
Abstract
Male adolescents with anorexia nervosa (AN) remain markedly underrepresented in clinical and technological research, limiting understanding of the gender-specific mechanisms that may shape how they interact with virtual environments. The primary objective of this study was to evaluate the feasibility and acceptability of an integrated virtual reality (VR)-based mirror exposure therapy and eye-tracking-driven attentional bias (AB) modification training protocol—previously tested in a female-based randomized controlled trial—in two male adolescents with AN. Both participants received concurrent multidisciplinary care, with one case featuring comorbid muscle dysmorphia. Feasibility was assessed via protocol adherence and technical stability. Acceptability was measured using the System Usability Scale (SUS). Secondary exploratory measures included eye-tracking AB and clinical questionnaire outcomes (body dissatisfaction, drive for thinness, body anxiety, body appreciation) at pretreatment, posttreatment, and 3-month follow-up. Feasibility indicators were consistently positive: Both participants completed all sessions, reported high perceived usability (SUS > 80), and no technical incidents occurred. Exploratory clinical observations suggested improvements in body dissatisfaction, weight-related anxiety, and body appreciation, with effects maintained at the 3-month follow-up. Eye-tracking data revealed divergent attentional profiles: the patient with a typical AN presentation showed heightened attention to weight-related body areas, whereas the patient with muscle dysmorphia displayed a more complex pattern oriented toward muscular regions. Given the concurrent multidisciplinary treatment, clinical improvements cannot be attributed solely to the VR intervention; however, these cases show that the protocol is a viable and well-tolerated tool that warrants further investigation in a randomized controlled trial with AN male adolescents.
Keywords
Introduction
Anorexia nervosa (AN) is a severe eating disorder characterized by low body weight, body image disturbance, and an intense fear of weight gain (FGW). 1 The disorder carries substantial medical complications, high comorbidity, and substantial chronicity.1,2 Virtual reality (VR) has emerged as a promising tool to enhance body-focused therapy through immersive, controllable environments. VR-based mirror exposure therapy (VR-MET) enables patients to confront a virtual avatar representing their body, whose size, or shape can be systematically manipulated, facilitating emotional processing and reducing avoidance.3–5
A key mechanism in body image disturbance is body-related attentional bias (AB), defined as the selective allocation of attention toward specific body regions associated with dissatisfaction or fear.6–10 Female AN samples consistently show heightened AB toward weight-related regions such as the abdomen, waist, and thighs.11–13 Because AB may reinforce negative beliefs and impair exposure effectiveness, modifying this pattern has therapeutic relevance. Attentional bias modification training (ABMT) using eye-tracking can redirect maladaptive visual patterns in real time and has shown encouraging results when combined with VR-MET,14–17 including reductions in AB and improvements in body image outcomes.18–21
AN in females follows established developmental trajectories with body dissatisfaction emerging as early as middle childhood 22 and often reinforced by sociocultural influences such as advertising. 23 While VR-MET is a promising tool for these patients, recent research emphasizes that mirror-based paradigms are particularly relevant for addressing self-recognition deficits 24 and allow patients to confront and process distorted body-related perceptions within controlled and immersive environments.3–5 However, research on male AN remains scarce, despite clear evidence that AN affects the male population25,26 and that their body concerns differ importantly. While females typically strive for thinness, males often experience dual pressure involving both leanness and muscularity.27,28 Muscularity-related concerns may present as muscle dysmorphia, involving preoccupation with insufficient muscularity. 29 Studies have shown that males with high levels of muscular dissatisfaction display distinct attentional patterns, including fixating on muscular or self-perceived unattractive features.30–35 Yet male AN patients are markedly underrepresented, 36 and despite comparable symptom severity across genders,37,38 empirical data on male-specific mechanisms remain limited.27,39 If males process body-related information differently, protocols validated only in females may not generalize.
To address this gap, we applied the ABMT + VR-MET protocol—previously validated in female populations20,21—to two male adolescents with AN, one of whom presented with comorbid muscle dysmorphia. The primary objective was to assess the feasibility and acceptability of this integrated VR intervention. As a secondary exploratory objective, we examined patterns of body-related AB in these male cases in relation to findings previously reported in female samples and tracked preliminary clinical trends in body dissatisfaction, body-related anxiety, FGW, and body appreciation, including their maintenance at a 3-month follow-up.
Cases Formulation
Patient A (16-year-old male) met Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision(DSM-5-TR1) criteria for restrictive-type AN and muscle dysmorphia, characterized by an excessive drive for muscularity. 40 Despite an admission body mass index (BMI) of 13.8 (first percentile, World Health Organization [WHO] 41 ), he desired weight gain to improve athletic performance. Treatment included individualized nutritional rehabilitation (1000–2400 kcal/day) and a multidisciplinary Home Treatment (HoT) program, involving cognitive behavioral therapy, family-based therapy, psychoeducation, emotion regulation, and social skills training.25,42,43
Patient B (14-year-old male) presented with restrictive-type AN and major depressive disorder, 1 triggered by family bereavement and bullying. Symptoms included intense FGW, body image distortion and dissatisfaction, and compulsive exercise. His admission BMI was 14.75 (first percentile, WHO41). Nutritional rehabilitation progressed from 1000 to 2200 kcal/day.
Both patients agreed to participate in the study during HoT program.
Materials and Methods
The study followed the logic of a replicated A–B single-case experimental design, which is appropriate for preliminary feasibility work in low-incidence populations. The structure allowed repeated measurement of key variables across sessions, enabling visual analysis of change within and across cases.
Instruments
Participants were immersed in a Unity™ 3D VR environment featuring a mirror 1.5 meters ahead (Fig. 1a). To enhance virtual body ownership, 44 both a third-person mirror view (Fig. 1b) and a first-person view (Fig. 1c) were provided. An HTC™ Vive Pro Eye head-mounted display (HMD) with motion tracking was used to map movements. A Tobii™ eye-tracker recorded gaze fixations on mirrored body areas.
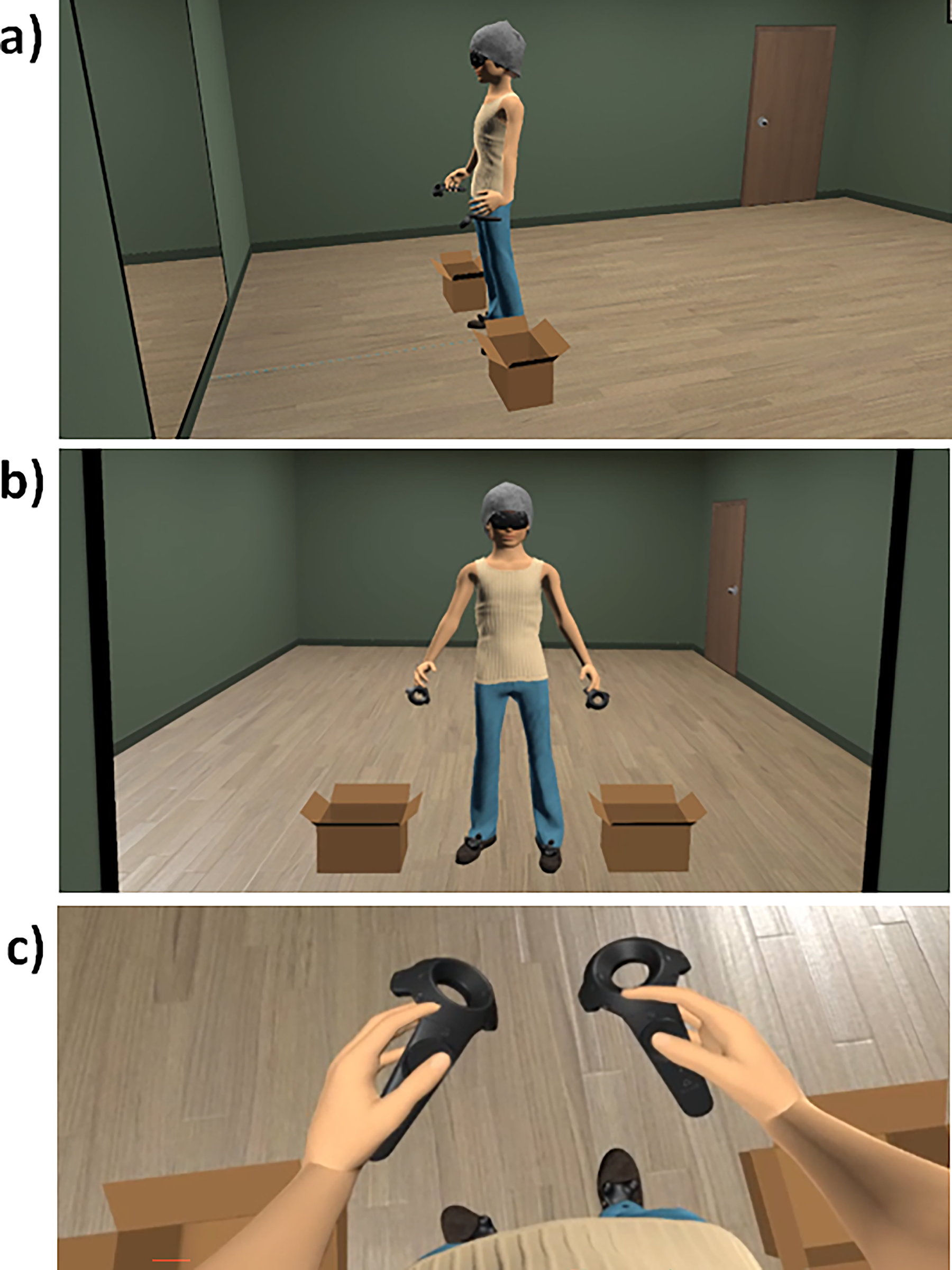
Virtual body and VR immersive environment.
Measures
Questionnaires and visual analog scales
Acceptability/Feasibility: Evaluated using attendance, session completion, 3-month follow-up, and the System Usability Scale (SUS).45,46 Feasibility was additionally monitored by recording any hardware or software issues. BMI: Calculated as weight(kg)/height2(m2). Body dissatisfaction/Drive for thinness: Assessed using Eating Disorder Inventory-Body Dissatisfaction (EDI-BD) and Eating Disorder Inventory-Drive for Thinness (EDI-DT) subscales, respectively, of Spanish EDI-3 (α = 0.74–.96; r = 0.86).47–49 Body anxiety: Assessed with the weight-related subscale of the Physical Appearance State and Trait Anxiety Scale (PASTAS) (α = 0.88; r = 0.89).
50
Body appreciation: Assessed with the Spanish Body Appreciation Scale (BAS) for adolescents (α = 0.91; r = 0.87).51,52 Visual analog scales (VAS): State measures (0 = not at all, 100 = completely) assessed:
Body Satisfaction (VAS_BS): “How satisfied are you with your body now?”
Anxiety (VAS_Anxiety):“How anxious do you feel right now?”
FGW (VAS_FGW): “How afraid are you of gaining weight right now?”
Embodiment (VAS_Embodiment): “To what extent did you feel the virtual body was your own?”
Body-related AB assessment
AB was assessed during a 30-second free-viewing period. Participants stood on markers with their arms slightly raised and observed their avatar in the virtual mirror, following prior standard procedures.7,18,20,21,53 Gaze fixations (≥100 ms) were recorded for predefined body areas of interests (AOIs). Two AOI categories were defined: weight-related AOIs (W-AOIs: abdomen, waist, stomach, hips, thighs, and legs) aligned with PASTAS weight-related regions 50 and non-weight-related AOIs (NW-AOIs: neck, shoulders, arms, chest), following established AB paradigms.6,8,54,55 Eye-tracking data were processed with OGAMA software, which yielded two indicators: complete fixation time (CFT) and number of fixations (NF).
Procedure
Written informed consent was obtained from both patients and their parents, ensuring confidentiality, voluntary participation, and the right to withdraw at any time. This study replicated prior research’s procedure with female AN patients,20,21 comprising seven weekly sessions and a 3-month follow-up.
Pretreatment session
Participants completed the EDI-BD, EDI-DT, PASTAS, and BAS questionnaires. Avatar creation used a photographic procedure.20,21 Eye-tracker calibration and a 5-minute visuo-motor/tactile protocol induced body ownership. 56 Participants then completed the VAS ratings and a baseline AB assessment.
Clinical sessions
Each session included ABMT followed by VR-MET. The avatar’s BMI increased progressively from actual to target values using WHO growth charts. 41 Sessions began with calibration, ownership induction, and VAS ratings. ABMT followed established procedures,16,18,20,21 presenting geometric figures on weight-related (45 percent), non-weight-related (45 percent), and neutral (10 percent) areas (optimized 150 trials to elicit AB significant changes 18 ; Fig. 2). VR-MET involved a guided examination from the shoulders to the feet with verbal emotional processing. BMI increases required ≥ 40 percent body anxiety reduction. AB was reassessed afterward.
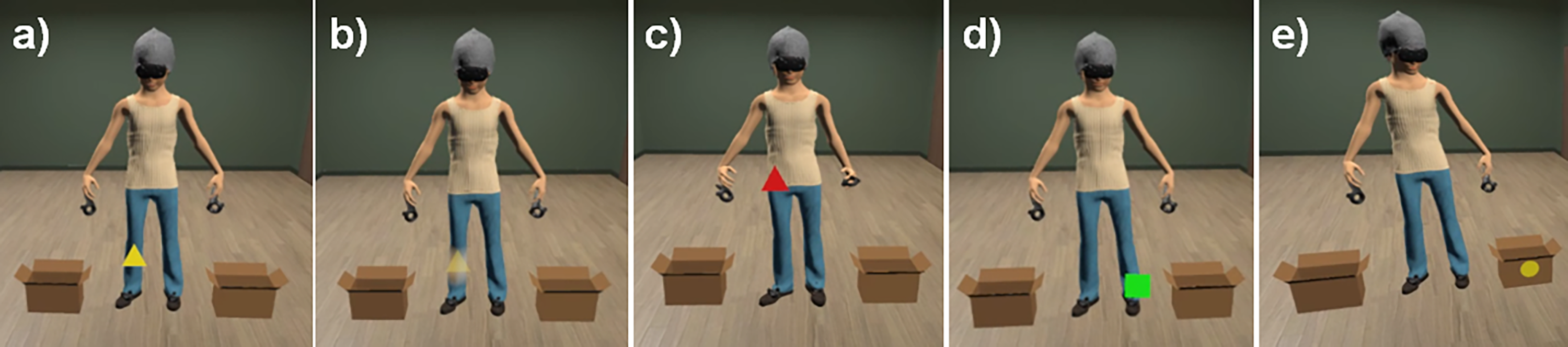
Attentional bias modification training. From left to right:
Posttreatment session and 3 months follow-up
BMI measure, VR immersion, VAS ratings, and AB reassessment were performed. Self-report questionnaires were completed after removing the HMD. SUS was administered only at posttreatment.
Data analysis
Reliable and clinically significant changes in EDI-BD, EDI-DT, and BAS were calculated using male community standard deviations: 11.35 (EDI-BD), 57 8.90 (EDI-DT), 57 and 9.39 (BAS). 52 Analyses followed Jacobson and Truax’s criteria 58 using the Leeds Reliable Change Index (RCI) calculator. 59 RCI estimation for PASTAS could not be performed due to the absence of male normative data.
Results
Primary outcomes: Feasibility and acceptability
Both participants completed the full seven-session protocol and the 3-month follow-up, representing 100 percent adherence to the experimental schedule. No hardware failures or software issues were reported during the sessions, indicating that the VR setup functioned reliably in this context. Posttreatment SUS scores (Patient A = 90; Patient B = 80) indicated excellent usability (i.e., “A grade” 60 ). These findings suggest that the combined VR-MET and ABMT interface was highly acceptable and intuitive for the participants.
Secondary exploratory outcomes: Clinical trajectories during intervention
Both patients showed gradual, clinically appropriate BMI increases throughout treatment. The progressive BMI increments applied to the avatar mirrored these changes, and both reached their target healthy BMI (based on WHO growth charts 41 ) by the fifth clinical session (Table 1). At follow-up, both exceeded the 25th percentile BMI targets (Patient A: 19.72; Patient B: 18.63), indicating continued weight restoration.
Body Mass Index Trajectories of Patients and Their Corresponding Avatars Throughout the Study
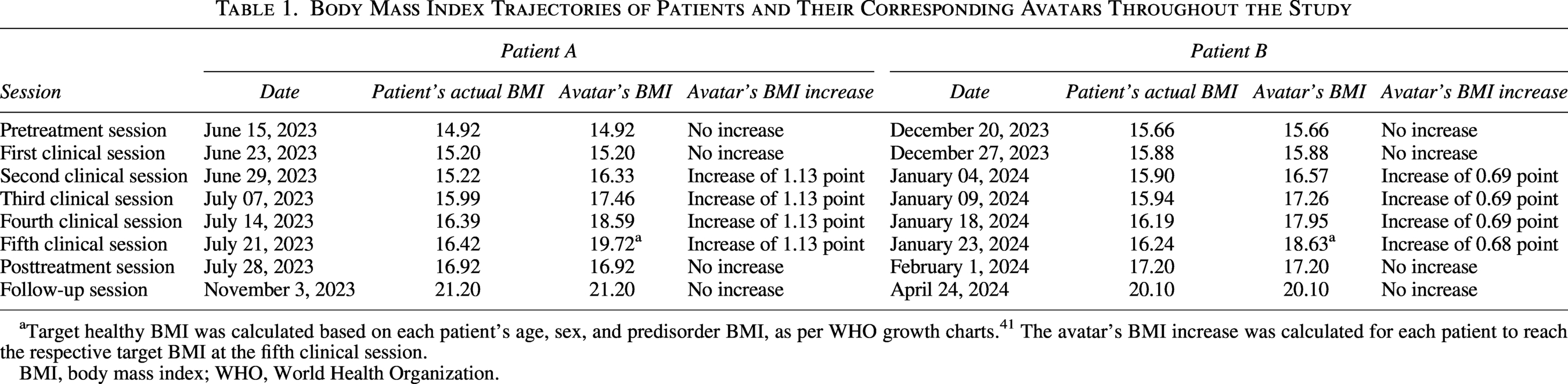
Target healthy BMI was calculated based on each patient’s age, sex, and predisorder BMI, as per WHO growth charts. 41 The avatar’s BMI increase was calculated for each patient to reach the respective target BMI at the fifth clinical session.
BMI, body mass index; WHO, World Health Organization.
Figure 3 summarizes session-by-session changes in state measures (VAS).
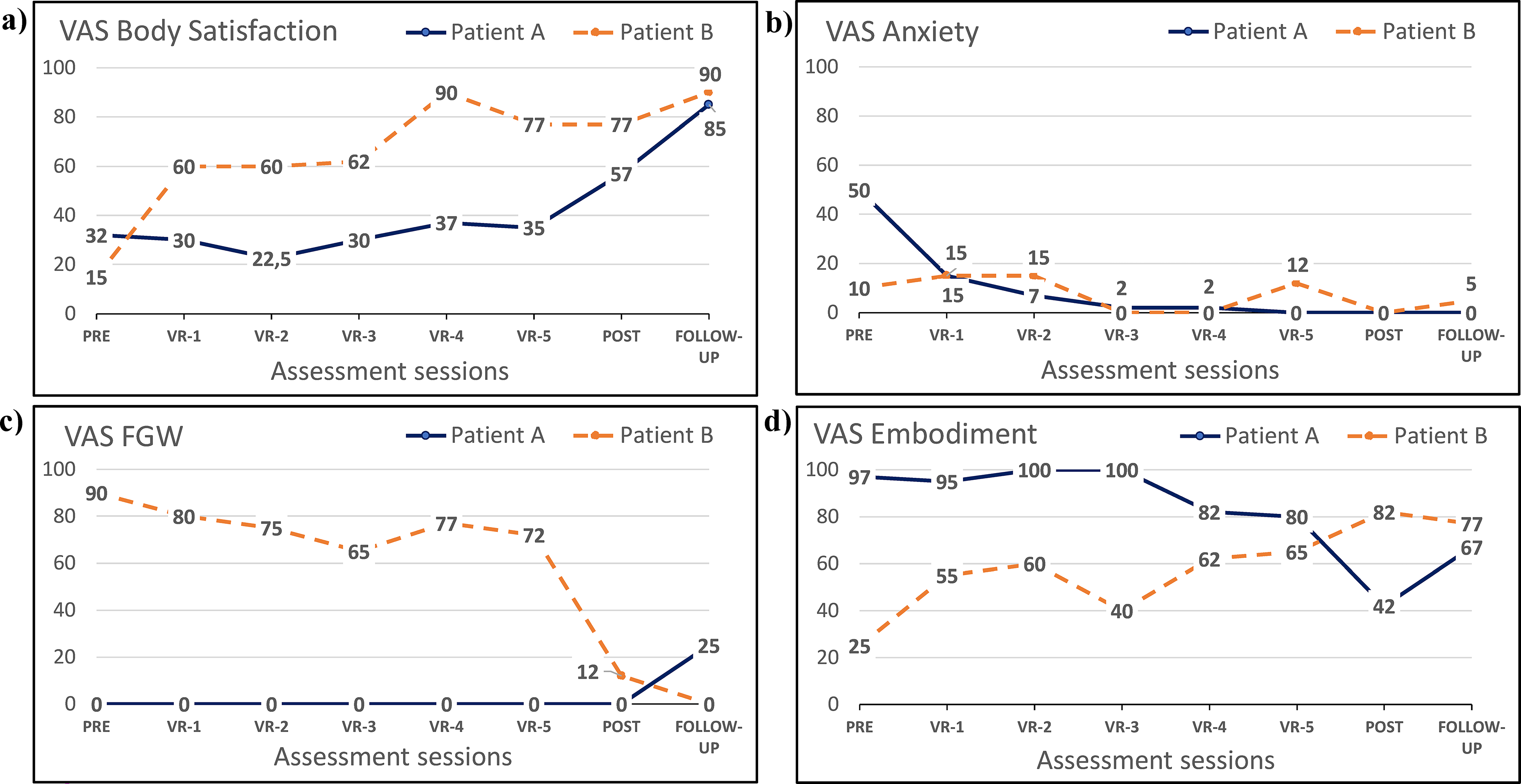
VAS assessments throughout treatment.
Table 2 presents self-reported questionnaires’ scores at pretreatment, posttreatment, and follow-up.
Self-Reported Questionnaire Scores
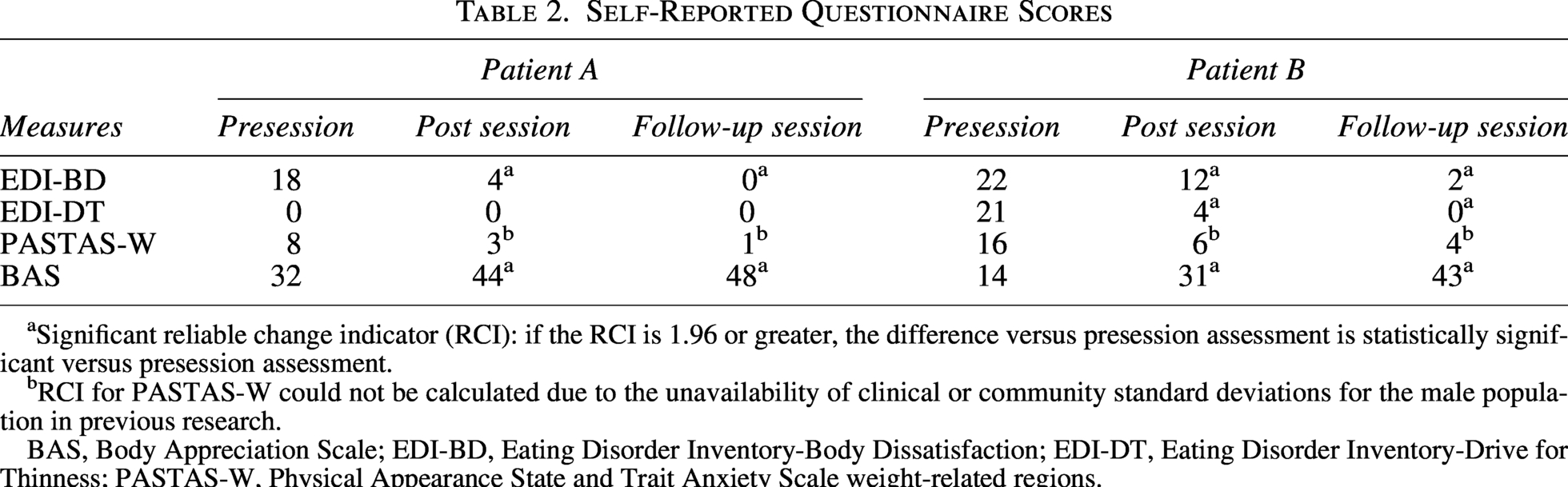
Significant reliable change indicator (RCI): if the RCI is 1.96 or greater, the difference versus presession assessment is statistically significant versus presession assessment.
RCI for PASTAS-W could not be calculated due to the unavailability of clinical or community standard deviations for the male population in previous research.
BAS, Body Appreciation Scale; EDI-BD, Eating Disorder Inventory-Body Dissatisfaction; EDI-DT, Eating Disorder Inventory-Drive for Thinness; PASTAS-W, Physical Appearance State and Trait Anxiety Scale weight-related regions.
Figure 4 shows the proportion of CFT and NF allocated to W-AOIs and NW-AOIs across sessions. At pretreatment, Patient B displayed greater attention to W-AOIs, consistent with patterns observed in female AN samples11–13 and with his own weight-focused body dissatisfaction. Visual analysis then showed immediate level change, with a reduction in W-AOI fixations from VR-1 onward, and a positive upward trend in NW-AOI fixations across sessions. In contrast, Patient A’s pattern showed immediate and stable allocation of attention to muscular regions (i.e., shoulders, arms, chest), indicating strong maintenance of muscularity-focused AB throughout the intervention. The substantially higher NF (in absolute values) observed in Patient A also suggests elevated attentional variability, potentially reflecting tension between restrictive AN symptoms and the drive for muscularity.
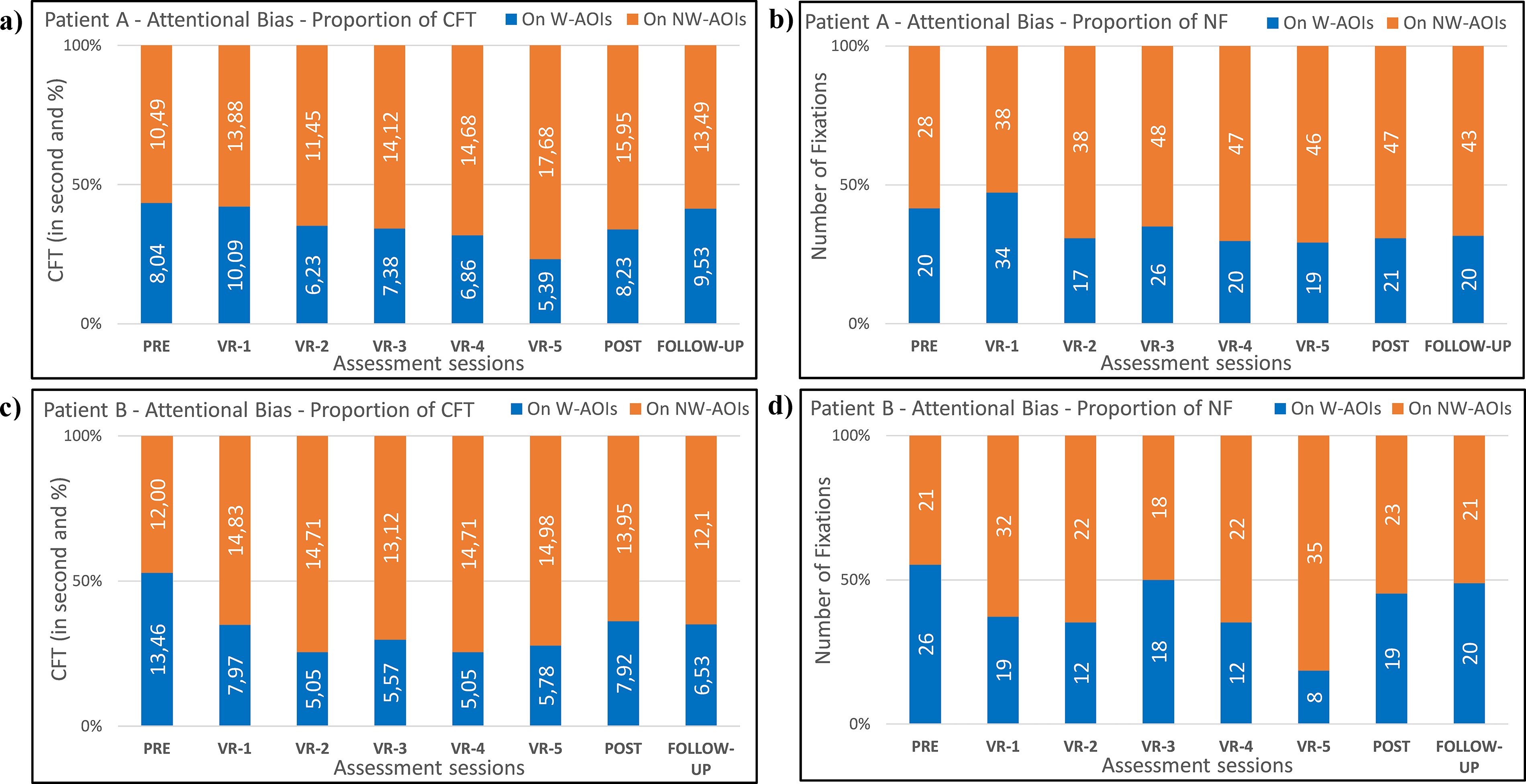
Attentional bias—evolution of CFT and NF across study sessions.
Discussion
Primary outcomes: Feasibility and acceptability
This study applied the ABMT + VR-MET protocol, previously validated in female AN patients,20,21 to two male adolescents to examine its acceptability and feasibility in this underrepresented population. The procedure showed high acceptability: both participants attended all sessions voluntarily, completed the full protocol, and reported excellent user experience (SUS > 80; “A-grade” usability). 60 No technical difficulties occurred, supporting the feasibility of VR-based intervention with male adolescents with AN.
Secondary exploratory outcomes: Clinical trajectories during intervention
Reductions in body dissatisfaction and weight-related anxiety, as well as increases in body appreciation and satisfaction throughout treatment, were observed in both patients, with improvements maintained at the 3-month follow-up. Such outcomes align with clinical observations that VR-based exposures enhance emotional engagement and reduce avoidance in body-focused interventions.3–5 Nevertheless, the specific therapeutic contribution of the VR protocol cannot be definitively isolated at this stage, as the intervention was delivered alongside a concurrent multidisciplinary HoT program. Consequently, larger-scale randomized controlled trials are necessary to determine the independent efficacy of this approach.
The two patients’ contrasting presentations illustrate the heterogeneity of male AN. Patient B showed a classical restrictive profile (FGW, body dissatisfaction, and body checking), whereas Patient A denied distortion, desiring weight gain for athletic performance. These differences may have influenced avatar perception: Patient B judged the avatar as thinner than his real body, while Patient A perceived weight-related areas as thinner and muscular regions as larger. These perceptual patterns likely influenced self-identification with the avatar (i.e., embodiment), with Patient B showing earlier and more stable increases, while Patient A showed a decline as the avatar’s BMI progressed. Patient A’s profile and feedback are consistent with features of Muscle Dysmorphia—a condition characterized by concern with insufficient muscularity.40,61 This suggests the importance of considering muscularity-oriented concerns in male-focused VR interventions. Baseline AB patterns further illustrated these features: Patient B focused on weight-related regions (similar to female AN,5,8–13,53), while Patient A prioritized muscular areas (shoulders, arms). Across treatment, AB trajectories diverged. Patient B increased attention to non-weight regions, potentially reflecting reduced avoidance. Conversely, Patient A displayed increasing AB toward muscular regions, possibly reflecting internal conflict between restrictive symptoms and a drive for muscularity. Although generalization is limited by the two-case design, these observed AB patterns may point to potential subtypes of attentional functioning. VR and eye-tracking gaze metrics thus provide a promising path toward personalized and gender-sensitive AB modification treatments. In addition, incorporating standardized muscularity measures (e.g., Drive for Muscularity Scale, 62 Exercise Dependence Scale, 63 Compulsive Exercise Test 64 ) and muscle-focused AOIs in future research would help clarify how muscularity concerns shape attentional patterns and embodiment responses in male adolescents with AN.
Conclusion
The primary goal of this preliminary report was to assess the feasibility of applying a virtual reality protocol for anorexia, combining mirror exposure and AB modification, previously validated in females, to males. While the findings suggest high acceptability and technical stability, inferences regarding clinical efficacy must be made with caution. The two-case design and the patients’ concurrent involvement in a multidisciplinary home treatment program prevent the isolation of treatment effects. However, these preliminary findings indicate that this protocol is a feasible and well-tolerated adjunct to multidisciplinary care in this case. The observed differences in AB between the two patients support the need for further large-scale research into male-specific body image mechanisms.
Authors’ Contributions
F.-A.M.-A.: Conceptualization, methodology, software, validation, formal analysis, investigation, data curation, writing—original draft, review and editing, and visualization. M.-R.: Methodology, validation, investigation, resources, writing—review and editing, and supervision. M.A.: Conceptualization, methodology, software, validation, formal analysis, investigation, and writing—review and editing. B.P.-G.: Conceptualization, software, and writing—review and editing. E.S.-T.: Resources, writing—review and editing, and supervision. M.F.-G.: Conceptualization, methodology, resources, writing—review and editing, and supervision. J.G.-M.: Conceptualization, methodology, validation, formal analysis, investigation, resources, writing—review and editing, supervision, project administration, and funding acquisition. All authors have read and agreed to the published version of the article.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and was approved by the Ethics Committee of Hospital Sant Joan de Déu in Barcelona (approval code: PS-21-20, approval date: March 25, 2021).
Informed Consent Statement
Informed consent was obtained from all subjects and their parents involved in the study.
Data Availability Statement
The data presented in this study are available upon request from the corresponding author.
Footnotes
Author Disclosure Statement
The authors declare no conflicts of interest. The funders had no role in the design of the study; the collection, analyses, or interpretation of data; the writing of the article; or the decision to publish the results. None of the authors have a financial arrangement or affiliation with any product or services used or discussed in this article.
Funding Information
This study was funded by the Spanish Ministry of Science and Innovation (Agencia Estatal de Investigación, Ministerio de Ciencia e Innovación, Spain), grant no. PID2019-108657RB-I00, funded by MCIN/AEI/10.13039/501100011033. This study also has the support of “Fundació La Marató de TV3” (grant no. 202217-10).