
Abstract
Drawing on two waves of the Chinese Longitudinal Healthy Longevity Survey, this study advances a Threshold–Care Climate–Place lens on late-life depression by asking whether any shortfall in assistance with daily activities relates to depressive symptoms, and how that link depends on the relational tone of family care and the contexts in which older adults live. To balance breadth with depth, depression is measured both as a cross-wave harmonized indicator and, within a single wave, as a continuous severity scale that preserves symptom gradation. Unmet support is defined in complementary ways as strict unmet, meaning help is not provided at all, and any unmet, meaning there is any shortfall; care climate is recoded as supportive or negative to capture the affective tenor of everyday care. A portfolio of estimators combines pooled models with year effects and clustered errors, doubly robust average-effect estimation, a four-cell configuration of unmet by care climate, and region-stratified and multilevel checks. Three patterns emerge: evidence is threshold-sensitive, with any shortfall linked to higher depressive risk when information is preserved or imbalance reduced; care climate amplifies the link, with strict unmet under a negative tone riskiest and supportive care attenuating risk; and place shapes baselines rather than slopes, with urban settings elevating background risk and eastern regions lowering it. The findings suggest that measurement and selection can mask meaningful associations and support practice that treats any shortfall as a screening trigger, pairs assistance with attitude-focused micro-interventions, and reads outcomes against local baselines.
Plain Language Summary
Help with everyday tasks—bathing, dressing, using the toilet, moving around at home, managing continence, eating—forms the basic “infrastructure” of daily life in older age. This study asks two simple questions: Does any shortfall in this help relate to depressive symptoms? And does that link depend on the mood and tone of family care and on where people live? We analyze two waves of a large national survey of older adults in China (2014 and 2018). To keep coverage broad yet retain detail, we looked at depression in two ways: a simple yes/no indicator across both years and, in 2018, a continuous score that preserves symptom intensity. We defined unmet help in two practical forms: strict unmet (help not provided at all) and any unmet (any shortfall). We also recoded the care climate as supportive or negative to reflect the feel of everyday family care, and we compared urban, town, and rural settings across regions. Three clear patterns emerged. First, a threshold: once any shortfall appears, the risk of depressive symptoms rises—especially when symptom detail is preserved or fair comparisons are made. Second, care climate matters: strict shortfalls combined with a negative tone of care show the highest risk, while a supportive tone softens it. Third, place sets the baseline: depression tends to be higher in urban settings and lower in parts of the east, with unmet help adding a relatively modest but consistent extra risk on top. The takeaway is practical. Treat any shortfall as a sensible trigger for brief screening and referral. Pair assistance with attitude-focused micro-interventions—better communication, predictable schedules, respite options—so limited help feels sufficient. Read outcomes against local baselines, and wherever possible use continuous symptom scales to avoid missing important changes.
Introduction
Late-life depression undermines healthy aging, compromises recovery from physical illness, and strains family systems that already carry substantial care burdens (Alfaro et al., 2022; Chen et al., 2025; Y. Li et al., 2025). Among the most plausible, proximate drivers is the experience of shortfalls in help with everyday activities—bathing, dressing, toileting, moving around indoors, continence, and eating (Wassink-Vossen et al., 2022). These are not peripheral conveniences but the substrate of daily life: when help falters, older adults absorb the shortfall as practical difficulty, social embarrassment, and emotional wear (Weziak-Bialowolska & Bialowolski, 2024).
Yet the empirical record remains uneven. Some studies report robust links between unmet assistance and depressive symptoms (Khattar et al., 2022; Yu et al., 2022); others find small or unstable effects (Kim et al., 2025; Muhammad, 2023). Much of this variability traces to two blind spots: how we measure both depression and unmet care, and how we situate unmet care inside the relational and structural contexts that make it matter.
The first blind spot is measurement compression. When symptoms are dichotomized into present/absent, a great deal of gradation is lost, and subtle but meaningful differences become difficult to detect (Courtney et al., 2021)—especially among the older adults, where symptom expression, reporting styles, and proxy responses are heterogeneous (Cao et al., 2023). Cross-wave analyses that harmonize different instruments exacerbate this compression: harmonization serves coverage, but the price is a muted signal (Mu et al., 2021). Without acknowledging this, one may interpret a small pooled effect as substantive null, when in fact it reflects a measurement decision that squeezes variance out of the outcome.
The second blind spot is relational and structural embedding. A common impulse is to treat unmet care as a dose that linearly transmits its influence to depressive symptoms, sometimes via a single mediator (Gao et al., 2023). But the care climate—the everyday emotional tone of family care—is not merely a conduit. A negative climate (impatience, reluctance, emotional withdrawal) can amplify the psychological salience of shortfalls; a supportive climate can blunt them (Iwuagwu et al., 2022; Woo et al., 2023). Likewise, place shapes the baseline against which shortfalls are experienced. Urban settings often entail higher background strain and tighter social comparison, while regional care ecologies and service infrastructures differ in systematic ways (Yan et al., 2021; Yuan et al., 2024). Ignoring these layers risks attributing to “dose” what is in fact an interaction between shortfall, climate, and context.
Guided by these observations, we advance a Threshold–Care Climate–Place (TCP) perspective. The threshold element asks a deliberately practical question: does any shortfall in basic assistance correspond to higher depressive risk, such that screening and referral are warranted as soon as a gap appears? The care-climate element reframes attitude from a linear mediator to a contextual amplifier, highlighting how the affective texture of care conditions the meaning and impact of unmet support. The place element treats urbanicity and macro-regional setting as structural baselines: they calibrate background risk and thus the psychological “distance” from baseline that an unmet shortfall represents. Together these layers convert a simple dose-response intuition into a small set of mechanism-consistent propositions.
The empirical challenge is to evaluate these propositions while making measurement choices visible. We therefore pair a pooled, harmonized binary indicator of depression—useful for cross-wave breadth—with a within-wave continuous symptom scale that preserves gradation. We represent unmet care in complementary forms: strict unmet, meaning help is not provided at all, and any unmet, meaning there is any shortfall relative to fully met assistance. We recode caregiver attitude into supportive versus negative to capture climate in a way that is simple enough for configuration analysis but faithful to lived care. Finally, we read effects against urban and regional contexts and quantify residual clustering to check whether unobserved provincial forces matter after observed structure is included.
This design yields three testable expectations, framed in associational terms. First (threshold), when symptom information is preserved or covariate imbalance is reduced, any shortfall is expected to align with higher depressive risk—even if pooled binary estimates appear small. Second (care climate), the strict unmet × negative climate configuration should display the highest risk, whereas supportive climates should attenuate the link between unmet care and depression. Third (place), differences should appear primarily as baseline shifts—urban higher, certain regions lower—rather than dramatic changes in the slope of unmet care. These expectations do not presuppose a single causal pathway; rather, they specify patterns that would be observed if threshold, amplification, and baselines are the mechanisms at work.
The conceptual contribution is to replace a fragile mediation narrative with a compact framework that foregrounds threshold sensitivity, relational amplification, and structural baselines. The methodological contribution is to show how pairing cross-wave breadth with within-wave depth, and combining pooled regressions with doubly robust estimators and configuration analysis, makes visible the phenomenon we call measurement–selection masking—the tendency for dichotomization and cross-wave compositing to suppress signals that re-emerge when symptom gradation is retained or balance is improved. The practical contribution is to articulate a screening logic that is easy to implement: treat any shortfall as a trigger, pair technical assistance with attitude-focused micro-interventions in families showing a negative climate, and interpret outcomes against local baselines rather than one-size-fits-all slopes.
China provides an analytically valuable setting for this inquiry. Family remains the primary site of everyday care, the older cohort is large and growing, and urban–rural and regional differences in services and expectations are pronounced (Gong et al., 2022; Lei et al., 2022; H. Li et al., 2022). Using two waves of a large, geographically diverse survey allows us to stage the TCP perspective empirically: test the threshold with average-effect estimators that align with practice, visualize care-climate as a four-cell configuration, and locate effects within place-based baselines. In doing so, the study speaks to broader debates in aging, caregiving, and measurement: when do shortfalls matter, how do families make them matter, and where do contexts make them more or less bearable?
The remainder of the article proceeds as follows. We first detail the data, measures, and identification strategy, emphasizing how the dual outcome design and complementary estimators answer the measurement challenge. We then present results organized by the TCP framework—threshold, care climate, and place—followed by robustness checks that triangulate across estimators and specifications. We close by discussing implications for screening and family-focused intervention, and by outlining a measurement agenda that reads late-life mental health against the texture of care and the terrain of place.
Literature Review
From Dose to Threshold: Reconceptualizing Unmet ADL Support and Late-Life Depression
A large body of gerontological and mental-health research links difficulties in everyday activities—bathing, dressing, toileting, moving indoors, continence, eating—to elevated depressive symptoms in later life (Chen et al., 2025; Wassink-Vossen et al., 2022; Zhao et al., 2022). Classical disablement accounts describe a chain from functional limitation to activity restriction and social participation loss (Griffith et al., 2017), while stress-process perspectives emphasize role strain, loss appraisal, and erosion of coping resources (Hobfoll, 2001). In both lines of work, shortfalls in practical support act as proximate stressors that threaten autonomy and dignity, heighten shame or embarrassment, and dampen engagement with everyday social worlds. The consistent theme is that failures in the “infrastructure of daily life” reverberate psychologically (Dourish & Bell, 2007).
Yet the field has not settled whether unmet support operates as a linear dose or as a threshold. Resource-based theories and socioemotional accounts suggest a different logic: for needs that safeguard bodily integrity and social personhood, any shortfall can be consequential (Hobfoll, 2001; Hobfoll et al., 2016). Below a minimal sufficiency line, older adults experience threat to control and self-presentation; above it, additional increments may matter less than the presence or absence of a gap.
A threshold perspective also aligns with practice. Screening, referral, and early intervention rarely hinge on fine-grained gradations of shortfall; they are organized around simple decision points—does a gap exist that warrants action? Conceptual clarity here has policy value. If the association between unmet support and depression is threshold-sensitive, programs that identify and respond to any shortfall, even small ones, are more likely to mitigate downstream psychological harm than those that reserve action for only the most severe cases (Yu et al., 2023).
A further complication comes from the temporal texture of aging. As horizons shorten and goals become present-oriented, immediate threats to comfort and independence carry more emotional weight than marginal gains in abstract domains (Cohen & Sherman, 2014). This implies nonlinearity near a sufficiency boundary and helps explain why associations sometimes surface in designs that retain symptom gradation but fade when symptoms are compressed into “present versus absent.”
Hypothesis 1 (Threshold)
Net of demographic and socioeconomic conditions, the presence of any shortfall in basic assistance is associated with higher depressive symptoms; severe shortfall (help not provided at all) is also expected to relate positively to depressive symptoms, with detectability contingent on how outcomes and exposures preserve gradation and contrast.
Beyond Mediation: Care Climate as an Amplifier of Unmet Support
Research on family caregiving has long documented the emotional labor of providing intimate assistance and the strain that accrues when demands outpace resources (Dean et al., 2022; Franzosa et al., 2019). Studies of expressed emotion, interaction rituals, and care ethics converge on the idea that the affective climate of routine care—patience or impatience, generosity or reluctance—conditions how recipients interpret and absorb shortfalls (Crespo et al., 2013; Olsson & Ingvad, 2001).
An amplifier view better fits this relational terrain. A negative climate communicates scarcity of time, patience, or regard, transforming a practical gap into a symbolic slight; a supportive climate reframes the same gap as a shared challenge and buffers its impact (Cristoforetti et al., 2011; Neves et al., 2019). Under normatively dense expectations of family responsibility, breaches are not merely instrumental failures; they can be read as erosions of respect or belonging (Qi, 2025). In such settings, the same objective shortfall acquires different psychological meanings depending on the emotional tone in which help is offered.
Amplification also explains why small material differences sometimes yield large psychological consequences. The meanings attached to care—who asks, who gives, how they give—are themselves resources. Where care is perceived as grudging, older adults may withdraw, suppress requests, or internalize stigma; where it is experienced as warm and collaborative, partial help may suffice to sustain mood and engagement even when tasks are not fully covered (Graff & Vabø, 2023; Liu & Gallois, 2022).
This logic suggests a configuration approach rather than an insistence on linear interaction terms. If care climate amplifies the salience of unmet support, the ordering of risk across four simple cells—no/partial versus strict unmet, crossed with supportive versus negative climate—should be informative even when formal moderation tests are underpowered. A relational lens thus complements dose-or threshold-based accounts by specifying when and for whom shortfalls become psychologically intolerable.
Hypothesis 2 (Care-Climate Amplification)
The association between unmet basic assistance and depressive symptoms is amplified under a negative care climate and attenuated under a supportive climate; descriptively, the configuration combining severe shortfall with a negative climate exhibits the highest depressive risk, whereas the configuration combining no/partial shortfall with a supportive climate exhibits the lowest.
Place and the Baselines of Risk: Urbanicity, Region, and Measurement
Older adults live in ecologies where services, norms, and stressors vary systematically. Urban environments often entail faster pace, tighter social comparison, and denser bureaucratic demands—features that can elevate background strain; at the same time, they offer richer service infrastructure (Muhammad, 2023; Yuan et al., 2024). Regions differ in welfare arrangements, community capacity, and expectations about family versus formal provision (Iwuagwu et al., 2022; Yan et al., 2021). These features suggest that place primarily shapes the baseline against which shortfalls are experienced rather than dramatically altering the slope linking unmet support to depressive symptoms.
A place-structured view aligns with evidence that neighborhood disadvantage, crowding, and social comparison heighten mood vulnerability even before specific shocks occur (Affleck & Tennen, 2024; Zhang, 2024). In such contexts, a given shortfall may push individuals across a subjective threshold more readily than in places where daily life is less demanding and services are easier to mobilize. Conversely, regions with stronger routine supports may render the same shortfall less psychologically costly. Recognizing baseline differences is therefore critical: interventions that focus only on “fixing the slope” risk underperforming when the background level of strain is high. Place also interacts with measurement in ways that matter for inference. Among the older adults, symptom reporting can be conservative for reasons of stigma (Adams et al., 2024).
Taken together, these strands imply that reading unmet assistance against urbanicity and regional setting is not merely descriptive; it is necessary for valid inference and actionable policy. If most heterogeneity resides in levels rather than slopes, targeting and interpretation should follow suit: screening thresholds can be uniform—treat any shortfall as a signal—but expectations about risk and needed supports should be calibrated to local baselines.
Hypothesis 3 (Place-Structured Baselines)
Urban residence is associated with higher baseline depressive risk and certain regional settings with lower baselines, while the slope linking unmet assistance to depressive symptoms remains comparatively modest across places; associations that are muted under pooled dichotomies become more discernible when symptom gradation is retained or comparisons are rebalanced.
Method
Data and Sampling Frame
This study uses two waves (2014 and 2018) of the Chinese Longitudinal Healthy Longevity Survey (CLHLS), a long-running survey of older adults in Mainland China that employs multistage, stratified probability sampling with broad provincial coverage. Interviews are conducted in respondents’ homes using standardized protocols, with field re-visits and consistency checks to safeguard quality. The design offers both spatial heterogeneity (rural/town/urban; West/Central/East) and repeated observation across time, which is essential for distinguishing cross-wave breadth from within-wave depth in measurement.
For analysis, we construct an unbalanced two-wave panel keyed by a stable person identifier, restricting to respondents aged 65+ at interview. This yields a person–year file in which individuals contribute one or two rows depending on data availability. To retain information while minimizing unnecessary case loss, we implement model-specific listwise deletion: each model uses the largest variable-complete subsample required for that specification.
The pooled, harmonized binary models include 1,853 person-wave observations (from 1,740 unique individuals). The 2018-only continuous depression models include 519 observations with complete CESD-10. The care-climate configuration models include 1,764 observations (1,658 unique individuals). Region-stratified models include 429 (West), 454 (Central), and 970 (East) observations, respectively.
Analytic Cohort and Inclusion Rules
All analytic samples are limited to respondents aged 65 years or older. We do not impose a global missing-data rule; instead, each model removes only those cases with missing values on variables required by that model. This ensures that, for example, continuous-outcome analyses in 2018 are not constrained by variables absent in 2014, and configuration analyses are not constrained by cases without care-attitude information in a given wave.
No survey weights are applied. The estimands are associations (and for IPWRA, average treatment effects under stated assumptions), not population prevalence. In sensitivity checks where proxy responses can be identified, we either include a proxy indicator or restrict to self-responses; results remain directionally unchanged and are therefore reported as robustness rather than in primary tables.
Measures
Depressive Symptoms
We operationalize depression in two complementary ways to balance cross-wave coverage and within-wave precision.
First, harmonized binary outcome (2014 and 2018). We code the presence of clinically relevant depressive symptoms as Yes/No in both waves. In 2014, this reflects a brief two-symptom screen; in 2018, it reflects whether the ten-item CESD crosses a clinical threshold. Pooled models include year fixed effects to absorb level differences across instruments. The variable-specific denominator for the harmonized indicator is 8,709, with 39.96% coded “Yes.”
Second, continuous outcome (2018 only). To preserve symptom severity, we construct a CESD-10 z-score as follows: (a) items phrased in a positive valence (e.g., hopeful, happy, good sleep) are reverse-scored so that higher values consistently indicate worse symptoms; (b) when at least 7 of 10 items are answered, we prorate scores by multiplying the row-mean by 10; (c) the resulting total is standardized to a z-score (mean 0, SD 1). The analytic denominator for the 2018 continuous outcome is 519.
Retaining symptom gradation addresses a well-known issue in late-life mental health measurement: dichotomization compresses variation and can mask meaningful but modest associations, particularly in the oldest-old where expression and reporting of symptoms are heterogeneous. Pairing a pooled binary outcome with a 2018 continuous outcome allows us detect and explain such attenuation.
Unmet Assistance for Activities of Daily Living (ADL)
We assess the adequacy of basic daily assistance in six domains (e.g., bathing, dressing, toileting, moving about indoors, continence, eating) using three reader-friendly forms that map onto distinct theoretical logics.
First, ordinal unmet ADL (three levels). We code fully met, partly met, and not met at all such that higher = more unmet. This captures a dose intuition—greater shortfall implies greater strain. Second, strict unmet. We code a binary indicator for “not met at all” on core daily assistance (vs. no/partial unmet). This isolates a severe failure of care that is likely to be clinically salient. Third, any unmet. We code a binary indicator for “any shortfall” relative to fully met on all tasks. This implements a threshold logic supportive of practice: any shortfall could be sufficient to trigger screening and referral. In our data, among those with valid ADL support information (N = 2,824), 48.16% are strict unmet and 96.88% are any unmet.
The ordinal form aligns with need–supply mismatch and stress-process theories; the any-unmet form aligns with screening thresholds in clinical and community practice; the strict-unmet form identifies catastrophic gaps in basic care.
Caregiver Attitude (Care Climate)
We capture the emotional tone of the primary family caregiver using a four-category response (unwilling; willing but constrained; impatient; willing and provides good care). For analysis, we retain the four-level description for documentation and create a binary recode: negative care climate (unwilling or impatient) versus supportive care climate (willing but constrained, or willing and effective). The variable-specific denominator for the recoded measure is 2,848, with 97.54% observed as negative and 2.46% supportive in the subsample that reports caregiver attitude.
Care climate is conceptualized as a contextual amplifier rather than a conduit: drawing on caregiving stress, appraisal, and affective climate perspectives, the same objective shortfall can register more strongly on mental health when the relational tone of care is impatient, reluctant, or emotionally withdrawn.
Covariates
We adjust for gender (male/female), age (years), current marital status (married/partnered vs. not), education (none; up to 9 years; more than 9 ears), subjective economic status (five-point ladder from “very difficult” to “affluent”; higher = better), household annual income (<50,000; 50,000–100,000; >100,000 RMB), macro-region (West, Central, East), residence (rural, town, urban), and survey year (2014/2018). These covariates situate unmet care and depression within socio-demographic, economic, and place-based contexts. Variance inflation factors are <2 in all pooled models, indicating no concerning collinearity.
Harmonization, Missingness, and Denominators
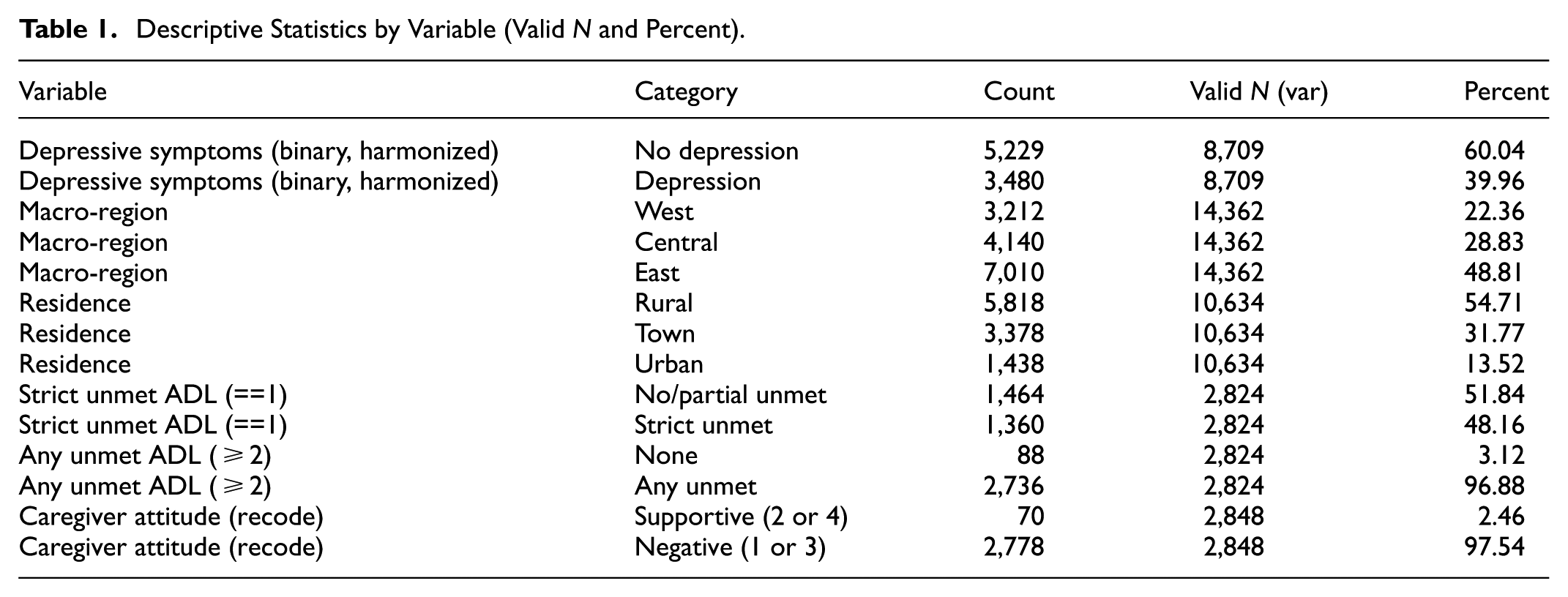
We explicitly separate cross-wave breadth (binary outcome) from within-wave depth (2018 continuous outcome). Positive-valence symptom items are reversed; prorating (≥7/10 items answered) balances inclusivity against noise. Rather than imposing one global rule for missingness, each model uses the largest variable-complete subsample; this keeps more information and makes the implied trade-offs transparent. Table 1 reports variable-specific denominators (e.g., depression binary 8,709; region 14,362; residence 10,634; ADL unmet 2,824; caregiver attitude 2,848), and each model lists its analytic N.
Descriptive Statistics by Variable (Valid N and Percent).
This design is not just technical; it supports the central inferential claim. If a relationship appears small or counter-intuitive under harmonized binary measurement but reappears under continuous measurement or doubly-robust weighting, we can attribute the difference to measurement compression and selection rather than to the absence of an underlying association—what we term measurement–selection masking.
Identification Strategy and Estimators
We target three mechanism-consistent patterns—threshold, care-climate amplification, and structural baselines—under observational data. We do not assert causal mediation. Instead, we combine estimators that privilege different identification logics and robustness properties:
First, pooled logit with year fixed effects (harmonized binary outcome). We regress the harmonized binary depression indicator on strict unmet (primary) and, in sensitivity, any unmet, adjusting for all covariates and survey year. Standard errors are cluster-robust at the individual level. We report odds ratios, 95% CIs, and predicted probabilities at representative values.
Second, 2018 continuous CESD-10 (symptom severity). We regress the z-standardized CESD-10 on strict unmet and covariates with robust standard errors. Coefficients (β) reflect standardized change in symptom severity. This specification directly tests whether retaining gradation restores the expected sign and magnitude.
Third, doubly-robust ATEs (IPWRA). We treat any unmet (primary) and strict unmet (sensitivity) as binary “treatments” and estimate average treatment effects using inverse-probability weighted regression adjustment (logit treatment model; linear probability outcome). Under conditional exchangeability (given modeled covariates), positivity (overlap), and stable unit treatment value, IPWRA remains consistent if either the treatment or outcome model is correctly specified.
Fourth, care-climate configuration (descriptive mechanism test). We compute predicted probabilities and 95% CIs for the four cells defined by unmet status (no/partial vs. strict) and care climate (supportive vs. negative). Because the interaction term is not statistically decisive and the attitude indicator is single-item, we present configuration as descriptive evidence of amplification.
Fifth, structural embedding and multilevel sensitivity. We estimate region-stratified pooled logits (West, Central, East) and compute predicted probabilities by residence and unmet status. We also fit a province-random-intercept logistic model with robust clustering at province to quantify the intraclass correlation (residual province variance) after accounting for observed structure.
Sixth, estimator ensemble for rare events and dependence. To address biases from low event rates and two-wave dependence, we replicate harmonized-binary models using population-averaged GEE (binomial logit, exchangeable correlation), rare-events logit, and Firth’s penalized logit. Concordance—or systematic divergence—with the continuous and IPWRA specifications informs our interpretation of masking.
Statistical Analysis and Reporting
All analyses were conducted in Stata 16. For pooled logit and GEE, we report odds ratios with 95% confidence intervals, and provide predicted probabilities to place effects on the response scale. For the 2018 continuous outcome, we report standardized coefficients (β). For IPWRA, we report ATEs with robust standard errors and 95% CIs. Tables include significance stars (*p < .05, **p < .01, ***p < .001). Figures use grayscale with unified typography and no in-figure titles; captions carry all titles and estimator details. The data processing workflow (harmonization, prorating, modeling, visualization) is scripted for reproducibility.
Ethical Approval and Informed Consent
This study uses publicly available, de-identified data from the Chinese Longitudinal Healthy Longevity Survey (CLHLS). The primary data collection of CLHLS was reviewed and approved by an accredited institutional ethics committee, and written informed consent was obtained from all participants or their legal representatives prior to each interview. The present analysis involved only secondary use of anonymized data; no direct contact with human participants occurred and no re-identification was attempted. In accordance with Section 8.05 of the APA Ethical Principles, no additional consent was required for this secondary analysis. Reporting follows the STROBE checklist for observational studies (see Supplemental File).
Results
Sample Profile
Table 1 summarizes the analytic landscape using variable-specific denominators, making missingness and coverage fully transparent. On the harmonized binary indicator of depressive symptoms (two-symptom screen in 2014; thresholded CESD-10 in 2018), prevalence is 39.96% (3,480/8,709). The macro-regional composition is East 48.81%, Central 28.83%, West 22.36%; residence is 54.71% rural, 31.77% town, and 13.52% urban. Within the subset reporting assistance for basic daily activities, strict unmet care—defined as “not met at all”—accounts for 48.16% of valid records, while any unmet care—any shortfall—covers 96.88%. Caregiver attitude is recoded for clarity into supportive (willing, even if constrained; able to provide good care) versus negative (unwilling or impatient).
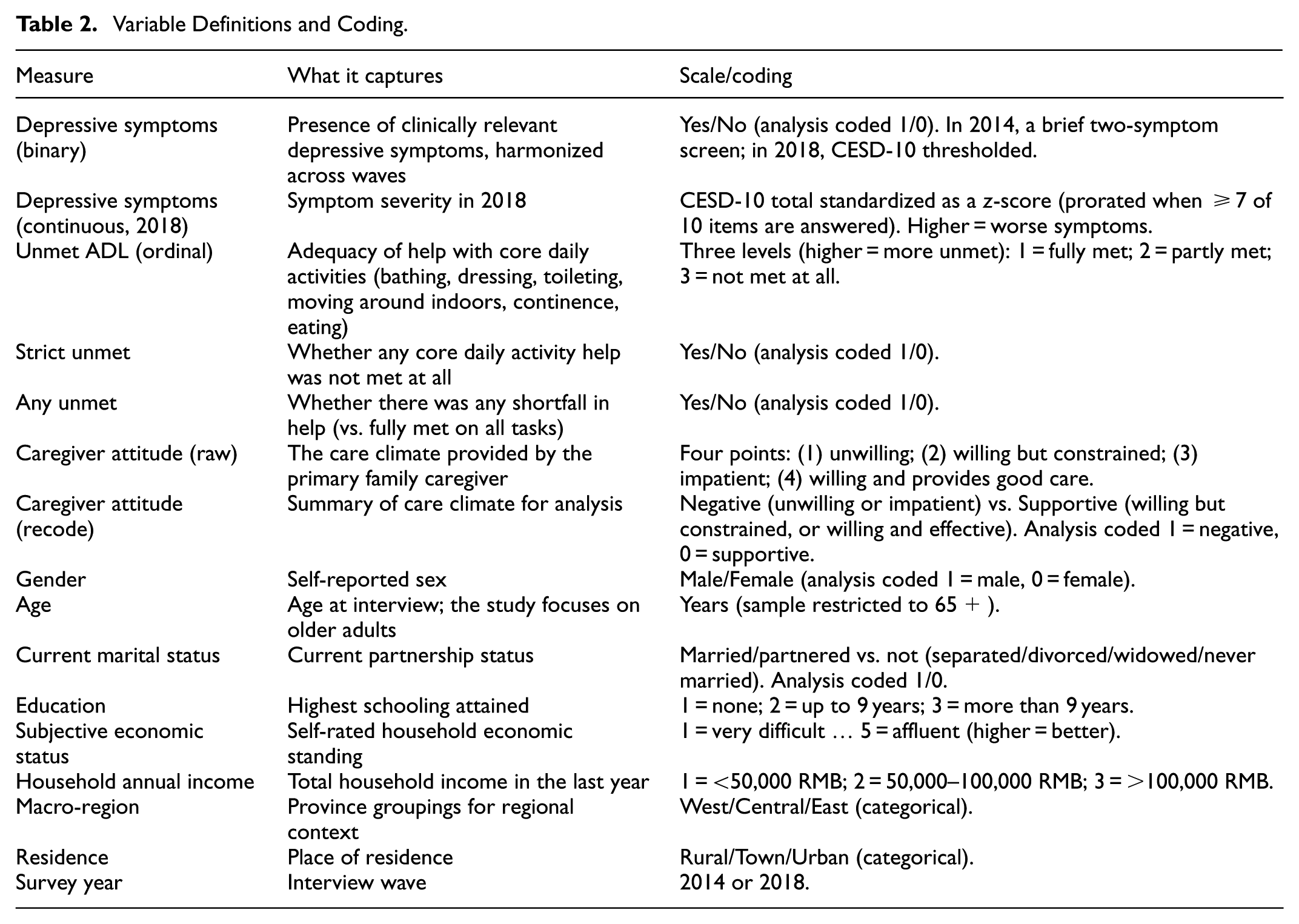
Table 2 provides a variable guide (no instrument codes), including the 2018-only continuous CESD-10 z-score that preserves symptom gradation after reverse-coding positive-valence items and prorating with ≥7 valid answers. This dual outcome strategy allows us to separate substantive association from aggregation effects that often mute signals in very old samples.
Variable Definitions and Coding.
Main Association: A Threshold Emerges When Information Is Preserved or Imbalance Is Reduced
Using the cross-wave binary outcome with individual-clustered standard errors and year fixed effects, the association between strict unmet care and depression is small and marginal (Table 3, OR = 0.798, p = .069).
Harmonized Binary Logit: Odds Ratios (OR) with p-value Stars.

Note. OR = odds ratio; CI = confidence interval.
p < .05; ***p < .001.
Figure 1 shows predicted probabilities of 0.395 for “no/partial unmet” and 0.359 for “strict unmet,” with overlapping confidence intervals—already hinting that dichotomization and cross-wave harmonization can dampen a true signal.
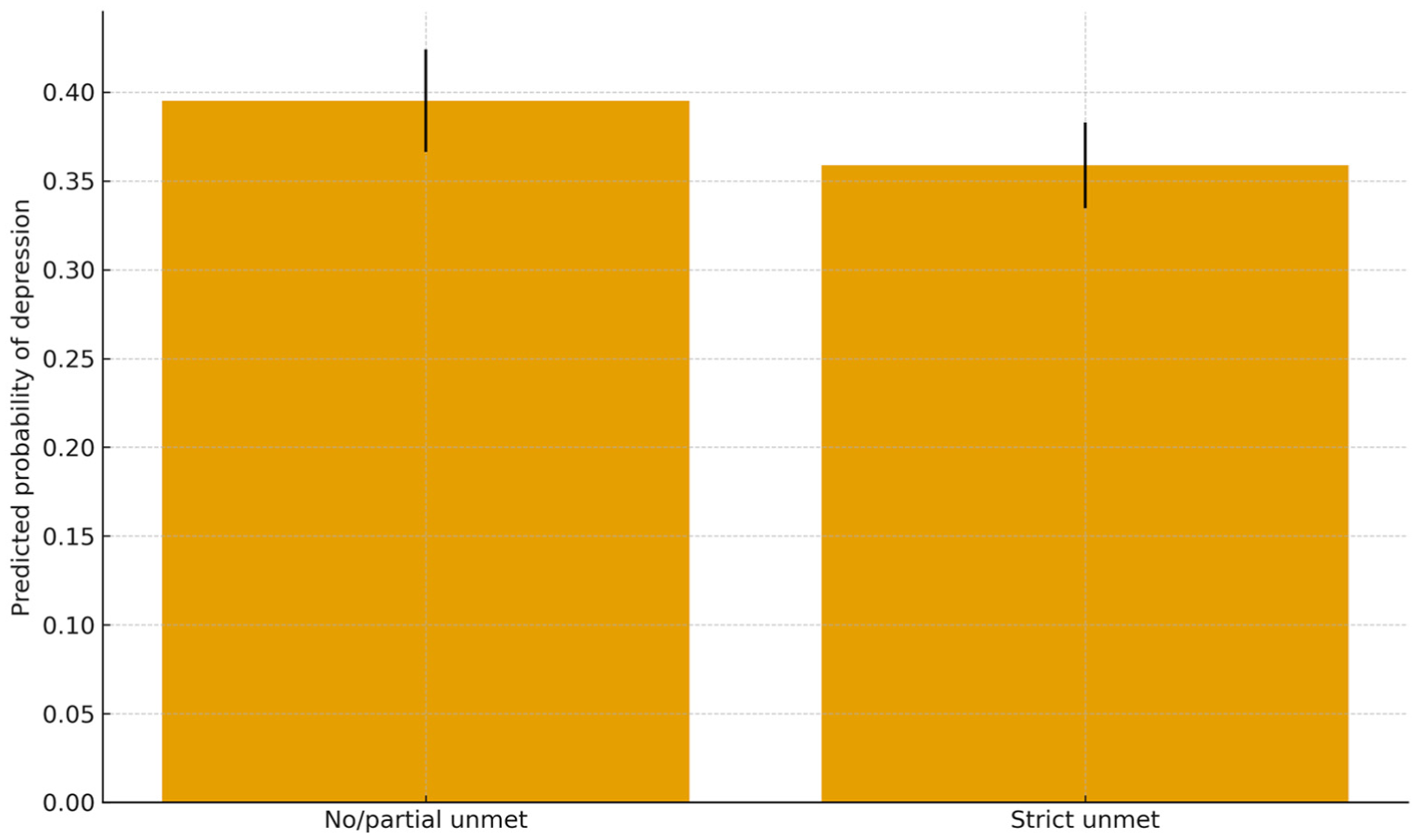
Predicted probability by strict unmet (harmonized binary).
When symptom information is retained, the association re-appears and aligns with theoretical expectation. In the 2018 continuous specification, strict unmet care is positively related to depressive severity (Figure 2, β = 0.296, SE = 0.089, p = .001).
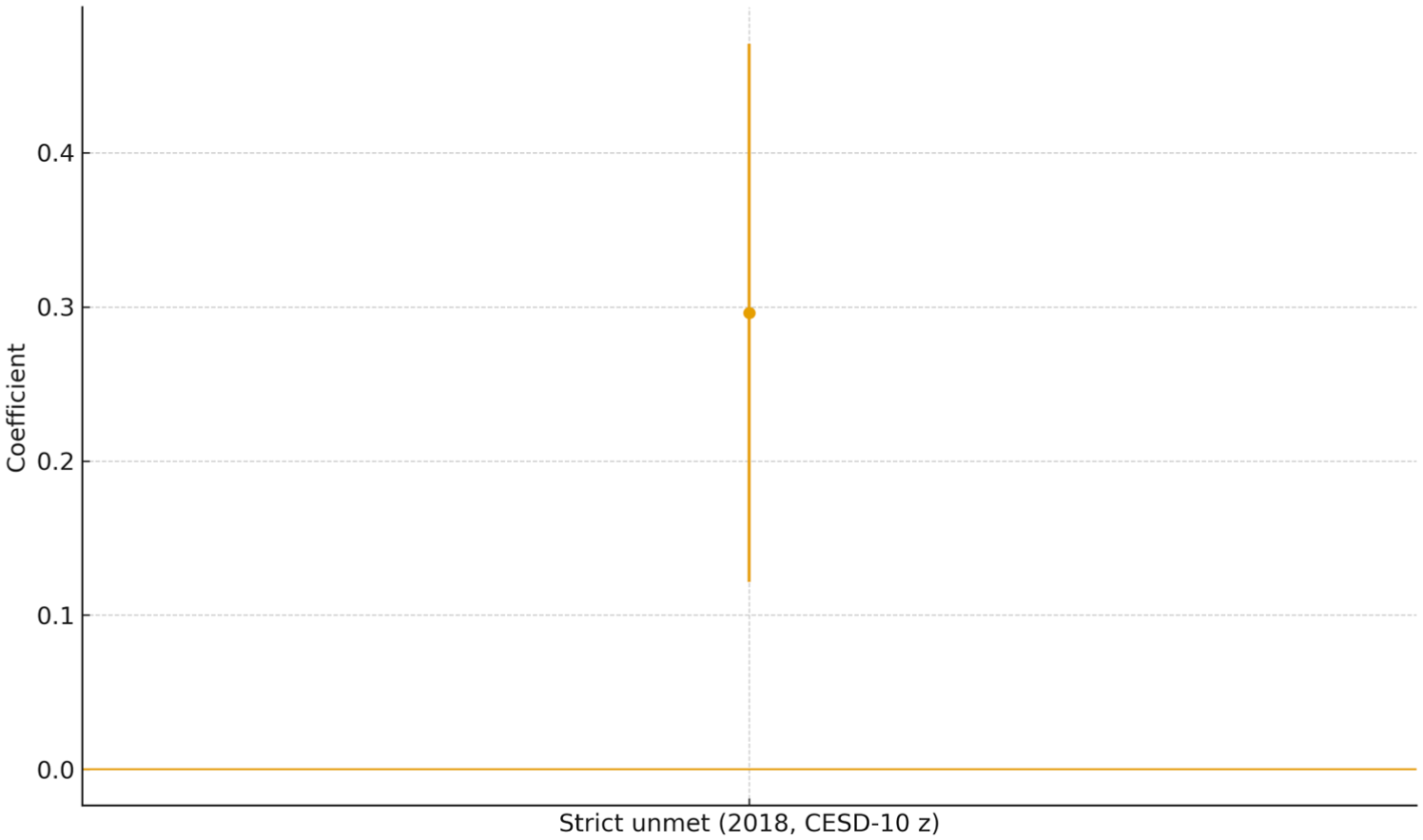
2018 CESD-10 z-score model: coefficient and 95% CI for strict unmet ADL.
A complementary doubly-robust IPWRA design that treats any unmet as the exposure yields a substantive ATE = 0.323 (SE = 0.066, p < .001), indicating a higher probability of depression among older adults reporting any shortfall after balancing on observed covariates (Figure 3; Table 4).
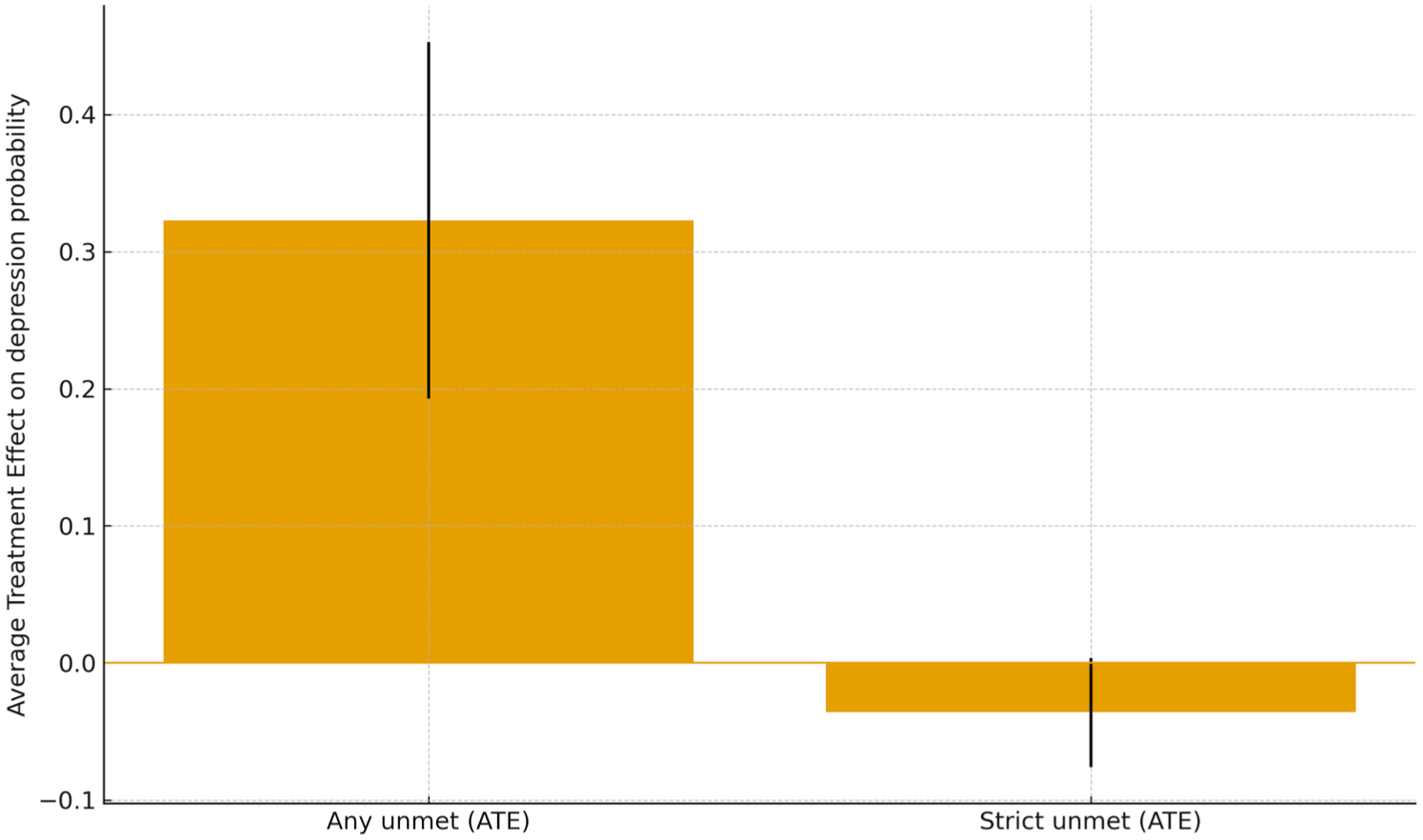
IPWRA ATEs (Any_Unmet; Strict_Unmet).
IPWRA ATEs (With SEs, 95% CIs, p-value Stars).

Note. ATE = average treatment effect; SE = standard error; CI = confidence interval.
p < .001.
The IPWRA estimate for strict unmet is smaller and marginal (ATE = −0.036, SE = 0.020, p = .076), which is plausible given the scarcity of “fully met” cases that constrains contrast.
Taken together, the ensemble implies a threshold-sensitive pattern: once any unmet appears, depressive symptoms tend to rise. Designs that preserve gradation (continuous CESD-10) or reduce imbalance (IPWRA) unmask this threshold, whereas cross-wave binary harmonization tends to attenuate it.
Configurational Evidence: Care Climate as an Amplifier Rather Than a Conduit
Average effects conceal how care climate colors the experience of unmet need. Figure 4 presents a 2 × 2 configuration by unmet status (no/partial vs. strict) and care climate (supportive vs. negative).
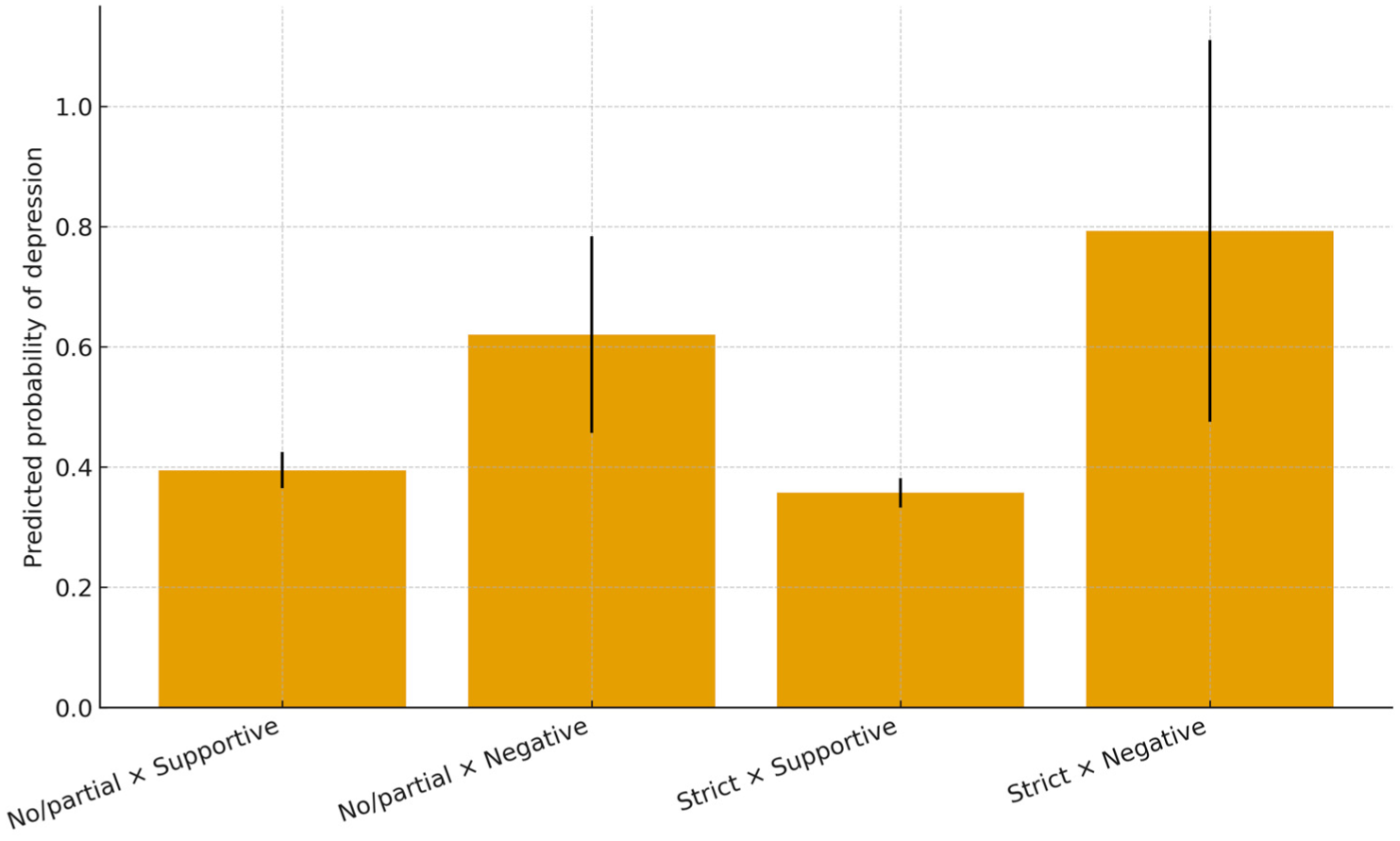
Configurational risk: strict unmet × caregiver attitude.
A monotone ordering emerges: the “strict unmet × negative climate” cell exhibits the highest predicted probability of depression (≈0.793, SE ≈ 0.162), while “no/partial unmet × supportive climate” is lowest (≈0.395, SE ≈ 0.016). Although the multiplicative interaction is not statistically decisive, the configuration provides descriptive evidence for a care-climate amplification mechanism: the same objective shortfall becomes more psychologically salient when the relational tone of care is impatient, reluctant, or emotionally withdrawn. Table 5 supplies cell means and confidence intervals for precise comparison.
Predicted Probabilities in the 2 × 2 Configuration (Strict Unmet × Caregiver Attitude).
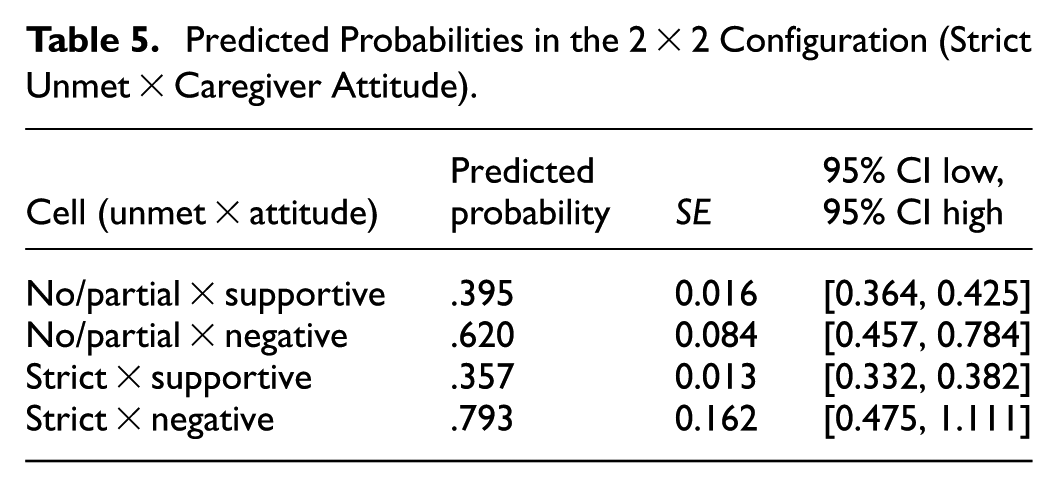
Two implications follow. First, the threshold is socially conditioned—not merely a matter of quantity of help but of how help is offered and felt. Second, “help on paper” may fail to protect mental health if the affective quality of care is eroded; summary counts of received help risk overestimating protection.
Structural Embedding: Baselines Vary by Place, Slopes Remain Modest
Unmet care operates against place-based baselines. Across specifications, urban residence is associated with higher depressive symptoms (Table 3, OR = 1.709, p = .001; GEE coefficient 0.515, SE = 0.170, p = .002). Compared to the West, the East shows lower odds (Table 3, OR = 0.752, p ≈ .051), with the Central region in between. Within each macro-region, slopes for strict unmet are small, while levels differ: in the West, predicted probabilities are 0.512 (no/partial) vs. 0.447 (strict); in the Central region, 0.390 versus 0.347; in the East, 0.347 versus 0.321 (Figure 5). A province-level mixed-effects logit yields a very small intraclass correlation (≈0.0004), indicating that once urbanicity and macro-regional contrasts are in the model, unobserved province-level variance adds little.

Predicted probabilities by region × unmet status.
Interpretively, where one lives—urban stressors, care ecologies, and social comparison regimes—sets the baseline, while unmet care adds a relatively stable, modest increment across contexts. The structural message is therefore asymmetric: baselines vary, slopes do not.
Estimator Ensemble and the Theory of Masking
To check estimator sensitivity under low event rates and two-wave dependence, we replicated the harmonized-binary models using population-averaged GEE, rare-events logit, and Firth penalized logit. Strict unmet remains small and marginal in all three (GEE: β = −0.228, p = .067; rare-events: β = −0.207, p = .091; Firth: β = −0.225, p = .064; Table 3). By contrast, the 2018 continuous model returns a positive, significant coefficient (Figure 2, β = 0.296, p = .001), and IPWRA recovers a substantive effect for any unmet (Figure 3; Table 4). The divergence suggests a measurement–selection masking mechanism: in very old samples with wave-specific instruments and potential proxy response, dichotomization and cross-wave compositing can bury meaningful associations that re-emerge once symptom gradation is preserved or assignment is balanced.
Age-band sensitivity (<85, 85–94, ≥95) shows small, non-significant slope differences for strict unmet, consistent with the idea that attenuation is structural to the combined outcome and harmonization, rather than localized in a single age stratum. The large year coefficient (2018 vs. 2014) is consistent with instrument change and level shifts, not a break in the unmet-care slope.
Synthesis: A Three-layer Mechanism for Late-life Risk
The evidence resolves into a three-layer account. Layer 1—Threshold: once any unmet support appears, depressive symptoms tend to rise; the signal is most visible when measurement retains symptom information or design balances covariates. Layer 2—Care-climate amplification: unmet care registers more sharply under a negative relational tone; “how help is given” modulates “how lack is lived.” Layer 3—Structural baselines: urbanicity and region anchor background risk; unmet care then adds a modest increment that is surprisingly stable across places. Methodologically, the divergence between harmonized-binary and continuous/weighted estimates formalizes masking as a socio-metric mechanism in very old populations: what looks like null under dichotomization may become legible once gradation is restored or imbalance reduced.
Therefore, late-life mental health is sensitive to basic care thresholds, relational climates, and place-based baselines. A direct policy corollary is evident in the data: treat any unmet assistance as a trigger for screening and referral; pair technical support with attitude-focused micro-interventions (communication, respite, small-grant relief) in families that exhibit a negative care climate; and interpret outcomes against urban/regional baselines rather than one-size-fits-all slopes.
Discussion
From Dose to Threshold: Reframing What Counts When Needs Are Basic
The evidence indicates that the relationship between unmet assistance and depressive symptoms is better understood as threshold-sensitive rather than smoothly dose–responsive. When symptom gradation is preserved or comparisons are rebalanced, even a small shortfall in help is associated with elevated risk. This pattern is consonant with conservation-of-resources theory, which assigns disproportionate weight to losses in essential goods, and with socioemotional selectivity and related self-regulation perspectives, which hold that in later life immediate threats to comfort and control loom larger than marginal gains elsewhere (Cohen & Sherman, 2014; Hobfoll, 2001; Hobfoll et al., 2016). In disablement terms, the presence of a gap in the infrastructure of daily living is sufficient to set a stress process in motion; further increments in shortfall add less than the crossing of the sufficiency line itself (Dourish & Bell, 2007; Griffith et al., 2017). This is consistent with work linking ADL limitations and unmet needs to mood and functioning in later life across settings, including nursing homes and community samples (Chen et al., 2025; Gao et al., 2023; Wassink-Vossen et al., 2022; Zhao et al., 2022).
This reframing has conceptual payoffs. It resolves ambiguity in literatures that treat unmet assistance as a linear dose, thereby underestimating the significance of small deficits. It also clarifies decision points for services: if the risk lies in the existence of a gap, then early, low-intensity responses to any shortfall are sensible on theoretical and practical grounds (Yu et al., 2023). It further helps explain why pooled dichotomies sometimes appear null: dichotomization compresses clinically meaningful variance and masks associations that re-emerge when symptom gradation is retained (Courtney et al., 2021). Against the broader backdrop of late-life distress—compounded by bereavement, multimorbidity, and cumulative role strain—such threshold-consistent patterns provide a compact, decision-relevant logic for screening and early action.
Care Climate as Amplifier: How Help Is Given Changes What Help Means
Findings support an amplification logic for the relational tone of care. Under a negative climate—impatience, reluctance, emotional withdrawal—the same objective shortfall carries a different psychological meaning than under a supportive one; it signals devaluation, burden, or rupture of moral expectations, and so weighs more heavily on mood. This aligns with research on expressed emotion, interaction rituals, and care ethics, which locates mental-health outcomes not only in the flow of practical resources but in the circulation of recognition and respect (Crespo et al., 2013; Cristoforetti et al., 2011; Neves et al., 2019; Olsson & Ingvad, 2001). It also resonates with studies of mental load and emotional labor in family care, underscoring how resource imbalance is experienced through relational meanings (Dean et al., 2022; Franzosa et al., 2019). In this view, attitude is less a mechanistic conduit and more a contextual lens that conditions how shortfalls are interpreted and absorbed.
The configuration approach—reading the four cells of unmet status by care climate—proves analytically useful. It shows the riskiest profile when strict shortfalls occur in a negative climate, and the most protective profile when shortfalls are absent or partial within a supportive climate. Rather than relying on fragile interaction tests, this ordering underscores a simple relational principle: how help is given conditions what help does. It also indicates realistic levers for change—communication routines, pacing, and predictability—through which families can make limited assistance feel sufficient (Graff & Vabø, 2023; Liu & Gallois, 2022; Woo et al., 2023). In normatively dense contexts of filial responsibility, breaches are not merely instrumental failures but can be read as erosions of respect or belonging, which helps explain why small material differences sometimes yield large psychological consequences (Qi, 2025).
Place as Baseline: Urbanicity and Region Anchor Background Risk
The data are consistent with a baseline interpretation of place. Urban settings carry higher background strain—faster tempo, denser comparison, more administrative demands—while certain regions exhibit lower background risk, likely reflecting service ecologies and expectations around family versus formal provision (H. Li et al., 2022; Muhammad, 2023; Yan et al., 2021; Yuan et al., 2024). Against these baselines, the incremental association of unmet assistance with depression is comparatively modest and relatively stable. In other words, context sets the starting level; unmet assistance shifts outcomes around that level rather than transforming the slope across places. This aligns with evidence that neighborhood safety, social comparison, and local service capacity shape mood even before specific shocks occur (Affleck & Tennen, 2024; Gong et al., 2022; Zhang, 2024).
This distinction matters for both inference and implementation. Analytically, a small pooled slope need not imply that unmet assistance is unimportant; it may reflect large, place-structured baselines that are not captured by averaged models. Practically, responses that only “chase the slope” risk underperforming where background strain is high. A more faithful reading treats any shortfall as a common trigger, while calibrating the intensity and mix of supports to local baselines—stronger linkage to community organizations and follow-up in urban neighborhoods, for example, and emphasis on access maintenance and continuity in regions with lower background risk (Cao et al., 2023; Lei et al., 2022; Yuan et al., 2024).
Measurement–Selection Masking: Why Design Choices Shape What We See
A consistent thread across estimators is the risk of measurement–selection masking. When heterogeneous instruments are pooled and symptoms are dichotomized, clinically meaningful gradations are compressed; when the older adults rely on proxy reporting or suppress symptoms due to stigma or perceived burden, comparisons become imbalanced (Adams et al., 2024; Alfaro et al., 2022; Courtney et al., 2021). These forces interact to mute signal in pooled dichotomies even when underlying associations persist.
Designs that preserve outcome gradation or rebalance comparisons make these patterns visible without claiming more causality than the data warrant (Khattar et al., 2022; Weziak-Bialowolska & Bialowolski, 2024). The lesson is not about a single “best” estimator; it is about aligning tools with theoretical stakes—threshold tests benefit from continuous outcomes and average-effect estimators that respect overlap, amplification tests benefit from configuration views, and place tests benefit from stratified predictions and explicit quantification of residual clustering.
Implications for Screening, Family Support, and Local Systems
Three practice-facing implications follow. First, treat any shortfall in basic assistance as a sensible trigger for brief screening and referral within stepped-care pathways; this advances detection without over-medicalizing late-life distress and aligns with evidence that modest resource losses can carry outsized psychological weight (Wassink-Vossen et al., 2022; Yu et al., 2023).
Second, address the care climate directly through light-touch, teachable tools—communication coaching, predictable scheduling, respite brokering, and small conditional grants—that convert reluctant routines into sustainable ones; attention to sleep and social support is also relevant where they co-vary with mood (Chen et al., 2025; Dean et al., 2022; Franzosa et al., 2019; Kim et al., 2025).
Third, read outcomes against local baselines: urban contexts may require stronger links to community organizations and follow-up routines, while regions with lower baselines may benefit from maintaining access and preventing backsliding; the availability of home- and community-based services and long-term care insurance are policy levers with demonstrated mental-health relevance (Lei et al., 2022; H. Li et al., 2022; Yu et al., 2022).
Monitoring and evaluation benefit from granular outcomes and balancing estimators. Continuous symptom scales provide sensitivity to change; doubly robust designs guard against specification risk; configuration visualizations help frontline teams see when climate is turning shortfalls toxic. Digital tools and community assets may also reduce disparities in detection and follow-up when tailored to local service ecologies.
Limitations and Agenda for Future Work
Several limitations invite further inquiry. The care-climate measure is a single item; developing compact multi-item scales that separate warmth, consistency, and perceived fairness would sharpen inferences and identify more precise levers for intervention. The two-wave design limits traction on temporal dynamics; higher-frequency panels or brief ecological assessments could capture how thresholds are crossed and climates evolve in real time. Observational data and standard controls reduce but do not eliminate confounding; designs that leverage staggered program rollouts, eligibility thresholds, or natural experiments would complement the present approach.
Generalizability is a second consideration. The setting is a large, heterogeneous country where family remains the primary locus of everyday care. Extending tests to systems with stronger formal provision, as well as to communities where intergenerational expectations differ, would clarify the scope conditions of the Threshold–Care Climate–Place framework. Cross-cultural comparisons and qualitative studies of how older adults narrate shortfalls—and of how caregivers perceive and regulate climate—would deepen the theoretical account.
Conclusion
Taken together, the findings consolidate a compact framework for understanding the link between unmet assistance and late-life depression. The threshold element clarifies when shortfalls matter: once a gap appears, risk rises when symptom information is preserved or comparisons are rebalanced. The care-climate element clarifies how shortfalls become consequential: a negative tone amplifies the psychological weight of even small deficits, while a supportive tone blunts it. The place element clarifies where background risk sits: urban and regional contexts anchor levels against which shortfalls are felt. This three-part structure integrates disablement, stress-process, relational, and ecological insights into a testable account that speaks to both scholarship and service design.
For practice, a straightforward workflow emerges: treat any shortfall as a screening trigger; pair technical support with attitude-focused micro-interventions that make relational patience easier; and interpret outcomes against local baselines, monitoring change with granular measures and balanced estimators. For research, priorities include developing brief, reliable care-climate scales; tracing threshold crossings with higher-frequency data; exploiting naturalistic variation for stronger identification; and extending tests across diverse care regimes. By reading late-life mental health through the threshold of basic care, the climate of everyday relations, and the place of living, systems can move earlier and act more precisely, while theory gains a stable scaffold that can travel across contexts.
Supplemental Material
sj-docx-1-sgo-10.1177_21582440261458495 – Supplemental material for Threshold, Care Climate, and Place: Unmet ADL Support and Late-Life Depressive Symptoms
Supplemental material, sj-docx-1-sgo-10.1177_21582440261458495 for Threshold, Care Climate, and Place: Unmet ADL Support and Late-Life Depressive Symptoms by Yan Xu and Yujie Zhang in SAGE Open
Footnotes
Ethical Considerations
The Chinese Longitudinal Healthy Longevity Survey (CLHLS) was approved by the Biomedical Ethics Committee of Peking University (IRB00001052–13074). The present study used publicly available, de-identified secondary data from the CLHLS. No attempt was made to re-identify participants.
Consent to Participate
Written informed consent was obtained from all participants or their legal representatives before each interview in the original CLHLS data collection. Because this study involved secondary analysis of publicly available, de-identified data, no additional informed consent was required in accordance with Section 8.05 of the APA Ethical Principles.
Author Contributions
Conceptualization: YX, YZ; Methodology: YX, YZ Formal analysis: YX; Data curation: YZ; Writing—original draft: YX, YZ; Writing—review & editing: YX, YZ; Funding acquisition: YZ; Supervision: YZ.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Chongqing Municipal Social Science Planning Doctoral and Cultivation Project (Grant 2023BS080).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.