
Abstract
Background:
Neurofilament light chain (NfL)is a promising biomarker of axonal injury and may facilitate earlier detection of chemotherapy-induced peripheral neuropathy (CIPN). This study evaluated longitudinal changes in NfL and its association with patient-reported CIPN symptoms in adolescents and young adults receiving neurotoxic chemotherapy.
Methods:
In this prospective, single-center study, patients >10 years of age with cancer receiving atubulin toxin were enrolled. Serum NfL and the Functional Assessment of Cancer Therapy—Gynecologic Oncology Group—Neurotoxicity (FACT-GOG-NTx) questionnaire were collected at baseline, midchemotherapy, and at the follow-up visit closest to 90 days after therapy initiation.
Results:
Eleven participants (median age 17 years [range, 12–24]; 63.6% male) were included. NfL levels increased longitudinally in all participants, with a median maximum increase from baseline of 112.5% (range, −32.0% to 4896.2%). Mean NfL levels increased from 2.32 at baseline (median 2.16) to 3.28 at mid-chemotherapy (median 3.47) and remained elevated at the follow-up visit (mean 3.85; median 4.38). Higher NfL levels were associated with worse FACT-GOG-NTx scores during chemotherapy (r = −0.32, p ≤ 0.01) and after chemotherapy (r = −0.31, p < 0.01).
Conclusions:
NfL increased throughout treatment and was associated with patient reported CIPN symptoms, supporting its potential as an objective biomarker for early detection and monitoring of chemotherapy-induced peripheral neuropathy in adolescents and young adults receiving neurotoxic chemotherapy.
Background
Chemotherapy-induced peripheral neuropathy (CIPN) is a common and distressing toxicity experienced by the majority of children adolescents and young adults (CAYAs) who are receiving chemotherapy. 1 CIPN is characterized by sensory, motor, and autonomic dysfunction, most notably leading to extremity numbness, tingling, and pain; lower extremity weakness, impaired tendon reflexes and balance; gait disturbances; and constipation. These toxicities can be both acute and chronic, the latter resulting in long-lasting effects on physical function, school performance, and health-related quality of life in CAYA cancer survivors. 2 In adolescent young adult (AYA) cancer survivors, 23% had continued CIPN pain lasting >12 months with moderate levels of pain intensity and pain-related interferences. 3
Early identification of CIPN is crucial, as timely intervention could significantly reduce long-term impacts. However, current detection methods are insufficient, leaving many adolescents and young adults (AYAS) at risk of irreversible damage. While CIPN occurs in up to 100% of children receiving chemotherapy, depending on risk factors and measurement approach, recent studies show that clinicians often miss CIPN in routine oncology care. 4 Clinicians diagnose CIPN using the Common Terminology Criteria for Adverse Events (CTCAE) grading system, which relies heavily on subjective clinical judgment, has poor interrater reliability, and lacks sensitivity in detecting early or subtle CIPN symptoms in CAYAs. 5 Objective measures including the modified Total Neuropathy Score (mTNS) and clinical Total Neuropathy Score (cTNS) are useful, however time-consuming and rely on specialized training and resources. 6 Alternatively, validated CIPN patient-reported outcome (PRO) measures can be incorporated into routine clinical practice settings. The use of the Functional Assessment of Cancer Therapy–Gynecologic Oncology Group–Neurotoxicity questionnaire (FACT-GOG-Ntx) in children ≥11 years of age undergoing chemotherapy has demonstrated strong validity, reliability, and interrater agreement. 7
While the FACT-GOG-Ntx is more sensitive and reliable when compared to the CTCAE, both are limited by their ability to detect CIPN after patients are experiencing symptoms. Novel, validated, objective measures are needed to detect preclinical CIPN earlier, before symptoms become severe and protracted. Biomarkers of axonal damage caused by neurotoxic chemotherapy, including neurofilament light chain (NfL), have recently emerged in the literature. Damage to nerves by neurotoxic chemotherapy leads to the release of these proteins into plasma and cerebrospinal fluid, allowing for the detection of NfL in serum. CIPN biomarkers have the potential to provide additional objective data about early axonal damage leading to CIPN symptoms.8,9
While published evidence is rapidly expanding regarding the promise of NfL to assess CIPN in adults, there are limited data on NfL as a potential biomarker correlating with axonal damage and patient symptoms in patients <18 years of age with cancer. A critical gap exists in our scientific knowledge to identify CIPN in an early and objective manner in adolescent young adults. To address this gap, we evaluated NfL changes from baseline and the relationship of NfL with a CIPN PRO in AYAs receiving neurotoxic chemotherapy.
Methods
Study design
This single-center, prospective study examined AYAs with B-acute lymphoblastic leukemia (B-ALL) or lymphoma who received a chemotherapy regimen that included a tubulin toxin (vincristine, vinblastine, or brentuximab). Patients were eligible if they were (1) between the ages of ≥10–26 years, (2) received a tubulin-toxic chemotherapy agent, and (3) received chemotherapy at Riley Hospital for Children. Enrollment must have been completed <5 days prior to receiving first dose of a tubulin toxin. Patients with preexisting neuropathy were excluded.
Blood samples (6 mL) and FACT-GOG-Ntx were collected from patients at each study timepoint. Study timepoints for patients varied based on disease type and included a baseline blood sample (drawn within 5 days of receiving chemotherapy), day 1 of each new chemotherapy cycle (∼every 4–8 weeks), end of therapy (defined as 6–12 weeks following the last dose of chemotherapy), and every 3 months posttherapy (±3 months) until FACT-GOG-Ntx demonstrated no CIPN symptoms.
All blood samples were processed by clinical research office staff and stored as part of the Indiana Biobank according to standard procedure. NfL was measured in aliquots of the plasma samples using the OLINK PCR assay (PPD Global Central Labs, LLC) with the Target 96 Neuro Exploratory panel (96 proteins), which includes NfL, and using the manufacturer’s recommended protocols. 10 Specifically, proximity extension assay technology used for the OLINK protocol has been well described and enables 92 analytes to be analyzed simultaneously, using 1 µL of each sample. 11 Samples were run in triplicate.
Statistical analysis
Participant characteristics were summarized by diagnosis for all subjects. Categorical variables were summarized as frequencies and percentages, and continuous variables were summarized via medians and ranges.
NfL values were reported as the Normalized Protein eXpression (NPX) per OLINK standard reporting on a log2 scale. Negative NfL values were excluded from percent change calculations. Values were calculated at baseline, the first follow-up, and at 90 days or the closest visit to 90 days.
Percent change from baseline NfL value was calculated at each sample date. The maximum percent change value for each subject was obtained and summarized in a waterfall plot. Due to non-normally distributed differences, the NfL value at the maximum percent change point within the 90 days was compared to the baseline NfL value using the Wilcoxon Signed Rank test.
CIPN was measured via the validated PRO measure FACT-GOG-Ntx in children ≥11 years of age. 7 This 11-item PRO captures CIPN symptom severity. 12 Each item is scored on a 5-point scale (0 = not at all, 4 = very much) with a 7-day recall period. Empirical evidence supports the FACT/GOG-Ntx’s satisfactory reliability, validity, sensitivity to change, and responsiveness to evaluate CIPN in CAYA cancer patients.13,14 Higher scores indicate less CIPN severity. Outcomes were evaluated at each study time point per patient.
Neuropathy scores and NfL values were plotted over time for all individuals. Spearman correlation coefficients were calculated between the percent change in NfL and percent change in FACT-GOG-Ntx score, as well as between NfL value and FACT-GOG-Ntx score. All analyses were performed using SAS version 9.4 (SAS Institute, Inc., Cary, NC, USA). All analytic assumptions were verified, and an α = 0.05 significance level was used for all analyses.
Results
Blood samples and PRO measures were collected from 11 participants; one patient was excluded from NfL analysis due to relapsed disease with preexisting neuropathy. The median age was 17 [range 12–24] years old. The majority of participants were diagnosed with Hodgkin lymphoma (n = 7, 63.6%), male (n = 7, 63.6%), White (n = 9, 81.8%), and non-Hispanic (n = 10, 90.9%). Median baseline NfL levels were 2.2 [range 0.0–6.0], and median baseline FACT-GOG-Ntx was 44.0 [range 37.0–44.0] (Table 1).
Subject Characteristics and Clinical Outcomes
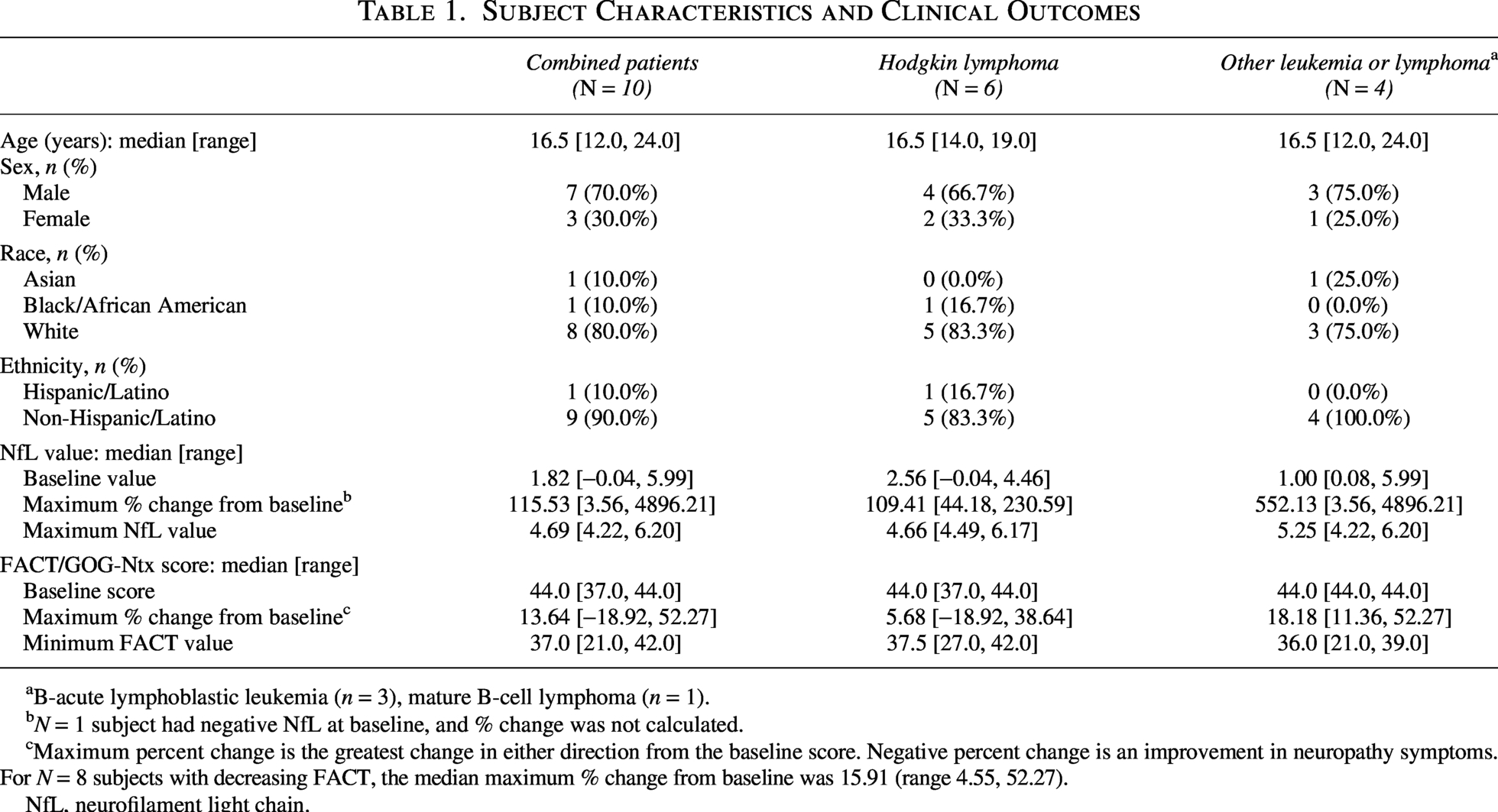
B-acute lymphoblastic leukemia (n = 3), mature B-cell lymphoma (n = 1).
N = 1 subject had negative NfL at baseline, and % change was not calculated.
Maximum percent change is the greatest change in either direction from the baseline score. Negative percent change is an improvement in neuropathy symptoms. For N = 8 subjects with decreasing FACT, the median maximum % change from baseline was 15.91 (range 4.55, 52.27).
NfL, neurofilament light chain.
Overall, NfL levels increased longitudinally throughout the study for all participants, with a median maximum percent change from baseline of 112.5% [range −32.0%−4896.2%] among the 10 participants with a positive baseline NfL value (Table 2). NfL values at the timepoint with maximum percent change significantly differed from baseline NfL (p = 0.004) (Fig. 1). Additionally, NfL values at or before 90 days were significantly different than baseline NfL (p = 0.001) (Fig. 2).
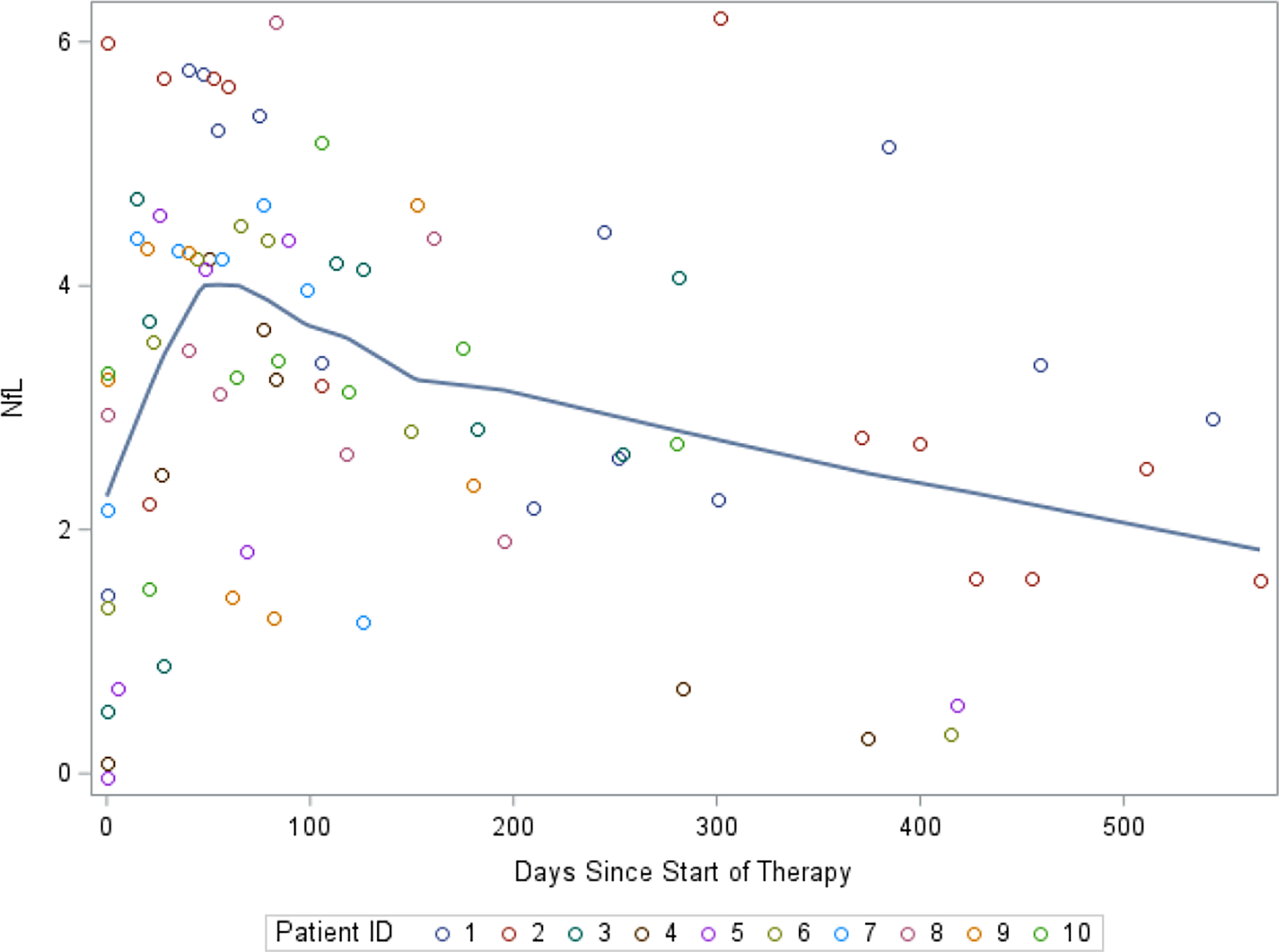
Average neurofilament light chain by subject over treatment course.
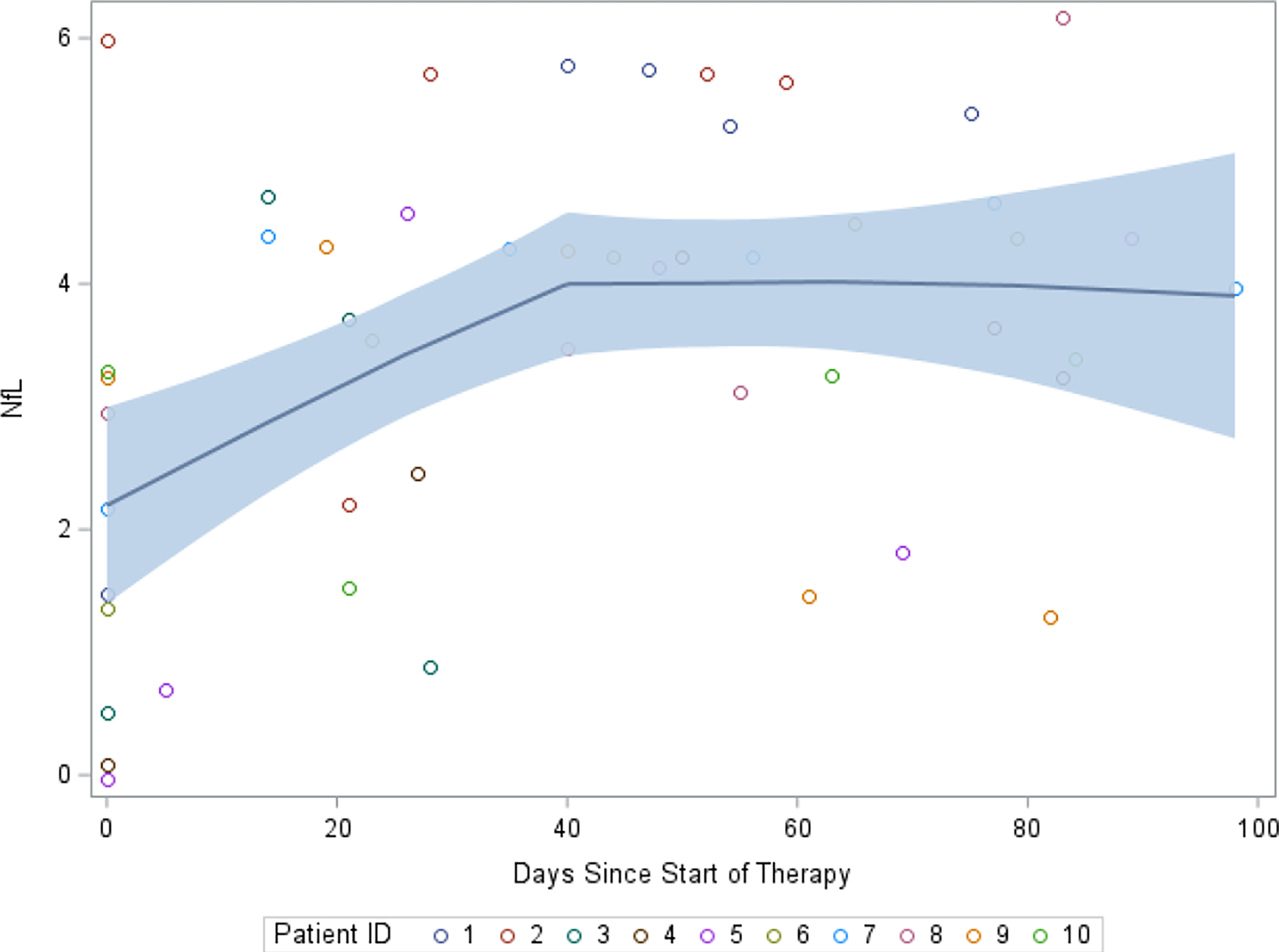
Average neurofilament light chain by subject over treatment course in first 100 days.
Individual Participant Characteristics
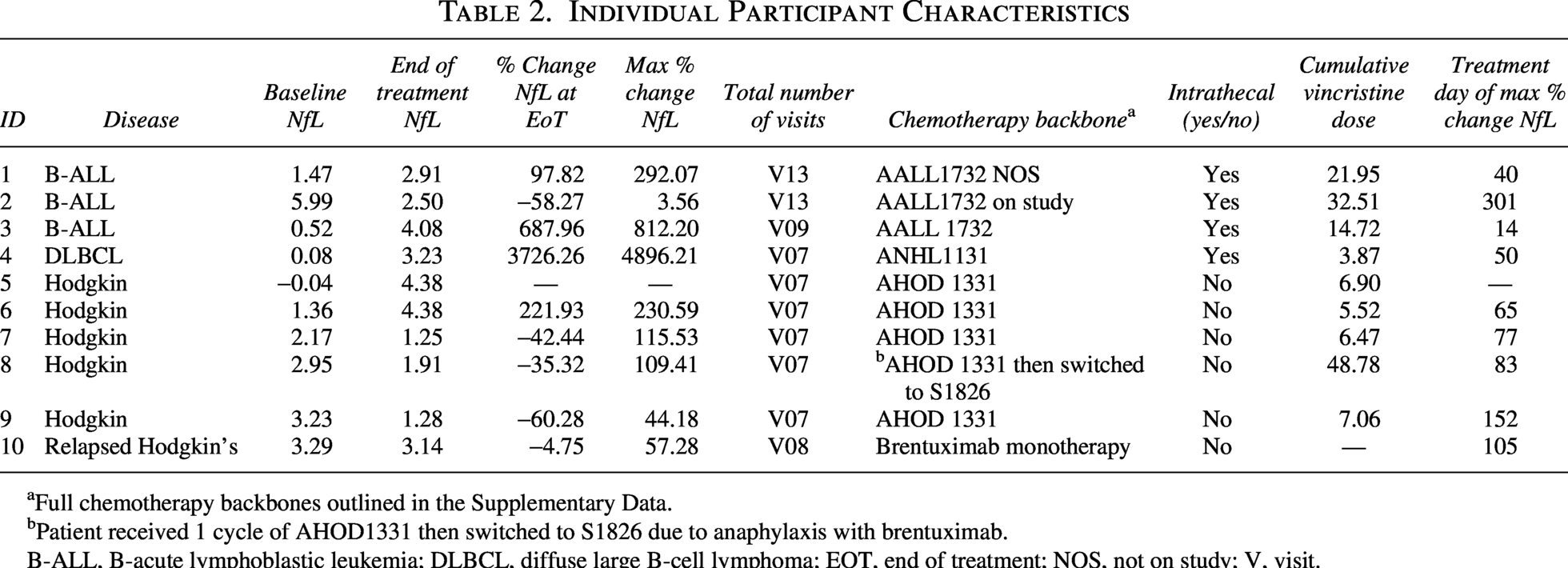
Full chemotherapy backbones outlined in the Supplementary Data.
Patient received 1 cycle of AHOD1331 then switched to S1826 due to anaphylaxis with brentuximab.
B-ALL, B-acute lymphoblastic leukemia; DLBCL, diffuse large B-cell lymphoma; EOT, end of treatment; NOS, not on study; V, visit.
All participants had CIPN as evidenced by increased FACT-GOG-Ntx scores (Table 1). Similar to NfL, most scores (n = 8) worsened over time with a maximum percent change from baseline ranging from 4.5% to 52.3% [median 15.9%]. Two subjects had improved neuropathy.
FACT-GOG-Ntx score was significantly correlated with NfL value both while receiving neurotoxic chemotherapy (r = −0.32, p ≤ 0.01) and postchemotherapy (r = −0.31, p < 0.01). Additionally, change in NfL was significantly correlated with change in neuropathy score (r = −0.45, p < 0.01) during neurotoxic chemotherapy treatment and persisted into survivorship (r = −0.45, p = < 0.01) with higher NfL correlating to lower FACT score and less change in NfL correlating to less change in neuropathy.
Discussion
Similar to data seen in the adult population, we observed changes in NfL from baseline in this AYA oncology population. Furthermore, our data show that changes in NfL significantly correlate with worsening CIPN symptoms that were measured using a well-validated AYA PRO.
Our pilot data suggest that NfL may correlate with the development of neuropathy in AYAs, given that it is responsive to change and was associated with the FACT-GOG-Ntx. NfL increased longitudinally over time and correlated with ongoing exposure to neurotoxic chemotherapy agents, allowing us to hypothesize regarding the timing of NfL release following axonal damage. NfL values were moderately correlated with a well-validated PRO (FACT GOG-ntx), revealing clinically detectable CIPN. Our results are consistent with several published adult studies investigating neurotoxic chemotherapy agents that showed a change in NfL during neurotoxic chemotherapy treatment.9,15,16
NfL could potentially be a more sensitive and specific measure of early axonal damage leading to CIPN compared to current PROs and objective measures, with the potential to detect more subtle changes prior to clinical symptom onset. Neurofilaments are a specific byproduct of axonal injury and thus offer significant advantages over other biomarkers. 17 Adult studies in both animal models and patients had originally demonstrated that NfL concentration can significantly increase in patients with inherited neuropathies secondary to nerve damage.18–21 Meregalli et al. demonstrated the potential of this biomarker in a rat model of CIPN secondary to vincristine. 8 Most recently, Cavaletti et al. studied the assessment of NfL as a biomarker of CIPN in patients aged >18 on the Epiphany trial (NCT03997981) and found a moderate to strong correlation between NfL and CIPN symptoms in patients who received paclitaxel. 9 These results are consistent with prior studies demonstrating a correlation between serum NfL and an increase in CIPN for patients receiving paclitaxel and carboplatin.16,17,22–26
NfL presents a promising option for objective, early detection, potentially allowing for earlier CIPN interventions. Current detection methods for CIPN are insensitive and result in late symptom detection, particularly in children and adolescents. Existing methods for CIPN detection include clinician toxicity grading (CTCAE), patient-reported outcomes such as the FACT-GOG-Ntx, and structured objective clinical assessments including the mTNS, pediatric-modified TNS, cTNS, and TNS-PV. 6 These objective assessments provide important advantages, including structured neurological evaluation and the ability to distinguish sensory and motor dysfunction, but still rely on clinically detectable neuropathic changes once injury has occurred. NfL may serve as a complementary biomarker by identifying axonal injury even earlier, potentially before abnormalities become apparent on formal clinical assessment. Although the FACT-GOG-Ntx has successfully been incorporated into trials for children <18 years of age, it is subject to bias, and in younger children, the test relies on parent reporting on their child’s symptoms. There is a critical need for a feasible point of care, reliable biomarker to detect axonal damage, as this is often the first sign of impending painful CIPN symptoms.
Earlier detection could facilitate timely supportive care interventions, including rehabilitative strategies, before the development of more severe functional impairment.4,5 In addition, the American Society of Clinical Oncology recommends, with moderate evidence, duloxetine in adolescent young adults experiencing painful CIPN. 27 By detecting axonal damage prior to symptom onset, NfL could help patients receive earlier therapy interventions, pharmacologic treatments, and even allow for small, earlier dose reductions of chemotherapy, ultimately improving dose intensity and patient outcomes. Emerging evidence in adults and young adults suggests that preventive strategies such as exercise and sensorimotor training may mitigate CIPN severity, highlighting the potential value of earlier biomarker-guided identification of at-risk patients.28–30 A reliable and accessible biomarker would enable more scientifically rigorous studies, allowing for earlier and more sensitive detection of changes and facilitating the evaluation of interventions with greater precision.
This study has several limitations, most notably a small sample size in a heterogeneous patient population. While we cannot infer a mechanism, these descriptive findings suggest a change in NfL from baseline in patients receiving neurotoxic chemotherapy. Further investigation into factors influencing biomarker variability is needed, including the potential contribution of concomitant neurotoxic exposures such as intrathecal methotrexate, which may independently affect NfL levels given its known central neurotoxicity profile. Additional potential factors influencing NfL may include disease type, adjunct drug interventions, and therapeutic interventions including physical and/or occupational therapy. A larger sample size with homogenous populations is needed in the CAYA patient population to determine the potential use of NfL as a biomarker of CIPN.
Conclusions
We report the early investigation of NfL in the CAYA cancer setting as a potential novel biomarker for early and sensitive CIPN detection. Changes in NfL were detectable early in therapy and were present in those with evidence of CIPN. Results from this pilot study will now serve as the foundation for larger, future studies to continue investigating NfL as an early and objective detection measure of CIPN in the CAYA patient population. The limited evidence of effective, evidence-based treatments for CIPN in CAYAs underscores the need for rigorous clinical trials to discover interventions that can prevent or treat painful peripheral neuropathy side effects.
Data Availability Statement
The data generated in this study are available upon request from the corresponding author.
Supplemental Material
sj-docx-1-jay-10.1177_21565333261464963 — Supplemental material for Neurofilament Light Chain: A Potential Biomarker for Chemotherapy-Induced Peripheral Neuropathy in Adolescent Young Adults
Supplemental material, sj-docx-1-jay-10.1177_21565333261464963 for Neurofilament Light Chain: A Potential Biomarker for Chemotherapy-Induced Peripheral Neuropathy in Adolescent Young Adults by Jennifer A. Belsky, Allie Carter, Michael E. Roth, Audrey Leisinger, Jeffery Dage, Etan Orgel, AnnaLynn M. Williams, Bryan P. Schneider, and Ellen M. Smith
Footnotes
Acknowledgments
The authors are grateful for their generous support, which made this research possible.
Author Disclosure Statement
The authors declare no potential conflicts of interest.
Funding Information
This work was supported by funding from the Indiana University Simon Cancer Center Pilot Funding Program, the Lions Club, and the Heroes Foundation.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.