
Abstract
Background:
Chemotherapy-related cognitive impairment (CRCI), commonly known as “chemobrain,” frequently occurs during breast cancer treatment and has been linked to altered brain function. This resting-state functional magnetic resonance imaging study examined chemotherapy-related changes in functional brain activity, network connectivity, and associations with cognitive outcomes.
Methods:
Twenty-eight patients with breast cancer were assessed prechemotherapy (BB) and postchemotherapy (BBF), alongside 27 healthy controls of comparable age at baseline (BH) and follow-up (BHF). Mean fractional amplitude of low-frequency fluctuations (mfALFF) and mean regional homogeneity (mReHo) quantified functional brain activity. Graph theoretical analysis (GTA) assessed network topology; network-based statistics (NBS) evaluated interregional connectivity. Cognitive performance was evaluated through standardized assessments.
Results:
Postchemotherapy patients exhibited reduced anxiety and lower FACT-Cog scores. Voxel-wise analyses showed increased mfALFF in frontal regions and mReHo in superior temporal and inferior frontal gyri, alongside decreases in postcentral, lingual, and parahippocampal areas. Healthy controls showed increased activity in medial frontal and cingulate regions, with reductions in the temporal lobe and putamen. GTA revealed higher global efficiency and reduced modularity, path length, and network complexity in the BBF group compared with BHF. NBS showed weaker structural connectivity in motor and occipital regions prechemotherapy and decreased parietal and insular connectivity postchemotherapy. Multiple regression showed brain–behavior correlations: declines in FACT-Cog, Digit Symbol Substitution, and mood scores were linked to altered activity in frontal, parietal, cingulate, and occipital areas, while positive correlations suggested compensatory activation.
Conclusions:
Chemotherapy was associated with longitudinal alterations in brain activity, network organization, and connectivity in breast cancer survivors. Brain–behavior associations suggest disrupted neural networks may underlie CRCI.
Keywords
Impact Statement
Our longitudinal fMRI study provides novel insights into how chemotherapy affects functional brain activity and network connectivity in breast cancer survivors. By integrating resting-state imaging metrics with neuropsychological outcomes, we identified dynamic alterations in neural function that correlated with cognitive changes over time. These findings highlight the vulnerability of specific brain networks to cancer therapy and underscore the need for monitoring neurocognitive health as part of survivorship care. Beyond advancing neuroscientific understanding, our results inform clinical practice by emphasizing early detection, prevention, and potential intervention strategies to mitigate treatment-related cognitive impairment and improve quality of life.
Introduction
As of 2022, breast cancer remained the second most commonly diagnosed cancer worldwide and one of the primary contributors to cancer-related deaths among women, with an estimated 2.3 million new cases and 666,000 deaths reported globally (Bray et al., 2024). Although therapeutic advances have enhanced survival outcomes, a considerable number of patients continue to experience persistent side effects. One such effect is cognitive dysfunction associated with chemotherapy, often described as “chemobrain.” Cognitive domains affected by this condition include memory, information processing, learning ability, and executive functioning (Lepage et al., 2014; Wefel and Schagen, 2012). Notably, more than 30% of patients exhibit cognitive decline even prior to systemic therapy, and up to 75% report symptoms during treatment, with approximately one-third experiencing persistent issues for years after therapy (Janelsins et al., 2014).
Although chemotherapy-related cognitive impairment (CRCI) research has focused largely on breast cancer, similar deficits have been reported in patients with lung, testicular, and colorectal cancers (Simó et al., 2015; Vardy et al., 2015; Wefel et al., 2011). Multiple predisposing factors have been identified, including age, menopausal status, socioeconomic status, comorbidities, and lifestyle variables (Ahles and Root, 2018; Janelsins et al., 2014; Wefel et al., 2015). Biological mechanisms such as elevated proinflammatory cytokines (IL-6, IL-1β, sTNFRI), genetic polymorphisms (e.g., APOE, COMT), and psychological conditions including post-traumatic stress have also been implicated (Ahles et al., 2008; Kesler et al., 2013; McDonald and Saykin, 2013; Williams et al., 2018). These findings highlight the multifactorial nature of CRCI, indicating that it may arise from a complex interaction of physiological and psychological factors rather than being solely attributed to chemotherapy.
Resting-state functional magnetic resonance imaging (rs-fMRI) provides a powerful noninvasive tool to investigate the underlying neural mechanisms of CRCI and has been effectively applied in cancer-related cognitive research (Dumas et al., 2013; Lee et al., 2013). Two key rs-fMRI indices include fractional amplitude of low-frequency fluctuations (fALFF), quantifying the strength of spontaneous neural activity, and regional homogeneity (ReHo), assessing the temporal coherence of neural activity among neighboring voxels (Zang et al., 2004; Zou et al., 2008). In this study, we focus on their mean values—mfALFF and mReHo—which are complementary rather than interchangeable: mfALFF reflects neural signal intensity, whereas mReHo captures local synchrony. Altered mfALFF may indicate changes in excitability or compensatory hyperactivation, while abnormal mReHo may suggest impaired local coherence. At the network level, graph theoretical analysis (GTA) and network-based statistics (NBS) quantify efficiency and connectivity across distributed circuits, with disruptions hypothesized to impair cognitive specialization and integration. Together, these metrics provide a mechanistic framework to understand how chemotherapy-related neural alterations may translate into deficits in attention, processing speed, and memory. Beyond localized measures, GTA characterizes large-scale network topology, while NBS identifies group differences in connectivity between distinct brain regions (Rubinov and Sporns, 2010; Zalesky et al., 2010). These neuroimaging techniques have proven effective in detecting CRCI-associated changes in brain network architecture (Chen et al., 2024a). In patients with breast cancer, both structural and functional brain alterations have been documented, regardless of chemotherapy exposure. These include disruptions in brain volume, network organization, and connectivity within attention and frontoparietal networks, which have been associated with cognitive dysfunction and blood-based biomarkers (Deprez et al., 2011; Hu et al., 2023; McDonald et al., 2010). However, much of the existing evidence is derived from cross-sectional studies, limiting the ability to infer longitudinal changes and causality. To address this limitation, our prior work demonstrated chemotherapy-related disruptions in white matter integrity and structural connectivity (Chen et al., 2024a; Chen et al., 2024b). Building on these findings, the present study employs resting-state fMRI to examine functional brain activity and large-scale network connectivity, providing a complementary perspective on the neurobiological mechanisms underlying CRCI.
This study had two aims: (1) to examine longitudinal alterations in spontaneous brain activity and connectivity following chemotherapy in patients with breast cancer compared with healthy controls using resting-state metrics (mfALFF, mReHo, GTA, NBS); and (2) to assess whether these alterations were linked to cognitive and affective outcomes. We hypothesized that chemotherapy would increase mfALFF/mReHo in frontal–temporal regions and decrease them in parietal–occipital regions, with reduced network efficiency and modularity. We further predicted associations between these neural changes and cognitive decline and mood symptoms.
Materials and Methods
Experimental design and study subjects
This study was approved by the Institutional Review Board of Chang Gung Memorial Hospital, Chiayi, Taiwan (IRB Nos. 104-5082B, 201700256B0, 201702027B0), and written informed consent was obtained from all participants prior to their enrollment. Inclusion criteria required women aged over 20 years with a confirmed pathological diagnosis of primary breast cancer. Participants were excluded if they had terminal-stage breast cancer; had previously received treatment for another type of malignancy; had undergone radiotherapy prior to enrollment; presented with cerebral metastasis or neurological disorders; had a documented psychiatric illness or substance abuse history; or had any contraindications to MRI scanning.
A total of 28 individuals with breast cancer scheduled for chemotherapy (BB group) and 27 healthy controls matched by age (BH group) participated in the study. For longitudinal follow-up, the 28 BB participants were reevaluated postchemotherapy (BBF group), and the 27 BH participants were re-assessed at a similar interval (BHF group), resulting in 28 BB/BBF pairs and 27 BH/BHF pairs. Data at baseline (T1) were gathered after surgery but prior to the initiation of chemotherapy, while longitudinal data at T2 were collected 8–39 months after chemotherapy completion. Assessments included resting-state fMRI and cognitive evaluations at both time points.
Clinical assessments
Subjective and objective cognitive function, along with mood symptoms, were assessed using self-reported questionnaires and standardized neuropsychological tests administered by trained staff under professional supervision. The Patient Health Questionnaire-9 (PHQ-9) (Kroenke et al., 2001), a commonly employed self-report measure, was used to assess depressive symptoms. It comprises nine items aligned with Diagnostic and Statistical Manual of Mental Disorders (DSM) criteria for major depressive disorder; a score between 0 and 3 is given for each question. A higher score within the 0–27 range corresponds to more severe depression. The self-reported Hospital Anxiety and Depression Scale–Anxiety subscale (HADS-A) (Snaith, 2003) was utilized to measure anxiety symptoms in clinical populations. This scale includes seven questions rated on a four-level scale, yielding a total score ranging from 0 to 21, with higher scores indicating more severe anxiety symptoms. The FACT-Cog Version 3 (Functional Assessment of Cancer Therapy–Cognitive Function) (Costa et al., 2018) is a self-administered instrument designed to evaluate cognitive functioning in individuals with cancer. It reflects individuals’ perceived impact of cognitive difficulties on everyday functioning and life satisfaction, where lower scores indicate more severe subjective cognitive decline. The Digit Symbol Substitution (DSS) (Jaeger, 2018) test is a commonly applied psychological testing tool that assesses processing speed, attention, and overall mental efficiency. Participants are instructed to connect symbols with their corresponding numbers using a reference table within a fixed time limit of typically 90–120 sec. Lower test scores reflect reduced cognitive performance. The DSS test was chosen as an objective cognitive measure because it is sensitive to deficits in processing speed and attention (domains frequently impaired in CRCI) and feasible for repeated administration within our clinical workflow.
Functional MRI
MRI scanning
Functional MRI data were collected on a 3.0-T Siemens Magnetom Verio system (Siemens Medical Systems, Erlangen, Germany) utilizing a 32-channel head coil. A gradient echo-planar imaging sequence was employed to capture resting-state functional scans. Each volume comprised 31 axial slices, and a complete set of 300 image volumes was obtained per session. A TR of 2,000 ms, TE of 30 ms, 90° flip angle, and voxel dimensions of 3.4 × 3.4 × 4.0 mm³ were used in the scanning protocol, achieving a temporal resolution of 2 sec. The acquisition of 300 volumes at this repetition time corresponded to a total resting-state scan duration of approximately 10 min per session. During the image acquisition, individuals were asked to keep their eyes shut, minimize movement, stay awake, and not focus on any task. Head cushions and hearing protection were applied to limit subject motion and attenuate scanner-related noise.
Functional image preprocessing
fMRI preprocessing was carried out with REST (v1.8) (Song et al., 2011) in combination with SPM12, implemented in MATLAB. The preprocessing pipeline included the workflow consisted of: (1) The initial 10 volumes of each scan were discarded to allow for signal stabilization; (2) slice timing was adjusted to correct for differences in acquisition order; (3) motion correction was performed by realigning all volumes to a designated reference image; (4) each participant’s functional data were co-registered to their corresponding T1-weighted anatomical image, followed by tissue segmentation and spatial normalization to the Montreal Neurological Institute (MNI) template with a voxel size of 3 mm³; (5) spatial smoothing was conducted using a Gaussian kernel with a 6 mm full width at half maximum; (6) low-frequency noise and signal drift were reduced through frequency transformation and detrending using REST; (7) temporal filtering was conducted using a 0.01–0.12 Hz band-pass to minimize scanner-related and physiological noise; and (8) smoothed data were used to compute mfALFF, while mReHo was derived from the original, unsmoothed images.
fMRI feature analysis
After preprocessing, two resting-state fMRI indices—ALFF and ReHo—were derived using the Automated Anatomical Labeling (AAL) (Tzourio-Mazoyer et al., 2002) atlas, which was employed to classify the brain into 90 anatomical segments. The amplitude of low-frequency fluctuations (ALFF) indicates the strength of spontaneous neural signals and is derived by averaging the square root of the power spectrum within a preselected low-frequency range on a voxel-wise basis. The fALFF metric quantifies the fraction of low-frequency power compared to the overall spectral power (Yue et al., 2015). The mALFF represents the average ALFF intensity across the brain, while mfALFF focuses on normalized fluctuations constrained to low-frequency oscillations(Zou et al., 2008). The temporal coherence between each voxel and its adjacent 26 voxels was measured with Kendall’s coefficient of concordance to compute ReHo (Zang et al., 2004). Nonbrain areas were filtered out through a brain mask, and mReHo was computed by normalizing voxel-wise Kendall’s Coefficient of Concordance (KCC) values to the average KCC within the mask. Both mfALFF and mReHo maps were computed within a whole-brain mask after normalization to MNI space, and voxel-wise analyses were restricted to gray matter regions defined by the AAL atlas to minimize partial volume effects from white matter.
Statistical analysis
Three analytical approaches were applied in this study: voxel-based analysis, GTA, and NBS. In addition, voxel-wise multiple regression analyses were performed to assess brain–behavior associations. Demographic and clinical data were analyzed using SPSS Statistics 25 (IBM Corp., Armonk, NY).
Longitudinal analysis of mfALFF and mReHo
Repeated-measures analysis of covariance (ANCOVA) was conducted across all four groups (BB, BBF, BH, BHF), testing the Group (breast cancer vs. healthy) × Time (T1 vs. T2) interaction. Age, education, and interscan interval (months) were included as covariates; in particular, age was adjusted for in all analyses to minimize confounding. Voxel-wise significance was defined at False Discovery Rate–adjusted q value (qFDR) <0.05 with a minimum cluster size of 50 voxels. When a significant interaction was observed, post hoc simple-effects analyses were performed using paired t-tests for within-group longitudinal comparisons (BB vs. BBF, BH vs. BHF). All results were corrected for multiple comparisons.
GTA and NBS analyses
GTA was performed on smoothed fMRI data using the CONN toolbox (Whitfield-Gabrieli and Nieto-Castanon, 2012). Functional connectivity matrices (90 × 90) were constructed from AAL atlas regions (Tzourio-Mazoyer et al., 2002) using Pearson correlations. Graph metrics were calculated in the Graph Analysis Toolbox across density thresholds (0.1–0.6), and the area under the curve (AUC) was derived. Group × Time interactions were tested with repeated-measures ANCOVA, and significance was assessed using 5,000 permutations with Holm–Bonferroni correction. NBS (Zalesky et al., 2010) were applied with a cluster-forming threshold of t = 3.1 and 5,000 permutations. Connected components were defined as contiguous supra-threshold edges, with significance assessed using component-level family-wise error correction (pFWE <0.05). The threshold of t = 3.1 was chosen based on prior NBS studies to balance sensitivity and false positives.
Brain–behavior associations
Voxel-wise multiple regression analyses were performed in SPM12 to assess associations between changes in mfALFF/mReHo and clinical measures (Δ = T2 − T1). Age, education, and baseline scores were included as covariates. Statistical significance was defined at pFWE <0.05 with a cluster threshold of 150 voxels. Significant clusters were further visualized, and scatter plots were generated for brain–behavior associations.
Results
Demographic features and clinical assessments
The longitudinal analysis included only participants who remained eligible and matched across both time points (T1 and T2). A total of 55 matched pairs were selected from participants at Chang Gung Memorial Hospital, Chiayi branch. The mean interval between assessments was 12.68 ± 8.29 months for patients with breast cancer and 13.85 ± 7.14 months for healthy participants with no significant difference between groups (p = 0.369). Interscan interval was also modeled as covariate in the longitudinal analysis. Table 1 summarizes the demographic and clinical characteristics of the participants, including age, years of education, and the interval between the two time points (TP1–TP2). Following surgical intervention, baseline assessments were performed before chemotherapy began. Among patients who received chemotherapy, the most commonly administered agents were cyclophosphamide and 5-fluorouracil. Across all patients, the duration of chemotherapy averaged 154.4 ± 29.4 days (range: 105–232), providing a surrogate measure of treatment intensity in the absence of detailed cycle counts. Detailed chemotherapy and radiation exposures are provided in Supplementary Table S1. Mood symptoms were assessed with the PHQ-9 and HADS-A, while cognitive performance was measured using the FACT-Cog and DSS. Effect sizes and p values are reported for group comparisons. Within the breast cancer group, postchemotherapy assessments showed a significant reduction in anxiety levels (HADS-A, p = 0.002, partial η2 = 0.162). In contrast, FACT-Cog scores declined significantly, indicating worsened self-reported cognitive function (p = 0.026, d = 0.44). No statistically significant variation was found in PHQ-9 or DSS scores between T1 and T2 within the patient cohort. Similarly, there were no notable differences in PHQ-9 or HADS-A scores between the initial and follow-up assessments among healthy controls.
Demographic and Clinical Characteristics of the Participants
Continuous variables are shown as mean ± SD. Age, education years, and TP1–TP2 interval were compared using the Mann–Whitney U test; PHQ-9 and HADS-A with repeated-measures ANCOVA (partial η²); and FACT-Cog and DSS with paired t-tests (Cohen’s d). p < 0.05 was considered statistically significant. Significance markers.
*p < 0.05; **p < 0.01; ***p < 0.001.
ANCOVA, analysis of covariance; BB, patient with breast cancer before chemotherapy; BBF, patient with breast cancer after chemotherapy; BH, healthy control at baseline; BHF, healthy control at follow-up; DSS, Digit Symbol Substitution; FACT-Cog, Functional Assessment of Cancer Therapy–Cognitive Function, Version 3; HADS-A, Hospital Anxiety and Depression Scale–Anxiety subscale; PHQ-9, Patient Health Questionnaire-9; SD, standard deviation; TP1, time 1; TP2, time 2.
Voxel-based analysis of mfALFF
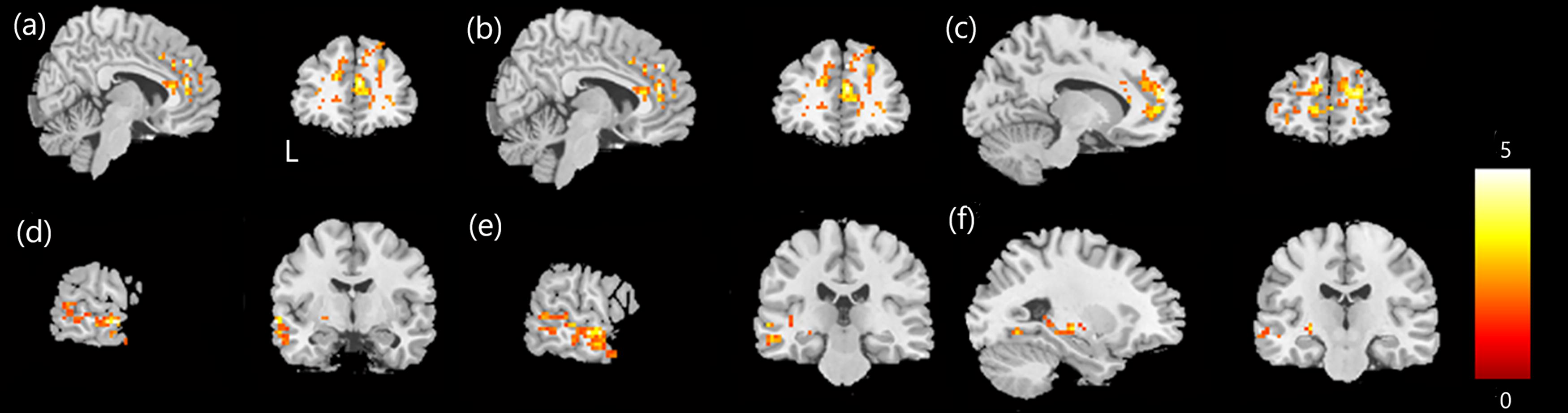
Repeated-measures ANCOVA revealed significant Group × Time interaction effects in the right postcentral gyrus, left precentral gyrus, and left inferior frontal gyrus (qFDR <0.05; minimum cluster size ≥50 voxels; Fig. 1 and Supplementary Table S2). Follow-up paired t-tests demonstrated that, in the breast cancer cohort (BB → BBF), mfALFF increased in the left inferior frontal, left medial frontal, and right middle frontal gyri but decreased in the left postcentral and right superior frontal gyri (p < 0.05; cluster size ≥150 voxels; Fig. 2 and Supplementary Table S3). In healthy controls (BH → BHF), mfALFF increased in the left precuneus, left inferior parietal lobule, and right cuneus but decreased in the left postcentral, left precentral, and left inferior frontal gyri (p < 0.05; cluster size ≥150 voxels; Fig. 3 and Supplementary Table S4).

Repeated-measures ANCOVA for mfALFF. Group differences were assessed across four time points: patients with breast cancer before and after chemotherapy and healthy controls at baseline and follow-up. Significant alterations were observed in the right postcentral gyrus
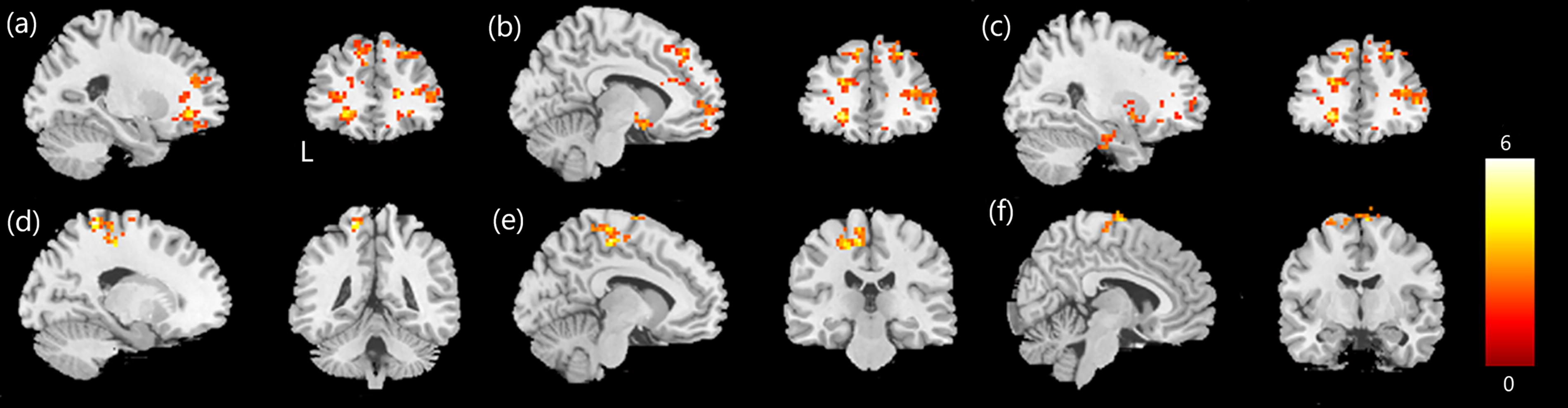
Paired t-tests for mfALFF changes in the patients with breast cancer. The BBF group (BB < BBF) showed increased mfALFF values from T1 to T2 in the left inferior frontal gyrus
Paired t-tests for mfALFF changes in healthy controls. In the BHF group (BH < BHF), mfALFF values significantly increased from T1 to T2 in the left precuneus
Voxel-based analysis of mReHo
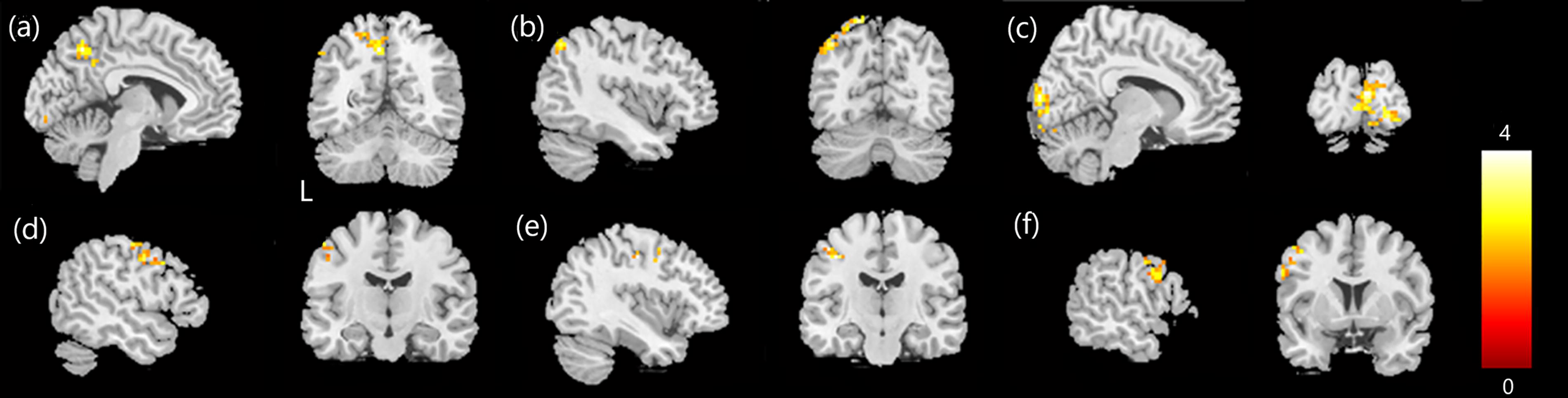
Repeated-measures ANCOVA identified significant Group × Time interaction effects in the left precentral gyrus, left putamen, right insula, and left middle frontal gyrus (qFDR <0.05; minimum cluster size ≥50 voxels; Fig. 4 and Supplementary Table S2). Follow-up paired t-tests demonstrated that, in the breast cancer cohort (BB → BBF), mReHo increased in the right superior temporal, right inferior frontal, and right medial frontal gyri but decreased in the left lingual gyrus and bilateral parahippocampal regions (p < 0.05; cluster size ≥150 voxels; Fig. 5 and Supplementary Table S3). In healthy controls (BH → BHF), mReHo increased in the right anterior cingulate, right medial frontal, and left anterior cingulate gyri but decreased in the left middle temporal, left superior temporal, and left putamen (p < 0.05; cluster size ≥100 voxels; Fig. 6 and Supplementary Table S4).
Repeated-measures ANCOVA for mReHo. Group differences were assessed across four time points: patients with breast cancer before and after chemotherapy and healthy controls at baseline and follow-up. Significant alterations were observed in the left precentral gyrus
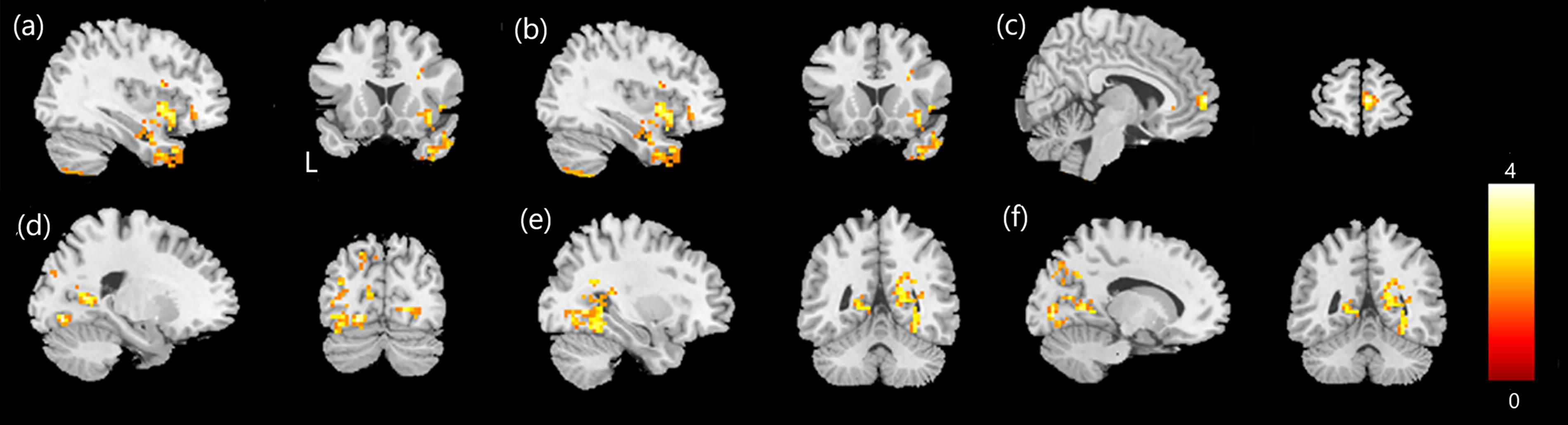
Paired t-tests for mReHo changes in patients with breast cancer. In the BBF group (BB < BBF), mReHo values significantly increased from T1 to T2 in the right superior temporal gyrus
Paired t-tests for mReHo changes in healthy controls. In the BHF group (BH < BHF), mReHo values significantly increased from T1 to T2 in the right anterior cingulate
GTA analysis
Group × Time interaction analyses across AUC-based global metrics (density 0.10–0.60) showed that postchemotherapy patients (BBF) exhibited lower characteristic path length, modularity, and normalized shortest path length but higher global efficiency compared with healthy follow-up (BHF) (permutation p < 0.05, Holm–Bonferroni corrected; Fig. 7). No significant within-group longitudinal changes were observed in isolation (BB vs. BBF; BH vs. BHF).
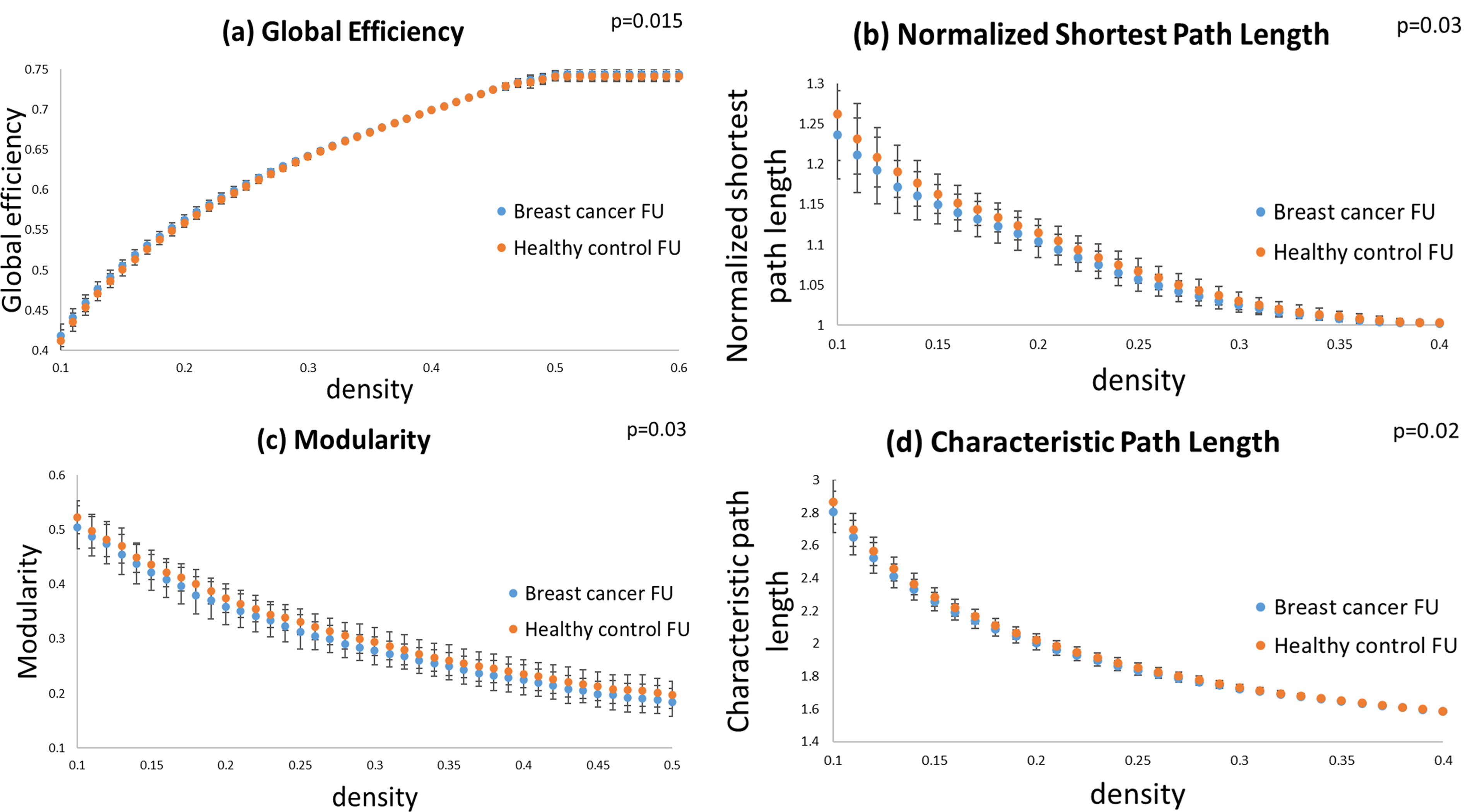
Topological properties of network connectivity. Group differences between BBF and BHF were observed in
NBS analysis
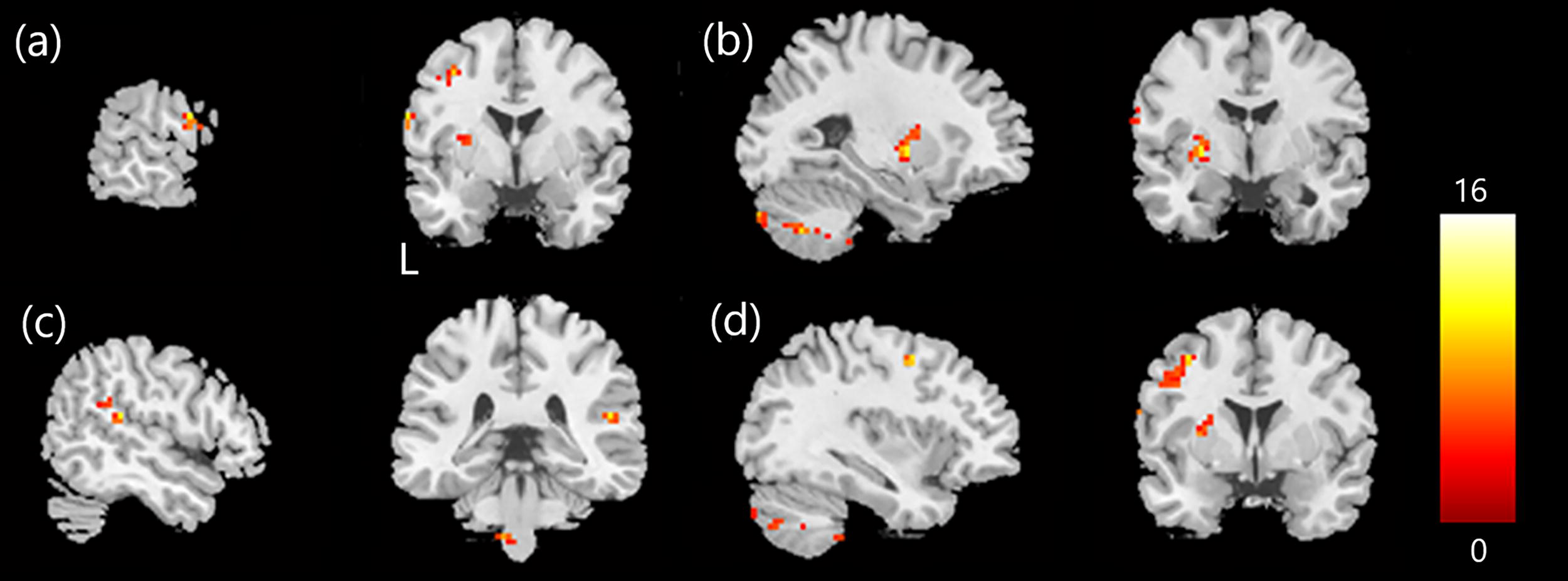
NBS revealed significant network-level Group × Time effects (threshold t = 3.1; 5,000 permutations; component-level pFWE <0.05). Prechemotherapy (BB vs. BH) patients showed reduced connectivity in subnetworks including the supplementary motor area, precentral gyrus, occipital cortex, and inferior frontal gyrus (Fig. 8a). Postchemotherapy (BBF vs. BHF) showed additional reductions in Heschl’s gyrus, parietal lobules, insula, precentral gyrus, and Rolandic operculum (Fig. 8b).
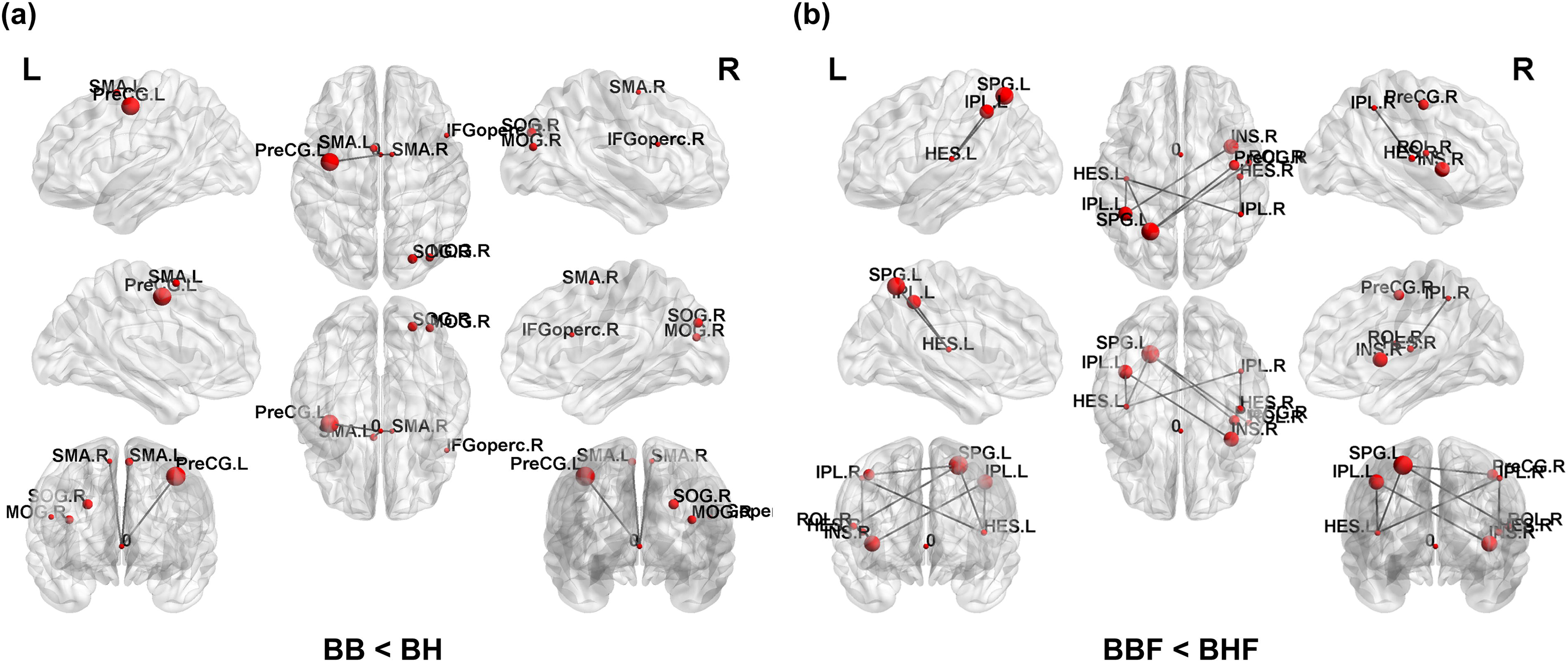
Network-based statistics (NBS) results showing significantly reduced functional connectivity.
Brain–behavior associations
Voxel-wise multiple regression analyses demonstrated significant correlations between changes in mfALFF/mReHo and clinical measures. Declines in FACT-Cog scores were linked to reduced activity in the posterior cingulate and lingual gyri, while DSS declines were associated with decreased activity in the cuneus and parietal lobule (Fig. 9). Increases in PHQ-9 scores correlated with reduced activity in the medial frontal and anterior cingulate regions. In contrast, higher FACT-Cog and DSS scores correlated with increased activity in the medial frontal, cingulate, and fusiform regions, and mood scores (PHQ-9, HADS-A) were positively associated with activity in the precentral and posterior cingulate regions (Fig. 10). Detailed clusters, MNI coordinates, and statistical values are provided in Supplementary Table S5. Representative scatter plots illustrating significant negative and positive correlations are shown in Supplementary Figures S1 and Figure S2, respectively.
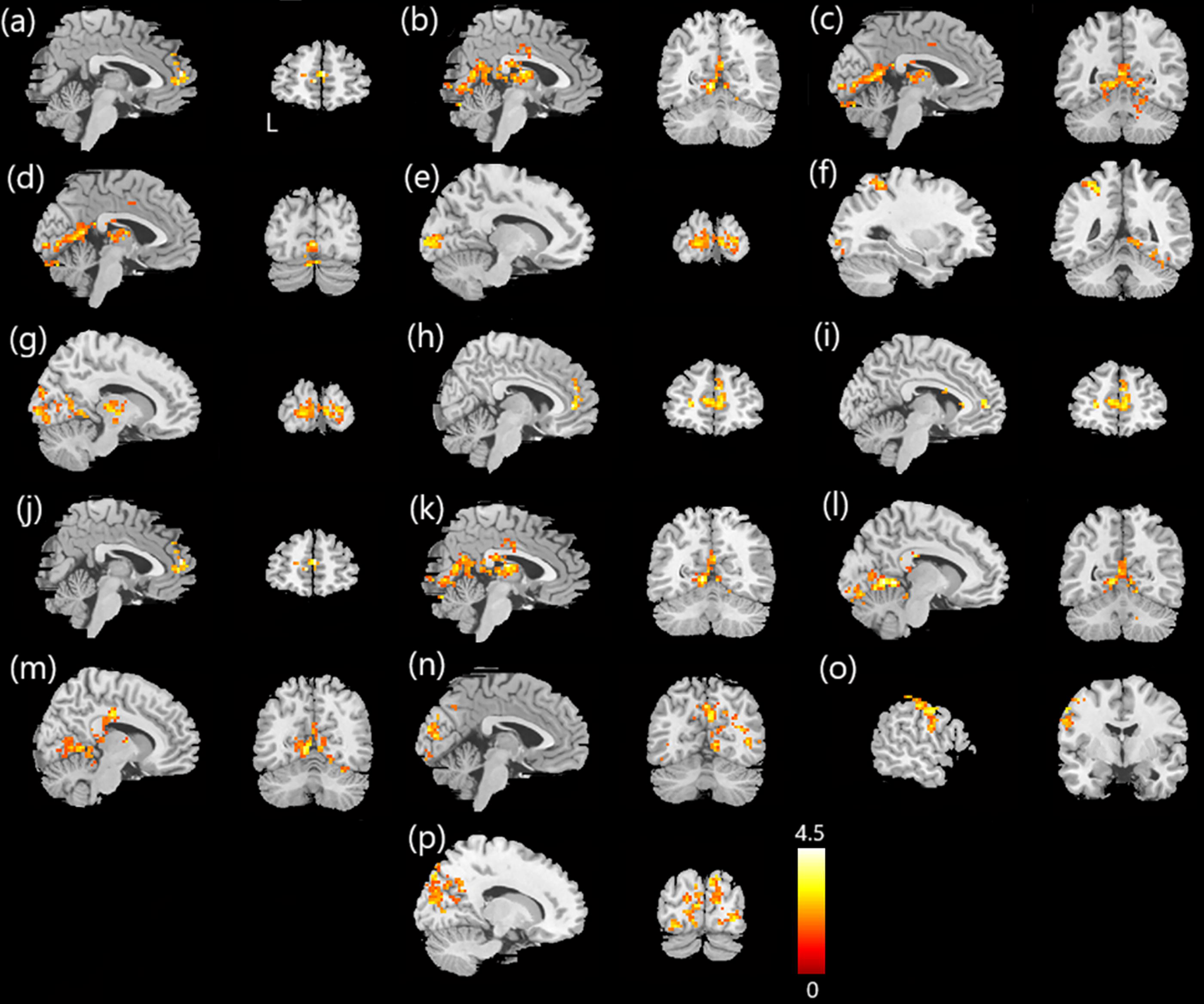
Negative correlations between changes in mfALFF/mReHo and clinical assessment scores in patients with breast cancer, based on multiple regression analysis. In the breast cancer group, negative correlations were observed between changes in mfALFF and clinical assessment scores:
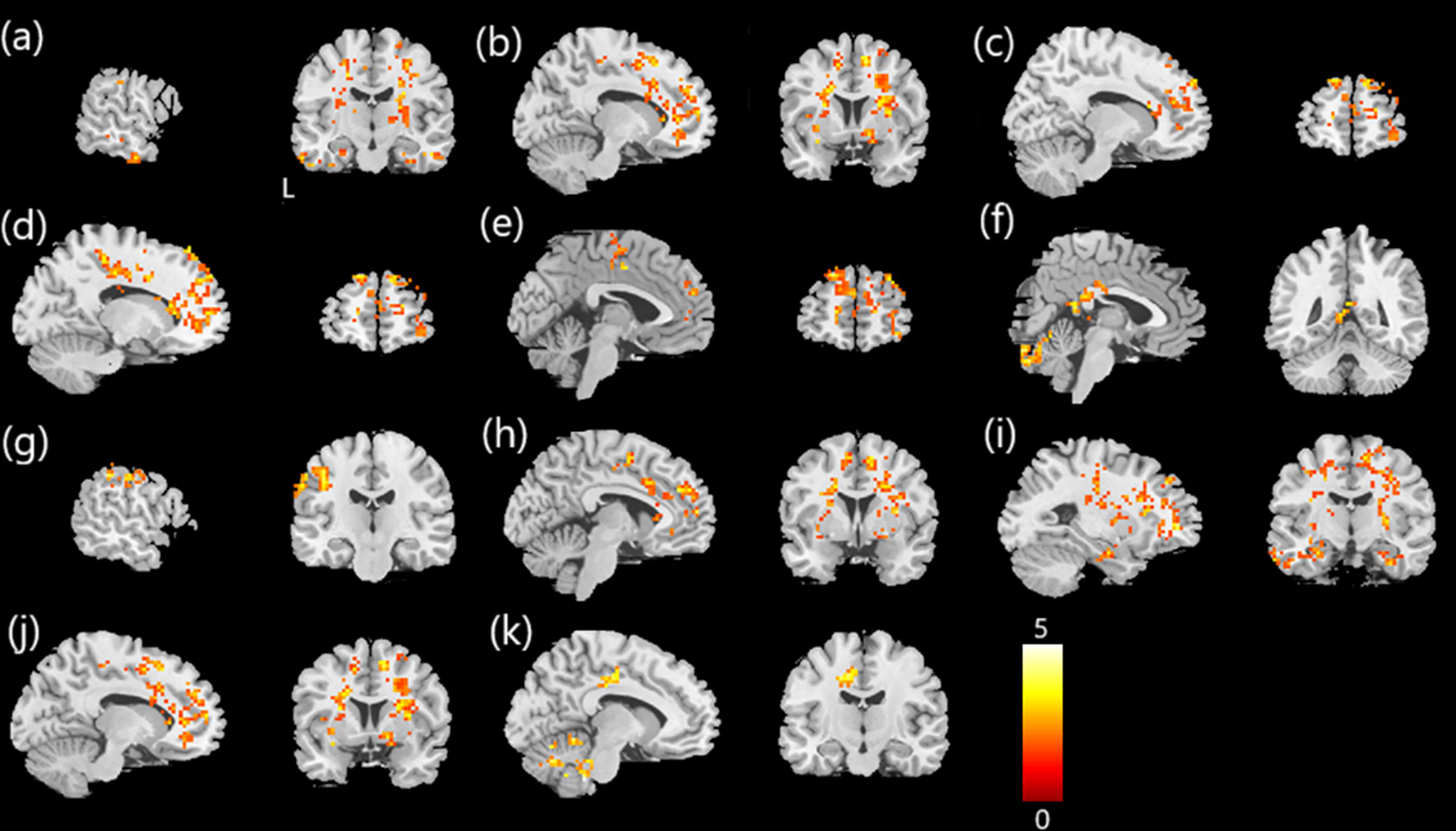
Positive correlations between changes in mfALFF/mReHo and clinical assessment scores in patients with breast cancer, based on multiple regression analysis. In the breast cancer group, positive correlations were observed between changes in mfALFF and clinical assessment scores:
Discussion
This longitudinal investigation examined changes in brain functional connectivity and cognitive functioning in patients with breast cancer undergoing chemotherapy, relative to healthy controls. Using a multimodal fMRI approach—encompassing mfALFF, mReHo, GTA, and NBS—we identified significant postchemotherapy changes in both local and large-scale brain network properties. These neural changes coincided with decreased anxiety symptoms and a measurable decline in self-reported cognitive function.
Our findings align with prior functional neuroimaging studies demonstrating disrupted network topology in breast cancer survivors, including those not exposed to chemotherapy, suggesting that connectivity changes may arise from both treatment and underlying disease (Chen et al., 2020). Voxel-wise analysis revealed both increases and decreases in mfALFF and mReHo values after chemotherapy, primarily in temporal, frontal, and postcentral areas, consistent with earlier reports of frontal and sensorimotor dysfunction (Deprez et al., 2011; McDonald et al., 2010). Importantly, mfALFF and mReHo reflect distinct neural properties: mfALFF indexes the strength of spontaneous low-frequency oscillations, whereas mReHo captures the local synchrony of neighboring voxels. Thus, increases in mfALFF may reflect heightened intrinsic activity, while decreases in mReHo suggest disruptions in local temporal coherence.
However, such interpretations remain speculative without direct mechanistic evidence or stronger behavioral correlations. Increases in activity could also represent maladaptive hyperactivation that signals greater cognitive effort rather than improved efficiency, while decreases in posterior regions may reflect either deterioration or adaptive downregulation. Thus, both maladaptive and adaptive processes likely coexist following chemotherapy, a duality that has been noted in prior CRCI studies (Deprez et al., 2012; Kesler et al., 2011; Pomykala et al., 2013).
Building on our lab’s earlier findings of chemotherapy-induced microstructural deterioration and disrupted white matter connectivity detected via diffusion MRI and Generalized Q-Sampling Imaging (GQI) (Chen et al., 2024a; Chen et al., 2024b), the current study extends this body of work by demonstrating parallel changes in functional brain activity and connectivity. These results highlight the involvement of structural and functional network disruptions in the cognitive decline observed among breast cancer survivors. Conversely, decreased activity in parietal and occipital regions may reflect functional deterioration or diminished neural efficiency (Deprez et al., 2011; Miao et al., 2016).
Group-by-time interaction effects were confirmed through repeated-measures ANCOVA for both mfALFF and mReHo, indicating that longitudinal changes in connectivity varied across breast cancer and control groups. Alterations in neural activity were localized to regions such as the precentral, postcentral, and inferior frontal gyri, which are associated with motor, attentional, and executive processing functions (Hu et al., 2023). Importantly, voxel-wise regression analyses demonstrated that longitudinal changes in mfALFF and mReHo were significantly associated with both cognitive and affective outcomes. Specifically, declines in FACT-Cog and DSS scores correlated with reduced activity in the posterior cingulate, lingual, and parietal regions, whereas increases in PHQ-9 scores were associated with dysfunction in the medial frontal and anterior cingulate cortices. In contrast, positive correlations in the medial frontal, fusiform, and cingulate areas suggested potential compensatory recruitment of alternative networks. These findings extend previous CRCI studies that primarily reported group-level imaging alterations (Deprez et al., 2014; Kesler et al., 2011; Pomykala et al., 2013) by directly linking longitudinal functional changes to cognitive performance and mood outcomes, thereby strengthening the clinical relevance of our results.
At the network level, GTA revealed reduced modularity, characteristic path length, and normalized shortest path length, alongside increased global efficiency. These findings suggest a shift toward a more randomized and less specialized architecture, a pattern associated with impaired cognitive specialization and integration (Bullmore and Sporns, 2012; Rubinov and Sporns, 2010). Such a topological shift reinforces the hypothesis that chemotherapy affects both the brain’s structural and functional architecture, impairing its capacity for efficient information processing (Kesler et al., 2015).
NBS further demonstrated diminished structural connectivity in both pre- and postchemotherapy groups. The prechemotherapy group exhibited weaker connectivity in the supplementary motor area, precentral and inferior frontal regions, and occipital cortex in contrast to healthy individuals. Postchemotherapy, additional disconnections were noted in the insula, parietal regions, and Rolandic operculum. These widespread alterations are consistent with prior findings of disrupted interregional coordination in patients with CRCI (Chen et al., 2024a; Kesler et al., 2015), supporting the notion that mechanisms attributable to the underlying disease as well as its treatment contribute to network degradation.
Our results support a physiological model in which chemotherapy alters intrinsic brain activity and connectivity at multiple levels. Collectively, the observed alterations in regional activity and global network topology converge to suggest a shift toward less efficient and more randomized organization. This framework links neural alterations to the clinical manifestations of CRCI, including slowed processing speed, attentional deficits, and subjective cognitive decline.
From a cognitive perspective, patients with breast cancer demonstrated significantly reduced FACT-Cog scores after chemotherapy, indicating perceived declines in cognitive function. Interestingly, anxiety symptoms significantly decreased over time, possibly reflecting post-treatment relief or psychological adaptation. However, no significant changes were observed in PHQ-9 or DSS scores. This dissociation supports the view that CRCI represents a distinct domain of cognitive dysfunction that cannot be fully explained by mood disturbances or general psychological distress (Ahles et al., 2012; McDonald and Saykin, 2013).
Several limitations should be considered. First, the modest sample size may limit generalizability. Second, the absence of a disease control group of non-chemotherapy patients with breast cancer restricts causal attribution, though our longitudinal design with healthy controls partly addresses this; future studies should include non-chemotherapy cohorts. Third, expectancy effects may have influenced both brain activity and self-reported cognition; while placebo-controlled chemotherapy is not feasible, future work could assess expectations or use blinded testing. Additional confounders—such as chemotherapy regimens, dosages, staging, and menopausal status—were not controlled and may have impacted results. Healthy controls were also younger than patients; although age was included as a covariate, residual confounding cannot be excluded. Neuropsychological testing was limited, with DSS used as the sole objective measure; memory domains, commonly affected in CRCI, were not assessed. Finally, while we demonstrated brain–behavior associations, further research is needed to identify which cognitive domains are most vulnerable and to validate these findings over longer follow-up periods.
Conclusions
This longitudinal study identified significant chemotherapy-related alterations in neural activity, functional connectivity, and cognitive performance among individuals with breast cancer. These neural alterations may underlie the cognitive difficulties frequently reported after treatment and suggest that interventions targeting network efficiency could help mitigate cognitive decline among the participants studied.
Authors’ Contributions
K.K.: Writing—original draft, writing—review and editing, and visualization. V.C.-H.C.: Conceptualization, data curation, resources, and writing—review and editing. Y.-H.T.: Data curation and resources. G.L.: Writing—review and editing. J.-C.W.: Supervision, conceptualization, methodology, software, project administration, funding acquisition, and writing—review and editing.
Footnotes
Acknowledgments
The authors gratefully acknowledge all contributors to this study. The authors extend special thanks to the clinical and research staff at Chang Gung Memorial Hospital, Chiayi, Taiwan, for their assistance with participant recruitment and MRI data collection. The authors also thank American Journal Experts for providing language editing and proofreading support.
Author Disclosure Statement
The authors declare that there are no conflicts of interest.
Funding Information
This research was funded by grants MOST107-2221-E-182-054-MY3 and NSTC112-2221-E-182-013-MY3 from the National Science and Technology Council, Taipei, Taiwan. Additional support was provided by grants CORPG6G0101∼3 and CORPG6G0121∼3 from Chang Gung Memorial Hospital, Chiayi, Taiwan. The funding sources had no role in the study design, data acquisition, analysis, interpretation, or the writing of the article.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.