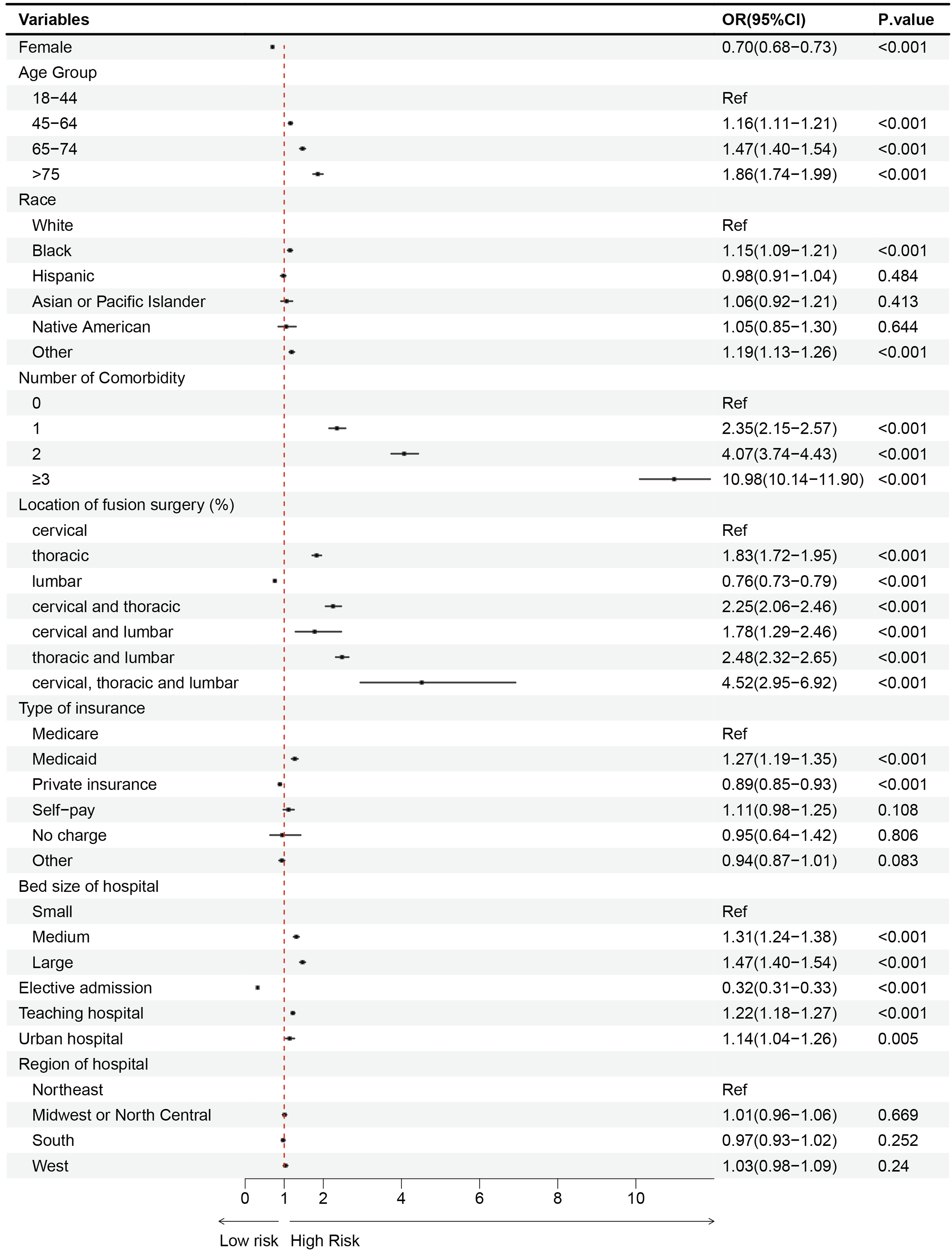
Relationship Between Pulmonary Complications and Postoperative Complications
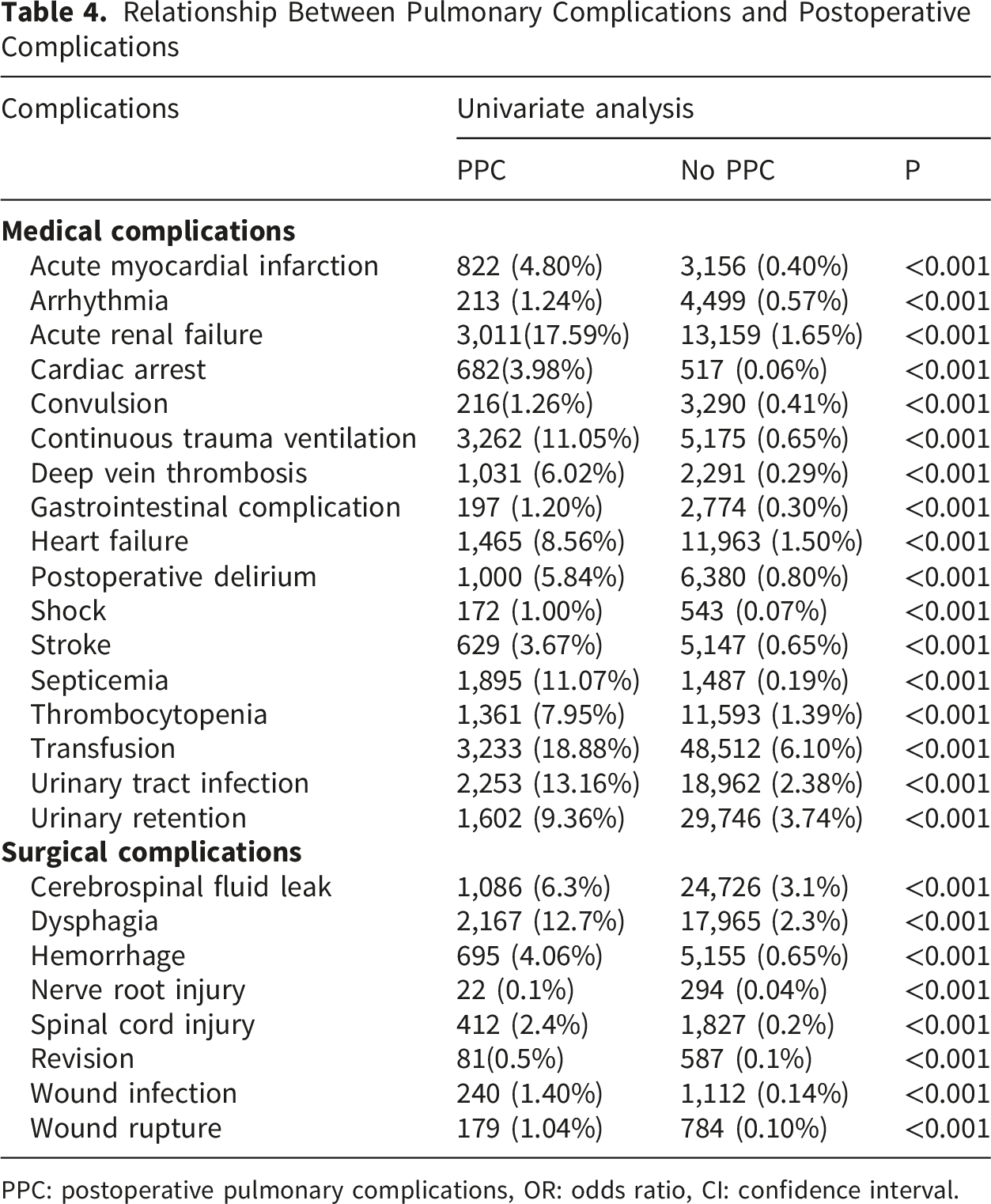
PPC: postoperative pulmonary complications, OR: odds ratio, CI: confidence interval.
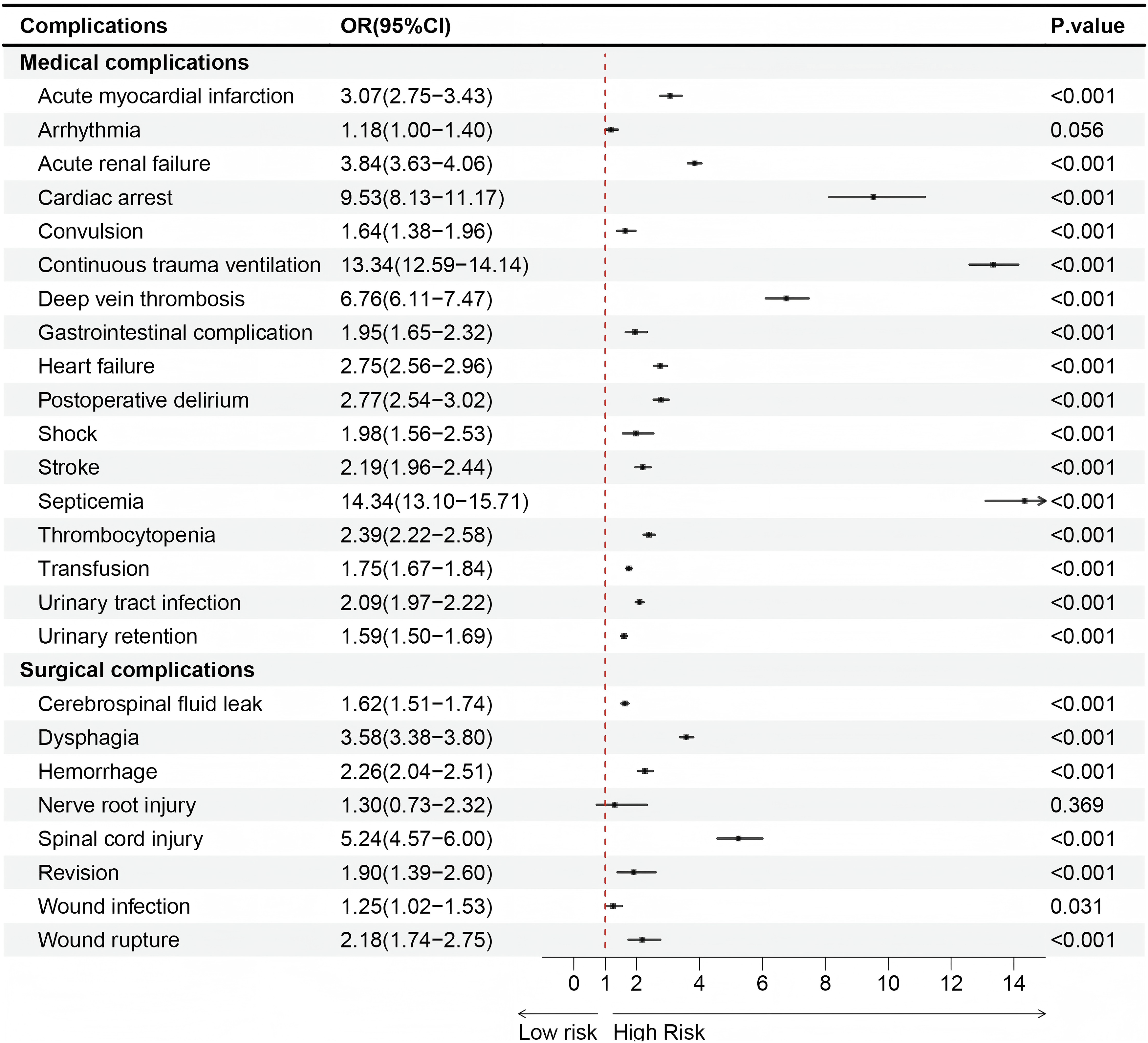
Multivariate analysis of between postoperative complications and postoperative pulmonary complications
To further characterize the heterogeneity of PPCs, we performed stratified analyses for each individual pulmonary complication (Figures 7 and 8). The associations between preoperative comorbidities and pulmonary outcomes differed across pulmonary embolism, pulmonary edema, pneumonia, and acute respiratory failure. Conditions reflecting impaired pulmonary reserve, frailty, or systemic illness, such as chronic pulmonary disease, weight loss, fluid and electrolyte disorders, and paralysis, were more consistently associated with pneumonia and acute respiratory failure. In contrast, variables related to venous stasis, pulmonary vascular disease, or coagulation abnormalities showed stronger associations with pulmonary embolism. Cardiac, renal, and fluid-related disorders were more clinically consistent with pulmonary edema and respiratory failure. Forest plots showing the associations between preoperative comorbidities and individual postoperative pulmonary complication subtypes. Conditions reflecting impaired pulmonary reserve, frailty, or systemic illness (e.g., chronic pulmonary disease, weight loss, fluid and electrolyte disorders, paralysis) were more consistently associated with pneumonia and ARF. Variables related to venous stasis, pulmonary vascular disease, or coagulation abnormalities showed stronger associations with pulmonary embolism. Cardiac, renal, and fluid-related disorders were more clinically consistent with pulmonary edema and ARF Forest plots showing the associations between postoperative complications and individual postoperative pulmonary complication subtypes. Severe postoperative events, including septicemia, continuous trauma ventilation, acute renal failure, cardiac arrest, shock, and postoperative delirium, were associated with specific pulmonary outcomes. The association between deep vein thrombosis and pulmonary embolism was particularly strong, consistent with the known pathophysiologic relationship between venous thrombosis and pulmonary embolism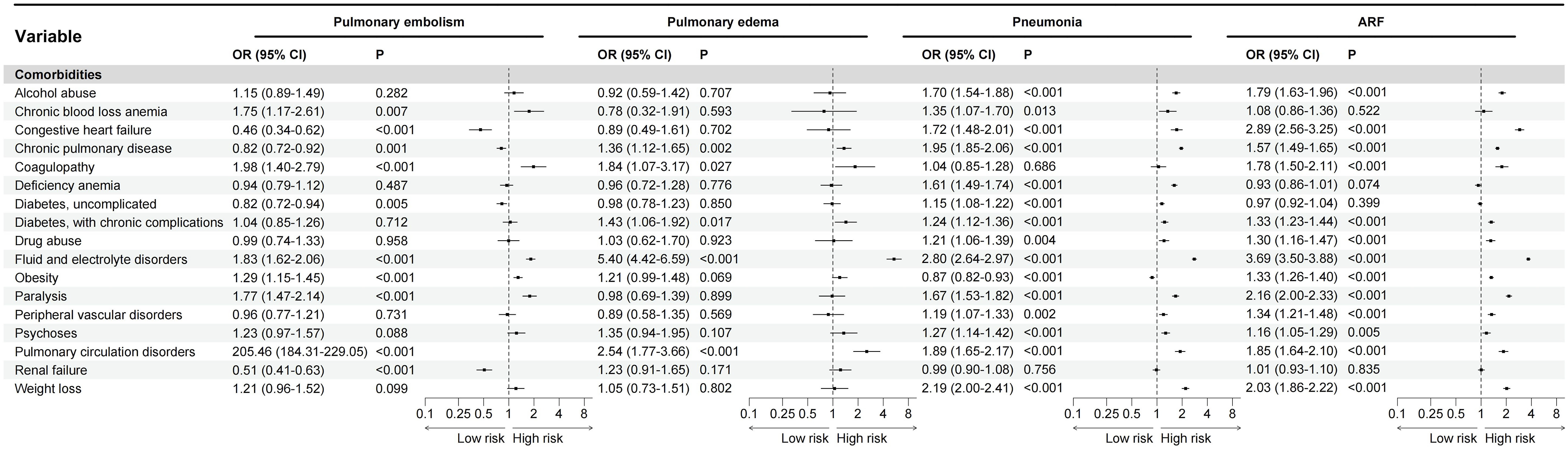
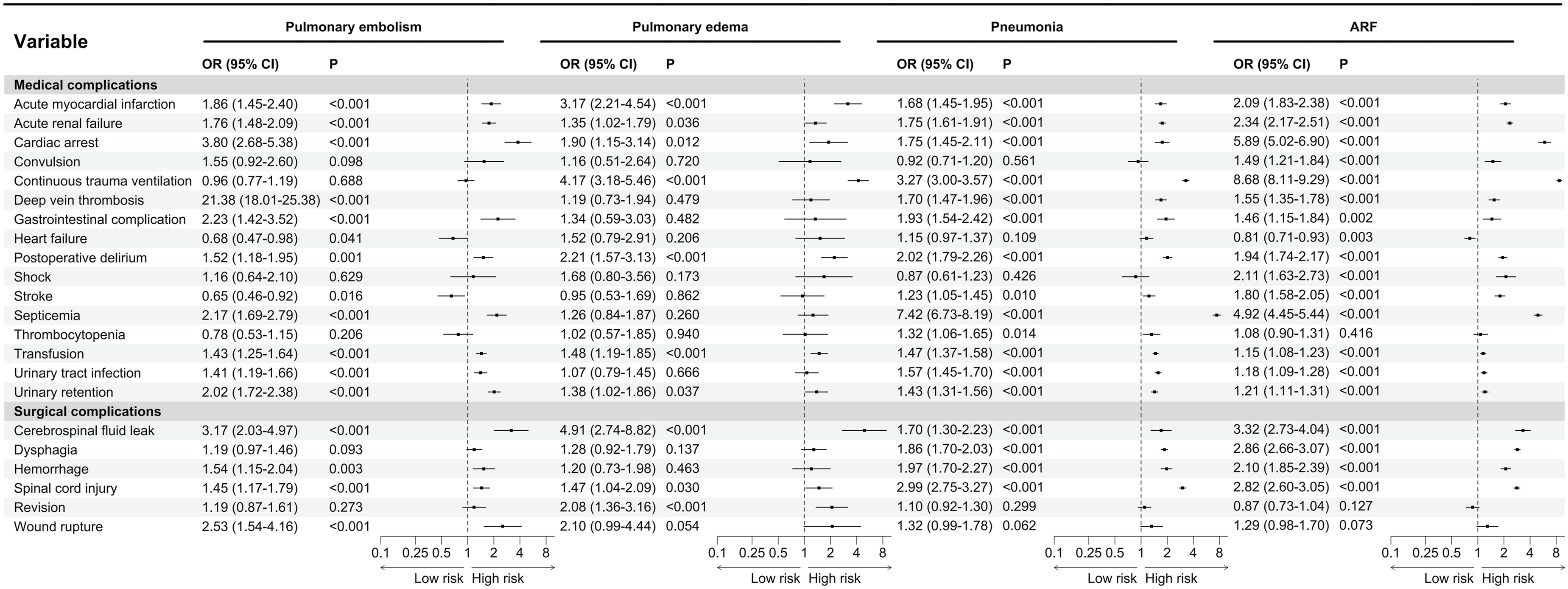
Similar heterogeneity was observed in the analysis of postoperative complications. Severe postoperative events, including septicemia, continuous trauma ventilation, acute renal failure, cardiac arrest, shock, and postoperative delirium, were associated with specific pulmonary outcomes. The association between deep vein thrombosis and pulmonary embolism was particularly strong, which is consistent with the known pathophysiologic relationship between venous thrombosis and pulmonary embolism.
4. Discussion
This statistical analysis of the NIS revealed that the incidence rate of PPCs following spine fusion surgery was 2.11% across the United States. Approximately one out of every 47 spinal fusion surgeries were found to have pneumonia, ARF, pulmonary embolism, or pulmonary edema. The incidence of pneumonia (0.91%) after spinal fusion surgery was similar to that previously described, ranging from 0.40% to 7.40%.4-7,10 However, the national incidences of ARF, pulmonary embolism, and pulmonary edema after spinal fusion surgery were previously not well described and depended on different spine diseases. Fatemi et al. reported that the incidence of pulmonary embolism was 0% after spinal surgery. 7 but some reports found that the incidence of pulmonary embolism was 0.7% after spinal fracture fixation and 1.0% in spinal deformity corrective surgery.6,9 Wu et al. and Wang et al. found that 0.14% to 0.62% rates of pulmonary edema in scoliosis procedures.10,11 Similarly, the incidence of acute respiratory failure was found to be 0.43% to 0.61% in scoliosis procedures, while 3.4% to 3.6% in spinal fractures.10,11
In our study, there was a significant decrease in the annual incidence of pneumonia (from 1.06% to 0.73%) and a relatively lower incidence of pulmonary embolism (mean: 0.27%) and pulmonary edema (mean: 0.07%) (Figure 3), which may be associated with perioperative care, anesthetic and surgical techniques optimization, and deep venous thrombosis prophylaxis. 21 Interestingly, our study revealed that the incidence of ARF increased annually, as did the total rate of PPCs from 2014 to 2019 (range: 2.08% to 2.36%). There are several possible explanations for this trend. First, the mean age of patients undergoing spinal fusion increased steadily from 55 to 61 years during the study period (Supplemental Figure 3). Since advanced age is a well-established risk factor for PPCs,4-6,9,10 this demographic shift likely contributed to the rising respiratory complication burden. 22 Second, the ARF increase may partly reflect diagnostic and coding changes rather than true biological worsening. The ICD-9-CM to ICD-10-CM transition in October 2015 introduced more granular respiratory failure codes, potentially increasing ARF capture sensitivity in administrative data.23,24 Growing clinical awareness and evolving reimbursement practices may also have led to more complete ARF documentation over time.23,24 Third, surgical complexity may have increased during the study decade, with more multilevel fusions, thoracic approaches, and revision surgeries, 1 though the NIS lacks detailed procedural data to confirm this. Intraoperative factors such as operative duration, blood loss, and fluid management—which are not captured in the NIS—could also have influenced PPCs trends and warrant investigation in prospective databases.
The stratified analyses further suggest that PPCs after spinal fusion surgery should not be interpreted as a single homogeneous outcome. Pneumonia, ARF, pulmonary embolism, and pulmonary edema may share several general risk factors, such as advanced age, frailty, comorbidity burden, and prolonged hospitalization, but they can arise through distinct pathophysiologic pathways.25-29 Established postoperative pulmonary risk models have shown that older age, impaired functional status, poor baseline pulmonary reserve, anemia, and prolonged or complex surgery are important predictors of postoperative pulmonary morbidity, which is consistent with the overall pattern observed in our cohort.26-29 In alignment with several studies,5-7,9 patients with advanced age, more comorbidities, alcoholism, diabetes mellitus, fluid and electrolyte disorders, chronic pulmonary disease, paralysis, or weight loss had a higher risk of developing pulmonary complications. In addition, patients who underwent cervical, thoracic, or multi-segment fusion had a higher incidence of PPCs than patients who underwent lumbar fusion did.5,7,9 This paragraph is intended to summarize the main risk factors and surgical-level differences only, whereas the potential mechanisms are discussed below according to pulmonary reserve, ARF pathways, thromboembolic risk, and cardiopulmonary or volume-related mechanisms.25,29
Reduced pulmonary reserve may represent a common mechanism linking advanced age, chronic pulmonary disease, paralysis, spinal cord injury, and frailty with pneumonia and pulmonary-source ARF.25,29 Aging is associated with reduced pulmonary elasticity, impaired respiratory muscle strength, decreased cough effectiveness, diminished immune reserve, and a higher prevalence of cardiopulmonary comorbidities, all of which may reduce tolerance to anesthesia, postoperative pain, immobility, and surgical stress.25,29 Airflow limitation, the presence of emphysema, and the use of inhaled corticosteroids are associated with the development of PPCs in patients with chronic pulmonary disease.4,9,18 Chronic pulmonary disease may further predispose patients to pneumonia and pulmonary-source ARF through impaired mucociliary clearance, atelectasis, secretion retention, ventilation-perfusion mismatch, and reduced ability to compensate for postoperative hypoxemia.25,29 Previous studies have demonstrated that patients with paralysis or spinal cord injury have significantly impaired lung function and an increased risk of PPCs due to damage to the respiratory muscles or nerves controlling the airways. This damage limits the function of the inspiratory muscles and the expulsion of airway secretions. 22 Therefore, patients with impaired pulmonary reserve may benefit from preoperative pulmonary optimization, smoking cessation when applicable, respiratory physiotherapy, postoperative pulmonary hygiene, adequate pain control, and early mobilization.25,29
ARF should be regarded as a multifactorial terminal pathway rather than a complication arising from a single mechanism.25,27 In our analysis, some factors associated with ARF were compatible with pulmonary-source mechanisms, including chronic pulmonary disease, pneumonia susceptibility, secretion retention, atelectasis, and impaired cough, whereas others were more consistent with cardiogenic, renal, inflammatory, or volume-related mechanisms.25,27,30,31 This distinction helps explain why ARF may be linked both to baseline pulmonary vulnerability and to systemic postoperative deterioration.25,27,31 Accordingly, ARF prevention after spinal fusion may require not only pulmonary optimization but also careful monitoring of oxygenation, fluid balance, renal function, hemodynamic status, and postoperative infection or inflammatory complications.25,30,31
Pulmonary embolism appeared to have a risk profile that differed from pneumonia and pulmonary-source ARF.32,33 Conditions related to venous stasis, immobility, pulmonary vascular disease, obesity, peripheral vascular disease, and coagulation abnormalities may increase the risk of venous thromboembolism after major spine surgery.32,33 This is consistent with Virchow’s triad, in which venous stasis, endothelial injury, and hypercoagulability contribute to thrombus formation.32,33 Spine fusion patients may be particularly vulnerable because of operative trauma, postoperative pain, delayed mobilization, and, in selected cases, cautious use or delayed initiation of pharmacologic thromboprophylaxis due to concern for bleeding or epidural hematoma.32,33 Therefore, individualized venous thromboembolism risk assessment and thromboprophylaxis strategies are warranted, balancing thrombotic risk against bleeding-related complications.
Preoperative comorbidities such as congestive heart failure, chronic blood loss anemia, deficiency anemia, pulmonary circulation disorders, and peripheral vascular disease, coupled with postoperative complications such as cardiac arrest, acute myocardial infarction, cardiac failure, acute renal failure, deep vein thrombosis, gastrointestinal bleeding, wound hemorrhage, shock, transfusion, and thrombocytopenia, can increase the risk of PPCs by affecting respiratory muscle movement, impairing the nerves involved in controlling respiration, and altering pulmonary hemodynamics.5,6,10,11 However, these associations should be interpreted according to the likely mechanism of each PPCs subtype. Pulmonary edema and non-pulmonary-source ARF may arise from cardiac, renal, inflammatory, and volume-related pathways.25,30,31 Congestive heart failure, renal failure, anemia, fluid and electrolyte disorders, transfusion, shock, and acute renal failure may reduce cardiopulmonary reserve, impair oxygen delivery, alter pulmonary hemodynamics, or decrease tolerance to perioperative fluid shifts.25,30,31 In susceptible patients, perioperative inflammation, fluid resuscitation, transfusion, renal dysfunction, and myocardial dysfunction may contribute to hydrostatic or permeability-related pulmonary edema, which may subsequently progress to hypoxemia and ARF.25,30,31 Therefore, patients with heart failure, renal dysfunction, anemia, or fluid and electrolyte disturbances may benefit from careful perioperative fluid management, optimization of cardiac and renal status, and close postoperative respiratory monitoring.25,30,31
The increased risk of PPCs in patients with diabetes might be related to depression of immunity against infection. 34 In addition, the associations between weight loss or fluid/electrolyte abnormalities and the development of PPCs remain unclear. This status may indicate underlying chronic disease, significant blood loss, and transfusion.2,35 Weight loss, deficiency anemia, chronic blood loss anemia, and diabetes may also reflect malnutrition, impaired physiological reserve, decreased oxygen-carrying capacity, immune dysfunction, and delayed recovery from surgical stress.25,29 From a preventive perspective, these findings support nutritional assessment, anemia correction when feasible, glycemic optimization, and early rehabilitation in high-risk patients undergoing spinal fusion surgery.225,29
Septicemia introduced the highest OR (14.34), which leads to acute lung injury and organ dysfunction by causing hemodynamic changes, inflammation, immune issues, and tissue damage.36,37 Intuitively, continuous trauma ventilation can produce physical lung injury through overdistension (volutrauma) and excessive transpulmonary pressure (barotrauma). 38 Furthermore, the pulmonary inflammatory response may be initiated during surgery. 39 Patients with dysphagia or alcohol abuse are likely to be infected with aspiration pneumonia due to high bacterial colonization rates in the oral and respiratory tracts. 40 Similarly, patients with cerebrospinal fluid leakage after oral or nasal spinal fusion surgery may also develop aspiration pneumonia through aspiration of cerebrospinal fluid, 41 but the risk of CSL increasing PPCs is still unclear in other spinal surgery sites. The associations involving alcohol abuse, drug abuse, psychoses, and other psychiatric or behavioral diagnoses should also be interpreted cautiously.25,29 These variables may not directly cause a specific pulmonary complication; rather, they may identify patients with increased perioperative vulnerability, including higher smoking prevalence, chronic lung disease, malnutrition, aspiration risk, sedative or opioid exposure, withdrawal syndromes, delirium, impaired participation in pulmonary hygiene, and reduced adherence to early mobilization.25,29
Postoperative delirium, convulsions, wound or urinary tract infections, and other complications mentioned above, either alone or in combination, can increase unplanned ICU hospitalizations, continuous mechanical ventilation, prolonged LOS, and other adverse outcome events.15,42,43 This complex physical condition reduces the patient’s tolerance and immune function to cope with stressors, making it easy to develop pulmonary complications. Nevertheless, associations between PPCs and other postoperative complications should be interpreted conservatively because the NIS database does not provide the exact timing of each postoperative diagnosis.25,29 Therefore, postoperative complications in this study should be regarded as co-occurring adverse events or markers of postoperative illness severity rather than definitive causal predictors of PPCs.25,29 This limitation is particularly relevant when interpreting associations involving urinary tract infection, urinary retention, gastrointestinal complications, septicemia, shock, renal failure, or mechanical ventilation, because these events may occur before, after, or concurrently with PPCs.25,29,44
Taken together, these distinct mechanisms support our decision to analyze each PPCs subtype separately rather than relying only on a composite PPC outcome.25,29 Evaluating pneumonia, ARF, pulmonary embolism, and pulmonary edema separately may reveal clinically meaningful risk profiles that could be obscured when PPCs are treated as a single endpoint.25,29
Patients with PPCs have a higher mortality rate and costly total charge. Memtsoudis et al. 16 found that 43.7% of patients who underwent lumbar spine fusion subsequently died with a diagnosis of PPCs. In our study, the mortality rate among patients who developed PPCs was 5.82%, a significantly higher figure than patients without PPCs (0.08%). In other words, 61.03% of all dead patients had developed PPCs, thereby highlighting the overall potential impact of this complication. However, due to the limitations of the NIS database, it was difficult to confirm the medium- and long-term mortality of patients with combined PPCs. Dimick et al. reported that the greatest financial burden was attributed to respiratory complications, 13 with an estimated cost of 52,466 dollars, following non-cardiac surgery at a single private-sector center. Furthermore, our findings indicated that the average admission costs (197,994 $ vs. 85,233 $) and length of stay (9 days vs. 3 days) doubled and tripled in the presence of pulmonary complications following spinal fusion surgery. Although these associations indicate a substantial clinical and economic burden, the retrospective and administrative nature of the data prevents us from determining whether PPCs directly caused these adverse outcomes or whether sicker patients were more likely to develop PPCs during complicated hospitalizations.25,44 Nevertheless, PPCs remain clinically important because they may contribute to prolonged hospitalization, intensive care use, ventilatory support, systemic inflammation, secondary organ dysfunction, and increased costs, while also serving as markers of postoperative deterioration and resource utilization.25,44 Therefore, based on the above findings, we should focus on reducing the incidence of PPCs after spinal fusion to alleviate the burden on patients and the healthcare system.
The current study is subject to limitations inherent in the NIS database. As a secondary analysis of an existing dataset, the sample size was predetermined by the database architecture and study period; therefore, a formal a priori sample size calculation was not performed. However, the large cohort size (n = 812,609) and the observed event rate ensured sufficient statistical precision to detect small but clinically meaningful associations with narrow confidence intervals. Additional limitations include potential coding errors, the absence of detailed clinical laboratory and imaging data, and a lack of follow-up information. The absence of follow-up data could lead to underestimation of the incidence rates for conditions such as pneumonia, pulmonary embolism, and pulmonary edema. According to the current data, the exact cause of acute respiratory failure is unknown and may be due to pneumonia, pulmonary embolism, cardiogenic, or other non-pulmonary factors. This makes the data potentially susceptible to classification bias. Furthermore, this study did not investigate the relationships between surgical procedures or diseases and PPCs. Most importantly, the temporal sequence of postoperative complications cannot be reliably determined in the NIS, and some observed associations may reflect residual confounding, frailty, prolonged hospitalization, or increased surveillance rather than direct biological causation.25,29 Further research is needed to address the above issues.
5. Conclusions
In conclusion, this nationwide analysis demonstrated that PPCs occurred in 2.11% of adult patients undergoing spinal fusion surgery and were associated with longer hospitalization, higher costs, and increased in-hospital mortality. The overall PPCs rate increased in recent years, mainly driven by the rising incidence of ARF. Older age, thoracic or multilevel fusion, and major systemic comorbidities were among the most clinically relevant predictors, but the risk profiles differed across pneumonia, ARF, pulmonary embolism, and pulmonary edema. These findings support separate assessment of individual PPCs subtypes and the development of individualized prevention strategies targeting impaired pulmonary reserve, thromboembolic risk, and cardiac, renal, or volume-related vulnerability after spinal fusion surgery.
Supplemental Material
Supplemental Material - Incidence and Related Risk Factors of Pulmonary Complications After Spinal Fusion Surgery: A Retrospective Nationwide Inpatient Sample Database Study
Supplemental Material for Incidence and Related Risk Factors of Pulmonary Complications After Spinal Fusion Surgery: A Retrospective Nationwide Inpatient Sample Database Study by Yue Wang, Yu-Dong Liao, Yuheng Zhang, Cong-Rui Liao and Jian-Ting Chen in Geriatric Orthopaedic Surgery & Rehabilitation.
Footnotes
Ethical Considerations
This observational study used de-identified publicly available data, hence there was no requirement for consent to participate and it was deemed exempt by the ethics committee. Therefore, there is no need to grant permission in the Ethics approval and consent to participate section. What is more, the data used in this study were no need anonymized before its use. All methods are carried out following relevant guidelines and regulations. The data used in this study were not need anonymized before its use.
Author Contributions
All authors contributed to the study conception and design. Material preparation, data collection, analysis and interpretation were performed by YW, YDL and YHZ. The first draft of the manuscript was written by YW and YDL with revision, guidance and feedback from JTC and CRL. All authors commented on previous versions of the manuscript. All authors read and ap proved the final manuscript. All authors agree to be accountable for all aspects of the work, ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (Grant No. 82202736).
Declaration of Conflicting Interests
The authors declare that they have no conflicts of interest related to this research, authorship, or publication.
Data Availability Statement
The Nationwide Inpatient Sample (NIS) database is a large publicly available full-payer inpatient care database in the United States. These data are easily available from the Agency for Healthcare Research and Quality (AHRQ’s) “Healthcare Cost and Utilization Project (HCUP)” and can be obtained after completing an on-line Data Use Agreement training session and signing a Data Use Agreement. The datasets are available at ![]() .
.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.