
Abstract
Relevance:
Adolescents and young adults (AYAs) diagnosed with cancer represent a particularly vulnerable group with unique developmental, psychosocial, and functional challenges. Beyond survival, improving health-related quality of life (HRQoL) has become a major priority in cancer survivorship and public health.
Purpose:
This umbrella review aimed to critically synthesize evidence from existing systematic reviews and meta-analyses evaluating the effectiveness of physical, psychosocial, and mixed interventions for improving HRQoL and related health outcomes in AYA (e.g., cancer-related fatigue, anxiety, and physical functioning) cancer patients and survivors.
Methods:
A comprehensive search of PubMed/MEDLINE, Web of Science, Cochrane Database of Systematic Reviews, and ScienceDirect identified eligible systematic reviews and meta-analyses published between 2015 and 2025.
Results:
Fifteen reviews were included. Physical activity interventions showed the most consistent moderate benefits, particularly in reducing fatigue and improving physical functioning and domain-specific HRQoL. Psychosocial interventions demonstrated small-to-moderate improvements in anxiety, depression, and emotional well-being. Mixed interventions showed promising but less robust evidence, particularly due to limited long-term follow-up. Overall evidence certainty ranged from low to moderate. Primary study redundancy was minimal (the corrected covered area = 1.7%).
Conclusions:
Psychosocial interventions, especially exercise-based and psychosocial programs, can improve key HRQoL domains in AYAs with cancer. However, more rigorous long-term studies are required, particularly for combined and digital approaches.
Keywords
Introduction
Cancer remains one of the leading causes of morbidity and mortality worldwide and represents a major global public health and sociomedical challenge. According to the GLOBOCAN 2022 estimates prepared by the International Agency for Research on Cancer of the World Health Organization, approximately 20 million new cancer cases and nearly 10 million cancer-related deaths were reported globally in 2022. Projections indicate that, by 2050, the annual number of new cancer diagnoses may reach 35 million, reflecting an increase of more than 70% compared with 2022. 1 These trends underscore the need not only to advance treatment modalities but also to adopt a comprehensive approach to the long-term consequences of cancer and survivorship.
Modern oncology is increasingly focused not only on survival outcomes but also on health-related quality of life (HRQoL) as a key endpoint of cancer care. Cancer and its treatment can substantially affect patients’ physical, psychological, and social functioning, leading to chronic fatigue, reduced physical activity, emotional distress, anxiety and depressive symptoms, as well as impairments in social adaptation, such as difficulties in reestablishing peer relationships, achieving educational milestones, or transitioning to independent living.2,3 Accumulating evidence suggests that diminished quality of life may persist for many years after completion of active treatment. 4
A particularly vulnerable subgroup of oncology patients consists of adolescents and young adults (AYAs), typically defined as individuals aged 15–39 years. 5 Global analyses for 2022 indicate that approximately 1.3 million new cancer cases and around 378,000 cancer-related deaths occurred among AYAs worldwide. 6 This developmental period is characterized by intense physical, psychological, and social transitions, including identity formation, educational attainment, career initiation, establishment of intimate relationships, and family planning.7,8 A cancer diagnosis during this critical life stage may severely disrupt these processes and result in long-term adverse consequences for quality of life. 9
Fertility and sexual health concerns are increasingly recognized as some of the most significant survivorship issues among adolescents and young adults with cancer, substantially affecting long-term quality of life. Previous studies have shown that up to 68% of young female cancer survivors report sexual dysfunction, while approximately 58% experience considerable reproductive concerns.10,11 These challenges are closely linked to key developmental processes characteristic of this life stage, including identity formation, body image adaptation, establishment of intimate relationships, and future family planning.12,13 Although clinical guidelines such as those issued by National Comprehensive Cancer Network and American Society of Clinical Oncology recommend discussing fertility preservation and sexual health from the time of diagnosis, these topics often remain insufficiently addressed in routine oncology care.14,15 Consequently, there is growing recognition of the need for specialized psychosocial interventions, including digital and self-guided supportive programs, aimed at reducing distress and improving long-term psychosocial adjustment and social functioning among AYA cancer survivors.16,17
Studies demonstrate that AYA patients and cancer survivors frequently experience a unique spectrum of challenges, including pronounced psychological distress, social isolation, difficulties in returning to education or employment, and persistent physical limitations.18,19 Compared with pediatric or older adult cancer populations, AYAs more often report unmet supportive care needs and lower HRQoL. Therefore, quality of life in this population has become a priority outcome in both clinical and research programs. 20
In response to these challenges, a wide range of interventions aimed at improving HRQoL and functional outcomes among AYA cancer patients and survivors has been actively developed and implemented in recent years. These include psychosocial, physical, and behavioral approaches designed to reduce psychological distress, increase physical activity, enhance social adaptation, and promote healthy lifestyle behaviors.21,22 Such interventions are increasingly recognized as essential complements to standard oncology treatment and survivorship care, particularly given the long-term sequelae of cancer.
Numerous systematic reviews and meta-analyses have examined interventions for AYAs with cancer. However, substantial variation in focus, intervention approaches, outcomes, and methodological quality limits the ability to derive coherent conclusions or inform practice and guideline development. Given this fragmentation, higher-level evidence synthesis is needed. An umbrella review provides an appropriate framework by integrating findings across reviews, evaluating their quality, and identifying gaps in the literature. 23 Such a synthesis is both timely and necessary to clarify the current evidence base and inform future research priorities in AYA oncology.
The aim of the present umbrella review is to provide a comprehensive analysis, critical appraisal, and integration of evidence from existing systematic reviews and meta-analyses addressing psychosocial, physical, and mixed interventions for AYA cancer patients and survivors.
Materials and Methods
This umbrella review was conducted in accordance with international methodological standards for overviews of reviews, including the PRIOR (Preferred Reporting Items for Overviews of Reviews) guideline and adapted elements of PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) for umbrella review methodology. The protocol was registered in PROSPERO (CRD420261283397). The main methodological steps included the following:
Inclusion and exclusion criteria for reviews
Included reviews
Systematic reviews and meta-analyses published between 2015 and 2025 that evaluated interventions targeting individuals diagnosed with cancer during adolescence or young adulthood (commonly 15–39 years) or reported extractable data for this subgroup. Addressing psychosocial, physical, behavioral, and mixed interventions aimed at improving HRQoL. Published in English in peer-reviewed scientific journals.
Excluded reviews
Primary studies (Randomized Controlled Trials [RCTs], cohort, cross-sectional studies, etc.) unless they were part of a systematic review or meta-analysis. Nonsystematic reviews (e.g., narrative reviews lacking a clearly defined search methodology). Reviews that did not report AYA-specific data or did not allow extraction of findings relevant to the AYA population or comparable subgroups.
Information sources and search strategy
A comprehensive literature search was conducted in the following electronic databases: PubMed/MEDLINE, Web of Science, Cochrane Database of Systematic Reviews, and ScienceDirect.
In addition, reference lists of included reviews were screened manually. The search strategy incorporated combinations of key terms such as “adolescents and young adults,” “cancer survivors,” “systematic review,” “meta-analysis,” “health-related quality of life,” “psychosocial intervention,” “physical interventions,” “dietary interventions,” and “digital interventions.”
Search strategies were adapted for each database and included both controlled vocabulary (MeSH terms) and free-text keywords.
Data extraction, quality assessment, and synthesis of results
A standardized extraction form developed in Microsoft Excel was piloted and refined prior to use. Extracted information included publication characteristics, population definitions, intervention components, outcome domains, and quantitative findings when available.
Data extraction was performed independently by two reviewers. Discrepancies were resolved through discussion, with involvement of a third reviewer when necessary.
The comparative impact of interventions was assessed by extracting data on key indicators of change reported in the included reviews, including standardized mean differences (SMDs), 95% confidence intervals (CIs), and p values for statistical significance. We evaluated intervention effectiveness primarily through comparisons with control groups (e.g., standard care or wait-list) and pre–post intervention outcomes as described in the source reviews. Clinical significance was interpreted based on the magnitude of effect sizes and the authors’ qualitative synthesis of domain-specific improvements.
Methodological quality assessment
The methodological quality of included systematic reviews and meta-analyses was evaluated independently by two reviewers using the AMSTAR-2 tool (A Measurement Tool to Assess Systematic Reviews), a validated and widely applied instrument for assessing the quality of health care intervention reviews. Each included review was assessed across 16 domains and was classified as high, moderate, low, or critically low. Disagreements between reviewers were resolved through discussion until agreement was reached. 24
Robustness of outcome results assessment
To evaluate the strength and reliability of the cumulative evidence, the robustness of outcome results was assessed using an adapted GRADE (Grading of Recommendations Assessment, Development, and Evaluation) approach as established by Guyatt et al. (2008). 25 This classification was achieved by evaluating five specific domains: risk of bias (assessed via AMSTAR-2), inconsistency of findings, indirectness, imprecision, and publication bias. Judgments regarding these criteria were independently performed by two authors (P.A. and L.I.) through a consensus-based process to ensure objectivity. Robustness was categorized into four levels: high, moderate, low, or very low. 25
Assessment of primary study redundancy
Primary study redundancy in an umbrella review occurs when the same primary studies are included in multiple systematic reviews. This can lead to the “double counting” of data and potentially biased results.
To quantify this, we used the corrected covered area (CCA) method proposed by Pieper et al. (2014) 26 :
CCA = (Nr − Np)/[Np × (N − 1)], where Nr (occurrences)—refers to the total count of primary studies as they appear across all included systematic reviews; Np (unique investigations) is defined as a single, discrete primary research study (e.g., a specific randomized controlled trial), regardless of how many reviews cite it; and N—indicates the total number of included reviews.
Example: If one specific randomized controlled trial (unique investigation) is included in three different systematic reviews within our analysis, it is counted as one unique study (Np) but as three occurrences (Nr). Identifying unique investigations is essential to avoid the “double counting” of participant data in the final synthesis.
According to the thresholds established by Pieper et al. (2014), 26 CCA values are interpreted as follows: 0%–5% indicates slight redundancy, 6%–10% moderate, 11%–15% high, and >15% very high redundancy. 26 новый.
Results
Characteristics of included reviews
A total of 15 systematic reviews and meta-analyses published between 2016 and 2025 were included in this umbrella review. These reviews evaluated the effectiveness of interventions aimed at improving HRQoL and associated outcomes among AYAs who have experienced cancer.
Initially, 17 reviews were considered eligible; however, full texts for two potentially relevant publications were unavailable despite attempts to contact the authors. Therefore, the final synthesis was based on 15 reviews.
Distribution of reviews by intervention type
The included reviews were classified into the following categories:
Physical interventions (n = 6): Reviews primarily focusing on structured exercise and physical activity programs27–32; Psychosocial interventions (n = 5): Reviews examining psychological support, behavioral (psychosocial) interventions33–37; Mixed interventions (n = 4): Reviews addressing combined approaches, including physical activity with dietary components, as well as technology-assisted psychosocial interventions delivered through digital platforms.38–41
The PRISMA flow diagram describing the process of review identification and selection is presented in Figure 1.
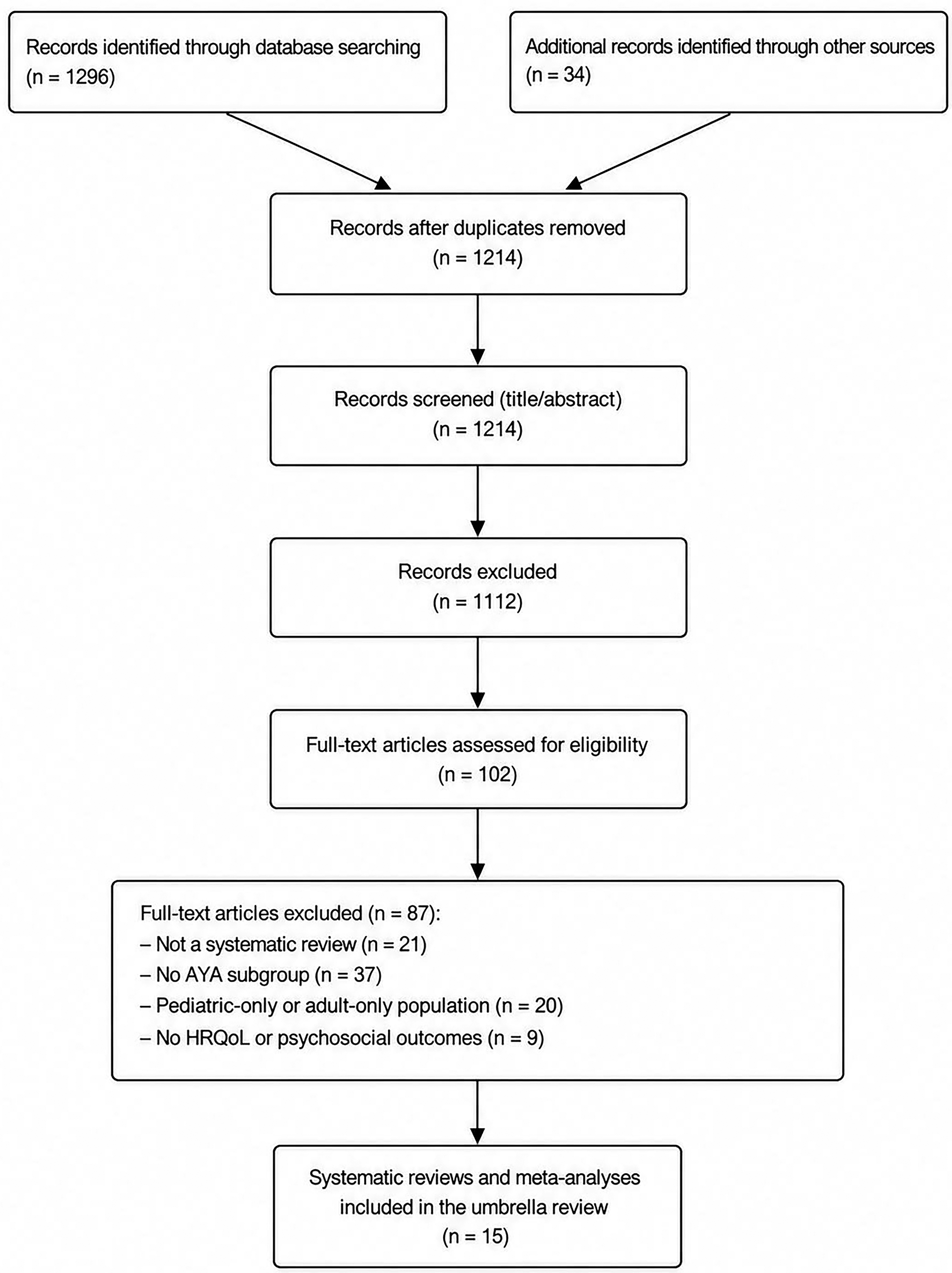
Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagram of the identification, screening, eligibility assessment, and inclusion of systematic reviews and meta-analyses in the present umbrella review. AYA, adolescents and young adults; HRQoL, health-related quality of life.
Population characteristics and geographic scope
Most included reviews addressed the AYA population, most commonly defined as individuals aged 15–39 years, although in several studies, the age boundaries varied and included adolescent, pediatric, and young adult groups.
Geographically, the evidence base was drawn predominantly from North America (the United States, Canada), Europe (the United Kingdom, Germany, the Netherlands), and Asia (China, South Korea). Detailed characteristics are presented in Table 1.
Characteristics of Included Systematic Reviews and Meta-Analyses Evaluating Interventions in Adolescents and Young Adults Oncology
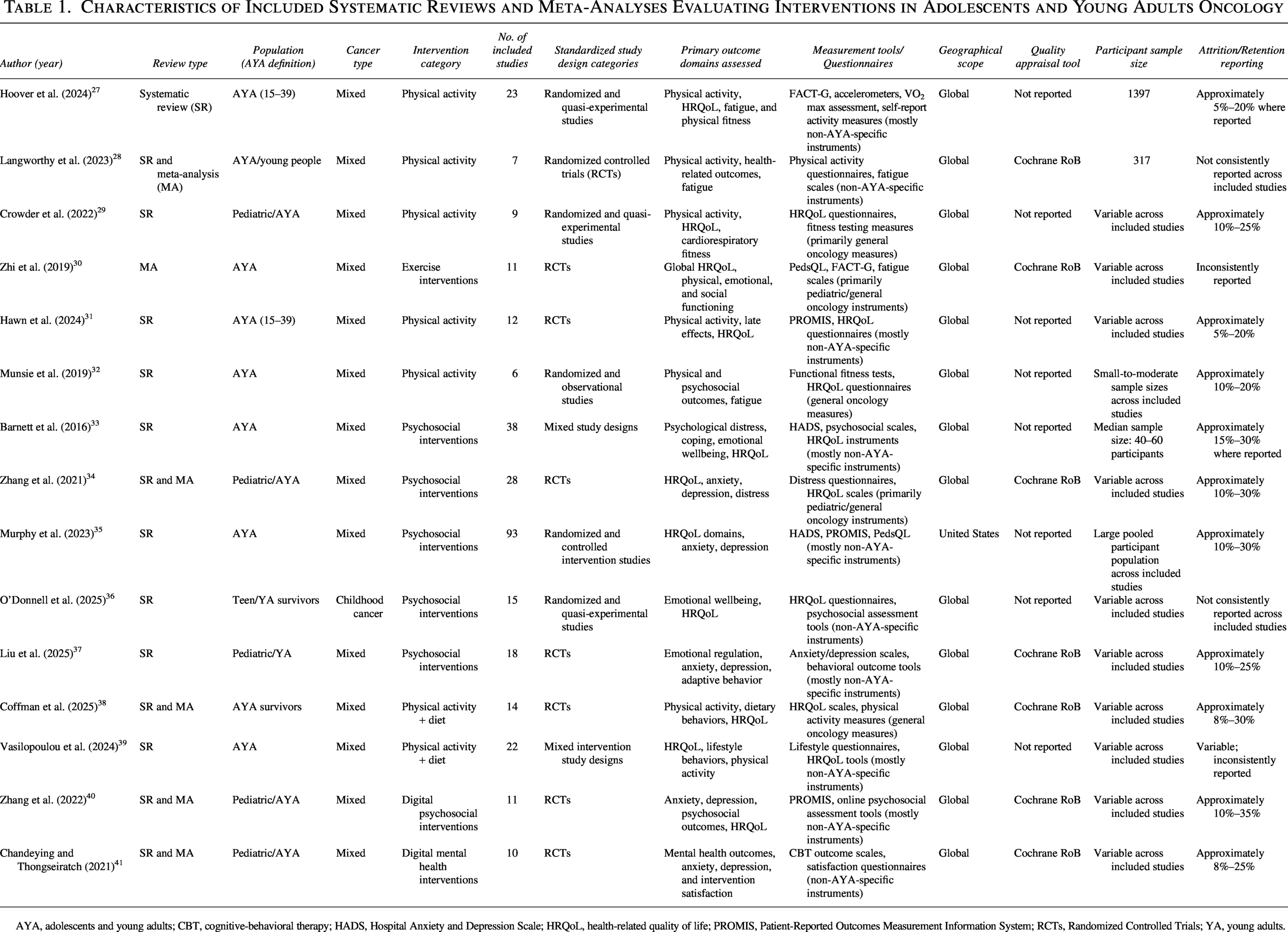
AYA, adolescents and young adults; CBT, cognitive-behavioral therapy; HADS, Hospital Anxiety and Depression Scale; HRQoL, health-related quality of life; PROMIS, Patient-Reported Outcomes Measurement Information System; RCTs, Randomized Controlled Trials; YA, young adults.
Methodological quality assessment
Methodological quality assessment using the AMSTAR-2 tool demonstrated the following distribution of robustness ratings (Table 2):
Methodological Quality of the Included Reviews According to AMSTAR-2 Classification
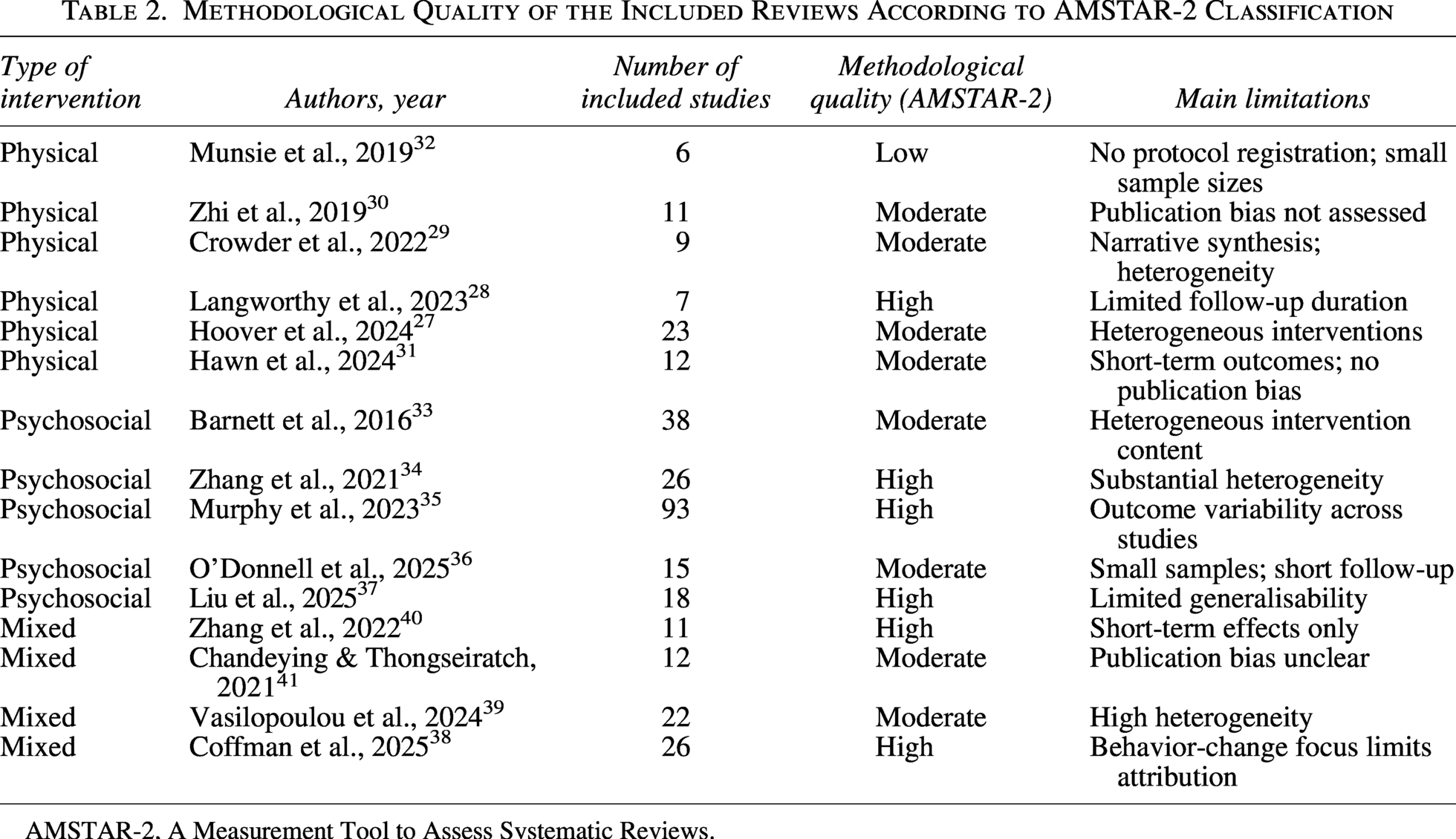
AMSTAR-2, A Measurement Tool to Assess Systematic Reviews.
High quality: 3 reviews (20%)
Moderate quality: 6 reviews (40%)
Low quality: 4 reviews (26.7%)
Critically low quality: 2 reviews (13.3%)
Common limitations included a lack of protocol registration, insufficient assessment of publication bias, and incomplete reporting of excluded studies.
Redundancy of primary studies
In our analysis of 15 reviews, we identified 214 occurrences of primary studies (Nr) corresponding to 173 unique investigations (Np) (discrete primary studies). The calculated CCA was 0.017 (1.7%). This indicates a low level of redundancy, confirming that the synthesis is based on diverse evidence bases with minimal risk of double counting.
Hierarchy and types of outcomes assessed
The impact of the reviewed interventions was measured using several associated indicators. Across the included meta-analyses, effectiveness was predominantly determined by effect sizes (SMD) and statistical significance (p < 0.05) relative to control groups. While this review synthesizes the evidence for physical, psychosocial, and mixed interventions, it does not provide a direct statistical head-to-head comparison between these categories but rather evaluates their independent contribution to HRQoL domains.
In this umbrella review, outcomes were categorized based on their clinical relevance, public health significance (i.e., their impact on health care resource utilization and social reintegration), and a temporal assessment perspective, which involves evaluating effects across different time frames, including short-term, medium-term, and long-term outcomes (≥12 months).
The primary outcome was HRQoL, including global scores and domain-specific measures (physical, emotional, and social functioning). These endpoints are central for evaluating supportive care needs in AYA populations.
Secondary outcomes comprised psychological indicators (anxiety, depression, distress, coping), physical activity and functional performance, and behavioral measures such as adherence and self-efficacy.
Most evidence referred to short- and medium-term effects (≤6 months). Data on long-term outcomes (≥12 months) were scarce.
Overall, findings were more consistent for domain-specific HRQoL and mental health outcomes than for global HRQoL or sustained long-term effects.
Physical interventions
Six systematic reviews and meta-analyses evaluated the effects of physical activity and structured exercise programs on physical, psychosocial, and health-related outcomes among AYAs living with and beyond cancer27–32 (Table 3).
Summary of Main Outcomes and Key Findings Across Included Intervention Categories
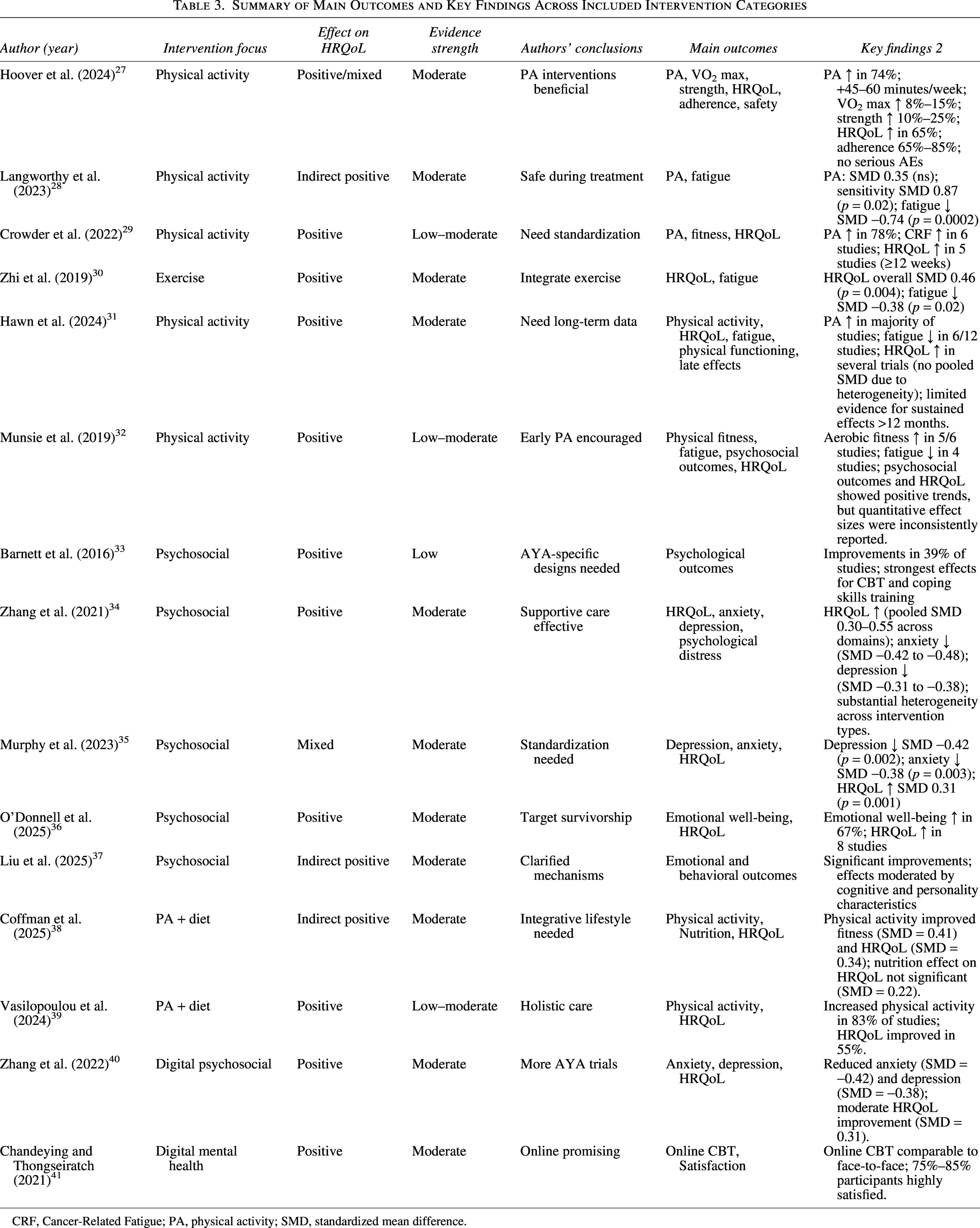
CRF, Cancer-Related Fatigue; PA, physical activity; SMD, standardized mean difference.
Characteristics of physical interventions
The reviews encompassed diverse exercise modalities, including aerobic, resistance, combined programs, yoga, and flexibility training. Delivery formats varied from supervised individual or group sessions to home-based and digitally supported approaches. Interventions typically lasted 6 weeks to 12 months, with 2–5 sessions per week, each 30–60 minutes, and progressive intensity. Overall, physical interventions showed generally positive effects on physical activity levels and functional performance among AYAs with cancer.
Hoover et al. (2024) 27 synthesized evidence from 23 studies involving 1397 participants and reported that 74% of the included trials (17 out of 23) observed statistically significant improvements in physical activity. Outcomes were measured via FACT-G, accelerometers, and VO2 max assessments. These instruments were largely non-AYA-specific. Reported attrition rates ranged from 5% to 20%. On average, moderate-intensity exercise increased by around 45–60 minutes per week. Positive changes were also documented in functional fitness outcomes: VO2 max increased by 8%–15% in 12 studies, and muscle strength gains ranged from 10% to 25%. Furthermore, improvements in HRQoL were identified in 15 studies (65%), most consistently within the physical functioning domain. Program adherence ranged from 65% to 85%, and no serious adverse events were reported. 27
In the meta-analysis by Langworthy et al. (2023 28 ; 7 RCTs, n = 317), the primary analysis did not identify a statistically significant effect of physical interventions on physical activity (SMD = 0.35; 95% CI: −0.39 to 1.09; p = 0.35). However, sensitivity analyses restricted to high-quality RCTs yielded a statistically and clinically significant effect (SMD = 0.87; 95% CI: 0.17–1.57; p = 0.02). Reduction in cancer-related fatigue emerged as one of the most consistent and reproducible outcomes, with a moderate effect size observed (SMD = −0.74; 95% CI: −1.13 to −0.35; p = 0.0002). Outcomes were measured via physical activity questionnaires and fatigue scales (general measures). Attrition was not consistently reported across the included primary studies. 28
Crowder et al. (2022 29 ; 9 studies with variable sample sizes) found that 7 out of 9 studies (78%) reported significant increases in physical activity. HRQoL questionnaires and fitness testing (primarily general oncology measures) served as the primary tools. Attrition rates were approximately 10%–25%. Cardiorespiratory endurance improved in six studies, and HRQoL improved in five studies, particularly when intervention duration exceeded 12 weeks. 29
The meta-analysis by Zhi et al. (2019 30 ; 11 studies with variable sample size) demonstrated a significant improvement in overall HRQoL (SMD = 0.46; 95% CI: 0.15–0.77; p = 0.004). PedsQL, FACT-G, and fatigue scales, which are pediatric or general cancer questionnaires, were used. Data on dropout rates were reported inconsistently. Domain-specific analyses showed the largest effect in physical functioning (SMD = 0.52), with moderate improvements in emotional (SMD = 0.38) and social functioning (SMD = 0.31). Fatigue was also moderately reduced (SMD = −0.38; 95% CI: −0.71 to −0.05; p = 0.02). 30
In the systematic review by Hawn et al. (2024 31 ; 12 studies with variable sample size), consistent positive effects of physical interventions were observed among AYAs with cancer. Increased physical activity was reported in 67% of included studies, while improvements in HRQoL were identified in 58% of studies. Reductions in fatigue were observed in 50% of studies. Outcomes were measured via Patient-Reported Outcomes Measurement Information System (PROMIS) and various HRQoL questionnaires (mostly non-AYA-specific). Attrition was estimated at 5%–20%. Most effects were small to moderate in magnitude (SMD ≈ 0.20–0.45). The authors emphasized that evidence regarding the long-term sustainability of intervention effects remains limited, as studies with follow-up periods beyond 12 months were rare and did not allow firm conclusions about the persistence of benefits over time. 31
Similarly, Munsie et al. (2019 32 ; 6 studies with small-to-moderate sample sizes) reported that physical activity interventions exerted beneficial effects on both physical and psychosocial outcomes during active cancer treatment and after treatment completion. Improvements in physical fitness and endurance were observed in five out of six studies, fatigue reduction in four studies, and positive effects on HRQoL in three studies. Effect sizes ranged from small to moderate (SMD ≈ 0.25–0.60). Outcomes were assessed through functional fitness tests and HRQoL questionnaires (general measures). Attrition rates ranged from 10% to 20%. 32
Summary of feasibility and sample size
Across the six reviews of physical interventions, the final aggregate sample sizes ranged from small-to-moderate cohorts in individual trials to large pooled populations exceeding 1300 participants. The attrition rates for this category generally ranged from 5% to 25%, although reporting was inconsistent across several primary studies.
Taken together, evidence from the included systematic reviews and meta-analyses suggests that physical interventions produce moderate positive effects on fatigue reduction and improvements in physical functioning among AYAs with cancer. Effects on overall physical activity levels and HRQoL are generally favorable but more variable, depending on study quality and intervention duration. Long-term outcomes beyond 12 months remain insufficiently studied.
Interpretation of physical intervention findings is limited by heterogeneity in program design, small samples, brief follow-up, and non-AYA-specific measures, with continuing uncertainty regarding optimal parameters, durability of benefits, and subgroup effects.27,29,31,32
Psychosocial interventions
Five included reviews focused on psychosocial and psychological interventions aimed at improving mental well-being, social adjustment, and quality of life among AYAs who have experienced cancer33–37 (Table 3).
Characteristics of psychosocial interventions
The included systematic reviews and meta-analyses encompassed a broad range of psychosocial interventions, including cognitive-behavioral therapy (CBT), coping skills training, psychoeducational programs, individual and group-based psychological support, as well as remote and digital intervention formats. These interventions were implemented both during active treatment and throughout survivorship, with substantial variability in intensity, duration, and delivery mode.
In their systematic review of 38 studies with a median sample size of 40–60 participants, Barnett et al. (2016) 33 noted that approximately two-fifths (39%) of the included investigations reported improvements in psychological outcomes. The strongest effects were observed for CBT-based interventions and coping skills training programs. Overall, psychosocial intervention effects were generally small to moderate in magnitude (SMD ≈ 0.30–0.50). Assessment relied on Hospital Anxiety and Depression Scale (HADS) and psychosocial scales (mostly non-AYA-specific). Attrition rates were reported between 15% and 30%. The authors highlighted limitations in long-term outcome data, as most studies involved only short follow-up periods, restricting assessment of sustained effects over time. 33
The meta-analysis by Zhang et al. (2021) demonstrated small-to-moderate but statistically significant positive effects of psychosocial interventions on HRQoL and psychosocial outcomes in pediatric, adolescent, and young adult cancer survivors. Analyzed 28 studies with variable sample size using distress questionnaires and HRQoL scales (pediatric/general instruments). Attrition rates were approximately 10%–30%. The pooled effect size across domains was approximately SMD ≈ 0.45 (p < 0.001), while HRQoL improvements varied between SMD 0.30 and 0.55 across different domains. Significant reductions in anxiety (SMD −0.42 to −0.48) and depressive symptoms (SMD −0.31 to −0.38) were also reported. However, substantial heterogeneity across intervention types was noted, and effects were less pronounced in the AYA subgroup compared with younger pediatric populations. 34
In the large meta-analysis by Murphy et al. (2023; 93 studies with a large combined sample), psychosocial interventions were associated with statistically significant reductions in depressive symptoms (SMD = −0.42; 95% CI: −0.68 to −0.16; p = 0.002) and anxiety (SMD = −0.38; 95% CI: −0.62 to −0.14; p = 0.003), as well as improvements in overall HRQoL (SMD = 0.31; 95% CI: 0.12–0.50; p = 0.001). Measurement tools included HADS, PROMIS, and PedsQL (non-AYA-specific). Attrition rates ranged from 10% to 30%. 35
The systematic review by O’Donnell et al. (2025; 15 studies with variable sample size) demonstrated the predominantly positive impact of psychosocial interventions on the emotional well-being of AYAs who had cancer in childhood and adolescence. Improvements in emotional well-being were documented in 10 out of 15 studies (67%), and 8 studies also reported HRQoL improvements, suggesting potential clinical relevance of these supportive approaches. Tools included HRQoL questionnaires and psychosocial assessment instruments. Attrition was not consistently reported. 36
In the meta-analysis by Liu et al. (2025; 18 RCTs with variable sample size), psychosocial interventions produced statistically significant improvements in emotional and behavioral outcomes. Outcomes were assessed using anxiety/depression scales and behavioral outcome tools (mostly non-AYA-specific). Attrition rates were between 10% and 25%. Most RCTs reported reductions in anxiety and depressive symptoms, alongside enhanced emotional regulation and adaptive behaviors. Effect sizes ranged from SMD ≈ 0.35 to 0.70, with larger effects observed for multicomponent interventions tailored to participants’ cognitive and personality characteristics, emphasizing the importance of individualized program adaptation. 37
Summary of feasibility and sample size
For psychosocial interventions (five reviews), sample sizes varied from small groups (median 40–60 participants) to large pooled datasets in meta-analyses. The observed attrition rates ranged from 10% to 30%, with higher drop-out rates frequently noted in programs with longer durations or those requiring sustained psychological engagement.
Taken together, evidence from systematic reviews and meta-analyses indicates that psychosocial interventions provide small-to-moderate but clinically meaningful improvements in psychological outcomes and quality of life among AYAs with cancer. The most consistent benefits are observed for reductions in depression, anxiety, and improvements in emotional well-being, particularly when structured approaches such as CBT and coping-focused interventions are applied. However, variability in effects and the influence of individual participant characteristics (e.g., age, baseline distress levels, and cognitive or personality traits) underscore the need for personalized research.
For psychosocial interventions, limitations include rare use of HRQoL as a primary endpoint, inconsistent measurement, short observation periods, and risk of bias. Risk of bias was identified based on methodological limitations reported in the included reviews, such as lack of protocol registration, insufficient assessment of publication bias, and heterogeneity in study designs.33,35,36
Mixed interventions
Four systematic reviews and meta-analyses examined combined intervention approaches, including physical activity and dietary interventions, as well as technology-assisted psychosocial interventions delivered through digital platforms38–41 (Table 3).
Physical activity and dietary intervention characteristics
Coffman et al. (2025), 38 which included 26 studies with variable sample size, reported that interventions targeting physical activity produced significant improvements in physical fitness (SMD = 0.41; 95% CI: 0.22–0.60; p < 0.001) and HRQoL (SMD = 0.34; 95% CI: 0.15–0.53; p < 0.001). The effect of dietary interventions on HRQoL was comparatively weaker and failed to achieve statistical significance in pooled analyses (SMD = 0.22; 95% CI: −0.05 to 0.49; p = 0.11). The assessment was carried out using HRQoL scales and physical activity measures (general oncological measures). The dropout rate was 8%–30%. 38
Vasilopoulou et al. (2024), including 22 studies with variable sample size, confirmed the positive impact of physical activity: 83% of studies reported increased activity levels, and HRQoL improvements were observed in 55% of studies. These findings suggest a more robust and consistent benefit of exercise-based interventions compared with interventions focusing solely on nutrition. Lifestyle questionnaires and HRQoL tools (not specific to AYAs) were used. Dropout rates varied and were reported inconsistently. 39
Overall, physical activity interventions demonstrate predominantly favorable effects on participant activity levels, whereas evidence supporting dietary components remains limited. Behavior change techniques (BCTs) appear to play a central role in achieving intervention effects; however, more integrated nutritional approaches are needed to enhance effectiveness.
Characteristics of digital psychosocial interventions
The meta-analysis by Zhang et al. (2022 40 ; 11 studies with variable sample size) showed that technology-assisted psychosocial interventions effectively reduced anxiety (SMD = −0.42) and depression (SMD = −0.38) while moderately improving HRQoL (SMD = 0.31). Outcomes were assessed using PROMIS and online psychosocial tools. Attrition rates were higher in this category, ranging from 10% to 35%. 40
Chandeying and Therdpong (2021 41 ; includes 10 RCTs with variable sample size) demonstrated that online CBT achieved effects comparable to face-to-face therapy in terms of clinical outcomes (e.g., reductions in anxiety and depression), while 75%–85% of participants reported high satisfaction, reflecting the acceptability of the intervention. Outcomes were assessed via CBT scales and satisfaction questionnaires. Attrition rates were approximately 8%–25%. 41
Summary of feasibility and sample size
Mixed and digital interventions (four reviews) exhibited highly variable sample sizes. The attrition rates in this category were the most pronounced, ranging from 8% up to 35%. While digital platforms showed high participant satisfaction (75%–85%), they also faced significant challenges in maintaining long-term engagement.
Overall, digital psychosocial interventions provide moderate positive effects on mental health and HRQoL, with some outcomes comparable in effectiveness to in-person approaches. However, most available evidence has been generated in pediatric populations, while data specific to AYAs remain limited. Intervention effectiveness appears enhanced when digital programs incorporate interactivity, personalization, and adequate technical support.
Evidence for mixed approaches remains restricted by scarce long-term data, intervention variability, and limited understanding of adherence and implementation barriers.38–41
Robustness of outcome results assessment
The robustness of outcome results was determined using an adapted GRADE framework. 25 Following this approach, two reviewers (P.A. and L.I.) independently evaluated the cumulative evidence across five key domains: risk of bias (incorporating AMSTAR-2 ratings), inconsistency of findings, indirectness, imprecision, and publication bias.
Based on this assessment, the most robust evidence base was observed for physical and psychosocial interventions, both demonstrating moderate robustness of outcome results. These interventions showed relatively consistent effects across several HRQoL domains, particularly physical functioning, fatigue, anxiety, and depressive symptoms.
However, the robustness of findings was reduced by several methodological limitations of the included reviews, including heterogeneity of interventions, variability in outcome measurement instruments, and limited follow-up durations.
For mixed interventions and technology-supported psychosocial interventions, the robustness of outcome results was assessed as low because of the limited number of reviews, variability in study designs, and insufficient evidence regarding long-term effectiveness.
Overall, the robustness of cumulative outcome results across intervention categories ranged from low to moderate, suggesting potentially beneficial effects of psychosocial and physical interventions while emphasizing the need for additional high-quality research specifically focused on the AYA oncology population. The overall robustness assessment based on the adapted GRADE framework is summarized in Table 4.
Certainty of Evidence Across Intervention Types Based on the Adapted Grading of Recommendations Assessment, Development, and Evaluation Approach
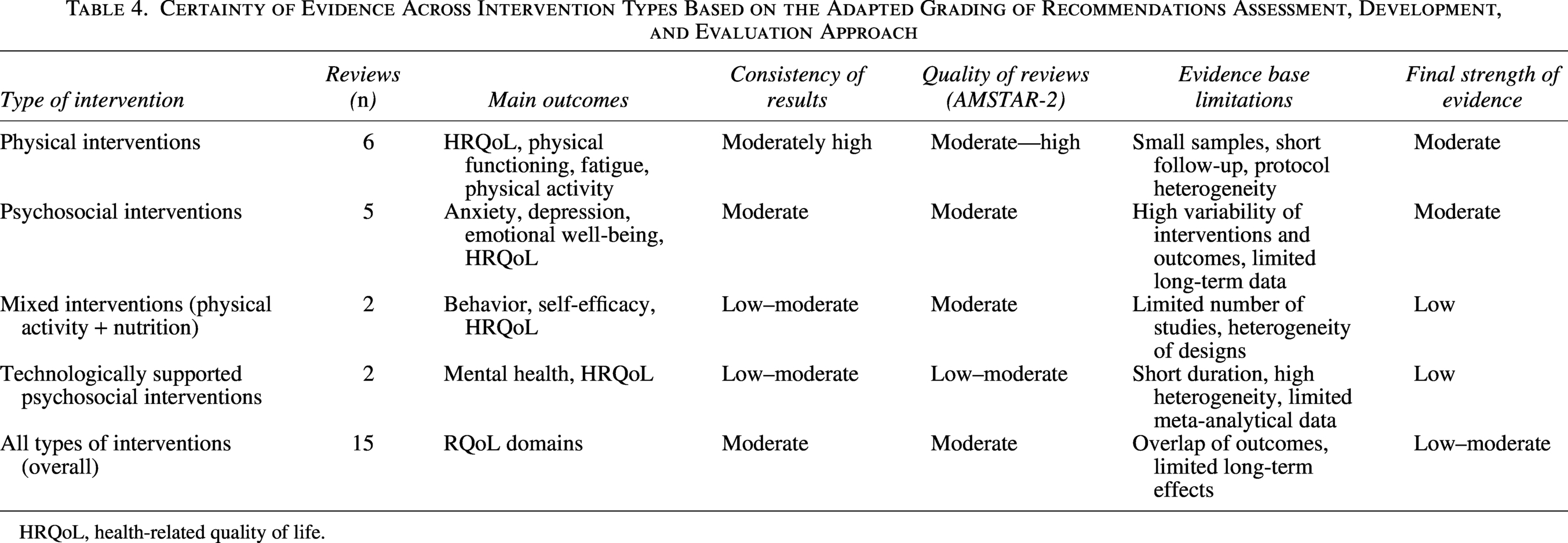
HRQoL, health-related quality of life.
Discussion
This umbrella review synthesizes evidence from systematic reviews and meta-analyses evaluating physical, psychosocial, mixed interventions targeting HRQoL in AYAs with cancer. By integrating heterogeneous interventions and outcomes, the review reduces fragmentation in the literature and provides a consolidated picture of effectiveness across HRQoL domains. From a public health perspective, this approach is critical because it informs scalability (i.e., the capacity to expand effective local programs to regional or national health care levels) and integration into psychosocial intervention programs, such as by embedding automated digital screening tools for distress into routine clinical care to trigger immediate referrals. The results offer clear strategies to reduce long-term population burden (i.e., the cumulative societal and economic impact of chronic disability and late effects in survivors). It also highlights needs specific to AYAs, such as the necessity for developmentally tailored programs that address identity and peer integration, which are often overlooked in general oncology services.
Physical activity–based interventions showed the most consistent evidence of benefit, particularly for physical functioning, fatigue, and emotional well-being. Meta-analyses indicate statistically significant and system-relevant improvements—those that significantly reduce health care resource utilization, such as decreasing the frequency of outpatient clinic visits or unplanned hospital readmissions. 30 These results align with broader oncologic rehabilitation literature emphasizing the role of physical activity as a key component of long-term supportive care and secondary prevention of functional limitations among AYA cancer survivors.36,42 Nevertheless, the sustainability of exercise effects over time and their influence on recurrent health episodes (e.g., secondary malignancies, chronic treatment–related late effects, or disease relapse) require further investigation, alongside the development of programs that account for both individual capacities and health care system resource constraints.
Psychosocial interventions yielded positive outcomes across emotional and psychological domains, including significant reductions in anxiety, depression, and distress.34,43 Such findings underline their relevance for mitigating long-term psychosocial consequences at the population level. Yet global HRQoL effects were heterogeneous and frequently nonsignificant. 35 Differences in intervention content, theoretical orientation, timing, and baseline burden (the preexisting severity of psychological or physical symptoms before starting the intervention) likely explain this variability.
Mixed and behavior-focused approaches, which incorporate specific BCTs such as goal setting, self-monitoring, and action planning to modify health habits (e.g., increasing physical activity measured via accelerometers or self-reports), demonstrated encouraging but less stable effects. Standardizing these outcomes according to the measurement tools used (e.g., using PedsQL or FACT-G for HRQoL) allows for a more robust comparison of intervention efficacy across different studies.34,44 Although firm conclusions cannot be drawn, these models may represent valuable multilevel strategies targeting modifiable determinants of health, supporting the development of adaptive and personalized programs.
Feasibility and retention challenges
A cross-categorical analysis revealed that attrition rates varied from 5% to 35%. Physical activity programs generally demonstrated lower dropout rates compared to psychosocial and digital interventions, potentially due to the supervised nature of many exercise regimens. The high attrition observed in digital interventions (up to 35%) highlights significant implementation barriers, such as digital fatigue or a lack of sustained interactivity, which may limit the scalability of these programs in routine clinical care.
Technology-supported interventions appear feasible and scalable, particularly for AYAs with reduced access to face-to-face care. Electronic and mobile-based programs demonstrated small-to-moderate statistically significant improvements, primarily within specific mental health domains.43,45 Nevertheless, long-term and global HRQoL benefits remain uncertain, with many reviews reporting nonsignificant pooled effects.35,45 Digital access, privacy, and sustained engagement remain major implementation challenges.
Across intervention categories, psychosocial and digital strategies most strongly influenced emotional and social outcomes during active treatment, 43 whereas physical domains responded more reliably to exercise during survivorship.30,43 This differentiation has implications for planning rehabilitation and reintegration pathways.
Evidence consistently indicates that HRQoL in AYAs is shaped by developmental processes such as identity formation, autonomy, peer integration, fertility, and transition into adulthood,20,46 yet many interventions lack explicit developmental grounding. Incorporating development-informed and intersectoral models spanning health care, education, and social support may enhance sustainability of benefits.47,48
Interpretation is further complicated by heterogeneity in measurement and reporting. Reliance on global HRQoL indicators may obscure domain-specific or developmentally meaningful changes.35,49 Public health frameworks therefore advocate standardized, age-appropriate tools, including PROMIS-based systems, to support comparability and surveillance across care phases.20,49,50
The evidence base is additionally limited by variable bias risk (e.g., lack of blinding in exercise trials or incomplete reporting of attrition data), few high-quality trials, short follow-up, and inconsistent reporting of implementation and adherence.34,35 Inclusion of broader age ranges in some reviews may dilute AYA-specific effects, reinforcing the need for targeted research.
From an organizational and public health viewpoint, current findings support embedding structured exercise and psychosocial support within comprehensive AYA care models, consistent with existing guidance.51,52 However, limited direction on tailoring interventions to specific HRQoL domains reveals a persistent gap between evidence synthesis and real-world delivery.
Future priorities include developmentally informed frameworks, multimodal programs, rigorous trials with longer follow-up, standardized and consistent outcome measurement approaches, and stronger attention to implementation, equity, and access, including digital delivery.35,49,53 Achieving these goals will require interdisciplinary collaboration and meaningful involvement of AYA communities.
Strengths and limitations of the review
The strengths of this umbrella review include its broad coverage of the available evidence base, incorporating systematic reviews and meta-analyses examining physical, psychosocial, mixed, and digital interventions aimed at improving HRQoL among AYAs with cancer. The umbrella review approach enabled integration of findings across heterogeneous intervention types and provided a comprehensive overview of the effectiveness of supportive care programs within the AYA population. Methodological rigor was enhanced through the formal quality appraisal of included reviews using the AMSTAR-2 tool, as well as assessment of evidence certainty via an adapted GRADE approach, thereby increasing the interpretability of findings in the context of health care decision-making. In addition, the degree of primary study redundancy across included reviews was evaluated. The calculated CCA was 1.7%, indicating a low level of redundancy. This suggests a minimal risk of double-counting evidence and reduces the likelihood of effect overestimation within the present umbrella review.
These findings should be considered with caution due to several methodological constraints. First, there was substantial heterogeneity across interventions in terms of content, intensity, and duration, as well as considerable variability in outcomes and HRQoL measurement instruments, limiting direct comparability of results. Second, most primary studies were characterized by small sample sizes and short follow-up periods, reducing statistical power and restricting conclusions regarding the long-term sustainability of intervention effects. Further limitations include the predominance of English-language publications and the relatively small number of high-quality randomized controlled trials specifically targeting the AYA population. Consequently, while the interventions appear promising, the overall certainty of the available evidence remains generally low to moderate. These constraints highlight the need for better-designed, adequately powered, and AYA-specific trials in future research.
Conclusion
This umbrella review synthesized evidence from systematic reviews and meta-analyses evaluating physical, psychosocial, and mixed interventions aimed at improving HRQoL among AYAs who have experienced cancer.
The findings indicate that physical activity programs demonstrate the most consistent moderate effects, particularly in reducing fatigue, improving physical functioning, and enhancing specific HRQoL domains. Psychosocial interventions, especially cognitive-behavioral approaches and coping skills training, contribute to improved emotional well-being and reductions in anxiety and depressive symptoms, highlighting their importance within comprehensive supportive care models and public health frameworks.
For mixed and technology-supported interventions, the evidence base remains less robust. Despite the promising potential of digital formats and combined intervention approaches, additional high-quality studies with long-term follow-up, specifically targeting the AYA population, are needed.
The findings support the effectiveness of these interventions; however, the overall robustness of results is limited by variable participant attrition (5%–35%) and inconsistencies in sample size reporting across the evidence base. Future research should prioritize strategies to enhance retention and standardize the reporting of feasibility indicators to ensure more reliable outcome assessments for the AYA oncology population.
Overall, the strength of evidence varies from low to moderate due to the methodological limitations of the included reviews, heterogeneity of interventions, and lack of data on long-term effects. At the same time, the low redundancy of primary studies (CCA = 1.7%) indicates a minimal risk of double counting of data and increases the stability of synthesis.
In conclusion, the results of this umbrella review support the need for the implementation of integrated, developmentally informed, and scalable physical and psychosocial supportive care programs for AYA cancer patients within public health systems. Future research should focus on outcome standardization, improved methodological quality, and the development of effective strategies for implementation in survivorship care practice.
Authors’ Contributions
All authors made equal contributions to the conception and design of the study. Material preparation, literature searching, data collection, and data analysis were performed collaboratively by all authors. The article was drafted and critically revised with equal contribution from all authors. All reviewed and approved the final version of the article.
Footnotes
Acknowledgments
The authors would like to express their gratitude to all researchers whose work was included in this umbrella review.
Author Disclosure Statement
The authors declare that they have no conflicts of interest related to this study or the preparation of the article.
Funding Information
This study received no external funding. The work was conducted as part of the authors’ academic research activities.