
Abstract
Background:
This clinical trial evaluated hepatic fat content and weight loss in adolescents with severe obesity and metabolic dysfunction–associated steatotic liver disease (MASLD) following short-term meal replacement therapy (MRT).
Methods:
Adolescents aged 12–17 years with severe obesity (BMI ≥1.2 × 95th percentile or ≥35 kg/m2) and magnetic resonance imaging–confirmed MASLD (hepatic fat fraction [HFF] ≥5%) completed a 4- to 8-week MRT program (∼500 kcal/day deficit) targeting ≥5% BMI reduction. Participants underwent 1H-magnetic resonance spectroscopy at baseline and at follow-up, along with 2-hour mixed-meal tolerance testing.
Results:
Seventeen adolescents [baseline mean (standard deviation or SD) BMI = 39.9 (4.1) kg/m2; age = 16.0 (1.6) years; 65% male; HFF = 15.6 (5.1)%] demonstrated a mean absolute decrease in BMI of 5.6% [−2.23 kg/m2; 95% confidence interval (CI): −2.45, −2.02; p < 0.001] and a 37.3% relative reduction (95% CI: 26.4%, 48.1%; p < 0.001) in HFF. Despite HFF reduction, 13 out of 17 had MASLD at study conclusion. Decrease in HFF corresponded to significant reductions in triglycerides [difference (95% CI): −5.8 mg/dL (−9.4, −2.1); p = 0.012], glucose area under the curve (AUC) [−2.2 mg/dL (−3.2, −1.3); p = 0.021], and leptin AUC [−40.5 pg/mL (−57.1, −23.9); p = 0.009]. No significant difference in alanine aminotransferase was observed.
Conclusions:
Short-term MRT was associated with reductions in liver fat and improvements in metabolic biomarkers among adolescents with MASLD. Large-scale trials are needed to evaluate the implementation of MRT as part of a multimodal treatment strategy in this population. [Clinical Trial Registration: Enhancing Weight Loss Maintenance with GLP-1 RA (BYDUREON™) in Adolescents With Severe Obesity, NCT02496611, https://clinicaltrials.gov/study/NCT02496611].
Keywords
Introduction
Metabolic dysfunction–associated steatotic liver disease (MASLD), characterized by excessive deposition of fat in the liver, is the most common pediatric liver disease. 1 Liver biopsy data suggest that ∼50%–80% of youth with severe obesity (BMI ≥1.2 × the 95th percentile or ≥35 kg/m2) have concomitant MASLD, the combination of which is further associated with a number of comorbid conditions including type 2 diabetes mellitus, hypertension, and dyslipidemia.2–6 Moreover, without successful treatment, MASLD may progress to metabolic-associated steatohepatitis (MASH), cirrhosis, and hepatocellular carcinoma, reducing lifespan and potentially requiring liver transplantation. 7 Therefore, the development of safe, effective, and scalable treatment strategies aimed at reducing hepatic fat and preventing hepatocellular injury prior to progression is of paramount importance.
Despite the high prevalence and significance of MASLD, effective treatment strategies in youth are limited. Lifestyle modification therapy is the cornerstone of pediatric MASLD and obesity treatment. However, even under ideal treatment conditions, lifestyle modification often fails to sustainably reverse MASLD in youth.8,9 While novel dietary approaches such as low sugar intake have been shown to be effective in the short term, they are impractical for most participants and families from an implementation and cost standpoint. 10 Additionally, medications repurposed for the treatment of other chronic diseases such as diabetes, including metformin, in particular, have shown limited impact.9,11–14 Metabolic and bariatric surgery (MBS) has been shown to offer some resolution of MASH and MASLD, yet access remains limited.15,16 Moreover, MBS is not indicated for individuals with less severe obesity, as well as those who have not yet developed significant metabolic complications of obesity. Thus, alternative solutions must be examined to fill this clinical treatment gap.
The purpose of this study was to evaluate changes in liver fat content following short-term meal replacement therapy (MRT) among adolescents with severe obesity. We examined youth with severe obesity and MASLD prior to and after a 4- to 8-week MRT program targeting a ≥5% BMI reduction. We hypothesized that youth with severe obesity and MASLD would demonstrate significant reductions in liver fat content following MRT-associated short-term weight loss.
Materials and Methods
Study Design
We performed a single-site, nonrandomized clinical trial to examine changes in weight and liver fat content following short-term (4–8 weeks) MRT in adolescents with severe obesity, the details of which have been previously published. 17 The primary inclusion criteria for the main trial were adolescents aged 12–17 years with a BMI ≥1.2 × the 95th percentile or ≥35 kg/m2, whichever was lower. Adolescents with type 2 diabetes, prior weight-loss surgery, and those taking medications that alter weight, lipid, or glucose metabolism were excluded. Of the 100 enrolled participants, 66 completed MRT. Magnetic resonance imaging (MRI) was optional, and only those who completed both a baseline and post-meal replacement MRI and had MRI-confirmed MASLD at baseline were eligible for the current analysis (n = 17). Participants were allowed 4–8 weeks to achieve the ≥5% BMI reduction target. Those who met the target after a minimum of 4 weeks underwent follow-up MRI at that time, while those who did not meet the target underwent follow-up MRI at 8 weeks. Participants and parents/legal guardians provided written informed assent and consent, respectively, before enrollment. The study protocol was approved by the University of Minnesota Institutional Review Board and registered at ClinicalTrials.gov (NCT02496611).
Meal Replacement Program
All participants were instructed to strictly adhere to a meal replacement program for at least 4 weeks and up to 8 weeks, with the goal of achieving ≥5% BMI reduction. 18 Once a participant achieved the ≥5% BMI reduction target (but no sooner than 4 weeks), they were scheduled for their follow-up MRI visit. Those who did not achieve the target were scheduled for their follow-up MRI visit at 8 weeks. The prescribed eating plan consisted of three SlimFast® shakes for breakfast and lunch, two prepackaged low-calorie frozen entrée meals for dinner (Weight Watchers®, Smart Ones®), two servings of fruit, and three servings of vegetables per day, totaling ∼1370 kcal. Shakes and frozen meals were provided free of charge to the participants. To monitor compliance, participants were required to maintain a food log throughout the meal replacement induction phase and received weekly telephone check-ins from the study coordinators. Additionally, all participants received the same lifestyle therapy curriculum, which was adapted from the National Institute of Diabetes and Digestive and Kidney Diseases-sponsored Treatment Options for Type 2 Diabetes in Adolescents and Youth study lifestyle modification therapy materials 19 and has been used in our previous clinical trials.20,21 Trained study coordinators delivered the lifestyle therapy that focused on making small, successive changes in physical activity behaviors with self-monitoring, goal setting, reinforcement for goal achievement, stimulus control, social support, problem-solving, and motivational techniques.
Clinical Measurements
All clinical measurements and hepatic fat fraction (HFF) assessments were performed in the morning under fasting conditions at baseline (prior to initiating MRT) and at the follow-up visit. Height and weight were measured using a calibrated, wall-mounted stadiometer and an electronic scale, respectively. Total percent body fat, visceral fat, and lean muscle mass were determined by dual-energy X-ray absorptiometry (GE Healthcare®). Tanner stage was determined by trained pediatricians. Fasting (≥12 hours) blood samples were collected for the measurement of lipids [total cholesterol, low-density lipoprotein (LDL) cholesterol (LDL-cholesterol), high-density lipoprotein (HDL) cholesterol (HDL-cholesterol), and triglycerides], glucose, insulin, alanine aminotransferase (ALT), and hemoglobin A1c (assayed in Fairview Diagnostics Laboratories, Minneapolis, MN, a CDC-certified laboratory). A mixed meal tolerance test (MMTT) was used to stimulate appetite and satiety hormones [amylin, gastric inhibitory polypeptide (GIP), glucagon-like peptide-1 (GLP-1), and leptin] that were measured over a 2-hour period. Hormone area under the curve (AUC) measurements were calculated across seven samples collected over 2 hours using the trapezoidal method and divided by 120 minutes to give a time-weighted average measurement.
Measurement of Hepatic Fat Content
HFF was measured by MRI via 1H-magnetic resonance spectroscopy (MRS) at the Magnetic Resonance Research Institute at the University of Minnesota. HFF was measured with single-voxel 1H-MRS on a 3.0-T Trio whole-body MRI scanner (Siemens Healthineers®, Erlangen, Germany) using the HISTO sequence software package from Siemens’ LiverLab. The MRS measurement was performed twice to assess the repeatability of the HFF concentration. Participants were positively identified as having MASLD after obtaining two consecutive HFF values ≥5%.
Statistical Analysis
Data were summarized as mean (standard deviation or SD) or N (%) for continuous and categorical participant characteristics, respectively, at baseline and after MRT. One-sample t-tests were utilized to assess absolute change in body composition measures as well as relative change in BMI and HFF from baseline to post-MRT. Additionally, multiple linear regression models were used to evaluate the effect of change in HFF on selected outcomes after adjusting for sex, Tanner stage, and baseline outcome measurements. Robust variance estimation was used for 95% confidence intervals (CIs) and p-values. All tests were two-tailed, and p-values <0.05 were considered statistically significant. All analyses were conducted using R version 4.3.1 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Seventeen adolescents with MASLD completed both baseline and post-meal replacement MRI. Most participants were male (65%) and identified as Caucasian (82%) (Table 1). Participants had a mean (SD) age of 16.0 (1.6) years, with a baseline BMI of 39.9 (4.1) kg/m2, HFF of 15.6 (5.1)%, and ALT level of 51.0 (36.6) U/L.
Demographic and Clinical Characteristics of Participants
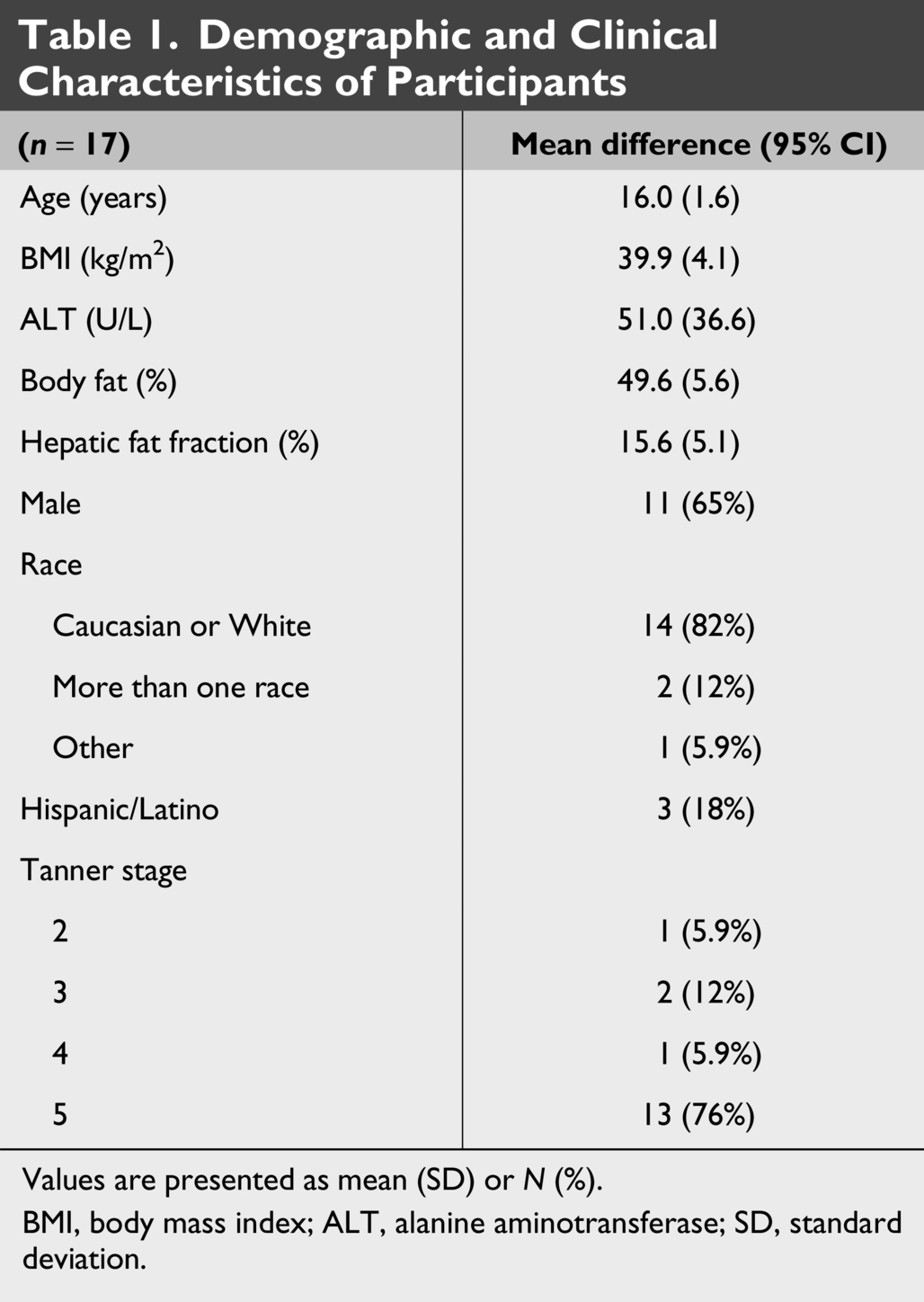
Values are presented as mean (SD) or N (%).
BMI, body mass index; ALT, alanine aminotransferase; SD, standard deviation.
The mean duration of MRT from initiation to follow-up liver measurements was 40.8 days (5.8 weeks). Following the MRT program, BMI decreased by a mean of 5.6% across the full cohort (absolute change, −2.23 kg/m2; 95% CI: −2.45 to −2.02; p < 0.001) (Fig. 1, Table 2). Participants also experienced a significant reduction in HFF, with a mean absolute decrease of 5.3% (95% CI: −7.0% to −3.6%; p < 0.001) and a relative reduction of 37.3% (95% CI: 26.4%–48.1%; p < 0.001) (Fig. 2). Liver volume decreased by a mean of 222.9 mL (95% CI: −354.1 to −91.7 mL; p = 0.002), corresponding to a 10.3% reduction from baseline (Table 2). Reductions were consistent across participants, with similar trends observed in both males and females (Fig. 3). Although the cohort demonstrated a statistically significant reduction in HFF, 13 out of 17 adolescents continued to meet criteria for MASLD at study completion. Statistically significant reductions were also observed in total tissue fat, visceral fat mass, subcutaneous fat mass, fasting insulin, triglycerides, HDL-cholesterol, and LDL-cholesterol, while fasting ALT did not change significantly.
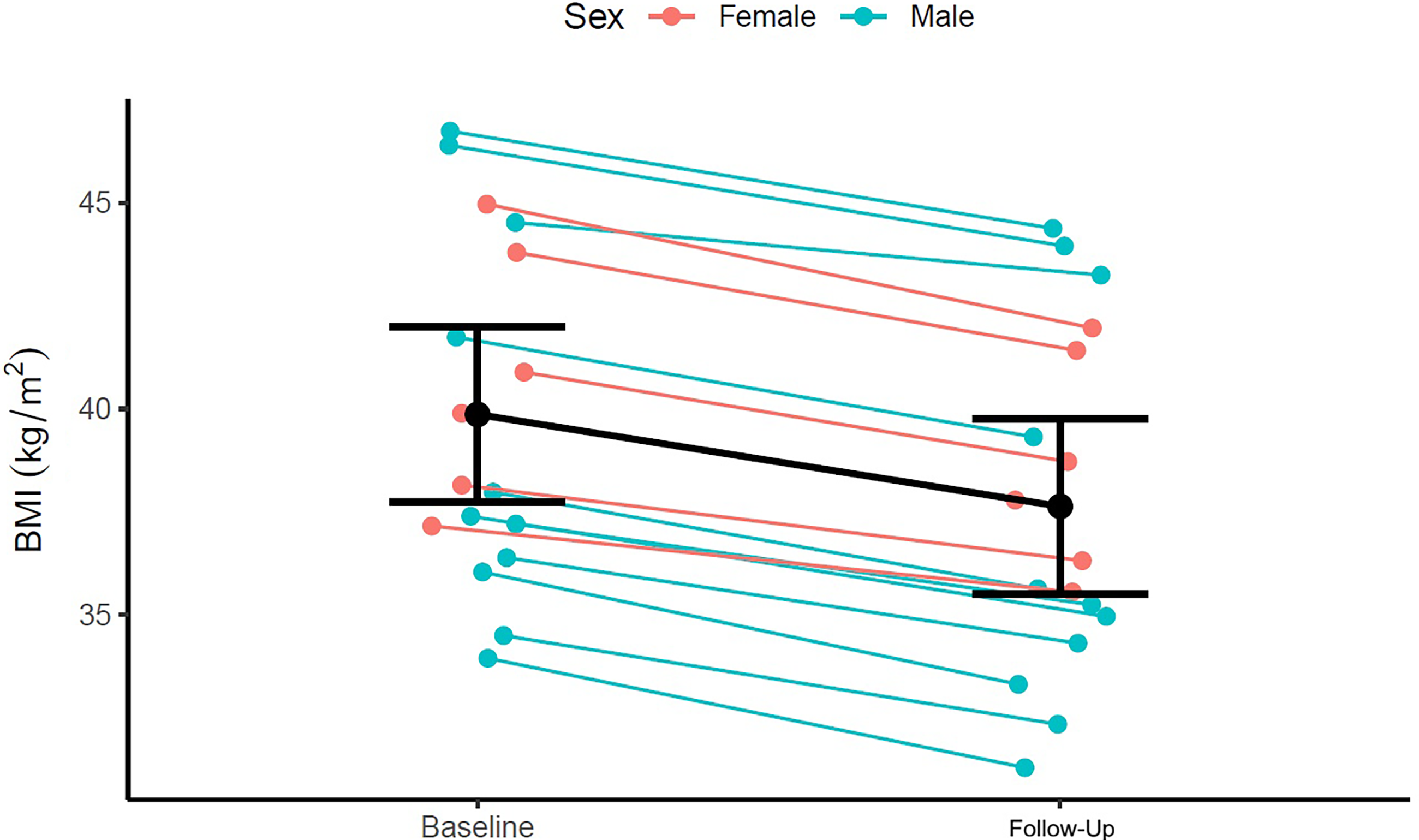
Change in BMI before and after MRT. Line plot depicts individual changes in BMI (kg/m²) at baseline and at follow-up, stratified by sex (see legend). Black line represents group mean and SD. Follow-up visit occurred between 4 and 8 weeks after MRT initiation (mean 5.8 weeks). MRT, meal replacement therapy; SD, standard deviation.
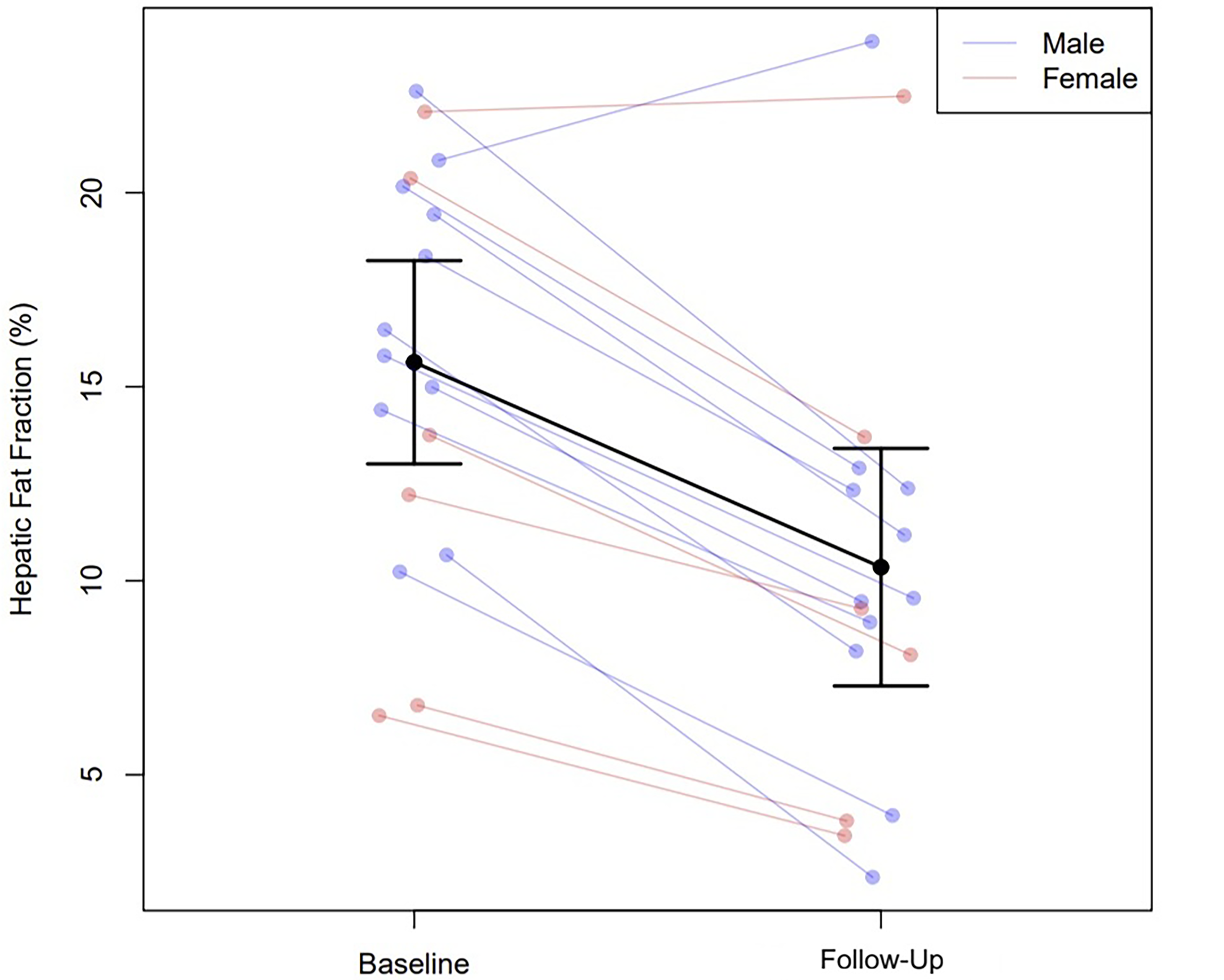
Change in HFF before and after MRT. Line plot depicts individual changes in HFF (%) from baseline to follow-up following a structured meal replacement intervention, stratified by sex (blue = male, red = female). Black line represents group mean and SD. Follow-up visit occurred between 4 and 8 weeks after MRT initiation (mean 5.8 weeks). HFF, hepatic fat fraction.
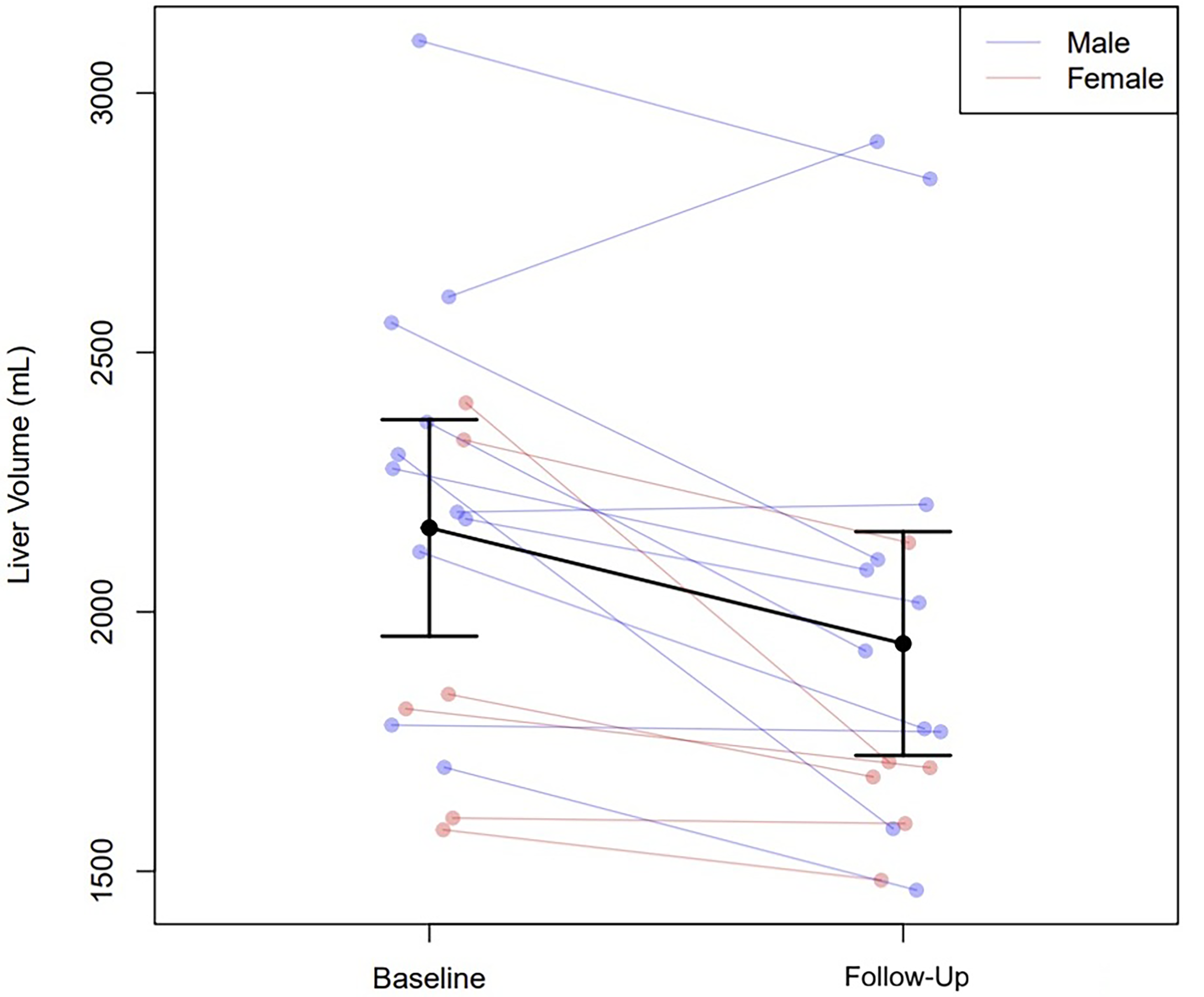
Change in liver volume before and after MRT. Line plot depicts individual changes in liver volume (mL) from baseline to follow-up following a structured meal replacement intervention, stratified by sex (blue = male, red = female). Black line represents group mean and SD. Follow-up visit occurred between 4 and 8 weeks after MRT initiation (mean 5.8 weeks).
Unadjusted Changes in Clinical Outcomes and Mixed-Meal Tolerance Test Values Between Baseline and Post-Meal Replacement
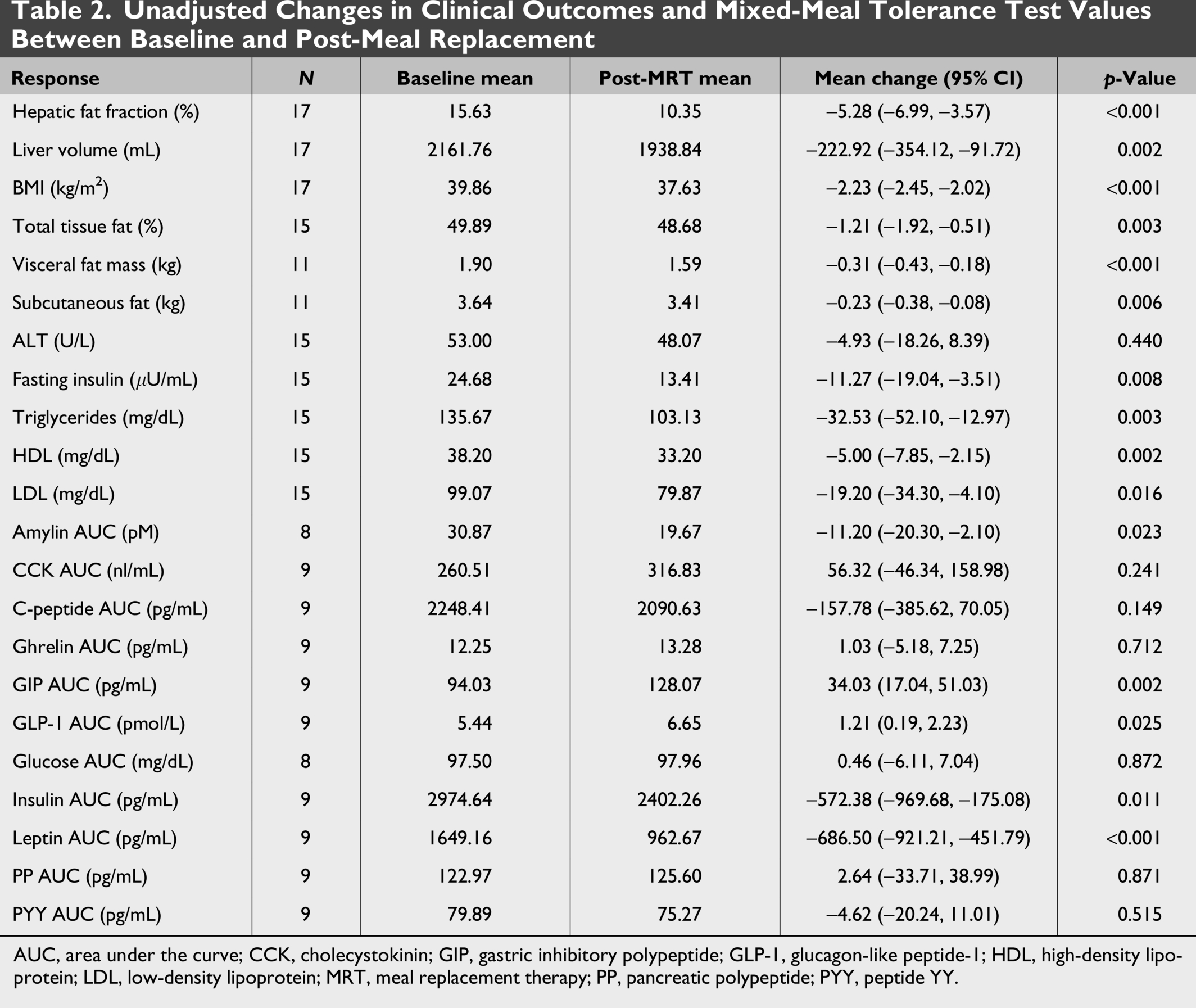
AUC, area under the curve; CCK, cholecystokinin; GIP, gastric inhibitory polypeptide; GLP-1, glucagon-like peptide-1; HDL, high-density lipoprotein; LDL, low-density lipoprotein; MRT, meal replacement therapy; PP, pancreatic polypeptide; PYY, peptide YY.
Under MMTT conditions, statistically significant absolute mean increases were observed in GIP AUC (34.0 pg/mL; 95% CI: 17.04–51.03; p = 0.002) and GLP-1 AUC (1.21 pmol/L; 95% CI: 0.19–2.23; p = 0.025). Statistically significant decreases were observed in amylin AUC (−11.20 pM; 95% CI: −20.30 to −2.10; p = 0.023), insulin AUC (−572.38 pg/mL; 95% CI: −969.68 to −175.08; p = 0.011), and leptin AUC (−686.50 pg/mL; 95% CI: −921.21 to −451.79; p < 0.001). No statistically significant differences were observed in other postprandial hormones.
Table 3 presents adjusted regression models evaluating associations between changes in HFF and follow-up outcomes, with adjustment for sex, Tanner stage, and baseline values. For each 1% decrease in HFF, statistically significant reductions were observed in triglycerides (−5.77 mg/dL; 95% CI: −9.43 to −2.10; p = 0.012), glucose AUC (−2.24 mg/dL; 95% CI: −3.22 to −1.26; p = 0.021), and leptin AUC (−40.52 pg/mL; 95% CI: −57.12 to −23.92; p = 0.009). No other adjusted associations reached statistical significance.
Adjusted Regression Models Estimating the Mean Difference in Follow-Up Clinical Outcomes Associated with Each 1% Reduction in Hepatic Fat Fraction from Baseline to Follow-Up
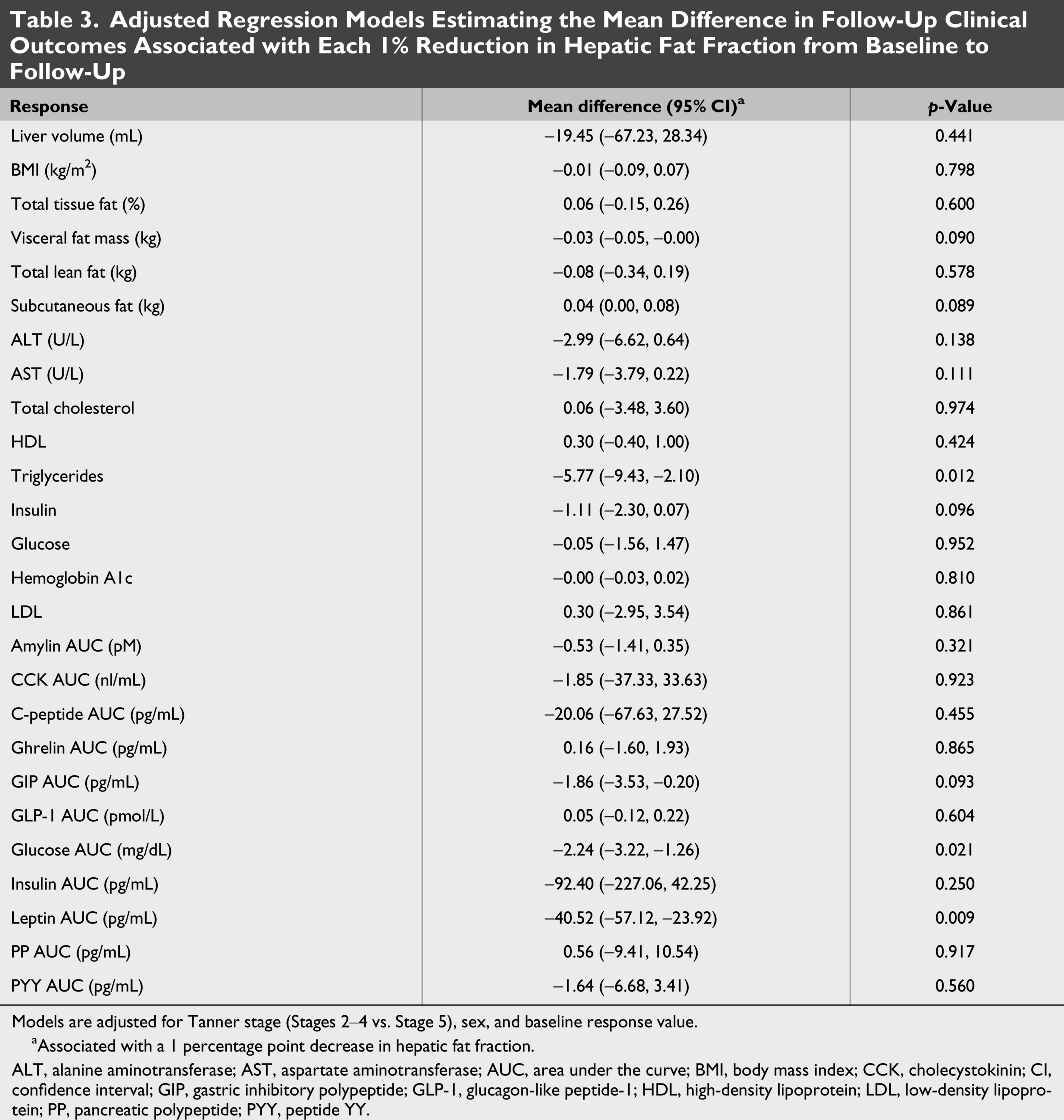
Models are adjusted for Tanner stage (Stages 2–4 vs. Stage 5), sex, and baseline response value.
Associated with a 1 percentage point decrease in hepatic fat fraction.
ALT, alanine aminotransferase; AST, aspartate aminotransferase; AUC, area under the curve; BMI, body mass index; CCK, cholecystokinin; CI, confidence interval; GIP, gastric inhibitory polypeptide; GLP-1, glucagon-like peptide-1; HDL, high-density lipoprotein; LDL, low-density lipoprotein; PP, pancreatic polypeptide; PYY, peptide YY.
Discussion
This study evaluated changes in weight and hepatic fat content following short-term MRT among adolescents with severe obesity and MASLD, targeting a
The hepatic fat reduction observed in our study aligns with previous pediatric trials demonstrating the efficacy of short-term dietary interventions in adolescents with obesity and MASLD. For instance, Schwimmer et al. 10 reported an 8% absolute (32% relative) reduction in hepatic steatosis following 8 weeks of a low-free sugar diet in adolescent males with MASLD. In comparison, using comparable measurement techniques, we observed a modestly lower absolute reduction in hepatic steatosis (5.3%), but a similar relative reduction (37.3%) over the same time frame. Although both approaches achieved reductions in hepatic fat content, they differ in implementation and mechanism. The nutrient-specific strategy employed by Schwimmer et al. relied on intensive free sugar restriction to <3% of daily calories using home-prepared meals and was mechanistically linked to reductions in de novo hepatic lipogenesis. 22 In contrast, our calorie-based, whole-meal replacement intervention, targeting a 500 kcal/day deficit within a structured lifestyle program, offers a potentially more scalable and pragmatic alternative to this approach, while likely operating through a disparate metabolic pathway. Additionally, inclusion of both male and female participants and assessment of postprandial hormone responses in our study enhance generalizability and provide insight into enteroendocrine adaptations not captured by fasting biomarkers alone.
Our findings are consistent with adult studies demonstrating that low-calorie and meal replacement-based interventions improve hepatic and metabolic health. In adults with obesity and an elevated fatty liver index, de Luis et al. reported reductions in hepatic steatosis and metabolic improvements with partial meal replacement hypocaloric diets. 23 Likewise, very-low-calorie diet (VLCD) studies have consistently shown substantial reductions in hepatic steatosis across adult cohorts, with Scragg et al. 24 demonstrating significant improvements in liver stiffness (13.0 kPa to 7.0 kPa) alongside enhanced metabolic control and quality-of-life measures in adults with clinically significant nonalcoholic fatty liver disease (NAFLD). Furthermore, Herrington et al.’s scoping review reinforced these findings, showing that VLCDs consistently reduced hepatic steatosis and improved metabolic parameters across multiple adult studies, with completion rates of 69%–93%. 25 Our results extend this literature by suggesting that comparable hepatic and metabolic improvements may be achievable in adolescents through a 4- to 8-week meal replacement intervention delivered within a structured lifestyle program. Although developmental differences in hepatic metabolism, inflammatory burden, and metabolic resilience may influence treatment response in adolescents, the concordance of outcomes across age groups supports meal replacement–based strategies as a promising therapeutic approach for MASLD.
The regression analyses presented in Table 3 demonstrate statistically significant dose–response relationships between hepatic fat reduction and select metabolic parameters following MRT. For each 1% decrease in HFF, participants experienced a 5.77 mg/dL reduction in triglycerides, a finding that is particularly relevant given the strong association between elevated triglycerides and cardiovascular risk in adolescents with obesity. Similarly, the observed 2.24 mg/dL reduction in glucose AUC per 1% decrease in HFF suggests improved glucose handling and enhanced insulin sensitivity, which may help prevent progression to type 2 diabetes. The decrease in leptin AUC of 40.52 pg/mL per 1% hepatic fat reduction is also noteworthy, as it reflects restoration of leptin sensitivity alongside fat mass reduction, potentially facilitating sustained weight management. While the majority of associations in Table 3 did not reach statistical significance, potentially reflecting the small sample size, those that did suggest that hepatic fat reduction through MRT may operate through multiple metabolic pathways, and that more intensive or prolonged interventions could yield proportionally larger effects, although this warrants investigation in larger trials.
Three unexpected findings emerged from our study that warrant further discussion. First, despite achieving significant hepatic fat reduction, ALT levels remained unchanged following MRT. This finding contrasts with Schwimmer et al., 10 who demonstrated concurrent reductions in both hepatic steatosis and ALT following an 8-week low free sugar diet in adolescent boys with NAFLD. Importantly, the ALT reduction observed in that study was suspected to be attributable to the specific restriction of dietary free sugars, and the consequent reduction in fructose-driven de novo hepatic lipogenesis, rather than caloric restriction or weight loss alone, as evidenced by the only moderate correlation between weight change and hepatic fat reduction reported in their cohort. Our calorie-based meal replacement intervention, which targeted an overall energy deficit rather than macronutrient-specific restriction, may therefore have been insufficient to reduce hepatic lipogenic substrate to a degree sufficient to drive ALT normalization over this timeframe. These findings highlight an important mechanistic distinction between dietary approaches and suggest that ALT may be a more sensitive marker of sugar-specific hepatic injury than of caloric restriction-mediated fat reduction. We also cannot exclude the possibility that unmeasured factors, such as intercurrent illnesses or medication changes during the intervention period, may have contributed to the lack of ALT response, representing a limitation of the study. Second, despite concurrent reductions in LDL-cholesterol and triglycerides, HDL-cholesterol also decreased modestly after 8 weeks of MRT. This pattern has been described during active, hypocaloric weight-loss phases, where transient reductions in HDL-cholesterol are theorized to result from decreased apolipoprotein A-I production, with levels typically recovering during weight maintenance or with reintroduction of dietary fat, particularly unsaturated fat.26,27 In this context, the HDL-cholesterol decline likely reflects energy deficit and diet composition rather than adverse atherogenic remodeling and may be a suboptimal biomarker for assessing the cardiovascular effects of short-term MRT. Last, our study found that MASLD persisted in 76% of participants despite achieving a statistically significant reduction in HFF. This finding suggests that complete resolution of MASLD may require more intensive interventions, longer treatment duration, or alternative therapeutic approaches beyond the 4- to 8-week MRT protocol employed in this study. This partial response pattern also raises important questions regarding optimal treatment targets and whether the current diagnostic threshold for MASLD resolution is appropriate for monitoring treatment efficacy in adolescents. Further investigation is needed to determine the clinical significance of partial vs. complete MASLD resolution and to establish evidence-based treatment protocols that achieve sustained hepatic fat normalization in this population.
While lifestyle interventions remain first-line therapy for adolescents with severe obesity, with or without MASLD, pharmacologic options are increasingly available. Glucagon-like peptide-1 receptor agonists, including liraglutide and semaglutide, have demonstrated significant short-term reductions in BMI and improvements in ALT among adolescents aged 12 years or older.28,29 Resmetirom, the only FDA-approved therapy for adults with MASH and moderate to advanced fibrosis, has been shown to lead to complete resolution of MASH in 25.9%–29.9% of patients but has yet to be evaluated in pediatric populations. 30 To date, bariatric surgery remains the most effective intervention for adolescents with severe obesity and MASLD.16,31,32 In adolescents with biopsy-confirmed NASH, laparoscopic sleeve gastrectomy has demonstrated superior hepatic improvement compared to intragastric weight-loss devices plus lifestyle therapy or lifestyle intervention alone, with 75% achieving steatosis resolution and complete NASH resolution at 1 year. 16 Similarly, among 109 adults with biopsy-proven NASH and/or fibrosis, Lassailly et al. 33 reported that MBS resulted in NASH resolution in 85% of patients, with 34% experiencing fibrosis improvement at 1 year post-surgery. However, longer-term studies are needed to determine the durability of these benefits, and access to bariatric surgery among adolescents remains limited for multiple reasons, including social stigma and insurance-related barriers. 34 In this context, our study addresses a critical gap in the treatment armamentarium by demonstrating that a standardized, accessible intervention can achieve short-term reductions in hepatic fat. This approach is readily implementable across diverse health care settings, requires minimal specialized resources, and may serve as an effective bridge between lifestyle interventions and more intensive treatments. Given the progressive nature of MASLD and its association with future cardiometabolic disease, early implementation of accessible treatments such as MRT may meaningfully influence long-term outcomes as pharmacologic and surgical options continue to evolve.
Our study has several limitations. First, the relatively small sample size, short duration, and single-center design may limit the generalizability of our findings to broader populations or care settings. Second, the ability for participants to opt out of MRI introduces potential selection bias, as participants who underwent MRI and completed the protocol may represent a more adherent or motivated subset of adolescents with obesity and MASLD. Third, while participants were monitored weekly via telephone check-ins and required to maintain food logs, detailed compliance data are not formally reported, and the reasons for noncompletion of study procedures such as the MMTT were not systematically collected. This limits conclusions regarding the relationship between adherence and treatment response, as well as our ability to characterize barriers to full protocol completion. Fourth, baseline dietary intake was not formally assessed, and the ∼500 kcal/day deficit therefore represents an approximation based on the prescribed meal replacement plan rather than a measured individualized deficit. Fifth, the absence of a control group and nonrandomized study design preclude definitive conclusions regarding causality and limit the ability to isolate the effects of the meal replacement intervention. Last, although hepatic fat content was rigorously measured using 1H-MRS and supported by robust internal validity metrics, we did not include liver histology or elastography to assess inflammation or fibrosis, which limits our understanding of broader hepatic remodeling in response to treatment.
Conclusions
Our study demonstrates that short-term MRT, delivered as part of a comprehensive lifestyle and behavioral intervention, is associated with reductions in hepatic fat content and improvements in metabolic health among adolescents with obesity and MASLD. These changes were accompanied by favorable shifts in body composition and postprandial hormone responses, suggesting early improvements in insulin sensitivity and enteroendocrine function. While further research is needed to assess long-term durability and histological outcomes, future studies should explore the integration of short-term MRT protocols into broader lifestyle, behavioral, and pharmacologic treatment frameworks, as well as their role in disease modification prior to irreversible hepatic injury. Based on the magnitude and consistency of observed changes, these results are likely to be reproducible and clinically meaningful in similar adolescent populations, particularly when paired with structured support and monitoring. Collectively, this work highlights the potential for early, structured nutritional interventions to alter the trajectory of pediatric MASLD and serve as a pragmatic entry point into long-term disease management.
Authors’ Contributions
J.B.R.: Formal analysis, visualization, and writing—original draft. J.M.W.: Conceptualization, methodology, investigation, formal analysis, validation, and writing—review and editing. P.J.B., E.P., and K.D.R.: Formal analysis, validation, and writing—review and editing. S.A.: Writing—review and editing. C.K.F., A.S.K., and J.R.R.: Conceptualization, methodology, investigation, supervision, and project administration.
Footnotes
Acknowledgments
The authors would like to thank all of the adolescents who participated in this study.
Ethical Considerations
The study was approved by the University of Minnesota Institutional Review Board, and all procedures were conducted in accordance with the ethical standards of the institutional and national research committees.
Consent to Participate
Written informed assent was obtained from all adolescent participants, and written informed consent was obtained from parents or legal guardians prior to study participation.
Consent for Publication
Not applicable. This article does not contain any individual-level identifying data, images, or videos requiring consent for publication.
Data Availability
The data supporting the findings of this study are not publicly available due to ethical and privacy considerations related to human participant data but are available from the corresponding author upon reasonable request and with appropriate institutional approvals.
Author Disclosure Statement
J.R.R. receives support from Boehringer Ingelheim Pharmaceuticals in the form of drug/placebo and serves as a site investigator for clinical trials sponsored by Eli Lilly and Recordati. He serves on the advisory board for Calorify and receives educational honoraria from Kraft Heinz. A.S.K. serves as a consultant for Vivus Pharmaceuticals, Novo Nordisk Pharmaceuticals, and Weight Watchers, but does not accept personal or professional income for these services. He also receives research support from AstraZeneca Pharmaceuticals in the form of drug/placebo. All other authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding Information
This work was supported in part by the National Center for Advancing Translational Sciences award UL1TR002494 and by R01DK105953 (A.S.K.).