
Abstract
Objective:
To examine changes in weight status after initiating zonisamide in children with epilepsy and elevated body mass index (BMI).
Study Design:
Retrospective chart review of children aged 2 to ≤18 years with epilepsy treated with zonisamide, assessing BMI changes over 2 years.
Results:
A total of 140 children were included; mean age (SD) at initiation was 9.60 years (3.93). BMI categories included 28 children with severe obesity, 28 with mild–moderate obesity, 28 with overweight, and 56 with healthy weight. Participants were 56.6% female, 91.4% non-Hispanic/Latino, and 88.6% White. At 2 years, BMI z score decreased significantly across all BMI groups: severe obesity −0.38 (N = 13, 95% CI −0.64 to −0.13; p = 0.003), mild-moderate obesity −0.39 (N = 15, 95% CI −0.62 to −0.16; p = 0.001), overweight −0.60 (N = 14, 95% CI −0.84 to −0.36; p < 0.001), and healthy weight −0.46 (N = 21, 95% CI −0.63 to −0.28; p < 0.001). Significant BMI z score reductions were also observed across age groups: 2–10 years −0.48 (N = 40, 95% CI −0.62 to −0.34), >10–13 years −0.27 (N = 15, 95% CI −0.50 to −0.04), and ≥13 years −0.63 (N = 12, 95% CI 0.89 to −0.36).
Conclusions:
BMI reduction persisted up to 2 years following zonisamide initiation in children with epilepsy. Further prospective studies are needed to evaluate the weight loss effect and safety of zonisamide in children with epilepsy and elevated BMI.
Introduction
Obesity represents a major public health challenge among the pediatric and adolescent population, with its prevalence having more than tripled over the past several decades. Current estimates indicate that approximately 21.1% of youth are affected by obesity, while severe obesity, defined as a body mass index (BMI) ≥120% of the 95th percentile for age and sex (%BMIp95), affects up to 7% of children and adolescents.1,2 This alarming upward trend is of particular concern given its well-established association with adverse cardiometabolic outcomes.1,3 Children with epilepsy have a higher prevalence of obesity compared with peers without epilepsy.4–7 In the 2017–2018 National Survey of Children’s Health (ages 10–17 years), the prevalence of obesity was 27.8% in adolescents with epilepsy compared with 15.1% in those without epilepsy, and epilepsy remained associated with higher odds of obesity after adjustment for various demographic and socioecological factors (adjusted OR 2.1, 95% CI 1.2–3.8). 4 In children with untreated, newly diagnosed epilepsy at a single center in the United States, 38.6% were overweight or had obesity. 6
The increased rates of obesity in children with epilepsy are likely due to interplay of several contributing factors, including the use of certain antiepileptic drugs (e.g., valproic acid), reduced levels of physical activity, sleep disruption and neurodevelopmental comorbidities.4,6,8–10
Zonisamide is approved by United States Food and Drug Administration (FDA) for the treatment of focal seizures in children older than 16 years of age and in Europe for children ≥6 years as an adjunctive treatment for focal seizures.11,12 Beyond its antiseizure activity, zonisamide has been associated with appetite suppression and weight loss.13–18 The precise mechanism by which zonisamide causes weight loss is not fully understood, though several pharmacological properties have been proposed. The most likely mechanisms involve modulation of serotonergic and dopaminergic neurotransmitter systems. Other potential mechanisms include weak carbonic anhydrase inhibition, which may alter taste and produce an anorexic effect. Additionally, zonisamide may affect appetite-regulating peptides in the brain and periphery, though these effects have not been fully characterized.13,19 This mechanism is similar to that of topiramate, an antiseizure medication which has been approved for weight management in adolescents 12 years of age and older when used in combination with phentermine. 20 Topiramate has also been used off-label as monotherapy for weight management in children including those below 12 years of age, a group for whom there are no currently approved obesity medications.21–24
Several studies have investigated the role of zonisamide in the management of obesity among adults.13–17 In one study, 57% of participants receiving zonisamide achieved ≥5% weight loss. 13 Treatment with zonisamide was associated with beneficial effects on body weight, cardiometabolic risk factors including serum triglycerides, HbA1c, and high-sensitivity C-reactive protein, and hepatic steatosis in patients with epilepsy.19,25 Data on the effect of zonisamide on weight status in children remains limited.26,27 In this study, we conducted a retrospective evaluation of the weight loss effects of zonisamide in children with epilepsy who also have overweight or obesity and examined the association between medication dose and BMI changes.
Methods
This retrospective cohort study was conducted through a chart review of children and adolescents (aged ≤18 years) who received zonisamide for seizure management in the outpatient setting at Mayo Clinic between May 2017 and November 2025. The study protocol was reviewed and approved by the Mayo Clinic Institutional Review Board.
Study Participants
The study initially included children and adolescents aged ≤18 years who had been prescribed zonisamide for seizure management at Mayo Clinic for a minimum duration of 3 months. A total of 558 patients were screened. Exclusion criteria comprised concurrent use of medications known to affect weight (e.g., valproic acid, steroids, antipsychotics), or medical conditions known to influence BMI status. Patients who declined Minnesota research authorization were excluded. In addition, individuals with fewer than two available BMI measurements during the treatment period were excluded. The final analytic cohort included 140 children. We identified 28 participants with overweight (BMI ≥ 85th to <95th percentile), 28 with mild to moderate obesity (BMI ≥ 95th percentile to <120% of the 95th percentile [%BMIp95]), and 28 with severe obesity (BMI ≥ 120%BMIp95). An additional 56 children with epilepsy and healthy weight (BMI ≥ 5th to < 85th percentile) were randomly selected resulting in 28 children per group at a 2:1 ratio.
Data Collection
Demographic and anthropometric data were obtained through a comprehensive review of electronic medical records. Extracted variables included race/ethnicity, sex, age, age at zonisamide initiation, height percentile and z score and BMI percentile and z score. BMI values were collected for the 3 months preceding zonisamide initiation and throughout the treatment period, up to 2 years following the start date. Data regarding antiseizure medications known to cause weight gain (e.g., valproic acid) discontinued within 6 months prior to starting zonisamide were obtained. Baseline BMI was defined as the most recent BMI measurement on or before the initiation of zonisamide. BMI data were included up to 2 years postinitiation or until the patient met an exclusion criterion, such as concurrent use of a medication known to influence weight or development of a medical condition affecting BMI while on therapy.
Changes in BMI z score were analyzed. For children with severe obesity, %BMIp95 was also utilized since z-scores and percentiles on the Centers for Disease Control and Prevention (CDC) growth charts lose precision at extreme BMI values.28,29 Thus, %BMIp95 was also used to classify obesity severity and quantify change in BMI status over time. 30
BMI z scores and %BMIp95 were calculated using CDC and National Center for Health Statistics reference standards. 31 Participants were categorized into four baseline BMI groups: healthy weight (BMI ≥ 5th to < 85th percentile), overweight (≥85th to <95th percentile), mild-to-moderate obesity (≥95th percentile to < 120%BMIp95), and severe obesity (≥120%BMIp95).
Changes in BMI were evaluated from baseline through 24 months following zonisamide initiation. Data were grouped into five time intervals: baseline, 3–6, 7–12, 13–18, and 19–24 months. When multiple measurements occurred within an interval, the most recent value was used. Charts were reviewed to verify exclusion of participants receiving weight-altering medications or those with medical conditions affecting BMI. Implausible or erroneous BMI values were excluded.
Height z-scores and percentiles were obtained at baseline and at the treatment endpoint corresponding to the last recorded BMI measurement. Additional variables extracted included the maximum tolerated zonisamide dose in mg/kg, duration of treatment, and any reported adverse effects, along with the corresponding dose and time to onset. All data were collected and managed using the Research Electronic Data Capture (REDCap) system hosted at Mayo Clinic. 32
Statistical Methods
The primary outcome was the change in BMI z score from baseline, while the secondary outcome was the change in BMI expressed as %BMIp95 for age and sex among participants in the severe obesity group, as well as changes in BMI metrics across each follow-up interval. Independent variables included duration of follow-up, baseline BMI category, age, sex, race, and ethnicity. To evaluate longitudinal changes, six-time bins were constructed to aggregate data across the 24-month follow-up period.
Quantitative variables were summarized using median and interquartile range (IQR) or mean and standard deviation (SD) according to data distribution. Categorical variables were summarized as frequencies and percentages. Histograms and quantile–quantile (Q–Q) plots were used to assess the normality of continuous variables.
Patients were categorized into four groups based on their baseline BMI and three groups based on their age prior to the initiation of zonisamide. Changes in BMI z score before and after treatment were assessed using the paired t-test. Nonparametric tests were used in the sensitivity analysis. The one-way ANOVA was utilized to evaluate differences in BMI z score changes among the four baseline BMI groups. A Kruskal–Wallis test was conducted to assess changes in height z-scores and height percentiles before and after treatment for the overall cohort.
A linear mixed-effects model was used to evaluate longitudinal changes in BMI z-score over time, accounting for repeated measurements within individuals and variable follow-up durations. The model accounted for age at zonisamide initiation, sex, race, ethnicity, baseline BMI category, treatment duration, and recent valproate discontinuation. Timepoint and BMI category were modeled as categorical fixed effects, including their interaction. Covariates were selected a priori based on clinical relevance and potential association with BMI trajectory and included recent valproate exposure, sex, age at medication initiation, and zonisamide dose in mg/kg. Recent valproate exposure and sex were modeled as binary categorical variables, whereas age at medication initiation and dose were modeled as continuous covariates. The model included a participant-specific random intercept to account for within-subject correlation from repeated BMI measurements, using a compound symmetry covariance structure.
For all hypothesis tests, point estimates, 95% confidence intervals (CI) (from the linear mixed-effects models and unadjusted data), and p-values (two-sided) were reported, with statistical significance defined as p < 0.05. All analyses were performed using BlueSky Statistics version 10.x.
Results
The study included 140 children treated with zonisamide, comprising 28 with severe obesity, 28 with mild to moderate obesity, 28 who were overweight, and 56 with healthy weight. Of the total cohort, 82 participants (56.6%) were female, 128 (91.4%) identified as non-Hispanic or Latino, and 124 (88.6%) were White (Table 1). The mean age (SD) at zonisamide initiation was 9.60 years (3.93), the median treatment duration was 18 months (IQR 12–24), and the median maximum tolerated zonisamide dose was 6 mg/kg (IQR 3.55–8.30). Valproic acid was discontinued within 6 months prior to initiation of zonisamide in 16 patients. Among these 16 patients, 4 had severe obesity, 6 had mild-to-moderate obesity, 2 were overweight, and 4 had healthy weight.
Baseline Characteristics of Study Cohort
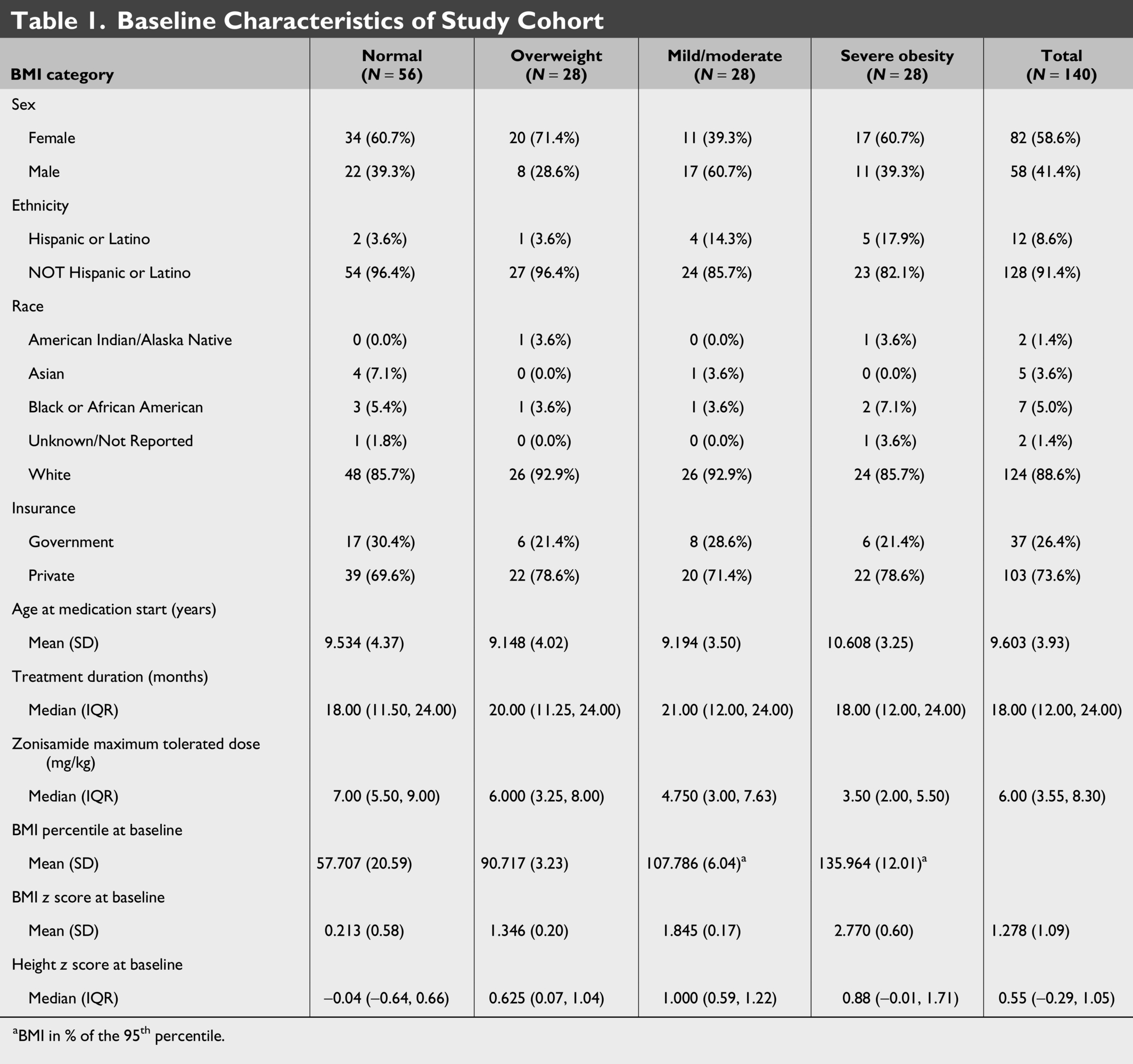
aBMI in % of the 95th percentile.
BMI Changes in BMI Subgroups
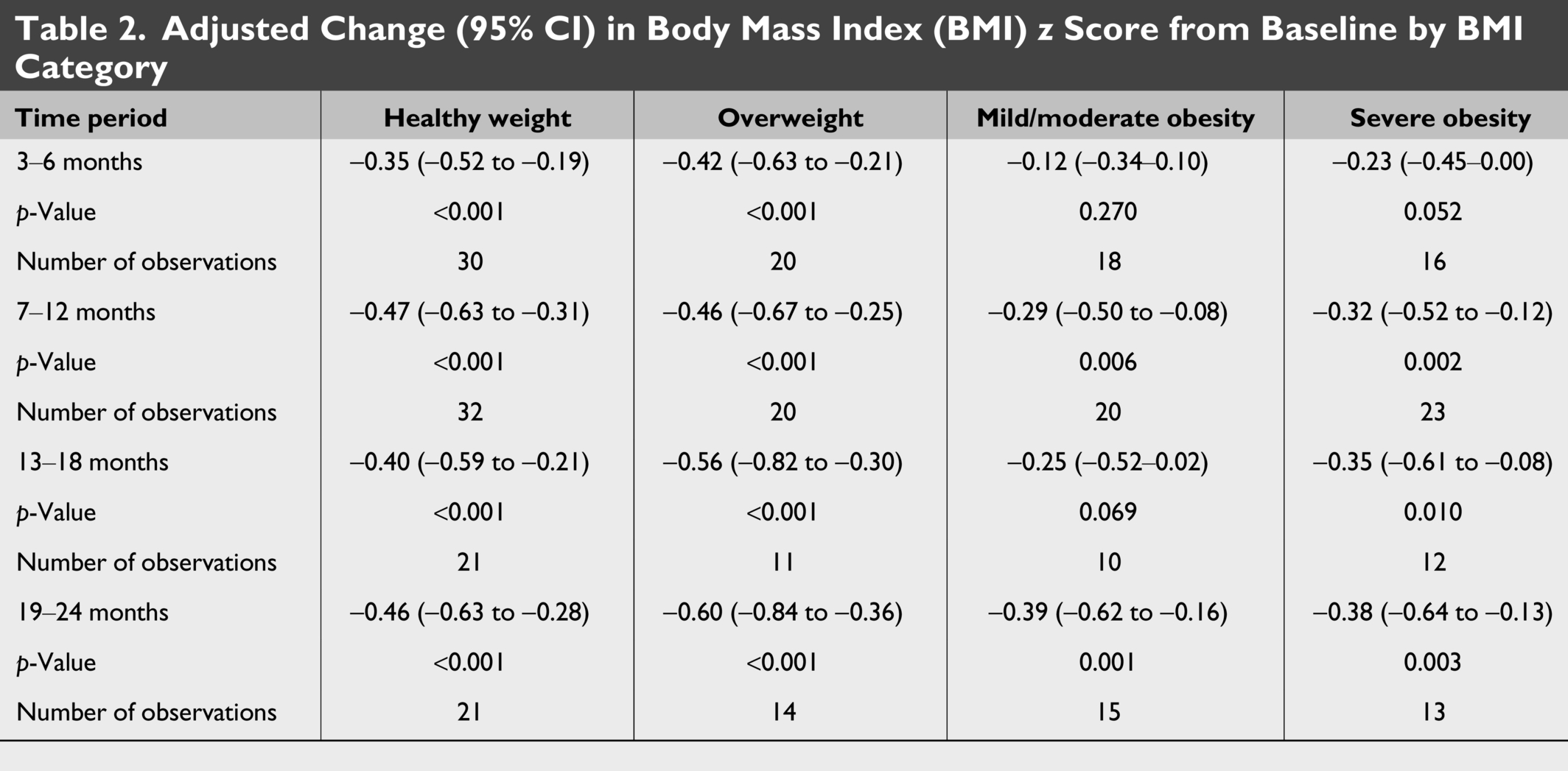
Overall BMI z score of the entire cohort decreased by −0.42 (95% CI: −0.52 to −0.32). A subgroup analysis was performed by stratifying the cohort into four groups according to baseline BMI prior to zonisamide initiation. Among children with healthy weight relative to baseline, BMI z score decreased by 0.46 (95% CI, –0.63 to –0.28; p < 0.001) by 24 months (Table 2, Fig. 1).
Adjusted Change (95% CI) in Body Mass Index (BMI) z Score from Baseline by BMI Category
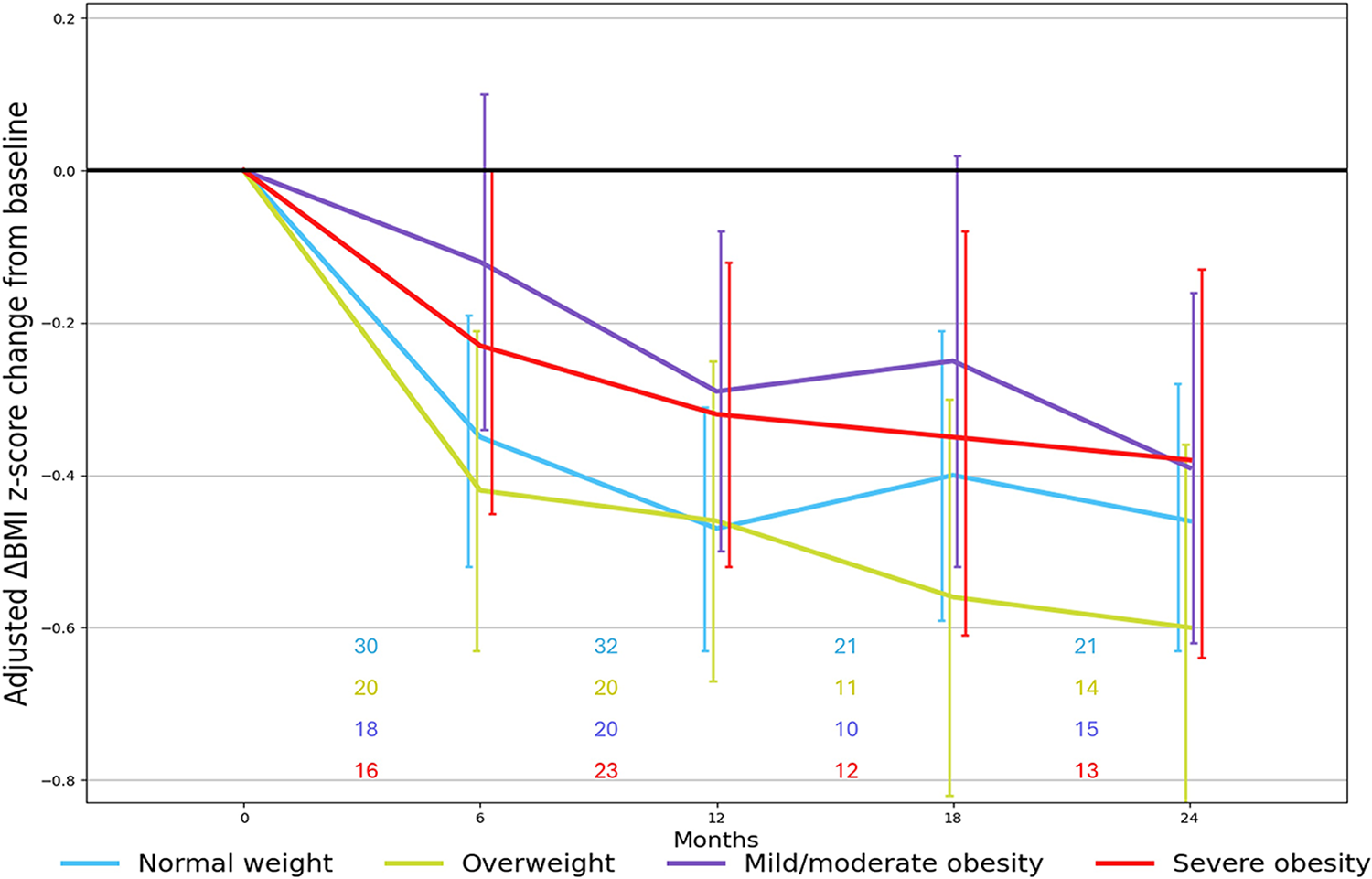
Longitudinal changes in BMI z score during the study observation period stratified by baseline BMI category. The trajectories depict the median change in BMI z score from baseline at each time point based on the number of available observations within each interval. Numbers above the x-axis indicate participants contributing data at each time interval. BMI, body mass index.
In the overweight group, after 24 months of treatment, BMI z score decreased by 0.60 (95% CI, –0.84 to –0.36; p < 0.001) (Table 2, Fig. 1).
Similarly, in the mild to moderate obesity group, decreased by 0.39 (95% CI, –0.62 to –0.16; p = 0.001) at 24 months (Table 2, Fig. 1).
The severe obesity group included 28 children, with a baseline median BMI z score of 2.60 (IQR 2.30–3.07) and a median %BMIp95 of 133 (IQR 127–141). Nineteen children met the criteria for class II obesity and nine for class III obesity. At 24 months of treatment, BMI z score decreased by 0.38 (95% CI, –0.64 to –0.13; p = 0.003), and %BMIp95 decreased by 11 points (95% CI, –24.49 to –3.00; p = 0.011) (Table 2). Overall, 17 of 28 children (60.7%) experienced a reduction of at least 5 points in %BMIp95, and 10 children (36%) no longer met criteria for severe obesity at their final follow-up.
Intergroup analyses did not demonstrate a significant difference in BMI z score changes among the different BMI categories (p = 0.07). Unadjusted data regarding change in BMI z score in the different subgroups are presented in Supplementary Table S1.
BMI Changes in Age Subgroups
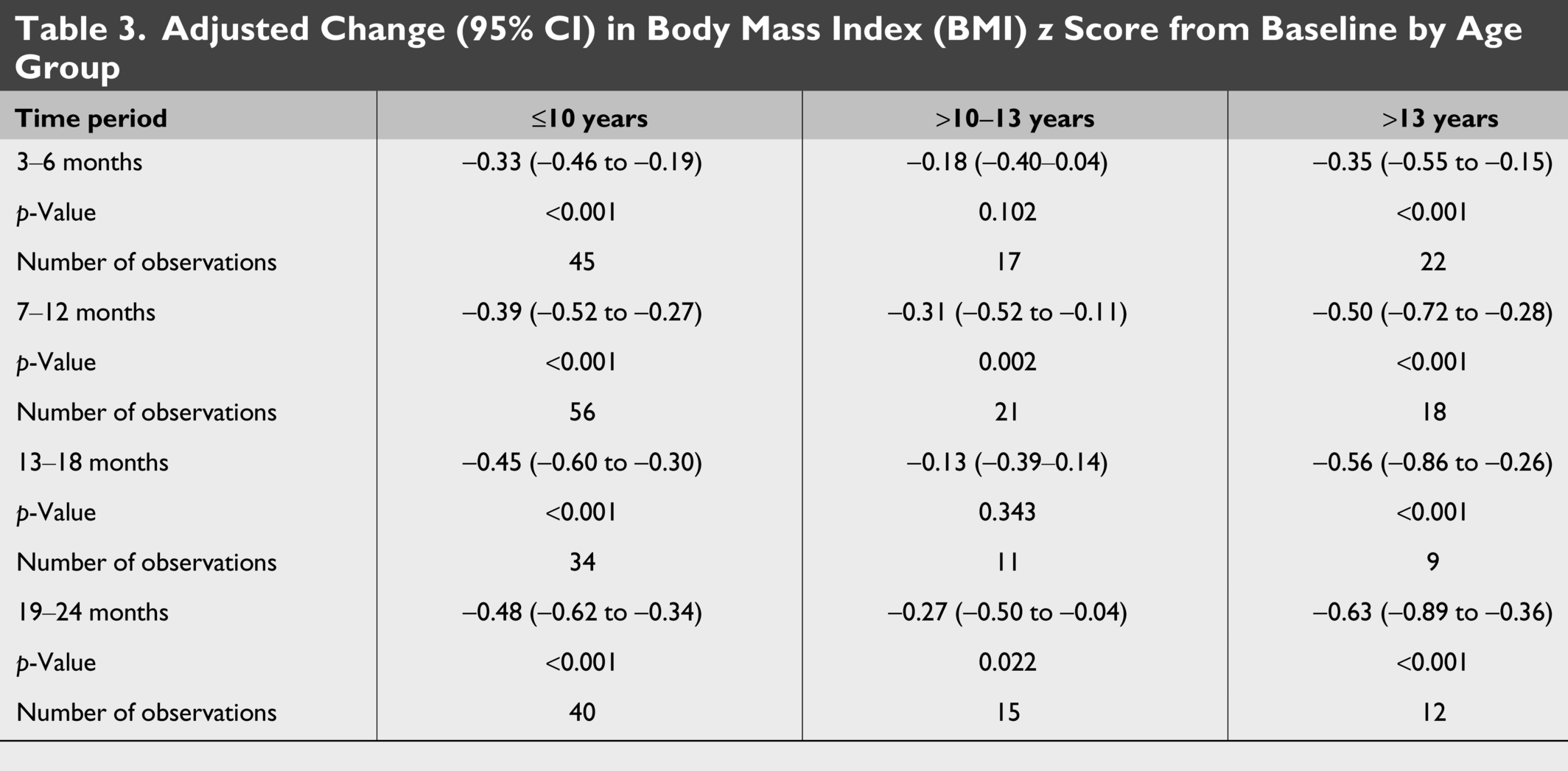
A subgroup analysis stratified patients by age at zonisamide initiation into three groups: ≤10 years (n = 76), >10–13 years (n = 34), and >13 years (n = 30). Among 40 children ≤10 years of age who were treated for 24 months, BMI z score decreased by 0.48 (95% CI, –0.62 to –0.34; p < 0.001) (Table 3, Fig. 2).
Adjusted Change (95% CI) in Body Mass Index (BMI) z Score from Baseline by Age Group
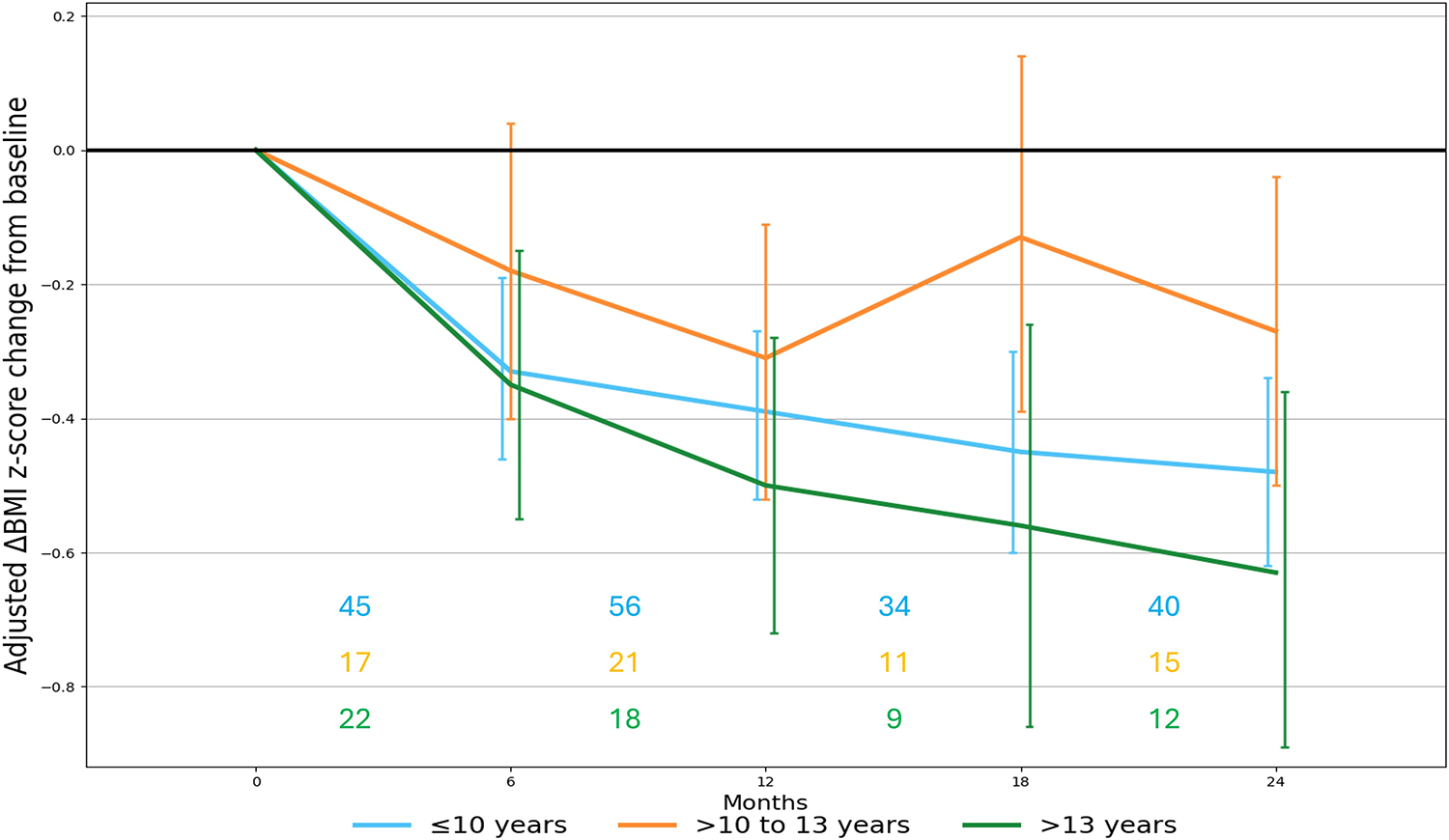
Longitudinal changes in BMI z score during the study observation period stratified by age at zonisamide initiation, with patients grouped as follows: (1) ≤ 10 years, (2) > 10–13 years, and (3) > 13 years. The trajectories illustrate the median change in BMI z score from baseline at each time point, based on the number of available observations within each interval. Numbers above the x-axis indicate participants contributing data at each time interval.
Among 15 children aged >10–13 years, after 24 months of treatment, BMI z score decreased by 0.27 (95% CI, –0.50 to –0.04; p = 0.022) (Table 3, Fig. 2).
In adolescents > 13 years, they had BMI percent change of 5.1%. The 12 adolescents treated for 24 months had a reduction in BMI z score was 0.63 (95% CI, –0.89 to –0.36; p < 0.001) (Table 3, Fig. 2).
Intergroup comparison demonstrated no significant difference in change in BMI z score across the three age groups (p = 0.069).
In the linear mixed-effects model, recent valproate discontinuation was not independently associated with BMI z-score change (p = 0.47). Race (p = 0.62) and ethnicity (p = 0.55) were not significantly associated with BMI z-score change in the adjusted analyses. Unadjusted data regarding the change in BMI z score in the different subgroups are presented in Supplementary Table S2.
Linear Growth Parameters and Reported Side Effects
When comparing height percentile and height z score at the final follow-up with baseline measurements, children demonstrated a small but statistically significant decline in linear growth parameters over the treatment period. The median change in height percentile was –0.15 (95% CI, –4.16 to –0.90; p = 0.002), and the median change in height z score was –0.07 (95% CI, –0.14 to –0.02; p = 0.015).
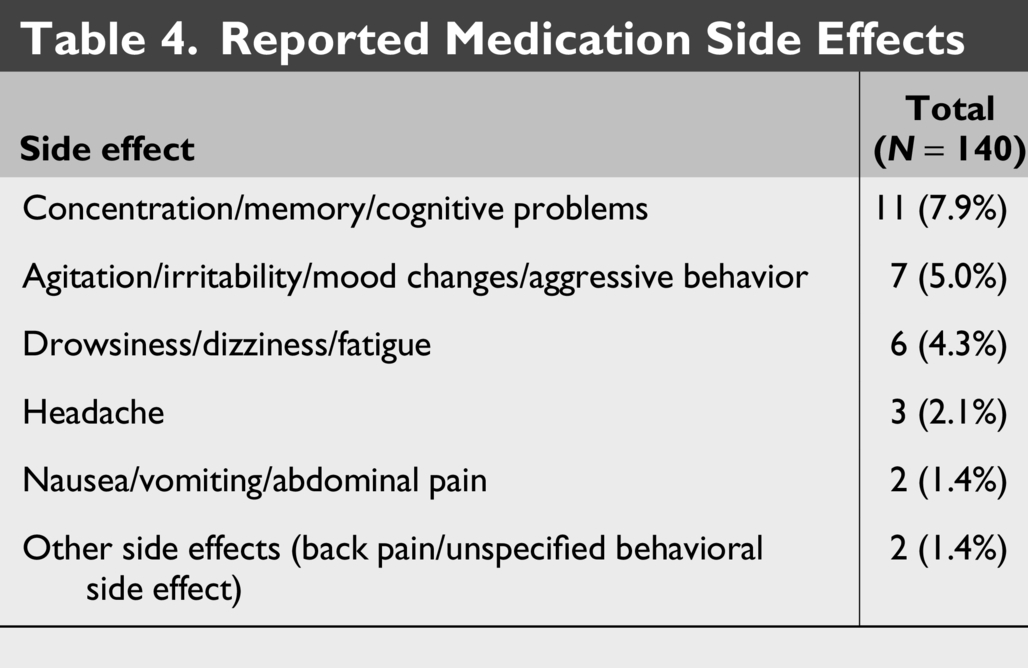
Side effects were reported in 26 (18.6%) patients. The most frequently reported side effects were concentration, memory, or other cognitive difficulties, occurring in 7.9% of the cohort. Agitation, irritability, mood changes, or aggressive behavior were reported in 5.0% of patients (Table 4). Among patients with documented timing of side effects (n = 18), 78% of side effects occurred within the first month of treatment.
Reported Medication Side Effects
Discussion
In this study of children and adolescents with epilepsy treated with zonisamide for up to 2 years, we observed a reduction in BMI across all baseline BMI categories, including healthy weight, overweight, mild-to-moderate obesity, and severe obesity. The weight reduction was sustained throughout the observation period and did not differ significantly between BMI groups. Notably, all age groups demonstrated significant reductions in BMI. To the best of our knowledge, this is the first study to quantitatively characterize the degree of zonisamide-associated weight loss in pediatric patients with epilepsy and elevated BMI and to evaluate the relationship between medication dose, age, and the magnitude of weight change.
In our cohort, we observed a median reduction in BMI z score of 0.38 across the entire study population, with significant decreases noted in all baseline BMI subgroups. Prior pediatric studies evaluating zonisamide have similarly documented weight loss among children with epilepsy.26,33 Lagae et al. reported ≥5% weight loss in a Phase III trial and extension study of 179 children aged 6–18 years who received adjunctive zonisamide for a mean duration of 370 days. 26 Another randomized, double-blind, placebo-controlled trial in children 12 years of age and older and adults reported weight loss of >5 lb in 21.6% of patients treated with zonisamide and 10.4% of those receiving placebo. 33 Unlike our study, these two previous studies in children did not quantify changes in BMI, limiting the precision of weight status assessment, particularly in younger, prepubertal children. Their sample also included fewer participants with elevated BMI (14 with obesity and 16 with overweight) compared with our cohort of 56 children with obesity and 28 with overweight, who were followed for a longer median treatment duration of 18 months and up to 2 years. In a retrospective study of 103 adults with epilepsy treated with zonisamide with a 13-month mean duration of treatment, patients who were overweight at treatment initiation experienced more pronounced weight loss compared with those with lower baseline BMI, which contrasts with our findings as we did not observe differences in the magnitude of BMI change across the various BMI subgroups. 34
The appetite-suppressing effect of zonisamide is thought to result from its modulation of dopaminergic and serotonergic pathways and also carbonic anhydrase–inhibiting properties that collectively contribute to reduced food intake and modest weight loss34–36 (Fig. 3). Owing to these effects, several clinical trials have evaluated zonisamide as a weight-loss therapy in adults with obesity or binge-eating disorder.13–17 In one randomized trial of 30 adults treated with zonisamide versus 30 controls, 57% of participants receiving zonisamide achieved ≥5% weight loss, with significantly greater mean weight reduction (5.9 kg) compared with placebo (0.9 kg; p < 0.001) after 16 weeks at a mean maximum tolerated dose of 427 mg. 13
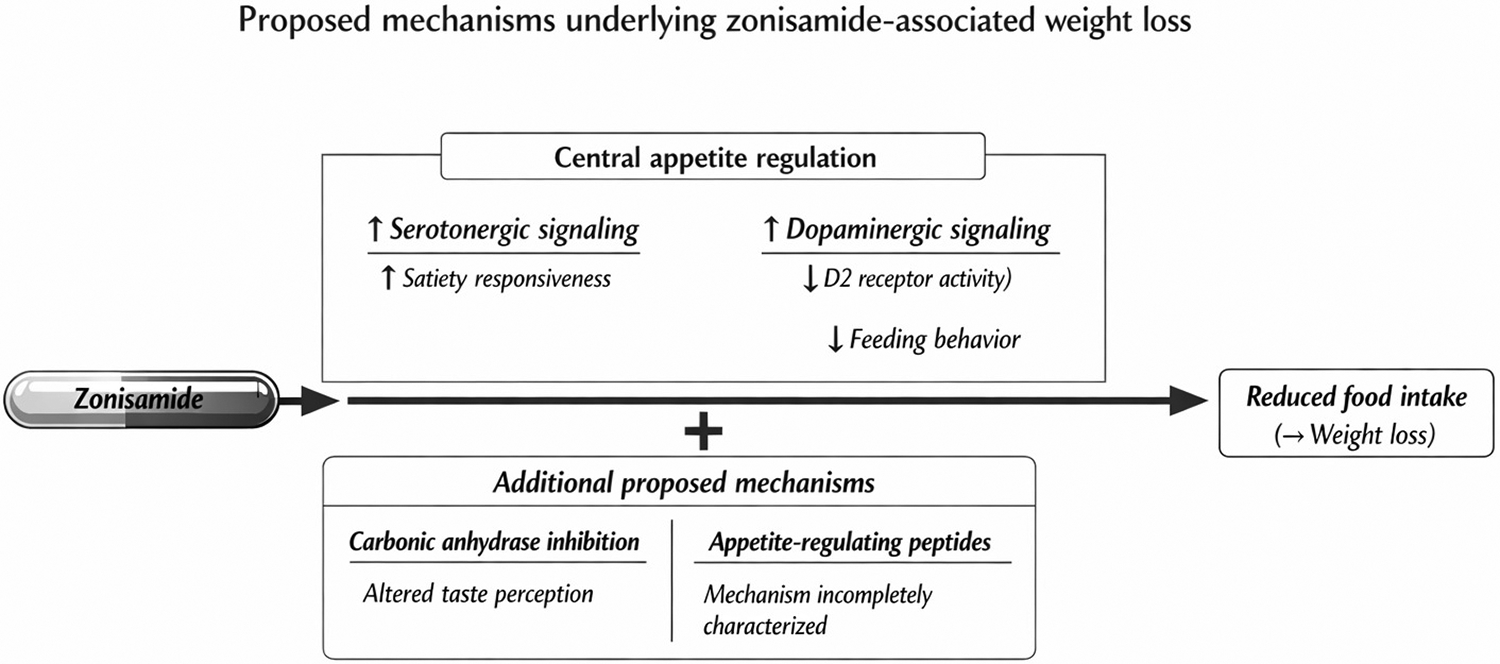
Proposed mechanisms underlying zonisamide-associated weight loss. Zonisamide may contribute to weight loss through central and peripheral mechanisms involved in appetite regulation. Proposed central mechanisms include modulation of serotonergic and dopaminergic signaling, leading to enhanced satiety and reduced feeding behavior, potentially mediated by increased serotonin turnover and dopamine D2 receptor activation. Additional proposed mechanisms include weak carbonic anhydrase inhibition, which may alter taste perception, and possible effects on appetite-regulating peptides that remain incompletely characterized.
In our study, 36% of children with severe obesity at baseline no longer had severe obesity by final follow-up, and 60.7% experienced a reduction of at least 5 points in %BMIp95 and their BMI z score decreased by 11 points after 2 years of treatment. Among children with elevated BMI, a reduction in BMI z score of –0.20 to –0.25 or a decrease of 5 percentage points in %BMIp95 have been associated with clinically meaningful improvements in cardiometabolic risk. 37 ,38 Data on the weight loss effect of zonisamide in children without epilepsy are scarce. 27 Nguyen et al. reported 16.25% reduction in body weight over a 5-month period in a 15-year-old adolescent male with depression and anxiety who was treated with zonisamide 200 mg for weight management. 27
Currently, there are no FDA-approved pharmacologic options for weight management in children younger than 12 years, with the exception of setmelanotide, which is approved for children aged ≥ 2 years with specific forms of monogenic obesity or Bardet–Biedl syndrome. In our cohort, children ≤10 years demonstrated clinically meaningful reductions in BMI with zonisamide therapy, with weight-loss effects comparable to those observed in older adolescents. Further prospective trials are needed to assess the safety and weight loss effect of zonisamide in young children with epilepsy and obesity, a population for whom therapeutic options for weight management are particularly limited.
We did not find any association between weight loss and dose of zonisamide. Zonisamide is typically initiated at 1–2 mg/kg/day with titration by 0.5–1 mg/kg/day every 2 weeks to a maintenance dose of 5–8 mg/kg/day, whereas in patients older than 16 years dosing generally starts at 100 mg/day and is increased by 100 mg every 2 weeks to a total daily dose of 200–600 mg, often divided twice daily. 11 There is no previous data on whether the weight loss effect of zonisamide in children is influenced by the dose of zonisamide. Our findings on lack of a dose response relationship are similar to those of Wellmer et al., in adults but contrast from the findings from another study in adults by Gadde et al. that reported the greatest weight loss in patients receiving a higher zonisamide dose (400 mg) than a 200-mg dose after 12 months of treatment.14,34
In our cohort, zonisamide was generally well tolerated, with adverse effects reported in 18.6% of participants. Cognitive concerns were the most frequently observed (7.9%), followed by mood changes (5%) and dizziness or fatigue (4.3%). In a pooled analysis of 398 children and adolescents receiving zonisamide, the most commonly reported treatment-emergent adverse events included decreased appetite (15.6%), somnolence (12.1%), fatigue (9.3%), dizziness (6.0%), decreased weight (5.8%), irritability (5.8%), and headache (5.3%). 11 We found a small but significant decrease in linear growth in children treated with zonisamide. However, it is not known if the decrease in linear growth noted in our study is clinically meaningful. Further studies are warranted to evaluate the effect of zonisamide on linear growth and puberty in prepubertal and early to mid-pubertal children. Additionally, given the significant reduction in BMI z score observed among children with healthy weight after zonisamide treatment, careful monitoring of weight trajectories is warranted, particularly following initiation of zonisamide therapy, to ensure appropriate growth and avoid unintended excessive weight loss.
Our study has several notable strengths. First, it represents one of the largest pediatric cohorts to date evaluating the weight and BMI effects of zonisamide in pediatric patients with elevated BMI, providing a more comprehensive assessment than prior studies that included smaller number of patients with obesity and did not quantify BMI based outcomes. Additionally, the longer follow up duration, extending up to 2 years, enabled evaluation of the persistence and clinical significance of BMI changes over time. Unlike earlier studies that reported only crude weight change, our use of BMI z scores offered a more developmentally appropriate measure of weight status in growing children. Since the cohort included children and adolescents receiving zonisamide for seizure management, this minimized attrition bias in our study, as continuation of zonisamide was determined by seizure control rather than changes in BMI.
Study limitations include its retrospective design and reliance on electronic medical record data that introduce potential inaccuracies, particularly in recorded height and weight measurements. Anthropometric measurements were reviewed however, and outliers were removed to minimize erroneous entries. Data on hunger, satiety, and lifestyle measures were unavailable. The cohort consisted predominantly of White, non-Hispanic children, which restricts the generalizability of our findings to more diverse populations. Additionally, the study did not evaluate weight trajectories following zonisamide discontinuation, important consideration given evidence in adults demonstrating frequent weight regain after cessation of therapy. 39 Finally, cardiometabolic markers were not available to further assess the potential metabolic benefits associated with zonisamide-induced weight reduction.
Conclusions
Our study demonstrates that zonisamide is associated with clinically meaningful reductions in BMI z score among children and adolescents with epilepsy and elevated BMI, with consistent effects observed across baseline BMI categories and age groups, including younger children. Further prospective studies are needed to assess the weight loss effect and safety of zonisamide as a medication for weight management in children with obesity without epilepsy.
Ethical Consideration
Research authorization status was obtained prior to study enrollment, and the study was approved by the Mayo Clinic Institutional Review Board (IRB Application #: 23-000965).
Footnotes
Data Availability
Original data generated and analyzed during this study and are available upon reasonable request.
Authors’ Contributions
M.S.: Conceptualized and designed the study, collected and curated the data, performed the statistical analyses, interpreted the results, and drafted the manuscript. E.T. and D.H.: Contributed to data collection and critical revision of the manuscript. L.W.-K. and G.K.: Contributed to study design, interpretation of the findings, and critical revision of the manuscript. S.K.: Conceptualized and supervised the study, contributed to study design and interpretation of the findings, and critically revised the manuscript. All authors reviewed and approved the final manuscript and agree to be accountable for all aspects of the work.
Author Disclosure Statement
S.K. is a clinical trial investigator for Rhythm Pharmaceuticals. However, none of the authors have any conflicts pertinent to the current article. All other authors do not have any conflicts of interest pertinent to the article to disclose.
Funding Information
The authors declare that they have no financial interests related to the research presented in this article.