
Abstract
Background:
The Starting Early Program (StEP) promotes healthy nutrition during early life and leads to healthier child weight, but whether dietary patterns contribute to weight or mediate StEP weight outcomes has not been studied.
Objectives:
This secondary analysis identified infant dietary patterns in StEP, determined associations between dietary patterns and child weight outcomes, and examined whether dietary patterns mediated the relationship between StEP and child weight.
Methods:
Data were from 377 mother-infant dyads in a randomized trial testing the efficacy of StEP. Dietary patterns at 10 months were identified using latent class analysis. Child weights were abstracted from medical records at 12, 24, and 36 months. Associations between infant dietary patterns and weight-for-age z-score (WFAz) and likelihood of being classified as overweight (WFA ≥85th percentile) were assessed using linear and logistic multivariable regression models. Mediation was used to assess intervention effects on WFAz via impacts on infant dietary patterns.
Results:
Four classes of infant dietary patterns were identified: Breastfed-High variety, Formula fed-High variety, Formula fed-Low variety, and Mixed fed-Low variety. Compared to the Breastfed-High variety class, infants in the Formula fed-Low variety class had higher WFAz and were more likely to be classified as overweight at 24 and 36 months. Participation in StEP increased membership in Breastfed-High variety, which mediated the association between StEP and lower WFAz at 24 months.
Conclusions:
Infant dietary patterns were identified, and some were associated with child overweight. StEP was associated with a dietary pattern most consistent with guidelines, which mediated intervention effects on child weight.
Introduction
Nearly 13% of children aged 2–5 years in the United States are classified as having obesity. 1 Childhood obesity persists throughout the lifespan and increases risks of poor health outcomes, 2 highlighting the need for early prevention. The time from conception until age 2 years is considered a critical period for the development of obesity when nutrition, lifestyle, and environmental exposures influence later behaviors and health outcomes. 3 Healthy infant feeding practices not only support optimal growth and development 4 but also establish flavor preferences and eating behaviors that are often maintained throughout childhood, 5 making infancy an important period to promote healthy dietary behaviors.
Considerable research has examined how individual feeding practices, including exclusivity, duration, and intensity of milk-based feedings6,7 and adherence to complementary food recommendations,8,9 contribute to child weight. However, studying individual aspects of infant feeding does not sufficiently account for the whole diet and the complex interactions of dietary components. 10 Studies in mostly non-Hispanic White middle- or higher-income populations have identified 9-month infant dietary patterns associated with weight at 12 months and in childhood.11–13 Children from Hispanic and lower-income populations experience the highest rates of obesity, 1 yet there is a lack of research investigating associations between later infant dietary patterns and weight in these populations.
The Starting Early Program (StEP) is a child obesity prevention intervention that supports optimal child feeding and lifestyle behaviors for Hispanic and low-income families. This secondary analysis of StEP aimed to examine associations between 10-month infant dietary patterns and child weight. Since StEP reduces child weight trajectories through 24 months 14 and improves maternal infant feeding knowledge, styles, and practices, 15 we also examined potential impacts of the StEP intervention on dietary patterns and whether these patterns mediated the relationship between StEP and child weight.
Methods
Study Design
Data were from the StEP trial, a randomized controlled trial to test the impact of a primary care-based child obesity prevention intervention beginning during pregnancy on early child weight outcomes in Hispanic families with low incomes (ClinicalTrials.gov Identifier: NCT01541761). 16 Ethics approval was obtained from the Institutional Review Boards of New York University Grossman School of Medicine (10-02175) and the New York City Health + Hospitals (StudyTX00001047). Written informed consent was collected from all participants. A detailed study design of StEP is published elsewhere.14,17
Study Sample
At 28–32 weeks gestation (baseline), participants were recruited from prenatal clinics affiliated with a large hospital system in New York City. Patients with self-reported Hispanic/Latina ethnicity, fluent in English or Spanish, ≥18 years of age with a singleton uncomplicated pregnancy, and planned continuation of pediatric care at the study site were eligible. Participants with a history of severe medical or psychiatric illness or drug/alcohol use disorder, as well as those with fetal abnormalities detected via ultrasound, were excluded.
For this secondary analysis, we identified dietary patterns of participants with a dietary recall at the 10-month assessment. Infants ≥12 months at the assessment were excluded because dietary recommendations change at 12 months. 18 Children with ≥1 recorded weight at 12, 24, or 36 months were included in the analysis of dietary patterns and child weight.
StEP Intervention
Participants were randomly assigned to either standard care or StEP. Standard care received standard prenatal and pediatric primary care. StEP received standard primary care visits plus individual counseling sessions (late pregnancy and infant age 2–3 days) and 13 group nutrition and parenting classes from infant age 1–33 months (5 sessions by infant age 10 months) delivered by dietitians and lactation counselors. 14 Individual sessions reviewed breastfeeding support, and group sessions discussed feeding, activity, and parenting.
Assessments
Infant dietary assessment
24-hour dietary recall
At infant age 10 months, participants completed a 24-hour dietary recall modified to collect information about infant feeding, including detailed information on the type (breast milk versus formula) and mode (breast versus bottle) of milk feeding, consumption of complementary foods, and self-feeding. All feedings in one 24-hour period were recorded in a paper-based format, which was entered into the Automated Self-Administered 24-Hour Dietary Assessment 2014 tool, developed by the National Cancer Institute (NCI, Bethesda, MD). 19 Food Pattern Equivalents Database (FPED) values were generated using a SAS program available from the NCI to estimate intake of food groups. 20
Dietary intake variables
Dietary variables were created following guidelines from the Child and Adult Care Food Program Infant Meal Patterns for 6–11-month-old infants 21 and informed by prior methods.11,13 Using the FPED values, dietary variables were dichotomized to identify daily intake of breast milk, formula, cow’s milk, other dairy (e.g., yogurt and cheese), infant cereals, grains (e.g., rice, pasta, and Cheerios), total vegetables (nonstarchy and starchy), whole fruits, fruit juice, animal proteins (e.g., meat, poultry, fish, and egg), legumes, and empty-calorie foods (e.g., sugary cereals, salty snacks, and French fries). Since the recall did not differentiate between 100% fruit juice and other juice drinks, any juice consumed was included in the juice category.
Breastfeeding or formula feeding intensity
Breastfeeding and formula feeding intensity were estimated as [breast milk feeds OR formula feeds/(breast milk feeds + formula feeds + cow’s milk feeds) * 100]. 22 Infants with breastfeeding or formula feeding intensity ≥80% were considered predominantly breastfed or formula fed, respectively. Infants who were neither predominantly breastfed nor formula fed were considered mixed fed (e.g., 50% of feedings from breast milk and 50% from formula).
Additional dietary variables
Other dietary variables were dichotomized based on meeting or not meeting the recommended daily servings. 21 For cow’s milk, juice, and empty-calorie foods, the recommendation is 0 servings. For infant cereal, other dairy, grains, animal proteins, and legumes, the recommendation is ≥1 serving (>0 tablespoons per serving). For fruits and vegetables, the recommendation is ≥4 servings total (>0 tablespoons per serving), which was split into ≥2 servings of fruits and ≥2 servings of vegetables.
Child weight outcomes
Child weights were obtained from the electronic medical record (EMR) at 12, 24, and 36 months. Sex-specific weight-for-age z-scores (WFAz) at each timepoint were calculated using the World Health Organization Anthro macro. 23 WFA ≥85th percentile was defined as overweight. We used WFA instead of weight-for-length due to identified inaccuracies in EMR-obtained length and height measurements, detailed elsewhere. 14
Covariates
Maternal age, parity, country of birth, and education were collected at baseline. Marital status, employment, household food security, and participation in the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) were completed at 10 months. Maternal anthropometric measurements were from the EMR. Prepregnancy body mass index (BMI, kg/m2) was calculated using measured weight (≤13 weeks gestation) and height or, if unavailable, self-reported values from the baseline assessment. Gestational weight gain (kilogram) was calculated by subtracting prepregnancy weight from delivery weight. Delivery mode, infant sex, and birthweight were from the EMR. Age at introduction of complementary foods and childcare was reported at 10 months.
Statistical analysis
To identify discrete, mutually exclusive latent classes of infant dietary patterns, latent class analysis (LCA) was performed using Mplus version 8.3 (Muthén & Muthén, Los Angeles, CA). StEP and standard care were combined for LCA, which was selected over an index-based approach because the StEP curriculum did not instruct participants to follow a single dietary pattern; rather, StEP targeted key obesity-related, age-appropriate feeding practices. Additionally, families who participated in StEP were culturally diverse, and LCA helps identify differences in food consumption across diverse cultural groups. Latent class models with two through five latent classes were compared. The best fitting model was selected based on Akaike’s Information Criterion (AIC), the Bayesian Information Criterion (BIC), the adjusted Bayesian Information Criterion (ABIC), a parametric bootstrapped likelihood ratio test (BLRT), relative entropy, the number of individuals within each class, and latent class interpretability. 24 After identifying the optimal number of classes, participants were categorized into the class that corresponded to their highest-class membership probability.
Descriptive analyses, regression models, and mediation analyses were performed using Stata Data Analysis and Statistical Software Version 14.2 (StataCorp LLC, College Station, TX). Maternal and infant characteristics were described by latent class membership using one-way analysis of variance (ANOVA) or chi-squared tests. Linear regression models were used to analyze the association between latent class membership and WFAz at 12, 24, and 36 months, and logistic regression models were used to analyze the association between latent class membership and likelihood of being classified as overweight at the same time points. Regression analyses were adjusted for infant sex, birthweight, delivery mode, maternal age, marital status, education, prepregnancy BMI, gestational weight gain, parity, country of birth, household food insecurity, WIC participation, age of introduction of complementary foods, and study group assignment. We ran mediation analyses to determine whether the StEP intervention effects on 12- and 24-month WFAz were mediated through 10-month dietary patterns. Since infant dietary patterns were measured at 10 months and milk feeding remains a significant source of energy for infants through 12 months, we expected that any intervention impacts on infant diet would likely mediate intervention effects on weight beyond 12 months. Therefore, the 24-month mediation analysis was adjusted for 12-month WFAz. We did not test for mediation at 36 months because StEP only impacted WFAz through 24 months.
Results
Of 933 eligible mothers, 566 signed consent, and 533 were randomized. Of those, 399 completed recalls at 10 months. We excluded 22 infants (5.5%) for being ≥12 months at the time of assessment. We included 377 participants (193 control, 184 intervention) in the LCA with weight data available for 331 participants (87.8%; 167 control, 164 intervention) at 12 months, 283 participants (75.1%; 130 control and 153 intervention) at 24 months, and 228 participants (60.5%; 122 control, 106 intervention) at 36 months (Fig. 1).
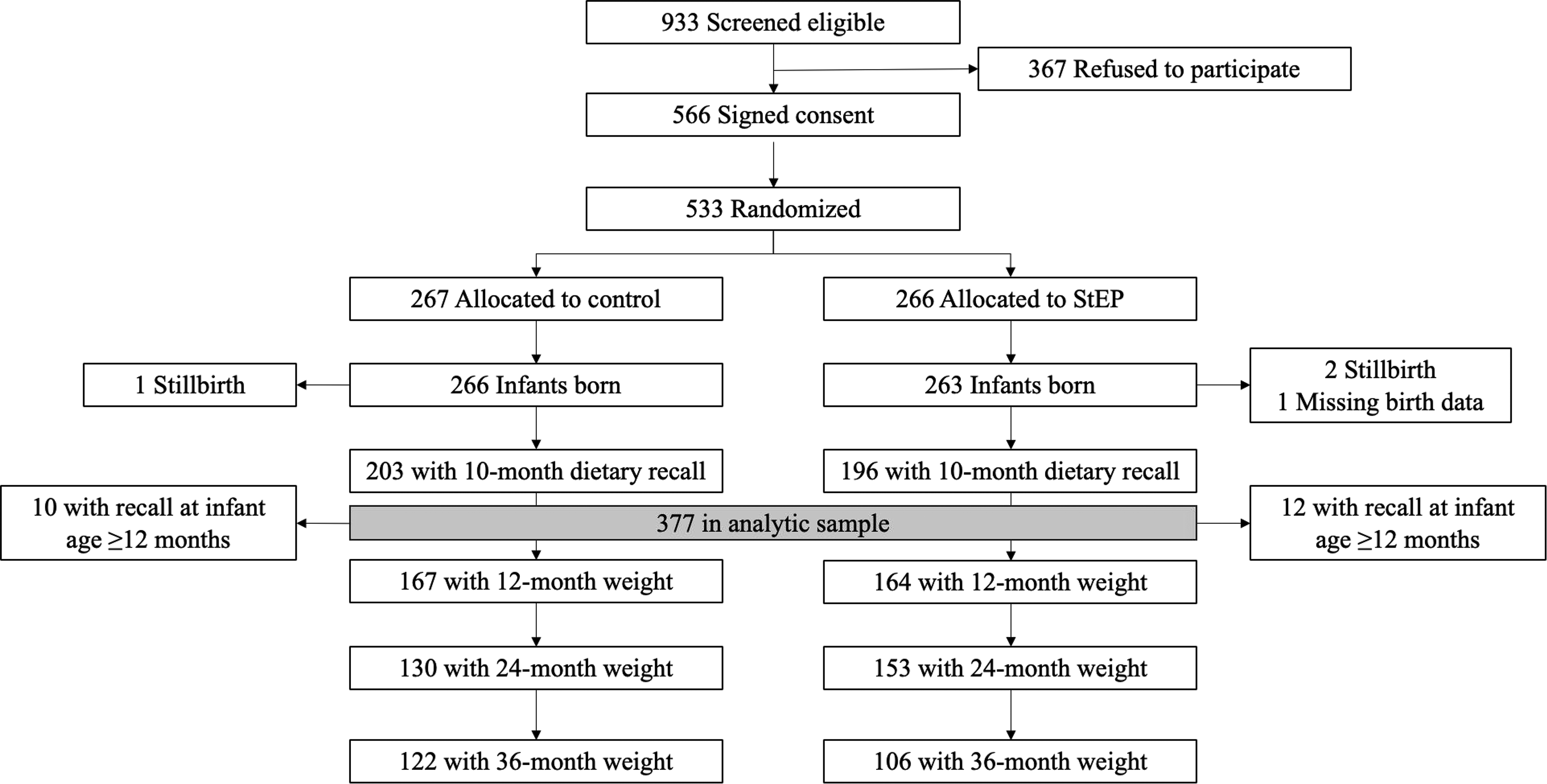
Participant flowchart for StEP: Starting Early Program.
Latent Classes of Infant Dietary Patterns at 10 Months
A four-class solution was determined to be the best fitting model after comparing the fit indices of the latent class profile solutions (Supplementary Table S1) and inspecting latent class interpretability. The model fit indices supported the superiority of both the three-class and four-class over the two-class model, as evidenced by lower AIC, BIC, and ABIC values. Both the three-class and four-class models demonstrated a significant BLRT, indicating better fit compared to models with one fewer class. Although the four-class model did not have the lowest BIC, it was selected as the best-fitting model over the three-class model because all four classes contained >10% of the sample, had significant BLRT results, and exhibited the lowest AIC and ABIC values. Additionally, the four-class model allowed for the identification of distinct classes that captured the variety of complementary foods consumed. A five-class model was also examined but ultimately rejected due to an insignificant BLRT and the presence of a class comprising <5% of the sample.
Figure 2 shows the food group item response probabilities for each of the four latent classes. Latent classes were labeled based on the high probability (≥0.50) of milk feeding mode and variety and developmental appropriateness of nutrient-dense complementary foods (fruits, vegetables, grains, other dairy, animal protein, and legumes) served. The first class, Breastfed-High variety (36.1% sample), was characterized by predominant breastfeeding and high variety of nutrient-dense complementary foods (fruits, grains, and animal proteins). The second class, Formula fed-High variety (25.5%), had a high probability of predominant formula feeding, consuming a high variety of complementary foods (grains, vegetables, fruits, and animal protein), and juice. The third class, Formula fed-Low variety (24.1%), had a high probability of predominant formula feeding and infant cereal. The fourth class, Mixed fed-Low variety (14.3%), had low probabilities of predominant breastfeeding or formula feeding, suggesting mixed feeding, and low variety of complementary foods (grains and animal proteins).
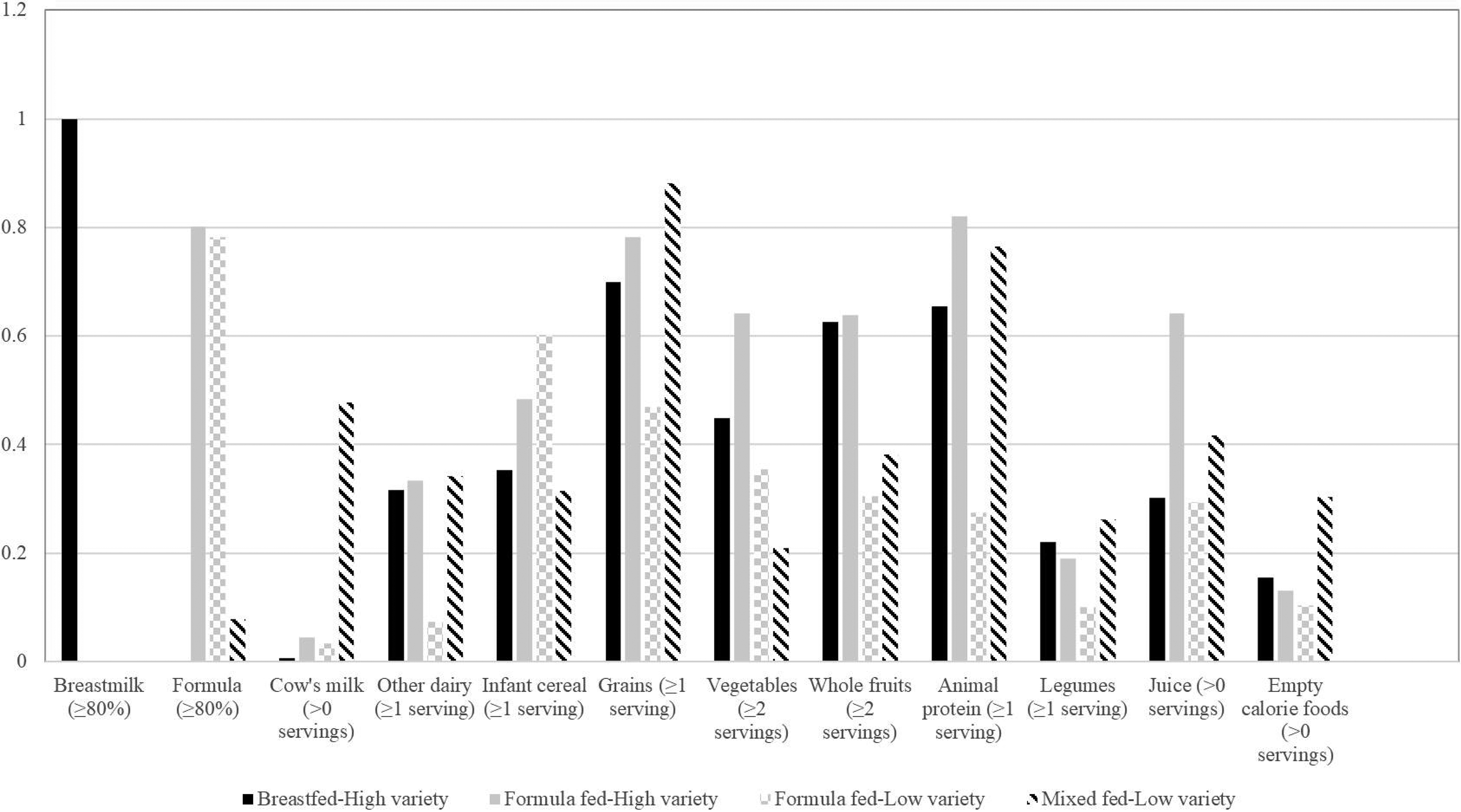
Daily food group item response probabilities for the four latent classes of infant dietary patterns at 10 months in the Starting Early Program Trial (N = 377) Food group items that have a probability ≥0.5 characterize the dietary pattern. Food group item response probabilities closer to one indicated that the infant was more likely to consume that item, whereas probabilities closer to zero suggested that the infant was less likely to consume that item.
Maternal and Infant Characteristics
Table 1 shows maternal and infant characteristics. The Breastfed-High variety pattern had a greater proportion of mothers who were legally married /living as married, born outside the United States, and in the StEP intervention arm and a lower proportion of mothers who were employed or used childcare at 10 months. The Formula fed-High variety and Formula fed-Low variety patterns had a greater proportion of mothers with a high school education or greater.
Maternal and Infant Characteristics by 10-Month Infant Dietary Pattern Class Membership in the Starting Early Program Trial (N = 377) a
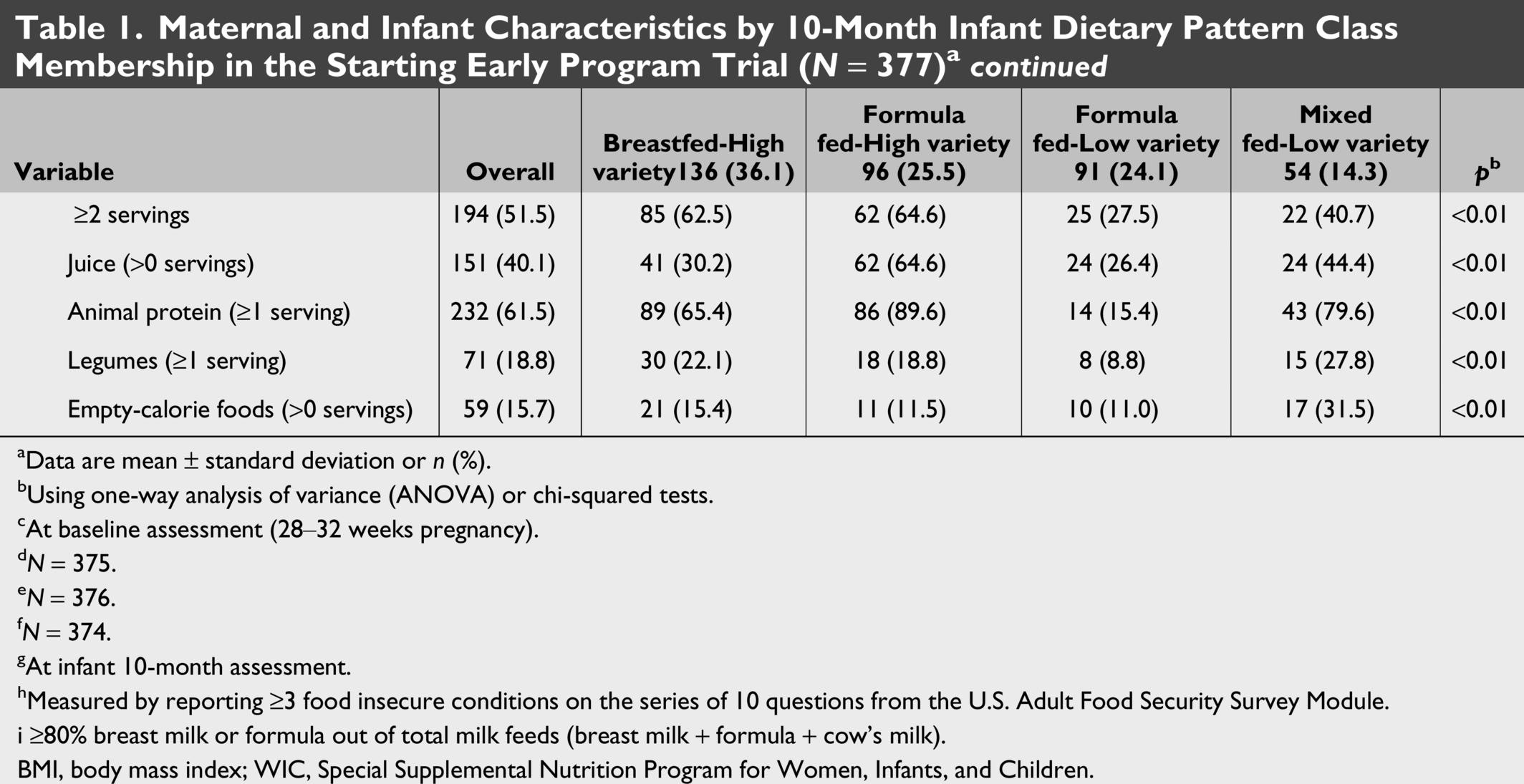
aData are mean ± standard deviation or n (%).
bUsing one-way analysis of variance (ANOVA) or chi-squared tests.
cAt baseline assessment (28–32 weeks pregnancy).
dN = 375.
eN = 376.
fN = 374.
gAt infant 10-month assessment.
hMeasured by reporting ≥3 food insecure conditions on the series of 10 questions from the U.S. Adult Food Security Survey Module.
i ≥80% breast milk or formula out of total milk feeds (breast milk + formula + cow’s milk).
BMI, body mass index; WIC, Special Supplemental Nutrition Program for Women, Infants, and Children.
Dietary Patterns at 10 Months and Child Weight Outcomes at 12, 24, and 36 Months
In adjusted analyses (Table 2), compared to the Breastfed-High variety pattern, infants in the Formula fed-High variety pattern had higher WFAz at 24 months, and infants in the Formula fed-Low variety pattern had higher WFAz at 24 and 36 months and a higher likelihood of being classified as overweight at 24 and 36 months. There was no association between the Mixed fed-Low variety pattern and weight outcomes compared to the Breastfed-High variety pattern.
Linear and Logistic Regression Analyses Assessing the Association Between 10-Month Infant Dietary Class Membership and Weight Outcomes in the Starting Early Program Trial a
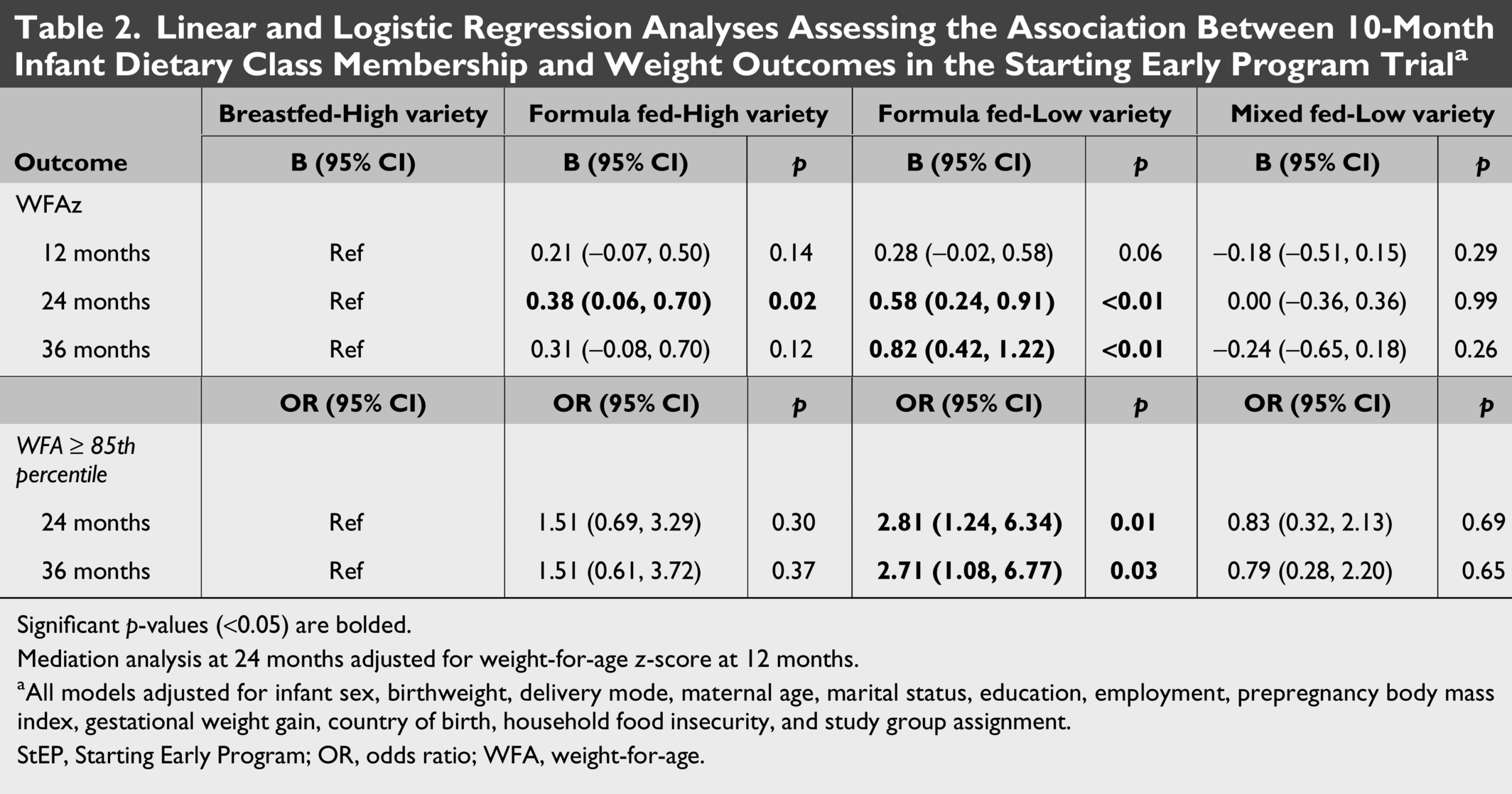
Significant p-values (<0.05) are bolded.
Mediation analysis at 24 months adjusted for weight-for-age z-score at 12 months.
aAll models adjusted for infant sex, birthweight, delivery mode, maternal age, marital status, education, employment, prepregnancy body mass index, gestational weight gain, country of birth, household food insecurity, and study group assignment.
StEP, Starting Early Program; OR, odds ratio; WFA, weight-for-age.
StEP Impacts on Child Weight at 12 and 24 Months as Mediated by Infant Dietary Patterns
When testing the relationship between intervention group and dietary patterns, StEP participants were 2.4 (95% CI: 1.4, 4.1; p = 0.002) times more likely to be in the Breastfed-High variety pattern compared to the Formula Fed-High variety pattern. We found similar trends when comparing membership of StEP participants in the Breastfed-High variety pattern to the Formula Fed-Low variety pattern (OR: 1.5, 95% CI: 0.9, 2.6, p = 0.121) and the Mixed Fed-Low variety pattern (OR: 1.8, 95% CI: 0.9, 3.4, p = 0.074). Since there were no associations between the intervention group and membership in any of the other dietary patterns, we dichotomized the dietary pattern variable for the mediation analysis as membership in the Breastfed-High variety pattern (yes or no). After transforming the variable, we found that StEP participants were 1.9 (95% CI: 1.2, 2.9; p = 0.004) times more likely to be in the Breastfed-High variety pattern compared to not being in this pattern.
Mediation analyses indicated a significant indirect pathway between the StEP intervention and WFAz at 24 months (indirect effect: −0.04, p = 0.049) via intervention impacts on infant dietary patterns (Fig. 3). There was no indirect effect observed for WFAz at 12 months.
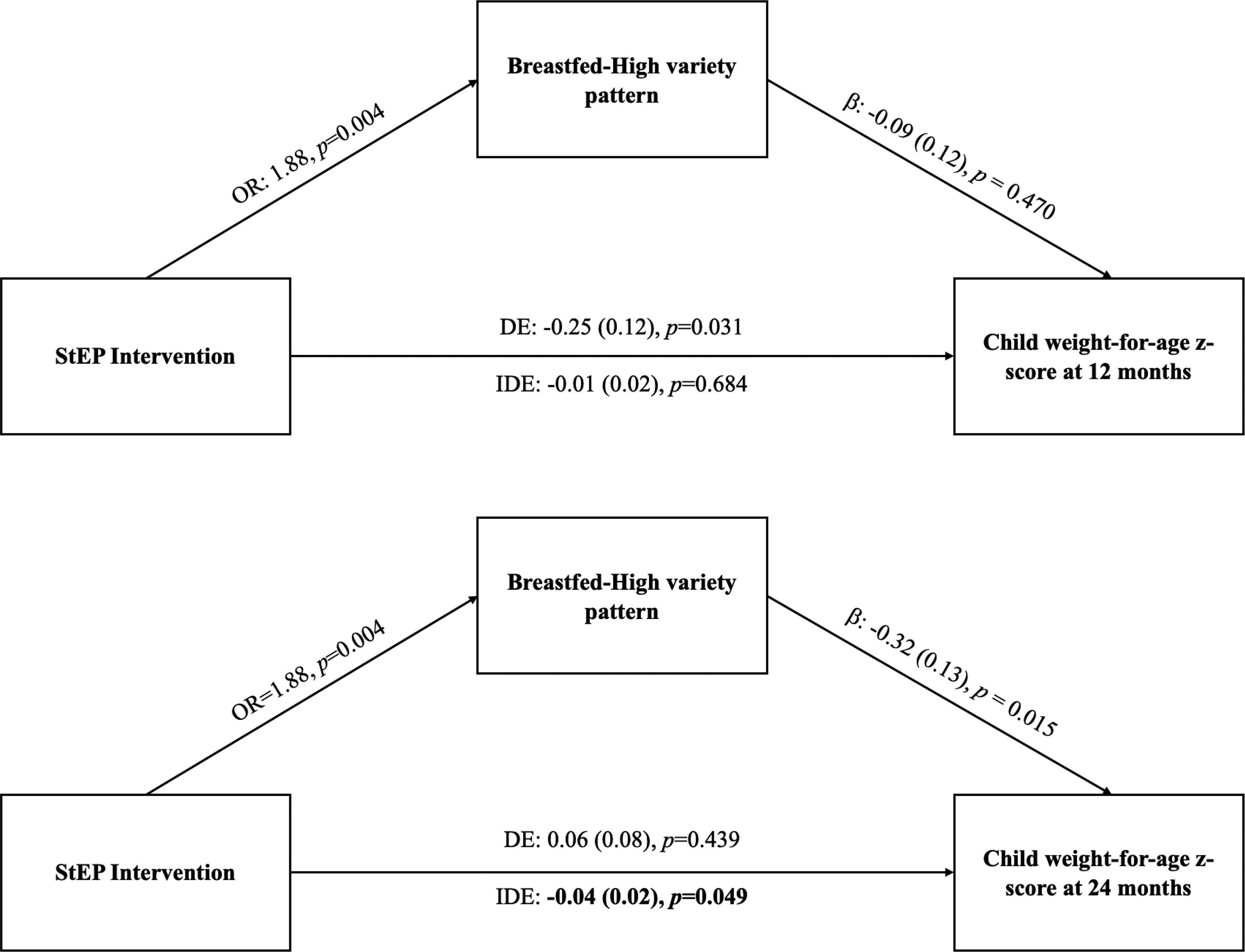
Indirect effects of the Starting Early Program Trial on child weight-for-age z-score at 12 and 24 months through dietary patterns at 10 months. StEP, Starting Early Program; OR, odds ratio; DE, direct effect; IDE, indirect effect.
Discussion
In this secondary analysis of StEP, we identified four infant dietary patterns as follows: (1) Breastfed-High variety, (2) Formula fed-High variety, (3) Formula fed-Low variety, and (4) Mixed fed-Low variety. Compared to the Breastfed-High variety pattern, infants in the Formula fed-High variety pattern had higher WFAz at 24 months, and infants in the Formula fed-Low variety pattern had higher WFAz and greater likelihood of being classified as overweight at 24 and 36 months. StEP participants were more likely to be in the Breastfed-High variety pattern, and participation in StEP was significantly indirectly associated with lower WFAz at 24 months through greater membership in this dietary pattern.
Prior research found that infant dietary patterns characterized by empty-calorie foods, juice, and/or a low variety of complementary foods were associated with increased child weight at 2 and 6 years.12,13 While our study found that dietary patterns characterized by juice and low variety were associated with increased weight, we did not find any associations with the Mixed fed-Low variety pattern. While nearly one-third of infants in this pattern had ≥1 serving of empty-calorie foods, this proportion is lower than what is reported in research that found associations with weight.11–13,25 Additionally, most infants in the Mixed fed-Low variety pattern received some breast milk, which may have a protective effect.26,27 Unmeasured confounding associated with breastfeeding may have occurred; the smaller sample size may have limited detection of significant differences. Infant dietary patterns that are characterized by a low variety of nutrient-dense complementary foods limit exposure to flavors and textures, which may prevent food acceptance later in childhood and lead to unhealthy food preferences.28–30 Continued exposure to these dietary patterns increases risks of nutritional deficiencies and obesogenic eating behaviors,31–33 potentially promoting excess energy intake, weight gain, and adiposity.34,35
Of the dietary patterns identified, the Breastfed-High variety pattern was considered the most consistent with infant feeding guidelines. StEP participants were more likely to follow the Breastfed-High variety dietary pattern, suggesting that StEP fostered adoption of guideline-concordant feeding behaviors. This finding aligns with the StEP curriculum, which promotes breastfeeding, optimal infant feeding practices, and modeling healthy behaviors, as well as prior research on the impacts of StEP on infant feeding behaviors, including greater maternal feeding knowledge and style, increased breastfeeding, and decreased juice. 15 We also documented indirect effects of StEP on WFAz at 24 months, but not 12 months, through intervention impacts on membership in the Breastfed-High variety pattern. Since milk-based feeding is still a significant form of energy in infants through 12 months, we did not expect that dietary patterns at 10 months would be strongly associated with 12-month WFAz. Rather, we conceptualized that infant dietary patterns may influence later child weight by establishing dietary patterns that continue throughout childhood.36,37 StEP may have facilitated continued support to maintain guideline-concordant dietary patterns beyond infancy, but additional research is needed.
Strengths of this analysis include LCA to assess the combination of infant feeding and type and variety of complementary foods in Hispanic and low-income families. Limitations include using a single 24-hour recall to assess infant dietary intake. 38 LCA did not take into account early infant feeding practices, such as breastfeeding and formula feeding duration, intensity, or exclusivity for the first 6 months; time of introduction of complementary foods; or variety of complementary foods beyond what was reported on a single day. Additionally, our study included a culturally diverse sample of Hispanic and low-income families who were from an urban setting, which may not be generalizable to other populations.
In conclusion, this study suggests that dietary patterns that are inconsistent with infant feeding guidelines, particularly a low variety of nutrient-dense complementary foods, are associated with child overweight, which may increase risk of developing future obesity. StEP promoted a dietary pattern that was most consistent with infant feeding guidelines, which mediated the intervention effects on WFAz at 24 months. Given the importance of early prevention, culturally relevant interventions that promote healthy nutrition and lifestyle behaviors in infancy may encourage families to provide a variety of developmentally appropriate and nutrient-dense complementary foods that promote health. More research is warranted to understand how dietary patterns change throughout childhood in Hispanic and low-income populations and determine factors that influence dietary patterns and associations with weight outcomes.
Authors’ Contributions
L.T.B., A.L.D., K.W., M.J.M., and R.S.G. designed the research. L.T.B., M.J.M., and R.S.G. collected and assembled the data. L.T.B. and C.N.K. analyzed the data. All authors interpreted the data and contributed to article writing and critical revision of the article for important intellectual content. All authors have read and approved the final article.
Ethical Considerations
Ethics approval was obtained from the Institutional Review Boards of New York University Grossman School of Medicine (Institutional Review Board number: 10-02175) and New York City Health + Hospitals (System to Track and Approve Research number: StudyTX00001047).
Consent for Publication
Not applicable.
Supplemental Material
sj-docx-1-cdo-10.1177_21532176261465101 — Supplemental material for Infant Dietary Patterns and Early Childhood Weight Outcomes: A Secondary Analysis from the Starting Early Program Trial
Supplemental material, sj-docx-1-cdo-10.1177_21532176261465101 for Infant Dietary Patterns and Early Childhood Weight Outcomes: A Secondary Analysis from the Starting Early Program Trial by Lauren T. Berube, Christina N. Kim, Andrea L. Deierlein, Kathleen Woolf, Mary J. Messito, and Rachel S. Gross
Footnotes
Acknowledgments
The authors would like to thank the StEP staff and study participants.
Consent to Participate
Trained bilingual research assistants obtained written informed consent from all participants.
Data Availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Author Disclosure Statement
We have no competing financial interests to disclose.
Funding Statement
This study was supported by the
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.