
Abstract
Shivering is a common complication of targeted temperature management (TTM), which could undermine its neuroprotective benefits by increasing cerebral oxygen consumption and metabolic demand. Buspirone, a 5-HT1A receptor partial agonist, is incorporated into many antishivering protocols for TTM following cardiac arrest, despite limited evidence supporting its efficacy in critically ill patients. We conducted a targeted literature review using PubMed to assess the evidence in favor of the use of buspirone in antishivering protocols during TTM. Experimental, physiological, and clinical studies were reviewed with emphasis placed on study design, patient population, and relevance to critically ill individuals undergoing TTM. Experimental studies in animals and healthy human volunteers show that buspirone can modestly lower core temperature or shivering thresholds. Two small studies (n = 8 each) in healthy male volunteers demonstrated that buspirone reduced the shivering threshold by approximately 0.7°C. A retrospective cohort study (n = 131) in post-cardiac arrest patients showed a reduction in shivering with a multidrug protocol including buspirone, but the independent contribution of buspirone could not be isolated. No randomized controlled trials have evaluated buspirone’s efficacy as a standalone antishivering agent in critically ill patients. Current evidence to support the buspirone’s use in antishivering protocols is limited and largely extrapolated from noncritical care settings. Given that most patients undergoing TTM already receive sedatives and analgesics with more potent antishivering effects, the incremental benefit of buspirone remains unproven. Furthermore, it adds to the already high burden of polypharmacy in ICU patients and could, in theory, increase the risk of serotonin syndrome. Randomized trials comparing protocols with and without buspirone are needed to determine its clinical utility.
Keywords
Introduction
Targeted temperature management (TTM) is a cornerstone of post-cardiac arrest care (Hirsch et al., 2025; Perman et al., 2023). TTM aims to preserve neurological function and improve outcomes following resuscitation by reducing cerebral energy consumption and metabolic demand (Huynh et al., 2022). Current guidelines recommend maintaining a temperature between 32°C and 37.5°C for at least 36 hours in comatose post-cardiac arrest patients following successful return of spontaneous circulation (Hirsch et al., 2025; Perman et al., 2023). Shivering is a thermoregulatory response triggered by a reduction in core body temperature and occurs in nearly 40% of patients undergoing TTM (Huynh et al., 2022). Shivering counteracts the intended neuroprotective benefits of TTM by increasing metabolic demand, cerebral oxygen consumption, and catecholamine release (Choi et al., 2011; Huynh et al., 2022). Therefore, suppression of shivering is vital for the successful implementation of TTM.
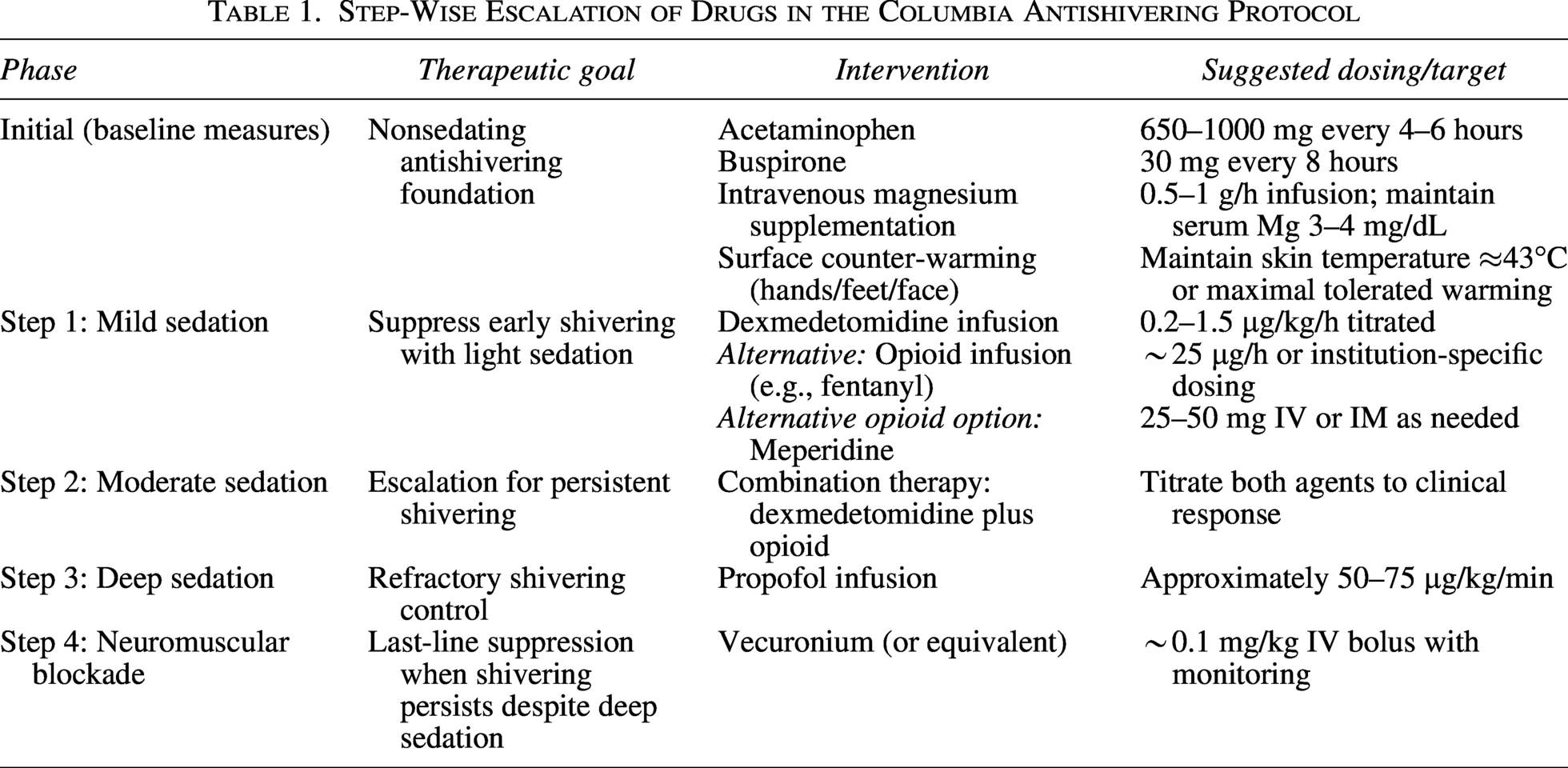
Buspirone is a serotonergic drug that acts as a 5-HT1A receptor partial agonist and has been incorporated into many institutional antishivering protocols. The widely adopted Columbia Anti-Shivering Protocol (Table 1) uses buspirone as a baseline nonsedating medication alongside acetaminophen, magnesium sulfate and skin counter-warming (Choi et al., 2011). However, the evidence supporting buspirone’s use in critically ill patients undergoing TTM is limited and mainly derived from studies in healthy volunteers rather than critically ill patients.
Step-Wise Escalation of Drugs in the Columbia Antishivering Protocol
Recent changes in temperature management guidelines add urgency to the question of buspirone’s continued inclusion in antishivering protocols. In 2021, the TTM2 trial found no added benefit of hypothermia at 33°C compared with normothermia at 37°C, and the American Heart Association (AHA) subsequently revised its recommendations to prioritize fever prevention over deep hypothermia (Hirsch et al., 2025; Nielsen and Friberg, 2023; Perman et al., 2023). The transition to less stringent temperature targets necessitates a thorough reassessment of complete antishivering regimens, particularly regarding the function of buspirone.
This review therefore aims to critically appraise the available experimental data and clinical evidence surrounding buspirone’s role in antishivering protocols during TTM. We assess whether existing data justifies its ongoing inclusion in these protocols and identify knowledge deficiencies that future research should address. While this review focuses mainly on post-cardiac arrest TTM, we must note that these antishivering protocols are frequently extrapolated to other neurocritical care populations requiring temperature control, such as stroke or traumatic brain injury, wherein the risk-benefit profile of buspirone may differ.
Antishivering Protocols in TTM and Their Importance
Temperature control has been recognized to be among the most potent methods of neuroprotection following global ischemia as seen post-cardiac arrest (Delhaye et al., 2012; Huynh et al., 2022). As mentioned earlier, the 2025 AHA guidelines recommend maintaining temperature between 32°C and 37.5°C for at least 36 hours following return of spontaneous circulation in cardiac arrest, with no clear superiority demonstrated for hypothermic versus normothermic targets (Del Rios et al., 2025; Hirsch et al., 2025).
Shivering is a thermoregulatory defense mechanism that is activated when core temperature falls below a critical threshold, typically around 36°C (Huynh et al., 2022). Shivering can significantly increase metabolic demand, elevate cerebral oxygen consumption, and lead to the generation of heat, counteracting cooling efforts and potentially negating the benefits of TTM (Delhaye et al., 2012; Huynh et al., 2022). This, in turn, led to the development of stepwise antishivering protocols.
The Columbia Anti-Shivering Protocol is one of the most widely used protocols that employs a four-step escalation strategy to control shivering. Step 0 includes baseline nonsedating medications including acetaminophen, magnesium sulfate, buspirone and skin counter-warming; steps 1–2 involve mild to moderate sedation with dexmedetomidine and/or opioids; step 3 employs deep sedation with propofol and Step 4 utilizes neuromuscular blockade (NMB) (Choi et al., 2011). The goal is to achieve minimal shivering as defined by a Bedside Shivering Assessment Scale score ≤1, while minimizing the use of sedatives and neuromuscular blocking agents that could obscure neurological examination and lead to complications (Choi et al., 2011). With such protocols however, the relative contribution of individual baseline agents is rather poorly defined. Buspirone is commonly included based on its favorable safety profile and theoretical benefit rather than robust clinical evidence (Choi et al., 2011; Jain et al., 2018). Furthermore, a 2017 systematic quality assessment found that published antishivering protocols lack methodological rigor, with most protocols targeting practice standardization over incorporating systematically reviewed evidence (Choi et al., 2017).
Mechanism of Temperature Lowering and Antishivering Properties of Buspirone
Buspirone is a 5-HT1A receptor partial agonist. It is the only drug of its class currently used in clinical practice, whereas others, such as gepirone and ipsapirone, are either unavailable or not FDA-approved. The temperature related properties of buspirone are exerted via a serotonergic pathway. However, the role of serotonin in thermoregulation is complex, species-dependent, and not clearly understood (Zeisberger and Roth, 1996). Animal studies in the 1980s found that 5-HT1A receptor agonists, particularly 8-hydroxy 2-(di-n-propylamine)-tetralin, decreased body temperature in rodents (Goodwin et al., 1987; Gudelsky et al., 1986). Goodwin and others surmised that this effect was likely mediated via presynaptic 5-HT1A receptors, although the exact mechanism remains controversial (Goodwin et al., 1987). Figure 1 offers visual interpretation of buspirone’s temperature regulating and antishivering properties.
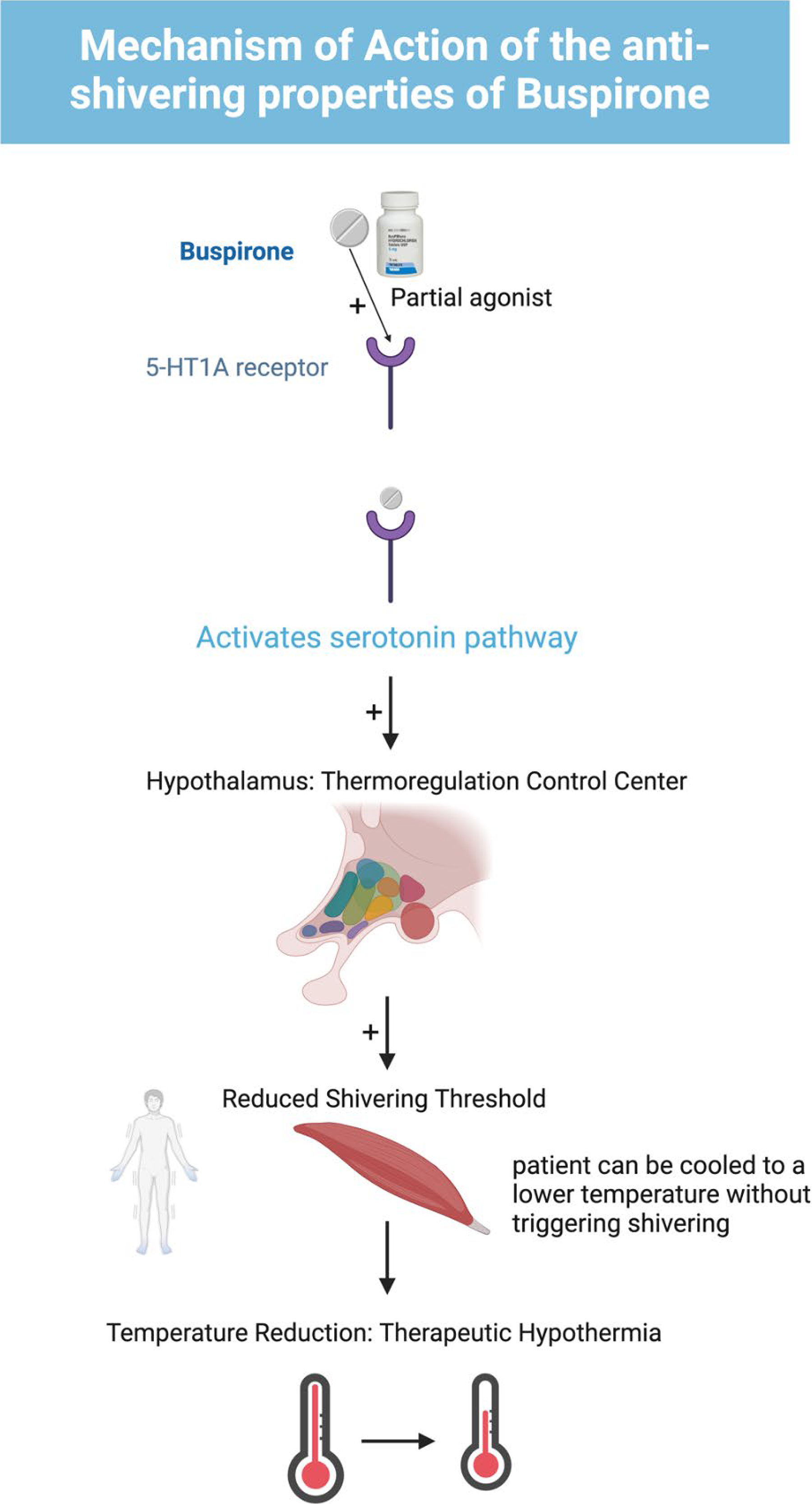
Mechanism of Antishivering Properties of Buspirone.
Human studies found modest hypothermic effects of 5-HT1A agonists. Lesch et al demonstrated that 0.3 mg/kg of ipsapirone significantly reduced core body temperature in healthy volunteers by approximately 0.4°C, but this effect was blunted in patients with active major depressive disorder (Lesch et al., 1990). Young and colleagues found that buspirone 30 mg produced a statistically significant hypothermic response of approximately 0.83°C versus 0.4°C with placebo in eight healthy male volunteers (Young et al., 1993).
Although these trials demonstrate that buspirone can produce hypothermia in healthy subjects, the impact size is minimal (0.4–0.83°C). Importantly, these trials fail to examine buspirone’s efficacy in preventing or mitigating shivering, which is the principal justification for its incorporation into antishivering treatments.
Materials and Methods
A targeted literature review was performed to evaluate the evidence supporting buspirone’s role in antishivering protocols during temperature management. A PubMed search was performed using the MeSH terms: (Buspirone) AND (Targeted Temperature Management), which yielded six results, of which two were relevant to our research question; and (Buspirone) AND (Shivering), which yielded six results, of which four were clinical trials and two were relevant.
We included studies that evaluated buspirone’s effects on shivering threshold or antishivering efficacy in human subjects. We excluded studies not published in English and those not involving human subjects. Given the limited number of studies identified, we also reviewed the references of included articles and relevant review papers to ensure comprehensive coverage. Notably, our search could not identify any randomized controlled trials evaluating buspirone’s role as an antishivering agent in critically ill patients undergoing TTM.
Results
Studies in healthy volunteers
Mokhtarani and colleagues (2001) performed a study on eight healthy male volunteers at the University of California San Francisco to assess whether buspirone and meperidine worked synergistically to reduce the shivering threshold. The volunteers underwent four separate study sessions: no drug, buspirone 60 mg, meperidine 0.4 ug/mL with buspirone 30 mg and meperidine 0.8 μg/mL. Buspirone by itself reduced the shivering threshold by approximately 0.7°C, while meperidine alone reduced it by 2.3°C. When combined at lower doses, the drugs produced a similar shivering threshold reduction to high-dose meperidine alone (approximately 2.3°C). While this could suggest synergistic effects, the authors stated that they could not explain this phenomenon and explicitly acknowledged that even high doses of buspirone resulted in minimal thermoregulatory inhibition compared with meperidine (Mokhtarani et al., 2001).
Lenhardt and colleagues (2009) conducted a similarly designed study to evaluate whether buspirone and dexmedetomidine synergistically reduced the shivering threshold. Eight healthy males underwent four study sessions: no drug, buspirone at 60 mg, dexmedetomidine 0.6 ng/mL, and a combination of both. They found that dexmedetomidine additively, but not synergistically, reduced the shivering threshold. While both the drugs individually produced statistically significant reductions (p < 0.001), buspirone reduced the threshold by only 0.7°C in comparison to dexmedetomidine’s 1.9°C reduction (Lenhardt et al., 2009). The combination of the two reduced the threshold by 2.5°C but did not reach statistical significance (p > 0.05), thereby confirming an additive, rather than a synergistic effect.
Studies in post-cardiac arrest patients
In 2022, Huynh et al. conducted a retrospective cohort study comparing outcomes before and after implementation of a pharmacologic antishivering protocol in 131 patients (51 patients preprotocol and 80 patients post-protocol) undergoing TTM targeting 33°C following cardiac arrest (Huynh et al., 2022). This is the only study in literature examining an antishivering protocol in post-cardiac arrest patients. Acetaminophen, buspirone, and meperidine were baseline medications in this protocol. The post-protocol group showed significantly reduced shivering incidence (57% vs. 39%, p = 0.03), reduced usage of neuromuscular blockade (19% vs. 6%, p = 0.02), and improved survival to discharge (35% vs. 55%, p = 0.02). At the same time, patients in the post-protocol group received significantly more buspirone (4% vs. 73%, p < 0.01), meperidine (8% vs. 34%, p < 0.01), and acetaminophen (12% vs. 65%, p < 0.01) as part of the bundle (Huynh et al., 2022). Since the medications were administered together as part of a protocol, it is impossible to assess buspirone’s independent contribution to the observed benefits. The improved outcomes could be attributed to meperidine, acetaminophen, or the overall approach to shivering management in the protocol rather than to buspirone specifically.
Evidence from reviews and meta-analyses
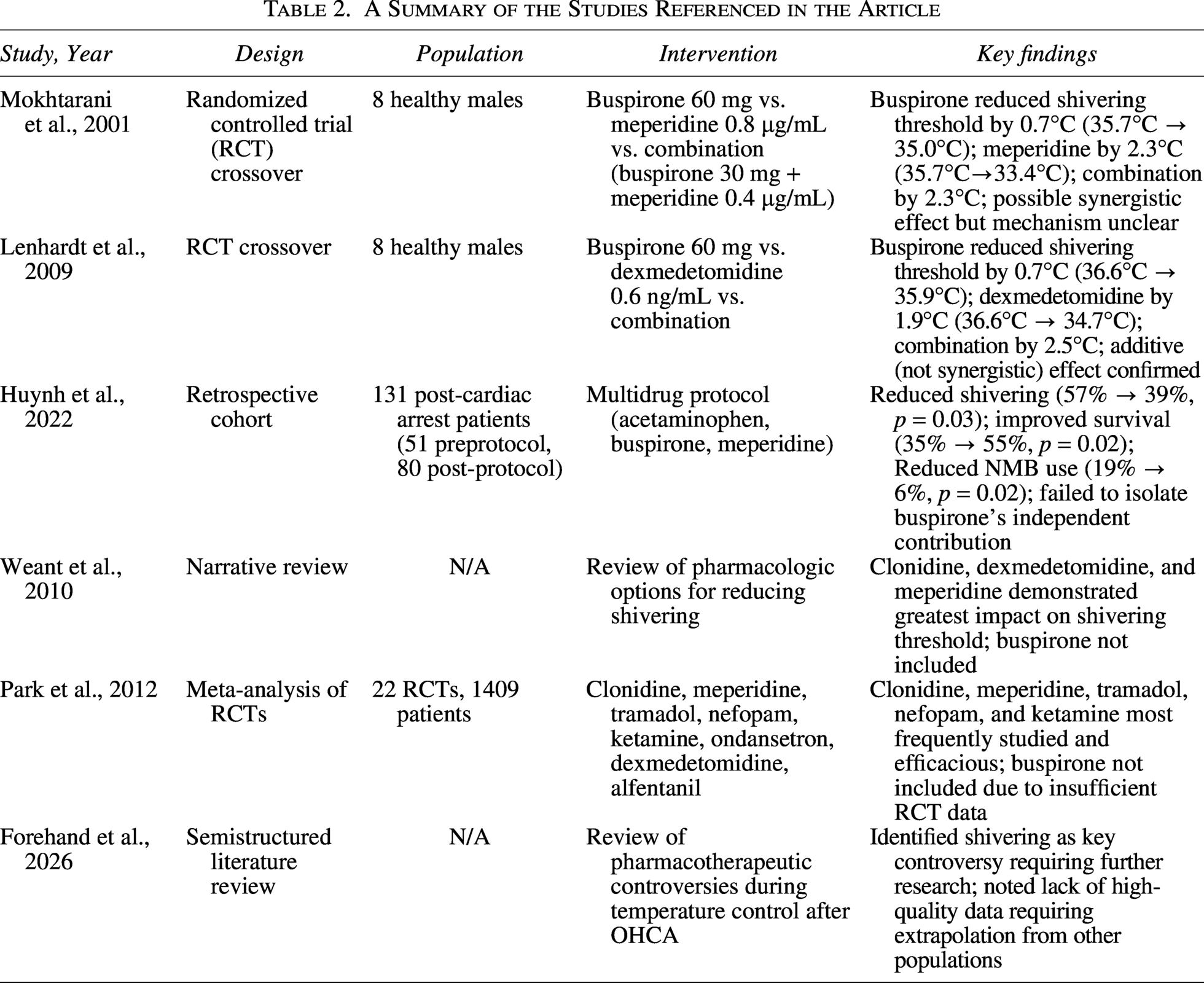
A 2010 narrative review by Weant et al found that clonidine, dexmedetomidine, and meperidine had the most clinically relevant impact on the reduction of the shivering threshold (Weant et al., 2010). Park et al performed a meta-analysis in 2012 examining the efficacy of antishivering medications. They found that clonidine, tramadol, meperidine, nefopam, and ketamine were the most widely studied and efficacious agents (Park et al., 2012). Buspirone was not included among them due to insufficient data from randomized controlled trials. This study did not highlight buspirone in this regard either. Recently a 2025 literature review specifically highlighted shivering control among pharmacotherapeutic controversies during TTM after out-of-hospital cardiac arrest as a key controversy requiring further research (Forehand et al., 2026). It noted that lack of information has led to providers extrapolating data from other patient populations (such as those with acute brain injuries), patient registries or observational studies. An at-a-glance review of referenced studies can be found in Table 2.
A Summary of the Studies Referenced in the Article
Discussion
As mentioned earlier, shivering minimizes the benefits patients obtain from TTM by increasing metabolic demand and increasing cerebral oxygen consumption (Huynh et al., 2022). This has led to the development of antishivering protocols to counteract shivering while also minimizing the use of sedatives and neuromuscular blocking agents. Such protocols (including the widely used Columbia Anti-Shivering Protocol) employ buspirone as a baseline nonsedating medication to control shivering (Choi et al., 2011). However, the fundamental problem here is that the evidence supporting buspirone’s inclusion in these protocols is derived almost exclusively from studies performed in healthy volunteers, not in critically ill post-cardiac arrest patients. The two randomized control trials that attempted to isolate and evaluate buspirone’s anti shivering properties (Mokhtarani et al, 2001 and Lenhardt et al, 2009) involved a sum total of 16 healthy male volunteers. Both studies demonstrated that buspirone reduced the shivering threshold by nearly 0.7°C, which is rather modest in comparison to the 1.9–2.3°C reductions achieved with dexmedetomidine or meperidine (Lenhardt et al., 2009; Mokhtarani et al., 2001). Importantly, these studies were performed in ideal conditions with healthy patients that bear little resemblance to the ICU environment.
Furthermore, the question that needs to be addressed is whether buspirone provides any incremental benefit in shivering control when added to the sedatives and analgesics post-cardiac arrest patients already receive. Post-cardiac arrest patients are typically sedated with propofol or dexmedetomidine while also receiving as-needed opioid analgesia. As shown, dexmedetomidine reduces the shivering threshold by 1.9°C, and the opioid meperidine by 2.3°C (Lenhardt et al., 2009; Mokhtarani et al., 2001). Given that buspirone’s additive effect with dexmedetomidine is only 0.7°C, the clinical significance of this incremental reduction in patients already receiving multiple agents with antishivering properties is questionable. The study by Huynh and colleagues demonstrated improved outcomes with a multidrug antishivering protocol, but in that study, buspirone’s individual role could not be quantified as it was administered alongside acetaminophen and meperidine (Huynh et al., 2022).
The evolving landscape of post-cardiac arrest temperature management also plays into the question of buspirone’s relevance as a nonsedating baseline anti-shivering agent with incremental benefit. The TTM2 trail found no added benefit of hypothermia at 33°C compared with normothermia targeting ≤37.5°C (Hirsch et al., 2025). The guidelines therefore have started prioritizing fever prevention over deep hypothermia. This shift has important implications for antishivering protocols, as shivering typically occurs when core body temperature drops below 36°C (Huynh et al., 2022). If normothermic targets (36–37.5°C) are the new benchmark in temperature management, the need for aggressive pharmacological control of shivering may be substantially reduced. In this setting, the marginal incremental benefit of buspirone becomes even more questionable.
Buspirone as a medication is relatively inexpensive, well-studied, and well-tolerated. However, its routine inclusion in various antishivering protocols contributes to the problem of polypharmacy in an already complex patient population. Each additional medication carries the risk of unwanted drug interactions, administration errors, and increases workload on clinical staff. If buspirone’s benefit is marginal and evidence is limited, its routine use represents an unnecessary addition to the medication regimen. Furthermore, the inclusion of buspirone contributes to the increased serotonergic burden in critically ill patients. Given that ICU patients are often exposed to polypharmacy, including serotonergic agents like tramadol, fentanyl, or home antidepressants, the addition of buspirone carries a theoretical risk that must be weighed against its limited benefit. Finally, buspirone’s inclusion into antishivering protocols is based on weak evidence, often extrapolated from other patient populations, and goes against the philosophy of evidence-based medicine.
Conclusion
No randomized controlled trials have evaluated buspirone’s role as a standalone antishivering agent in critically ill patients. In healthy volunteers, buspirone’s antishivering effect is modest. Prior reviews and meta-analyses have not identified buspirone as an effective antishivering agent either. This should prompt institutions and provider groups to critically evaluate if buspirone provides any meaningful benefit in their antishivering protocols, particularly for intubated post-cardiac arrest patients already receiving sedatives and analgesics with antishivering properties. Moreover, we emphasize that the existing data and protocols discussed in this review are derived exclusively from adult populations, and there is a paucity of evidence currently regarding the efficacy and safety of buspirone for shivering prevention in pediatric TTM. In the face of evolving guidelines recommending fever prevention and normothermia in temperature management following cardiac arrest, the incremental benefit of buspirone’s antishivering properties merits re-examination.
Future research is needed in the form of randomized controlled trials comparing antishivering protocols with and without buspirone in post-cardiac arrest patients. Research should also address if antishivering protocols developed for hypothermic targets (33°C) remain necessary with normothermic targets (36–37.5°C) based on the new guidelines. Until more robust evidence is available, the inclusion of buspirone in antishivering protocols should be considered based on clinical tradition rather than evidence-based practice.
Authors’ Contributions
A.G.: Conceptualization, literature review, article drafting and editing, and final revision. S.B.: Literature review, article drafting, figure and table generation, and critical revision. A.H.: Literature review, article editing, and critical revision. All authors approved the final article. All listed authors meet authorship criteria and have reviewed and approved the final version of the article and agree to its submission to Therapeutic hypothermia and Temperature Management.
Footnotes
Acknowledgments
The authors have no conflicts of interests, financial or otherwise, to disclose. The authors have no funding to disclose for this literature review study. The authors would like to acknowledge the use of the artificial intelligence platform Open Evidence to assist in the structuring and truncation of the introduction and discussion portions of the article, in addition to checking for grammar and spelling. The authors have individually reviewed the article and have approved it for submission to the journal Therapeutic Hypothermia and Temperature Management.
Author Declarations
Compliance with instructions for authors: The authors confirm that this article complies with all instructions for authors of Therapeutic hypothermia and Temperature Management.
Originality Statement
This article is original, has not been published previously, and is not under consideration for publication elsewhere.
Ethics Statement
This article does not involve human subjects research. Institutional Review Board approval and informed consent were not required.
Reporting Guidelines
This article was prepared in accordance with the SANRA (Scale for the Assessment of Narrative Review Articles) reporting recommendations for narrative reviews.
Author Disclosure Statement
The authors declare no conflicts of interest, financial or otherwise.
Funding Information
No external funding was received for this work.