
Abstract
Effective temperature management in critically ill patients with cerebrovascular injuries is vital. A transnasal temperature modulation device (tnTMD) has shown promise in achieving normothermia, but challenges with its dual-nostril configuration limited its efficacy. This study evaluates the efficacy and safety of a single-nostril configuration and identifies the optimal flow rate for effective cooling. This was a prospective, multi-center, open-label study of temperature reduction to achieve normothermia utilizing a tnTMD. Thirty adult patients with ischemic or hemorrhagic stroke, seizure, or metabolic encephalopathy underwent cooling with the tnTMD. Ten patients were treated with the dual-nostril configuration for 8 hours at 60 L/min, and another 10 patients for 24 hours at the same flow rate. Ten patients were treated with the single-nostril configuration for 24 hours at incrementally escalating flow rates (30, 40, and 50 L/min). Core temperature, shivering, and adverse events were reported. The statistical analysis compared reductions in temperature and safety outcomes across flow rates in the single-nostril cohort. The analysis also compares efficacy data from the dual-nostril treatment with those from single-nostril treatments of the tnTMD. A total of 10 patients underwent single-nostril cooling. The 40 L/min flow rate achieved the most consistent normothermia within 4 hours, with reduced temperature burden over 24 hours compared with 30 L/min (p = 0.03). Cooling efficacy at 40 and 50 L/min was similar, but 40 L/min showed lower variance. Shivering occurred in three cases; however, no severe cases of shivering were observed. There were no severe adverse effects. The single-nostril device demonstrated efficacy comparable to that of the dual-nostril approach, with improved practicality. The tnTMD effectively achieved normothermia with a novel single-nostril design with an optimal flow rate of 40 L/min. Given its ease of use and benign safety profile, future research should explore its applicability in non-intubated patients and in longer-duration cooling intervention.
Introduction
Fevers lead to downstream secondary injuries that worsen neurological outcome in a variety of neuropathologies, including ischemic stroke and hemorrhagic stroke (Greer et al, 2008) and seizures, where they introduce an inflammatory response that increases neuronal excitability, glutamate release and lead to a cyclical cascade of recurring seizures (Kammersgaard et al., 2002; Kaur et al., 2022; Reith et al., 1996). Fevers also exacerbate neurological injury in metabolic encephalopathies such as anoxic injury post-cardiac arrest, sepsis, drugs, and respiratory failure (Marois et al., 2019). Refractory fever, a common occurrence in the early acute stages of cerebrovascular disease, is defined as fever despite the management with antipyretics, with consensus guidelines recommending aggressive treatment and maintenance of normothermia as able (Gowda et al., 2018; Greer et al., 2008; Powers et al., 2019; Scaravilli et al., 2011).
Multiple temperature modulating device (TMD) strategies have been trialed to maintain normothermia and are often impeded by shivering, reducing their efficacy (Badjatia et al., 2004, 2007, 2008; Choi et al., 2011; De Witte and Sessler, 2002; Hata et al., 2008; Lord et al., 2014; Lyden et al., 2016; Oddo et al., 2010; Presciutti et al., 2012). Shivering increases metabolic demand, hindering cooling effects, while anti-shivering therapies incur additional costs and deterioration of neurological status (Badjatia et al., 2007,2008; Choi et al., 2011; Greer et al., 2008; Hata et al., 2008; Khan et al., 2018; Madden et al., 2017).
The efficacy and safety of a transnasal (tn) high-flow dry air evaporative cooling device (via the CoolStat transnasal TMD) in the induction and maintenance of normothermia in patients who suffered from ischemic and hemorrhagic cerebrovascular injury have been previously reported (Arnold et al., 2023; Badjatia et al., 2021). As noted in the previous study, tn cooling was more effective than surface cooling in preventing shivering, with fewer incidences of shivering and use of anti-shivering medications (Badjatia et al., 2021). While the majority of patients achieved and maintained normothermia in previous studies, increased back pressure limited dual-nostril delivery of therapy and may have affected the overall efficacy of the tn approach. This study hypothesized that single-nostril delivery of high-flow dry air would be equally effective at achieving the targeted temperature while avoiding the challenges of elevated backpressures associated with the previously reported dual-nostril mask configuration. Additionally, the study aimed to identify the flow rate (liters/minute) associated with the most effective cooling rate. This was accomplished by analyzing data across three prospective studies, including previously reported data utilizing the double-nostril configuration, and comparing it to single-nostril configuration data.
Methods
Patient selection
Patients selected for this analysis were from three cohorts of a prospective, multi-center, open-label clinical trial evaluating the safety and efficacy of the CoolStat tnTMD using either a dual-nostril or a modified single-nostril mask in critically ill, febrile, ventilated patients (endotracheal tube or tracheostomy). Inclusion criteria for patients enrolled using the dual nostril device have previously been published (Arnold et al., 2023; Badjatia et al., 2021). Patients selected for the study were admitted with a diagnosis of intracerebral hemorrhage, acute ischemic stroke, subarachnoid hemorrhage, or seizures and met additional inclusion/exclusion criteria (Table 1). Informed consent was obtained from authorized legal representatives, as all patients included in the study were unable to provide consent due to the nature of their illness and endotracheal intubation. The study was approved by the site’s institutional review board and by the Food and Drug Administration through an investigational device exemption. Funding for this study was granted by the Maryland Industry Partnerships program.
Study Criteria
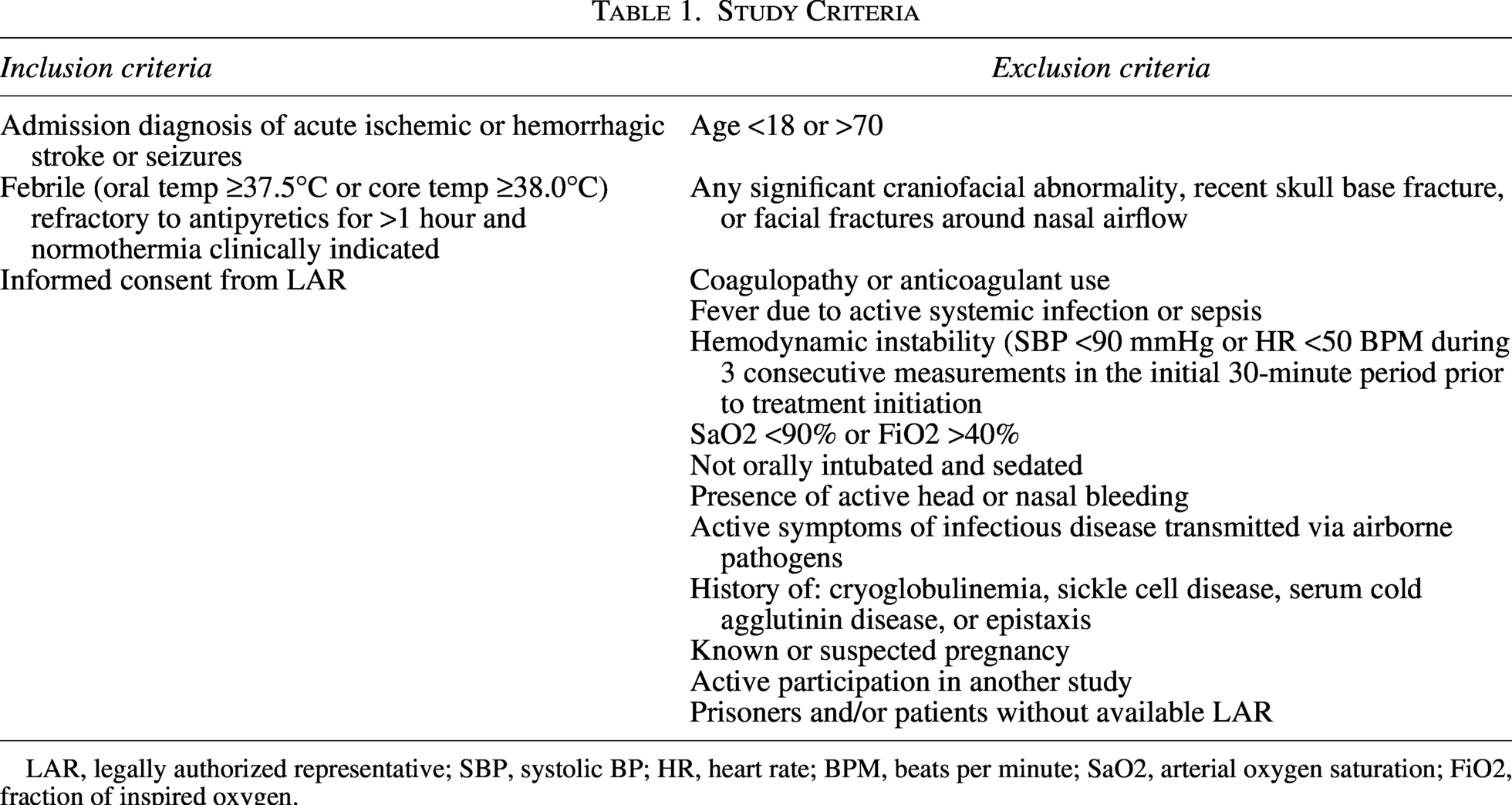
LAR, legally authorized representative; SBP, systolic BP; HR, heart rate; BPM, beats per minute; SaO2, arterial oxygen saturation; FiO2, fraction of inspired oxygen.
Data collection
Clinical data collection included continuous core temperature measured via a bladder probe, an esophageal catheter, or a superficial temporal temperature sensor (3M™ SpotOn™ system). A study by Wagner et al. (2021) showed good agreement with superficial temporal temperature sensors and core temperature measures. In addition, blood pressure and the presence of shivering were monitored throughout the cooling period. Safety was assessed as the severity and frequency of adverse events (SAEs) and unanticipated adverse events (UADEs) with an additional focus on a priori defined thresholds for systolic blood pressure, temperature (core and tympanic), and shivering using the Bedside Shivering Assessment Scale (BSAS). Safety oversight was conducted by an independent data and safety monitoring board at predetermined intervals.
CoolStat device
The CoolStat tnTMD regulates core temperature via a closed-loop system that adjusts airflow rates based on the patient’s core temperature, continuously fed to the device by the subject’s core temperature monitoring device. The CoolStat tnTMD device uses a predetermined algorithm to automatically adjust airflow to achieve temperatures at or above the lower temperature threshold of 36.5°C. Further details on the mechanism of evaporative cooling using the CoolStat tnTMD have been previously published (Lord et al., 2014).
The previously described CoolStat dual-nostril airflow device was found to be an effective method for achieving and maintaining normothermia (Arnold et al., 2023; Badjatia et al., 2021). Still, it had an incidence of high back pressures, resulting in reduced target airflow. The single nostril tnTMD was implemented to address high backpressures and their impact on airflow to achieve and maintain normothermia. In the single-nostril configuration of the CoolStat tnTMD, evaporative cooling is achieved by delivery of dry ambient air to one nostril that unidirectionally flows over the nasal turbinates before flowing out through the opposite nostril and mouth. The dry air delivered by the CoolStat device flows over the highly vascularized, mucous-filled membranes of the nasal turbinates, inducing a change in mucous from liquid to gas using energy produced from the turbinates’ membrane tissue.
Ten subjects were cooled with the modified CoolStat single-nostril mask to evaluate its safety and efficacy using a dose-escalation model (Fig. 1). The dual-nostril airflow rate of 60 liters per minute (L/min) was divided equally between the two nostrils in the prior study. The initial flow rate in the single-nostril study was set at 30 L/min to demonstrate the safety of this flow rate through one nostril. The first three subjects were cooled at a flow rate of 30 L/min. The flow rate was increased after assessing the SAEs and UADEs of the prior set of patients. The following three subjects were cooled at 40 L/min, and the final four at 50 L/min. The selected rates represented maximum flow rates, but allowed for adjustment based on core temperature feedback. As done in previous studies, antipyretic treatment was continued upon initiation of the CoolStat tnTMD.
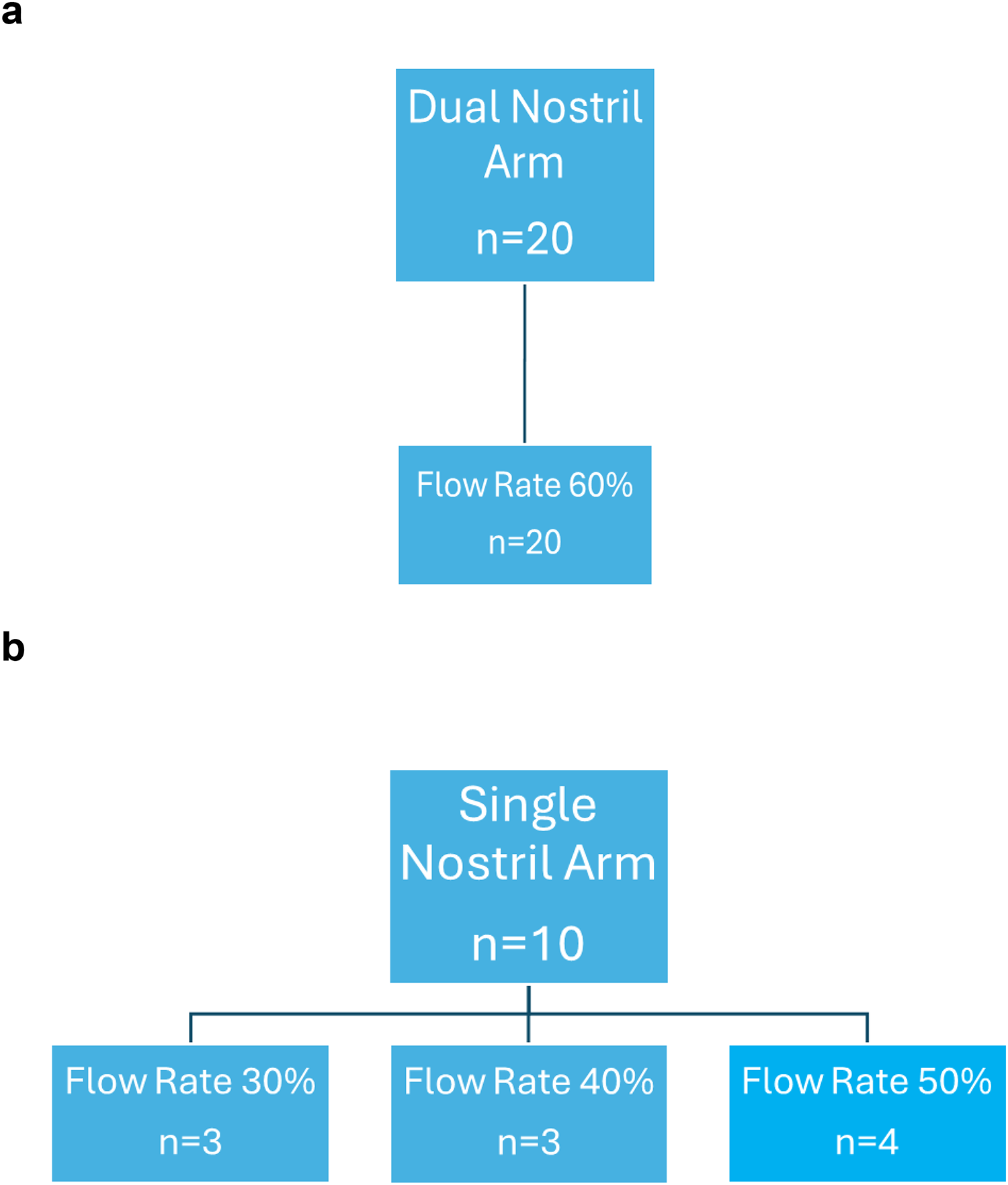
Flow rates for
Statistical analysis
The primary endpoint was defined as the CoolStat tnTMD system’s ability to safely and adequately achieve and maintain normothermic cooling therapy over 24 hours for subjects enrolled in the study. The CoolStat tnTMD was considered successful if it achieved the goal cooling performance and temperature maintenance. Successful cooling performance was defined as the percentage of subjects that reached normothermia within 4 hours of starting CoolStat treatment. Temperature maintenance was defined as the percentage of subjects held within a 1.5°C temperature band between 36°C and 37.5°C for 80% of the steady-state time following the initial achievement of 37.5°C. Secondary endpoints included the incidence of shivering and temperature burden over the 24-hour cooling period. Safety outcomes of the study assessed included (1) incidence and severity of all adverse events and (2) contributions to an AE that may be device-related or related to tn cooling therapy. Data from earlier cohorts in this study were used to identify the relationship between delivered flow rates, using either a single- or dual-nostril approach, and reductions in temperature over the first 4 hours of cooling. Data are presented as mean and standard deviation and were analyzed using SPSS software (version 24.0; IBM Corp., Aronk, NY) with a level of significance set at p < 0.05. Data from the single nostril analysis were compared with truncated data from previously reported double-nostril 8- and 24-hour data, with a focus on corresponding data points from each group. A paired t-test was used to compare baseline temperature readings with those at the completion of 24 hours of treatment. When indicated, statistical analysis was performed using a paired t-test and a chi-square test.
Results
Patient and cooling characteristics
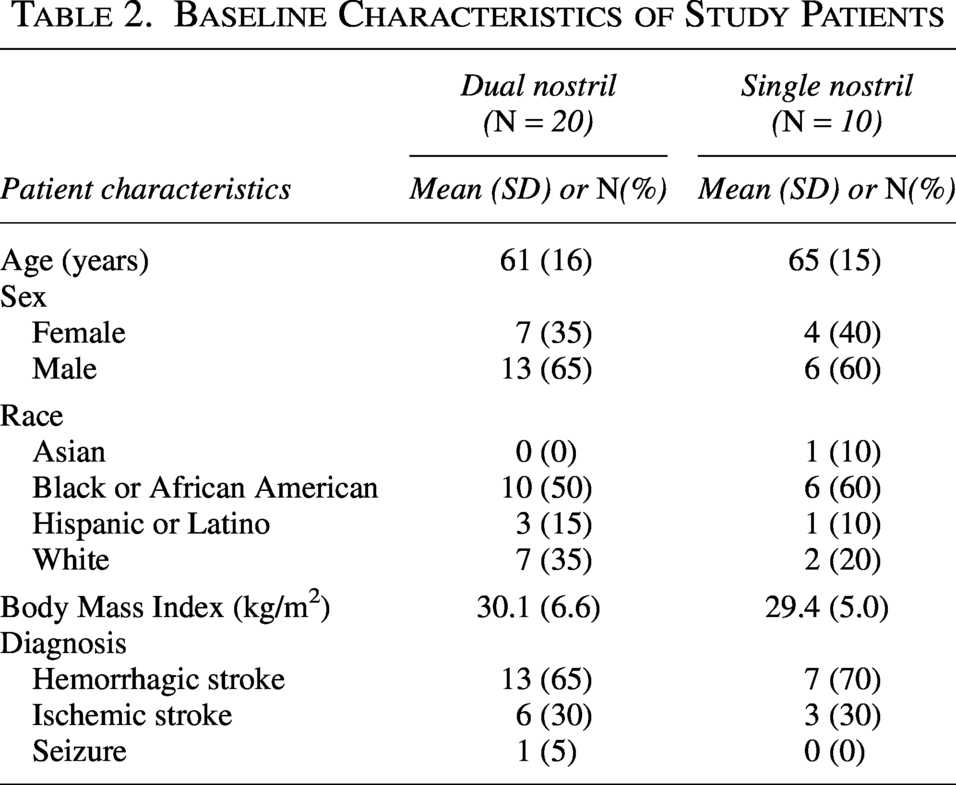
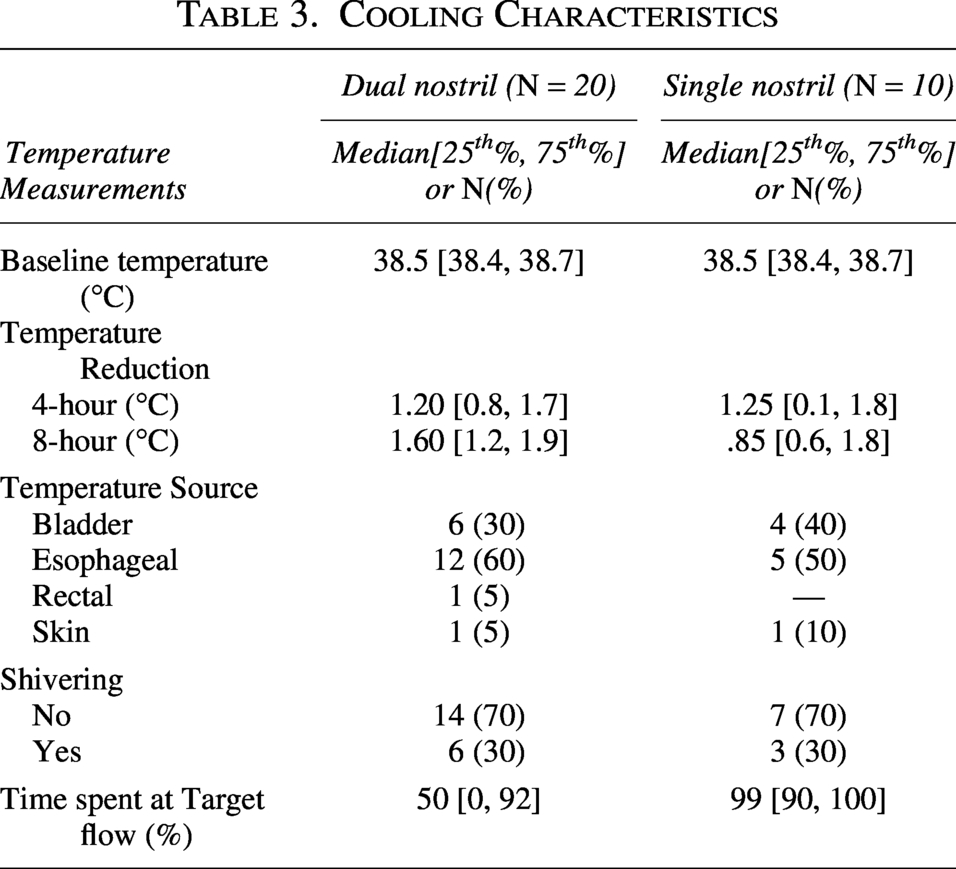
This analysis included data from 30 patients treated with the CoolStat tnTMD: 20 patients from the two previously published dual-nostril cohorts (8-hour and 24-hour) and 10 patients newly enrolled in the single-nostril dose-escalation cohort. As seen in Table 2, both groups had similar demographics. Hemorrhagic stroke was the most common admitting diagnosis. Starting temperatures were 38.5°C in both groups, and both groups achieved a median temperature reduction of 1.2°C over the 4-hour period (Table 3).
Baseline Characteristics of Study Patients
Cooling Characteristics
In the 24-hour single-nostril dose-escalation cohort, none of the patients undergoing cooling at 30 L/min achieved normothermia, whereas two of the four patients at 50 L/min and all three at 40 L/min achieved normothermia within the target window of 4 hours. A comparison of the cooling rates over 24 hours is shown in Figure 2a and b. Both 40 L/min and 50 L/min were more effective at reducing temperatures at 4 hours. The most consistent performing rate was 40 L/min, which reduced the temperature quickly and maintained it better than the other subgroups (Fig. 2). The single-nostril approach (>40 L/min) maintained normothermia throughout the 24-hour cooling period, as indicated by the median temperature burden (−0.14°C*hr [−0.3°C*hr, −0.03°C*hr]).
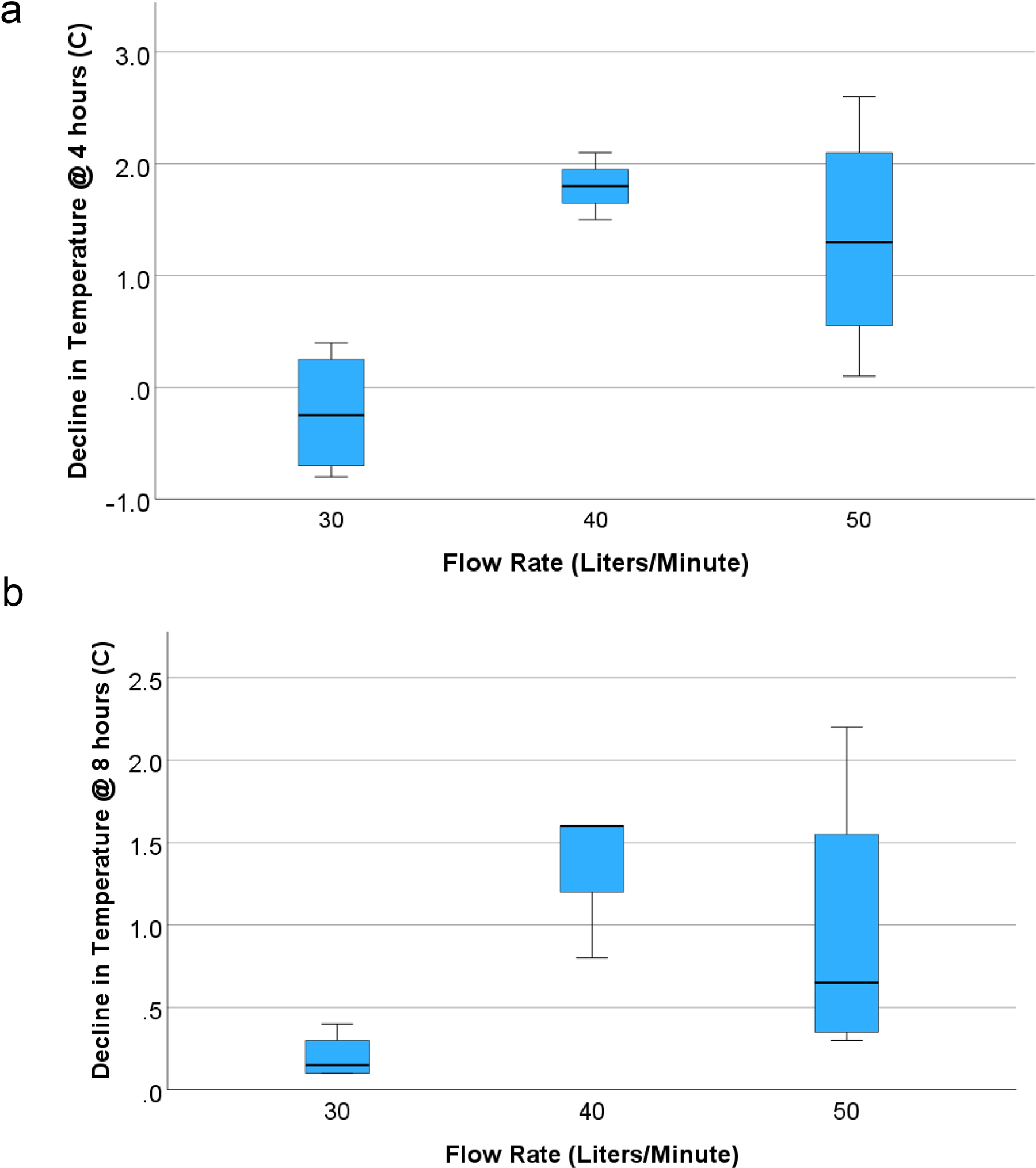
Reduction in temperature from baseline at
One patient in each of the single-nostril subgroups (30%) experienced shivering (BSAS > 1); however, no severe shivering episodes (BSAS 3) were reported. Additional adverse events included insufficient cooling and one incident of an adverse effect on the subject’s blood pressure. No direct correlation was made between the impact on the blood pressure and the CoolStat tnTMD. No local adverse effects were identified upon examination of the nares and nasal mucosa.
Discussion
This study found the following: (1) a novel single-nostril design resulted in successful and consistent normothermia targets for up to 24 hours and within 4 hours of initiation, (2) flow rates of 40 L/min and 50 L/min were necessary to achieve normothermia targets (with the 40 L/min group being more effective), and (3) tn cooling resulted in less shivering. The single-nostril tn cooling device allowed a longer time at the target temperature than the dual-nostril device (99% vs. 50%), making it superior at maintaining normothermia (Table 3).
This is the third reported analysis of the CoolStat tnTMD device, confirming the efficacy of this novel tn device in achieving normothermia among febrile patients with cerebral injury (Arnold et al., 2023; Badjatia et al., 2021). We have found this approach to be a feasible and effective method of attaining and maintaining normothermia in an at-risk population. Importantly, normothermia was achieved without serious adverse events and minimal shivering. As seen in the recently published INTREPID trial, shivering during targeted normothermia is the most common adverse effect of targeted temperature management (TTM) with surface cooling, occurring in nearly 90% of patients (Greer et al., 2024). Shivering is metabolically costly and impacts the overall effectiveness of the fever prevention intervention in this trial. Our data from these three cohort analyses indicate that there will almost always be a shivering response to declining body temperatures regardless of the cooling method; however, the tn approach is associated with a far lower incidence of shivering than existing cooling techniques.
This study was novel for demonstrating that normothermia could be achieved via single-nostril airflow, which has important practical and physiological implications. This approach allows continued use of nasogastric tubes and supplemental oxygen, opening the possibility of using tn cooling in non-tracheally intubated patients. In the 2024 INTREPID trial, approximately one-third of patients were not endotracheally intubated at the time of intervention, and many were extubated during the cooling intervention (Greer et al., 2024). Anti-shivering medication cessation, required for safe extubation, necessitated the interruption of cooling efforts, potentially exacerbating the detrimental effects of hyperthermia. A technique that does not rely on moderate levels of sedation would simplify TTM therapy and make it widely available to neurologically injured patients.
Tn cooling relies on the evaporation of water over the large volume of circulating venous blood on the nasal turbinates, resulting in systemic cooling with a simple tn system rather than surface cooling pads, which increase the risk of dermatologic injury. The cooling effect may directly impact the closely located hypothalamic thermoregulatory regions of the brain. This direct brain-cooling mechanism is well established in animals, with studies demonstrating significant selective brain cooling and systemic cooling in porcine models (Madden et al., 2017).
There are several limitations to this study. First, the sample size was small, and there were no control subjects to compare the cooling efficacy. However, as noted previously, tn cooling was comparable to surface cooling in terms of cooling effectiveness and with fewer shivering complications. The transition from a dual-nostril to a single-nostril device midway through the study made the analysis more complex. This study was also conducted across multiple institutions, increasing the generalizability of our findings. Additionally, previously reported cohort analyses were not identical, limiting direct comparability. Finally, the duration of cooling was limited to 24 hours, and the results from this or previous reported cohort analyses cannot comment on the durability of trans-nasal cooling over multiple days.
Conclusions
The results of this study indicate that tn cooling of febrile patients can be achieved using single-nostril airflow at a minimum flow rate of 40 L/min. Future studies evaluating the effectiveness of therapeutic normothermia should use a tn approach to minimize the impact of shivering on outcomes. A confirmatory study investigating this approach is underway (NCT06038513:).
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.