
Abstract
Accurate temperature monitoring is essential for detecting perioperative hypothermia during spinal anesthesia, where rapid redistribution of body heat commonly occurs. Although zero-heat-flux (ZHF) thermometry has emerged as a noninvasive method for estimating core temperature, the reliability of chest skin temperature monitoring in this context remains unclear. In this prospective observational study, temperature measurements were obtained at 5-minute intervals using a forehead ZHF sensor, an infrared tympanic thermometer, and a non-axillary chest skin probe in patients undergoing orthopedic surgery under spinal anesthesia. Agreement between methods was evaluated using Bland—Altman analysis for repeated measurements, the proportion of paired measurements within ±0.5°C, and Lin’s concordance correlation coefficient. Ninety-nine patients completed the study. ZHF and tympanic temperatures showed good agreement, with a mean difference of 0.04 ± 0.35°C, limits of agreement from −0.63°C to 0.72°C, and 89% of paired measurements within ±0.5°C. In contrast, chest skin temperature demonstrated poor agreement with both ZHF and tympanic measurements. The mean difference between ZHF and chest skin temperature was 0.99 ± 1.11°C, with wide limits of agreement (−1.18°C to 3.17°C), and no measurements met the predefined ±0.5°C threshold. Similar discrepancies were observed when chest skin temperature was compared directly with tympanic temperature. These findings indicate that non-axillary chest skin temperature does not reliably reflect core temperature during redistribution hypothermia under spinal anesthesia and should not be used as a surrogate. ZHF thermometry showed substantially better agreement with tympanic temperature and may provide a more reliable noninvasive alternative for perioperative temperature monitoring.
Keywords
Introduction
Perioperative hypothermia remains a common complication during regional anesthesia and is associated with adverse outcomes including coagulopathy, increased blood loss, surgical site infection, delayed recovery, and prolonged hospitalization (Winkler et al., 2000). During spinal anesthesia, patients are particularly vulnerable to a rapid decline in core temperature—often exceeding 0.5°C within the first 30 minutes—driven primarily by internal heat redistribution from the core to the peripheral compartments (Matsukawa et al., 1995). Accurate monitoring of core temperature is therefore essential during spinal anesthesia. However, many established core temperature monitoring techniques, including esophageal and nasopharyngeal probes, are impractical in awake or lightly sedated patients. Consequently, clinicians frequently rely on noninvasive alternatives, including tympanic, skin-surface, and zero-heat-flux (ZHF) thermometry. Although esophageal temperature represents the gold standard for core temperature measurement, it is impractical in awake patients under spinal anesthesia; infrared tympanic temperature was therefore selected as the closest accessible clinical reference in this population. Previous investigations have demonstrated clinically acceptable agreement between infrared tympanic membrane temperature and esophageal temperature in the intraoperative setting. Notably, Poveda and Nascimento (Poveda and Nascimento, 2016) reported a mean difference of 0.03 ± 0.37°C between these two methods, supporting the use of tympanic temperature as a practical surrogate for core temperature in awake patients. Because insertion of esophageal or nasopharyngeal probes would have been poorly tolerated during spinal anesthesia, infrared tympanic thermometry represented the least invasive clinically available reference method in this population.
The physiological behavior of peripheral skin temperature during redistribution hypothermia differs substantially from that of core temperature. Skin temperature is influenced by local perfusion, ambient conditions, patient positioning, surgical draping, and warming interventions. Despite these limitations, chest skin temperature monitoring is commonly used in orthopedic procedures when access to axillary sites is restricted. However, its ability to reflect core thermal status during spinal anesthesia has not been adequately quantified.
ZHF thermometry was developed to provide a noninvasive estimate of core temperature by creating a thermally insulated measurement zone at the skin surface. Previous studies have demonstrated reasonable agreement between ZHF and various core temperature measurements in perioperative settings (Aksu Erdost et al., 2021; Eshraghi et al., 2014; Lauronen et al., 2022), though performance has been shown to vary by surgical context and patient population. Nevertheless, relatively little information is available regarding the comparative performance of ZHF and chest skin temperature monitoring during the rapid redistribution phase that characterizes spinal anesthesia.
The primary objective of this prospective observational study was to determine whether non-axillary chest skin temperature can reliably track core temperature during orthopedic surgery performed under spinal anesthesia. A secondary objective was to compare the performance of chest skin monitoring with that of ZHF thermometry using tympanic temperature as a clinical reference.
Methods
Between July 2019 and June 2022, a total of 116 patients scheduled for orthopedic surgery under spinal anesthesia were prospectively enrolled after providing informed consent. Patients with active infections on the forehead or ear canal or those with changes in anesthesia plans were excluded.
All patients received spinal anesthesia with heavy bupivacaine, targeting blocks from dermatome level T6 to L10. To maintain normal body temperature, a fluid warming system (Barkey S–line fluid warmer (Barkey GmbH, Germany) and upper-body thermal blanket (Bair Hugger Upper Body Convective Warming Blanket, 3M, UK) were employed throughout surgery. Forehead temperatures were measured using a ZHF thermometer (SpotOn, 3M, UK), tympanic membrane readings with an infrared thermometer, and skin temperatures from the chest with a specialized probe (Drägerwerk AG & Co., Germany) at locations not affected by thermal blankets, all at 5-minute intervals during the operation.
The temperature differences were calculated for each pair of measurements. If the observed limits of agreement (±1.96 standard deviation [SD] around the mean difference), within which 95% of the differences were expected to fall, were clinically acceptable, the two methods were considered equivalent. An a priori acceptable clinical limit of ±0.5°C was selected because perioperative decisions regarding hypothermia management are driven by absolute temperature differences rather than correlation coefficients. Accordingly, the proportion of paired measurements within this pre-specified ±0.5°C threshold was designated as the primary metric of clinical agreement, as it directly quantifies the probability of a clinically consequential measurement error at the individual patient level. Lin’s concordance correlation coefficient (LCCC) was used as a complementary descriptive measure; however, because LCCC incorporates both random error and systematic bias, it may not fully reflect the clinical usefulness of measurements when the magnitude and direction of bias are themselves of primary interest. Therefore, LCCC was not used as the sole or primary basis for evaluating agreement. (Winkler et al., 2000). A Bland–Altman plot was generated to illustrate agreement between methods; narrower limits indicate better concordance.
Additionally, the proportion of the ZHF measurements that were within 0.5°C of the corresponding method of reference was calculated, and the 95% confidence interval (CI) for the proportion was estimated using bootstrap percentiles based on 10,000 resamples.
A formal a priori sample size calculation was not performed, as no published data at the time of study design provided Bland–Altman limits of agreement for ZHF versus tympanic temperature specifically in orthopedic spinal anesthesia patients. The target enrolment of 116 patients was determined on a feasibility basis, informed by the magnitude of agreement reported by Eshraghi et al. (Eshraghi et al., 2014) in a related perioperative ZHF validation study, and adjusted for an anticipated 10% dropout rate. Ultimately, 99 patients completed the study protocol. The absence of a formal sample size calculation is acknowledged as a study limitation.
Results
Patient characteristics
A total of 116 patients scheduled for orthopedic surgery under spinal anesthesia were initially screened. Seventeen patients were excluded after opting for general anesthesia or different techniques, leaving 99 patients who completed the study protocol (Fig. 1). The study population had a mean age of 47 ± 11 years and a mean BMI of 25 ± 3 kg/m2. The average surgical duration was 87 ± 31 minutes (Table 1).
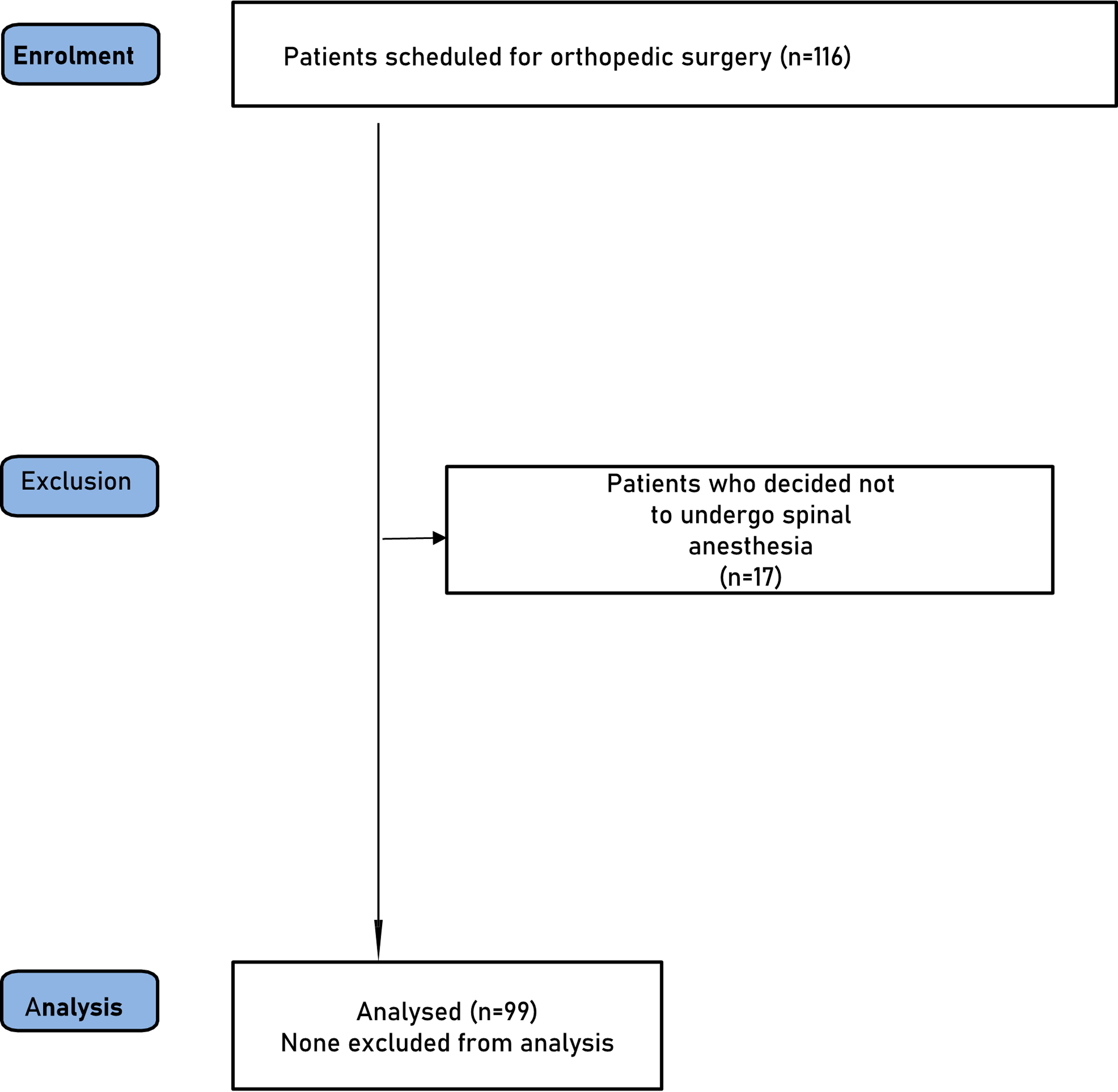
Enrollment Flow Chart.
Demographic and Surgical Characteristics
Temperature trends and mean bias
Throughout the intraoperative period, temperatures measured via ZHF and tympanic (Ttymp) methods remained closely synchronized. The mean intraoperative ZHF temperature was 35.4 ± 0.6°C. In contrast, chest skin temperature (Tskin) consistently lagged behind core readings, failing to converge with either ZHF or Ttymp even after 60 minutes of monitoring (Fig. 2).
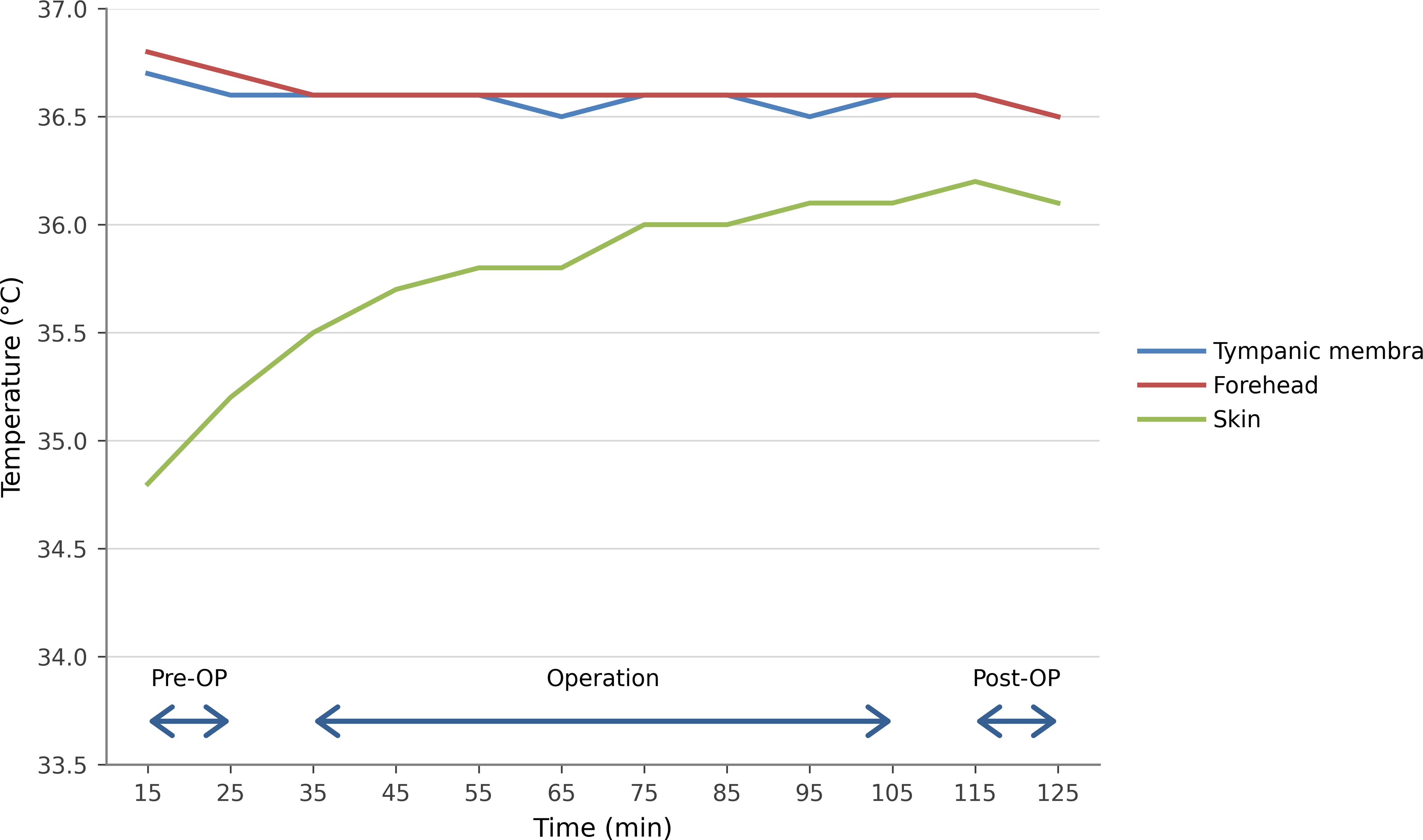
Mean temperatures during surgery.
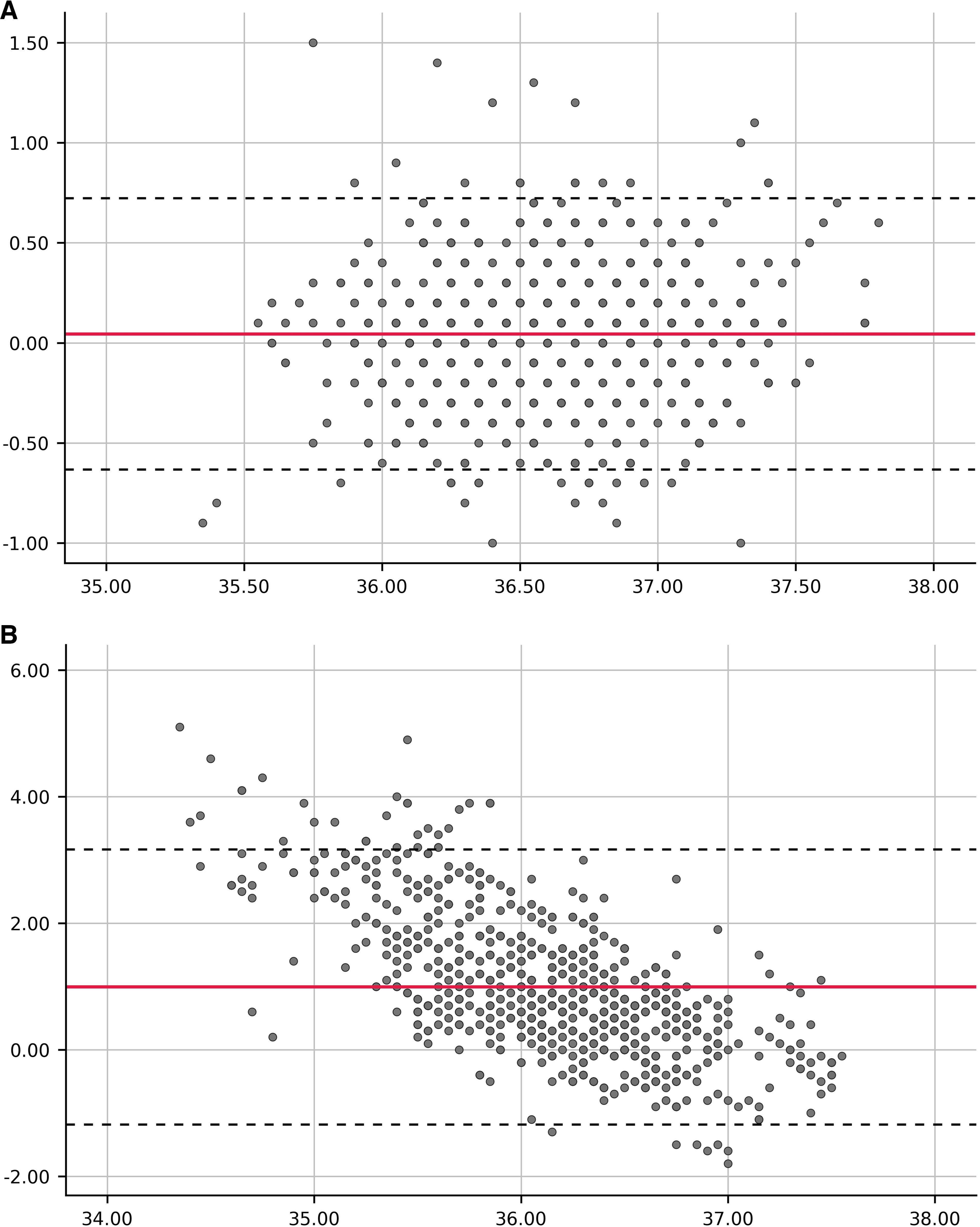
The mean bias between ZHF and Ttymp was minimal at 0.04 ± 0.35°C (95% limits: −0.63 to 0.72°C). However, the discrepancy between ZHF and Tskin was significantly larger, with a mean bias of 0.99 ± 1.11°C and much wider limits of agreement (−1.18 to 3.17°C) (Table 2).
Comparison between ZHF and Reference Methods

ZHF, temperatures were measured at the forehead using a zero-heat fluxs cutaneous sensor; Ttymp, tympanic membrane temperature; Tskin, skin temperature; CI, confidence interval; SD, standard deviation; LCCC, Lin’s concordance correlation coefficient.
Clinical agreement and concordance
Clinical agreement, defined as the proportion of paired measurements within a threshold of ±0.5°C, was high for ZHF vs. Ttymp at 89%. Conversely, Tskin demonstrated 0% clinical agreement with ZHF, as no paired measurements fell within the ±0.5°C range (Table 2). This lack of agreement was further visualized in the Bland–Altman plots, where ZHF vs. Ttymp showed tight clustering around the mean bias (Fig. 3A), while ZHF versus Tskin showed significant dispersion (Fig. 3B).
Bland–Altman plots:
Similarly, the comparison between the two reference methods (Ttymp vs. Tskin) showed a mean bias of 0.95 ± 1.08°C and 0% clinical agreement (Table 3). The discordance between tympanic and skin readings was consistently observed across all time points (Fig. 4). LCCC for ZHF versus Ttymp was 0.69. Because LCCC may be affected by restricted biological variability and systematic bias, these findings were interpreted together with Bland–Altman analysis and the proportion of measurements within clinically acceptable thresholds. LCCC values for comparisons involving Tskin were considerably lower (0.04–0.06) (Tables 2 and 3).
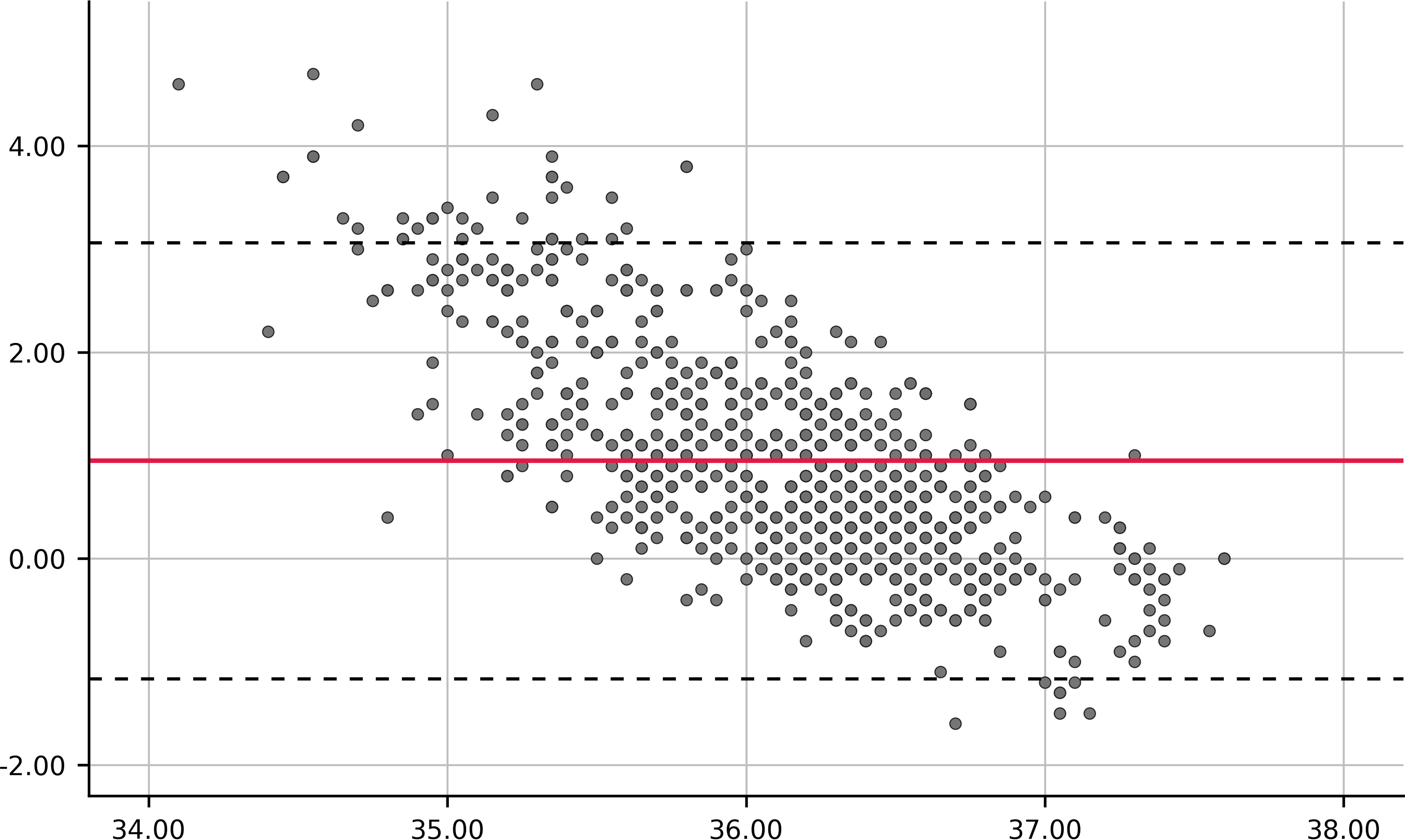
Bland–Altman plot: Ttymp versus Tskin. Limits of agreement (dotted lines) on the plot indicate the range where 95% of the differences between the two methods are expected to fall.
Comparison between Ttymp and Tskin

Ttymp, tympanic membrane temperature; Tskin, skin temperature; CI, confidence interval; LCCC, Lin’s concordance correlation coefficient.
Discussion
The principal finding of this study is that non-axillary chest skin temperature demonstrated poor agreement with both tympanic membrane temperature and ZHF thermometry during orthopedic surgery performed under spinal anesthesia. Across the study period, chest skin measurements consistently underestimated temperatures obtained from both reference methods and exhibited wide limits of agreement. These findings indicate that chest skin temperature does not reliably reflect core thermal status during redistribution hypothermia and should not be considered a surrogate for core temperature monitoring in this setting.
Physiological mechanisms and redistribution
The observed discordance between chest skin and core temperature measurements is physiologically plausible. Redistribution hypothermia following spinal anesthesia results from sympathetic blockade, peripheral vasodilation, and internal transfer of heat from the core to peripheral tissues (Matsukawa et al., 1995; Rajek et al., 2001). During this dynamic period, skin temperature is influenced by local blood flow, environmental exposure, surgical draping, and active warming measures. Consequently, peripheral skin temperatures may change independently of core temperature and may not accurately represent the magnitude or timing of core thermal decline.
ZHF thermometry as a secondary comparator
A secondary finding was that ZHF thermometry demonstrated substantially closer agreement with tympanic temperature than chest skin monitoring. The mean difference between ZHF and tympanic measurements was small (0.04°C), suggesting minimal systematic bias. Although the limits of agreement exceeded the predefined ± 0.5°C criterion, agreement remained markedly superior to that observed with chest skin monitoring. Correlation-based measures such as LCCC are influenced by both population homogeneity and systematic bias and do not necessarily reflect clinical interchangeability. In the present study, the moderate LCCC observed for ZHF versus tympanic temperature likely reflects the restricted biological variability of intraoperative core temperatures in this relatively homogeneous population rather than clinically unacceptable disagreement. By contrast, the very low LCCC values observed for comparisons involving chest skin temperature are consistent with the substantial and clinically meaningful underestimation demonstrated by Bland–Altman analysis. For these reasons, agreement within the pre-specified ±0.5°C threshold was emphasized as the primary clinical metric because it more directly reflects the probability of clinically consequential measurement error. These findings are consistent with previous ZHF evaluations in perioperative settings (Aksu Erdost et al., 2021; Eshraghi et al., 2014; Lauronen et al., 2022) and extend this literature by demonstrating that the relative superiority of ZHF over chest skin monitoring is particularly pronounced during the redistribution phase of spinal anesthesia.
Clinical implications for awake patients
The present findings have practical implications for perioperative temperature monitoring. In many orthopedic procedures performed under regional anesthesia, placement of esophageal or nasopharyngeal probes is impractical, and axillary access may be limited by positioning or surgical draping. Under such circumstances, clinicians may rely on alternative monitoring locations. Because chest skin temperature underestimated core temperature by approximately 1°C on average, clinically significant hypothermia may remain unrecognized when chest skin monitoring is used as the sole temperature-monitoring modality. When noninvasive monitoring is required, ZHF thermometry appears to provide a more informative estimate of temperature trends.
Monitoring considerations in awake patients
For patients undergoing spinal anesthesia, comfort and maintenance of sedation are important considerations. Invasive core monitoring is poorly tolerated by awake or lightly sedated patients. ZHF thermometry provides a noninvasive forehead application with reasonable average accuracy; however, clinicians should remain aware of the individual-level uncertainty margin of approximately ±0.7°C. When ZHF readings approach the hypothermia threshold of 36.0°C, confirmatory tympanic measurement is advisable.
Limitations
Several limitations should be acknowledged. First, tympanic membrane temperature rather than a gold-standard core temperature measurement was used as the clinical reference. Although esophageal temperature is generally considered the preferred reference standard for core temperature measurement, its use is impractical in awake patients undergoing spinal anesthesia, as probe insertion would be poorly tolerated. Previous studies have demonstrated clinically acceptable agreement between infrared tympanic and esophageal temperatures intraoperatively; Poveda and Nascimento reported a mean difference of 0.03°C ± 0.37°C between the two methods, supporting the use of tympanic temperature as a practical surrogate in this setting. Tympanic membrane thermometry therefore represented the least invasive and most clinically appropriate reference method available in this population. Temperature-sensing urinary catheters represent an alternative core temperature reference and may be considered in future studies where catheterization is clinically indicated. (Poveda and Nascimento, 2016). Second, the duration of surgery was relatively short (mean 87 minutes), limiting assessment of monitoring performance during prolonged procedures. Third, this was a single-center observational study, and the findings may not be generalizable to other patient populations or warming protocols. Fourth, the number of patients who completed the study protocol (n = 99) was smaller than the originally targeted enrolment, which should be considered when interpreting the precision of the agreement estimates. Finally, because the study was not designed as a formal equivalence trial, the results should be interpreted as an assessment of monitoring agreement rather than proof of interchangeability among devices.
Conclusion
Non-axillary chest skin temperature does not reliably reflect core temperature during spinal anesthesia for orthopedic surgery and should not be used as a surrogate for core temperature monitoring in this setting. ZHF thermometry demonstrated substantially closer agreement with tympanic temperature than chest skin monitoring. These findings highlight an important gap in current perioperative monitoring practice and support the need for further studies comparing ZHF against gold-standard references in regional anesthesia populations.
Authors’ Contributions
B.S. and S.W.A.: Conceptualization; S.W.A.: Methodology; B.S. and S.W.A.: Formal analysis; B.S., S.O., and L.K.: Investigation; B.S., S.O., and L.K.: Resources; S.O., L.K., and S.W.A.: Data curation; B.S. and S.W.A.: Writing—original draft preparation; S.W.A.: Writing—review and editing; B.S. and S.W.A.: Visualization; S.W.A.: Supervision; S.W.A.: Project administration. All authors have read and agreed to the published version of the article.
Footnotes
Acknowledgments
Dongwook Kim assisted with the statistical analysis for this study.
Ethics Approval and Consent to Participate
This study was approved by the CHA Bundang Medical Center CHA University Hospital Ethics Committee for Research with Medicines (CHAMC–04–043, Gyeonggi–do, Korea) on May 8, 2019.
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent was obtained from all individuals included in the study.
Availability of Data and Materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Author Disclosure Statement
The authors declare that they have no competing interests.
Funding Information
None of the authors have any personal financial interest in this research.