
Abstract
Health disparities scholars describe the existence of a race mental health paradox—specifically, when black adults face higher levels of adversity compared with whites yet have similar or better mental health outcomes. Whether such a paradox exists among youth is unclear. Using data from the Longitudinal Studies of Child Abuse and Neglect, I examine black–white differences in children’s internalizing problems scores and consider the role of childhood adversities. Black children experience more adversity within family and neighborhood domains and cumulatively across ecological levels yet have comparable or better mental health at age 4 that endures over the early life course compared with white children (p < .05). Evidence suggests that among children with the greatest adversity (at the parent level), having three supportive adults and high degrees of support at age 6 were more effective for black youth than their white peers in diminishing risk for internalizing problems later in childhood (p < .05).
Chronic exposure to adversity over the life course puts people at immense risk for developing health problems, in general, and mental health problems including anxiety and depression, in particular (Pearlin etal. 2005). Childhood adversities, such as maltreatment, parental divorce, or family financial strain, are shown to be as or more detrimental to health over the life course than other poor health behaviors like smoking (Schafer and Ferraro 2011). Research shows that the effect of adversities across several ecological levels—child, parent, family, and neighborhood (Bronfenbrenner and Morris 2006)—can accumulate over time and produce negative health outcomes (Ferraro, Shippee, and Schafer 2009).
Racial and ethnic inequalities in adversities such as income, education, housing, stress exposure, and access to medical care persist (Dunn 2000; Farmer and Ferraro 2005; Williams etal. 1997). People of color not only face more hardship in many of these domains but also live with the added burden of racism and discrimination that can exacerbate negative life events (Williams 1999). Lifetime exposure to such adversities is greater among black than white adults, and these experiences contribute to racial disparities in health (Lewis, Cogburn, and Williams 2015). Despite greater exposure to adversity, black adults have similar or better mental health outcomes than white adults—a phenomenon known as the race mental health paradox (Barnes and Bates 2017; Erving and Thomas 2018).
Although the race mental health paradox is documented in studies of adults (Barnes and Bates 2017), it remains unclear whether such patterns exist among youth, and the following question arises: At what point in the life course does the race mental health paradox emerge? Studies suggest that protective factors promoting better mental health despite adversity among black adults are developed during childhood (Breslau etal. 2006). Thus, the race mental health paradox may emerge much earlier in the life course.
In this study I examine black–white differences in children’s risk of developing mental health problems, specifically internalizing problems, throughout the early life course to determine whether the race mental health paradox emerges. If black children have higher levels of adversity but have similar or better mental health outcomes than white children, this would be evidence of a race mental health paradox. Then, I investigate childhood adversities across four ecological domains—child, parent, family, and neighborhood—to distinguish whether and under what contexts the race mental health paradox endures.
Cumulative inequality theory (CIT) states that exposure to adversities may increase the risk of poor outcomes but that available resources and human agency can offset the accumulation of adversity and diminish risk (Ferraro and Shippee 2009). Researchers deliberate regarding which factors drive the race mental health paradox among adults, such as social support and kin networks, religious and racial identities, and poor health behaviors (Ellison etal. 2001; Fischer and Shaw 1999; Jackson, Knight, and Rafferty 2010; Mezuk etal. 2010; Mouzon 2013, 2014). Poor health behaviors among adolescents coping with adversity have been examined (Boardman and Alexander 2011), but questions remain about childhood adversities, available resources, and their influence on black–white differences in mental health. Thus, I explore two aspects of social support that may help explain the paradox among youth.
Background
Mental Health Problems
Internalizing problems are a subset of mental health problems identified by emotions or feelings of inner turmoil, anxiety, fear, and excessive sadness (Perle etal. 2013). Symptoms include those consistent with depression and anxiety, somatic complaints (e.g., physical pains or aches without a known medical cause), and social withdrawal (Achenbach 1991). Children with high levels of adversity are often at the greatest risk for developing internalizing problems (Schilling, Aseltine, and Gore 2007). Moreover, youth with internalizing problems in early childhood are at high risk of engaging in aggressive, destructive, delinquent, and risk-taking behaviors later in life (Perle etal. 2013).
Cumulative Inequality Theory
Adversity can be an isolated, one-time negative event or experience or a chronic reoccurring strain or condition. CIT explains that the effects of multiple negative events, experiences, and conditions over the life course can accumulate and heighten risk for poor outcomes (Ferraro and Shippee 2009). Black–white disparities in adverse events, experiences, and conditions are shown to perpetuate racial disparities in health (Williams and Mohammed 2009).
Black children are more likely than white children to live in poverty and low-income neighborhoods with fewer resources, come from families with higher stress exposures, experience certain types of maltreatment, and battle racism and discrimination (DeNavas-Walt and Proctor 2014; Hussey, Chang, and Kotch 2006; Leventhal and Brooks-Gunn 2000; Turner and Avison 2003). Considering the differential risk of adversity, the accumulating effects of multiple adversities, and the increased risk of internalizing problems among those with the greatest adversity, I hypothesize that (H1) black children will have higher internalizing problems scores than white children. If black children have similar or better mental health than white children, this may be evidence of a race mental health paradox.
Childhood Adversity across Ecological Domains
If the race mental health paradox exists among youth, under what contexts might it endure? In highly stratified societies, such as the United States, where the sources of privilege and hardship vary depending on one’s position in the larger social hierarchy, childhood adversity is often clustered among the most socially and economically vulnerable (Turner etal. 2016). Ferraro and Shippee (2009) explained that family circumstances due to shared living environments and the neighborhoods in which families reside should be considered as domains where adversities may accumulate. Previous studies often sum up adversities, treating all events, experiences, or conditions as equivalent; however, this method fails to capture the impact of exposures within distinct domains (Schafer, Ferraro, and Mustillo 2011).
Drawing on CIT and studies from child development to understand where adversities might accumulate to increase children’s risk of mental health problems, this study considers four distinct domains: child, parent, family, and neighborhood levels (Bronfenbrenner and Morris 2006). From an interventionist standpoint, understanding how adversities in specific domains contribute to mental health problems in children can allow for more precise targeting of resources to offset or prevent negative outcomes associated with adverse experiences (Schafer etal. 2011).
Child Level
Adverse childhood events, conditions, and experiences that a child directly faces has implications for mental health. Children who witness violence or drug use in their home or neighborhood report higher levels of distress and fears of being at home (Martinez and Richters 1993). Black male children from low-income families are more likely to be victimized or to witness violence than children from more privileged, white families (O’Donnell, Schwab-stone, andMuyeed 2002). Such violence exposure is also associated with higher levels of anxiety, depression, and somatization (O’Donnell etal. 2002). Consistent with CIT, children with polyvictimization—violence exposure in many domains—have the worst outcomes and fewest coping resources (Turner etal. 2016).
Some methods of discipline also qualify as adverse experiences, particularly if the strategies used to control child behavior are linked with poor developmental outcomes. Yelling and threatening children in order to gain compliance is associated with high rates of internalizing problems as children age (Teicher etal. 2006). Likewise, physical punishment is still frequently used, despite considerable evidence of toxic outcomes (Gershoff 2016; Straus and Donnelly 2008). Black children and those from low-income families are more likely to experience physical punishment (Taillieu etal. 2014).
Maltreatment patterns also vary by race and age; black children report higher levels of physical neglect and sexual abuse, but their white peers are more apt to face supervisory neglect and physical abuse (Hussey etal. 2006). Children who experience maltreatment and also develop internalizing problems are at high risk of physiological damage affecting their ability to cope with future adversity (Cicchetti etal. 2010). Because maltreatment is among the most severe forms of adversities (Perle etal. 2013), in this study I separately analyze maltreatment from other types of child level adversities.
Overall, black children are at higher risk for many adverse childhood events, experiences, or conditions at the child level compared with white children. Based on the evidence and CIT, I expect that (H2) for each additional adverse event, experience, or condition at the (a) child level or (b) exposure to maltreatment, internalizing problems scores will increase and will be highest for black children.
Parent Level
Parent level adversities are those a child does not directly face, but the impact of such adversities has the potential to disrupt the child’s environment or parent-child interactions in ways that are detrimental to mental health. Having a parent with a mental health problem or a mother with poor health is associated with more internalizing and health problems in children (Connell and Goodman 2002; Waters etal. 2000). Black adults have greater stress exposure than white adults (Lewis etal. 2015; Williams and Mohammed 2009); although some mental health outcomes are better despite stress (Erving and Thomas 2018), physical health outcomes are typically worse due to unhealthy coping strategies (e.g., drinking alcohol, smoking, and overeating) (Jackson etal. 2010; Mezuk etal. 2013).
Socioeconomic factors at the parent level are also associated with children’s mental health; problems are more likely to persist with more symptoms among children of parents with less than a high school education or long-term unemployment compared with those with college degrees or steady jobs (Harland etal. 2002; McLaughlin etal. 2011; Reiss 2013; Sleskova etal. 2006). Black adults are less likely to hold a bachelor’s degree (Ryan and Bauman 2016), have nearly double the unemployment rate (U.S. Bureau of Labor Statistics 2017), and are paid lower wages for the same work compared with their white counterparts. Moreover, because of racism and patriarchy in the workplace, upward mobility with higher income potential is further restricted to black versus white mothers (Tomaskovic-Devey 1993).
Also associated with children’s mental health risk is parents’ history of childhood and adulthood victimization. Adults who were maltreated during their childhoods are more likely to abuse or neglect their own children (Widom, Czaja, and Dumont 2015). Those who were victimized as adults, including verbal, psychological, or physical domestic violence, are at high risk of mental health problems themselves and internalizing problems among their children (Moylan etal. 2010). Black women have a higher prevalence of physical and sexual violence over their lifetimes than white women and both black and white men (Centers for Disease Control and Prevention 2014).
Adversity that parents face can influence their parent-child interactions, disrupt the availability of resources to care for their child, and ultimately affect children’s mental health. Black adults in general and black women in particular are at greater risk for many of the adverse exposures described at the parent level; thus, I expect that (H3) for each additional adverse event, experience, or condition at the parent level, children’s internalizing problems scores will increase and will be highest for black children.
Family Level
Family level adversities can establish a lineage of inequality that can be passed on for generations via biological, social psychological, economic, and ecological forces (Ferraro etal. 2009). Childhood mental health problems are especially high among children in families living in persistent poverty (Reiss 2013). From 2015 to 2016, the median income for white and black households was $65,041 and $39,490, respectively, and the poverty rate was 8.8 percent of white people versus 22 percent of black people (Semega, Fontenot, and Kollar 2017). Racial disparities in household income and poverty contribute to greater economic strain for black families than for whites (Conger etal. 2002).
Black families are at especially high risk for everyday stressors due to their marginalized social, economic, and political positions (Barnes and Bates 2017). Even when families receive social services, which are designed to reduce disparities in health, income, and housing, the threat for internalizing problems among children is still high. Medicaid is meant to increase access to health care services for those living in poverty; having Medicaid or related child health insurance programs does not cause mental health problems in children. Rather, social patterning of mental health problems tends to cluster among the most vulnerable in society, including those who qualify for federal social services. The highest prevalence of mental health problems among children is found among families living below the federal poverty line and among those with Medicaid (Howell 2004).
Union formation within families can also be a source of adversity; children of recently divorced or separated parents and single parents are at high risk for internalizing problems compared with children with married parents (Harland etal. 2002). Children born to unmarried mothers have decreased in the United States since 2007, representing only 39 percent of births overall; however, nearly 70 percent of births among black women are to single mothers compared with 28.5 percent of births among white women (Martin etal. 2018). Although single parents are as effective in parenting as their partnered peers, the reduction in resources can create financial challenges for single parents that affect children (Cain and Combs-Orme 2005).
Family level adversities contribute to the environmental circumstances that influence children’s mental health, especially when adversities accumulate within and across generations. Based on previous research and the evidence that black families face more family level adversities, I hypothesize that (H4) for each additional adverse event, experience, or condition at the family level, children’s internalizing problems scores will increase and will be highest for black children.
Neighborhood Level
Neighborhood level adversities are associated with worse mental health outcomes among children (Leventhal and Brooks-Gunn 2000). Neighborhoods in the United States are racially and socioeconomically segregated; high-income black families live in neighborhoods spatially separate from lower-income black families, who are then isolated in homogenous neighborhoods with fewer educational resources and employment opportunities (Reardon and Bischoff 2011). Moreover, living in high-poverty, chaotic, unsafe, and unsupportive neighborhoods has such a strong influence on children’s risk of internalizing problems that not even maternal sensitivity diminishes the association (Coley, Lynch, and Kull 2015). Black children are more likely to reside in high-poverty neighborhoods that have a greater incidence of violence than their white peers (Brown 2008).
Neighborhood level adversities provide the broadest context through which adverse events, experiences, and conditions influence children’s mental health. Drawing on previous research, I anticipate that (H5) for each additional adverse event, experience, or condition at the neighborhood level, internalizing problems scores will increase but will be highest among black children.
Multiple Domains
Social systems generate inequality through demographic and developmental processes over the life course with variability on multiple levels or domains (Ferraro and Shippee 2009). Perhaps the impact of adversity is less about a specific domain but more about facing challenges in more than one domain. Drawing on CIT and the literature within each domain that suggests black children, their parents, and families are at especially high risk for adversity (Mezuk etal. 2010), I expect that (H6) for each additional domain in which adverse events, experiences, or conditions are present, internalizing problems scores will increase and will be greatest among black children.
Race Mental Health Paradox and Social Resources
The race mental health paradox suggests that despite higher lifetime exposures to adversities, black adults have similar or better outcomes than white adults (Erving and Thomas 2018; Mouzon 2014, 2013). One explanation for the paradox is the high degree of poor health behaviors among black adults. Smoking, drinking alcohol, and overeating high-calorie, fatty foods were examined to see whether they are used to cope with high stress. Black adults with no poor health behaviors had worse mental health than those with frequent poor health behaviors, so such behaviors account for some of the paradox (Jackson etal. 2010; Mezuk etal. 2010). In a nationally representative study of adolescents, Boardman and Alexander (2011) found that poor health behaviors moderated depression for black youth with high stress but not because they are engaging in more of these unhealthy behaviors than white youth.
Poor health behaviors aside, consistent with CIT, many resources are found to buffer the effects of childhood adversities on mental health (Ferraro and Shippee 2009), including social ties (Pearlin 2010). In a review on social ties and mental health, Kawachi and Berkman wrote, “Smaller social networks, fewer close relationships, and lower perceived adequacy of social support have all been linked to depressive symptoms” (2001:458). Social ties cushion the effects of adversity when people sense support that helps them cope with stressful situations; however, the effectiveness of social ties can vary across groups in society based on cultural differences and timing.
In early childhood, children often form close ties with those in their immediate families, which lowers risk of depression later in life (Stewart and Suldo 2011), and they expand that network to include more extended family in middle childhood. For adolescents, peer networks supplant the extended family network to some degree (Levitt, Guacci-Franco, and Levitt 1993). However, the importance of extended family members remains most salient among children of color (Levitt etal. 1993). Social networks may buffer adversity more so for black youth because they, “place less emphasis on individual autonomy and are more likely to draw on extended family relations” (Levitt etal. 1993:817).
Drawing on past scholarship on social ties and support during early childhood, mental health, and CIT, I hypothesize that (H7) (a) for each additional adult a child perceives to be especially helpful during early childhood, there will be an increasingly positive effect on mental health, and (b) as the total amount of help from the helpful adults increases, children will have lower internalizing problems scores. If black children with high levels of adversity and the maximum number of supportive adults or the greatest amount of help have better mental health than those with fewer resources and high adversity, this may in part identify mechanisms that play a role in the race mental health paradox among children.
The Present Study
Research documents the race mental health paradox among adults; however, no studies to date have examined this phenomenon among children. It is unlikely that the paradox emerges at a socially constructed age of adulthood (i.e., 18 years) but rather emerges due to the timing and context of adversity and resources (Elder, Johnson, and Crosnoe 2003). This study seeks to expand existing knowledge on the race mental health paradox and improve our understanding of (1) whether such a paradox emerges during childhood, (2) under which circumstances the paradox might endure, and (3) what factors potentially mitigate the effects of childhood adversity on children’s mental health.
Data
Sample
The Longitudinal Study of Child Abuse and Neglect (LONGSCAN) data are from 1,354 child-participants, their families, teachers, and Child Protective Services (CPS) across five sites in the Eastern, Midwest, Southwest, Northwest, and Southern regions of the United States. Purposive sampling methods were used at each site to recruit children deemed at risk for maltreatment and other adversities; thus, the data are not representative, and findings are not generalizable beyond the scope of the sample. LONGSCAN collected seven waves of data beginning in 1991 when the child-participants were age 4 and then biennially through age 18 (except age 10). For more detailed information about the LONGSCAN study, see work by Runyan and colleagues (2014). The use of LONGSCAN for this study received Institutional Review Board approval (IRB 18-0036).
LONGSCAN is a racially diverse data source, and for the purpose of investigating the race mental health paradox among youth, the analytic sample is restricted to 976 black and white children with internalizing problems scores at age 4. As for evaluating the contexts under which the paradox may endure, LONGSCAN captures childhood adversity in many domains and across the entire early life course (i.e., early childhood to young adulthood). LONGSCAN also has measures of early social support reported on by the child-participants to determine whether support is influencing the paradox.
Measures
Dependent Variable: Internalizing Problems Scores
The Child Behavior Checklist measures anxiety, depression, somatic complaints, and social withdrawal and combines them into an internalizing problems score (see Achenbach 1991 for full list of measures). Parents respond to 100 statements about their child’s behavior, reporting whether the behavior is “not true,” “sometimes true,” or “very true.” LONGSCAN researchers converted raw scores into age-standardized T scores for analyses (Hunter etal. 2001). Children in the analytic sample had scores, on average, in the “normal range” (T scores less than 60) (Figure 1). From ages 6 to 18 years, black children had lower scores than white children (p < .001) (Tables 1-3).
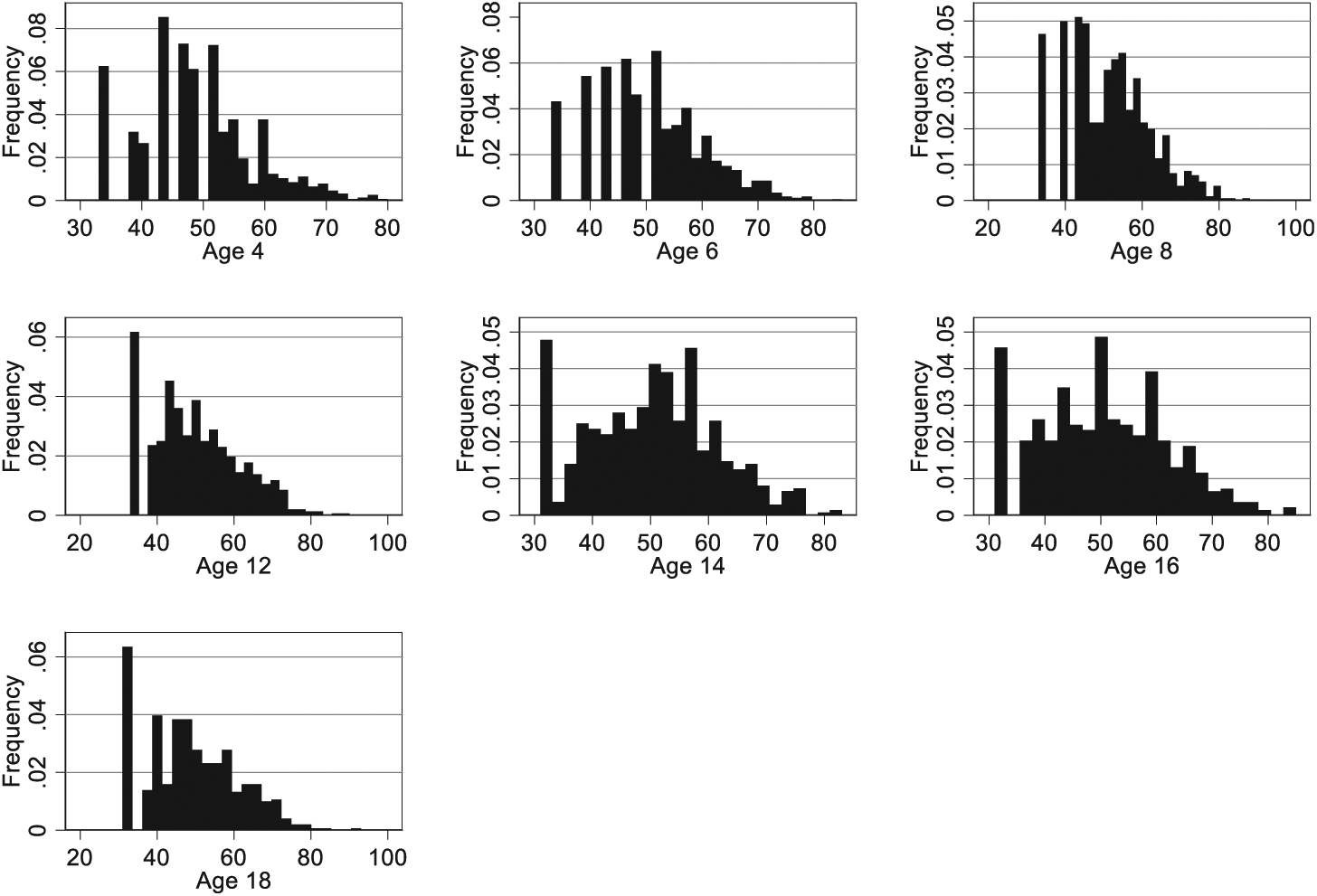
Frequency distributions of internalizing problems T scores by age.
Sample Characteristics by Race for Ages 4, 6, and 8: Longitudinal Study of Child Abuse and Neglect (LONGSCAN).
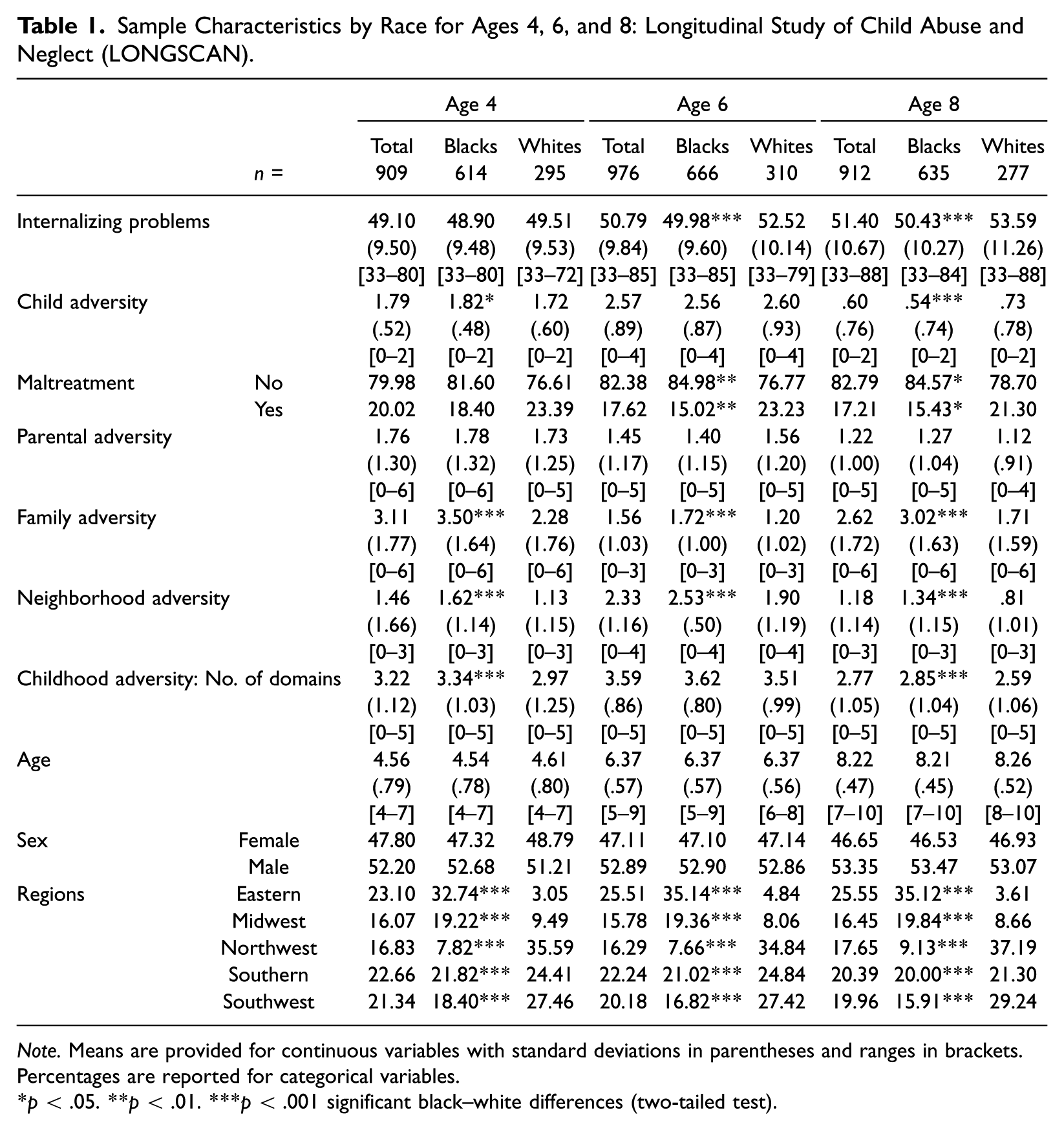
Note. Means are provided for continuous variables with standard deviations in parentheses and ranges in brackets. Percentages are reported for categorical variables.
p < .05. **p < .01. ***p < .001 significant black–white differences (two-tailed test).
Sample Characteristics by Race for Ages 12, 14, and 16: Longitudinal Study of Child Abuse and Neglect (LONGSCAN).
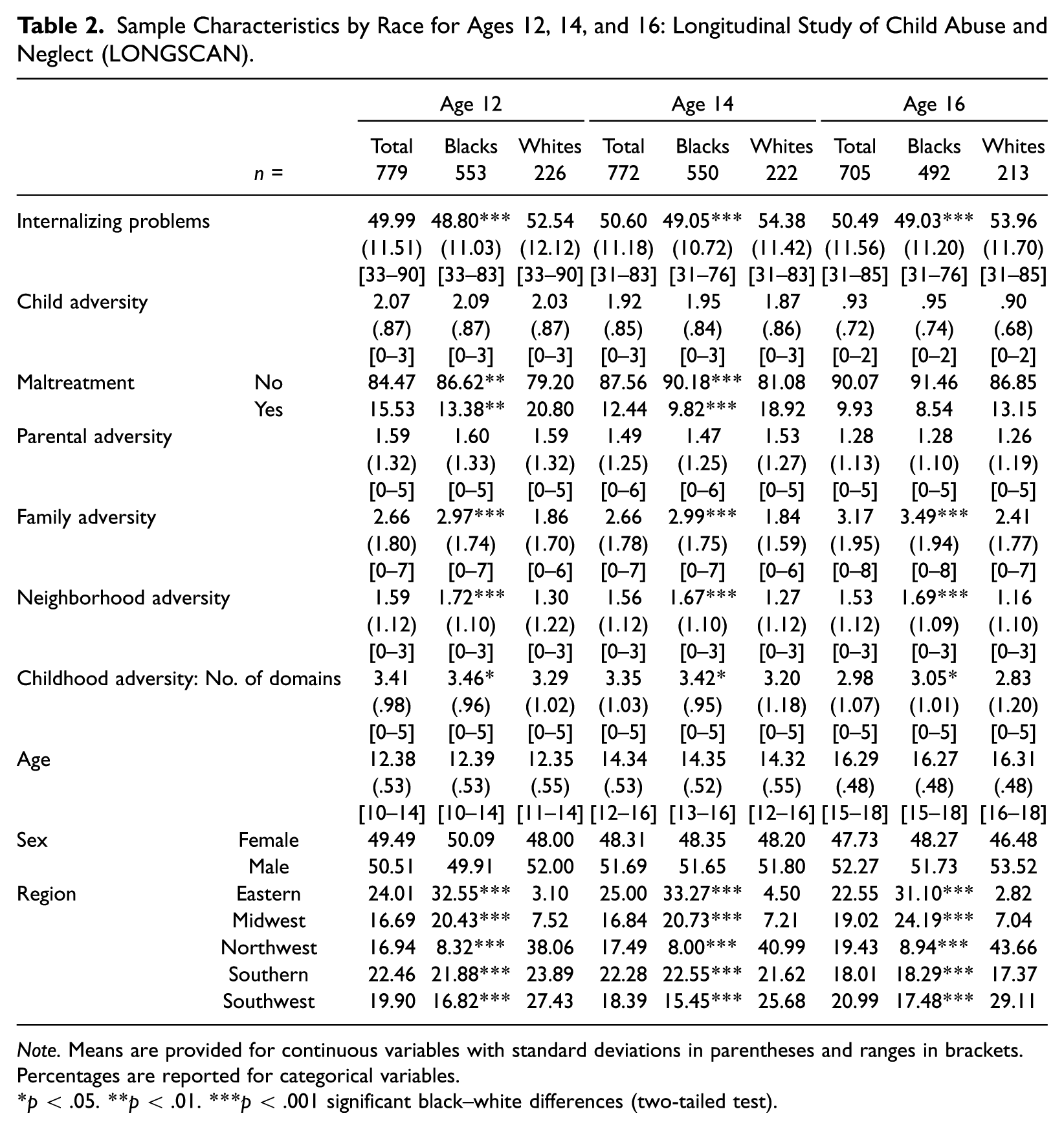
Note. Means are provided for continuous variables with standard deviations in parentheses and ranges in brackets. Percentages are reported for categorical variables.
p < .05. **p < .01. ***p < .001 significant black–white differences (two-tailed test).
Sample Characteristics by Race for Age 18: Longitudinal Study of Child Abuse and Neglect (LONGSCAN).
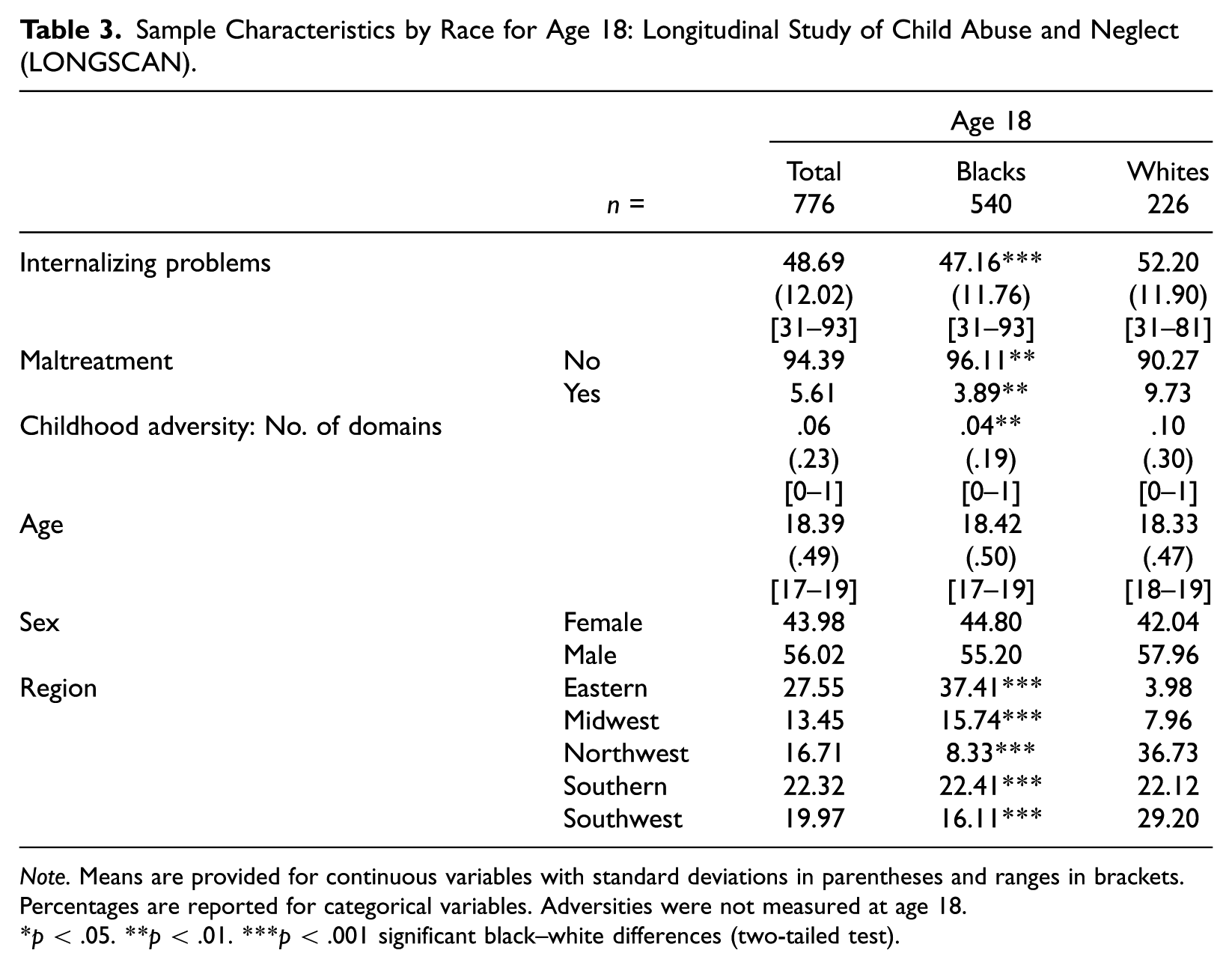
Note. Means are provided for continuous variables with standard deviations in parentheses and ranges in brackets. Percentages are reported for categorical variables. Adversities were not measured at age 18.
p < .05. **p < .01. ***p < .001 significant black–white differences (two-tailed test).
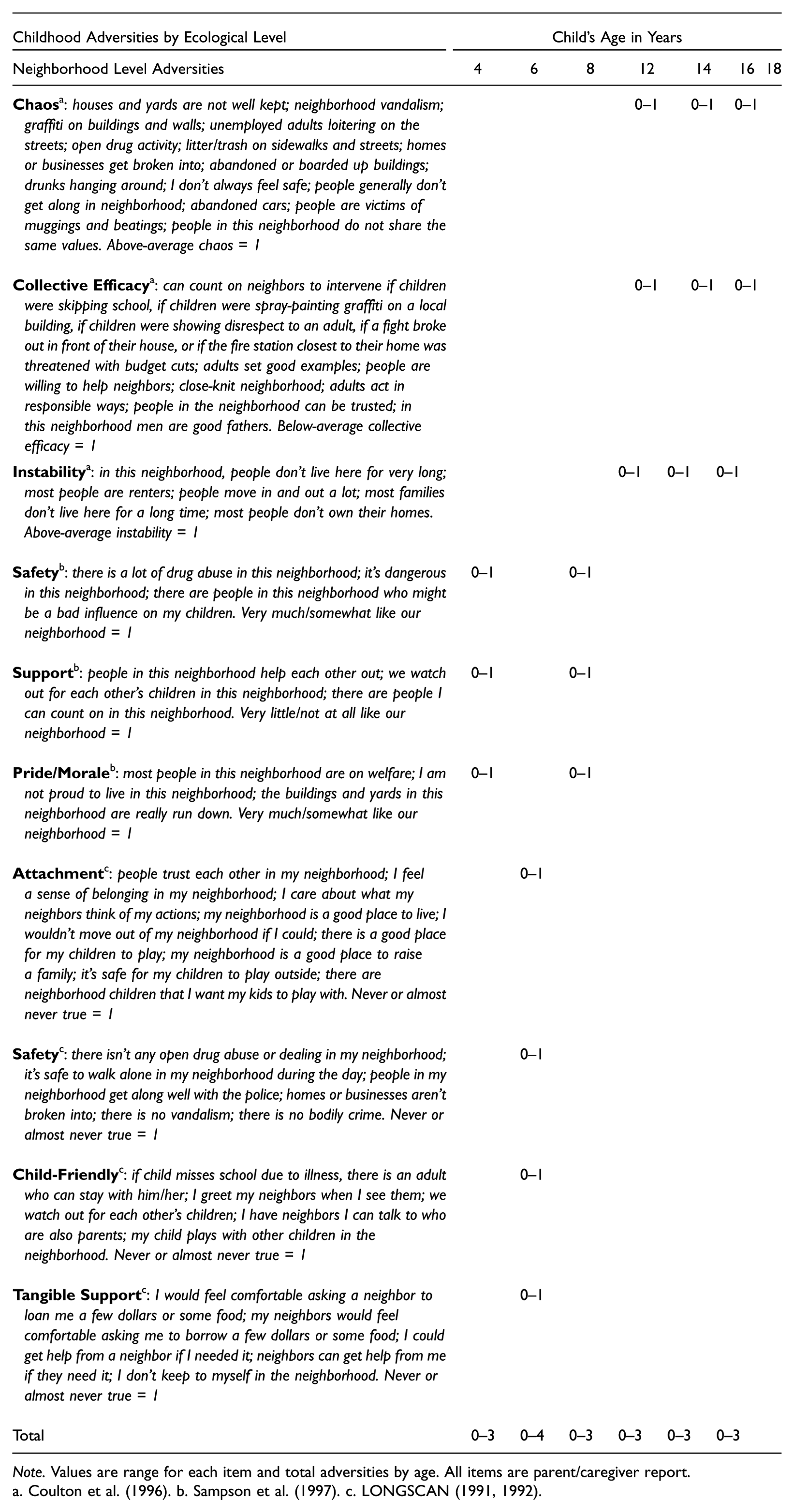
Childhood Adversities
Childhood adversity is measured across four ecological domains: child, parent, family, and neighborhood levels and separately for child maltreatment. Adverse events, experiences, and conditions vary across domain by time and respondent (see Appendix A for a full list of adversities by time point and respondent). If the adversities measured were present = 1, an additive measure was created within each domain at each time point. A higher score indicates greater childhood adversity.
Child Level
Adverse events, experiences, or conditions at the child level are those a child directly faces. Black children had higher child level adversities at age 4 (p < .05) but the same or less adversity than white children at ages 6 to 18. Maltreatment is analyzed separately from other child level adversities; children with any allegations of maltreatment, physical or sexual abuse, or neglect made to CPS = 1 and those without allegations = 0. Even when cases of maltreatment cannot be substantiated (i.e., proven), children’s mental health is still adversely affected; thus, using allegations is common in research (Villodas etal. 2012). At age 4, about 20 percent of the sample had maltreatment allegations. White children had more maltreatment allegations at ages 6–14 and 18 than black children (p < .05).
Parent Level
Parent level adversities describe events, conditions, or experiences that a parent or caregiver directly faces, and the adverse effects can indirectly affect a child. Among this sample, parent level adversities did not vary by race and on average were fewer than two per wave.
Family Level
Adversities at the family level describe circumstances that affect the entire family or family functioning. Black children and their families reported more adverse events, experiences, and conditions than their white counterparts at ages 4 to 16 (p < .001).
Neighborhood Level
Neighborhood level adversities were reported by the parent or caregiver. On average, black children in this sample had more adverse events, experiences, and conditions in their neighborhoods than white children from ages 4 to 16 (p < .001).
Number of Domains
If any adversity was present at the child, parent, family, or neighborhood levels or if maltreatment was present they were coded as = 1 and a count variable was generated with a range 0–5 at ages 4–16 and 0–1 at age 18. Black children had significantly more domains with adverse events, experiences, and conditions than white children at ages 4 and 8–16 (p < .05).
Race
Children’s race was reported by a parent or caregiver at the baseline interview. Sixty-six percent of the analytic sample was black and 34 percent white.
Child’s Age
Children’s age was measured in years, and the LONGSCAN study design intended children to be relatively close to the target age ranges (e.g., 4, 6, 8, 12, 14, 16, and 18). Due to variations in the date of data collection at each site, there is a range for each time period, but the average at each time point is close to the target age (e.g., target age 4 years, mean 4.55 years, range 4–7 years).
Child’s Sex
Female children (0) served as the reference category in the study, and males (1) made up approximately 52 percent of the baseline sample.
Region
Due to the purposive sampling in the LONGSCAN study by region, a regional covariate was included in the models. The Eastern region is the reference group and makes up 23.10 percent of the baseline sample, Midwest is 16.07 percent, Northwest is 16.83 percent, Southern is 22.66 percent, and Southwest is 21.34 percent.
Social Support
Two social support measures were captured when children were 6 years old—the number of supportive adults and the total amount of social support from these adults. Although social support was measured at only one time point, studies show the importance of early social support for later mental health (Stewart and Suldo 2011). Children were asked three times, “In your life has there been any adult that has been especially helpful to you?” If the child responded yes, this was coded as = 1 and the responses were summed for 0–3 supportive adults. On average, children reported having 2 especially helpful adults.
The total amount of social support from helpful adults was determined by asking the children four questions per each helpful adult (up to three times): How much has the adult “shown you that s/he cares about you”; “explained things to you, told you things that you need to know, or helped you solve a problem”; “spent time with you”; and “helped you get food, clothes, and other things you need.” Children responded with “a lot” = 3, “some” = 2, “a little” = 1, and “not at all” = 0. Scores ranged from 0 to 36, and children with 0 helpful adults were coded as 0 for this measure. The average score for total amount of social support was 21.63. Neither social support measure varied by race (Table 4).
Social Support Characteristics by Race at Age 6.
Note. Means are provided with standard deviations in parentheses and ranges in brackets.
p < .05. **p < .01. ***p < .001 black–white differences (two-tailed test).
Analytic Strategy
Data analyses were completed in Stata 15 (StataCorp 2017b). For the descriptive statistics, the Wilcoxon rank sum test was used to determine statistically significant black–white differences for analytic variables due to the nonnormal distribution of internalizing problems scores and dissimilar sample sizes (Wilcoxon 1945). P values are reported for a two-tailed hypothesis test (Tables 1–4).
Beyond descriptive statistics, attrition from ages 4 to 18 was approximately 19 percent. Sensitivity analyses showed no black–white differences in the likelihood of having missing internalizing problems scores, but white children were more likely to withdraw from the study. Attrition is not dependent on internalizing problems scores or the random effects; it is due to covariate-dependent missingness, so “analysis of the complete cases is not biased, although it is subject to a loss of efficiency” (Little 2008:422). Little (2008) suggested using maximum likelihood methods to make use of all available data, even subjects without complete data, to give more consistent and efficient estimations.
Therefore, I use multilevel mixed-effects generalized linear models (GLMM) to examine black–white differences in children’s risk of developing internalizing problems and the impact of childhood adversity, because the method maximizes data available at all time points and children have repeated observations that are correlated over time. GLMM adjusts for correlations between time points and reduces the risk of Type I errors compared with other ordinary least squares methods (Edwards 2000). Moreover, GLMM handles unbalanced designs (i.e., uneven intervals between waves) (Edwards 2000).
Results from a likelihood ratio test supported using random intercept models. The fixed effects results showed the intercept for the model and slopes for each covariate along with standard errors. The random effects portion of the model included the variance of the Level II errors and the residual for the Level I errors and their standard errors. A Wald test and goodness-of-fit tests—Akaike’s and Schwarz’s Bayesian information criteria scores—are presented for each model (StataCorp 2017a).
As for examining the effect of social support at age 6 on each time point for ages 6 to 16, generalized linear models (GLM) were used with the maximum likelihood option. Interaction terms were included to test for statistically significant black–white differences in internalizing problems over time (Question 1), then adding moderating effects of childhood adversity (Question 2), and to test for the impact of social support (Question 3). Postestimation margins were calculated from a previously fit model with fixed values, and internalizing problems scores could be estimated for different groups specified in the models. Pairwise comparison tests were used to determine whether the differences between black and white children’s internalizing problems scores were statistically significant (p < .05) (StataCorp 2017a).
Results
Are there black–white differences in children’s risk of developing internalizing problems or evidence of a race mental health paradox? Table 5 shows the association between race, childhood adversity, and internalizing problems across the early life course. In Model 1, internalizing problems scores do not differ by race at age 4, but with each additional year of age, white children’s scores increase by .16 whereas black children’s decrease by .24 (p < .001). Figure 2A illustrates that by age 12, black adolescents have better mental health outcomes than white peers, suggesting that the race mental health paradox emerges during the early life course.
Internalizing Problems, Race, Childhood Adversity, and Covariates (Full Sample, N = 976).
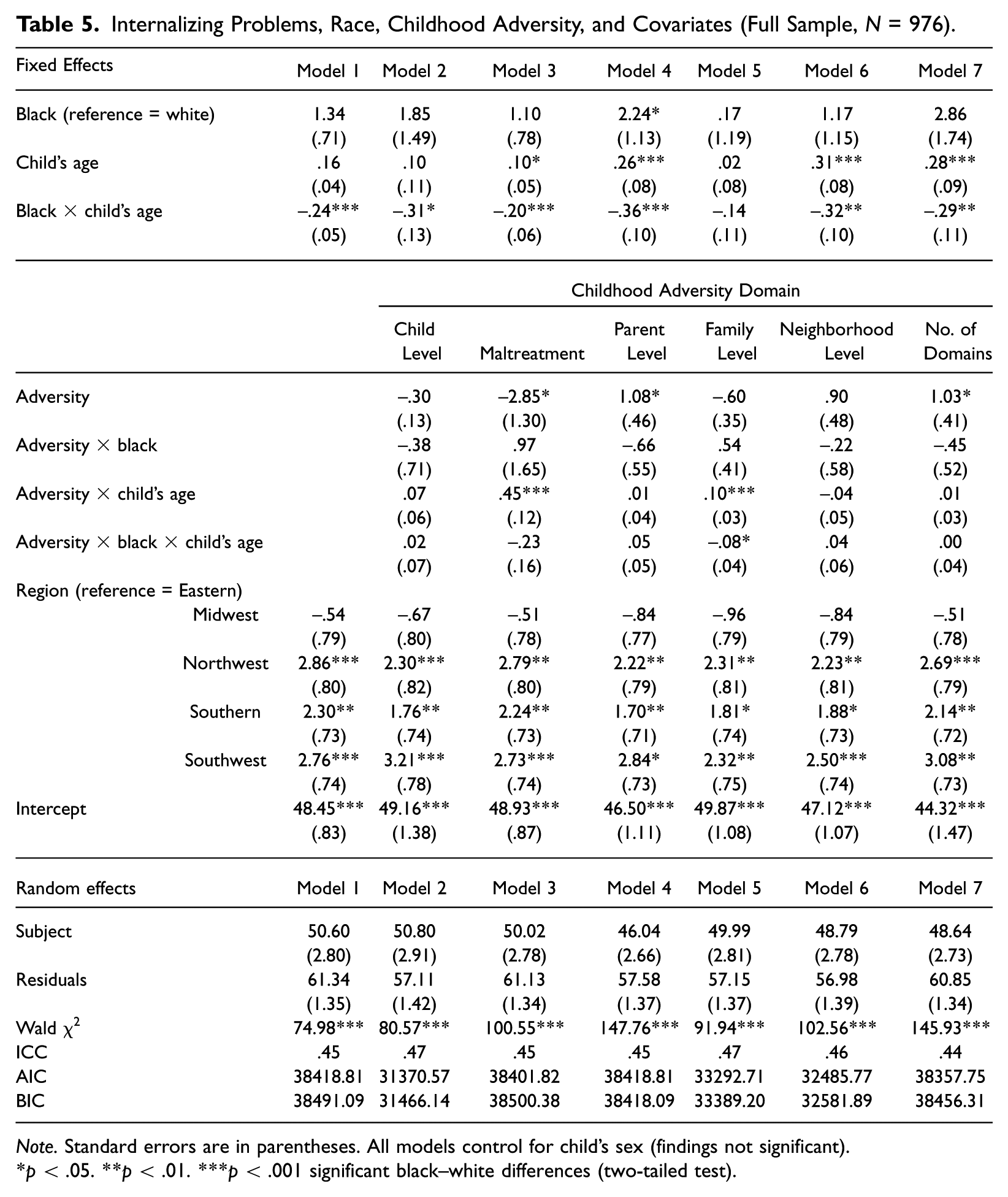
Note. Standard errors are in parentheses. All models control for child’s sex (findings not significant).
p < .05. **p < .01. ***p < .001 significant black–white differences (two-tailed test).
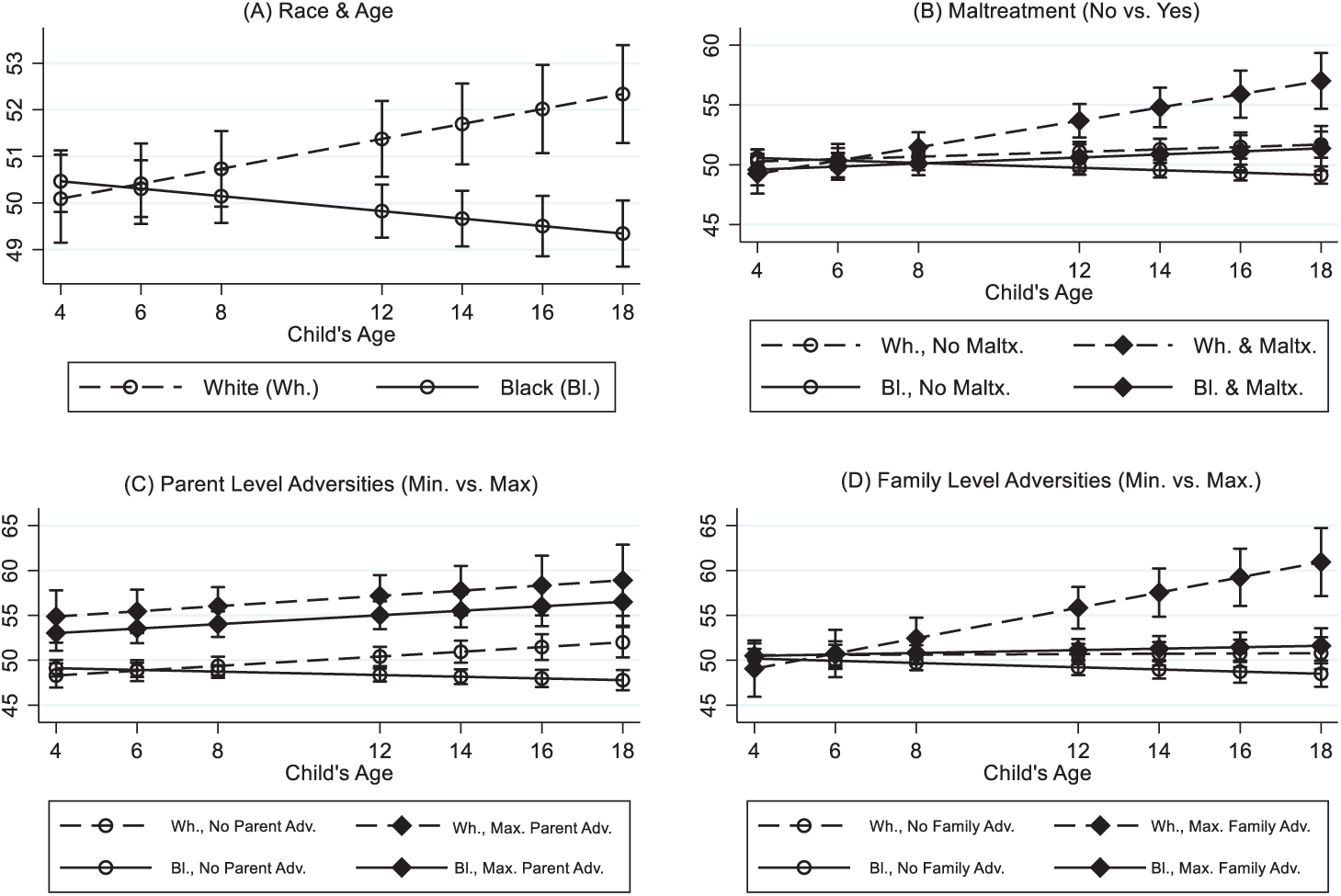
Marginal predicted internalizing problems scores by race, childhood adversity, and age.
Under what contexts does the race mental health paradox endure? Models 2 through 7 present findings from childhood adversities across four ecological domains and child maltreatment. Child level adversities in Model 2 show no black–white differences in mental health risk at age 4 and indicate that child level adversities are not statistically significant. However, despite child level adversities, black children’s scores decrease by .31 for each additional year of age (p < .05), indicating better mental health.
Child maltreatment is among the most severe forms of adversity at the child level. Model 3 indicates that white children’s scores increase by .1 with each additional year of age (p < .05), while black children’s risk decreases by .20, net of all controls (p < .001). Maltreatment allegations are associated with lower internalizing problems scores at age 4, but over time, internalizing problems increase faster for children with allegations than those without (p < .001). Figure 2B offers further support of the race mental health paradox; specifically, black children with maltreatment allegations have scores similar to white and black children without maltreatment experiences. White children with maltreatment allegations have the worst mental health compared with all other groups.
Model 4 presents the effects of parent level adversities; for every additional adversity, children’s internalizing problems scores increase by 1.08 (p < .05). Black children have more internalizing problems at age 4 (p < .05) but scores decrease by .36 with each year of age (p < .001). Alternatively, white children have better mental health at age 4 but face poorer mental health over time.
Figure 2C shows white and black children with no reported parent level adversities compared with those with the most adversity. Among those with no reported adversity, black children’s mental health risk is lowest compared with their white peers. Yet the threat of internalizing problems is greatest among all children with the highest amounts of parental adversity, regardless of race. This means that the paradox does not persist despite all adversities, and it clarifies the need for early interventions for children and their parents struggling with physical or mental health problems, addiction, or intimate partner violence.
In Model 5, among white children, with each additional family level adversity at each time point, internalizing problems scores increase by .10 (p < .001). For every additional adversity at each time point among black children, scores decrease by .08 (p < .05). This suggests that family level adversities have the potential to affect mental health, especially among white families, and that black families may have better mechanisms to cope with family or economic stressors. This model and Figure 2D support the race mental health paradox, where black children with the highest levels of family adversity have similar mental health outcomes as white and black children with no reported family adversities.
Model 6 shows findings for neighborhood level adversities, which are not statistically significant, but black and white children continue to have differential mental health outcomes. For each additional year of age, white children’s scores increase by .31 and black children’s decrease by .32 (p < .01), holding all other factors constant.
An additive measure examines the impact of having childhood adversities across multiple domains in Model 7. A child with the maximum score has adversities at the child, parent, family, and neighborhood levels and maltreatment allegations. For each additional domain of adversity, internalizing problems scores increase by 1.03 (p< .05). Even with all potential adversities in the analytic model, evidence for the race mental health paradox persists. For each additional year of age, white children’s scores increase by .28 and black children’s scores decrease by .29. Inearly childhood, as the number of domains withadversity increases, internalizing problems scores do not vary by race, as seen in Figure 3. By age 12, though, among children with adversities in three, four, or five domains, white children’s scores increase at a faster rate than black children. This pattern is consistent at ages 14 and 16.
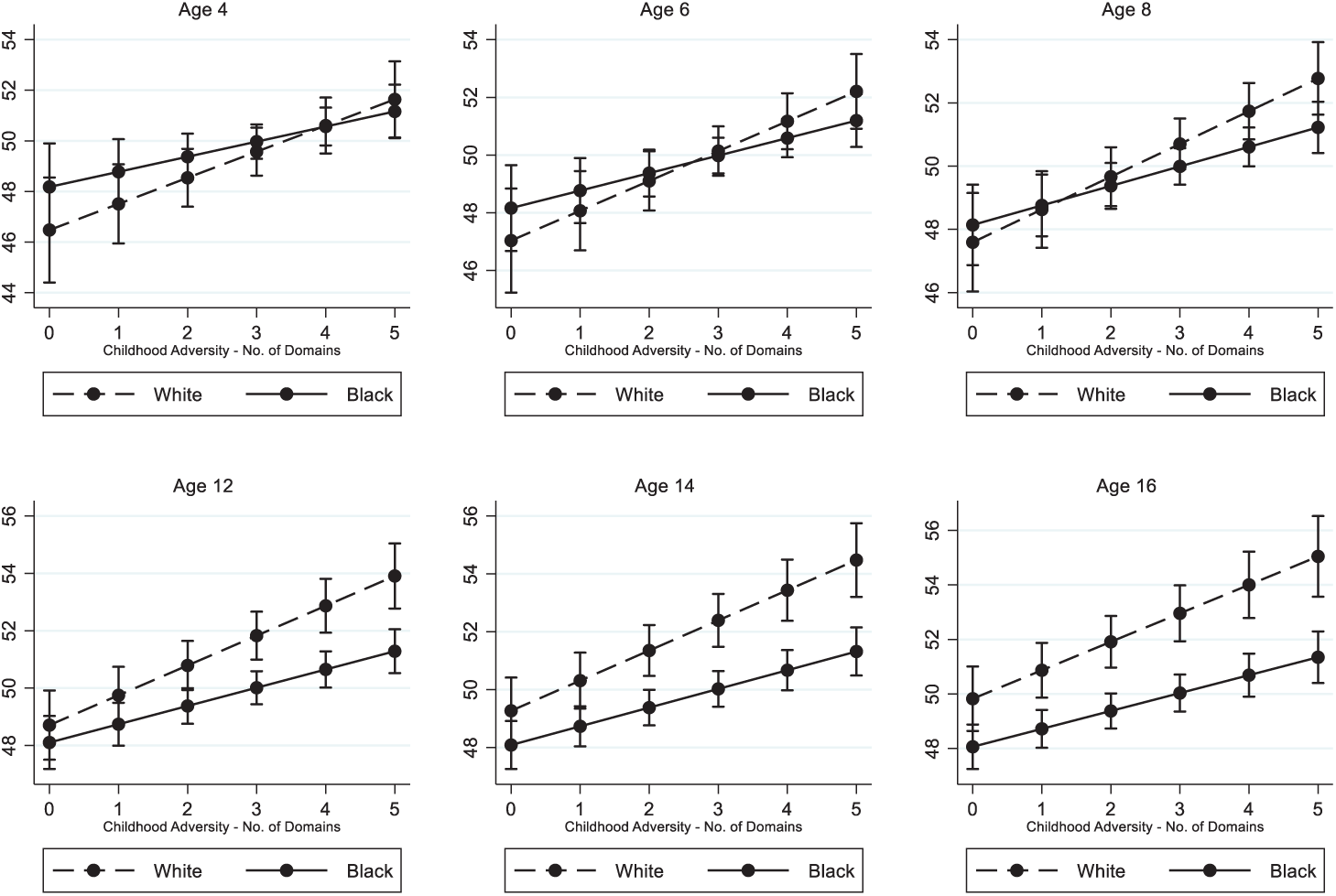
Marginal predicted internalizing problems scores and number of childhood adversity domains by age.
These models give significant evidence for the race mental health paradox—that it emerges during childhood and endures. Even when considering adversities in multiple domains, including those that children directly face as well as those they indirectly bear the consequences of, black children have better mental health than their white peers. Questions remain as to the mechanisms driving better mental health among black children and adults despite high levels of adversity, or alternatively, such poor mental health among whites. Sociologists have associated social ties with better mental health (Kawachi and Berkman 2001); therefore, I examine two potential moderating characteristics.
Early social support—the number of helpful adults as identified by the child—has an enduring effect on children’s mental health, but patterns are complex and vary by race, as seen in Table 6. Among those with 0 supportive adults at age 6 and low (0 or 1) parent level adversities at age 8, black children have lower scores at age 8 compared with white children. This suggests that black compared with white children have resilient mental health despite no supportive adults and few parent level adversities. Among children with 3 supportive adults and low parent level adversities, internalizing problems do not vary by race, yet when adversities are high, black children have better mental health than their white peers. In other words, Figure 4 shows that having 3 supportive adults at age 6 diminishes the effects of high parental level adversity at age 8 more so for black than white children (p < .05). Patterns for other types of adversities, race, and social support are similar and therefore omitted from the table.
Effects of Early Social Support, Race, and Adversity on Internalizing Problems.
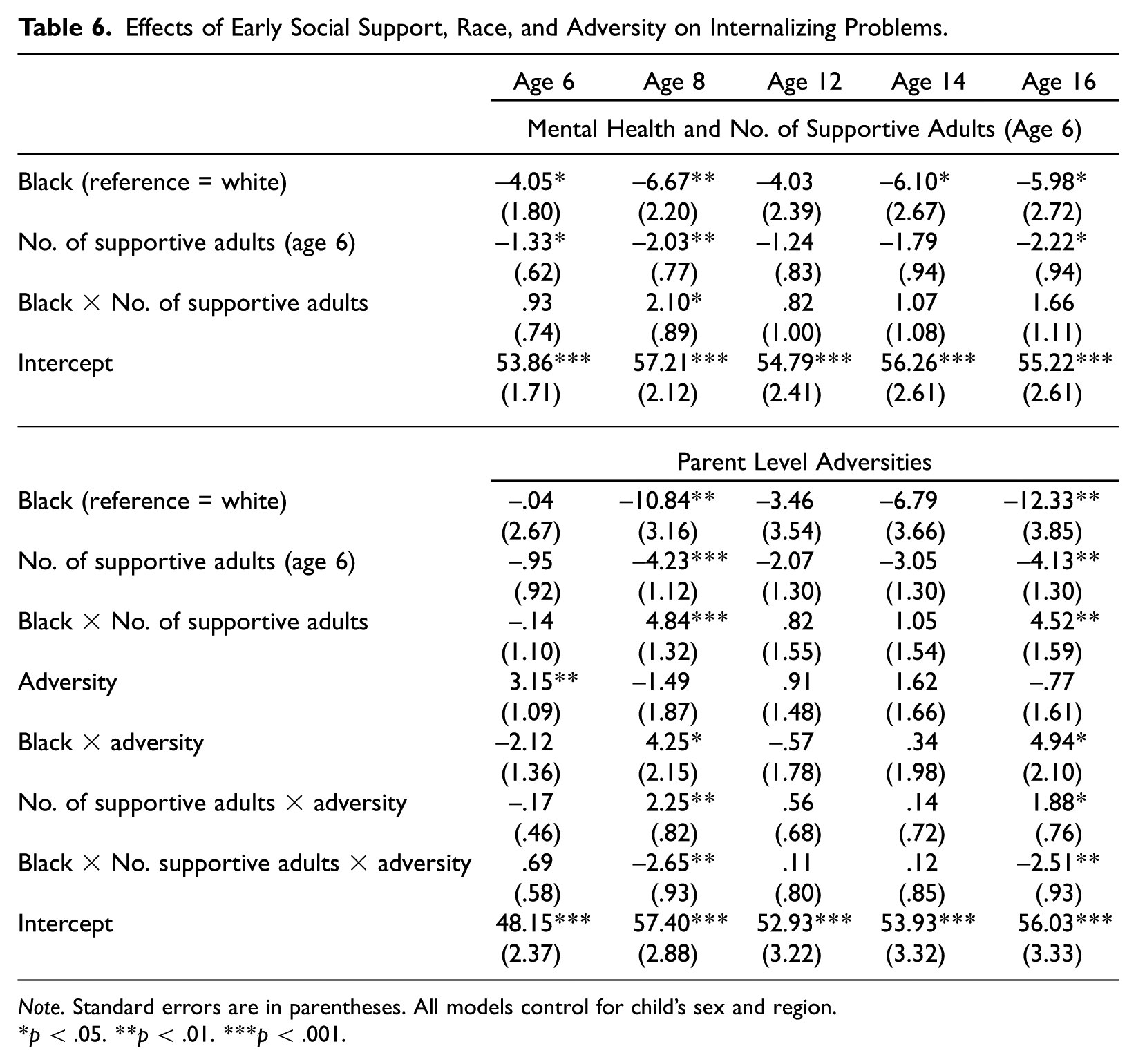
Note. Standard errors are in parentheses. All models control for child’s sex and region.
p < .05. **p < .01. ***p < .001.
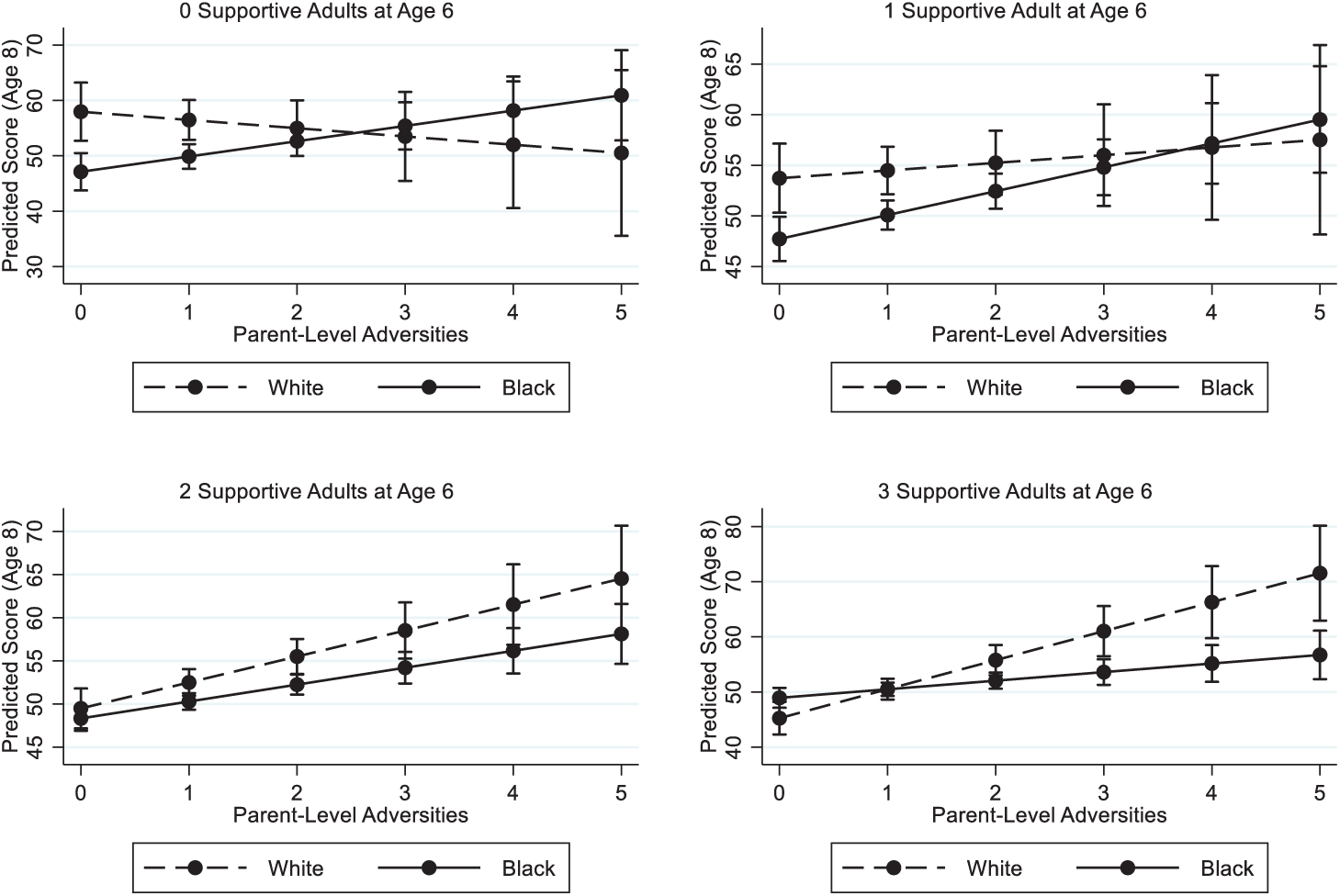
Effect of supportive adults at age 6 on internalizing problems scores at age 8.
The final set of models examined the total amount of support by the supportive caregivers at age 6 from the child’s perspective, with higher scores indicating more support in caring, explaining, spending time, and helping with necessities. The total amount of support at age 6 has a lingering effect on children’s mental health depending on the context and magnitude of adversity. When parent level adversity is lowest (= 0) at age 8, having no support from adults at age 6 has an adverse effect for white but not black children. When parent adversity is highest at age 8, black children have lower scores than their white peers when the total amount of support from helpful adults is high, shown in Table 7 and Figure 5 (p < .05). Thus, some of the paradox among black youth in this sample is likely due to high levels of support from adults and indicates that high levels of support are not enough to diminish mental health risk among white youth with many parent level adversities.
Effects of Early Social Support, Race, and Adversity on Internalizing Problems
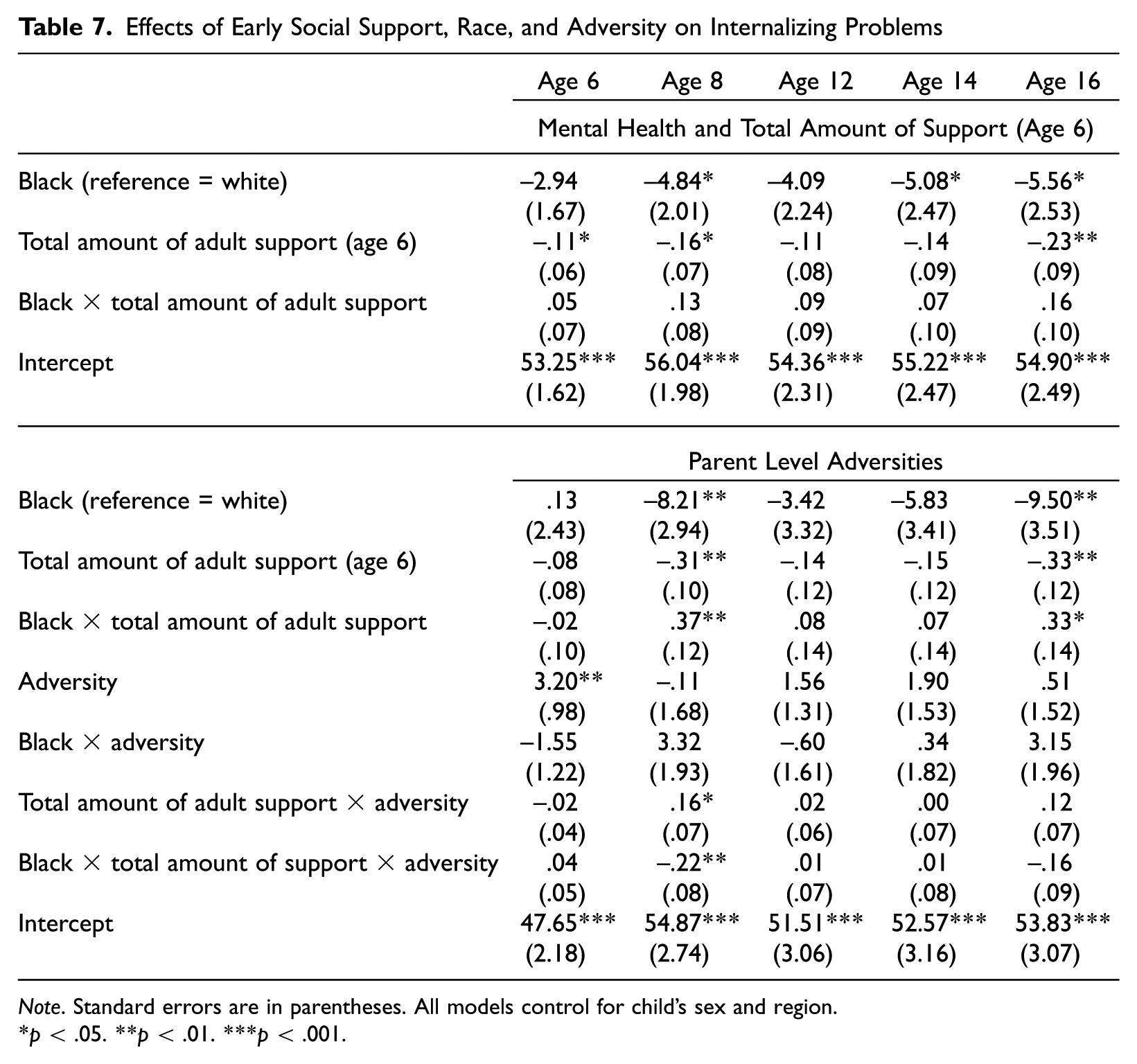
Note. Standard errors are in parentheses. All models control for child’s sex and region.
p < .05. **p < .01. ***p < .001.
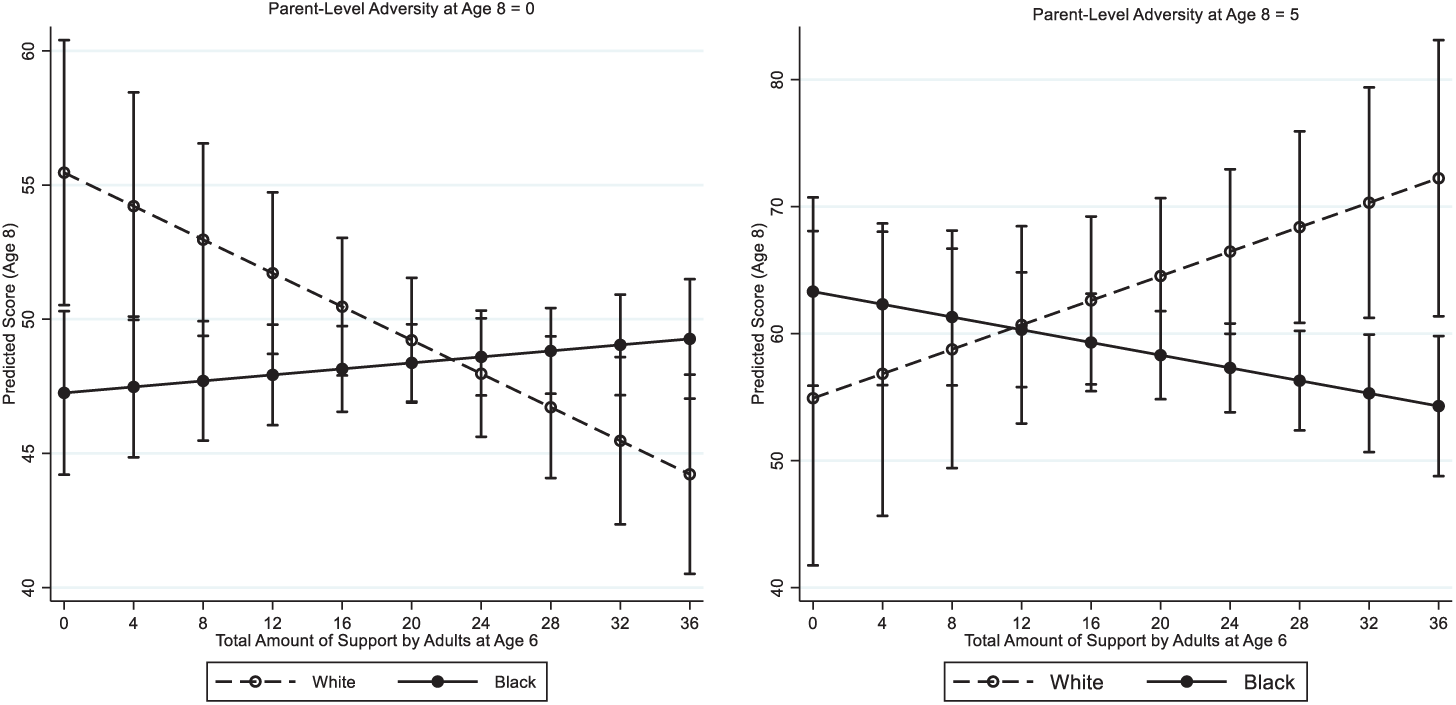
Total amount of support by helpful adults at age 6 on internalizing problems scores at age 8.
Discussion
The race mental health paradox has received considerable attention in its antecedents and consequences among adults (Erving and Thomas 2018; Mezuk etal. 2013). However, the existing description of the paradox, that black adults have similar or better mental health than white adults despite greater stress exposure, omits the accumulation of adversity and mental health trajectories that are established well before a socially constructed age of adulthood (Elder etal. 2003). Adverse childhood events, experiences, and conditions and the resulting outcomes that emerge early in the life course are important for understanding inequalities in health and aging (Ferraro and Shippee 2009). By expanding our knowledge of when and under what contexts the paradox emerges, researchers can isolate the critical periods and mechanisms promoting better mental health among black youth despite adversity. Such mechanisms protecting mental health may come at a steep price (e.g., poorer physical health—Jackson etal. 2010) that helps perpetuate racial health disparities throughout the life course.
This study has three purposes: first, to examine black–white differences in children’s risk of developing internalizing problems and determine whether the race mental health paradox emerges prior to adulthood; second, if the paradox exists, to investigate under what contexts the paradox endures; and third, to explore whether social support promotes better mental health among black children despite adversity. In these pursuits I tested the hypotheses shown in Table 8:
Hypotheses.
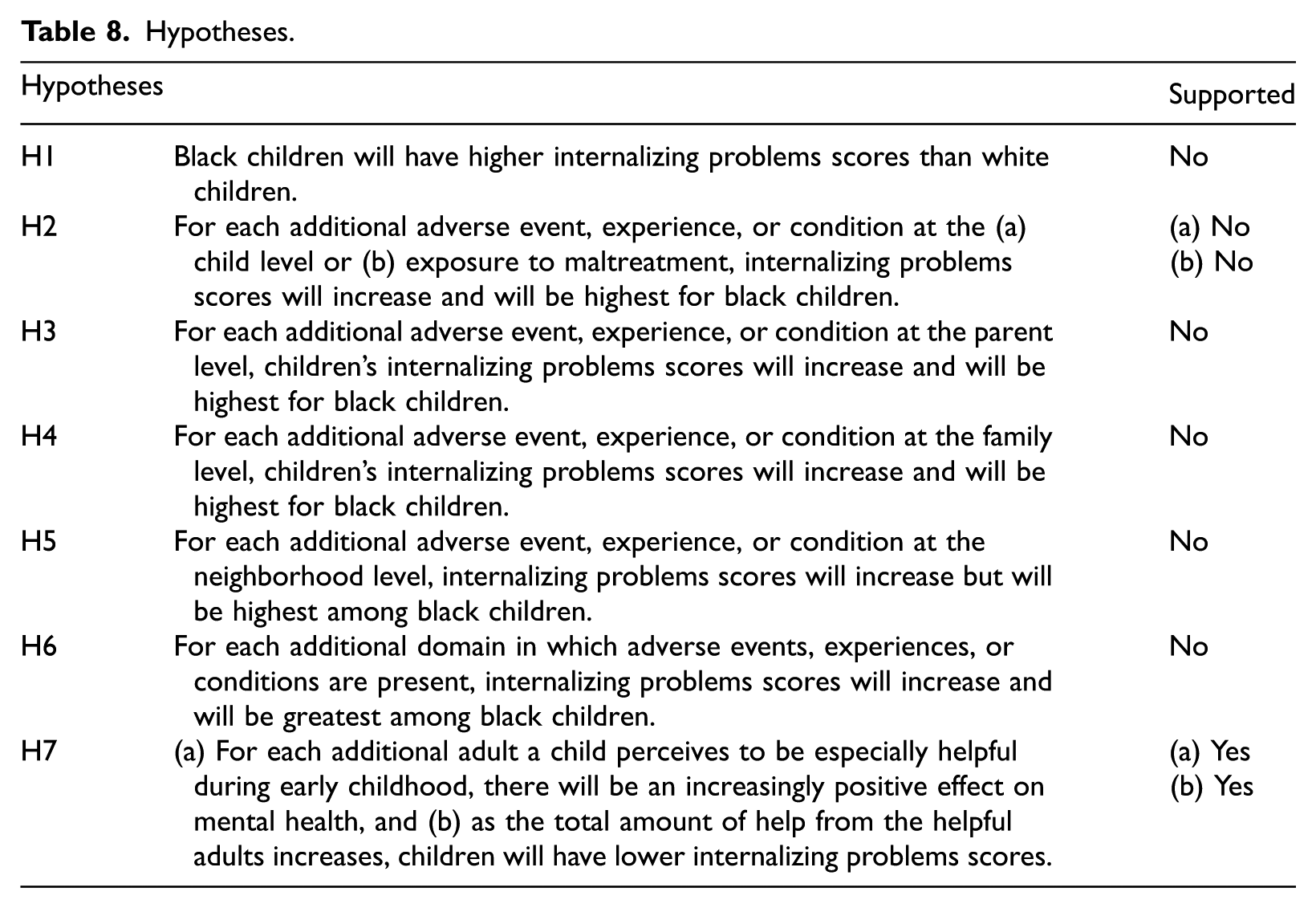
Based on prior scholarship and CIT (Ferraro and Shippee 2009), I anticipated that black children would face more adversity and as a result worse mental health outcomes. Consistent with previous studies, black children in the LONSCAN sample faced more adversity in some domains (e.g., family and neighborhood levels and the total number of domains) (DeNavas-Walt and Proctor 2014; Leventhal and Brooks-Gunn 2000; Turner and Avison 2003; Williams etal. 1997); however, mental health problems were greatest among white children. In fact, black children had similar or better mental health than white children as early as age 4, which supports the early emergence of the paradox.
Social systems generate inequality on multiple levels, and inequality can spread across life domains (Ferraro etal. 2009). By examining adverse events, experiences, and conditions across domains, we can best understand the nature of inequality and the implications for children’s differential mental health risk. In some contexts (e.g., maltreatment and family level adversity), black children with any allegations of maltreatment or the highest levels of family adversity had internalizing problems scores more in line with black and white children without such adversities. These results provide further evidence of the paradox emerging prior to adulthood and despite multiple domains of adversity.
Although there is strong evidence of a race mental health paradox when family level adversities are considered, when parent level adversities are examined, the mental health paradox is not as evident. Black children whose parents reported the most adversity had internalizing problems scores similar to white children with high adversity, and both groups were worse off than black and white children without parenting adversities. These contrasting results at the parent and family levels highlight the importance of considering the context of adversities rather than summing up all adversities into a singular, indistinct measure. Moreover, parental adversity—be it health, education, employment, or history of trauma—can negatively affect children’s mental health, and the findings make clear the need for early and effective interventions to support parents with such adverse experiences (Connell and Goodman 2002; Mclaughlin etal. 2011; Moylan etal. 2010; Reiss 2013; Waters etal. 2000).
Evidence of the race mental health paradox among children with family level adversities may also suggest that the dynamics or support within black families is especially effective in protecting children’s mental health despite such adversities (Brown 2008). Adversities can increase the risk of poor outcomes, but the availability of resources or human agency can help offset risk (Ferraro and Shippee 2009). Therefore, I examined the moderating effects of early social support (at age 6).
Young children often form strong attachments with their primary caregivers, and even among middle-school-aged children, feeling support from parents was the strongest predictor of better mental health (Stewart and Suldo 2011). Considering the perceptions of social support from the child’s perspective is important; individual perceptions of support, social comparisons, and timing of resources can influence psychosomatic processes (Ferraro and Shippee 2009). Social support for children can come from multiple sources, and the type of support provided is also important in combatting adversity (Kawachi and Berkman 2001; Levitt etal. 1993; Stewart and Suldo 2011).
I expected that as the number of adults a child perceived to be especially helpful increased, there would be a positive effect on mental health. This hypothesis was supported: As the number of supportive adults at age 6 increased, internalizing problems scores decreased at ages 6, 8, and 16 years (p < .05). Even when adverse events, experiences, and conditions at the child, parent, family, and neighborhood levels were considered (only parent level is shown), the positive impact of early social support persisted (p < .05). These findings illustrate the profound influence that supportive adults can have on a young child throughout childhood and that this support can come from multiple sources in addition to parents.
For most of the children in the LONGSCAN sample, mothers and fathers were the first helpful adult reported, followed by grandmothers and non–family members. Other adults also played influential roles, including foster parents, extended family members, teachers, religious community members, and social and health care workers. This may mean that for young children with limited or inconsistent supportive adults, community-based mentoring programs could fill a valuable need particularly among children with high levels of childhood adversity (Garner and Shonkoff 2012).
Descriptive analyses revealed that among the LONGSCAN sample there were no significant black–white differences in the number of supportive adults or the total amount of support these adults provided. Yet, the influence of social support differentially influenced black and white children’s mental health. Among children with no supportive adults at age 6 and low levels of parental adversity at age 8, black children had better mental health than white children; however, as adversities increased, black–white mental health differences diminished. Among children with 3 supportive adults at age 6, as the number of adversities increased at age 8, white children had the highest risk of mental health problems.
In other words, having multiple supportive adults early on is more effective in moderating mental health risk for black children with high levels of parental adversity than for white children. This is consistent with research that emphasize the strength and benefits of extended kin networks for protecting black children’s mental health (Brown 2008). It is possible that other mechanisms are also working in collaboration with social support, including racial socialization, strong religious identities, and/or poor health behaviors (Boardman and Alexander 2011; Ellison etal. 2001; Jackson etal. 2010; Keyes 2009).
This study is not without limitations; one concern is that children’s mental health is reported on by a parent or caregiver, rather than using the child’s self-report. Parents may not always be able to accurately report or observe when their child is experiencing symptoms of depression, anxiety, or somatic issues and, therefore, may underreport such problems in children (Herman etal. 2018). Alternatively, when parents suffer from mental and physical health problems themselves, it is possible that they could overreport symptoms in their children as well.
Supplemental analyses (results not shown) indicated that parental depression symptoms were positively correlated with children’s internalizing problems scores, although the strength of these correlations was weak to moderate. This indicates that as parents’ depressive symptoms increased, so too did reporting children’s internalizing problems (p < .001). Moreover, children with parents who self-reported as having fair or poor health had higher internalizing problems scores, on average, than children with healthier parents (p < .001). Future studies should consider internalizing problems scores from multiple report sources (Herman etal. 2018) and from child reports when possible and age-appropriate.
Another limitation of this study is the purposive sampling design of the original LONGSCAN data, which means the findings from this research are not generalizable beyond the scope of the sample. LONGSCAN also has some challenges with attrition, as do most panel datasets. However, LONGSCAN provides an excellent opportunity to examine changes in children’s mental health over seven waves of data, with sufficient sample sizes to test for racial differences in outcomes, adversities measured across four ecological domains, and information on social support. Thus, LONGSCAN yields a way to test for when the race mental health paradox emerges, under which contexts the paradox endures, and which resources may play a role in driving the paradox, at least in a high-risk sample. Future research should expand on this work using a more representative sampling design.
Overall, this study confirms that the race mental health paradox emerges much earlier in the life course than previously identified and that differential mental health patterns persist in the context of various adversities. In terms of understanding the mechanisms that drive such a paradox, this study specifically examined social support. Although social support was operationalized in terms of early childhood support from helpful adults and the types of support provided, this study investigated only the moderating effects of this mechanism. Future studies should consider potential mediating factors related to childhood adversity (and other accumulation methods), race, social support, and children’s mental health. In addition, scholars need to examine other factors that promote mental health resilience during childhood and adolescence and whether such resilience comes at the expense of poor physical health or adverse outcomes elsewhere (Brown 2008; Jackson etal. 2010; Keyes 2009; Mouzon 2014).
Footnotes
Appendix
| Childhood Adversities by Ecological Level | Child’s Age in Years | ||||||
|---|---|---|---|---|---|---|---|
| Neighborhood Level Adversities | 4 | 6 | 8 | 12 | 14 | 16 | 18 |
|
|
0–1 | 0–1 | 0–1 | ||||
|
|
0–1 | 0–1 | 0–1 | ||||
|
|
0–1 | 0–1 | 0–1 | ||||
|
|
0–1 | 0–1 | |||||
|
|
0–1 | 0–1 | |||||
|
|
0–1 | 0–1 | |||||
|
|
0–1 | ||||||
|
|
0–1 | ||||||
|
|
0–1 | ||||||
|
|
0–1 | ||||||
| Total | 0–3 | 0–4 | 0–3 | 0–3 | 0–3 | 0–3 | |
Note. Values are range for each item and total adversities by age. All items are parent/caregiver report.