
Abstract
This cross-sectional study described oncofertility experiences of adolescent/young adult cancer survivors in Saskatchewan, Canada. Thirty-two AYAs (21.2 years, 56.3% male, 32.3% Indigenous) completed questionnaires. Medical records were reviewed. Distance to single centralized fertility clinic was calculated using geocoding software. 46.6% recalled oncofertility discussions, 35.5% had discussions documented, and 22.6% received fertility preservation referrals. Barriers included lack of available procedures and cost, but not travel. AYAs diagnosed ≤12 years were less likely to have FP referral (p = 0.03). Sex, treatment-related infertility risk, and distance did not impact discussion or FP referral odds. These data will inform our provincial oncofertility algorithm.
Introduction
Adolescent and young adult (AYA) cancer survivors (aged 15–39) represent a subset of patients with distinct care needs. 1 Fertility is a concern for AYA cancer survivors, with impaired fertility negatively impacting interpersonal relationships and quality of life.2,3 Early provider-initiated discussions about potential treatment-related impacts on fertility and options for fertility preservation (FP) are critical. The American Society of Clinical Oncology clinical practice guidelines recommend timely oncofertility counseling for all patients and prompt referrals to reproductive specialists for those interested in or uncertain about FP. 4 Disparities exist in counseling and referrals among racial and ethnic minorities, patients of lower socioeconomic status (SES), and individuals residing in nonurban areas.5,6
In Saskatchewan, Canada, oncofertility services are highly centralized, with one tertiary pediatric hospital and one reproductive endocrinology/infertility (REI) clinic. Both located in Saskatoon (population 366,168), they serve a provincial population of 1.2 million people, geographically distributed across 651,900 square kilometres. 7 The province has many rural/remote residents and a significant Indigenous population (17%, including 11% First Nations, 5.7% Métis, 0.3% Inuit).8,9 There is a paucity of data highlighting barriers to oncofertility care faced specifically by Indigenous patients.10,11 Saskatchewan utilizes a universal single-payer system. Oncofertility counseling appointments with REI specialists do not incur costs to patients. FP procedures (i.e., surgical fees) and tissue processing/storage fees are paid by patients out of pocket. Most patients access philanthropic funding. 12
Oocyte/embryo freezing and sperm banking (with option for testicular wedge resection and sperm extraction) are available to postpubertal patients. Ovarian tissue cryopreservation (OTC, the only option for prepubertal patients with ovaries) and testicular tissue cryopreservation (TTC) for prepubertal patients with testes (experimental biobanking) are not yet available.13,14 There is currently no standardized provincial oncofertility algorithm established. These care gaps, along with centralized services and a nonmetropolitan population, present an opportunity to examine our oncofertility practices and the experiences of a small yet diverse, equity-deserving AYA cohort.
Objectives
The aim of this preliminary cross-sectional needs assessment conducted in Saskatchewan, Canada, was to describe the oncofertility experiences of AYAs, aged 15–39 years at the time of study, who received care in our long-term follow-up (LTFU) clinic at our single, centralized tertiary pediatric hospital after treatment for pediatric and/or AYA cancers (>5 years off-treatment).
Our primary aim was to describe AYA oncofertility experiences, including perceived barriers, utilizing a quantitative patient questionnaire and self-reported demographic survey alongside retrospective chart review. Our exploratory aim was to determine if clinical variables or distance between home residence and the centralized REI clinic were predictive of odds of oncofertility discussion or FP referral.
Methods
Recruitment and study visit
With institutional ethics approval (USask REB #Bio-4562), participants were recruited from May 9 to December 6, 2024, at the Jim Pattison Children’s Hospital. The LTFU Clinic occurred monthly. Eligible participants included AYAs (15–39 years at the time of study) who were >5 years off-treatment for a cancer diagnosed in childhood, adolescence, or young adulthood. Those who were not fluent in English were excluded. Clinic schedules were reviewed to identify potential participants. Investigators contacted potential participants by telephone 48 hours prior to their appointments and introduced the study using a standardized recruitment script. Those who expressed interest were approached in person during their appointments to obtain informed consent. Consenting participants completed a demographic form that included postal code information and a survey with questions regarding their diagnosis, treatment, oncofertility experiences, and rank-order list regarding perceived barriers to FP. All questions had “I Don’t Know” and “Prefer Not to Answer” as options. Participants could leave questions blank.
Demographic and clinical variables
Patient/clinical variables (age, sex assigned at birth, diagnosis category, month/year of diagnosis, treatments, and documentation regarding oncofertility discussions and formal preservation referrals) were collected from medical records using a standardized data collection form. Self-reported variables (race/ethnicity, Indigenous/First Nations/Metis/Inuit identity, gender identity, sexual orientation, relationship status, education, employment, household income quintile, and postal code at time of diagnosis) were obtained from demographic forms. If participants did not document a postal code on their questionnaire, the postal code documented in the medical record was used as a surrogate. All variables were determined a priori.
Data analysis
Descriptive statistics were calculated for all study variables. The median and interquartile range (IQR) were reported for continuous variables. Categorical variables were summarized using frequencies and percentages.
Distance to REI Clinic from participant’s residence was calculated using Haversine’s formula from PCF+ (Postal Code Conversion File Plus) version 8B data. Univariate logistic regression was conducted to determine if geographic distance (in kilometres) to REI Clinic was predictive of odds of documented oncofertility discussion or FP referral, with median distribution-free 95% confidence interval (CI) calculated at p = 0.05.
Clinical variables for exploratory analysis (sex, age at diagnosis, infertility risk category) were determined a priori. Age cutoff of 12.99 versus 13.01 years was determined as a surrogate for pubertal status at diagnosis. Treatment-related infertility risk was assigned categorically (high risk vs. not) using our evidence-based institutional guidelines and reviewed by two independent pediatric oncologists, each with additional training or clinical experience in oncofertility, AYA oncology, and/or survivorship (Supplementary Data S1). Any discrepancies were resolved via discussion and source data review. Univariate analyses (2 × 2 contingency tables, Fisher’s exact test) were conducted to assess if clinical variables were predictive of odds of documented oncofertility discussion or FP referral in the medical record. Effect sizes were quantified using odds ratios. All tests were two-sided, with p = 0.05 significance and 95% confidence intervals. All statistical analyses were performed using SAS version 9.4 (SAS Institute Inc., Cary, NC).
Results
Of 39 eligible AYA patients invited to participate, 32 participants (82.1%) completed study visits. Mean age was 21.5 years; mean age at diagnosis was 8.9 years (median age = 21 years, age at diagnosis = 8 years). The cohort was 56.3% male and 32.3% Indigenous. Most AYAs (40.9%) endorsed the lowest socioeconomic quintile (<$36,000 CAD annual income). The most common diagnosis was leukemia/lymphoma (53.1%). Treatment-related infertility risk was high for 11 participants (34.4%.) One AYA (3.2%) had biological children, while 83.9% were considering having biological children in the future (Tables 1 and 2). Mean distance from participants’ residence to centralized REI clinic was 122.7 km, with median distance of 50.25 km (IQR = 6.15–206.8 km) (Supplementary Data S2).
Participant Demographics
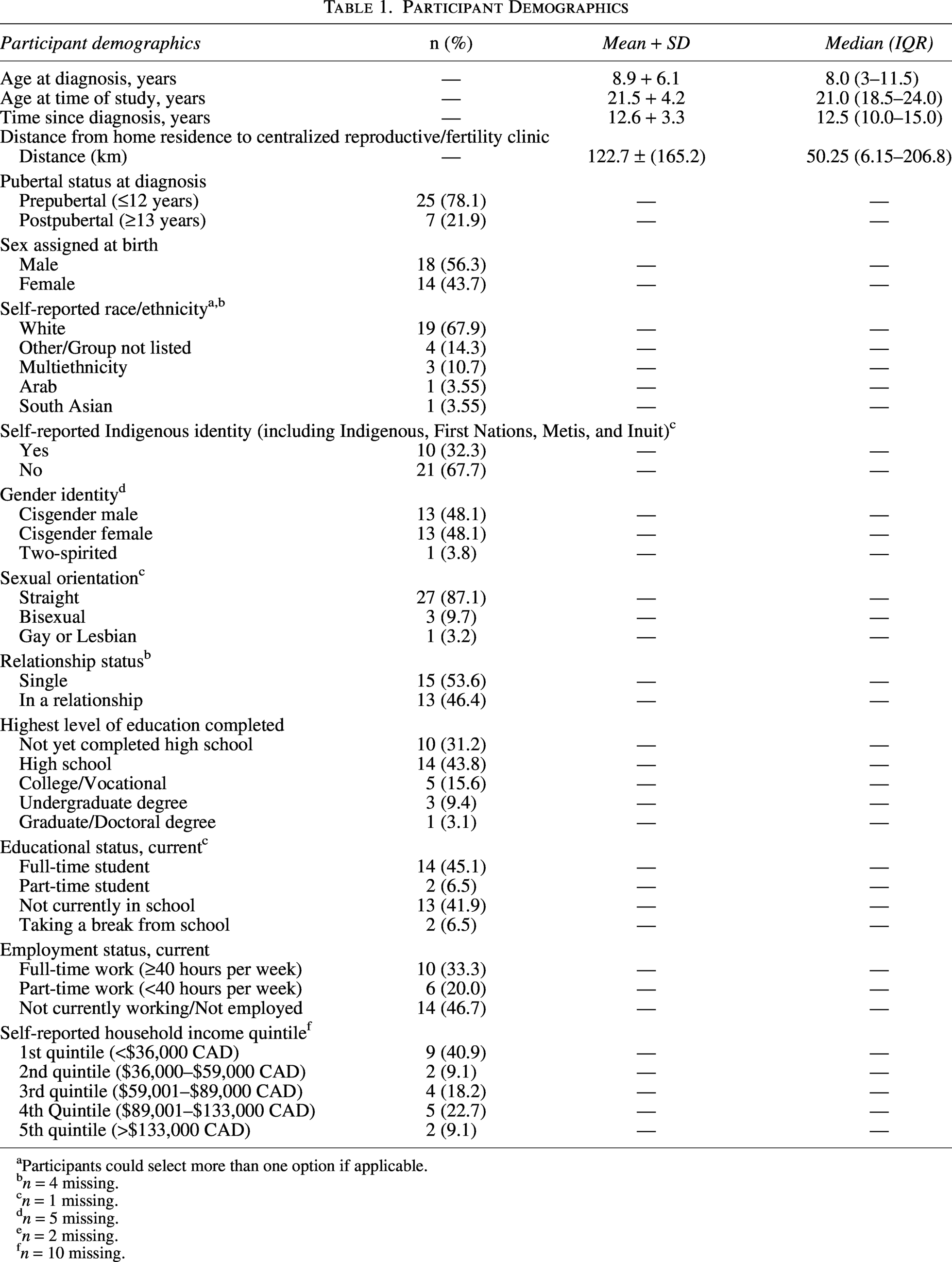
Participants could select more than one option if applicable.
n = 4 missing.
n = 1 missing.
n = 5 missing.
n = 2 missing.
n = 10 missing.
Clinical Variables and Oncofertility Experiences
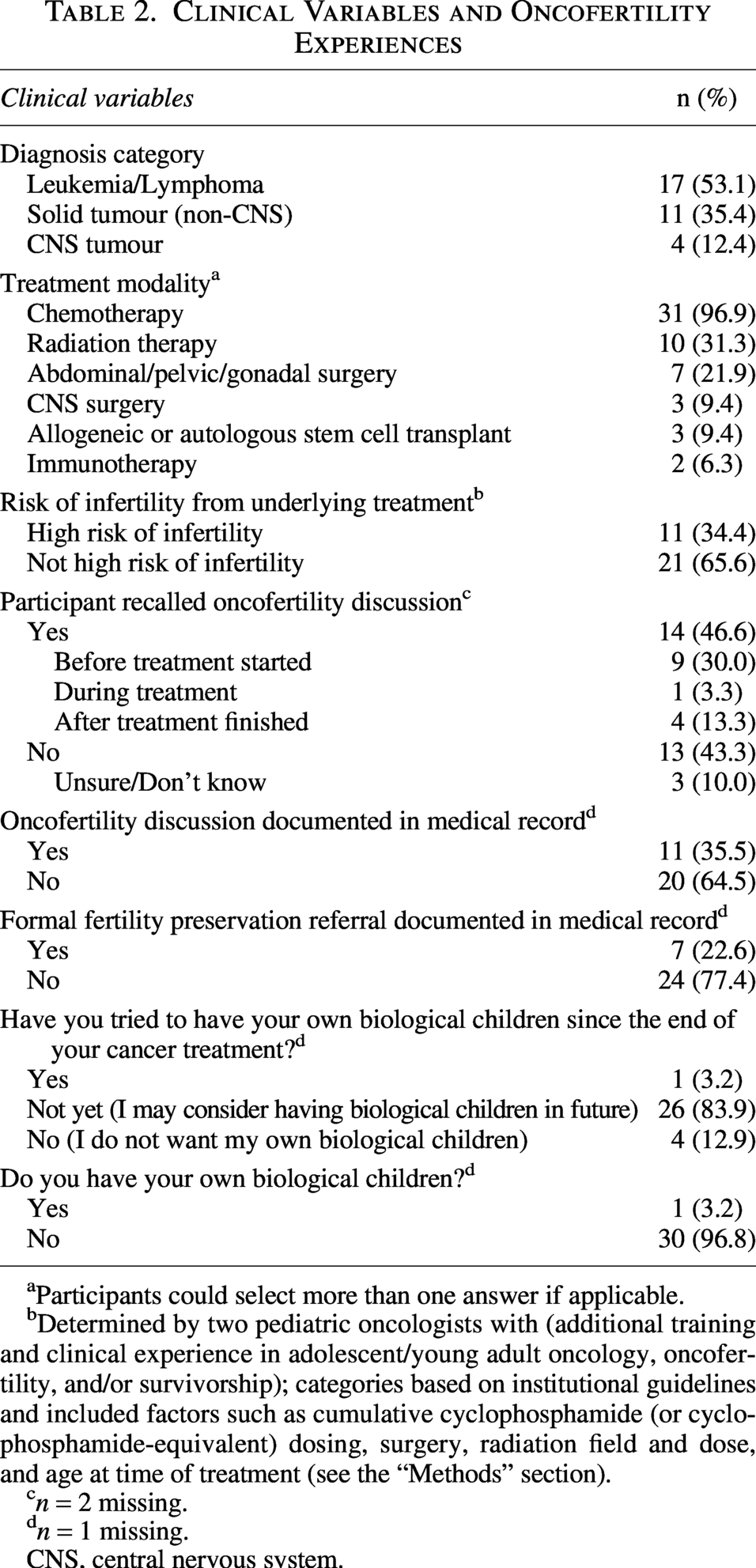
Participants could select more than one answer if applicable.
Determined by two pediatric oncologists with (additional training and clinical experience in adolescent/young adult oncology, oncofertility, and/or survivorship); categories based on institutional guidelines and included factors such as cumulative cyclophosphamide (or cyclophosphamide-equivalent) dosing, surgery, radiation field and dose, and age at time of treatment (see the “Methods” section).
n = 2 missing.
n = 1 missing.
CNS, central nervous system.
The most frequently endorsed self-reported barriers were having to undergo extra procedures (56%), being too ill at diagnosis (48%), lack of available procedures (44%), and cost (44%) (Fig. 1).
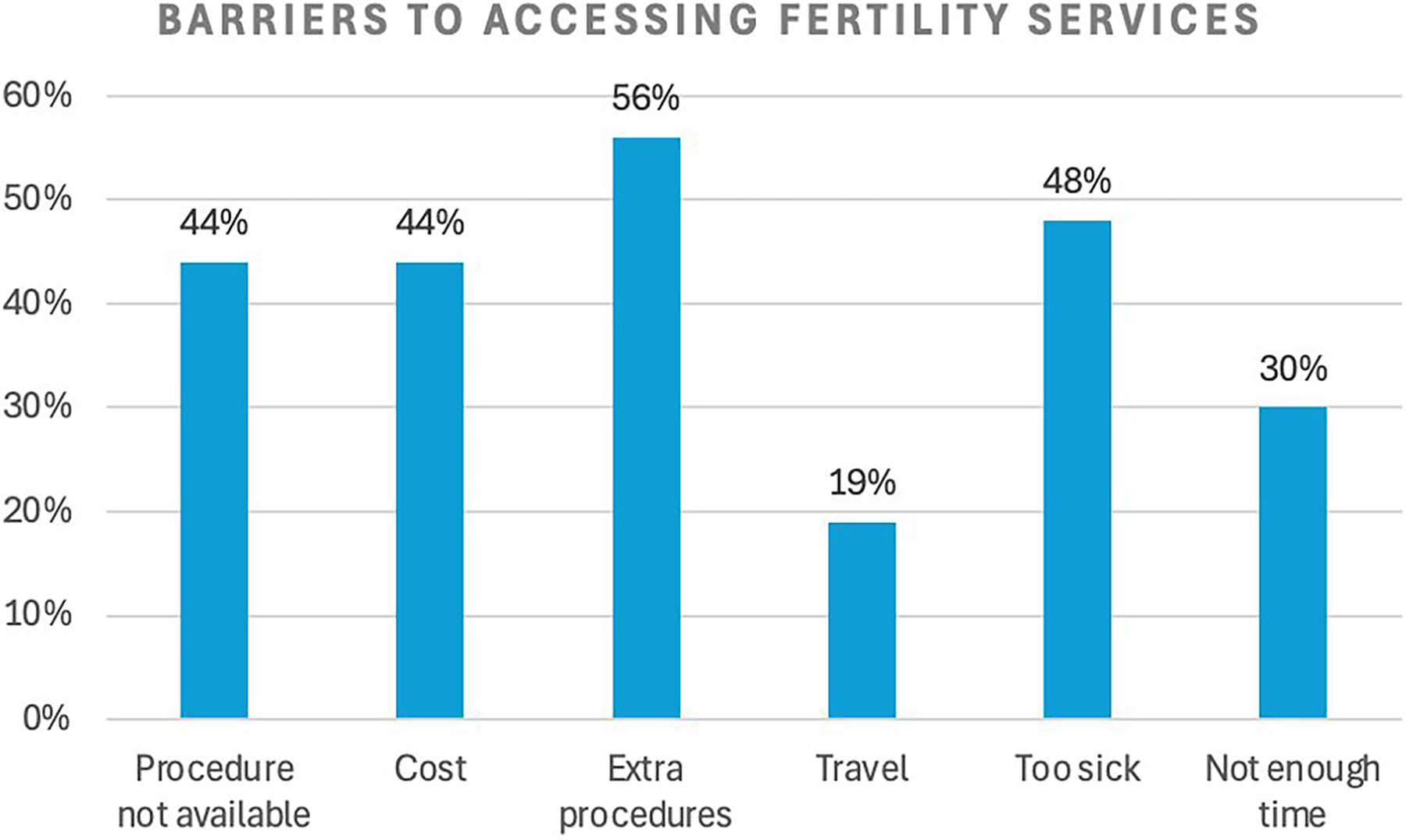
Participants were asked to rank perceived barriers to accessing fertility services. Predetermined barriers were ranked from 1 (most important) to 6 (least important) and then dichotomized as “endorsed” (ranked 1–3) or “not endorsed” (ranked 4–6).
Oncofertility discussions were recalled by 46.6% of AYAs, while 35.5% had a documented discussion in their medical record. Formal FP referrals were documented for 22.6%. AYAs aged ≤12 years at diagnosis were less likely to have FP referrals (p = 0.03) (Supplementary Data S2). Additionally, there was a trend toward a lower likelihood of oncofertility discussions documented in the medical records for AYAs aged ≤12 years at diagnosis (p = 0.067). Sex, high-infertility risk treatment, and distance to fertility clinic were not predictive of odds of oncofertility discussions or FP referrals documented in medical records (p > 0.05).
Discussion
This needs assessment provided insights into the oncofertility experiences of AYAs attending our LTFU Clinic at Saskatchewan’s single tertiary pediatric hospital. Fewer than half of the cohort recalled discussing fertility during their cancer care, and fewer than one quarter had a referral to a fertility specialist.
Our cohort was notably diverse, with over half of participants biologically male; 41% in the lowest SES quintile; one third identifying as Indigenous, First Nations, Metis or Inuit; and a meaningful proportion identifying as 2SLGBTQ+. The cohort also represented a young AYA population (mean age 21.5 years at study, 8.9 years at diagnosis). Only one AYA had children, while 84% reported considering having biological children in the future. In addition to there being no clinical FP option for prepubertal males outside of experimental biobanking for research, sperm cryopreservation has been underutilized by male AYAs despite its feasibility. 15 As such, male AYA perspectives are necessary to understand barriers impacting engagement with oncofertility care. Additionally, patients from racial or ethnic minorities and lower SES may be less likely to receive FP referrals and utilize FP services.6,16,17 Patients identifying as 2SLGBTQ+ may also experience unique barriers to fertility counseling and FP referral, and providers may unconsciously limit or alter discussions based on assumptions about patients’ identities. 18 This underscores the need for inclusive AYA stakeholder involvement to inform equitable oncofertility practices.
When examining perceived self-reported FP barriers, AYAs in our cohort endorsed having to undergo extra procedures; being too ill at the time of diagnosis; lack of available FP options; and cost, which have been well-documented barriers in other populations.19,20 The largely low SES profile of our cohort may have further contributed to the endorsement of cost as a barrier.
The Canadian oncofertility landscape is changing, with many provincial governments recently implementing tax credits for fertility procedures. However, these credits were unavailable to this cohort before/during treatment. It is notable that 60% of our cohort endorsed having to undergo extra procedures as a barrier. Additional procedures for FP may be undesirable when navigating treatment decisions and emotional and psychological distress at the time of diagnosis. Given the representation of Indigenous AYAs in our cohort, it is important to acknowledge that this population may face unique barriers to engaging with medical procedures related to historical and ongoing discrimination; culturally unsafe care; and intergenerational trauma experienced within the Canadian health care system.21–23 Future qualitative work is needed to better understand and contextualize procedural burden as a barrier in this cohort.
Travel and insufficient time were less frequently endorsed in our cohort. Geographical distance was not found to be associated with the odds of fertility discussions or referrals. Although travel and distance to centralized resources may be perceived as a barrier, many Canadian pediatric/AYA cancer patients already travel great distances within provinces and regions at baseline to access centralized tertiary pediatric oncology care. 24 Given that all patients would have already traveled to Saskatoon for treatment at our tertiary pediatric hospital at the time of their diagnosis, this may have mitigated the potential barrier of travel to the REI clinic.
Our data revealed a significantly lower likelihood of documented FP referrals among patients diagnosed before the age of 13, as well as a trend toward fewer documented discussions about potential impacts on fertility in this age group. AYAs who are younger at diagnosis are more likely to have unmet needs regarding infertility information and services. 25 In our cohort, this disparity likely reflects the limited FP options for prepubertal patients. Considering the young age at diagnosis for our cohort and the lack of OTC and TTC in our province, our low discussion rate may reflect historical health care provider bias that counseling is not beneficial when there are no FP options available. This assumption has been refuted: oncofertility discussions are therapeutic and minimize future regret and fertility-related distress, even if no FP option is undertaken. 4 These findings highlight the importance of both integrating standardized fertility discussions into future algorithms and expanding available FP options as means to increase future utilization and access.
Limitations and Future Directions
This study was limited by a small sample size. C-statistics for linear regression modeling for exploratory aims approached 0.5, suggesting limited discriminative ability. The impact of distance to centralized services could be tested in a larger expansion cohort after provincial algorithm implementation. Age at diagnosis served as a surrogate for pubertal status, and postal code geocoding software was utilized to estimate travel distance. These variables may have more complexity when factored into clinical decision-making. Approximately 30% of patients did not self-report income quintile data, which may have skewed results to suggest a lower SES cohort.
Results may not be generalizable to larger AYA populations. This study was conducted at a single time point. It could be meaningful to repeat measures over time as this cohort ages into their reproductive years, particularly since 84% reported interest in future biological children. Additionally, as our nonmetropolitan cohort included male, Indigenous, and 2SLGBTQ+ AYAs, future qualitative studies may further explore experiences of these groups.
Conclusions
Needs of AYA cancer survivors in Saskatchewan have been unmet, with historically low rates of documented oncofertility discussions and FP referrals. Despite centralized resources and vast geography, AYAs did not endorse travel as a barrier and distance to a single centralized REI clinic was not predictive of odds of oncofertility discussion/FP referral. These findings will serve as a baseline from which practice changes can be measured after standardized oncofertility algorithm implementation and may offer insights for health care providers who work with equity-deserving AYAs in comparable jurisdictions globally.
Authors’ Contributions
H.T.V. and P.R.D. conceived and designed the study, with contribution from L.H. S.K.L. and H.T.V. collected the data, with support from S.A. and P.R.D. S.K.L., S.A., and P.R.D. analyzed and interpreted the data. S.K.L. drafted the article. All authors (S.K.L., H.T.V., S.A., E.E.M., T.S.D., L.H., and P.R.D.) reviewed the article and provided final approval of the version to be published. All authors agree to be accountable for all aspects of the work.
Ethics Approval
This research was conducted with ethics approval granted by the University of Saskatchewan Research Ethics Board (REB #Bio-4562).
Footnotes
Author Disclosure Statement
P.R.D. has received an honorarium from Merck Inc.
Funding Information
The Saskatchewan Oncofertility Algorithm is being developed through funding support from the Canadian Partnership Against Cancer.
Supplemental Material
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.