
Abstract
Early endometrial metastasis from triple-positive breast cancer is a rare phenomenon in young patients, especially when anti-human epidermal growth factor receptor 2 (HER2) target therapy is used as the primary treatment. We present a case of a 24-year-old patient with advanced triple positive breast cancer. The patient developed abnormal uterine bleeding during chemotherapy combined with anti-HER2 therapy (trastuzumab plus pyrotinib). Due to the transvaginal sonography are not characteristic and the low incidence rate of endometrial metastasis from breast cancer, this potential diagnosis was overlooked. The disease progressed rapidly thereafter, and the overall survival was only 13 months. The swift and devastating progression highlight the immense challenges in managing such complex cases. It remains a current challenge to identify such cases at an early stage and explore more effective therapeutic regimens. Based on this case review and previous studies, we speculate that disease progression might be attributed to the absence of endocrine therapy, chemotherapy resistance, or insufficient anti-HER2 therapeutic intensity. This case provides new insights into the metastatic pattern of HER2-positive breast cancer under targeted drug resistance. Clinicians should be alert to the possibility of reproductive system metastasis during anti-tumor treatment. Timely diagnosis and appropriate treatment are expected to improve patient prognosis.
Keywords
Background
Breast cancer is one of the major causes of cancer-related morbidity and mortality among women worldwide. 1 The incidence of human epidermal growth factor receptor 2 (HER2) positive (+) breast cancer is approximately 20%−25%, 2 with a 5-year survival rate 44% lower than HER2 negative (−) patients. 3 However, the use of trastuzumab has significantly improved the prognosis of HER2 (+) advanced breast cancer patients. 4 Among HER2 (+) tumors, the expression of hormonal receptor (HR) indicates a good prognosis.5,6 HR (+) breast cancer is most likely to metastasize to bone, the HER2 (+) tumor is more likely to develop liver metastases. 7 Breast cancer metastasis to endometrium is rare, only limited cases were reported. 8 Sole metastasis to the uterus occurs via hematogenous spread, 9 the small volume of cervix, rich in fibrous connective tissue, limited blood supply and periodic shedding of the endometrium, all of which hinder the dissemination and retention of tumor cells. Invasive ductal carcinoma (IDC) is the most common histological subtype of breast cancer, comprising 70%–80% of cases, while invasive lobular carcinoma (ILC) accounts for 5%–15% of all invasive breast cancer. 10 Among cases with endometrial metastasis, IDC is rare, compared with ILC. 11 Here we first report a case of advanced triple-positive IDC, who developed endometrial metastasis after treatment failure with pyrotinib and trastuzumab. Based on case reports and analysis of previous studies, this study aims to provide further evidence for the diagnosis and treatment of endometrial metastasis of breast cancer.
Case Report
A 24-year-old unmarried and non-pregnant woman was admitted to hospital on October 23, 2024 for a left breast mass detected 2 months prior. Breast magnetic resonance imaging (MRI) revealed multiple nodules and masses (BI-RADS 4C) in the left breast, the largest one located in the upper inner quadrant, approximately 22 × 20 × 32 mm, the abnormality demonstrates restricted diffusion, appearing bright on diffusion weighted imaging (DWI) and dark on apparent diffusion coefficient (ADC) map, left axillary lymph nodes were hyperintense (Fig. 1). Histopathology of needle biopsy from left breast and axillary lymph node showed IDC, grade 2, CK (+++), E-cadherin (+++), p120 (membrane +++), CK5/6 (−), GATA 3(+++), P63 (−), Vimentin (−), estrogen receptor (ER, +, 90%), PR (+, 60%), Ki-67 (60%), HER2 (++), fluorescence in situ hybridization (FISH) showed amplification (Fig. 2). Bone imaging revealed multiple bone metastases, while brain, both lungs, abdomen and pelvis were clear. Regrettably, the patient did not receive antitumor treatment. Until March 24, 2025, the patient was readmitted to hospital due to erythema on the left breast skin. Computer tomography scans revealed multiple nodules in both lungs, including new bone metastases. Pathology confirmed the metastatic breast cancer to left supraclavicular lymph node, left lung and ilium. Given the rapid disease progression, high tumor burden and Ki-67 expression, an aggressive therapy was performed between March 24 and August 1, 2025, doxorubicin liposome + cyclophosphamide + pyrotinib (four cycles), followed by sequential therapy with paclitaxel + trastuzumab (one cycle). The patient underwent vaginal ultrasonography on July 31, 2025 due to abnormal uterine bleeding lasting approximately 20 days. Examination showed normal uterine size and morphology, homogeneous echogenicity of the uterine cavity, and a markedly thickened endometrial thickness of 17 mm with heterogeneous echogenicity. Considering her young age, previously regular menstrual cycles (30-day cycle, 5-day duration), and ongoing antitumor therapy, the abnormal uterine bleeding was initially attributed to chemotherapy-associated menstrual disorders at that time.
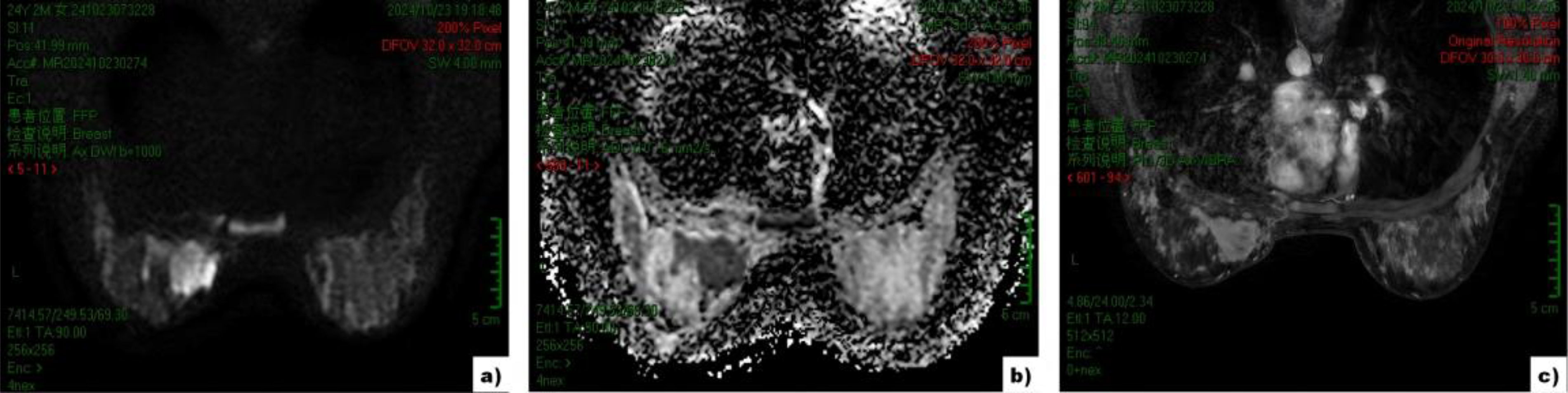
Breast MRI image.

Histology of primary breast cancer tissues, magnification: ×20.
Until August 21, 2025, abnormal uterine bleeding reappeared, but she did not immediately report to physician about the situation, until her hemoglobin levels rapidly decreased from 84 g/L to 56 g/L. Transvaginal sonography (September 1, 2025) showed normal uterine size and shape, the myometrium echogenicity is uniform, a 64 × 42 × 24 mm heterogeneous hypoechoic mass in endometria and the upper segment of the cervical canals, punctate blood flow signals around the mass (Fig. 3). Human Chorionic Gonadotropin 0.418 MIU/mL, the possibility of pregnancy or incomplete abortion was ruled out. Dilation and Curettage was performed, pathology showed GATA3 (+), PAX8 (−), E-cadherin (+), p120 (+), ER (+, 80%), PR (+, 5%), Ki-67 (45%), HER2 (+++), supporting a diagnosis of endometrial metastatic tumor of breast original IDC (Fig. 4). Brain MRI revealed diffuse meningeal metastases (Fig. 5). Due to her Eastern Cooperative Oncology Group score of 3 and poor nutritional status, follow-up treatment was discontinued. The patient developed severe headaches 2 months later, brain MRI (November 21, 2025) revealed diffuse leptomeningeal and parenchymal metastases, accompanied by significant cerebral edema. The patient subsequently died on November 25, 2025, due to brain herniation (Fig. 6). The progression of disease and treatment are shown in Figure 7.
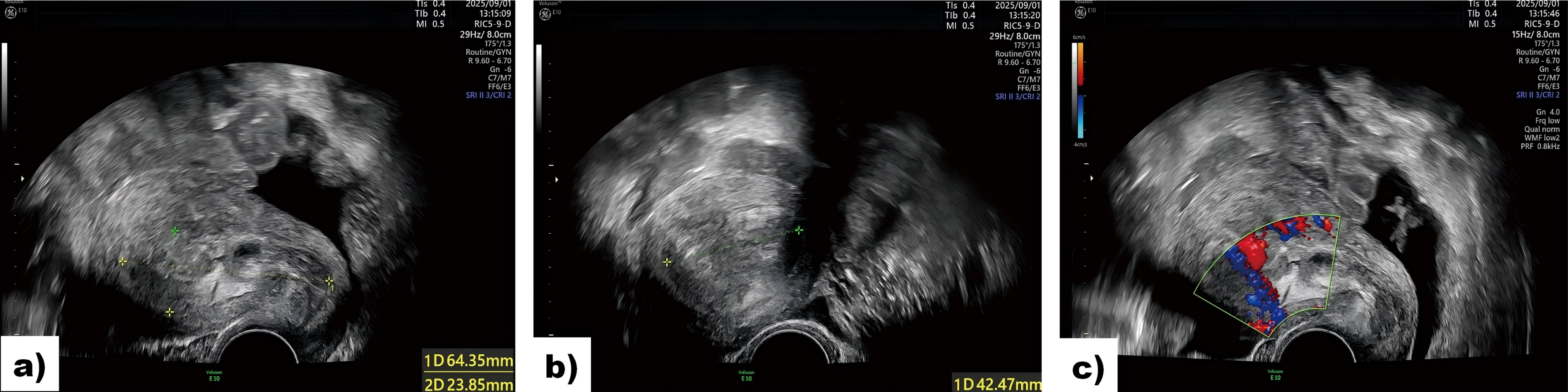
Transvaginal sonography image.

Histology of endometria tissues, magnification: ×20.
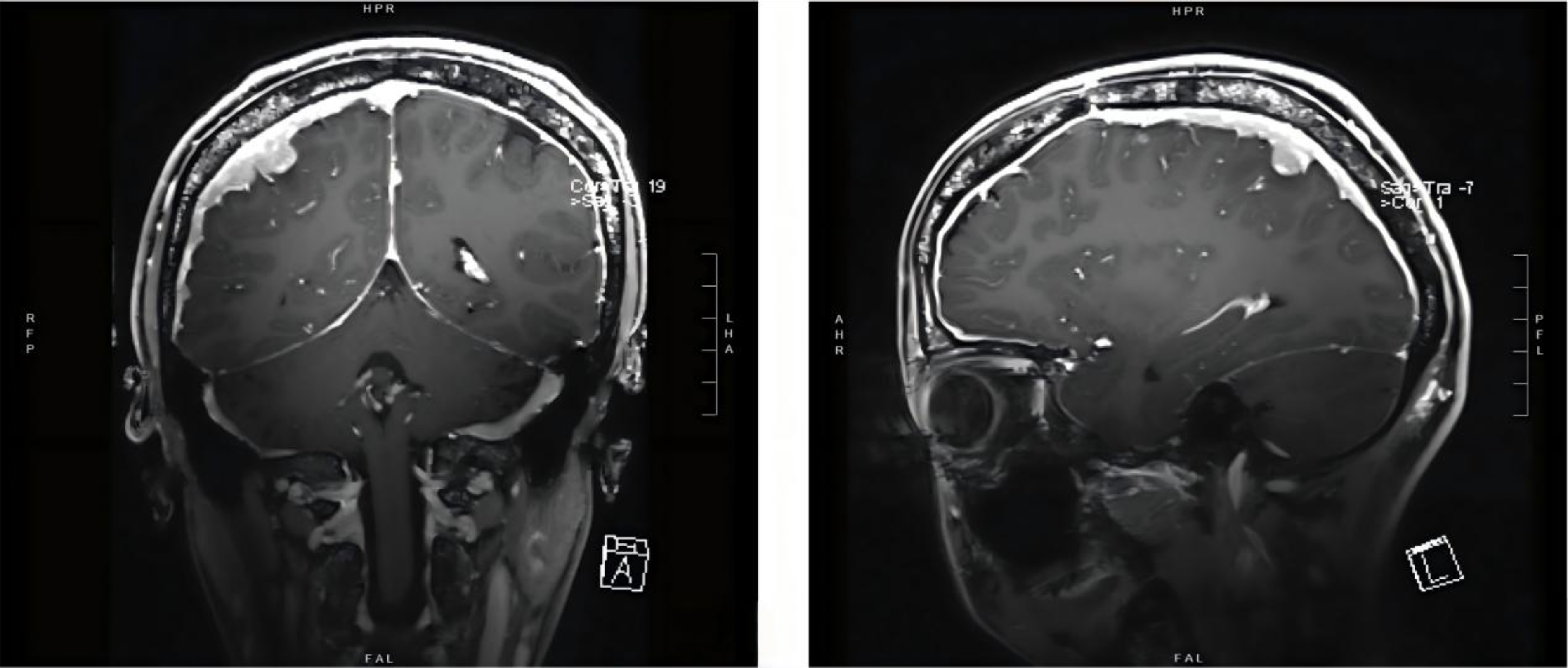
Brain MRI image. Diffuse meningeal metastases. MRI, magnetic resonance imaging.
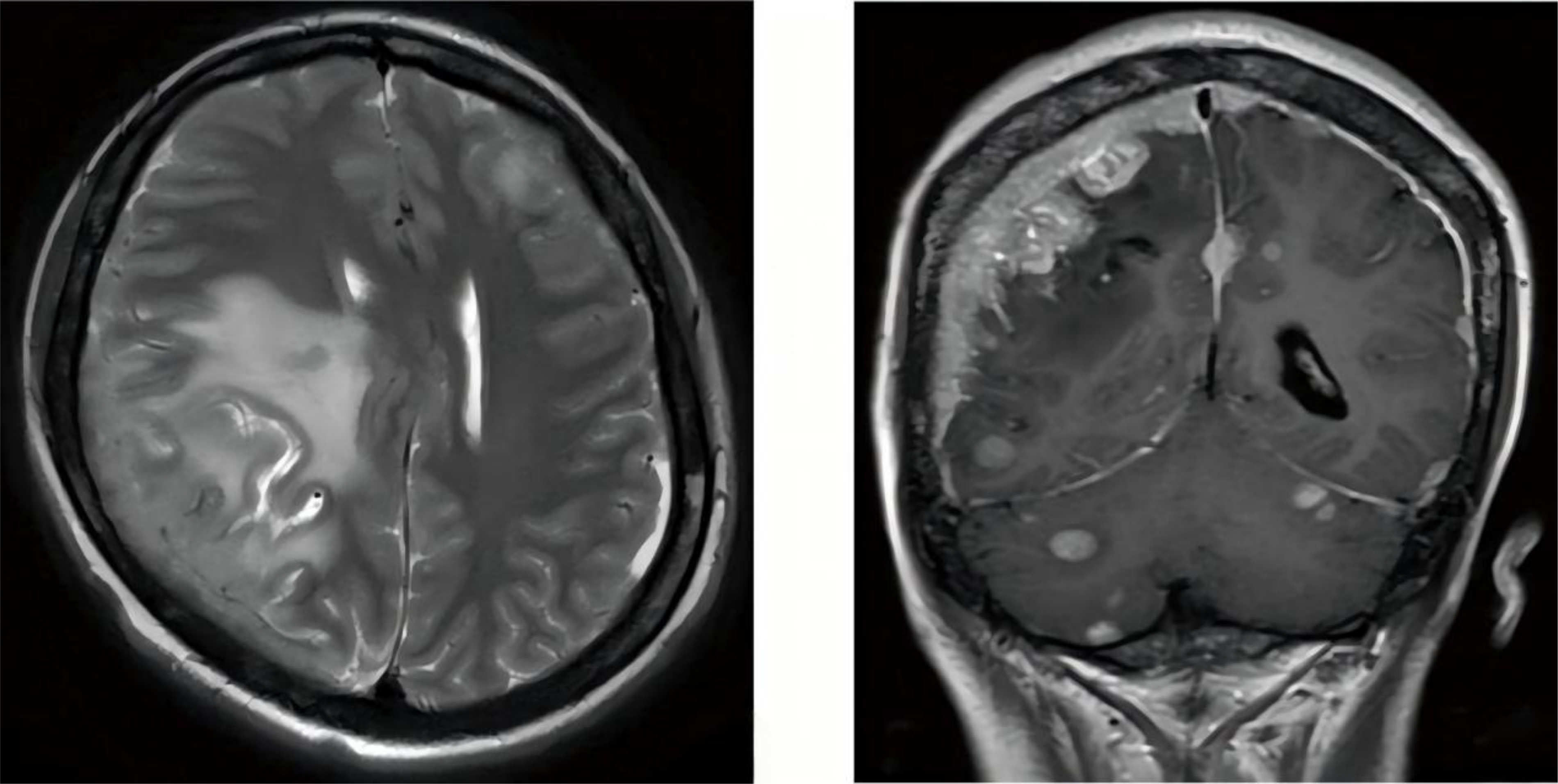
Brain MRI image. Significant cerebral edema, diffuse leptomeningeal and parenchymal metastases.
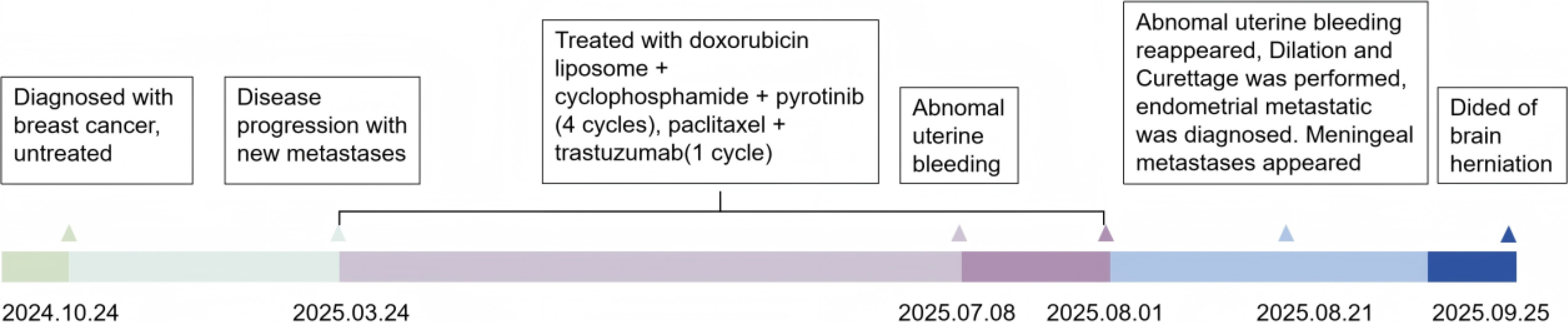
Timeline diagram of the patient’s disease progression and treatment.
Due to the lack of guidelines of endometrial metastases from primary breast cancer, we reviewed the existing literature by querying the electronic databases, from January 1985 to October 2025, the following MeSH terms were used: “ductal carcinoma” [All Fields], “IDC” [All Fields], “invasive ductal carcinoma” [All Fields], “endometrial neoplasm” [All Fields], “endometrial secondary” [All Fields], “myometrium neoplasm” [All Fields], “myometrium secondary” [All Fields], “uterine neoplasm” [All Fields], “uterine secondary” [All Fields], “Breast Neoplasms” [All Fields], “breast cancer” [All Fields], “breast neoplasm” [All Fields]. No geographical restrictions were applied. Inclusion criteria were as follows: (1) Clear histopathological diagnosis with IDC; (2) Clear histopathological diagnosis with endometrial metastases; (3) no history of other cancers. We excluded studies that did not provide complete individual data. Finally, nine publications were included,12–20 Table 1 showed the baseline characteristics of patients.
Baseline Characteristics of Patients
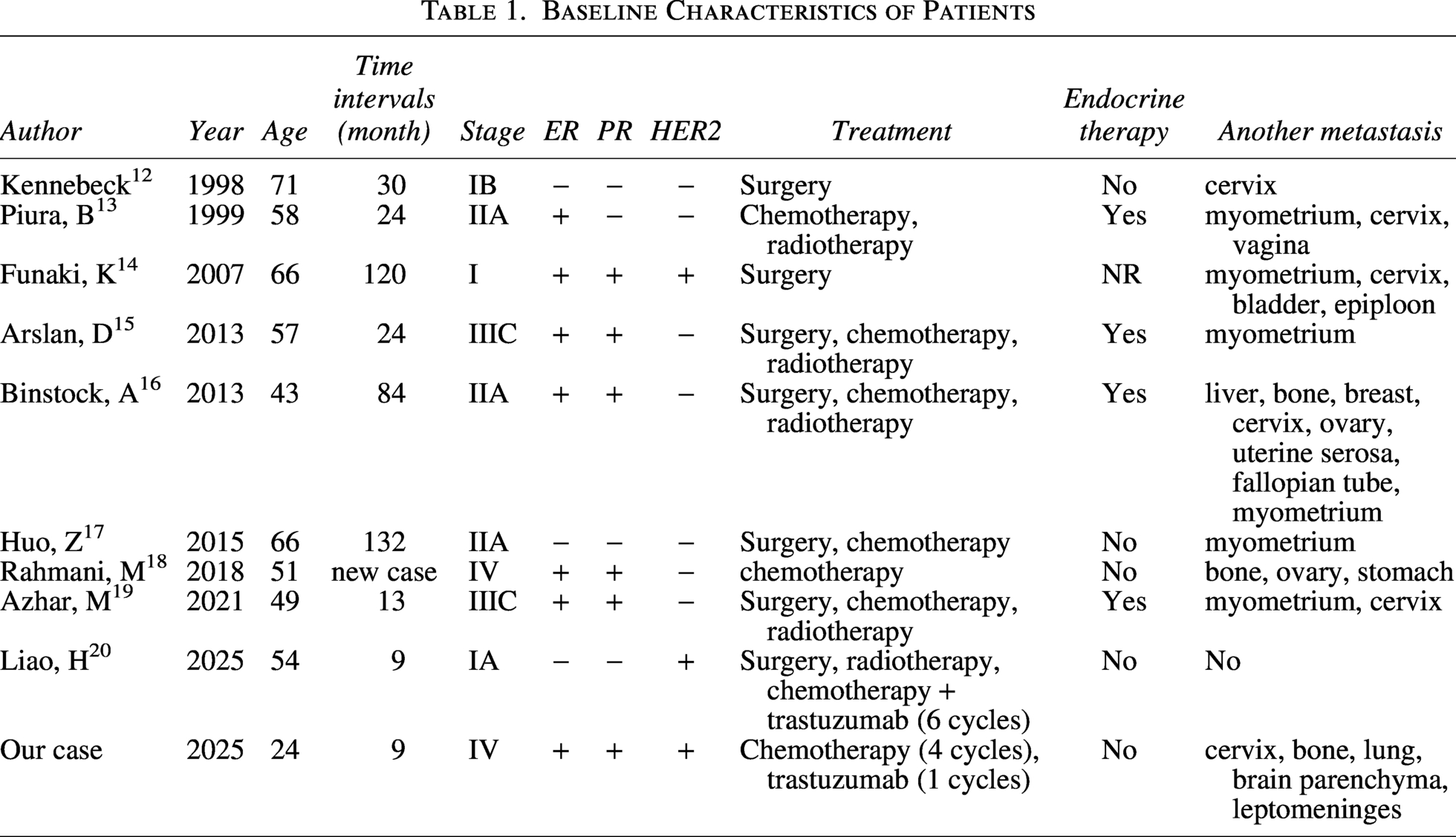
The age between 43 and 71 years, older patients appear to be more prone to endometrial metastasis. Time intervals from initial diagnosis to endometrial metastasis between 9 months and 132 months. 3 patients were stage I, 3 patients were stage II, 2 patients were stage III, and 1 patient was stage IV. They all received initial antitumor treatment. 6 cases were HR (+) and 4/6 cases received hormonotherapy, in HR (+) patients, those who underwent endocrine therapy seems to have a higher probability of endometrial metastasis. Two patients were HRE2 (+) and one of them received the therapy of trastuzumab (six cycles), who was HR (−). Endometrial biopsy was implemented on all patients. Our case was the youngest, triple positive breast cancer, stage IV at the initial diagnosis, disease progresses rapidly, and the endometrial metastasis occurs during targeted therapy. When endometrial metastasis occurs some of them received abdominal hysterectomy and bilateral salpingooophorectomy, chemotherapy, or other treatment. Due to the lack of survival data, we could not evaluate the improvement of different treatment regimens on prognosis.
Discussion
When abnormal uterine bleeding occurs, we should be alert to the possibility of endometrial metastasis. Immunohistochemistry staining should be performed to clarify the presence of primary or secondary endometrial malignancies; GATA-3 and PAX8 are considered optimal markers. GATA-3 was found positive in 91%−100% of IDC and ILC cases, but the expression rate in endometrial carcinoma was only 2%. The expression rate of GATA-3 in primary or metastatic breast cancer shows almost no difference. GATA-3 is a sensitive marker to support the diagnosis of breast original tumor.21,22 PAX8 is a transcription factor linked with Müllerian system organogenesis, negative staining suggested no involvement of uterus and cervix. 23 Among cases with endometrial metastasis, ILC is the predominant histological type. It may be related to the characteristics of E-cadherin deficiency, the loss of E-cadherin expression on tumor cell membranes, caused by CDH1 inactivation, is a hallmark of ILC. 24 This loss not only disrupts the E-cadherin-catenin complex, impairing cell adhesion, but also interferes with multiple intercellular and intracellular signaling pathways. Interestingly, our case was E-cadherin strongly positive IDC. The underlying mechanisms remaining incompletely understood.25,26
Breast cancer is a largely hormone-driven disease and the relationships with estrogens was well established. 27 HR (+) breast cancer is more likely to metastasize to distant organs, which may be related to high estrogen levels.28,29 Premenopausal women with HR strongly positive, 5-year recurrence risk and mortality were reduced with endocrine therapy, high expression of ER indicated less benefit from chemotherapy.30,31 For patients with HER2 (+) and ER (+) tumors, the combination of endocrine and anti-HER2 therapy achieve therapeutic benefits, 32 the absence of endocrine therapy may be one of the reasons for rapid progression of disease in our case. However, other studies proposed that ER (+), HER2 (+) tumors seem to gain less benefit from endocrine therapy compared with ER (+), HER2 (−) tumors further underlines that these patients need chemotherapy and should not be deprived of such treatment in the adjuvant setting. 33 According to PERTAIN trial, 55% of triple-positive breast cancer patients have received neoadjuvant chemotherapy combined with pertuzumab and trastuzumab, follow by endocrine therapy and anti-HER2 therapy is more appropriate, 34 choose an optimal timing for chemotherapy or endocrine therapy is crucial, but there is still no definitive answer.
In our case, the patient did not immediately report to the physician about the situation of abnormal uterine bleeding, until we found out she was severely anemic. Review the patient’s previous medical history, we have to suspect that the endometrial metastasis has occurred at the first time of abnormal uterine bleeding, unfortunately, the pathological basis for the diagnosis is absent, and the sonographic findings are not characteristic. Since endometrial metastasis from breast cancer is rare, this condition may be overlooked. The patient received chemotherapy combination with trastuzumab and pyrotinib, no endocrine therapy, disease progression might be attributed to the absence of endocrine therapy, the chemotherapy resistance or inadequate intensity of anti-HER2 therapy. The question of whether the combination of trastuzumab deruxtecan and pertuzumab should be used as first-line treatment for advanced triple-positive breast cancer is a clinical issue worth exploring. Interim analysis results from the DESTINY-Breast09 showed that the trastuzumab deruxtecan plus pertuzumab group achieved a median progression-free survival (PFS) of 40.7 months, providing a statistically significant and clinically meaningful improvement in PFS compared to the trastuzumab plus pertuzumab and taxane group. The absolute benefit in median PFS reached 13.8 months (40.7 months vs. 26.9 months), reducing the risk of disease progression or death by 44%. Hysterectomy and bilateral salpingooophorectomy are the main surgical approach, but according to prior report patient died 10 months after the operation,16 which does not extend the patient’s survival. Some scholars suggest that the occurrence of uterine metastasis indicates that the patient is in the terminal stage of the tumor, and it is not suitable for surgical treatment. This is worth exploring more. Early detection of metastatic lesions and timely intervention may improve the prognosis of patients.
Conclusion
We should notice the possibility of breast cancer metastasis to the reproductive system during antitumor therapy. There are no consensus or guidelines about breast cancer metastasizes to the endometrium management. The optimal treatment regimen for triple-positive breast cancer still needs to be explored.
Authors’ Contributions
S.D.: Formal analysis; investigation; methodology; software; validation; visualization; writing—original draft; writing—review and editing. J.X.: Conceptualization; data curation; methodology; software; supervision; writing—review and editing. D.D.: Conceptualization; investigation; methodology; supervision; writing—review and editing. X.L.: Conceptualization; data curation; supervision; writing—review and editing. C.Y.: Conceptualization; data curation; supervision; writing—review and editing. H.M.: Conceptualization; project administration; resources; supervision; writing—review and editing. J.-G.Z.: Conceptualization; data curation; funding acquisition; methodology; project administration; resources; supervision; writing—review and editing.
Footnotes
Ethics Approval and Consent to Participate
This study has been approved by the Medical Ethics Review Committee of the Second Affiliated Hospital of Zunyi Medical University (KYLL-2025-154). This study was conducted in accordance with the ethical principles of the Helsinki Declaration. Patient written consent for the publication of the study data was waived by the ethical committees because the clinical record of the anonymous patients was retrospectively used.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the