
Abstract
Purpose:
This study aimed to characterize affected-limb pain and its associated factors among adolescent and young adult (AYA) survivors of lower extremity osteosarcoma in Japan. We hypothesized that both physical and psychosocial factors would be associated with pain, with an interaction between pain intensity and pain interference.
Methods:
A cross-sectional study was conducted among osteosarcoma survivors aged 18–39 years who had completed treatment at least 2 years earlier. Self-administered questionnaires assessed pain intensity and interference, physical function, fatigue, sleep disturbance, anxiety, depression, and perceived social support. Multiple regression analyses were performed to identify factors associated with pain outcomes. Semistructured interviews were also conducted to provide supplementary insights into pain characteristics and contextualize the quantitative findings.
Results:
Among 64 participants, 65.6% reported pain or pain interference during the preceding 7 days. Pain intensity was significantly associated with poorer physical function, older age at diagnosis, and lower perceived social support, whereas pain interference was primarily associated with greater fatigue severity. Pain intensity and pain interference were strongly correlated. Qualitative analysis identified four pain characteristics prosthesis-related pain, phantom limb pain, secondary pain, and weather-related pain. Interviews further illustrated how physical limitations, fatigue, and social support shaped pain experiences.
Conclusion:
Pain among long-term osteosarcoma survivors is influenced by multiple biopsychosocial factors. Although average pain severity was relatively mild, substantial interindividual variability was observed. Comprehensive survivorship care should address physical function, fatigue management, and social support to optimize long-term pain management and self-care among AYA osteosarcoma survivors.
Introduction
Survivors of lower limb osteosarcoma may experience persistent pain in the affected limb following limb-sparing surgery or amputation with tumor resection.1–4 Persistent pain is influenced by physical, psychological, and social factors and can interfere with activities of daily living and the ability to fulfill social roles.5,6
Osteosarcoma is a rare malignancy that predominantly affects adolescents and young adults, most commonly in their teens and twenties. In Japan, approximately 2,300 cases of osteosarcoma were reported among individuals aged 0–39 years between 2006 and 2022. 7 The extremities are the most frequent tumor site (45%). 8 While amputation was historically the primary treatment, advances in surgical techniques have enabled more than 80% of patients to undergo limb-sparing procedures as first-line treatment.9,10 Adolescent and young adult (AYA) survivors face psychosocial challenges during critical developmental periods, including reduced autonomy, difficulties with identity formation, academic and employment challenges, interpersonal difficulties, and fertility concerns.11,12
Existing studies on pain in malignant bone tumors have largely focused on postoperative pain,1,2 with limited research on chronic affected-limb pain among long-term survivors. Previous studies include retrospective cohort analyses based on medical records, 13 quality-of-life comparisons between limb-sparing and amputation groups in which pain is assessed as a single item, 14 and studies focusing on phantom limb pain.15–17 Survivors reporting pain have been shown to have poorer physical function and greater uncertainty, 4 and pain may further impair daily activities and social participation. 6 However, no studies have directly measured affected-limb pain in long-term osteosarcoma survivors or explored its characteristics and associated factors.
Pain is defined by the International Association for the Study of Pain as “an unpleasant sensory and emotional experience associated with, or resembling that of, actual or potential tissue damage.”18,19 Pain is inherently subjective, and individuals’ self-reports should be respected.18–20 Pain reflects an interaction of sensory, emotional, cognitive, and social factors rather than tissue damage alone.20,21 Assessing both pain intensity and pain interference is essential for a comprehensive understanding of pain.22,23 The biopsychosocial model provides a holistic framework for chronic pain assessment, such as physical injury, neural function, psychological responses, and social context, rather than focusing exclusively on nociceptive signal transmission. 20 This model has identified anxiety, depression, sleep disturbance, and fatigue as relevant factors in pediatric and AYA cancer survivors. 13 This study hypothesized that pain would be associated with physical and psychosocial factors, with an interaction between pain intensity and interference. Supporting survivors experiencing affected limb pain requires clarifying not only the presence of pain but also its characteristics and associated factors from both subjective and objective perspectives.
This study aimed to identify affected-limb pain and its associated factors in osteosarcoma survivors and to explore the pain characteristics and subjective pain experience of associated factors through interviews. This approach provides a comprehensive perspective on pain in the affected limb among osteosarcoma survivors, highlighting potential challenges and opportunities for enhanced support.
Materials and Methods
Study design
The study primarily employed a quantitative cross-sectional design, supplemented by interviews to explore the characteristics of affected-limb pain. Guided by the biopsychosocial model, we hypothesized that pain in the affected limb would be associated with physical, psychological, and social factors (Fig. 1). In this exploratory study, hypotheses were tested using quantitative data, and survivor-narrated interview data were subsequently analyzed to deepen understanding of the findings and to interpret the characteristics of affected-limb pain and its associated factors from multiple perspectives.
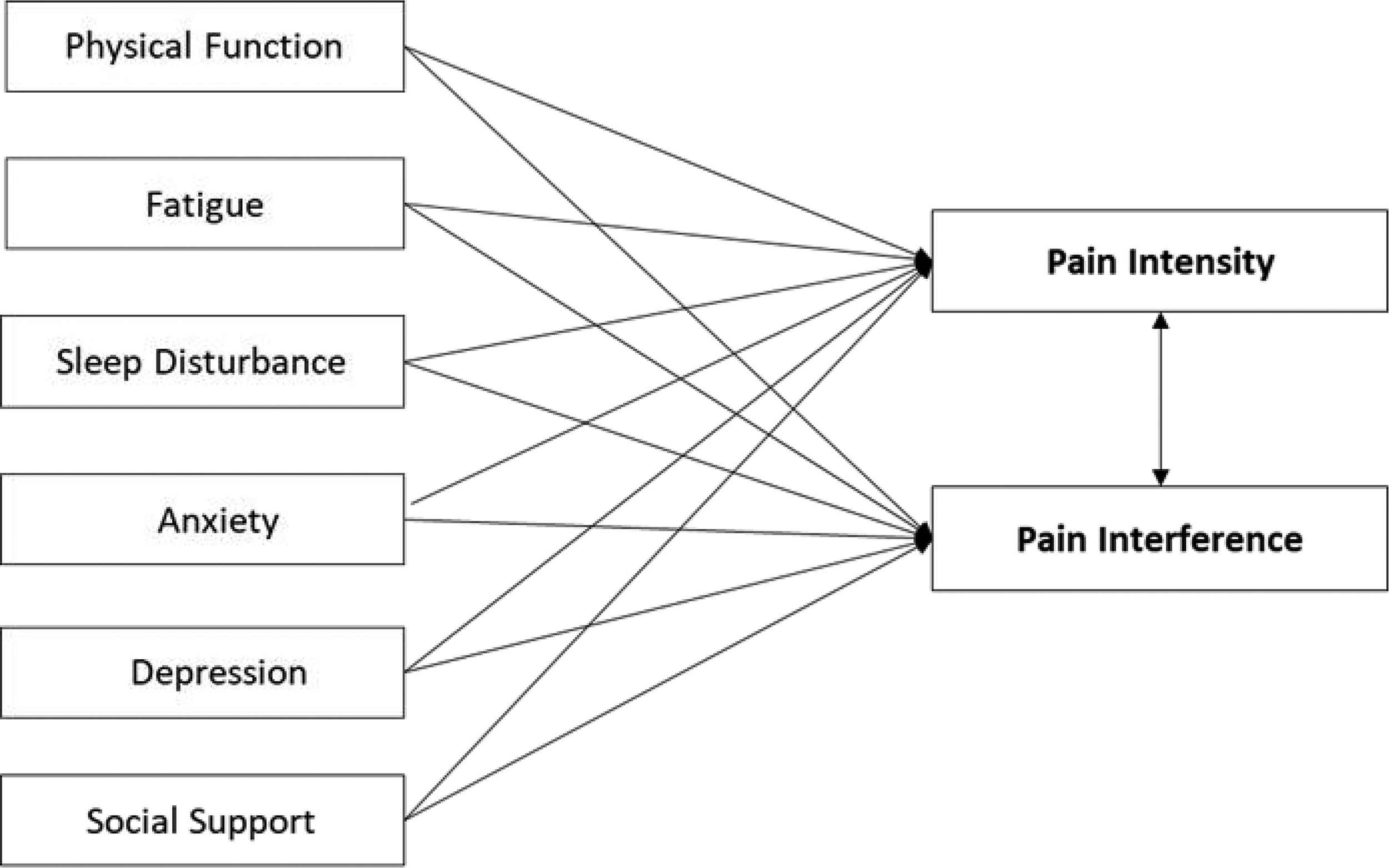
Hypothesis of related factors for pain.
Participants
Participants who met the selection criteria were recruited from four oncology hospitals in the Tokyo metropolitan area. Inclusion criteria were as follows: survivors aged 18–39 years who had been diagnosed with lower extremity osteosarcoma, had been informed of their diagnosis, had completed osteosarcoma treatment, had remained disease-free for at least 2 years, and were under routine follow-up at the time of the study. Exclusion criteria included individuals with osteosarcoma arising outside the lower extremity and those considered unable to respond due to evident psychiatric disorders or cognitive developmental impairments, as determined by their treating physicians.
Procedures
Potential participants meeting the eligibility criteria were identified by coauthors who were orthopedic surgeons at oncology hospitals. A written invitation and detailed study information were mailed to eligible individuals. Those who provided informed consent were enrolled, and self-administered questionnaires were distributed by mail. Upon questionnaire return, participants were asked about their willingness to participate in interviews; those who agreed were contacted by e-mail, and interviews were conducted either online or in person. All questionnaire respondents and interview participants received an honorarium. The study was conducted between May 2022 and August 2023 and was approved by the Ethics Review Committee of Tokyo Medical and Dental University (now the Institute of Science Tokyo) and collaborating institutions.
Self-administered questionnaire
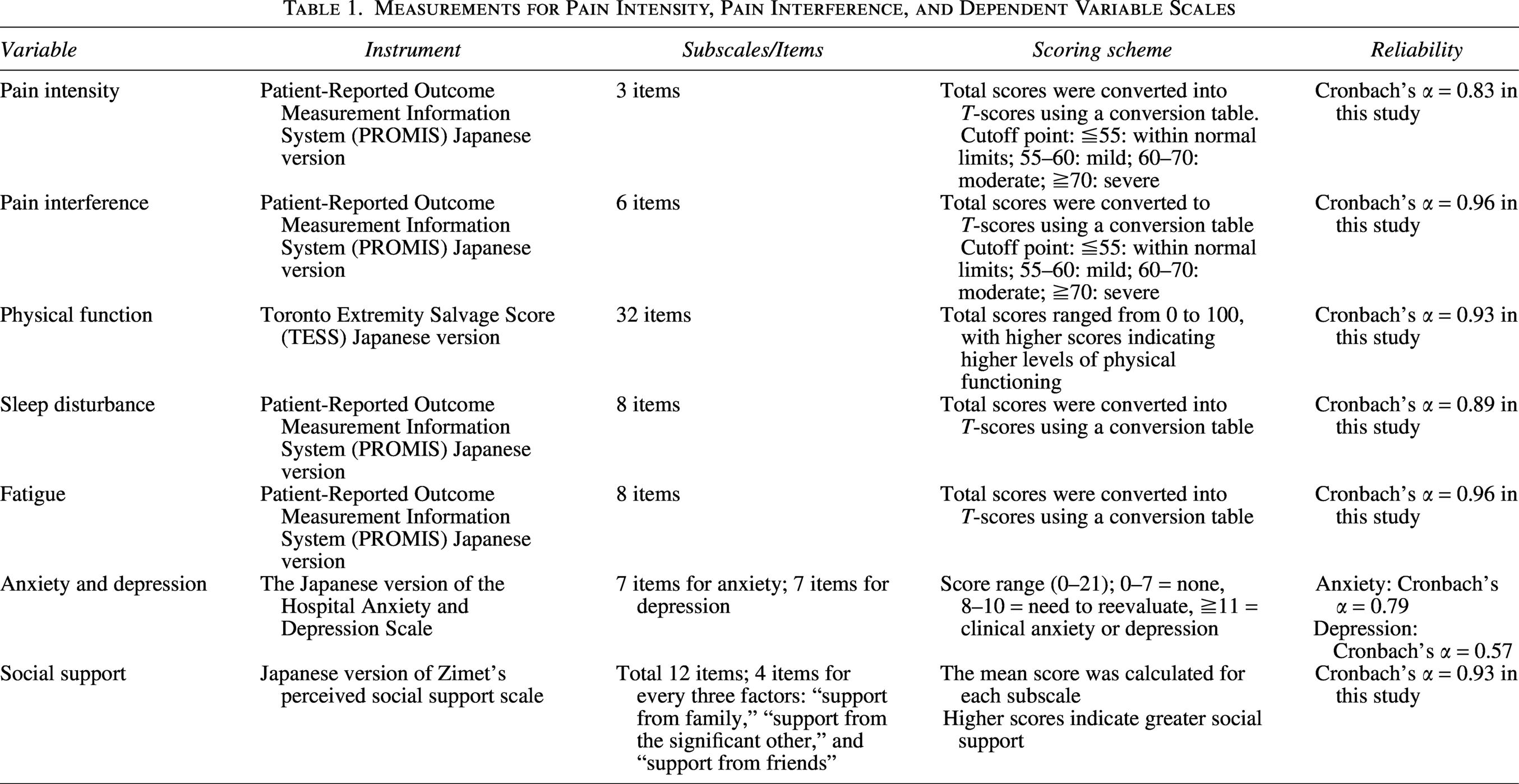
Demographic data (gender, education, employment status), as well as disease-related information, were collected. The following factors: pain intensity and pain interference from Patient-Reported Outcome Measurement Information System (PROMIS),24,25 physical function using Toronto Extremity Salvage Score (TESS),26,27 fatigue and sleep disturbances from PROMIS, anxiety and depression (The Japanese version of the Hospital Anxiety and Depression Scale), 28 and social support (The Japanese version of Zimet’s perceived social support scale) 29 were considered (Table 1).
Measurements for Pain Intensity, Pain Interference, and Dependent Variable Scales
Interview survey
Semistructured interviews lasting approximately 60 minutes were conducted either online or in person, according to the participants’ preference. In-person interviews were held in a private room at the first author’s office. All interviews were conducted by the first author and audio-recorded with participants’ consent. The interview guide included the following prompts: (1) “Tell me about the pain in the affected limb” and (2) “Tell me about your perception of the pain in the affected limb.”
Analysis
Quantitative data analysis
Statistical analyses were performed using SPSS version 30. Descriptive statistics summarized participants’ demographic characteristics, disease-related variables, and assessment scale scores. Differences in demographic characteristics, pain intensity, and pain interference were examined by conducting the Mann–Whitney U test or the Kruskal–Wallis test, as appropriate. Spearman’s rank correlation coefficients were calculated to examine relationships among the eight variables in the hypothesized model (pain intensity, pain interference, physical Functioning, fatigue, sleep disturbance, anxiety, depression, and social support), as well as variables showing significant bivariate differences (educational status and age at diagnosis). Multiple regression analyses were conducted to identify pain intensity and pain interference predictors. Given the limited sample size, variable reduction was applied to derive the final regression models, with selection based on the F-statistic and clinical interpretability.
Qualitative data analysis
The analysis of interview data aimed to identify (1) the characteristics of pain experienced by survivors and (2) pain-related experiences that complemented the multiple regression analysis model. After statistically analyzing quantitative data, interview transcripts were analyzed through Braun and Clarke’s reflective thematic analysis (TA), following a six-phase process with NVivo version 15. 30 Reflective TA is not limited to a single approach and can be flexibly selected according to research objectives. In this study, inductive coding was used to clarify pain characteristics, while deductive coding was utilized to clarify the explanation of the multiple regression analysis model.
Results
Demographic data
Of the 100 potential participants identified by coinvestigators across four oncology hospitals, 67 survivors consented to participate. Questionnaires were mailed to all 67 individuals, and 64 completed responses were received, yielding a response rate of 95.5%. Among the respondents, 33 participants (51.5%) expressed willingness to participate in interviews, and 26 (40.6% of respondents) ultimately completed the interviews.
The study sample comprised 38 male (59.4%) and 26 female (40.6%) participants, with a mean age of 27.5 years. The mean age at diagnosis was 16.3 years, and the mean time since diagnosis was 11.2 years. Educational attainment was categorized into two groups: 52 participants had post-high school education, and 12 had a high school or junior high school diploma. At the time of the survey, 46 participants were employed, and 18 were married (Table 2).
Pain Intensity and Pain Interference with Participants’ Characteristics
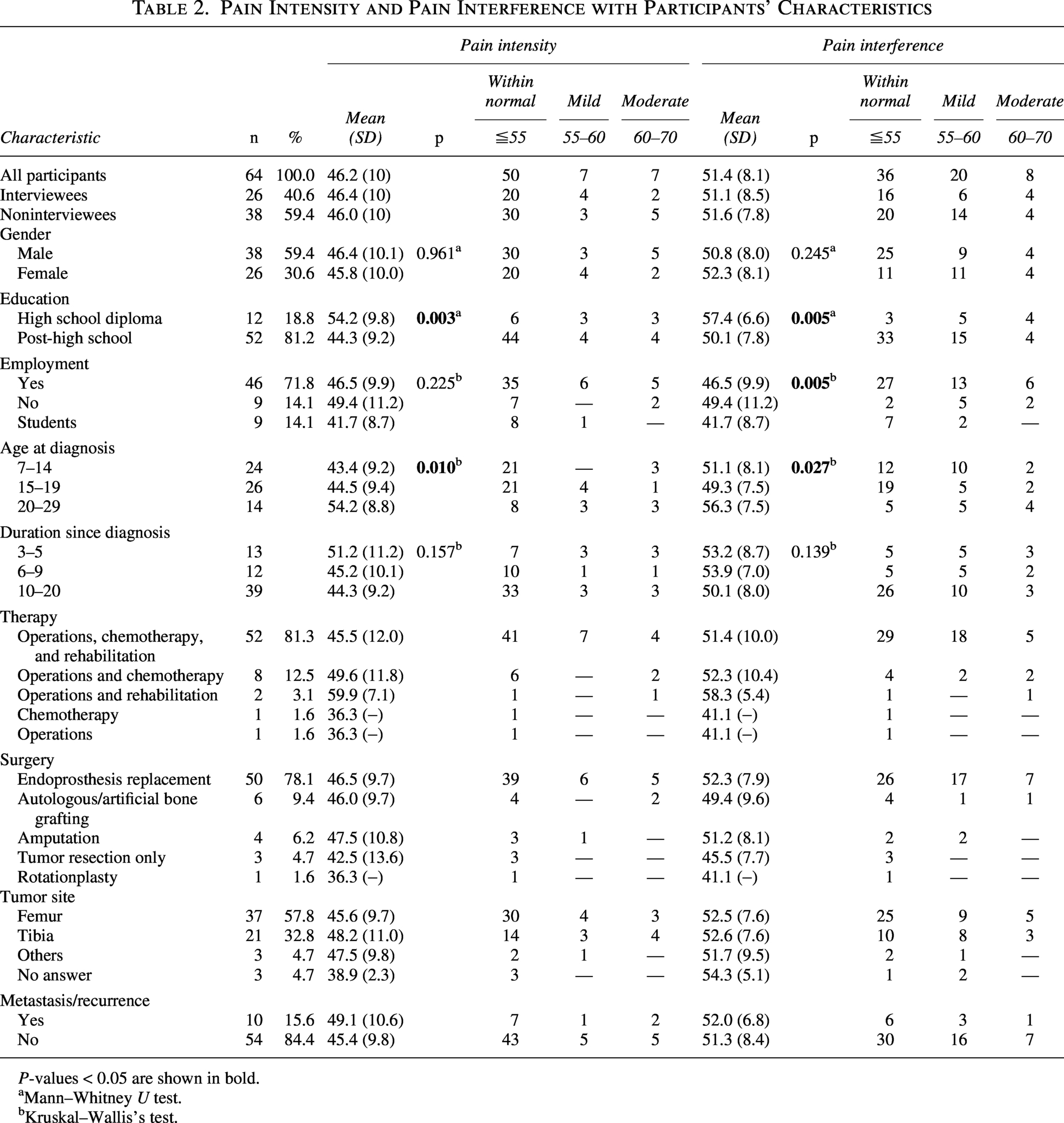
P-values < 0.05 are shown in bold.
Mann–Whitney U test.
Kruskal–Wallis’s test.
The interview sample included 26 participants (16 male [61.5%] and 10 females [38.5%]). Interviews were conducted online or in person and lasted an average of 63 minutes. The mean age of interviewees was 28.2 years, the mean age at diagnosis was 16.7 years, and the mean time since diagnosis was 11.5 years. Regarding treatment history, 20 participants underwent endoprosthesis replacement, two underwent amputation, two underwent tumor resection only, and two underwent autologous or artificial bone grafting. At the time of the interview, 21 participants were employed, two were students, and three were unemployed.
Characteristics of pain in the affected limb
The mean and median scores for pain intensity and pain interference within the 7 days before the survey were as follows: pain intensity, 46.2 (SD = 10, range 36.3–64.9); pain interference, 51.4 (SD = 8.1, range 41.1–68.7). Participants who responded “None at all” to all three items on the pain Intensity scale and all six items on the pain Interference scale (n = 22) were classified as having no pain in the past 7 days. Accordingly, 42 participants (65.6%) reported experiencing some pain or pain interference. Comparisons of scores between interviewees and noninterviewees showed no distinctive pattern for the interviewee group. Pain intensity differed significantly by education status and age at diagnosis, whereas pain interference differed significantly by education status, employment status, and age at diagnosis (Table 2). Qualitative analysis of interviews identified four themes characterizing survivors’ pain in the affected limb: endoprosthesis-related pain, phantom limb pain, secondary pain from strain on the legs, and weather-related pain (Table 3).
Characteristics of Pain Determined from Interviews
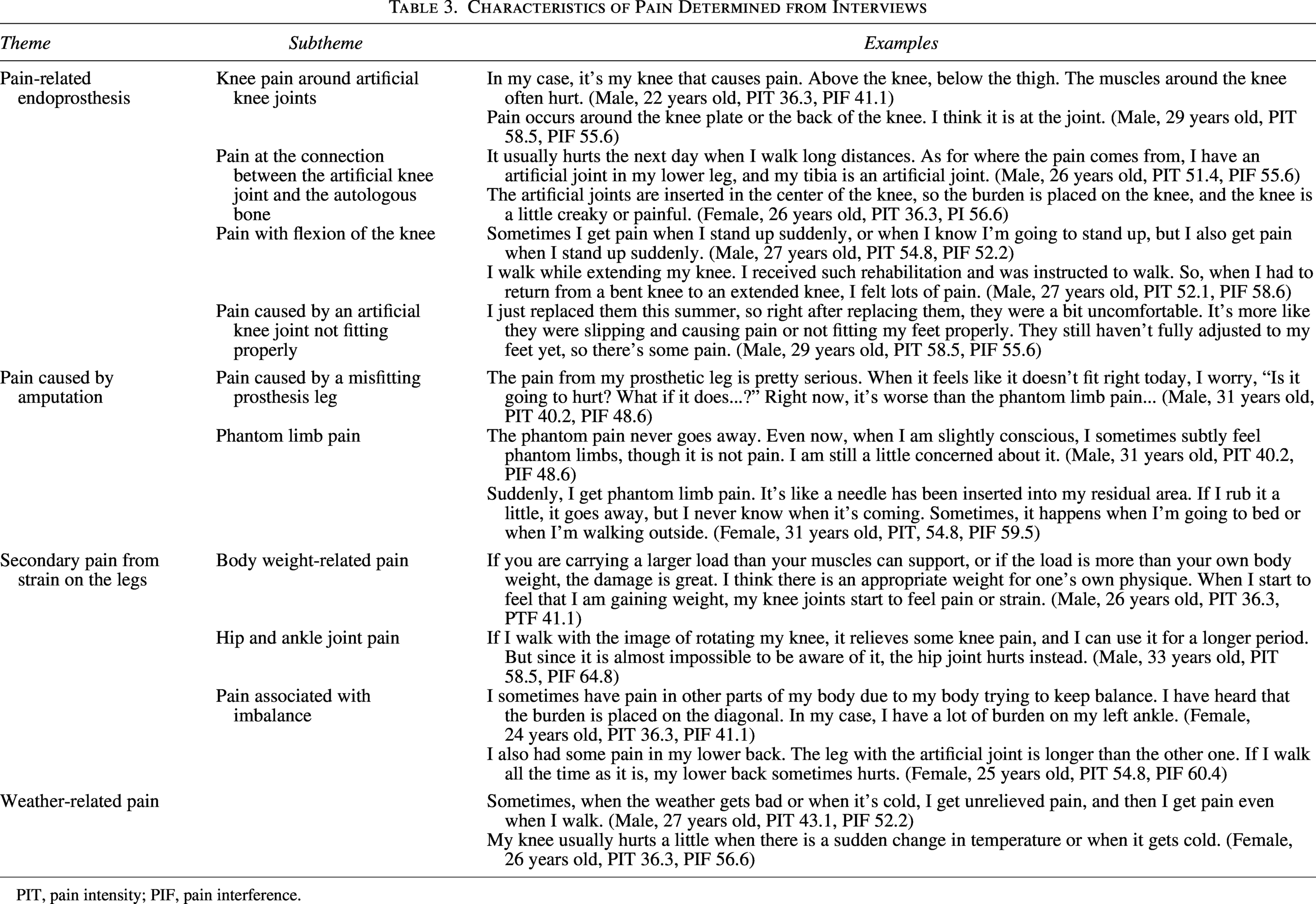
PIT, pain intensity; PIF, pain interference.
Variables related to pain intensity and interference
Factors related to pain-including physical functioning (TESS), fatigue, sleep disturbance, anxiety, depression, and social support-were measured. Scores were calculated separately for interviewees and noninterviewees, with no distinctive pattern observed in the interviewee group. Variable scores for all participants, interviewees, and noninterviewees are presented in Table 4.
Descriptive Statistics of Related Variables
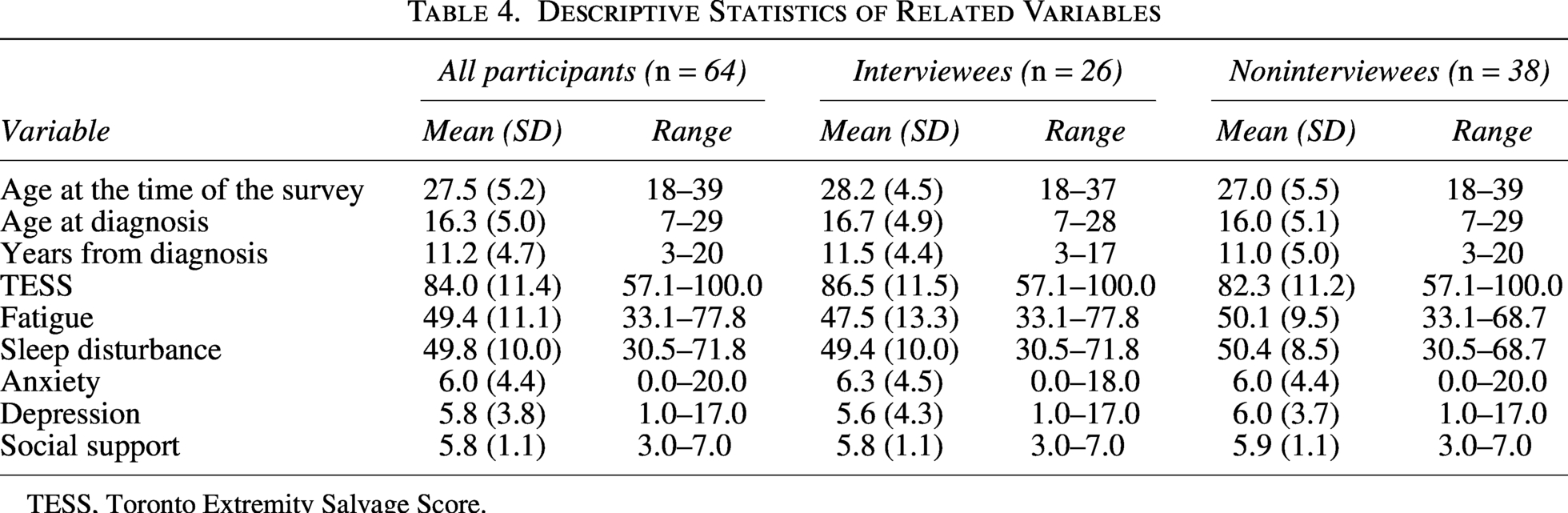
TESS, Toronto Extremity Salvage Score.
Multiple regression analysis with pain intensity and pain interference
Tables 5 and 6 present the correlation and multiple regression analyses. Pain intensity was positively correlated with pain interference, fatigue, sleep disturbance, depression, and age at diagnosis, and negatively correlated with physical functioning and education status. Multiple regression analysis (adjusted R2 = 0.56) showed that pain interference (β = 0.49, p < 0.001), physical functioning (β = −0.21, p = 0.035), social support (β = −0.16, p = 0.039), and age at diagnosis (β = 0.20, p = 0.003) significantly predicted pain intensity.
Factors Related to Pain Intensity
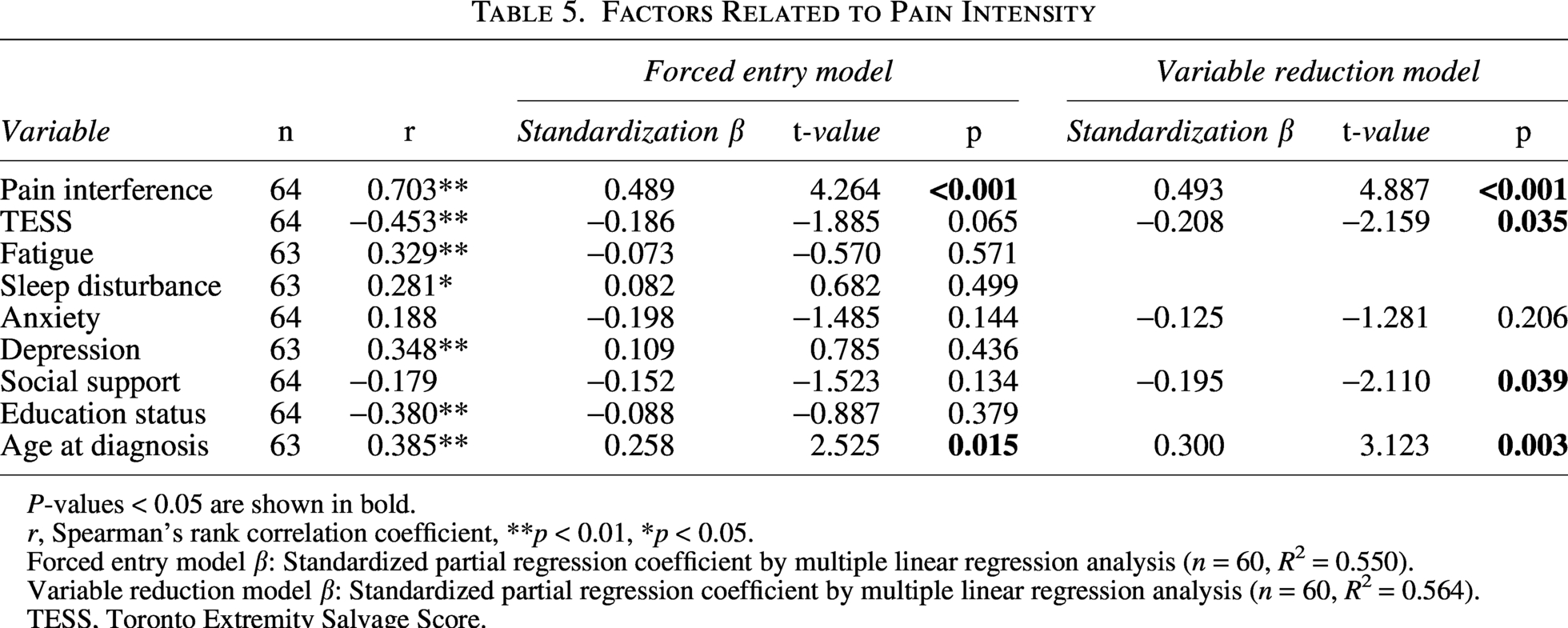
P-values < 0.05 are shown in bold.
r, Spearman’s rank correlation coefficient, **p < 0.01, *p < 0.05.
Forced entry model β: Standardized partial regression coefficient by multiple linear regression analysis (n = 60, R2 = 0.550).
Variable reduction model β: Standardized partial regression coefficient by multiple linear regression analysis (n = 60, R2 = 0.564).
TESS, Toronto Extremity Salvage Score.
Factors Related to Pain Interference
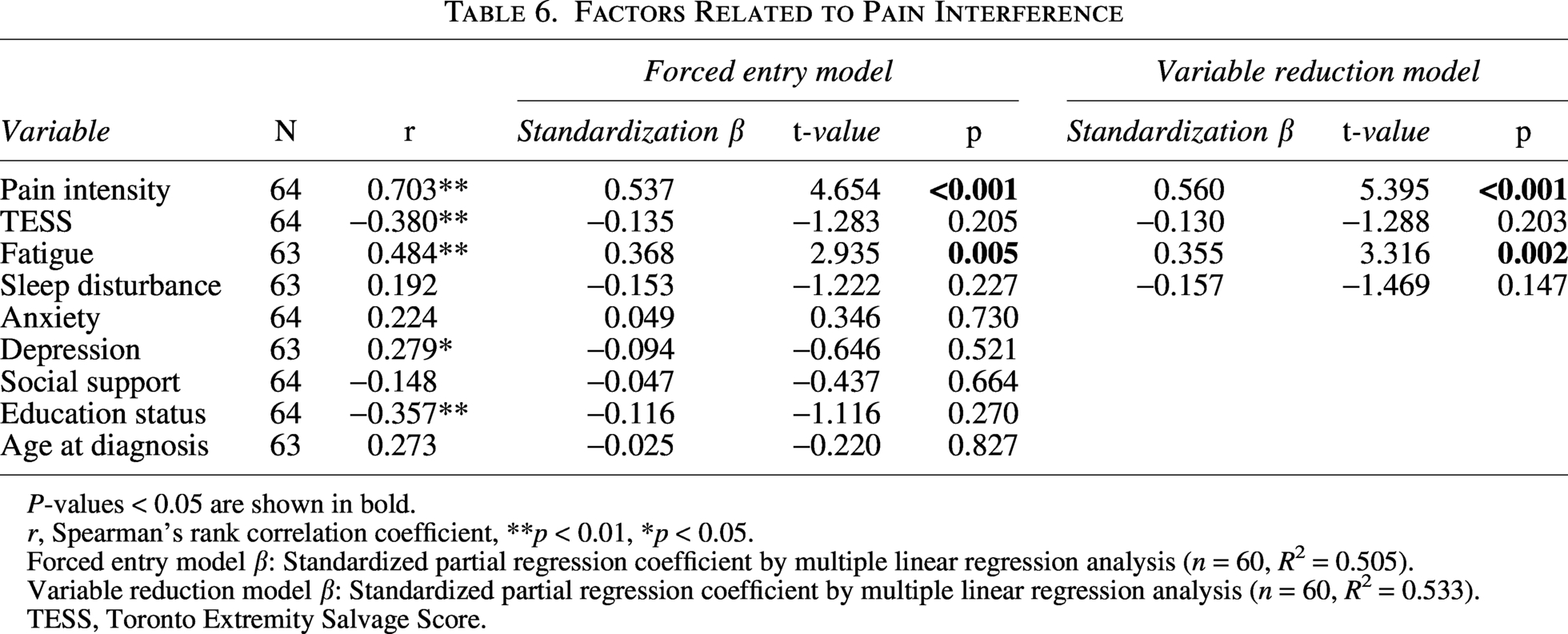
P-values < 0.05 are shown in bold.
r, Spearman’s rank correlation coefficient, **p < 0.01, *p < 0.05.
Forced entry model β: Standardized partial regression coefficient by multiple linear regression analysis (n = 60, R2 = 0.505).
Variable reduction model β: Standardized partial regression coefficient by multiple linear regression analysis (n = 60, R2 = 0.533).
TESS, Toronto Extremity Salvage Score.
Pain interference was positively correlated with pain intensity, fatigue and depression, and negatively correlated with physical functioning and education status. Multiple regression analysis (adjusted R2 = 0.53) indicated that pain intensity (β = 0.56, p < 0.001) and fatigue (β = 0.36, p = 0.002) significantly predicted pain interference.
Interview results complemented by multiple regression analysis findings
Based on the multiple regression analysis results, we identified three themes: “Physical Function and Pain Intensity,” “Social Support and Pain Intensity,” and “Fatigue and Pain Interference” (Table 7).
Interview Results Complemented by Multiple Regression Analysis Findings
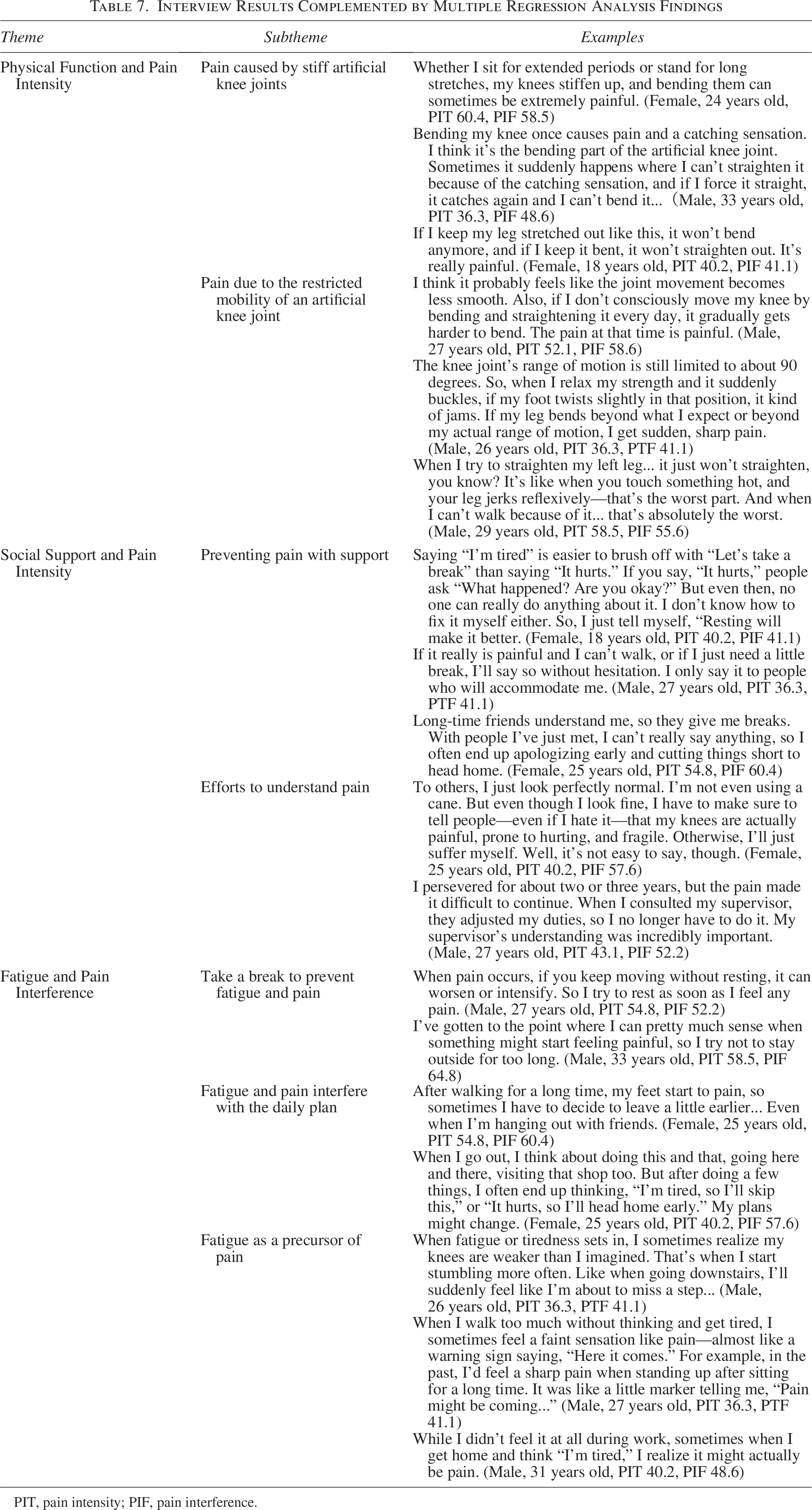
PIT, pain intensity; PIF, pain interference.
Discussion
In this study, low physical function, older age at diagnosis, and perceived lack of social support were associated with pain intensity, while fatigue severity was associated with pain interference. Pain intensity and pain interference were strongly related. To our knowledge, this is the first study to investigate self-reported pain characteristics in the affected limb of long-term osteosarcoma survivors, including pain intensity, pain interference, and associated factors.
The prevalence of pain among survivors was 65%, exceeding the 40% reported in previous studies.4,13,31 However, mean PROMIS pain intensity and interference scores were 46.2 and 51.4, respectively. Although direct comparisons with prior studies of malignant bone tumor survivors are not possible, the general US population mean of 50 suggests that many participants remained within the normal range. 24 Nonetheless, individual variability indicated considerable differences in both pain intensity and interference within the cohort. Fifty participants had undergone endoprosthesis replacement in this study. Complications of endoprosthesis are defined as soft-tissue failures, aseptic loosening, structural failures, infection, and tumor progression. 32 It is unclear whether complications occurred in this study’s participants. However, they reported the pain around knee endoprosthesis in interviews, suggesting a possible association with some form of complication. In addition, survivors’ lived experiences suggested that pain may occur within recurring contextual patterns. Future research requires to identify potential causes of pain around knee endoprosthesis.
The pain intensity model identified low physical function, older age at diagnosis, and perceived lack of social support as significant predictors. Pain interference was primarily exacerbated by severe fatigue. Older age at diagnosis was associated with greater pain intensity,2,4,33 and lower social support correlated with higher pain, which may reduce from support by family, friends, and health care orividers.34,35 Interviews suggested that empathetic support, understanding of pain, and daily life adjustments may alleviate pain. Malignant bone tumors such as osteosarcoma are rare cancers, so the number of survivors is relatively small, making it difficult to understand their pain. Therefore, they worked hard to gain that understanding. Mindfulness intervention studies suggest that family support may reduce postoperative pain in children. 36 Young adult survivors who are financially independent may have less access to family support compared with childhood and may experience higher pain intensity. For AYA survivors, peer support has been shown to reduce isolation and promote coping. 37 Facilitating peer networking and providing guidance on self-care may mitigate pain experiences.
The mean TESS score was 84.0, consistent with prior studies (82.9–89.0),38,39 and low physical function has been linked to pain.3,4,40 Exercise interventions have been found to improve walking function, and physical performance 41 and may reduce pain. In this study, several participants also reported that moderate leg activity helped improve their pain. In addition, although interview responses included descriptions of becoming easily fatigued during daily activities and rescheduling plans to avoid pain, the term “fatigue” itself was not explicitly mentioned. This suggests that participants’ fatigue awareness or recognition may be limited. However, some participants often described fatigue as “feeling tired” preceding pain, which can contribute to mental health difficulties 42 and affect role functioning. 40 Interventions targeting fatigue, including exercise, are therefore important. 43 The relatively low average pain scores suggest that survivors may be effectively managing their pain, 44 highlighting the need for further research on self-care and pain management strategies.
Several limitations should be noted. The cross-sectional design precluded assessment of temporal changes and causal inference. Despite being the largest self-reported sample of long-term osteosarcoma survivors in Japan, the sample size was insufficient for robust statistical analyses, and nonparticipant data were unavailable, potentially underestimating pain prevalence. Subjective self-report introduces possible response bias. Routine analgesic use was not assessed, which may have influenced reported pain intensity. In addition, orthopedic data, including tumor resection status and prosthesis details, were limited. Future studies should address these factors and evaluate analgesic use to clarify pain mechanisms and management.
Conclusion
This study demonstrated that pain among long-term osteosarcoma survivors is influenced by multiple biopsychosocial factors. Lower physical function, older age at diagnosis, and perceived lack of social support were associated with higher pain intensity, while greater fatigue severity was associated with pain interference. Although average pain scores were within the normal range, substantial individual variability indicated heterogeneous pain experiences. Qualitative findings described prosthesis-related pain and the importance of understanding and support from others. These results imply the need for comprehensive pain management in AYA cancer survivors, incorporating interventions to improve physical function, reduce fatigue, and enhance social support. Future studies are needed to examine the effectiveness of these interventions. Health care providers should recognize the characteristics of pain in AYA osteosarcoma survivors and its long-term impact on daily life.
Authors’ Contributions
S.K.: Conceptualization (lead), Methodology (lead), investigation (lead), formal analysis (lead), writing—original draft (lead), and writing—review and editing (equal). M.O.: Conceptualization (supporting), methodology (supporting), formal analysis (supporting), writing—original draft (supporting), and writing—review and editing (equal). S.Y.: Conceptualization (supporting), methodology (supporting), formal analysis (supporting), writing—original draft (supporting), and writing—review and editing (equal). S.I.: Investigation (supporting) and writing—review and editing (equal). K.A.: Investigation (supporting) and writing—review and editing (equal). K.H.: Investigation (supporting) and writing—review and editing (equal). T.G.: Investigation (supporting) and writing—review and editing (equal). T.Y.: Investigation (supporting) and writing—review and editing (equal).
Disclaimer
Portions of this study were presented at a scientific meeting; this article represents the first full publication.
Ethics Approval and Consent to Participate
Ethical approval for this study was obtained from the Ethics Committee of Tokyo Medical and Dental University (Currently Institute of Science Tokyo) School of Medicine under a batch review (M2021-186). Following this, permission was granted by the director of the collaborating institution. Participants were informed in writing about the study’s purpose and the protection of personal information. Consent was obtained by allowing participants to indicate agreement in the questionnaire survey and by explaining the study’s purpose in writing, online, or in person during interviews. Participants provided signed consent either manually or through an electronic signature.
Footnotes
Acknowledgment
The authors sincerely thank the survivors of lower limb osteosarcoma who participated in this study. The authors also express gratitude to Dr. Mitsue Maru (Vice Superintendent and Director of Nursing, Yodogawa Christian Hospital) for providing expert opinion and advice during the development of research plans and data analysis, as well as Professor Iori Sato (Institute of Science Tokyo) for providing expert opinion and advice during data analysis and reviewing and editing the article as a supervisor.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by a grant-in-aid of the