
Abstract
Purpose:
Childhood cancer survivors (CCS) face increased morbidity and mortality compared to the general population. Diet quality is an important modifiable factor influencing long-term outcomes. This study aimed to evaluate the diet quality of young adult CCS and compare it with age- and gender-matched peers.
Methods:
Dietary intake from 25 young adult CCS was assessed using the Automated Self-Administered Dietary Assessment Tool (ASA24) and compared with 100 age- and gender-matched healthy control participants from the National Health and Nutrition Examination Survey 2017–2018. Differences in Healthy Eating Index (HEI) 2020 total and component scores were analyzed using independent t-tests.
Results:
Overall, HEI scores did not differ between CCS and controls (p = 0.76). The CCS sample had a significantly higher intake of the following adequacy components: whole fruit (p = 0.03), total vegetables (p = 0.01), greens and beans (p = 0.01), total protein foods (p < 0.001), and dairy (p = 0.03). However, the CCS sample also reported a significantly lower unsaturated-to-saturated fatty acid ratio (p = 0.01) and a higher total fatty acid intake (p < 0.001).
Conclusions:
Excessive consumption of saturated and total fatty acids may exacerbate long-term health risks; therefore, young adult CCSs may benefit from cancer-specific education and resources to encourage reducing unhealthy food consumption.
Keywords
Introduction
Childhood cancer survivors (CCS) are a growing population, as 5-year survival rates have increased from approximately 58% in the 1970s to over 85% today, resulting in a substantial expansion of the survivor population in the United States.1,2 Despite these improvements in survival, CCSs experience significantly higher rates of chronic health conditions, cardiovascular disease (CVD), and premature mortality compared with the general population. 1 Due to genetic predisposition, adverse treatment effects, and their primary cancer diagnosis, CCS have three to six times greater risk of secondary cancers compared to the general population, and this risk increases with age. 1 For example, certain cancer treatments, including anthracycline chemotherapy treatment and mediastinal radiation exposure, predispose survivors to late cardiac effects (e.g., arterial disease, cardiomyopathy, and heart failure). 1 Therefore, the Children’s Oncology Group (COG) recommends that CCS receive annual guideline-based cancer survivorship care that is specific to their cancer history. 3 Notably, CCS engagement in positive health behaviors, such as adherence to a high-quality diet, can mitigate some of these concerns.3,4 However, adolescent and young adult survivors of childhood cancer may experience barriers related to time constraints, food costs, and food preparation that hinder adherence to a high-quality diet. 5
The developmental stage of young adulthood (ages 18–39 years) is a period of transition where individuals take on responsibilities of self-management, including managing health behaviors. 6 Young adults attain new freedoms at this time and, simultaneously, often report worse lifestyle behaviors, such as poor diet quality, increased alcohol consumption, and recreational substance use.5–7 Moreover, habits formed during young adulthood can persist into mid- and late-adulthood.5,8,9 As a result of unhealthy lifestyle behaviors, young adults experience the fastest weight gain of all age groups, averaging 1–2 pounds a year, which can exacerbate the already increased risk of secondary cancers, late cardiac effects, and premature mortality. 9 Previous studies have identified that survivors of adult cancer report poorer dietary scores compared to control patients without a cancer history.10,11 However, there is limited information on the dietary intake of CCS, specifically during the period of young adulthood. 11 An improved understanding of the dietary quality and composition of young adult CCS may point to specific intervention targets that could improve short- and long-term health outcomes in this high-risk group.
Diet quality is an important modifiable lifestyle factor that can reduce the morbidity and mortality of cancer survivors and healthy individuals.12,13 The American Cancer Society (ACS) and COG provide survivorship guidelines that emphasize adherence to healthy dietary patterns.14,15 However, no dietary recommendations have been developed specifically for young adult survivors of childhood cancer. Previous research suggests that diet quality among CCS is often suboptimal, with many failing to meet national dietary recommendations for fruits, vegetables, whole grains, and saturated fat intake.16–18 Most existing studies have focused on broad survivor populations or older adult cohorts, with limited emphasis on the young adult developmental stage or direct comparison to age-matched population controls. Therefore, further evaluation of the diet quality in young adult CCSs would better characterize dietary patterns during this transitional life stage.
In the absence of survivor-specific dietary standards, the ACS directs survivors to follow dietary patterns consistent with the United States Department of Agriculture’s (USDA) Dietary Guidelines for Americans 2020–2025 (DGA).19,20 The four main recommendations of the DGA 2020–2050 are to follow a healthy dietary pattern at every life stage, customize and enjoy nutrient-dense foods to reflect personal preferences, focus on meeting food group needs with nutrient-dense foods while staying within caloric limits, and limit added sugars, saturated fat, sodium, and alcohol in one’s diet. 20 Furthermore, the USDA has provided a quantitative dietary quality scoring index, the Healthy Eating Index (HEI) 2020, based on the recommendations in the most recent DGA. 21 The HEI evaluates for adequacy components (e.g., food groups that are encouraged) and moderation components (e.g., dietary elements with recommended limits of consumption). 21 Observational studies have found that a high HEI score is associated with a reduced risk of cardiovascular mortality, cancer mortality, and all-cause mortality. 22
This study has two aims: (1) to quantitatively compare the HEI scores of young adult CCS to age- and gender-matched National Health and Nutrition Examination Survey (NHANES) controls and (2) to determine the differences in dietary component scores between the prospective and control groups. By using NHANES data to compare young adult cancer survivors to age- and gender-matched controls, this study aims to highlight the most important opportunities for dietary improvement in this at-risk population.
Methods
Participants
This study is part of a larger study that sought to examine the relationship between stress and health behaviors among young adult CCS. Recruitment took place from March 2024 to October 2024. The inclusion criteria for the present study were as follows: (1) participants were young adults between the ages of 18 and 39 years at the time of study participation; (2) participants were diagnosed with cancer before 18 years of age; and (3) participants were proficient in the English language. Young adult CCS were excluded if they were currently receiving treatment for cancer recurrence or a secondary cancer diagnosis. Purposive sampling was implemented to include survivors across the study’s target age range (18–39) with varying racial and ethnic backgrounds. The participants were compensated for their time.
Procedure
Participants were recruited from an existing patient registry maintained between a pediatric hospital and an adult patient-centered hospital. The registry contained participants who were diagnosed with cancer between infancy and 25 years of age. Patients consented to participate in the registry during a routine care appointment at the pediatric- or adult-focused survivorship clinic. All participants in the registry were reviewed for eligibility using a verified electronic health record (EHR) review. Eligible registry participants were then approached for this study via an online health portal message or telephone call. Trained staff provided study information to potential participants and obtained informed verbal consent following the procedures of the Institutional Review Board (IRB) (University of Kansas Medical Center IRB #00150595). After consent was obtained, the participants completed online surveys for the larger study. Following the completion of these surveys, a subset of participants agreed to complete an online dietary recall for up to 3 days.
Measures
Demographics
Demographic information, including age, race, ethnicity, address, and insurance, was abstracted from existing patient registry and EHR data. Participants then reported updated demographic information using the Diversity Dimensions Measurement Tool. 23 This tool uses the ADDRESSING (age & generation, developmental disability, disability, religion, ethnicity and race, socioeconomic status, sexual orientation, national origin and language, gender) Framework to capture the complexities of individuals’ identities. 24
Dietary behavior
Dietary behavior was assessed for 3 days using the Automated Self-Administered Dietary Assessment Tool (ASA24)from the National Cancer Institute. 25 Participants completed the ASA24 independently using the web-based platform on their own personal devices. The ASA24 has acceptable face validity and has close agreement with interviewer-administered recalls.25,26 Participants were asked to complete 3 days of dietary recall within 7 days using the Automated Self-administered 24-h (ASA24) Dietary Assessment Tool website, which guided them through the process of inputting their complete dietary intake from the previous day. Participants were instructed to complete three consecutive 24-h dietary recalls within 7 days, including 2 weekdays and 1 weekend day. However, all completed recalls were included in the analyses regardless of whether they occurred on consecutive days or met the intended distribution of 2 weekdays and 1 weekend day. Participants were sent text and email reminders to complete their dietary intake logs if they had not logged 3 days of dietary data within 7 days. If fewer than 3 days were completed, all available recalls (minimum 1 day) were used in the analysis.
HEI scores
HEI scores were calculated based on the most recent scoring guidelines published by the USDA and using the open-source R package “dietaryindex,” 27 The HEI is made up of nine adequacy components (total fruits, whole fruits, total vegetables, greens and beans, whole grains, dairy, total protein foods, seafood and plant proteins, and fatty acid ratio) and four moderation components (refined grains, sodium, added sugars, and total fatty acids). A higher total HEI score indicates better diet quality as defined by the USDA’s DGA. 21 HEI scores range from 0 to 100, and HEI scores greater than 80 indicate a high-quality diet, scores ranging from 51 to 80 reflect a diet that needs improvement, and HEI scores less than 51 indicate a low-quality diet. 28 HEI and component scores were calculated separately for each completed recall day and then averaged across available recall days for each participant.
Analytic plan
A control sample of 100 age- and gender-matched individuals without a history of cancer and with at least 2 days of dietary recall was randomly selected from the NHANES 2017–2018 dataset. A 1:4 ratio of cases to controls was utilized to improve the study’s power. 29 Furthermore, the control sample was created from the NHANES 2017–2018 dataset, as it was the most recent NHANES dataset not affected by the COVID-19 pandemic, which was considered a potential confounding factor. 30 Selection was performed through IBM SPSS’s individual matching function based on both gender and age. 31 HEI scores were calculated based on the USDA guidelines and using the open-source R package described above.
The statistical significance between the two groups’ HEI and component scores was calculated using a two-tailed t-test. Linear regression was used to evaluate whether current young adult age significantly predicted HEI scores in the CCS sample. The significance of the relationship between gender and HEI scores of the young adult CCS sample was calculated with a two-tailed t-test. The level of significance was set at p < 0.05.
Results
Participants
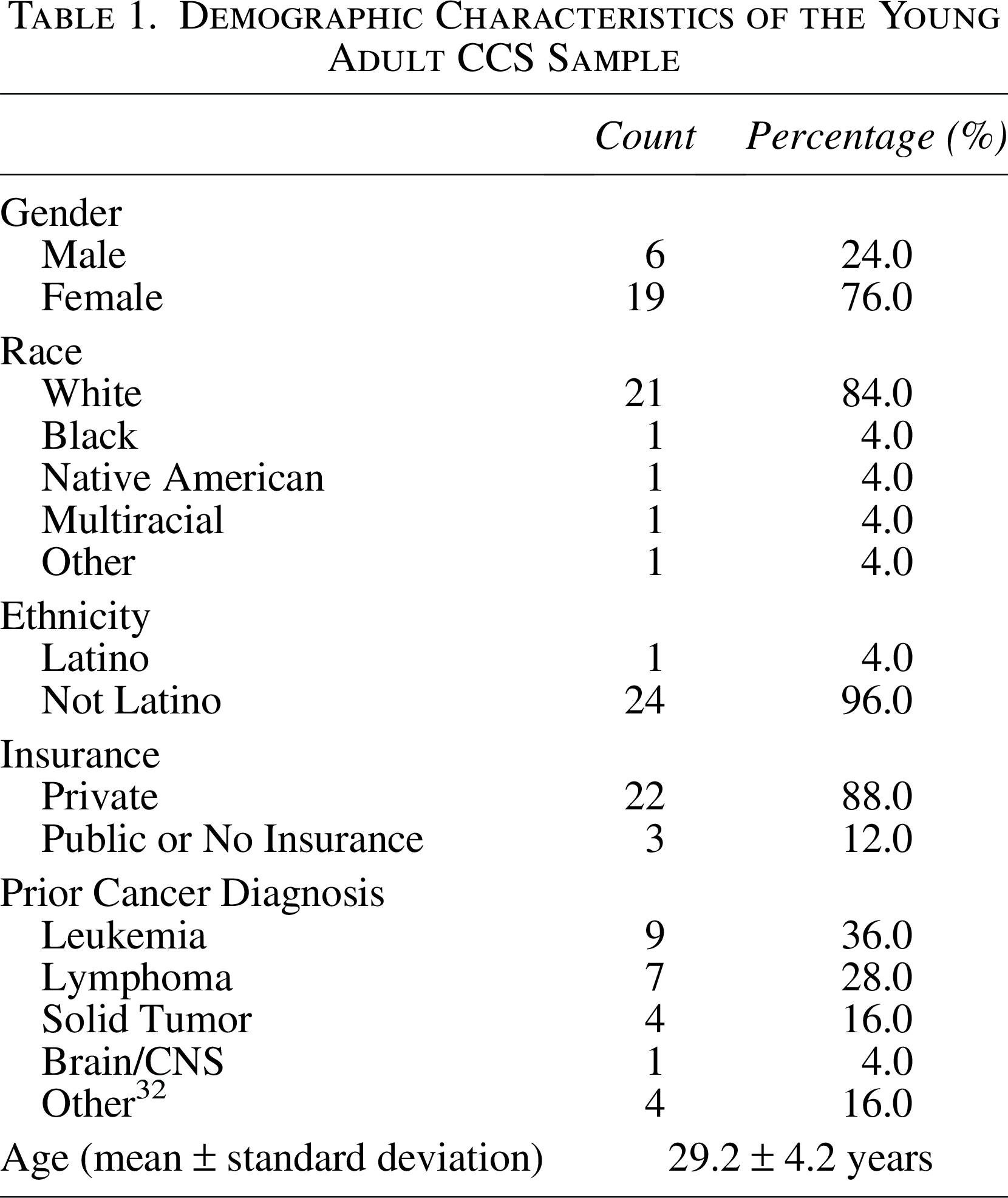
Of the 51 CCSs who completed the surveys as part of the broader study, 25 completed at least 1 full day of dietary recall. The demographics of participating in the CCS are presented in Table 1. Of the 25 CCSs who participated in the dietary recall, four completed 1 day, six completed 2 days, and 15 completed 3 days of recall (2.4 ± 0.77 days). Six participants were male (24%), and 19 were female (76%). Nine had a prior cancer diagnosis of leukemia (36%), seven had lymphoma (28%), four had a solid tumor (16%), one had a brain/central nervous system cancer (4%), and four had an unspecified cancer diagnosis (16%) (Table 1). There was no statistically significant difference between the sample that completed at least 1 day of ASA24 dietary recall and the larger study sample in terms of participant age (p = 0.56), gender (p = 0.24), race (p = 0.08), ethnicity (p = 0.34), or insurance status (p = 0.46).
Demographic Characteristics of the Young Adult CCS Sample
HEI scores of the young adult CCS sample compared to the control sample
The young adult CCS sample had an HEI score of 49.0 ± 11.8 compared to the control sample’s HEI score of 48.1 ± 13.1 (p = 0.76) (Table 2). The CCS sample did report significantly higher consumption of whole fruits (2.9 ± 2.3 vs. 1.8 ± 2.0; p = 0.03), total vegetables (3.4 ± 1.2 vs. 2.6 ± 1.3; p = 0.01), greens and beans (2.7 ± 2.2 vs. 1.4 ± 1.6; p = 0.01), total protein foods (4.8 ± 0.7 vs. 4.0 ± 1.1; p < 0.001), and dairy (6.2 ± 3.0 vs. 4.7 ± 2.7; p = 0.03), indicating that the CCS sample exceeded age- and gender-matched controls in their healthful consumption of these dietary components (Table 2). The control sample had significantly higher scores for the fatty acid ratio (5.0 ± 3.0 vs. 3.1 ± 2.9; p = 0.01) and fatty acids (5.8 ± 2.9 vs. 2.2 ± 2.7; p < 0.001) components, indicating that the CCS sample had a worse ratio of poly- and mono-unsaturated fatty acids to saturated fatty acids and consumed an excess of all fatty acids (Tables 2 and 3).
Dietary Component Intakes for the Young Adult CCS and Control Samples Compared to the USDA Reference Targets
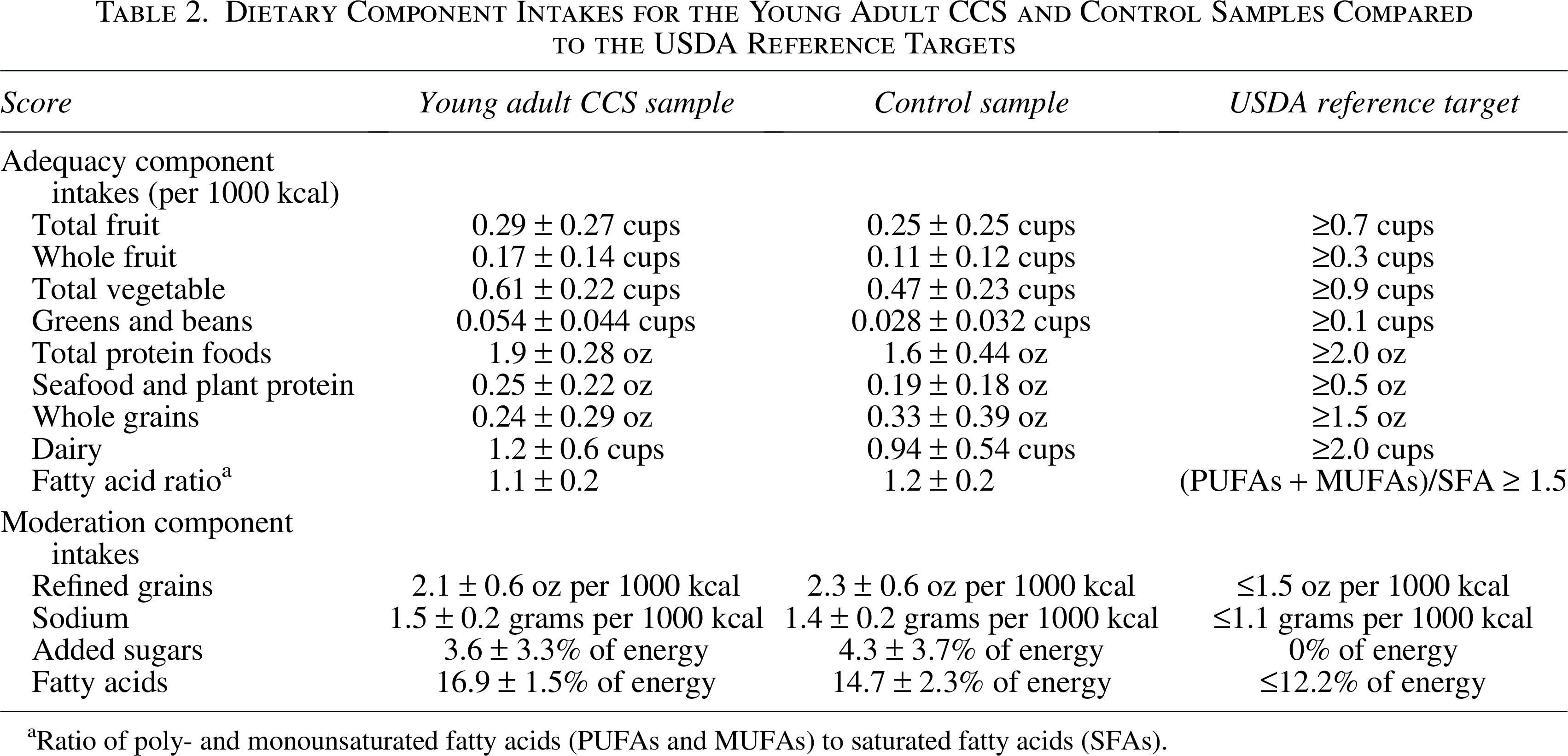
Ratio of poly- and monounsaturated fatty acids (PUFAs and MUFAs) to saturated fatty acids (SFAs).
HEI Score and Component Score Means ± Standard Deviations for the Young Adult CCS and Control Samples
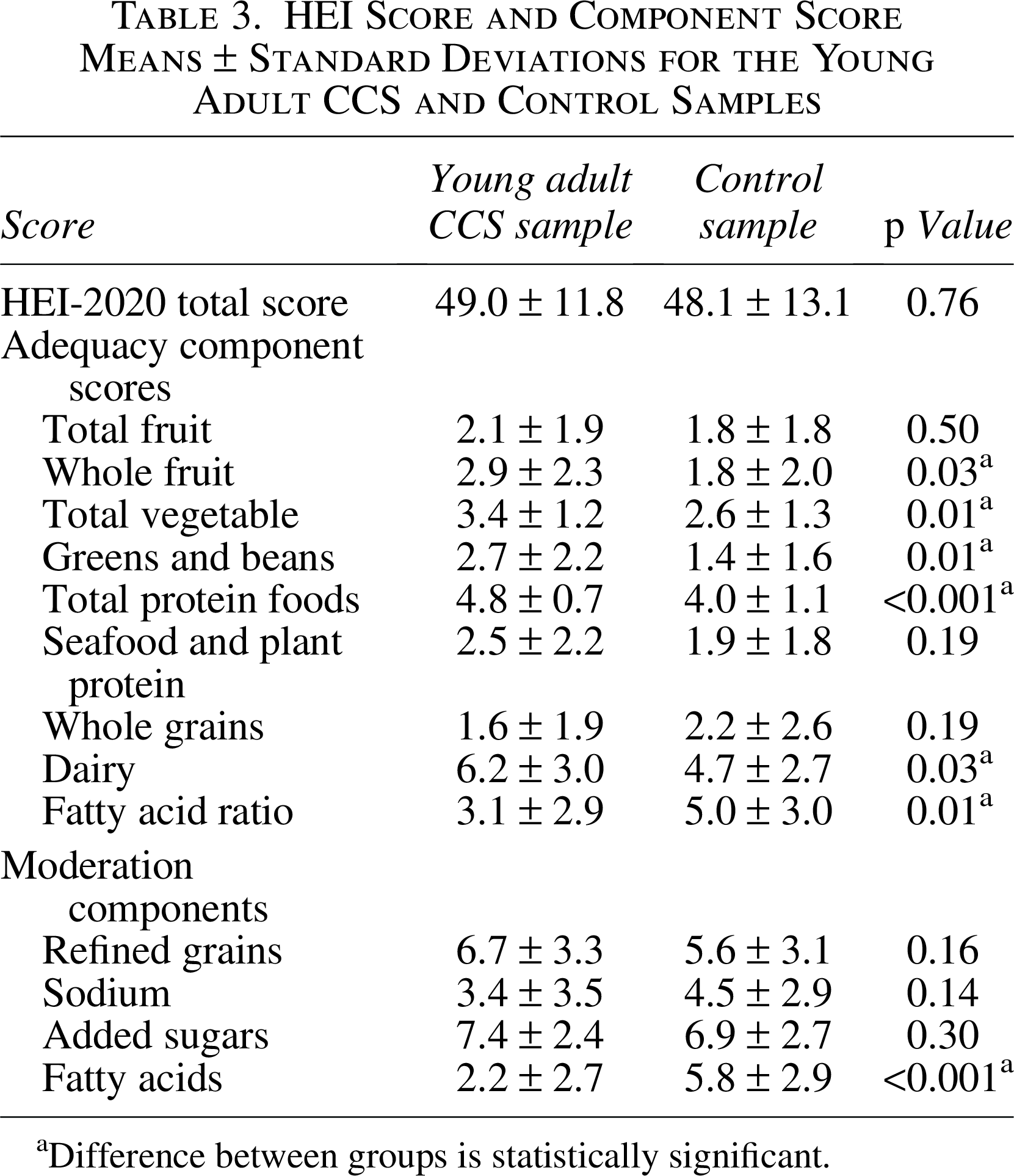
Difference between groups is statistically significant.
HEI score by gender and age
In the CCS sample, age was positively associated with HEI score (β = 0.88, SE = 0.56); however, this association was not statistically significant (p = 0.13). Furthermore, the young adult CCS sample’s male participants had a mean HEI score of (52.9 ± 12.7) compared to the female participants’ mean HEI score of (47.7 ± 11.6). However, this difference was not statistically significant (p = 0.36).
Discussion
The results of this study suggest that young adult CCS did not differ significantly from age- and sex-matched peers without a cancer history in overall diet quality as measured by total HEI score. However, CCS demonstrated a lower unsaturated-to-saturated fatty acid ratio and higher total fatty acid intake compared with controls. Notably, both samples had an average HEI score below 50% of the maximum HEI score, indicating an overall poor adherence to the 2020 Dietary Guidelines for Americans. This may be due to the many barriers that young adults face in making healthy dietary choices. 5 Previous studies have found that this age group is significantly limited by time constraints, food costs, and barriers to food/preparation and planning. 5 Specifically, studies investigating barriers to healthy eating among CCS include personal food taste preferences, a lack of dietary knowledge, and limited food availability. 33 Among our study participants, the young adult CCS had a significantly higher consumption of whole fruits, total vegetables, greens and beans, total protein foods, and dairy components compared to the control sample. However, they also had a higher consumption of the unhealthy components of fatty acids and saturated fats, which are commonly found in processed meats, fried foods, commercially baked goods, and high-fat dairy products.
Prior studies have found that cancer survivors have significantly worse dietary quality than a matched control group.11,33,34 For instance, one previous study found that NHANES adult cancer survivors had slightly lower HEI 2010 scores compared to an age, sex, and race/ethnicity control group. 11 Specifically, this study identified the cancer survivors’ “empty calorie” score, calories from solid fats, alcohol, and added sugars, to be significantly lower than the control sample. Another study found that CCS between the ages of 13 and 35 years had significantly worse diet quality and higher rates of “picky eating” than age-matched controls. 34 A European case-control study found that CCS had a significantly lower quality of diet compared to the general population. 17 The lack of a significant difference in overall HEI scores may be due to the way the comparison groups were selected. Our study used age- and sex-matched population-level controls from NHANES, which may provide a broader representation of typical dietary patterns. 35 Although no significant difference was detected in overall HEI scores, the dietary patterns observed remain clinically relevant. This is particularly important for young adult CCS, who face a heightened risk of developing chronic health conditions, and this risk can be further exacerbated by suboptimal dietary practices. 11
We also found that gender and age did not have a significant relationship with the HEI scores within our young adult CCS sample. Although some previous studies have found that women have a higher diet quality than men, we did not observe a statistically significant difference by gender.36,37 This discrepancy could be due to several different factors, including a limited prospective sample size and a disproportionately higher number of women than men in both samples. Previous studies have also suggested that diet quality improves throughout adulthood.38,39 Although we found a positive correlation between age and HEI scores, this correlation was not statistically significant, which may be due to our sample size. However, the observed trend merits further investigation with a larger, more diverse cohort to ascertain whether subtle age-related dietary improvements exist among young adult cancer survivors.
While the young adult CCS sample did not have a significantly different overall dietary quality than the control group, they did have worse fatty acid and saturated fat component scores. The CCS’s lower score indicates a high overall intake of fatty acids with a low ratio of unsaturated fatty acids to saturated fatty acids. 21 There is strong evidence that diets high in saturated fatty acids are associated with negative long-term outcomes such as CVD and obesity.40,41 As CVD is a significant cause of long-term morbidity and mortality in cancer survivors, reducing overall fatty acid intake and increasing the ratio of unsaturated fatty acids to saturated fatty acids may play an important role in reducing long-term negative health effects in this population.20,42–44 Previous studies have also demonstrated that young adults are very responsive to dietary-induced changes to cholesterol and lipoproteins, health markers used to monitor for CVD risk. 45 Given this susceptibility, higher intakes of saturated and total fatty acids among cancer survivors may reflect broader patterns of poor dietary habits and limited access to nutrition guidance. 34 Survivors frequently report challenges with adopting healthful eating practices and confusion about dietary fats. 34 Thus, shifting from nutrient-specific messaging toward food-based patterns that promote healthy fats and other beneficial foods while reducing unhealthy components would have the strongest impact on this age group.
Previous studies have found that meat products, particularly red and processed meats, and dairy products are the predominant sources of saturated fatty acids in the diet of Americans.46,47 Increased saturated fatty acid intake from both meat and dairy sources has been associated with an increased risk of mortality and CVD.47,48 But saturated fats from meat sources have been associated with a significantly greater impact on these risks compared to saturated fats from dairy products.46–48 Although omitting or restricting dairy and meat products from the diet of CCS may limit these negative long-term outcomes, both are rich sources of micronutrients (i.e., iron, vitamin D, and several B vitamins) and are considered a standard part of the American diet. 49 Furthermore, young adults have significant limitations in their dietary choices due to time constraints, food costs, and barriers to food preparation. 5 Thus, encouraging substitution with lower dietary fat alternatives, such as lean meats and reduced-fat dairy products, may provide realistic and impactful dietary targets for this population. Future research should explore the drivers of dietary choices in CCS, such as cost, taste preferences, and stressors, to better inform tailored interventions.
The strengths of this study included the use of validated dietary measuring tools (ASA24) to collect dietary information from a novel prospective sample and the use of an age- and gender-matched NHANES control sample. This study also uniquely focuses on a specific high-risk group, young adult CCS, and identifies addressable weaknesses in their dietary habits. However, some limitations must be considered. First, the prospective sample was recruited from one geographical area, whereas the NHANES control sample comprises individuals from a sample representative of the United States population. Additionally, the prospective group was limited in size due to recruitment difficulties. Notably, adolescents and young adults are less likely to participate in cancer research than younger and older individuals. 50 This population of survivors is especially challenging to recruit, as they are transient and more difficult to contact and are more likely to experience interruption of care in oncology settings due to loss of insurance. 51 Consequently, cancer type and treatment exposures were not included in regression analyses due to limited sample size and insufficient detail regarding specific diagnoses and treatment regimens, which restricted our ability to examine these variables as potential confounders.
Overall, both young adult CCSs and young adults without a history of cancer had a low dietary quality and adherence to the 2020 Dietary Guidelines for Americans. Specifically, the young adult CCS sample had worse component scores in the fatty acid and saturated fat categories. Dietary interventions encouraging the substitution of high-saturated-fat meat and dairy products with reduced-fat alternatives may help reduce long-term cardiovascular risk in high-risk CCS. Cancer survivorship clinics, primary care physicians, and other health care providers can play an important role in reducing the intake of unhealthful foods, including reducing total fat and saturated fat intake, and providing resources that are available to this developing age group.50,52 Integrating dietary counseling into survivorship clinics may provide a feasible setting for these interventions.
Authors’ Contributions
K.M.: Conceptualization, methodology, funding acquisition, data curation, formal analysis, investigation, visualization, writing—original draft preparation. R.G.: Conceptualization, methodology, funding acquisition, investigation, visualization, writing—original draft preparation. K.D.: Methodology, supervision, validation, writing—review and editing. K.A.: Investigation, supervision, project administration, writing—review and editing. B.N.L.: Supervision, methodology, writing—review and editing. E.-L.N.: Supervision, methodology, writing—review and editing. C.R.B.: Conceptualization, methodology, funding acquisition, investigation, visualization, writing—review and editing. All authors reviewed and approved the final article.
Footnotes
Acknowledgments
The authors are grateful for the support of the 2024 Children’s Miracle Network Fellowship Grant for funding this project.
Author Disclosure Statement
This study was approved by the University of Kansas Medical Center Institutional Review Board (Study ID: STUDY00150595). All participants provided informed consent prior to participation.
Funding Information
This work was supported by the 2024 Children’s Miracle Network Pediatric Fellowship Grant. The funding source had no role in study design, data collection, analysis, interpretation, or article preparation.