
Abstract
Purpose:
Non-Hodgkin lymphoma (NHL) is a heterogeneous group of cancers. Published recommendations and guidelines for fertility preservation are very general and heterogeneous. Therefore, a very first meta-analysis analyzing the worldwide-published data on the risk of infertility after treatment of NHL is required to better counsel patients regarding fertility issues and to develop further strategies to evaluate the gonadotoxicity of treatments in NHL.
Methods:
A systematic literature search was conducted using Medline, Embase, and Cochrane Database of Systematic Reviews and Cochrane Central Register of Controlled Trials (CENTRAL), including articles published since 2000. Exclusion criteria were cases with disease relapse, follow-up of <1 year, testicular NHL, studies with <40% reproductive markers, and case reports. A total of 4602 records were identified. For the systematic review, 58 studies met the inclusion criteria. In this meta-analysis, 51 studies were included.
Results:
The prevalence of expected infertility is 27% (95% confidence interval [CI] 0.20–0.37) overall, 23% (95% CI: 0.14–0.35) in females, and 35% (95% CI: 0.27–0.44) in males. It is highest after chemotherapy and radiotherapy to the pelvis and testis ± bone marrow transplantation, 43% (95% CI: 0.20–0.69) in females and 57% (95% CI: 0.21–0.86) in males. After alkylating agents in females, it is 24% (95% CI: 0.17–0.34).
Conclusion:
The results of this review and meta-analysis indicate a broad heterogeneity of data regarding the risk of infertility. Therefore, fertility counseling and, if necessary, fertility preservation measures are mandatory before oncologic treatment for NHL. Prospective studies stratified by chemotherapy regimen and including new treatment regimens are urgently needed.
Keywords
Introduction
Non-Hodgkin lymphoma (NHL) is a very heterogeneous group of cancers that arise from lymphocytes, lymph nodes, and lymphoid tissues. Fortunately, it is a relatively rare cancer in patients of reproductive age, but nevertheless, children and adolescents can be affected in exceptional cases. 1 The chances of cure depend on many different factors, such as the type and stage of the lymphoma, the patient’s age, and comorbidities.
Multiagent chemotherapy, immunotherapy, radiotherapy, and high-dose chemotherapy and autologous stem cell transplantation in selected situations and patients have significantly improved survival, with 5-year survival rates in patients aged 14–44 being 90% in women and 87% in men. 1 However, the drawback of these therapies is the relevant long-term complications, including gonadal dysfunction and infertility.2–8
Interestingly, infertility does not seem to be a consequence of gonadotoxic therapy alone; altered sperm DNA and altered spermatogenesis prior to NHL treatment have been described.9–12 In men, there is a correlation between the specific type of drug, cumulative doses, radiation dose to the testes, bone marrow transplantation (BMT), and an alteration of spermatogenesis. 9 Gonadotoxicity of chemotherapy drugs also applies to women. 13
It is therefore very important to discuss fertility preservation measures before starting a gonadotoxic therapy. However, although we know that chemotherapy, BMT, and radiotherapy can cause germ cell and gonadal damage and infertility in girls and boys, 14 as well as in men and women, 15 data on the prevalence of infertility after cancer therapy are still limited. 16
The question of how to assess the risk of infertility after a particular type of cancer treatment is important to avoid unnecessary fertility preservation treatments, especially in women who require invasive and time-consuming ovarian stimulation and oocyte retrieval or ovarian tissue cryopreservation. However, in addition to the psychological and medical stress of fertility preservation for women and the question of whether it is indicated, costs and reimbursement matters are also relevant. In Switzerland, for example, fertility preservation is only reimbursed in cases with a risk of infertility, defined as amenorrhea or azoospermia, of >20%.
However, the existing recommendations and guidelines for the preservation of fertility are both general and heterogeneous, and there is no specific guideline for NHL. Therefore, this systematic review and first meta-analysis aim to provide an approximation of the risk of infertility after NHL treatment in order to give clinically relevant guidance for improved fertility counseling of patients. The meta-analysis is part of the FertiTOX project (www.fertitox.com), which aims to fill the data gap on gonadotoxicity of cancer therapies to enable more accurate fertility counseling. 17
Methods
Registration of protocols
This study protocol was registered in the International Prospective Register of Systematic Reviews (PROSPERO; registry number: CRD42024511940). The Preferred Reporting Items for Systematic Reviews and Meta-Analyses were applied. 18
Search strategy
We conducted a systematic literature search of the Medline, Embase, and CENTRAL and Cochrane Database of Systematic Reviews in April 2024, including articles published since 2000 (Supplementary Data S1). A medical information specialist developed and tested an initial Embase search strategy, using a list of basic references. After refining and consulting, complex search strategies were established based on database-specific controlled vocabulary (i.e., thesaurus terms/subject headings) and text words. Synonyms, acronyms, and similar terms were included in the text word search.
By using a double-negative search strategy based on Ovid “humans-only” filters, animal-only studies were excluded from all searches. The detailed final search strategies are presented in Supplementary Material (Supplementary Data S2). In addition to the search of electronic databases, reference lists and bibliographies of pertinent studies were reviewed for other relevant publications. All identified citations were imported into Covidence. Duplicate entries were removed. 19
Inclusion and exclusion criteria
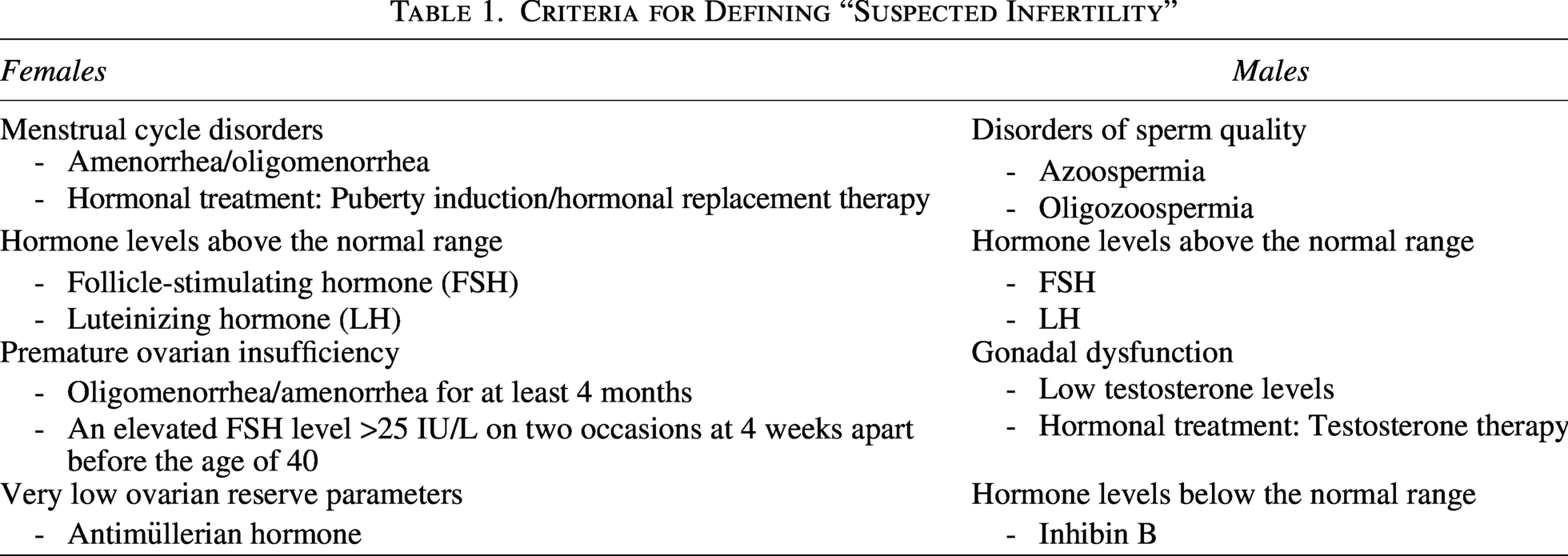
The studies were independently assessed by two investigators (A.V. and D.W.) for inclusion by the Covidence software (www.covidence.org). 20 All original articles with information on the type of tumor therapy and fertility outcome (elevated follicle-stimulating hormone [FSH] levels, low ovarian reserve parameters, amenorrhea, oligomenorrhea, premature ovarian insufficiency [POI], indication for hormonal replacement therapy, oligozoospermia, azoospermia, indication for testosterone substitution) were included. Table 1 describes the criteria for the definition of suspected infertility. Exclusion criteria were cases with disease relapse, follow-up of <1 year, testicular NHL, studies with <40% reproductive markers, and case reports.
Criteria for Defining “Suspected Infertility”
Data extraction
The studies were independently reviewed by two investigators (DW and AV), and the extracted data were summarized in detail by one investigator (ES) (Tables 2 and 3). The following characteristics of the study populations were the key variables of interest: patients’ age at diagnosis and outcome; duration of follow-up, tumor types, tumor class, type of oncological treatment, and fertility parameters.
Characteristics of the Included Studies Females
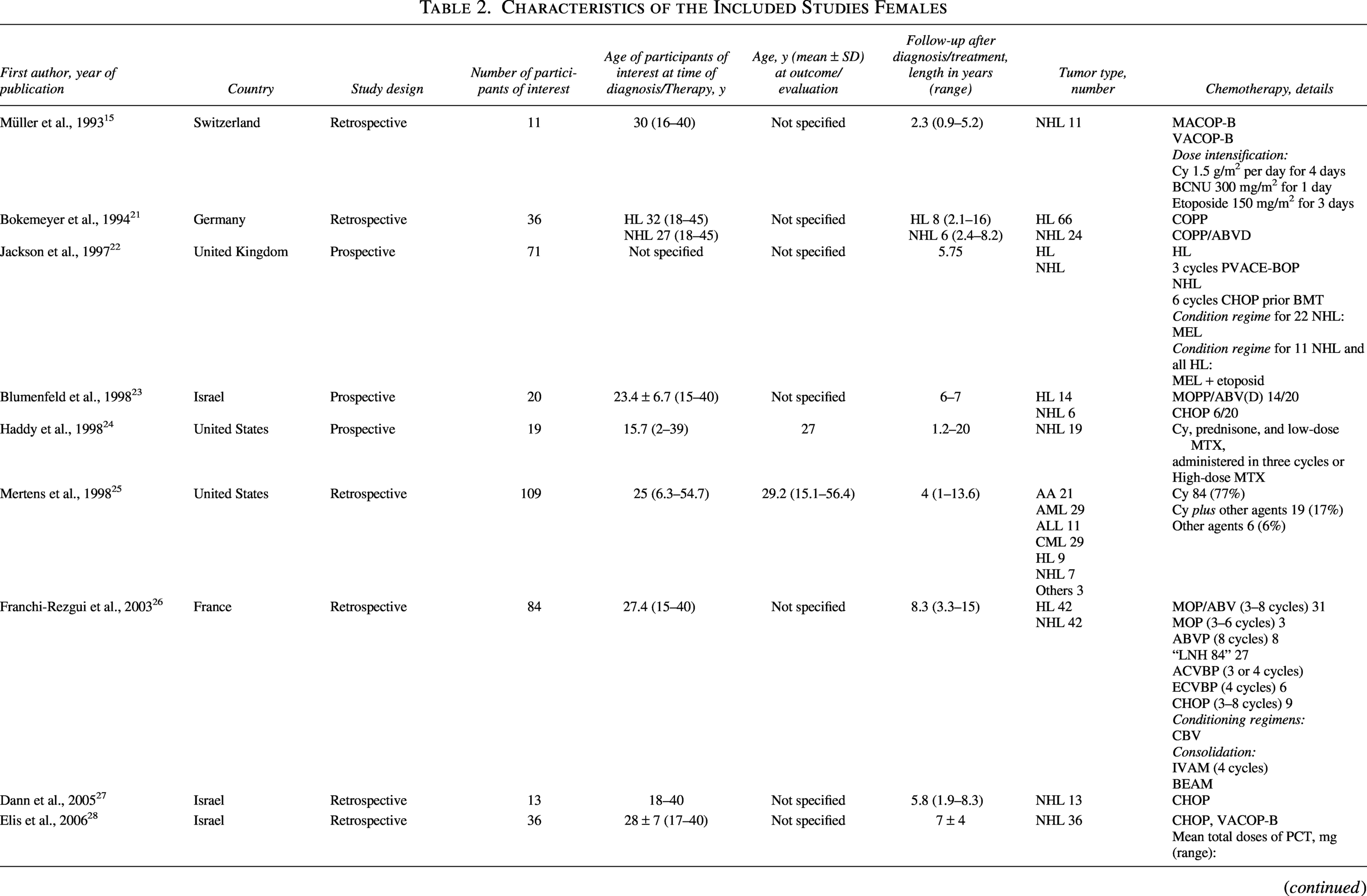
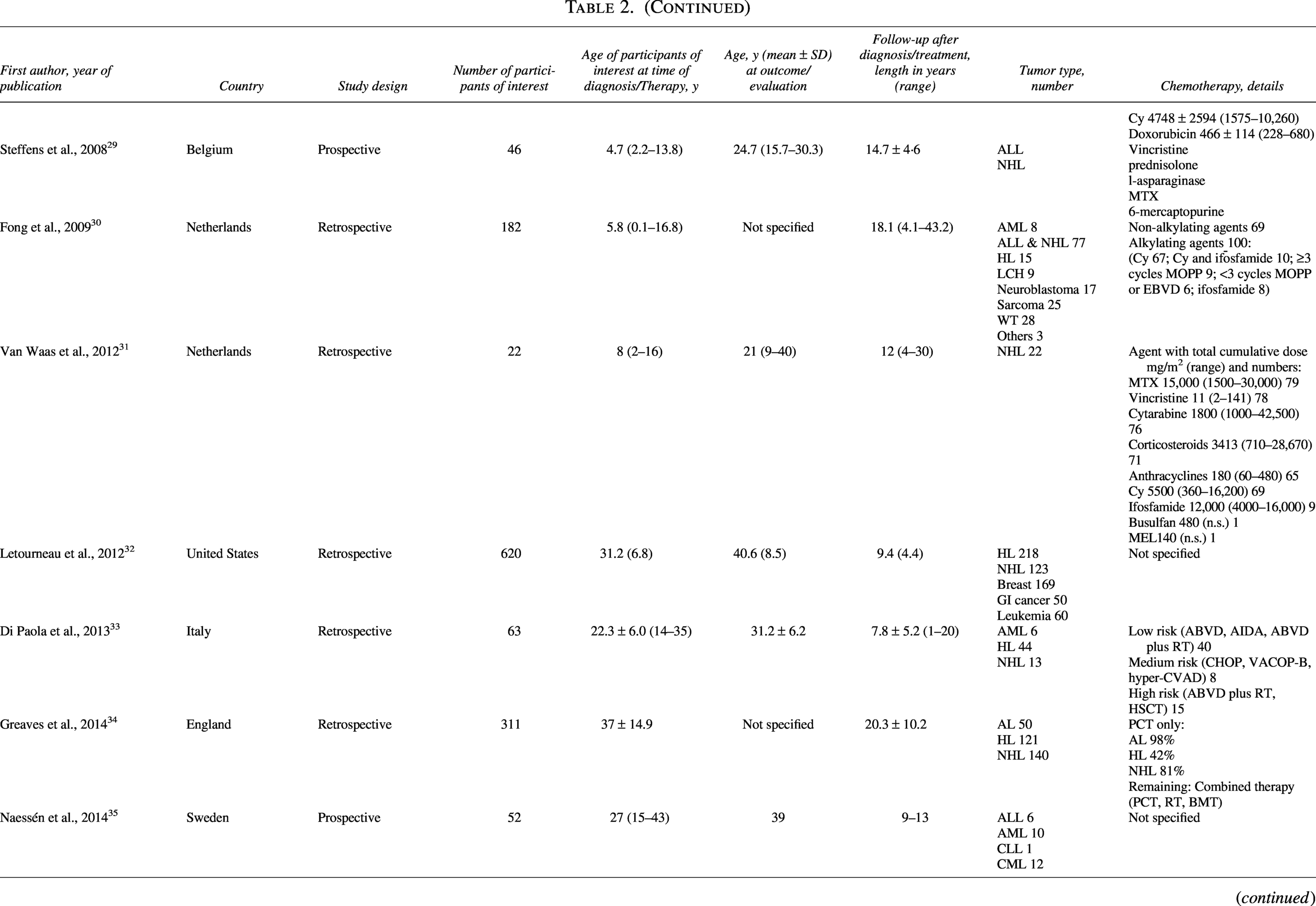
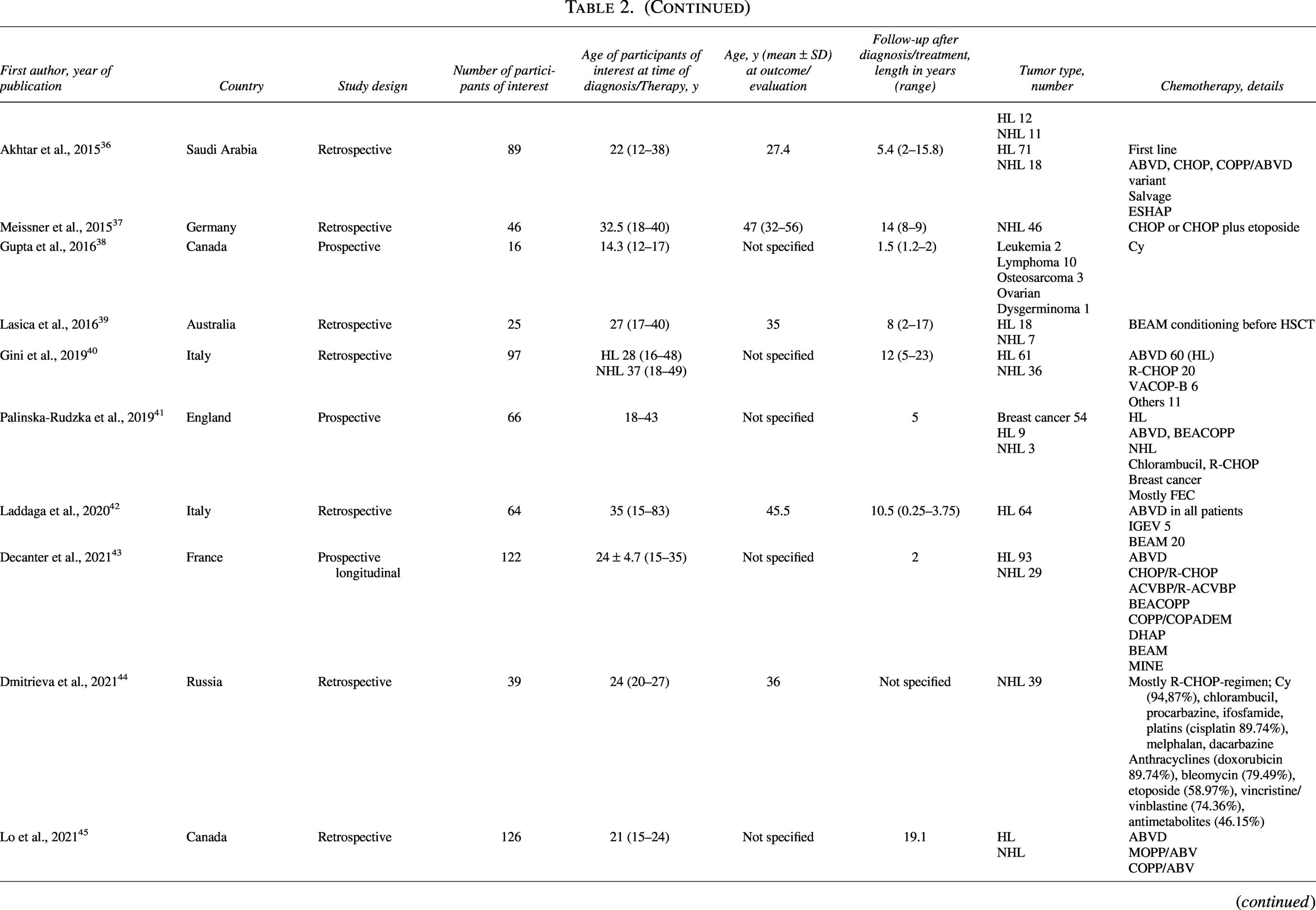
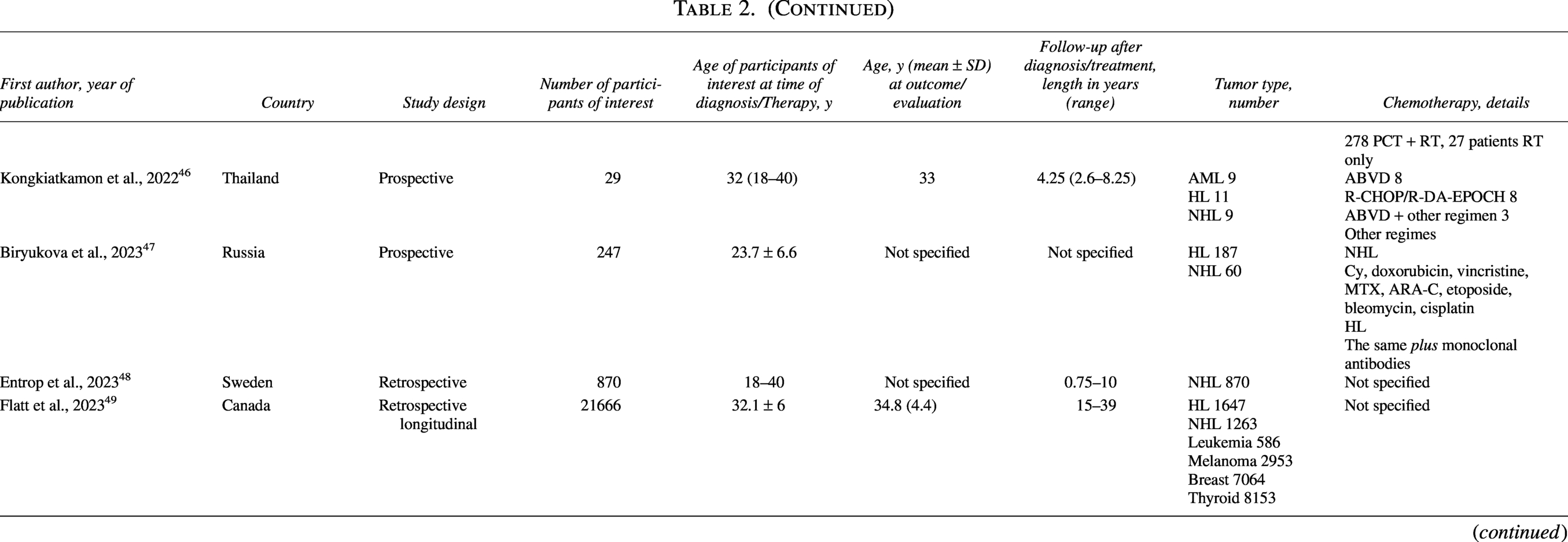
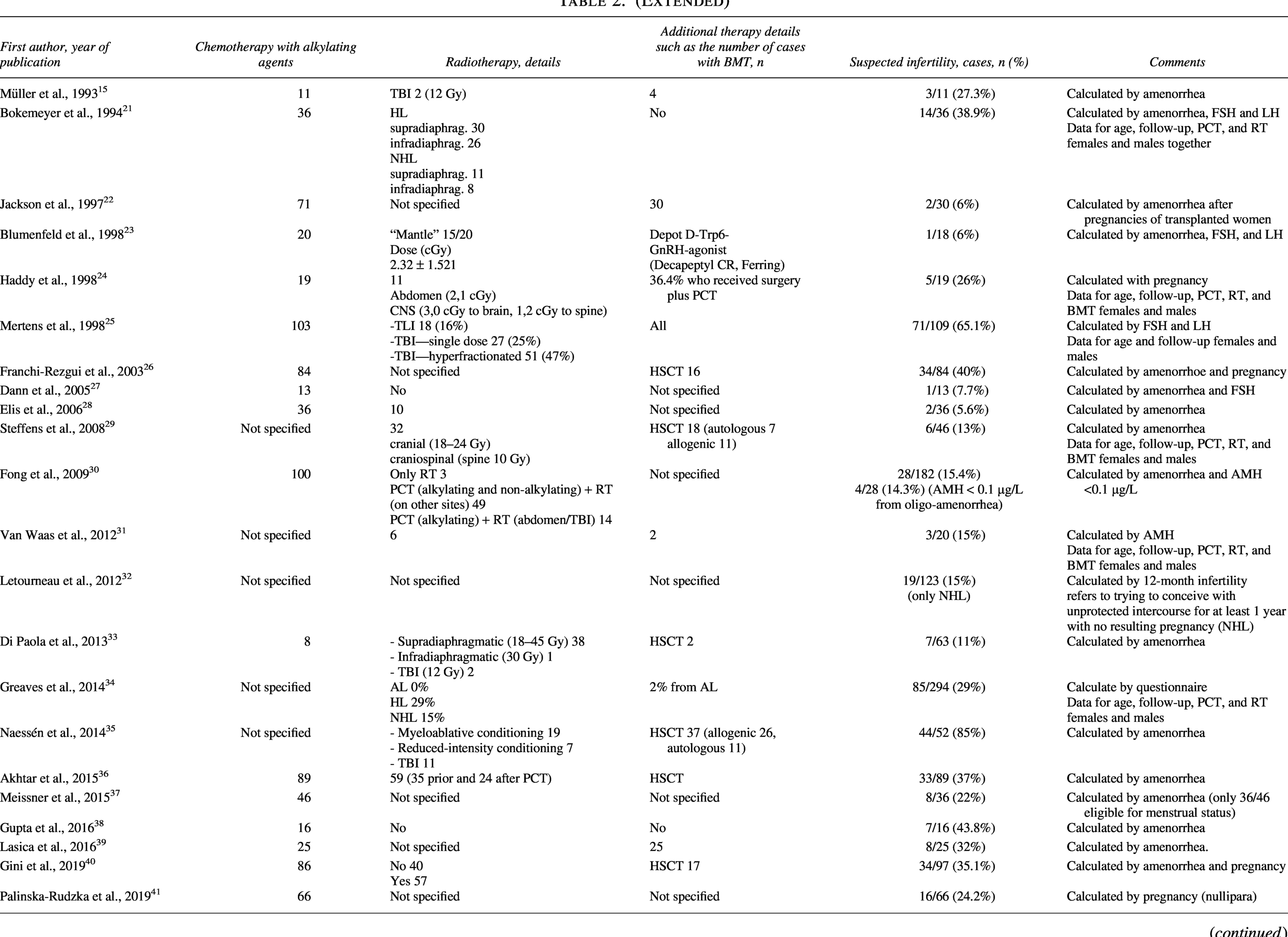
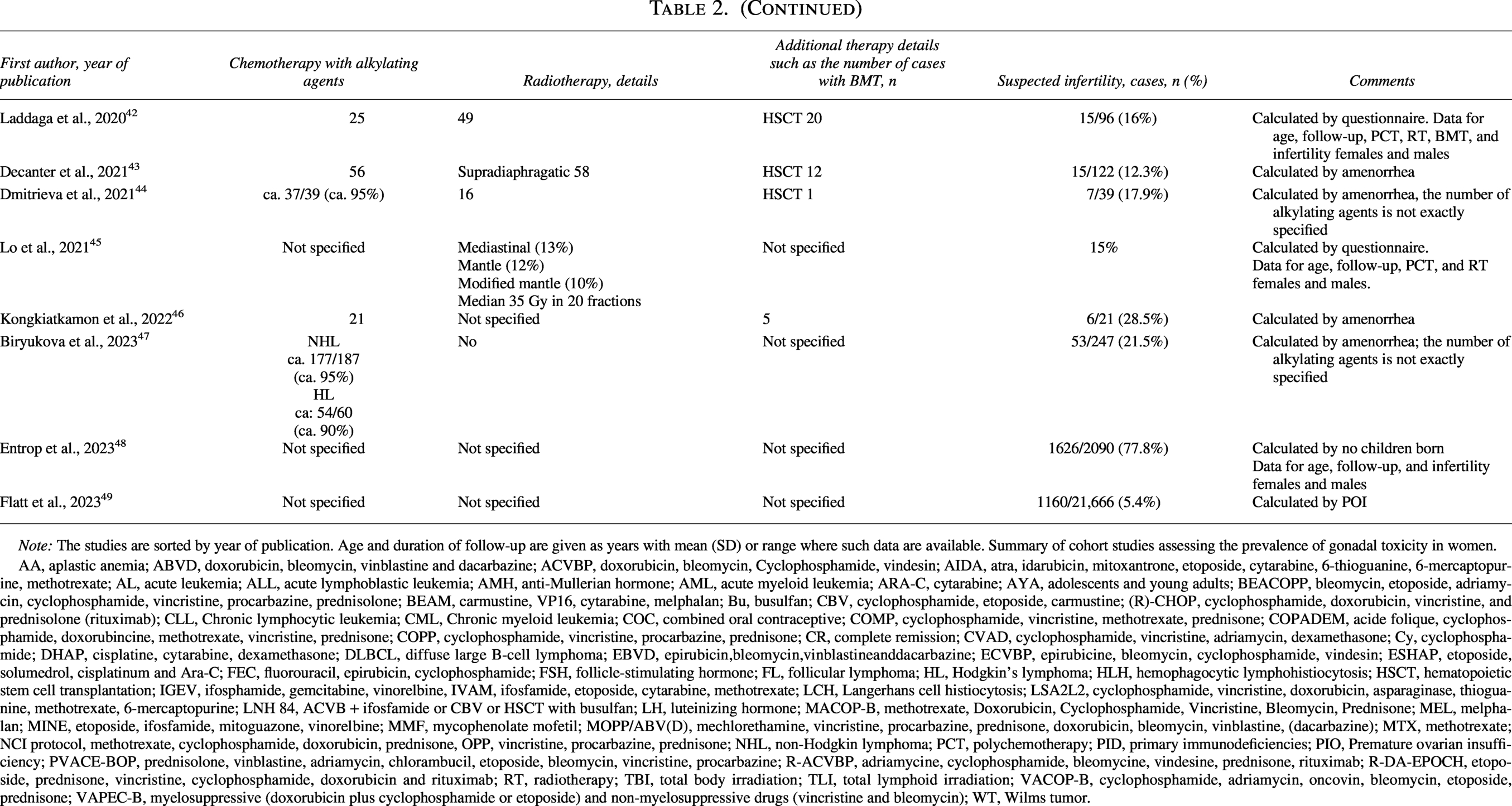
Note: The studies are sorted by year of publication. Age and duration of follow-up are given as years with mean (SD) or range where such data are available. Summary of cohort studies assessing the prevalence of gonadal toxicity in women.
AA, aplastic anemia; ABVD, doxorubicin, bleomycin, vinblastine and dacarbazine; ACVBP, doxorubicin, bleomycin, Cyclophosphamide, vindesin; AIDA, atra, idarubicin, mitoxantrone, etoposide, cytarabine, 6-thioguanine, 6-mercaptopurine, methotrexate; AL, acute leukemia; ALL, acute lymphoblastic leukemia; AMH, anti-Mullerian hormone; AML, acute myeloid leukemia; ARA-C, cytarabine; AYA, adolescents and young adults; BEACOPP, bleomycin, etoposide, adriamycin, cyclophosphamide, vincristine, procarbazine, prednisolone; BEAM, carmustine, VP16, cytarabine, melphalan; Bu, busulfan; CBV, cyclophosphamide, etoposide, carmustine; (R)-CHOP, cyclophosphamide, doxorubicin, vincristine, and prednisolone (rituximab); CLL, Chronic lymphocytic leukemia; CML, Chronic myeloid leukemia; COC, combined oral contraceptive; COMP, cyclophosphamide, vincristine, methotrexate, prednisone; COPADEM, acide folique, cyclophosphamide, doxorubincine, methotrexate, vincristine, prednisone; COPP, cyclophosphamide, vincristine, procarbazine, prednisone; CR, complete remission; CVAD, cyclophosphamide, vincristine, adriamycin, dexamethasone; Cy, cyclophosphamide; DHAP, cisplatine, cytarabine, dexamethasone; DLBCL, diffuse large B-cell lymphoma; EBVD, epirubicin,bleomycin,vinblastineanddacarbazine; ECVBP, epirubicine, bleomycin, cyclophosphamide, vindesin; ESHAP, etoposide, solumedrol, cisplatinum and Ara-C; FEC, fluorouracil, epirubicin, cyclophosphamide; FSH, follicle-stimulating hormone; FL, follicular lymphoma; HL, Hodgkin’s lymphoma; HLH, hemophagocytic lymphohistiocytosis; HSCT, hematopoietic stem cell transplantation; IGEV, ifosphamide, gemcitabine, vinorelbine, IVAM, ifosfamide, etoposide, cytarabine, methotrexate; LCH, Langerhans cell histiocytosis; LSA2L2, cyclophosphamide, vincristine, doxorubicin, asparaginase, thioguanine, methotrexate, 6-mercaptopurine; LNH 84, ACVB + ifosfamide or CBV or HSCT with busulfan; LH, luteinizing hormone; MACOP-B, methotrexate, Doxorubicin, Cyclophosphamide, Vincristine, Bleomycin, Prednisone; MEL, melphalan; MINE, etoposide, ifosfamide, mitoguazone, vinorelbine; MMF, mycophenolate mofetil; MOPP/ABV(D), mechlorethamine, vincristine, procarbazine, prednisone, doxorubicin, bleomycin, vinblastine, (dacarbazine); MTX, methotrexate; NCI protocol, methotrexate, cyclophosphamide, doxorubicin, prednisone, OPP, vincristine, procarbazine, prednisone; NHL, non-Hodgkin lymphoma; PCT, polychemotherapy; PID, primary immunodeficiencies; PIO, Premature ovarian insufficiency; PVACE-BOP, prednisolone, vinblastine, adriamycin, chlorambucil, etoposide, bleomycin, vincristine, procarbazine; R-ACVBP, adriamycine, cyclophosphamide, bleomycine, vindesine, prednisone, rituximab; R-DA-EPOCH, etoposide, prednisone, vincristine, cyclophosphamide, doxorubicin and rituximab; RT, radiotherapy; TBI, total body irradiation; TLI, total lymphoid irradiation; VACOP-B, cyclophosphamide, adriamycin, oncovin, bleomycin, etoposide, prednisone; VAPEC-B, myelosuppressive (doxorubicin plus cyclophosphamide or etoposide) and non-myelosuppressive drugs (vincristine and bleomycin); WT, Wilms tumor.
Characteristics of the included studies males
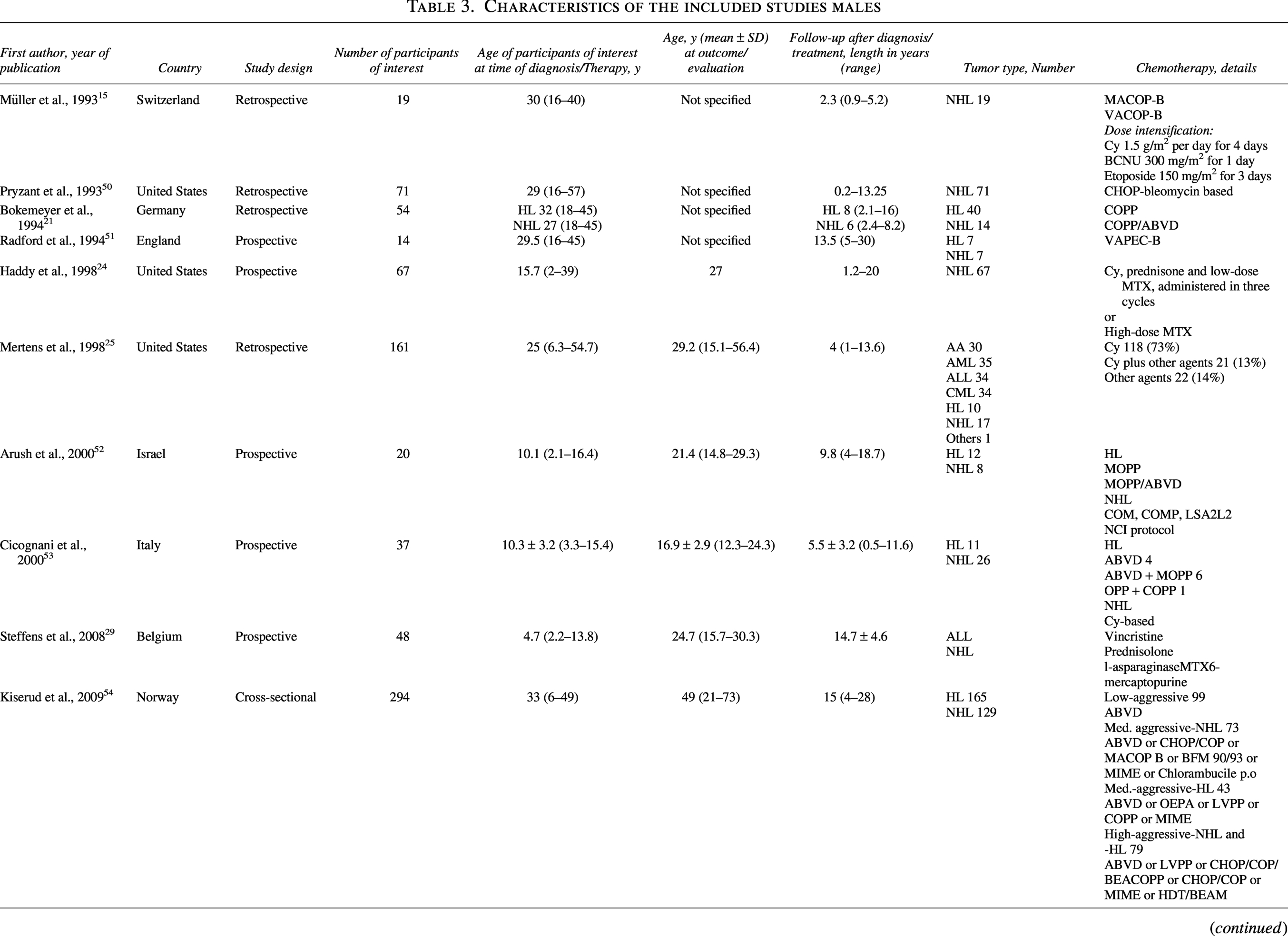
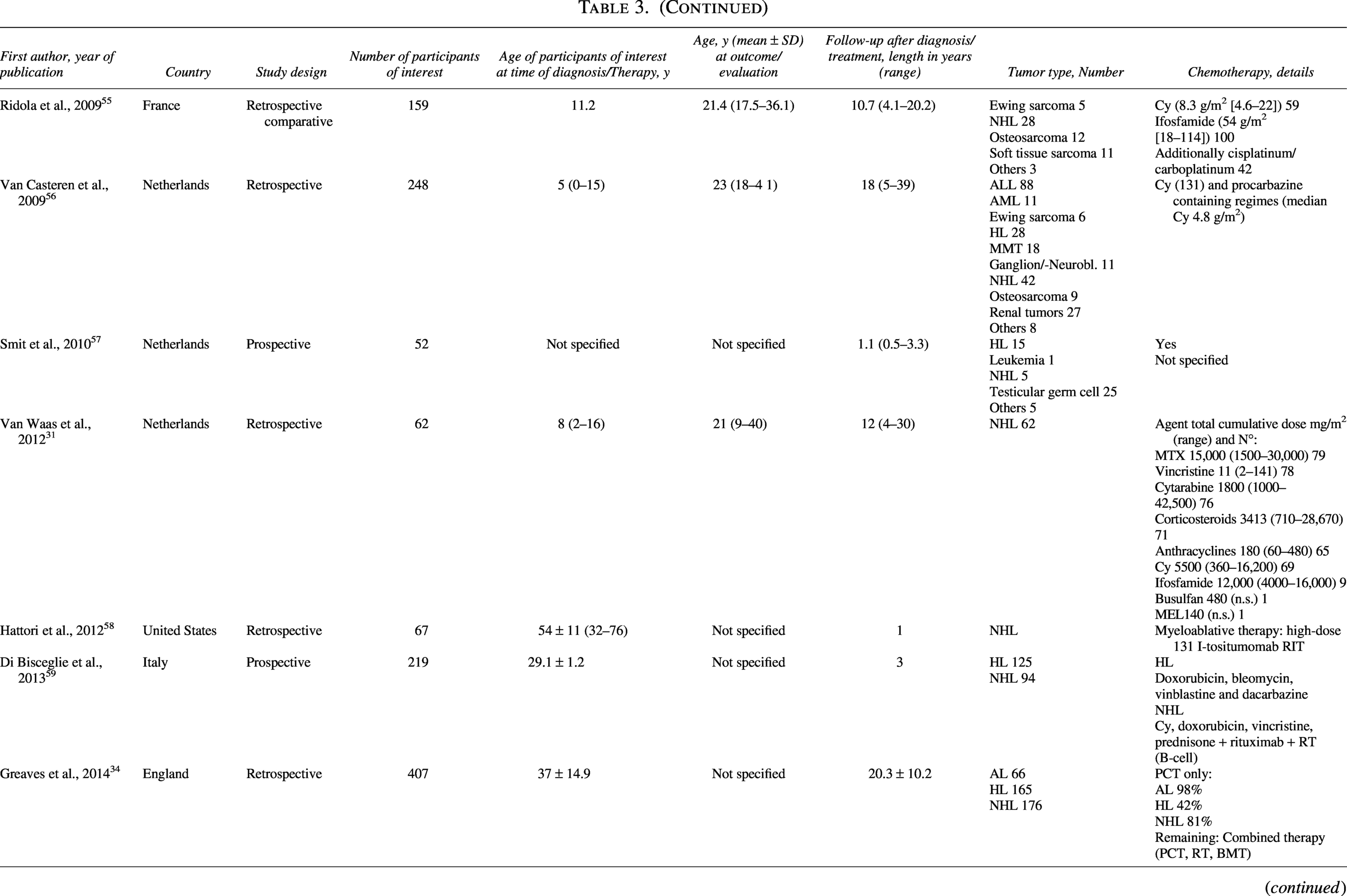
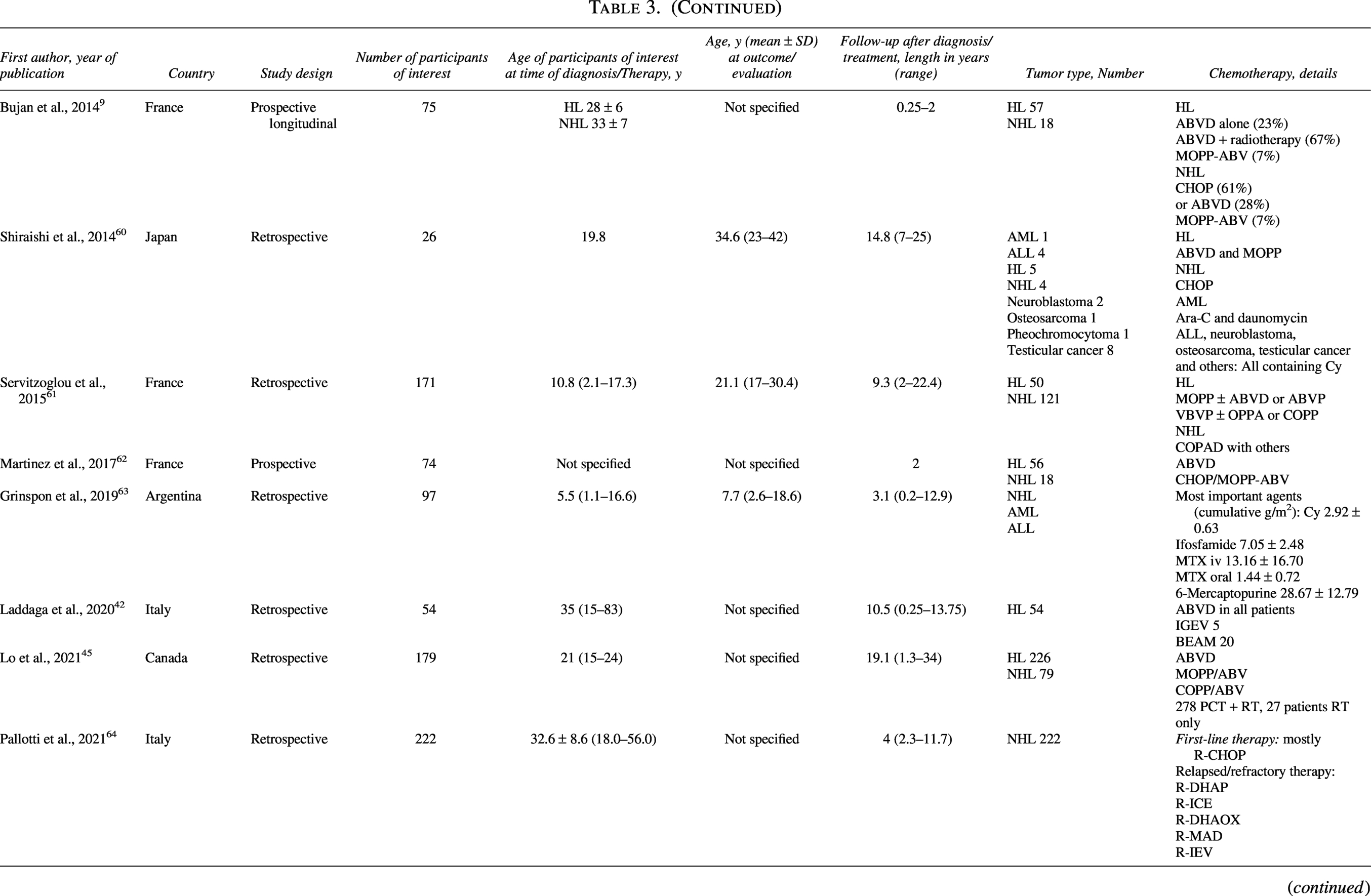
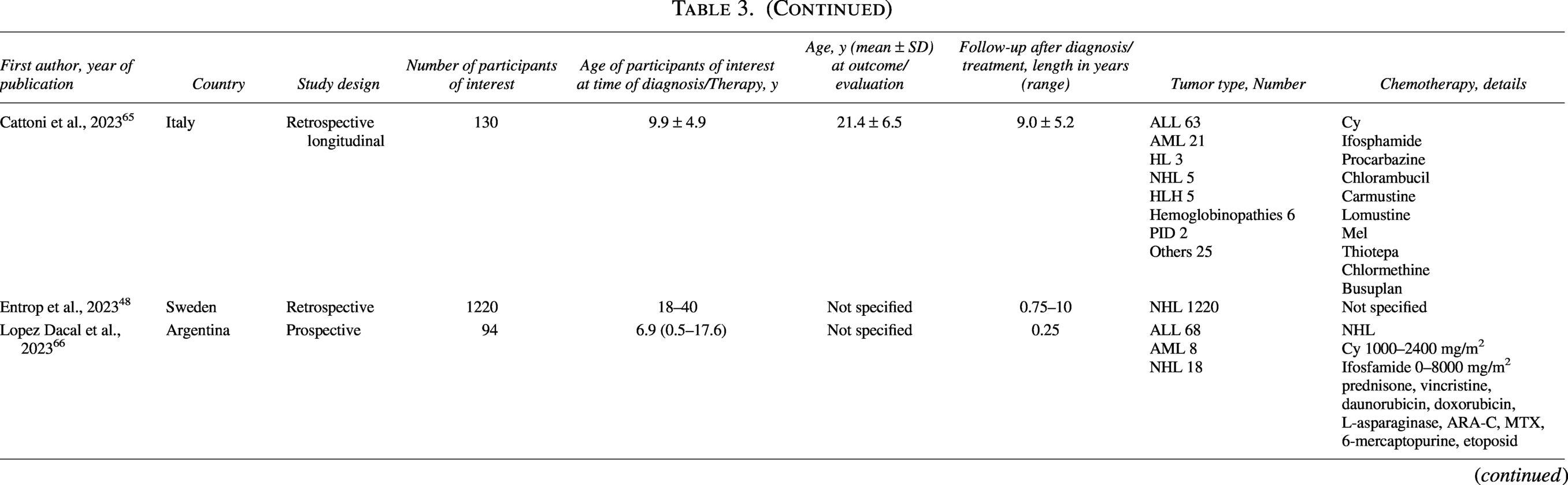
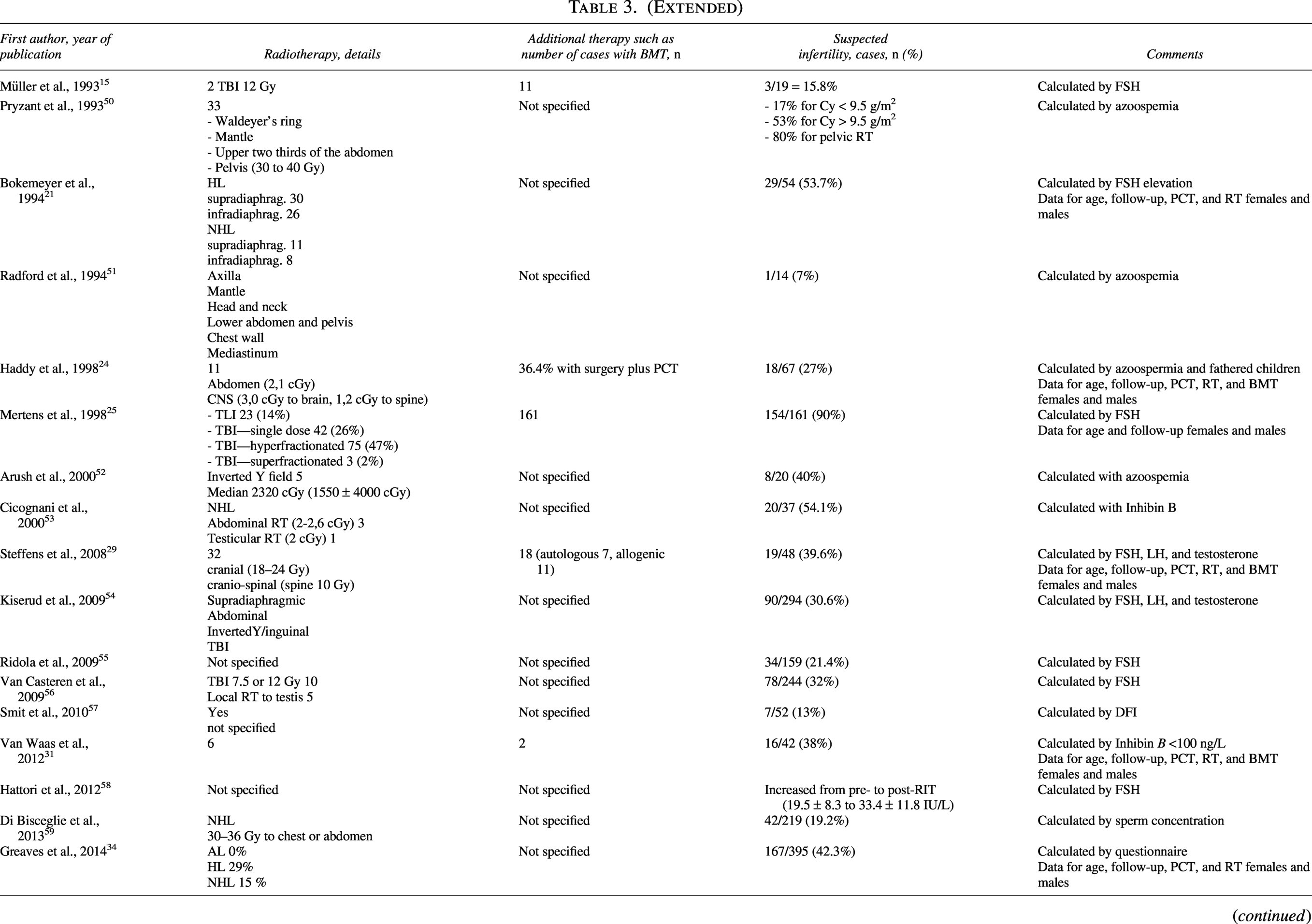
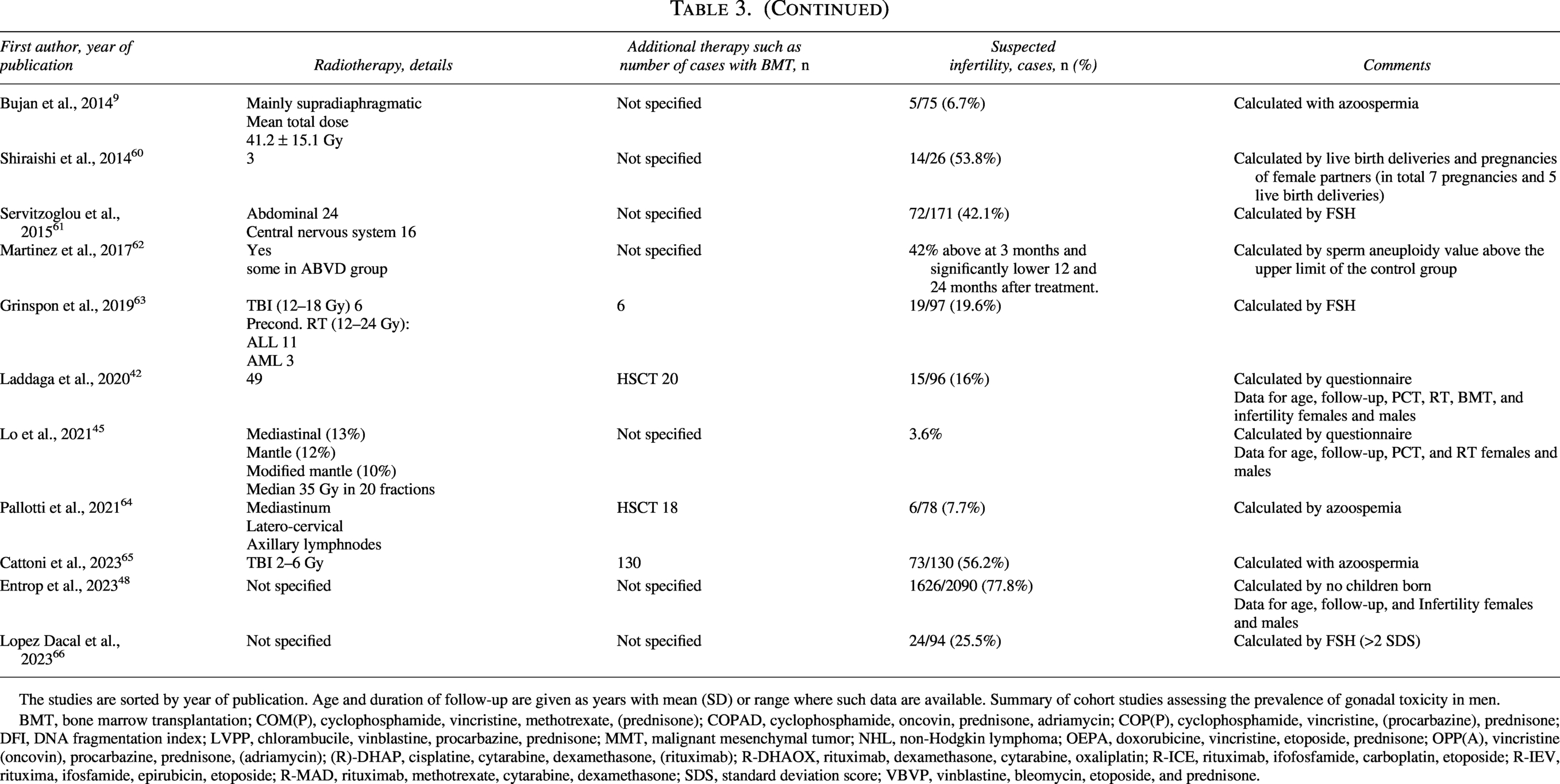
The studies are sorted by year of publication. Age and duration of follow-up are given as years with mean (SD) or range where such data are available. Summary of cohort studies assessing the prevalence of gonadal toxicity in men.
BMT, bone marrow transplantation; COM(P), cyclophosphamide, vincristine, methotrexate, (prednisone); COPAD, cyclophosphamide, oncovin, prednisone, adriamycin; COP(P), cyclophosphamide, vincristine, (procarbazine), prednisone; DFI, DNA fragmentation index; LVPP, chlorambucile, vinblastine, procarbazine, prednisone; MMT, malignant mesenchymal tumor; NHL, non-Hodgkin lymphoma; OEPA, doxorubicine, vincristine, etoposide, prednisone; OPP(A), vincristine (oncovin), procarbazine, prednisone, (adriamycin); (R)-DHAP, cisplatine, cytarabine, dexamethasone, (rituximab); R-DHAOX, rituximab, dexamethasone, cytarabine, oxaliplatin; R-ICE, rituximab, ifofosfamide, carboplatin, etoposide; R-IEV, rituxima, ifosfamide, epirubicin, etoposide; R-MAD, rituximab, methotrexate, cytarabine, dexamethasone; SDS, standard deviation score; VBVP, vinblastine, bleomycin, etoposide, and prednisone.
Quality assessment
The Newcastle–Ottawa Scale (NOS) 67 was used to assess the quality of individual studies. In the scoring of individual studies, the NOS considers three parameters: subject selection (0–4 stars), comparability (0–2 stars), and study outcome (0–3 stars). The scoring differentiates three distinct groups: good quality (3 or 4 stars in the selection domain AND 1 or 2 stars in the comparability domain AND 2 or 3 stars in the outcome/exposure domain), fair quality (2 stars in the selection domain AND 1 or 2 stars in the comparability domain AND 2 or 3 stars in the outcome/exposure domain), and poor quality (0 or 1 star in the selection domain OR 0 stars in the comparability domain OR 0 or 1 stars in the outcome/exposure domain). Supplementary Data S3 shows the terms used for scoring and the biases.
Data synthesis
The primary outcome of our systematic review was the prevalence of suspected infertility in women and men after different oncological therapies for NHL.
The prevalence was calculated by the number of patients who met the criteria for suspected infertility divided by the number of patients at risk of infertility, as provided by the individual studies. Statistical analyses for the pooled prevalence were done by the “metafor” function of the R software (R Core Team, Vienna, Austria, 2013), and heterogeneity was calculated using Cohen’s Q statistic and the I statistic. Random-effects models were used in the case of high heterogeneity. Studies with unspecified treatments or <10 patients were excluded for outcome assessment. However, they were included in the qualitative synthesis and tabular summaries of study characteristics (see Tables 2 and 3).
Results
Results of the systematic review
A total of 4602 records were identified for abstract screening. After screening of the abstracts and full texts, a total of 51 studies were included in the meta-analysis; 4551 studies did not meet the prespecified inclusion criteria and were excluded. In the systematic review, 58 articles were included (Supplementary Data S1).
Study characteristics
The characteristics of the 58 studies are shown in Tables 2 and 3. The included studies were retrospective (n = 37), prospective (n = 20), and cross-sectional (n = 1). The majority (n = 34) were rated as being of poor methodological quality, 13 were of good, and one of fair quality. This was mainly due to the lack of a comparison group or small sample sizes (Tables 2 and Table 3).
In females, a total of 25,197 patients diagnosed with NHL, were eligible for fertility analysis. Study sample sizes ranged from 11 to 21,666 patients. The included studies originated from various regions, Europe (n = 16), the United States (n = 3), Australia (n = 1), Russia (n = 2), Canada (n = 3), Asia (n = 1), Israel (n = 3), and Saudi Arabia (n = 1).
Study participants included prepubertal and postpubertal females, with a median age of 24.9 years (range 0.1–83) at the time of cancer diagnosis and 33.7 years (range 9–56) at the time of outcome evaluation. The follow-up periods of the studies were 8.7 years, with a range of 0.25–43.2 years.
In males, a total of 4341 patients diagnosed with NHL were eligible for fertility analysis. Study sample sizes ranged from 14 to 1220 patients. The included studies originated from various regions: Europe (n = 19), Asia (n = 1), the United States (n = 4), Canada (n = 1), Israel (n = 1), and South America (n = 2).
Study participants included prepubertal and postpubertal males, with a median age of 22 years (range 1.1–83) at the time of cancer diagnosis and 24.6 years (range 7.7–56.4) at the time of outcome evaluation. The follow-up periods of the studies were 8.8 years, with a range of 0.2534 years.
Treatment options included various types of chemotherapy and/or different doses and types of radiotherapy and/or stem cell therapy. The exact proportion of patients with each specific type of treatment could not be determined.
Results of the meta-analysis
A total of 51 studies were included in the meta-analysis. Seven studies that assessed fertility outcomes in fewer than 10 patients were excluded to provide clinically meaningful estimates (Supplementary Data S1).
Pooled overall prevalence of suspected infertility
Fifty studies were eligible for inclusion in the analysis of the overall prevalence of infertility. A total of 30,182 malignant NHL cases were included in this meta-analysis. The overall prevalence of suspected infertility was 27% (95% CI: 0.20–0.37) (Fig. 1). The heterogeneity test revealed significant heterogeneity among the studies (I2 = 99, p = 0). In females, the prevalence was 23% (95% CI: 0.14–0.35) (Fig. 2) and in males 35% (95% CI: 0.27–0.44) (Fig. 3). The heterogeneity test in females and males revealed significant heterogeneity among the studies (I2 = 99, p = 0 and I2 = 95, p < 0.01, respectively).
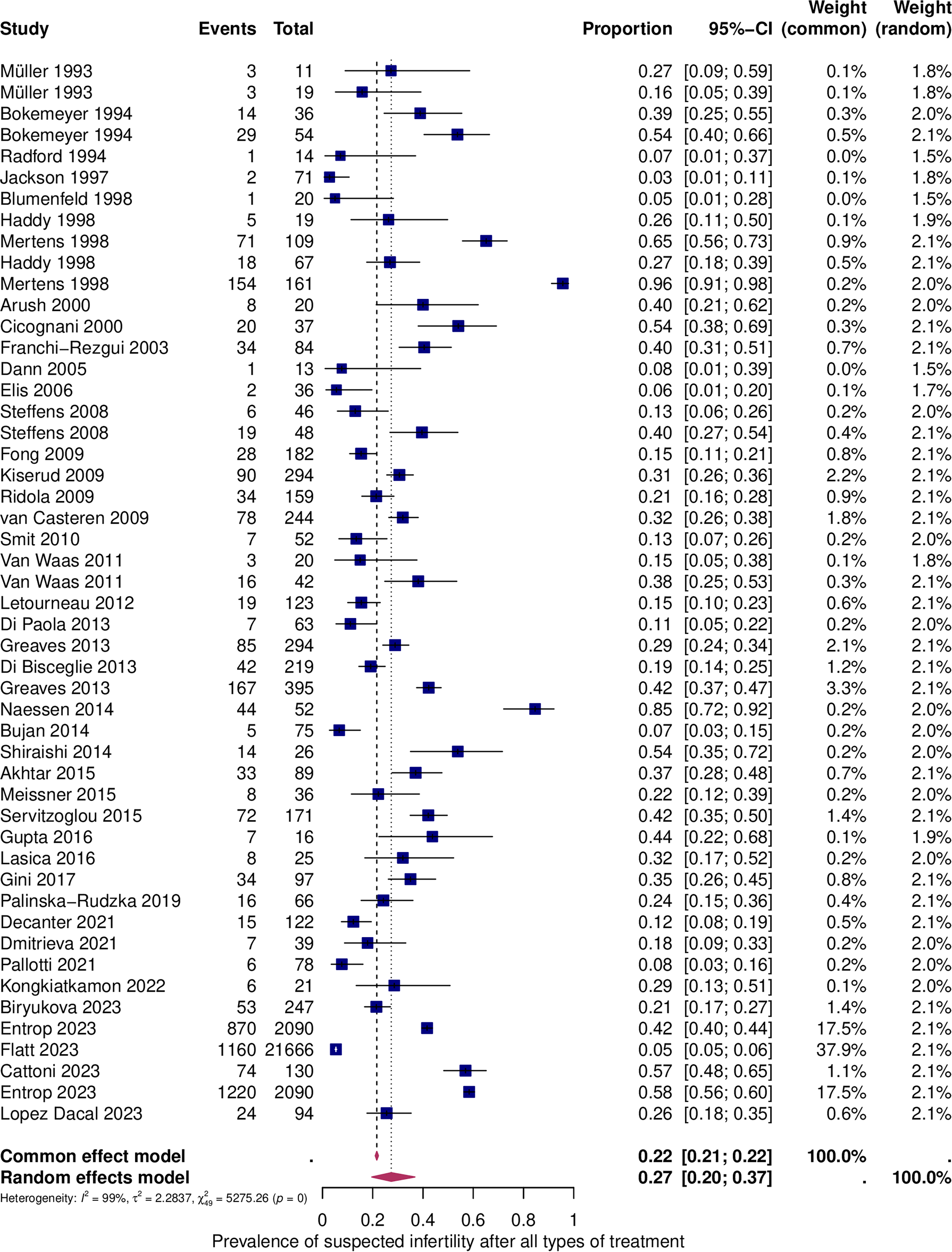
Prevalence of suspected infertility after all types of treatment. Forest plot of proportions and 95% confidence intervals (CIs) for studies evaluating the prevalence of suspected infertility after all types of treatment. Blue squares for each study indicate the proportion, the size of the boxes indicates the weight of the study, and the horizontal lines indicate the 95% CI. The data in bold and pink diamonds represent the pooled prevalence for post-treatment infertility and 95% CI. Overall estimates are shown in the fixed- and random-effect models.
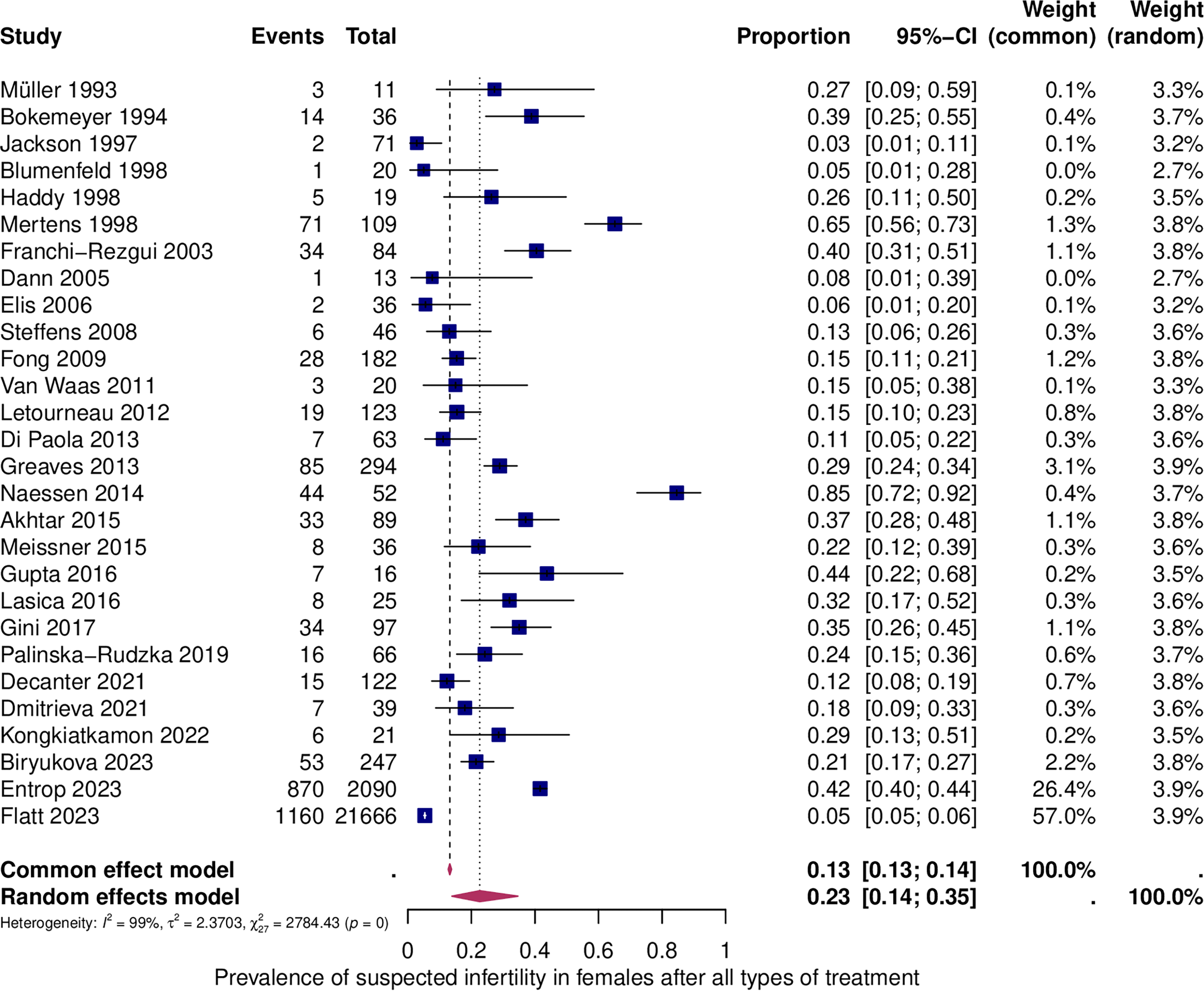
Prevalence of suspected infertility in females after all types of treatment. For details, see legend of Figure 1.
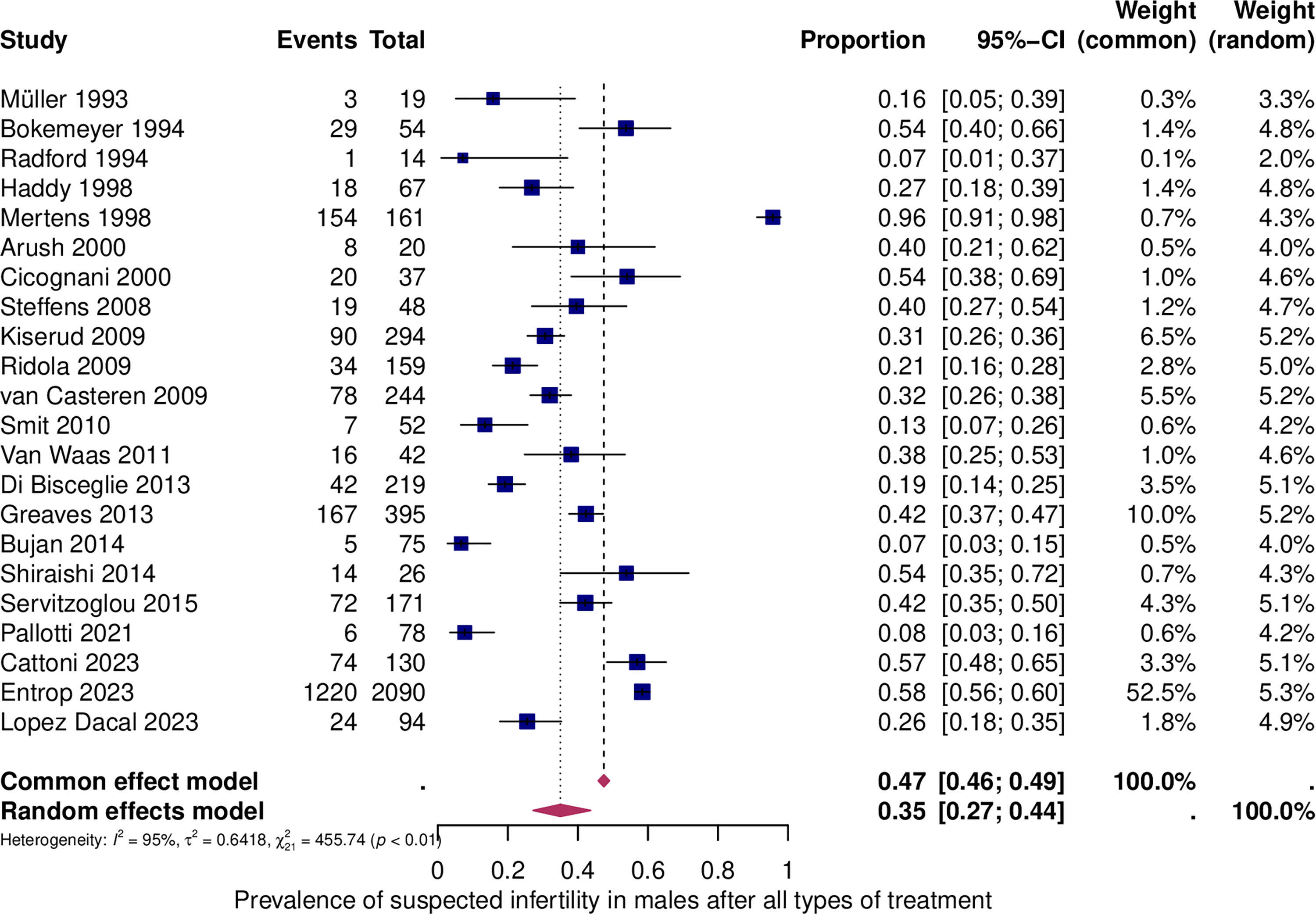
Prevalence of suspected infertility in males after all types of treatment. For details, see legend of Figure 1.
Subgroup analysis: Suspected infertility in patients after BMT
The prevalence of suspected infertility was found to be 43% in females treated with BMT (95% CI: 0.20–0.69) (Fig. 4). The prevalence in males, however, was found to be higher, reaching 57% (95% CI: 0.21–0.86) (Fig. 5). Significant heterogeneity was observed in both the female (I2 = 84%, p < 0.01) and male (I2 = 96%, p < 0.01) groups.
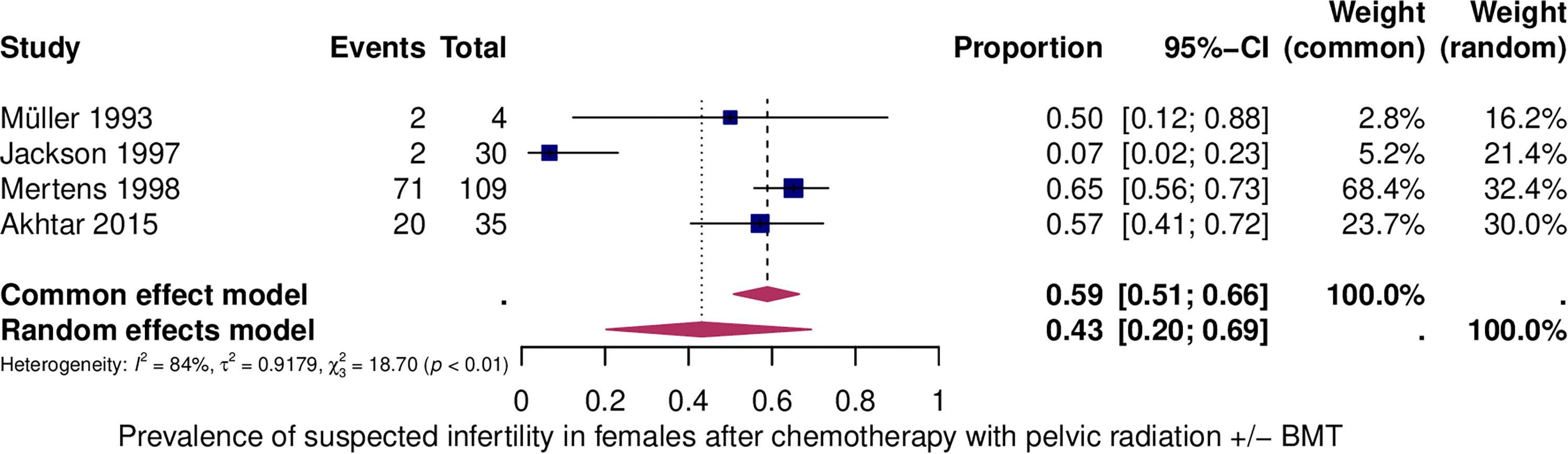
Prevalence of suspected infertility in females after bone marrow transplantation (BMT). For details, see legend of Figure 1.
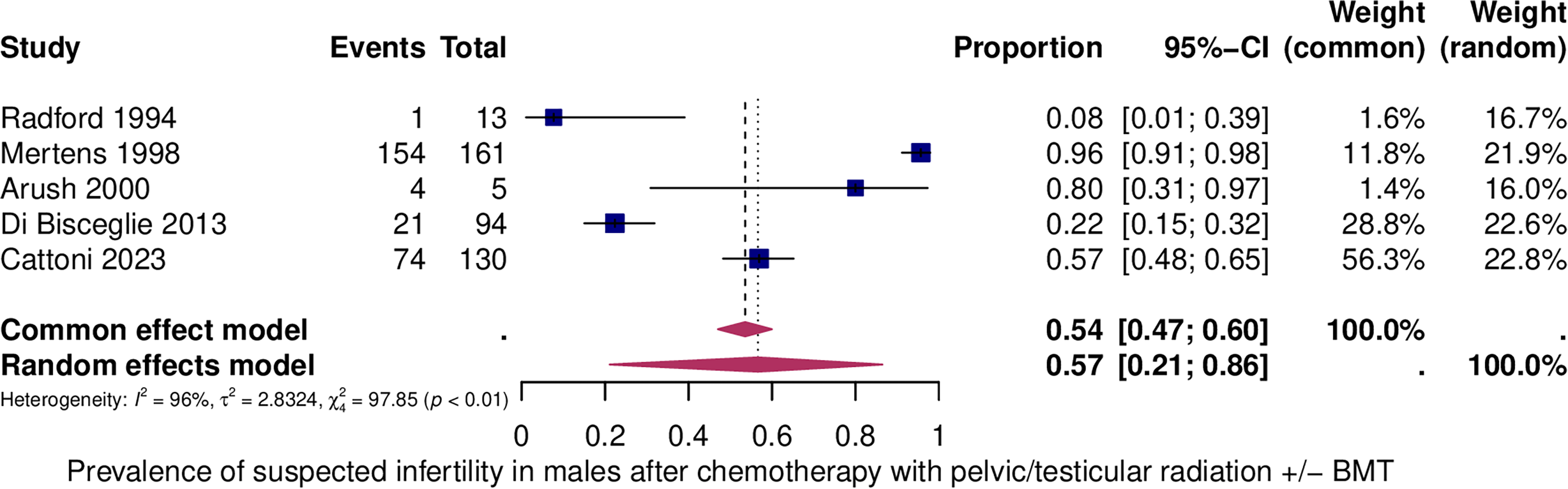
Prevalence of suspected infertility in males after bone marrow transplantation (BMT). For details, see legend of Figure 1.
Subgroup analysis: Suspected infertility in females after chemotherapy with alkylating agents
A total of 440 women were analyzed in order to evaluate the prevalence of suspected infertility in women who were treated with alkylating agents (Fig. 6). The prevalence was found to be 24% in females (95% CI: 0.17–0.34). Data heterogeneity was I2 = 71%, p < 0.01.
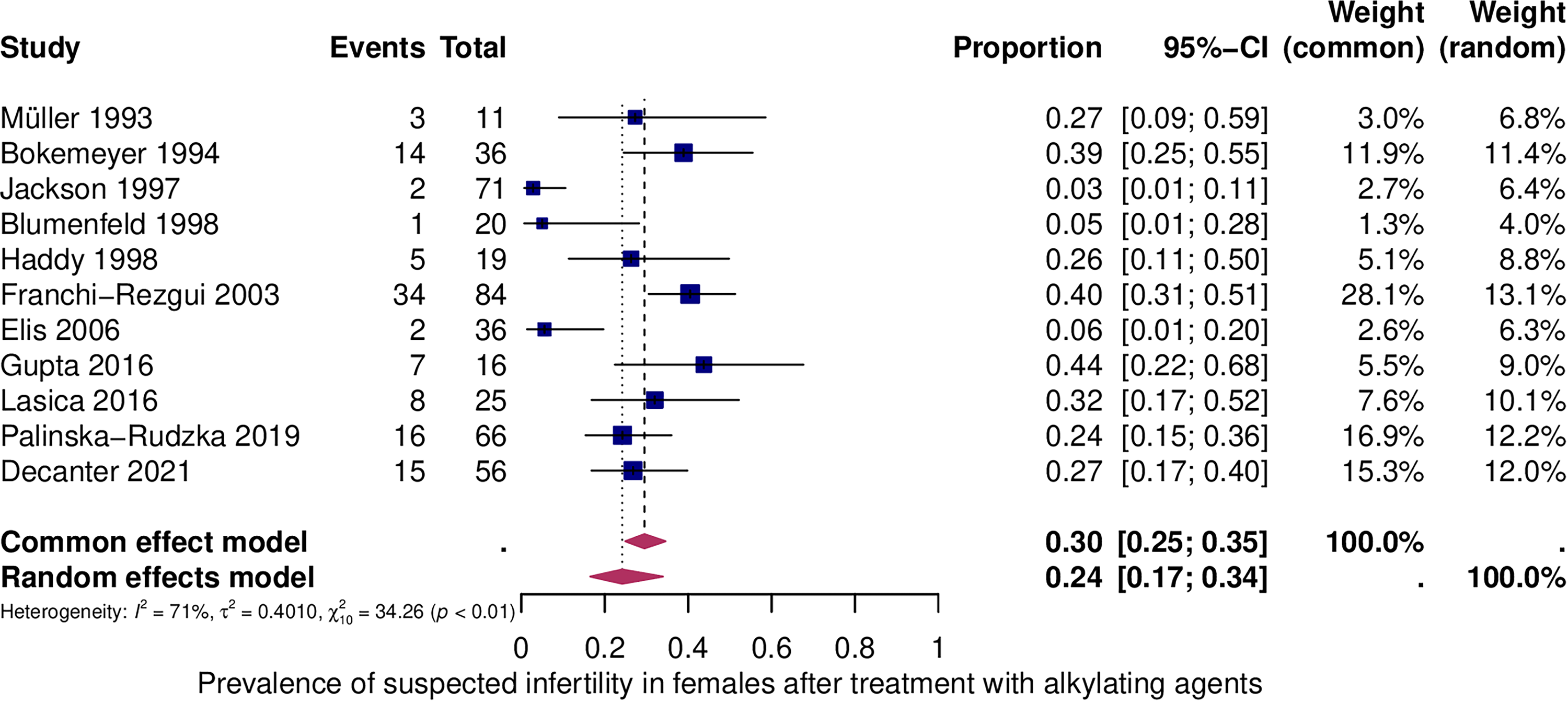
Prevalence of suspected infertility in females after treatment with alkylating agents. For details, see legend of Figure 1.
Discussion
Our study revealed the following important findings: First, the prevalence of suspected infertility of all patients is 27% (95% CI: 0.20–0.37). Second, the prevalence (with or without pelvic radiation ± BMT) is higher in men (35%; 95% CI: 0.27–0.44) compared with women (23%; 95% CI: 0.14–0.35). After chemotherapy with alkylating agents, the prevalence in women is 24% (95% CI: 0.17–0.34). Third, the prevalence of suspected infertility is after chemotherapy with pelvic/testicular radiation ± BMT, with 57% highest in men (95% CI: 0.21–0.86), compared with 43% women (95% CI: 0.20–0.69). Fourth, the published data are very heterogeneous, either due to the variety of cancer therapies performed or the differences in fertility evaluation methods. This makes comparing studies difficult.
Assessing gonadal toxicity is crucial for implementing fertility-protective measures in patients at high risk of infertility.
In men, the strategy for fertility preservation is simple, as sperm can be preserved easily and without any relevant time expenditure.
The procedures in women are more complex. Ovarian stimulation, which takes 2 weeks and oocyte cryopreservation, rather than ovarian tissue cryopreservation, is generally advised in NHL, due to the risk of malignant cells in ovarian tissue. However, in the case of NHL, the time available before the start of chemotherapy or the patient’s health status may make ovarian stimulation and oocyte freezing impractical. In these cases, ovarian tissue can be preserved in an experimental setting. Nonetheless, there is a relevant risk of contamination of the ovaries with lymphoma cells, particularly in cases of high-grade NHL. For this reason, patients must be informed before ovarian tissue freezing that transplantation of the tissue cannot be guaranteed, as this is only possible if lymphoma cells can be excluded by immunhistochemical and molecular techniques prior to transplantation.
In the rare case of NHL in children and adolescents, the decision for or against fertility-preservation measures is always an individual case decision based on the kind of oncological treatment and the wishes of the patients and their parents.
GnRH analogs can be administered to women with NHL to prevent uterine bleeding. However, there is insufficient data in NHL on its effect in protecting ovarian function. Add-back therapy involving low-dose estrogen and progestin preparations should be considered to alleviate menopausal symptoms, reduce bone mass loss, and prevent bleeding.
Although recovery from ovarian insufficiency has been documented, 68 the prevalence of POI following oncological treatment is increased. A prospective study has shown that the presence of regular menstrual cycles following cancer treatment does not necessarily indicate normal fertility, and that POI may still occur. 69 The higher the age of the patient, the higher the risk of POI, particularly in women >30 years.70,71 The type of chemotherapy, the agents used, and the doses are also relevant factors for the risk of developing POI.
However, the risk of POI does not only increase after high-dose gonadotoxic treatment. It was demonstrated in females undergoing low-dose gonadotoxic regimens for hematological malignancies that low-dose gonadotoxic therapies can also exhibit impairment of ovarian reserve when evaluated a few years after the end of therapy. 33
To evaluate ovarian reserve, anti-Mullerian hormone (AMH) has been shown to be the most sensitive and practical hormone parameter for detecting changes in ovarian reserve, compared with FSH or inhibin B,33,72 even though pregnancies have been reported in women with low AMH values after cancer.33,73
While the risk of infertility following cancer treatment is substantially increased, the use of cryopreserved gametes or embryos after remission is surprisingly low. According to a recent study, the utilization rate for embryos varied between 9% and 22.4%, for oocytes between 3.1% and 8.7%, for cryopreserved ovarian tissue between 6.9% and 30.3%, and for cryopreserved sperm between 2.6% and 21.5%. 74 Despite these low utilization rates, it is crucial to counsel patients on the option to undergo fertility preservation.
Another important issue concerning family planning after gonadotoxic treatments is whether cancer therapies impose a higher risk of birth defects in children born after cancer therapies. Two studies of patients receiving lymphoma treatment addressed this question and found no increase in malformations,22,75 even though sperm DNA damage was observed after cytotoxic therapy. 76 Although these results are reassuring, the number of cases studied is low, and more follow-up studies are needed.
One study indirectly addressed this issue in males by investigating the DNA fragmentation index (DFI) in NHL patients. They found that sperm DNA integrity is compromised even before oncological treatment and is damaged further after treatment, particularly after radiotherapy. 57 A high DFI index is known to compromise fertility. However, it is still unclear whether high DFIs could have a negative impact on the health of newborns. 57 It is therefore important to address these unknown risks and to consider, in assisted reproductive technology treatments, the use of sperm that has been cryopreserved before cancer therapy.
A large, prospective, multicenter study of sperm parameters in patients with NHL and Hodgkin lymphoma (HL) also showed that sperm aneuploidy is higher in these patients, and that sperm quality is lower even before oncological treatment. 62 The exact mechanism by which sperm chromosomes are affected in patients with HL and NHL is unknown. An interesting finding of this prospective study is that, 12 months after treatment with ABVD ± radiotherapy, aneuploidy rates decreased and fell even below pre-treatment levels. This is in contrast to other therapies, where aneuploidy rates remained elevated for up to 2 years after treatment. 62
Another factor that could influence a woman’s decision to become pregnant after gonadotoxic treatment is the increased risk of prenatal and obstetrical complications such as premature delivery, which can lead to severe health issues for the newborn. An increased risk of miscarriage, intrauterine growth restriction, stillbirth, abnormal placentation, and uterine rupture has also been reported, especially after total body irradiation.77–81
The heterogeneity of data in our study required an extended interpretation of the diagnosis “infertility.” In males, evaluation of the sperm parameters (i.e., azoospermia, sperm aneuploidy tests, fragmentation index) was performed after treatment in eight studies, hormonal values (FSH, luteinizing hormone, inhibin B) were assessed in 13 studies and in 6 studies, evaluation of infertility was based on questionnaires/pregnancies of the spouses. In females, the diagnosis of “infertility” was defined based on the presence of oligomenorrhea/amenorrhea in 15 studies, on the presence of elevated levels of FSH and/or undetectable levels of AMH in two studies, on both in four studies, on the presence of premature ovarian failure in women in one study, and on questionnaires/pregnancies in eight studies. The use of different parameters allowed us to define suspected but not definite infertility.
Although we strictly followed the recommendations to produce high-quality evidence summaries, there are some limitations to our study: First, the heterogeneity of the included studies, due to treatment variations and the diverse characteristics of the study populations with wide age ranges, is high in all groups: in males with all types of treatment, in females with alkylating agents, and in females and males after chemotherapy with pelvic/testicular radiation ± BMT. This hampers subgroup analyses that depend, for example, on pubertal status and a more granular view on fertility counseling before an oncological treatment. For this initial limitation, the heterogeneity of the included studies is at the same time also a very important finding because it highlights this dilemma precisely. It serves as a basis for future studies and underscores the urgent need for more prospective, large-scale studies to obtain more specific data. The FertiTOX project (www.fertitox.com) aims to provide such specific data. 17 A series of systematic reviews has been published to provide data on gonadal toxicity after different cancers and treatments.2–8
A second limitation is that most of the included studies were based on retrospective or registry data, lacking precise information on treatment protocols and dosage of chemotherapy, as well as on radiotherapy doses and additional therapy details. This precluded the possibility of performing a subanalysis in order to assess the intensity of the therapy. Third, the outcome parameters of the studies in males and females were not homogeneous; some lacked reliable information on proven infertility after gonadotoxic treatment. Later, yet importantly, some of the studies assessed schemes that are currently no longer used. This might overestimate the prevalence of infertility.
In conclusion, the results of this review and meta-analysis support the clinical need for fertility counseling and preservation in women and men undergoing oncologic treatment for NHL. However, due to the heterogeneity of previously published studies, there is an urgent need for further prospective studies that specifically address the individual impact of the broad spectrum of treatments for NHL and the new treatment agents.
Authors’ Contributions
D.W.: Design of the systematic Review, Selection of the studies, Article writing. E.S.: Selection of the studies. A.V.: Design of the systematic Review, Selection of the studies. J.P.: Data analysis. T.K.: Preparation of the search strategy for the literature search. U.N.: Oncological advice. M.v.W.: Design of the systematic Review, Article revision. All authors approve publication of the article.
Ethical Considerations
No ethical approval is required for a systematic review and meta-analysis.
Consent to Participate
No consent to participate is required for a systematic review and meta-analysis.
Consent for Publication
All authors approve publication of the article.
Data Availability Statement
All the data utilized in the study are publicly available and/or contained within the article or Supplementary Material.
Study Registration
This systematic review is registered with the PROSPERO under CRD42024511940.
Footnotes
Acknowledgment
The authors would like to thank the
Author Disclosure Statement
The authors have no relevant financial or non-financial interests to disclose.
Funding Information
This work was supported by the public university and by a Grant of the Swiss Cancer League (grant number: KLS-5650-08-2022).
Supplemental Material
Supplemental Material
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.