
Abstract
Purpose:
Adolescents and young adults (AYAs) with cancer are at risk for treatment-related infertility, yet gaps in fertility preservation (FP) counseling persist. While patient-level barriers are well described, provider-level factors remain understudied. We evaluated oncology providers’ perceived versus demonstrated knowledge of FP guidelines and identified barriers to oncofertility care.
Methods:
We conducted a cross-sectional survey of oncology providers at a single academic medical center caring for postpubertal AYA patients receiving gonadotoxic therapy. The survey assessed demographics, prior FP training, counseling and referral practices, and perceived barriers. Participants self-rated their FP knowledge and completed guideline-based clinical vignettes to assess demonstrated knowledge, enabling direct comparison of perceived versus demonstrated knowledge.
Results:
Providers reported limited formal oncofertility training, with most rating prior education as fair or poor. Knowledge varied across FP strategies, with high familiarity for ovarian suppression and sperm cryopreservation and lower familiarity for ovarian transposition and male-directed surgical techniques. A trend toward discordance between perceived and demonstrated knowledge was observed but was not statistically significant. Awareness of institutional FP resources and referral pathways was limited. Providers most frequently cited patient-level barriers, including treatment urgency and cost, although provider- and system-level barriers were also reported.
Discussion:
Oncology providers may overestimate oncofertility knowledge, contributing to inconsistent counseling and missed opportunities for FP. This pattern, combined with gaps in training and awareness of institutional protocols, highlights the need for competency-based education, clearer institutional communication, and improved referral systems. Objective assessments may better identify knowledge gaps and guide targeted interventions to support guideline-concordant FP care.
Introduction
In the United States, approximately 85,000 adolescents and young adults (AYAs) aged 15–39 years are diagnosed with cancer each year. 1 Many are exposed to gonadotoxic therapies (GTTs) that may cause hypogonadism and infertility. 2 Reproductive health is an important quality-of-life measure, and patients experiencing infertility are more likely to experience psychosocial distress characterized by depression, anxiety, and relationship stress. 3 As survival outcomes improve with available therapies, discussions about fertility preservation (FP) should be an integral part of AYA cancer care from the time of diagnosis.
Multiple fertility preservation strategies (FPS) are available. For postpubertal males, sperm cryopreservation remains the standard of care, while testicular tissue cryopreservation is considered experimental. 4 For postpubertal females, oocyte and embryo cryopreservation are established options, 4 and ovarian tissue cryopreservation is an option for those who cannot delay treatment, have contraindications to hormonal stimulation, or have hormone-sensitive malignancies. 5 Gonadotropin-releasing hormone agonists (GnRHa) should not replace established FP methods but may be offered for menstrual suppression for patients with oncologic emergencies requiring urgent therapy and adjunctively in females with breast cancer. 6 National organizations such as the American Society of Clinical Oncology (ASCO), American Society for Reproductive Medicine (ASRM), and Children’s Oncology Group (COG) recommend that all oncology providers discuss potential fertility risks and offer timely referrals to reproductive specialists.4,7 Despite these guidelines, significant variability exists in the consistency, timing, and quality of FP counseling and referrals across settings. 8
Existing research has largely focused on patient-level disparities in fertility counseling, demonstrating that demographic and socioeconomic factors influence whether counseling or referrals occur.7,9–13 Less is known about provider-level factors that contribute to these disparities. Few studies have examined how provider awareness, comfort, and knowledge of FPS affect counseling and referral practices. 14 The extent to which providers’ self-perceived knowledge aligns with their demonstrated knowledge of FPS and relevant guidelines also remains unclear.
This study sought to address this gap by assessing perceived versus demonstrated knowledge of FPS among oncology providers caring for postpubertal AYA patients. We hypothesized that perceived knowledge would exceed demonstrated knowledge, reflecting overconfidence and potential gaps in guideline-based understanding. Secondary objectives included characterizing providers’ counseling and referral behaviors and identifying perceived barriers to providing oncofertility care.
Methods
Study design and setting
This was a cross-sectional study surveying oncology health care providers caring for AYA patients with various malignancies at the University of Chicago Medical Center (UCMC)—an urban, quaternary care facility with an NCI-designated comprehensive cancer center. 15 UCMC also includes Comer Children’s Hospital, a freestanding pediatric acute care hospital. UCMC is home to the Pediatric, Adolescent, and Young Adult Fertility Preservation Program, which was established in 2022 to provide comprehensive multidisciplinary care to young patients to protect their future reproductive health before undergoing cancer therapy. This program offers all FPS that are currently available in the United States, including testicular tissue cryopreservation under research designation. 16
Study population
Eligible participants included attending and fellow physicians, advanced practice providers (APPs), nurses, and pharmacists involved in the care of postpubertal AYA patients receiving GTT. Providers were identified from departmental rosters within the following UCMC divisions: Obstetrics/Gynecology, Pediatric Hematology/Oncology, and Adult Hematology/Oncology—which included subspecialty services including Breast, Gastrointestinal, Head & Neck, Gynecologic, Genitourinary, and Orthopedic Oncology. Recruitment was limited to providers employed at UCMC between October 1, 2024, and May 1, 2025.
Survey instruments and data collection
An electronic survey was developed using UCMC’s Research Electronic Data Capture (REDCap) and distributed via institutional email. Study data were collected and managed also using REDCap.17,18
The survey instrument included the following sections:
Demographics (e.g., gender, race/ethnicity) Provider characteristics (e.g., clinical role, department) Prior FP training: Participants self-reported the amount, type, and perceived quality of prior training, with perceived quality reported using a 5-point Likert scale ranging from poor to excellent. Comfort with FP counseling: Assessed using a 5-point Likert scale ranging from strongly disagree to strongly agree with statements describing specific counseling practices. Practice patterns related to counseling, documentation, and referral: Providers indicated the frequency they engaged in each practice using a 5-point Likert scale from never to always. Perceived barriers to FP counseling and referrals: A list of barriers from prior research was presented,5,6,19,20 and participants were asked to select those they had personally experienced. A space for free-text responses was provided for participants to indicate perceived barriers not included in this list. Perceived knowledge of FP modalities: Participants self-rated their knowledge of each modality using a 4-point Likert scale ranging from not at all knowledgeable to very knowledgeable. Responses were assigned numeric values (1 through 4), and a total knowledge score was calculated as the sum across all responses. Demonstrated knowledge: Two clinical vignettes described hypothetical clinical scenarios in which AYA patients (one male and one female) might qualify for FPS. Participants were asked to select the correct responses for counseling in each scenario. These vignettes were developed by a multidisciplinary team with expertise in AYA oncology and FP and were informed by guidelines from ASCO, ASRM, and COG to ensure clinical relevance and guideline concordance.4,6,7,21 Responses were scored by awarding or deducting one point for each correct or incorrect answer, respectively, generating a composite score for each participant.
Participants were offered a $10 Amazon gift card for survey completion. All survey responses were de-identified and stored securely within REDCap, accessible only to approved study personnel. A waiver of informed consent was granted by the UCMC Institutional Review Board due to minimal risk.
Statistical analyses
Descriptive statistics, including frequencies and percentages, were used to summarize provider demographics, training experiences, and self-reported FP experiences, practices, and knowledge. We explored how providers’ counseling and referral behaviors related to barriers they perceived regarding FP discussions and FPS referral.
To assess our primary outcome of concordance between perceived and demonstrated knowledge of FPS, we first dichotomized perceived and demonstrated knowledge scores into high and low categories using the median scores for each as cutoffs. McNemar’s test was used to assess concordance between binary perceived and demonstrated knowledge scores. Spearman’s rank correlation coefficient and Kendall’s tau were used to assess the association between perceived and demonstrated knowledge scores. All statistical analyses were conducted using R software version 4.0.3, 22 with significance set at p < 0.05.
Results
Demographics
A total of 35 out of 73 eligible respondents completed the survey (48% participation rate). The majority of participants were female (n = 28, 80%) and identified as White (n = 20, 57%) (Table 1). Participants represented a range of oncology specialties, with Adult Hematology/Oncology being the most common (n = 14, 40%). Participants were primarily attending (n = 12, 34%) and fellow (n = 12, 34%) physicians. Other roles included APPs (n = 9, 26%), pharmacists (n = 1, 3%), and nurse navigators (n = 1, 3%). With respect to patient population, most reported that AYAs comprised less than 25% of their practice (n = 14, 40%), while seven (20% of participants) reported more than 75% of their patients were AYAs.
Demographics
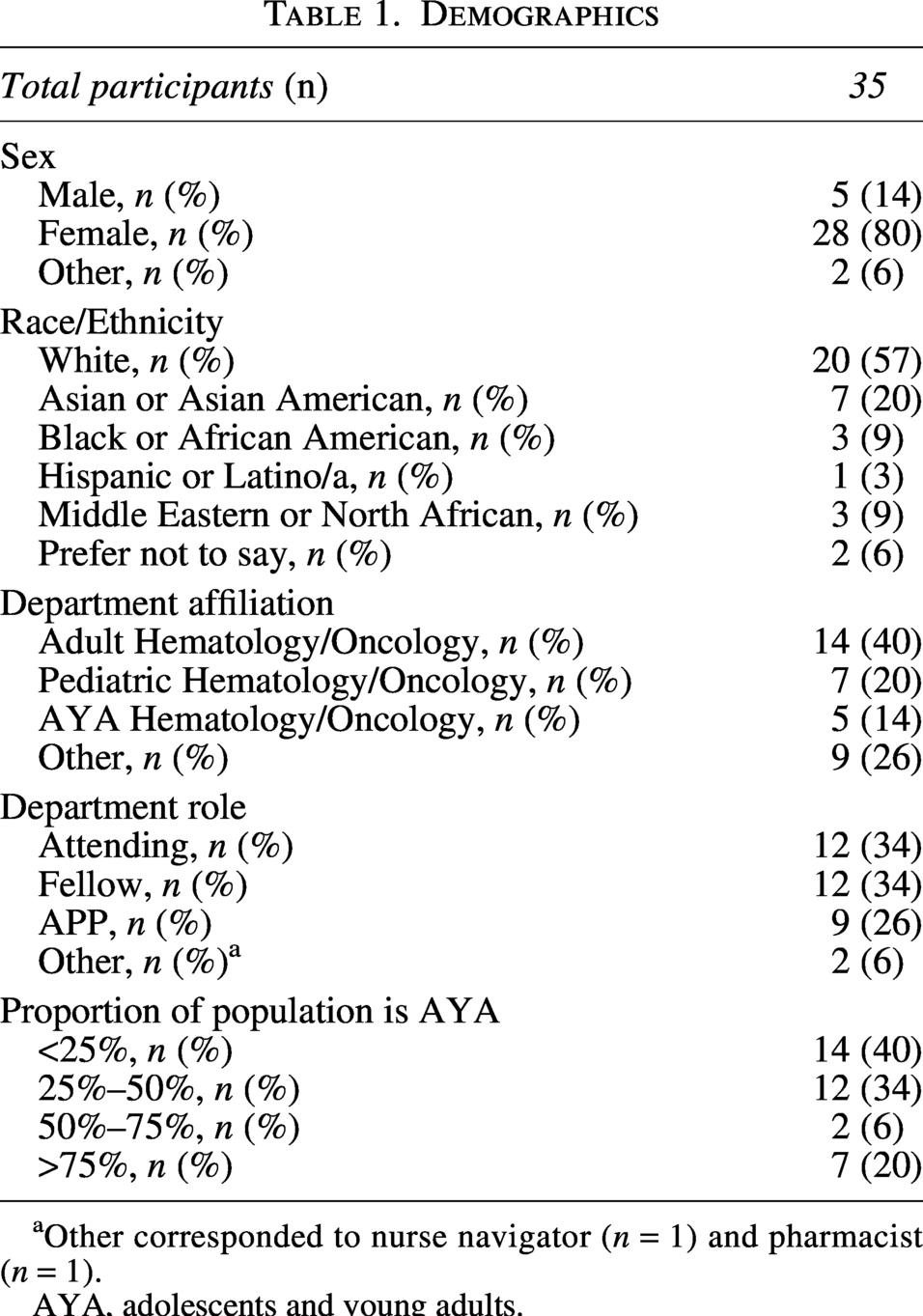
Other corresponded to nurse navigator (n = 1) and pharmacist (n = 1).
AYA, adolescents and young adults.
FP education and training
Most participants reported little or no formal FP training (n = 22, 63%), and training quality was most commonly rated as fair or poor (n = 21, 60%) (Table 2). Educational exposure most frequently occurred through independent reading of scientific literature (n = 23, 66%), with fewer participants citing formal trainee education or continuing medical education (CME). Forty percent (n = 14) reported knowledge of a standardized institutional FP protocol; however, 20% (n = 7) reported no protocol existed, and 34% (n = 12) were unsure or unaware of one.
Education on Fertility Preservation Strategies
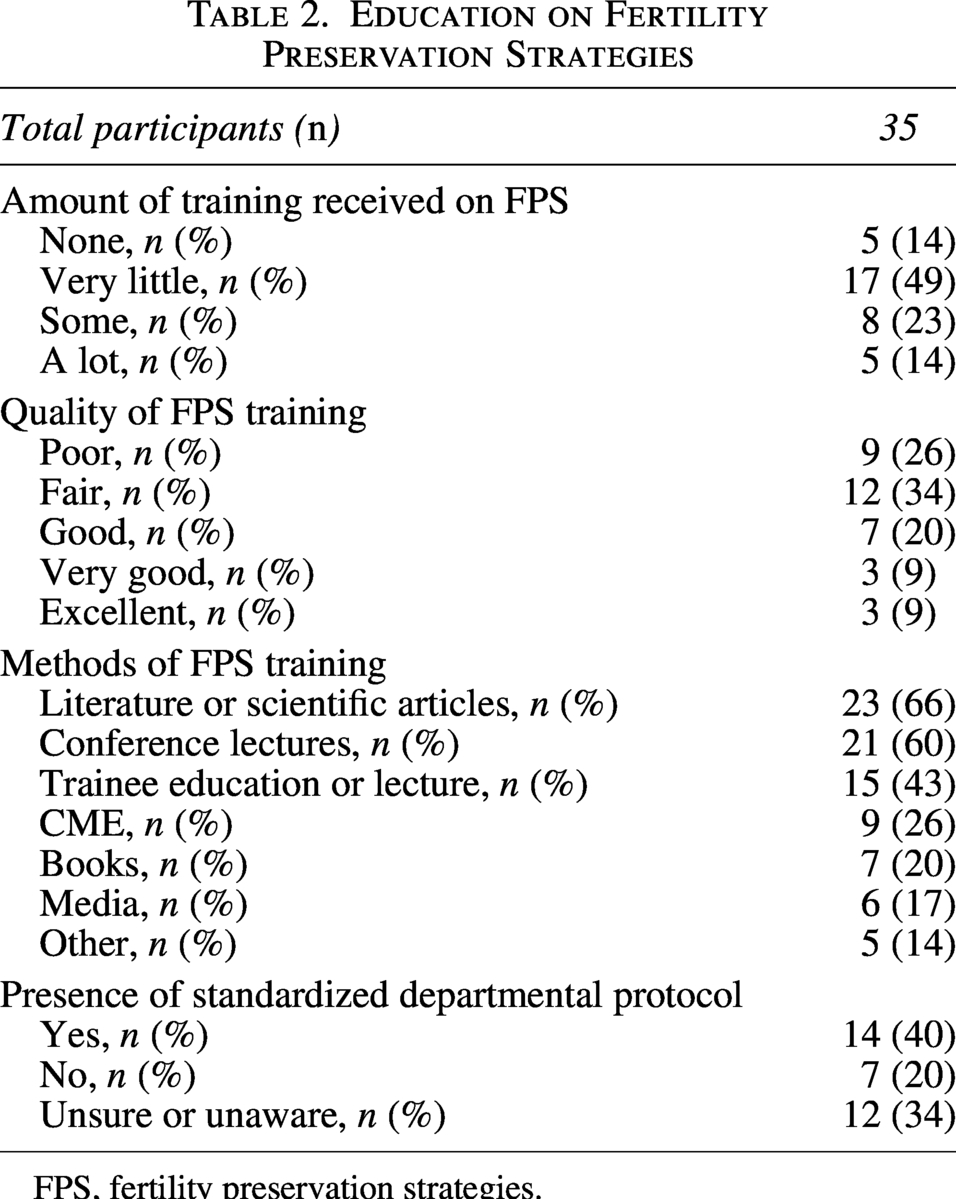
FPS, fertility preservation strategies.
Clinical practice and comfort with FP
Overall, 65% (n = 23) of providers reported comfort in identifying GTT (Fig. 1). Most also felt comfortable counseling both male (n = 23, 65%) and female (n = 20, 57%) postpubertal patients on FP. Referral to FP resources demonstrated the highest reported comfort, with 72% (n = 25) indicating so.
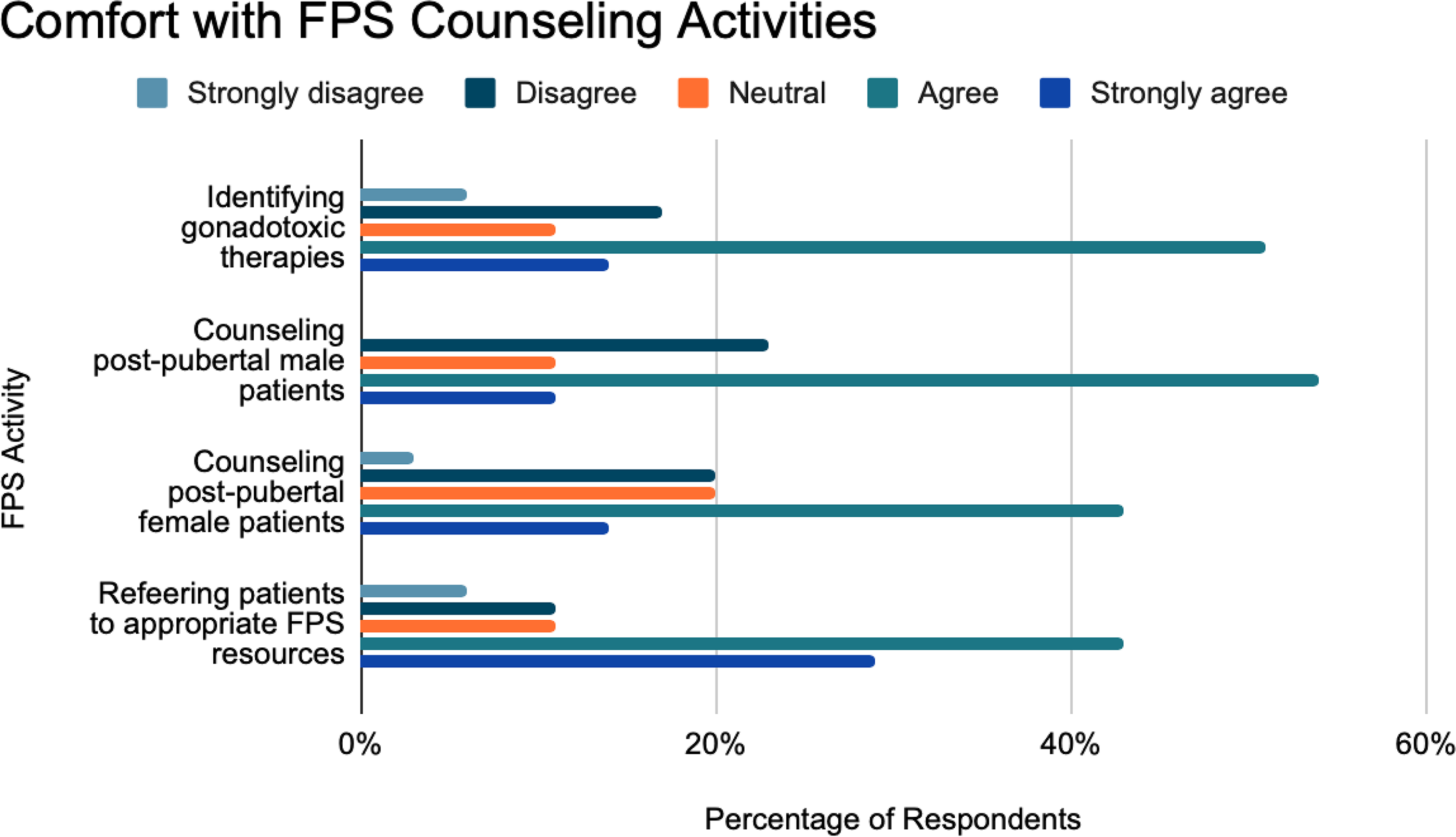
Comfort with FPS counseling activities. FPS, fertility preservation strategies.
Most providers (n = 26, 74%) reported almost always or always assessing the importance of future fertility to patients (Fig. 2). Sixty-two percent (n = 22) reported accounting for fertility desires in treatment planning, and 62% (n = 22) reported routinely discussing potential fertility impacts of disease or treatment. Referral practices were more consistent, with 77% (n = 27) almost always or always referring patients to a fertility specialist, and 69% (n = 24) documenting fertility-related conversations in the electronic medical record (EMR). All three participants who responded “Not Applicable” were APPs.
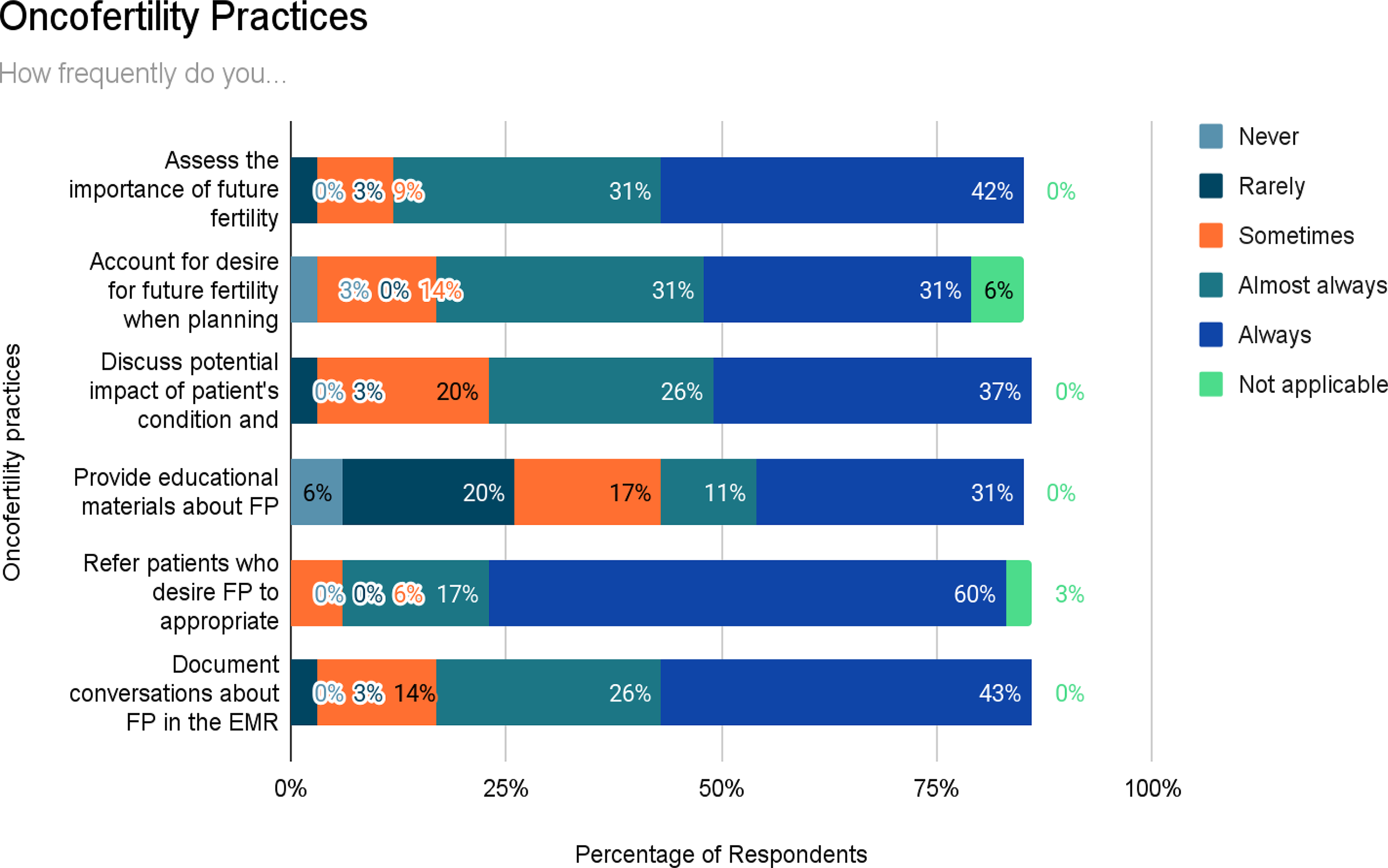
Oncofertility practices. FP, fertility preservation.
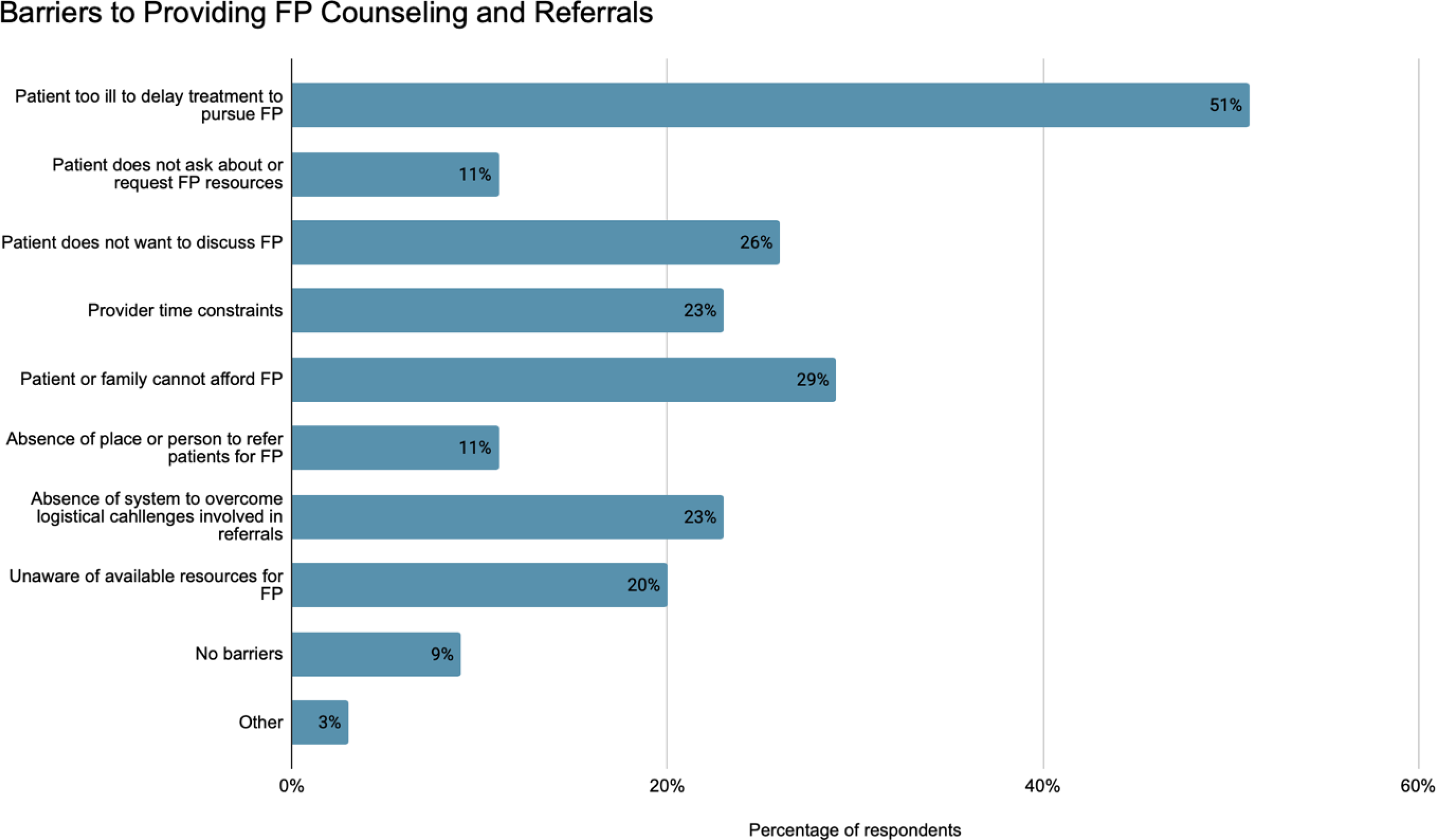
Barriers to counseling and providing FP referrals.
Perceived barriers to providing FP-related care
Participants most frequently cited patient-level factors as perceived barriers to FP, including their perception that patients were too ill to delay treatment (n = 18, 51%) or could not afford FP (n = 10, 29%) (Fig. 3). Provider-level barriers commonly cited included time constraints (n = 8, 23%) and lack of awareness of available FP resources (n = 7, 20%). Four participants (11%) were unaware of referral resources for FP. One provider (3%) cited “Other” barriers, writing that “frequent changes in staffing, availability, and scope of practice contributed to difficulties in offering inpatient reproductive consultations.”
Self-reported perceived FP knowledge
Self-reported knowledge varied across FPS. Percentages reflect respondents reporting feeling knowledgeable or very knowledgeable about various FPS. The greatest proportion reported familiarity with ovarian suppression using GnRHa (n = 22, 63%), sperm cryopreservation (n = 20, 57%), and oocyte cryopreservation (n = 17, 49%) (Fig. 4). In contrast, relatively few respondents reported feeling knowledgeable about ovarian transposition or radiation shielding (14%, n = 5). Familiarity with male-directed surgical techniques, including testicular tissue cryopreservation (n = 8, 23%), testicular sperm extraction (n = 6, 17%), and testicular shielding (n = 3, 9%), was limited.
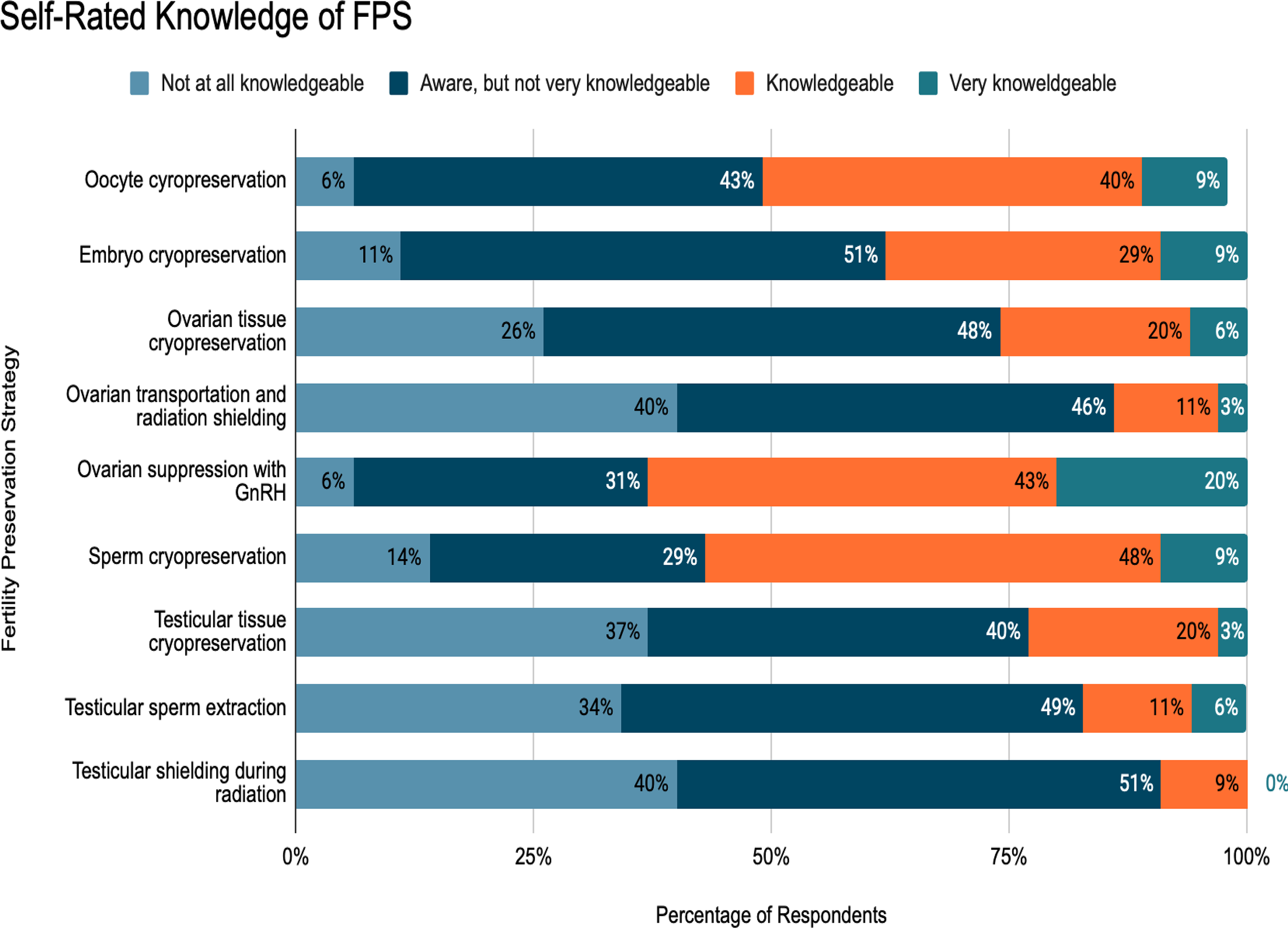
Self-rated knowledge of fertility preservation strategies.
Concordance between perceived and demonstrated FP knowledge
Among 23 participants who completed both perceived and demonstrated FP knowledge assessments, 43% (n = 10) demonstrated both high perceived and demonstrated knowledge, while 17% (n = 4) demonstrated both low perceived and demonstrated knowledge. Discordance was observed in a total of nine cases (39%): Seven (30%) providers perceived their knowledge as high but demonstrated low knowledge, whereas two (9%) perceived their knowledge as low but demonstrated high knowledge. There was no statistically significant difference between perceived and demonstrated knowledge scores (p = 0.18). When analyzed as continuous variables, perceived and demonstrated knowledge scores demonstrated a weak-to-moderate positive correlation that did not reach statistical significance (Spearman’s ρ = 0.35, p = 0.11; Kendall’s τ = 0.25, p = 0.10). Exploratory analyses comparing attending and fellow physicians demonstrated no significant differences in either perceived FP knowledge (p = 0.34) or demonstrated knowledge scores (p = 0.66).
Discussion
In our study of oncology provider-level barriers to FP care at a large academic institution, providers reported limited formal education in oncofertility and demonstrated gaps in awareness of institutional FP resources, resulting in providers overestimating their knowledge. These findings are especially notable given that our study was conducted at a quaternary-level academic center with an established multidisciplinary oncofertility program. Although national guidelines emphasize timely FP counseling and referral, there is less guidance on provider education and institutional communication strategies.6,21 Focusing on both areas may improve delivery of guideline-concordant oncofertility care.
One prominent observation in this study was the discordance between perceived and demonstrated knowledge of FPS. A substantial proportion of providers rated their knowledge as high despite demonstrating lower knowledge scores on vignette-based assessments. Although not statistically significant, the observed pattern suggests a tendency toward overestimation of knowledge. While several studies have evaluated oncology providers’ attitudes and self-reported knowledge regarding FP, to the best of our knowledge, this is the first study to directly compare perceived knowledge with objectively assessed oncofertility knowledge using clinical vignettes or other similar assessment tools.14,23,24 Duffy et al. reported that oncologists frequently expressed moderate confidence in their understanding of fertility issues among young patients with cancer. 24 Our findings build on this literature by objectively measuring FPS knowledge using guideline-concordant clinical vignettes. The observed discordance has important implications. Overestimation of knowledge may contribute to incomplete counseling or missed opportunities to discuss guideline-supported FPS. Objective assessment tools, such as vignette-based evaluations, may better identify knowledge gaps and inform targeted oncofertility education initiatives.
Limited formal education and training in FP likely contribute to existing provider knowledge gaps. In this study, nearly two-thirds of providers reported little or no formal training in oncofertility, and the quality of prior training was most often rated as fair or poor. These findings are consistent with prior studies, which have demonstrated that oncofertility care providers receive limited theoretical and practical education in this field during medical training.24–26 The lack of consistent and high-quality educational experiences may lead to providers feeling inadequately prepared to navigate complex fertility counseling scenarios. This need for education is particularly important given the variability in exposure to AYAs. While many respondents reported that AYAs comprised less than a quarter of their practice, one-fifth reported that AYAs represented the majority of their patient population. This variability suggests that even providers who encounter AYAs less frequently must maintain familiarity with FP guidelines and referral resources. Foundational oncofertility education is necessary for oncology providers to ensure that all patients, regardless of where they receive care, have access to timely and guideline-concordant fertility counseling. Oncofertility education could be strengthened by the use of more interactive learning opportunities, such as simulation-based learning and case-based workshops.
Another notable finding was providers’ limited awareness of institutional FP programming and resources, despite the presence of an established multidisciplinary FP program offering the full spectrum of currently available FPS. Our program follows a team-based model in which the primary oncology team initiates fertility discussions and completes a standardized referral form, after which a dedicated FP team performs risk stratification to guide referral and procedure-specific recommendations based on patient characteristics. Fewer than half of respondents reported awareness of a standardized institutional FP protocol, while a majority either believed no protocol existed or were unsure. Additionally, when asked about barriers to providing FP care, several providers reported not knowing where or to whom to refer patients for FP services or were simply unaware of available resources for FP. Similar gaps in awareness of FP resources and referral pathways have been described.14,27 These findings suggest that the presence of FP programs alone may be insufficient if referral pathways and available services are not clearly, broadly, and repeatedly communicated to frontline oncology care team members. Improving provider education through structured curricula, interdisciplinary training, and case-based learning may help to mitigate knowledge gaps, while clearer institutional protocols and referral pathways may increase awareness of available FP resources.
Regarding perceived barriers, participants most frequently cited patient-level barriers to FP care, including perceptions that patients were too ill to delay treatment or unable to afford the cost of FP. The predominance of these explanations may reflect a tendency to externalize barriers, attributing missed FP opportunities primarily to patient circumstances rather than to provider- or system-level factors. Patient-level challenges have been well described in prior literature examining disparities in access to FPS, where factors such as treatment urgency, cost, insurance coverage, socioeconomic status, and other demographic factors may influence whether patients pursue FP.9–12 However, provider-level factors, such as lack of familiarity with FP guidelines, limited training in oncofertility counseling, and uncertainty regarding referral pathways, also significantly influence whether FP discussions take place.14,27 Pairing rigorous and multidisciplinary educational initiatives with standardized referral pathways and clear institutional protocols can ensure consistent FP counseling and reduce the risk that knowledge gaps and overconfidence contribute to disparities in access to FP care. Integrating FP counseling into routine oncology workflows, such as through EMR prompts or standardized documentation templates, may improve the consistency of FP discussions, reinforce completion of referral processes, and encourage coordination with FP teams to reduce disparities through system-level interventions.
Our study has several limitations. First, the study was conducted at a single academic institution, which may limit generalizability to community or nonacademic settings with different resources and referral infrastructure. However, the study included a diverse cohort of adult, pediatric, and AYA oncology providers across multiple specialties, allowing us to capture a broad range of perspectives and experiences within a single center. Second, the overall response rate was modest, and participation may have been subject to selection bias, as those with greater interest or awareness of oncofertility may have been more likely to participate. Third, the small sample size may have limited the statistical power to detect significant differences between perceived and demonstrated knowledge and precluded multivariable analysis of demographic or specialty-level predictors. Despite this limitation, to the best of our knowledge, this is the first institutional assessment of its kind to directly compare oncology providers’ perceived versus demonstrated knowledge of FPS using case-based clinical vignettes grounded in national FP guidelines. While vignette-based assessments provide a more objective measure of knowledge than self-report alone, they may not fully capture real-world clinical decision-making or interdisciplinary collaboration that occurs in practice. In addition, these vignettes were not subjected to formal psychometric validation or external pilot testing. Vignette-based evaluations, however, offer a practical, standardized approach to evaluating provider knowledge and guideline familiarity that would otherwise be difficult to measure objectively, underscoring the need for future work to formally validate vignette-based assessment tools.
In summary, we demonstrate that oncology providers report limited formal training in oncofertility and demonstrate gaps in awareness of institutional FP resources, which may contribute to overestimation of FP knowledge. Addressing these gaps through competency-based education and improved institutional communication may help ensure that AYAs receive timely, guideline-concordant counseling regarding fertility risks and preservation options. Future studies should evaluate provider educational interventions and competency assessments and expand this work across multiple institutions—including community and safety-net settings—to determine whether similar knowledge and training gaps exist across practice environments. Qualitative studies involving provider interviews or focus groups may further clarify contextual barriers and facilitators not captured by surveys. Ultimately, aligning provider knowledge and clinical practice with national guidelines is essential to ensure that AYAs undergoing GTT have the opportunity to make informed, patient-centered decisions about their future fertility.
Authors’ Contributions
A.D.K. contributed to conceptualization, data curation, investigation, methodology, project administration, visualization, and writing of the original draft. S.M.L. contributed to data curation, formal analysis, methodology, provision of analytical resources, and writing—review and editing. L.F.S. contributed to conceptualization, funding acquisition, investigation, methodology, project administration, supervision, and writing—review and editing.
Data Availability Statement
Article data, analytic methods, and study materials are included in the main article and Supplementary Data.
Ethics Approval Statement
The study protocol was approved by the Institutional Review Board of the University of Chicago.
Patient Consent Statement
This study involved survey responses from health care providers and did not include patient participants or protected health information. The institutional review board approved the study with a waiver of informed consent.
Footnotes
Acknowledgments
The authors are grateful to the providers who participated in this study for their time and valuable contributions. They also thank Dr. Austin Wesevich for his assistance.
Author Disclosure Statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding Information
L.F.S. receives support from the U.S. Department of Defense (
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.