
Abstract
Background:
Youth patient organizations have taken action to address the specific needs of adolescents and young adults (AYAs), and the third National Cancer Control Plan has made this a requirement. This study presents the center’s rehabilitation program.
Patients and Methods:
Following initial treatment, patients aged 18–25 were seen annually for 5 years by a multidisciplinary team. Quality of life using the World health organization quality of life (WHOQOL)-BREF and anxiety and depression using the Hospital Anxiety and Depression Scale (HADS) were assessed. The sexologist developed his own scale. The Patients’ Global Impression of Change scale (P-GIC) was used to evaluate patients’ feedback about the program.
Results:
Forty-five patients were included. The main reason for being unable to work effectively was cancer and/or its treatment for 20 patients out of 23 in activity (87%). Ten patients (22.2%) reported financial difficulties, and 14 patients (31.1%) received support from a social worker. Regarding sexological accompaniment, only 17 patients could be evaluated; most of these patients (N = 11, 65%) required a sexologist appointment more than a year after the end of their treatment. Regarding psychological support, 44 patients completed the WHOQOL-BREF questionnaire. No particular trend was observed over time. A total of 45 patients completed the HADS. Symptoms of depression may decrease over time, from the end of the treatment to up to 5 years later, whereas anxiety symptoms may not. Of the 48 responses received for the P-GIC satisfaction survey, 43 (89%) indicated satisfaction.
Conclusion:
The AYA team conducts systematic needs assessment and works to address these needs.
Highlights
The adolescent and young adult (AYA) team must be built based on the care ecosystem to optimize management; there is certainly not just one model. Multiple needs arise at the time of cancer diagnosis and may persist or emerge beyond the treatment period. Identifying these needs early on makes it possible to anticipate them and address them. This rehabilitation program has been widely accepted by patients and would not be possible without the AYA team and its financial support.
Introduction
At the turn of the 21st century, data from the United States and Europe revealed that cancer was one of the leading causes of death among adolescent and young adult (AYA) patients, with lower survival rates than in children.1–3 In France, 2000 new cases are reported each year in AYAs aged 15–25 years, 60% of whom are aged 20–25.4,5 This incidence rate is lower than that reported in the United States, where 100,000 new cases are reported each year using a broader definition of the AYA population (aged 15–39 years), ∼18% of whom are aged 15–25 years. For this latter population, there is a ratio of two solid cancers to one hematological cancer.2,6
The concept of dedicated care for AYA patients is relatively new in cancer management but is now widely accepted in both the United States and Europe. This holistic approach does not only focus on the need for longer follow-up of cancer survivors due to the well-established late effects of treatment and secondary malignancies.7–10 These care pathways are still often in development, and it should be noted that AYAs were involved in developing the care program from the outset, working alongside health care professionals. Since the Ligue organized the 1998 States General of Patients in France, young patients’ associations have been advocating for the specific needs of AYAs with cancer to be taken into account and for a coordinated care system to be established, similar to those in the United States and other countries.11–13 In this context, the French Cancer Institute (INCa) developed the “Supporting the emergence of integrated and innovative projects for young people with cancer” project as part of the Third Cancer Plan (2009–2013). The Groupe Onco-hématologie Adolescents Jeunes Adultes (Go-AJA), a French national collaborative group comprising 27 dedicated teams across the country, has now been operating for 13 years.4,14 It was agreed that health care establishments should set up a team of health care professionals trained in managing AYA patients, to take into account all the specific dimensions relevant to AYAs to address their personal concerns. These issues include identity development, body changes, self-perception, friendships and relationships, sexuality, financial independence, the impact of the disease and treatment on fertility, immediate and long-term side effects, and continuation of education and employment.
The Institut Cancérologique de l’Ouest (ICO Saint-Herblain) Comprehensive Cancer Center (CCC) has been involved in this project since 2012 as one of eight experimental AYA teams, 14 with a dedicated team including a nurse, a social worker, a sexologist, a psychologist, and an oncologist who oversees patient care during and after cancer treatment.
The AYA follow-up program has evolved over time. Initially, the team was available to address the needs of AYAs. Subsequently, it became a mandatory component of patient care at the start of treatment and every year for 5 years after the end of treatment. The primary objective of the prospective SAJAC study was to assess the feasibility of a coordinated multidisciplinary consultation.
Patients and Methods
Methods
Patients aged 18–25 years at the time of their cancer diagnosis were included in the study. The ICO is a CCC that treats patients with solid tumors from the age of 18 years. Therefore, patients aged 15–17, as well as those with hematological diseases, were not included. The SAJAC program is a systematic short follow-up program over 5 years after the end of the initial treatment. At the end of the initial treatment, the SAJAC program was offered to every new AYA patient at the discretion of the treating oncologist. If the AYA patient agreed to participate, the secretary assigned to the “AYA care pathways” scheduled an appointment with the dedicated AYA team. Ideally, this consultation was intended to allow the patient to meet with the AYA nurse, psychologist, sexologist, and oncologist. When this was not possible due to scheduling conflicts involving either the patient or AYA team members, multiple appointments were nevertheless scheduled within the same time frame if a single appointment could not be arranged on the same day. These consultations were conducted separately from the disease-specific follow-up visits and focused on evaluating patients’ supportive care needs. All patients were informed to ensure that they were not opposed to the use of their data for research purposes. A medical questionnaire covering the disease and treatment side effects as well as identifying needs requiring intervention by professionals other than the AYA team was distributed by the oncologist, who collected the patients’ responses.
Another questionnaire was administered during the appointment with the AYA nurse as part of a shared educational assessment. This questionnaire focused on social life, employment or school status, financial situation, treatment-related side effects, sexual health, and fertility, to identify needs for intervention by a social worker, psychologist, sexologist, or fertility specialist.
Anxiety and depression were assessed at the end of treatment and annually for 5 years using the Hospital Anxiety and Depression Scale. 15 The scale consists of 14 items (seven anxiety-related items and seven depression-related items), to which patients were asked to reply on a 4-point Likert scale. Anxiety and depression scores range from 0 (no symptoms) to 21 (high number of symptoms). A score between 0 and 7 means no anxiety or depression; a score between 8 and 10 means a moderate level of anxiety or depression; and a score ≥11 means severe anxiety or depression. Quality of life (QoL) was measured at the end of treatment and annually for 5 years using the World health organization quality of life (WHOQOL)-BREF questionnaire. 16 This questionnaire consists of 26 items: seven items assess physical health, six items are used for psychological health, three items explore social relationships, eight items investigate the environment, and two additional items examine the overall satisfaction with life and personal well-being. Each item is rated on a scale from 1 to 5. Scores for the domains “physical health,” “psychological health,” “social relationships,” and “environment” domains range from 0 (low health related quality of life [HRQoL]) to 100 (high HRQoL), whereas scores for “overall perception of QoL” and “overall perception of health” range from 0 (low HRQoL) to 5 (high HRQoL).
Because the Usual Female Sexual Function Index (FSFI) and the Male Sexual Health Questionnaire (MSHQ) questionnaires used in the sexologist’s daily practice were not appropriate for this AYA rehabilitation program, the sexologist at our CCC developed their own questionnaire (Supplementary Appendix SA1). To evaluate patient feedback about this program, the Patients’ Global Impression of Change scale (P-GIC) was administered annually.
Health authority approval
In accordance with Deliberation No. 2018-155 of May 3, 2018, approving a reference methodology for the processing of personal data used in the context of research, not involving the human person, studies, and evaluations in the health field, the ICO has undertaken to adhere to reference methodology MR-004 (number 2021-007) of the French data protection authority (CNIL in French). The data were duly recorded in the data processing register, accessible under the following number, 333.
Objectives
The primary objective of the prospective SAJAC study was to assess the feasibility of a coordinated multidisciplinary consultation program, defined as the proportion of patients with more than two multidisciplinary consultations over the 5-year follow-up period. The secondary objectives were to describe treatment-related side effects, to assess the feasibility of multidisciplinary consultations, through the follow-up of patients, with the number of professionals seen per visit in the short term (0–5 years), to describe the posttreatment needs of AYAs, and to evaluate patient-reported satisfaction (P-GIC). This analysis includes baseline characteristics and follow-up data available through the end of 2023. Because follow-up remains incomplete for more than 80% of patients, the primary objective was not assessed in the present analysis and will be reported once the study has been completed.
Statistical analysis
Descriptive statistics were used to summarize patient characteristics, psychological outcomes, and follow-up data. Continuous variables are presented as medians with ranges or means with standard deviations, as appropriate. Categorical variables are expressed as frequencies and percentages. No inferential tests were performed because of the limited sample size and heterogeneity of follow-up intervals. To describe patients’ sociodemographic and clinical characteristics, we used baseline data; when an entire questionnaire was missing at baseline, data from the subsequent consultation were used instead, without imputation of individual missing items. All analyses were carried out using SAS software version 9.4 (SAS Institute Inc., Cary, NC, USA) and R (version 4.1.2).
Results
Study population and follow-up
In total, 45 patients were included in the SAJAC program, including 16 who were enrolled after the end-of-treatment visit. At the end of 2023, when the database was locked for this analysis, five patients had completed the full follow-up (Fig. 4).
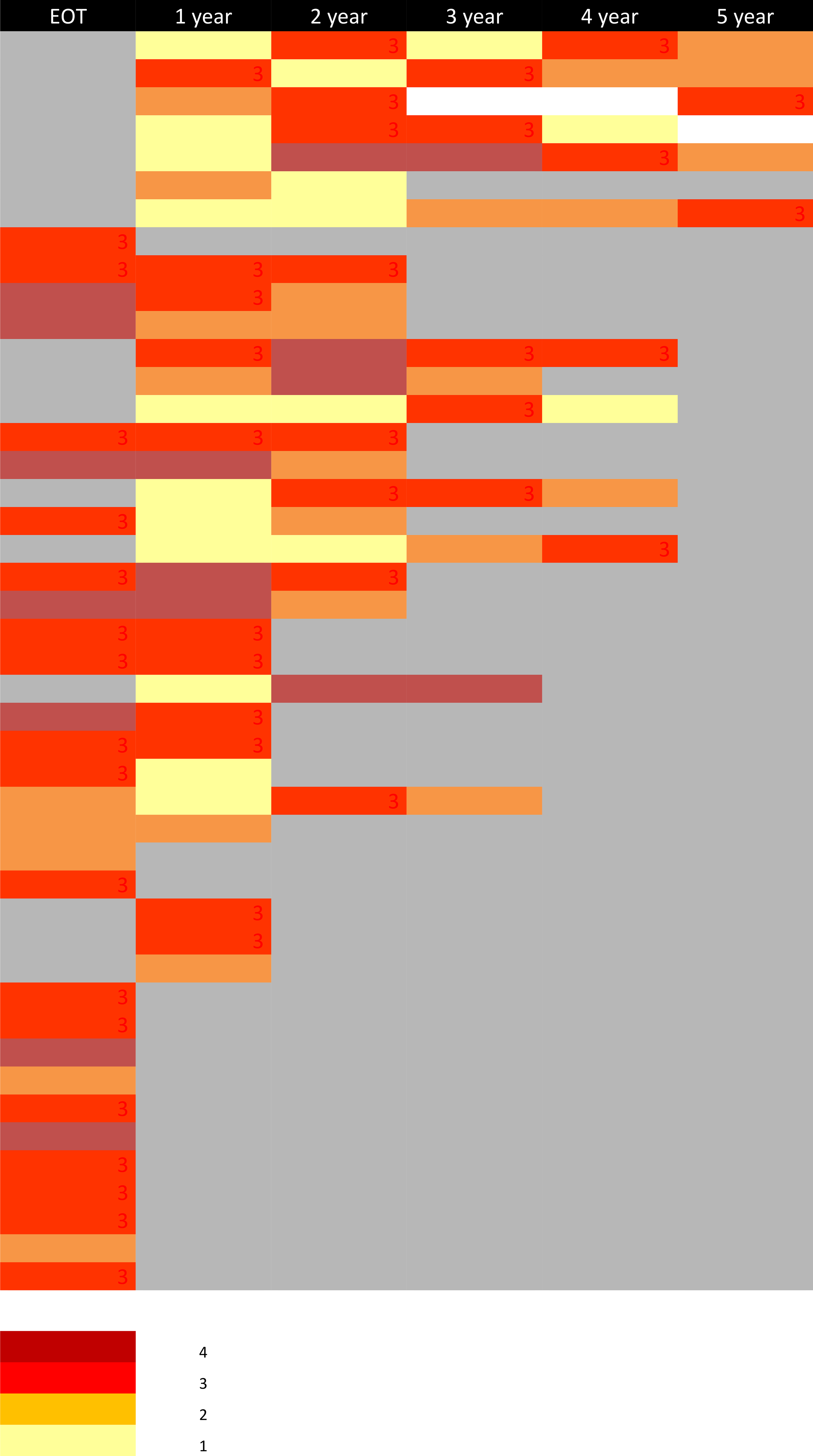
Follow-up with number of health care professionals for a shared consultation.
Patient characteristics
Characteristics of cancer, treatment, and side effects
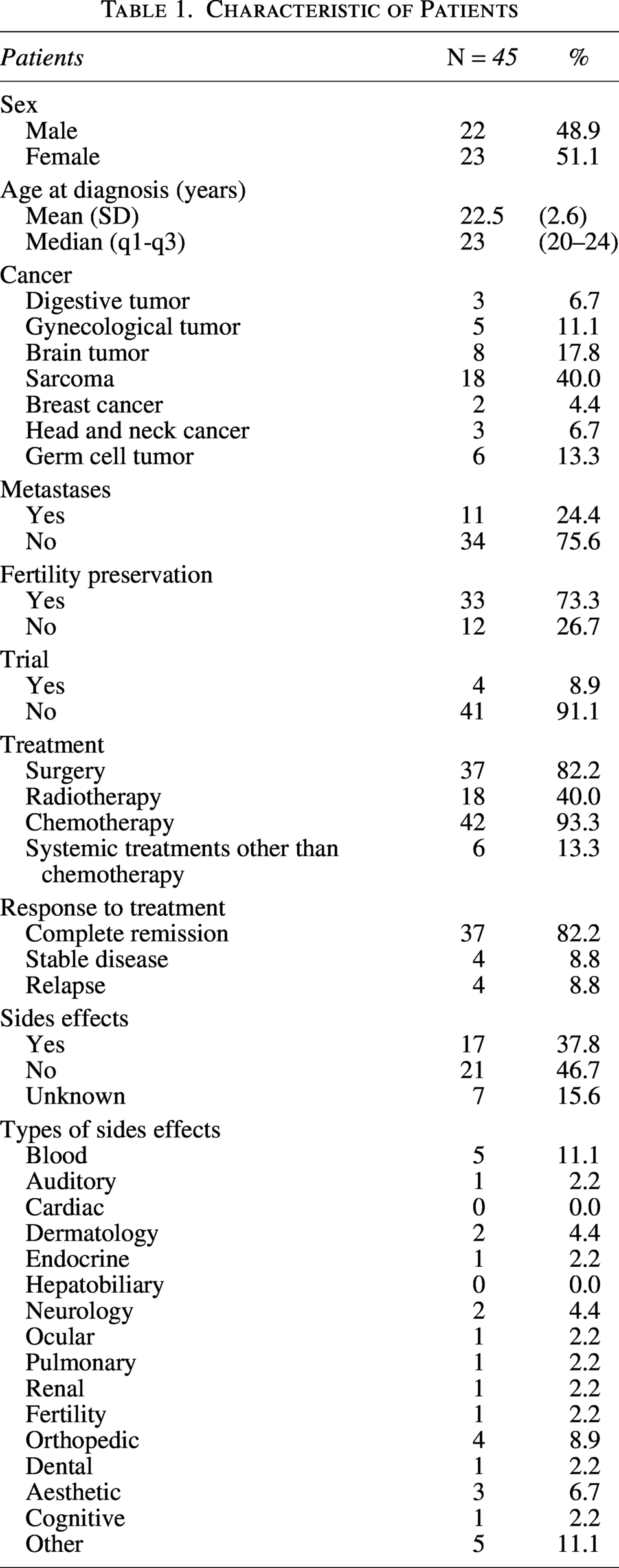
Between April 2017 and December 2023, a total of 45 patients were included in this study, of whom 23 were women, with a median age of 23 years (range: 20–24). At the time of enrollment, 34 patients (71%) were in complete remission after the first-line treatment, 3 patients (6.6%) were in complete remission after relapse treatment, 4 patients (8.8%) had stable disease, and 4 patients (8.8%) had relapsed. During follow-up of the cohort, two additional patients relapsed. The most common diagnoses were sarcoma, brain tumors, and germ cell tumors for 18 (40%), 8 (17.8%), and 6 (13.3%) patients, respectively. One-quarter of the patients had synchronous metastases. Before treatment, two-thirds of the patients opted for fertility preservation. Of the 13/45 patients who did not undergo preservation, nine received chemotherapy. Fertility preservation was discussed with all of these patients prior to treatment. Four patients refused, one patient was unsuccessful, and for two patients with hormone-dependent cancer, stimulation was medically contraindicated. For one patient, the procedure was impossible during the pandemic, and there was no information available for one patient with a brain tumor who was treated with temozolomide. Adverse events were observed in 17 patients (37.8%): The most common were hematological toxicity (10%), cosmetic sequelae (10%), and two cases of dermatotoxicity (radiation fibrosis and bleomycin-related eruption), orthopedic sequelae (8.9%), and neurological sequelae (4%). Of the 45 patients, one patient with an ovarian tumor had fertility problems and had previously undergone fertility preservation. One patient experienced panhypopituitarism, which was correlated more with the tumor’s location than with treatment toxicities (Table 1).
Characteristic of Patients
Social characteristics
The following social characteristics were collected: 21 patients (46.7%) had left the family home, and 10 patients (22.2%) were living with a partner. Twenty-seven patients (60%) were no longer students. In terms of educational qualifications, information was available for all patients except one: 14 patients (31.8%) had obtained a high school qualification (the French baccalaureate), 24 patients (56.8%) had pursued further education after obtaining their baccalaureate qualification, and six patients (13.6%) had completed a school- or apprenticeship-based training program.
At the start of the study, 19 patients (42%) were unemployed: 4 due to disability, 10 due to sick leave, and 5 were looking for work. Meanwhile, 26 patients (57%) were either studying or engaged in a professional activity. Fourteen patients reported being able to work without difficulty, whereas 23 patients had either not returned to work or school (18 patients) or had difficulty doing so (5 patients). Twenty of these 23 patients (87%) stated that the main reason for being unable to work well was related to cancer and/or its treatment. Changes in activity (work or study) were observed in 5 patients out of 26 (19.2%), 2 of whom attributed this to their disease and/or treatment.
Ten patients (22.2%) reported financial difficulties, and 14 patients (31.1%) received support from a social worker.
After treatment, 9 out of 22 patients (40.9%) who had played sports stopped due to the disease and/or its treatment. Thirty-three patients (70%) returned to their leisure activities, and 41 patients (89%) returned to their social lives.
Psychological characteristics
Forty-four patients completed the WHOQOL-BREF. On average, patients filled in the questionnaires twice over time. The number of patients decreased from N = 45 at the end-of-treatment visit to N = 5 at the year 5 visit because many patients were still undergoing follow-up.
Overall perception of QoL and health remained stable throughout the follow-up period, with a median score of 4 on the 0–5 scale. Median scores for the social relationships domain fluctuated between 75 and 83 on the 0–100 scale. Scores for the environment domain remained stable at ∼80.
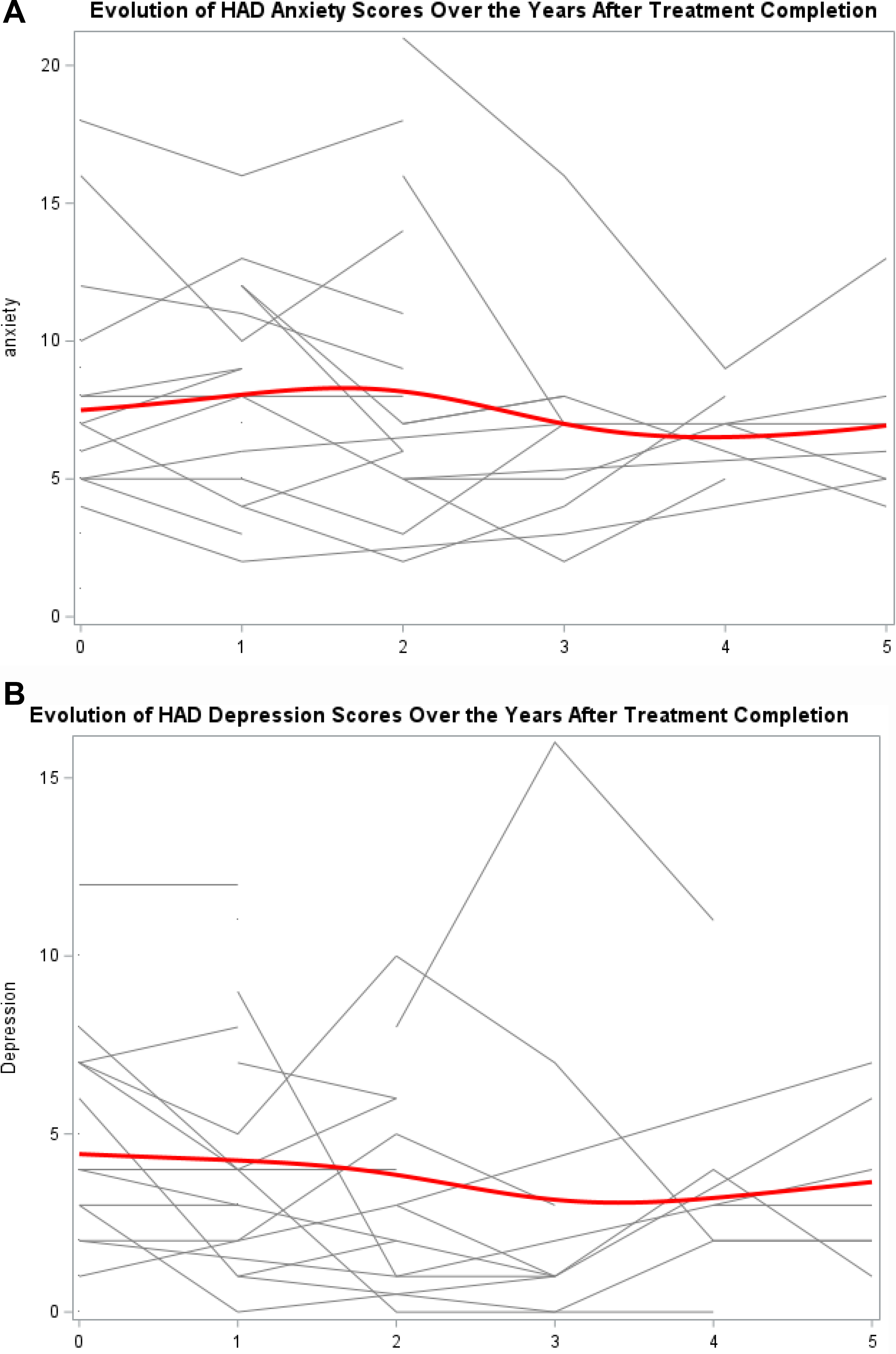
Forty-five patients completed the HADS. On average, patients filled in the questionnaires twice over time.
Symptoms of anxiety remained stable throughout the follow-up period, with a median score around 7 (Fig. 1A).
Finally, symptoms of depression decreased from 4 at the end of treatment to 2 at year 5 (Fig. 1B).
Sexological characteristics
A total of 17 patients, including 11 women and 6 men, met with the sexologist. Five patients (two women and three men, 29%) requested more than one appointment. Most of these patients (N = 11, 65%) required a sexologist appointment more than 1 year after the end of treatment. Two patients had sexologist consultations outside the ICO before their inclusion in the study. Twelve of the 17 received an introductory consultation from the oncosexology team at the start of their treatment within the framework of this study.
Three women and three men (N = 6, 35% of the sample) completed the FSFI and MSHQ surveys. According to the sexologist’s own scale (Supplementary Appendix SA1), patients’ responses regarding whether or not they had an emotional and/or sexual life (Fig. 2A) and whether they experienced difficulties in this area during their oncological care (Fig. 2B) were reported. Four women (36%) and one man (16%) reported that the disease and its treatments impacted their emotional and/or sexual life. Regarding nonqualitative data and verbatim records, women questioned whether they would have enough energy, be able to make room for someone else, or be able to learn how to love or be loved. They also reported concerns about side effects on their libido and desire, as well as significant vaginal and vulvar dryness and apprehension about future intercourse with penetration.
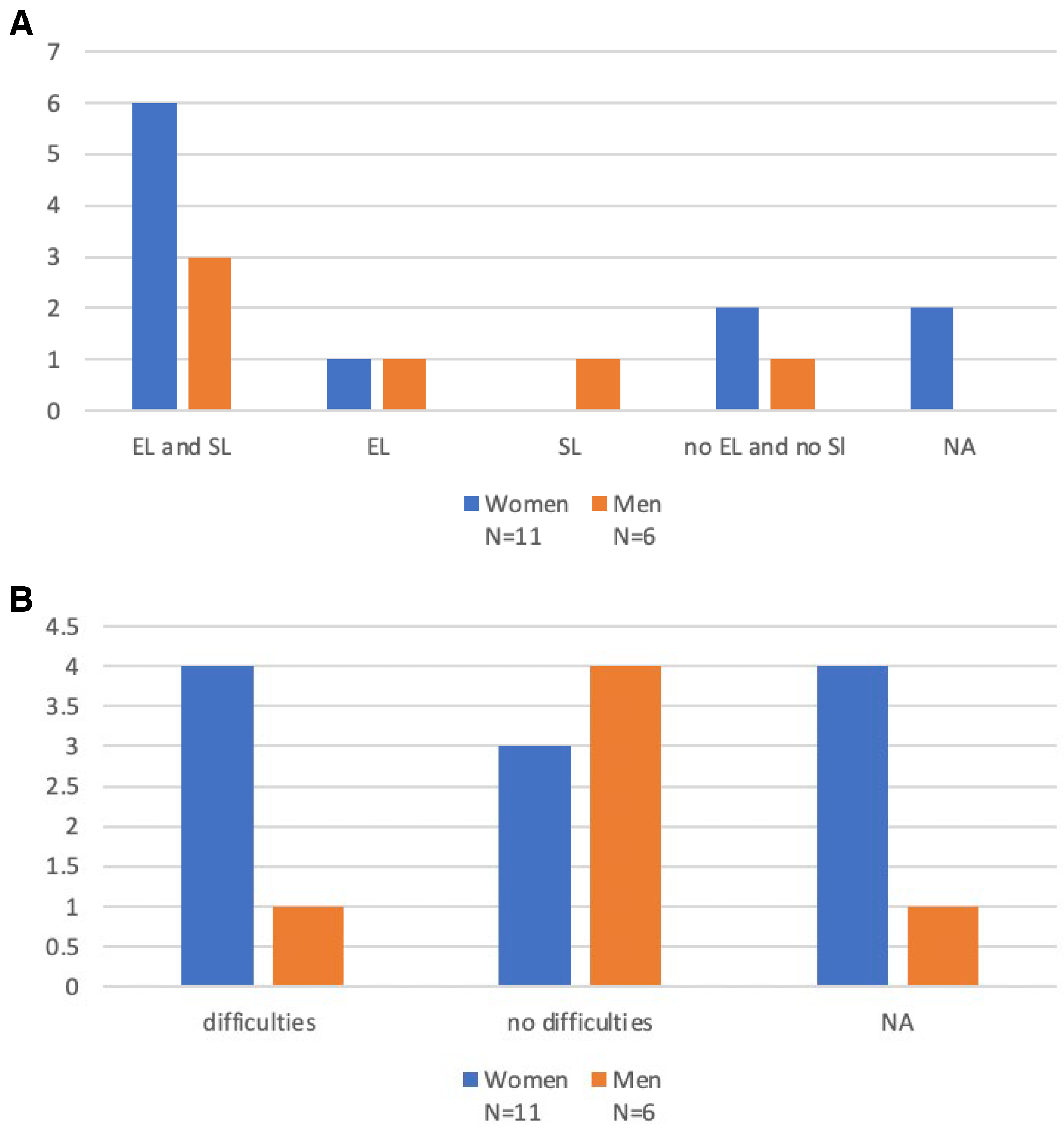
Emotional and sexual life of patients
Follow-up with the multidisciplinary consultation
This was a prospective longitudinal study, and the follow-up is still ongoing because not all patients were included at the same time (Table 2) At the time of the first analysis, 108 consultations involving members of the dedicated AYA team (consisting of a nurse, social worker, sexologist, and psychologist) had been registered. AYA patients were able to meet with one, two, three, or four professionals in 17.6%, 24.1%, 43.5%, and 14.8% of cases, respectively (Fig. 3). Figure 4 shows the number of shared consultations attended by each patient during the 5 years of follow-up. Only two patients did not attend their appointments: one during years 3 and 4 (it was during the period of the COVID-19 pandemic), and one during year 5.
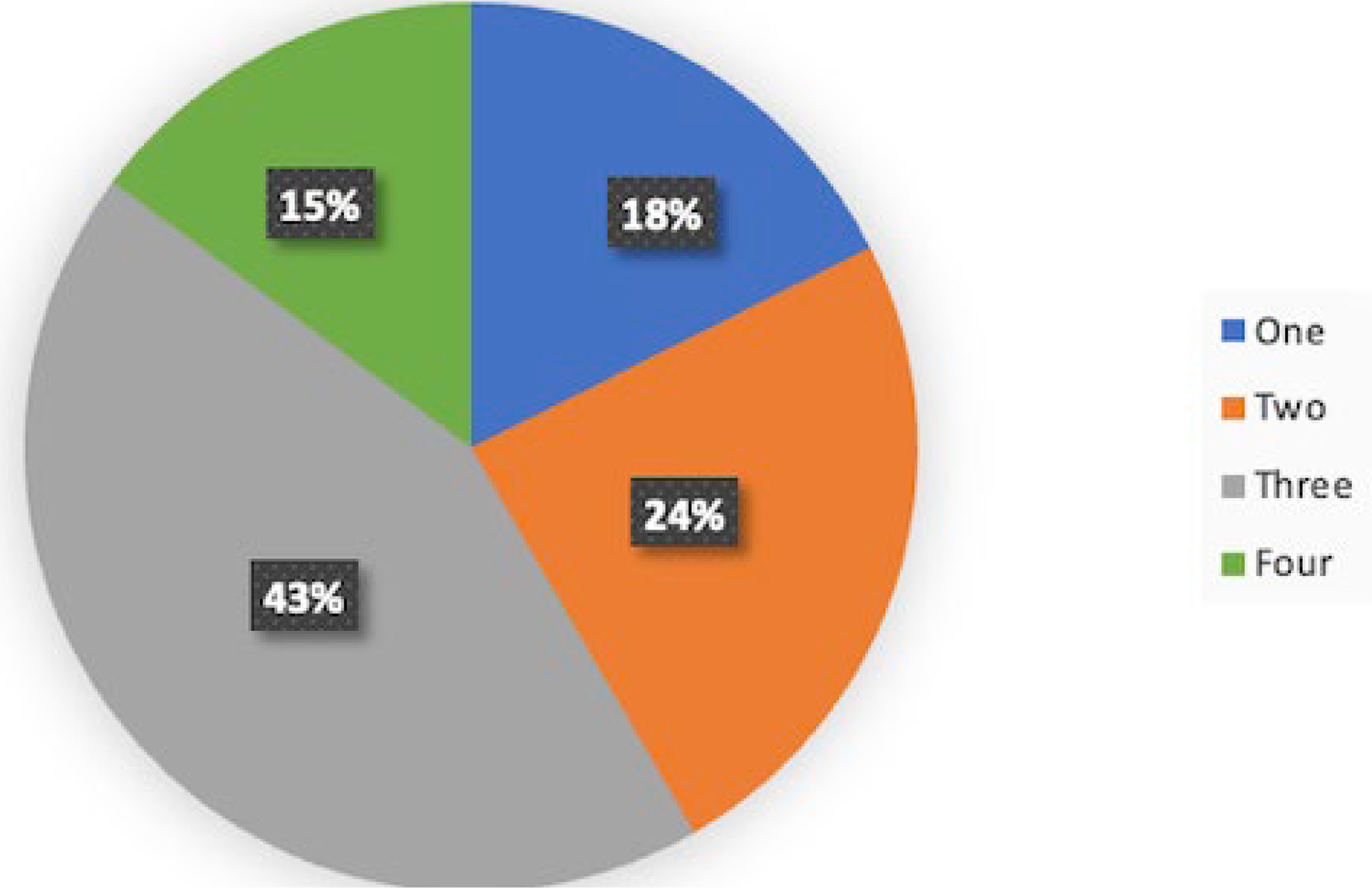
Number of health care professionals for a shared consultation.
Follow-up
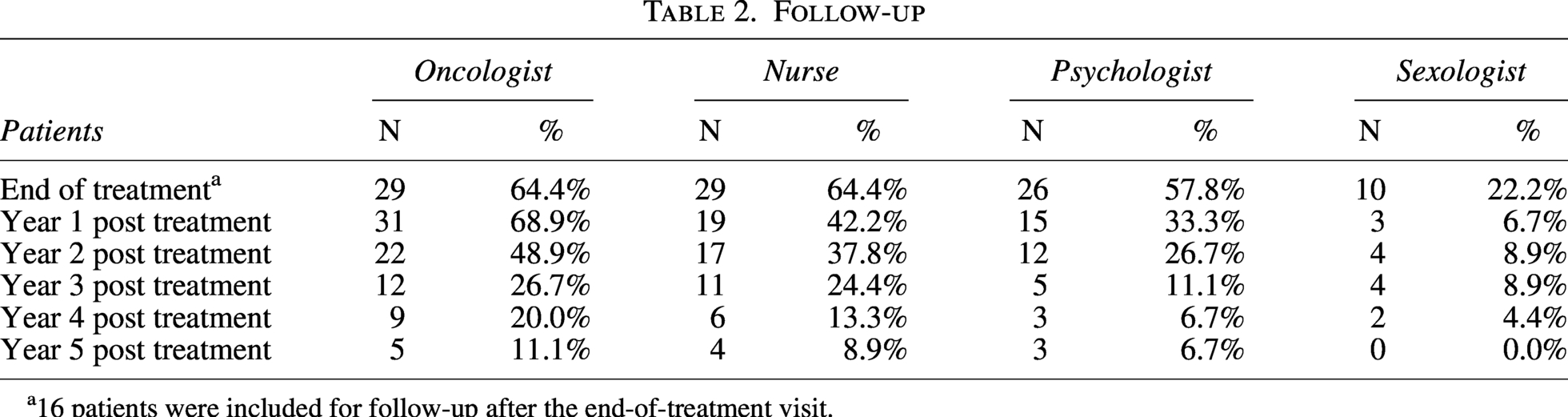
16 patients were included for follow-up after the end-of-treatment visit.
Identifying needs
A total of 144 AYA needs were identified during 92 appointments. The most common needs were related to professional career and social needs (31%), sexual life (44%), psychological state (23%), and adapted physical activity (APA) (14.5%) (Fig. 5).
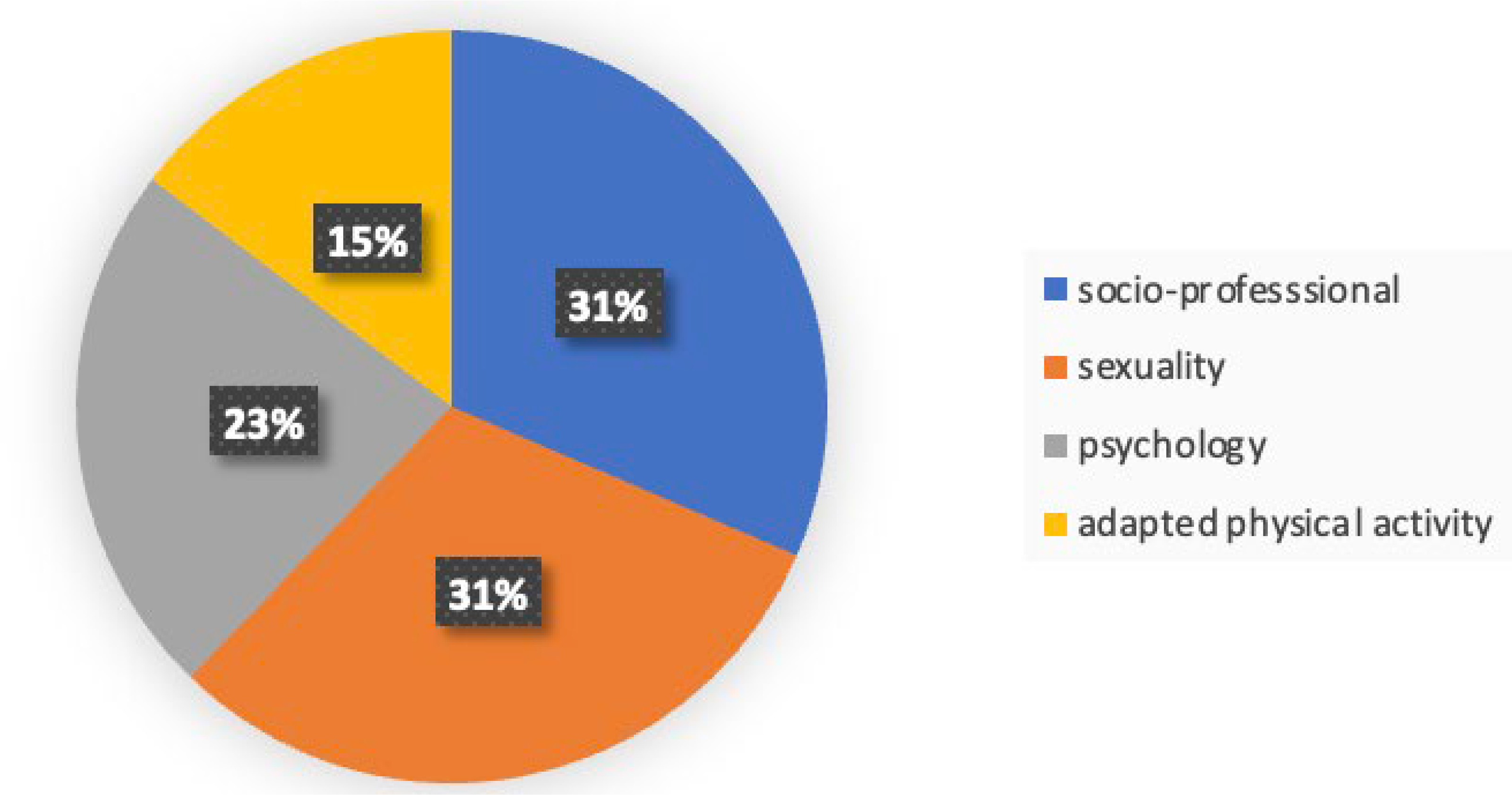
Identified needs.
Patients’ perception
The P-GIC satisfaction survey explores patients’ perceptions of consultations involving members of the dedicated AYA team, as well as the impact of the rehabilitation program on their situation. It was given after two consultations each year for 5 years. The question was phrased as follows: “Compared to your situation at the time of your first multidisciplinary consultation, what impact do you think the SAJAC program has had?” (Fig. 6).
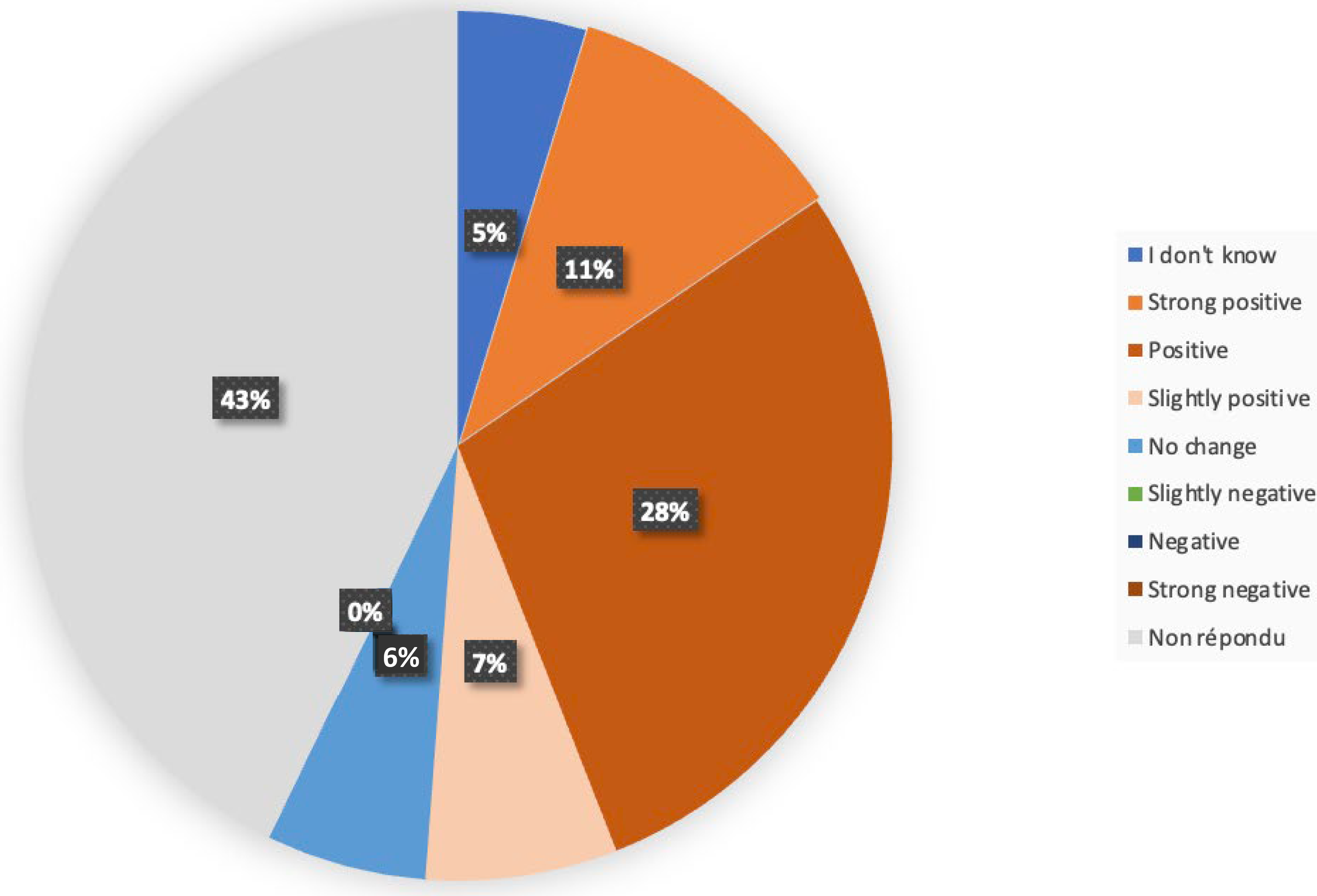
Satisfaction survey.
Of the 84 questionnaires completed at the time of the initial analysis, 48 responses were available, of which 43 (89%) reflected patient satisfaction. No change was observed for five questionnaires.
Discussion
In accordance with the literature and taking into account the exclusion of hematological diseases, the types of cancer identified in AYA patients treated at the ICO include sarcomas, germ cell tumors, and brain tumors.2,6,17 However, there are differences between France and the United States, with a higher incidence in the United States of thyroid carcinoma and melanoma. 5 Regarding cancer treatment, the AYA population was treated according to pediatric protocols when justified, as outlined in the literature.18–20 Unlike for the AYA population under the age of 18 years, for whom difficulties have been emphasized,12,21 clinical trials are usually available at comprehensive cancer centers for AYAs over the age of 18 years. Nevertheless, fewer than 10% of patients were included, as outlined both in the literature22,23 and in an analysis of the scientific data by the CNCR (National Research Coordination Committee) in France. Two hypotheses can explain this finding: the pandemic period and the fact that fewer open trials were available for these tumors at that time. There is a consensus in France that efforts should be made to include the AYA population in trials wherever possible.
In line with the recommendations of France’s Third Cancer Plan, an AYA team was established in 2012 as part of the eight experimental AYA teams. 14 As documented by others and well described in Haines’s report, 6 the AYA team has evolved over time and faced similar challenges to those experienced by other teams, including limited financial resources and staffing availability. In France, AYA teams are able to operate thanks to financial support from the ARS (French Regional Health Agency). This motivated us to adopt a consultation-based model at our institution, one of several models used in France and in other countries:11,12,24 AYA teams offering consultations, dedicated units, and mobile teams for different hospitals. All these models are represented within the French organization Go-AJA (https://go-aja.fr). There is no need to prioritize one model over another; the important consideration is that they align with the health care ecosystem in which they operate. The key to success is to start small and be patient, building on existing staff at an institution, as well as employing AYA “champions,” as described by Haines: Motivated caregivers who are willing to support AYAs.
Over time, the ICO’s AYA team changed the way they worked to provide systematic care for AYA patients, supporting them through “a 5-year rehabilitation program” following treatment. This approach was developed following the observation that AYAs do not spontaneously ask for help, that chronic issues are more difficult to solve, and that caregivers find it easier when problems are addressed early. It is always difficult to ascertain whether medical decisions meet patients’ expectations. Identifying a need does not necessarily mean that a patient will ask for help or expect a health care provider to address it. The help needed and the help desired are not necessarily the same. 25 Nevertheless, with the exception of two patients who missed one and two annual appointments, respectively, at the date of analysis, all agreed to see different health care professionals in a shared consultation. This study is still ongoing, and the participation rate throughout the 5-year follow-up period will only be determined at the end of the study.
Regarding the feasibility of offering multidisciplinary expertise through a single consultation, we observed that not all team members were always available on the same day, as was initially intended. Nevertheless, three or four health care professionals were present on the same day in 58% of cases. This could be seen as a weakness of this study, as it was anticipated from the outset. We have overcome this obstacle and now use virtual consultations in our daily practice. Furthermore, the pandemic taught us new ways of working and are now being used for this population, when appropriate.
The main question concerns the impact of cancer care programs for AYAs. There is no consensus on the tools to use to assess this impact. This study is purely descriptive and it does not include any statistical tests or a control group for comparison purposes, therefore, no conclusion can be drawn from it. We can simply note that patients were globally satisfied, as reflected by the responses to the P-GIC questionnaire available at the time of analysis. It partly reflects patients’ views on the impact of this program, and helps identify their needs to provide support beyond merely treating the disease.
AYA patients with cancer have specific needs due to their transition through life milestones. This prospective study does not claim to reveal anything new, but reports as literature their social, professional, psychological, fertility, sexual health, and physical activity needs.2,26
As previously reported, the rates of professional, financial, and social difficulties reported in this study are striking. For instance, 84% of participants in the Livestrong workshop reported making changes to their work following their cancer diagnosis, and 39% of AYAs in the United States reported that they or their families had borrowed money or incurred debt because of cancer.25,27 Furthermore, the National Health Interview Survey reported that 55% of cancer survivors did not receive psychosocial care. 28 In our study, one-third of patients requested support from a social worker, highlighting the strategic role played by social workers within the AYA team. This is now recommended practice by the INCa. 29 One limitation of our AYA team is the lack of a professional guidance counselor; however, this is partly offset by a dedicated program run by the AYA patient association.
Regarding fertility, the need AYAs have to preserve their fertility was rapidly identified when the health authority built a workshop around AYAs. Only a quarter of those who participated in the Livestrong study had undergone fertility preservation. Several reasons were listed, including cost, lack of time, and lack of information about the risk of infertility and fertility preservation.2,27 According to recent oncofertility recommendations, 30 fertility was discussed with all patients in our study. Jakes et al. mentioned the late toxicity of treatment and the risk of lower adherence to treatment in cases of treatment-induced infertility. 31
Regarding APA, its benefits are promoted by learned societies, 32 and programs offering it are available in France.33,34 However, it seems that there is less adherence among AYA patients 10 as illustrated in our study, despite the APA team being well established at our center. Efforts to engage these patients in APA must be maintained.
Cancer and its treatments have a profound impact on emotional and sexual health during and beyond cancer treatment,35–37 affecting individuals biologically, psychologically, and relationally through various sexual dysfunctions.38–41 For instance, Wettergren et al. reported that 49% of AYAs experienced negative effects on sexual function 1 year after cancer diagnosis, with 70% of these effects persisting 2 years after diagnosis. 35 Patients in our study expressed this specific need, which is probably under-reported due to the taboo surrounding sexuality (particularly among men) and the lack of systematic screening as reported by other teams. 35 An Italian experience reported by Veroni et al. relayed the voices of patients: “most patients (67%) reported not having the chance to talk to someone about having sex while receiving treatment, and 79% of patients felt this topic deserved more attention.” 42 An International Symposium held during the First Global AYA Cancer Congress was dedicated to sexual health issues and discussed strategies for addressing these problems in a systematic way. 43 In this context, sexology consultations were offered as part of our rehabilitation program. However, only slightly more than one-third of patients met the sexologist, despite no patients registering a refusal. The ICO has the opportunity to employ two sexologists and nurses dedicated to AYAs for this specific concern, and we hope that, in the future, all AYA patients will be able to access these services if they wish. The ICO is currently developing approaches that may include group patient education or digital formats. 44
In terms of psychological support, the results of our descriptive study do not suggest any particular trend in QoL over time. However, it will be possible to draw conclusions once all patients have completed the follow-up. A systematic review found that AYA cancer survivors report lower QoL than healthy AYAs and older cancer survivors, which is probably due to unmet needs, including for psychological support. 45 AYA cancer survivors are more likely than their peers and older cancer survivors to report anxiety and depression. 46 In this study, the initial data suggest that symptoms of depression may decrease over time from the end of treatment to 5 years later, while anxiety symptoms may not. This result may be partly explained by the fear of cancer recurrence, which appears to be common among young adults and adolescents who have survived cancer and is associated with high anxiety. 47 The results of our study thus highlight the importance of conducting research and creating interventions that address HRQoL to promote the well-being of AYA survivors. 48 In line with the study by Phan, 49 which focused on psychological adjustment, our descriptive results help us to both understand how AYAs’ QoL evolves over time and identify relevant time points at which to support them. Addressing patients’ psychosocial needs is a care priority at the time of diagnosis and beyond. 26
Conclusion
The AYA team, which specializes in this field, conducts a systematic needs assessment and works to address those needs. Different models exist in relation to the care ecosystem and its financial support, which we hope will be renewed.
Supplemental Material
sj-docx-1-jay-10.1177_21565333261464958 — Supplemental material for Prospective SAJAC Study of Rehabilitation for Adolescents and Young Adults with Cancer in a Comprehensive Cancer Center
Supplemental material, sj-docx-1-jay-10.1177_21565333261464958 for Prospective SAJAC Study of Rehabilitation for Adolescents and Young Adults with Cancer in a Comprehensive Cancer Center by Emmanuelle Bompas, Audrey Blanc Lapierre, Josselin Sebille, Sophie Allain, Marie Quereau, Solene Wallez, Nelly Soulard, Dominique Berton, Ludovic Doucet, Hélène Senellart, Jean-Sébastien Frenel, Mélanie Doré, Frédéric Rolland, Mario Campone, Sandrine Hiret, Emmanuelle Bourbouloux, Pierre Kubicek, Baptiste Sauterey, Céline Thomas, and Marianne Bourdon
Footnotes
Author Disclosure Statement
The authors declare that they have no known competing financial interests or personal relationships that could appear to influence the work reported in this paper.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.