
Abstract
This study evaluates the effectiveness of a web-based self-help psychoeducation intervention delivered through the Si-Konseling platform, which uses strengths-based cognitive-behavioral therapy (CBT) to address mental health issues such as anxiety, depression, and stress in survivors of abuse. A randomized controlled trial (RCT) was conducted with 182 participants from three Indonesian provinces. Participants were randomly assigned to the experimental group (n = 91), which received the intervention, or the control group (n = 91), placed on a waiting list. Psychological outcomes were measured using the Depression Anxiety Stress Scale-21 (DASS-21) and the Psychological General Well-Being Index (PGWBI) before and after the intervention. The results of Multivariate Analysis of Variance (MANOVA) showed a significant improvement in participants’ mental health outcomes in the experimental group compared to the control group, with large effect sizes observed across anxiety, depression, stress, and well-being. Post-hoc analysis revealed significant differences between the groups, confirming the intervention’s efficacy in reducing psychological distress and enhancing well-being. These findings suggest that the Si-Konseling program can serve as an effective tool for addressing mental health concerns in populations affected by abuse.
Plain Language Summary
This study tested Si-Konseling, an online self-help program designed to help survivors of violence in Indonesia improve their mental health. The program uses strengths-based counseling–focusing on users’ inner strengths—and includes guided sessions in storytelling, mindfulness, and positive thinking through a virtual counselor. 182 young women and men from three provinces took part. Half used the Si-Konseling program for four weeks; the other half waited without using it. Before and after the program, everyone answered questions about their anxiety, depression, stress, and overall well-being. Results showed that those who used Si-Konseling felt much better: their anxiety, depression, and stress dropped by more than half, while their sense of well-being nearly doubled. The waiting group showed no change. These improvements were large enough to make a real difference in daily life. The program was especially effective in reducing psychological distress and enhancing well-being among survivors of abuse. This shows that digital tools like Si-Konseling can offer effective, low-cost support to vulnerable people, even in places with few mental health resources. The findings support using similar online programs to help more survivors heal and regain their emotional strength.
Keywords
Introduction
Violence against women and children remains a pervasive global public health and human rights crisis. According to global estimates, approximately one in three women worldwide has experienced physical or sexual violence, while hundreds of millions of children suffer physical, emotional, or sexual abuse annually (Hillis et al., 2016; Mannell et al., 2022). These figures are further amplified by structural risk factors such as poverty, gender inequality, childhood exposure to violence, and sociocultural norms that normalize or silence abuse (Abrahams et al., 2014; Cara & Steinert, 2021). The onset of the COVID-19 pandemic intensified these vulnerabilities, with lockdowns and economic stressors contributing to increased incidence and reduced access to support services (Nation et al., 2023; Qu et al., 2022). Comprehensive and sustainable interventions are thus urgently needed to mitigate the profound consequences of violence and promote long-term recovery (Western & Varley, 2018).
While violence affects individuals of all genders, this study focuses specifically on women and children due to their disproportionate vulnerability and systemic barriers to care. Globally, women and girls face higher rates of intimate partner violence, sexual assault, and coercive control, often compounded by gender norms that discourage help-seeking (Kaul et al., 2024; Rodríguez et al., 2009). Children, meanwhile, are uniquely susceptible to developmental disruption, behavioral sequelae, and intergenerational transmission of violence (Chiodo et al., 2008; McFarlane et al., 2014). Although men can also be victims, particularly of emotional or psychological abuse, the prevalence, severity, and societal impact of violence against women and children necessitate targeted intervention research. This strategic focus aligns with national and international public health priorities aimed at protecting populations with the greatest unmet mental health needs.
The psychological toll of violence on survivors is well-documented. Women often experience elevated levels of anxiety (characterized by excessive worry, physiological arousal, and fear), depression (marked by persistent sadness, anhedonia, and hopelessness), stress (a state of chronic psychological and physiological tension), and post-traumatic stress symptoms (Boeckel et al., 2014; Satyanarayana et al., 2015). Concurrently, physical and reproductive health complications are common (Daligand, 2015; Popa, 2006). In children, exposure to violence is linked to behavioral dysregulation, cognitive delays, and heightened risk of perpetrating violence in adulthood (Leray, 2014; Moore et al., 2013). These outcomes underscore the critical need for accessible, evidence-based psychological support to interrupt cycles of harm.
In this study, we operationalize four core mental health outcomes: (a) Anxiety: persistent and excessive fear or worry, often accompanied by autonomic arousal (e.g., rapid heartbeat, restlessness); (b) Depression: a mood disorder involving sustained low mood, loss of interest, and feelings of worthlessness; (c) Stress: a non-specific state of psychological strain in response to perceived threats or demands; dan (d) Well-being: a multidimensional construct encompassing positive affect, self-control, vitality, and overall life satisfaction (Dupuy, 1984; Ifdil et al., 2023).
Existing interventions, such as trauma-focused CBT, parent-child CBT, EMDR, and empowerment-based group programs, have demonstrated efficacy in reducing trauma symptoms (Bowland et al., 2012; Caro et al., 2023). However, accessibility remains a major barrier, especially in low-resource or stigmatized contexts (Fullilove et al., 2024; Trevillion et al., 2016). Survivors frequently encounter cultural taboos, logistical constraints (e.g., cost, transportation), and fragmented service systems that impede care (Das et al., 2022; Simmons et al., 2015).
Digital mental health platforms offer a promising alternative. Web-based interventions like ACT and the SAFE program have shown significant reductions in anxiety, depression, and PTSD among abuse survivors, with high user satisfaction and perceived safety (Fiorillo et al., 2017; van Gelder et al., 2023). Similarly, preventive tools such as “Cool and Safe” have effectively enhanced children’s safety skills without increasing distress (Müller et al., 2014).
Recent advances in digital learning and artificial intelligence further validate the potential of technology-mediated psychoeducation. For instance, Firdaus et al. (2024) demonstrated that integrating wireless local area networks (WLAN) with analytical hierarchy processes enhances online learning adoption through improved accessibility and usability, a principle directly applicable to Si-Konseling’s design philosophy. Furthermore, Al-Worafi et al. (2024) found that generative AI models like ChatGPT can serve as effective educational guides when used responsibly, supporting curriculum development and learner engagement. This suggests that digital platforms, even those not fully autonomous, can function as credible, scalable, and supportive tools for delivering structured mental health content, especially in resource-constrained environments. The integration of virtual counselors and immersive features reflects an emerging trend in digital pedagogy, where technology is leveraged not only for delivery but also for enhancing user experience and therapeutic alliance (Ting et al., 2024). As Wang and Akhter (2025) show, even non-human agents can influence emotion regulation and vocabulary retention, indicating that digital interfaces can elicit meaningful psychological responses, especially when designed with cultural sensitivity and cognitive scaffolding.
Building on this evidence, we developed Si-Konseling (Sistem Informasi Konseling), a web-based psychoeducation platform grounded in strengths-based CBT (Suranata et al., 2021). Unlike traditional deficit-focused models, strengths-based CBT emphasizes personal resilience, agency, and existing coping resources (Padesky & Mooney, 2012). The Si-Konseling program integrates three evidence-informed modules, namely, (a) Narrative therapy to reframe trauma into empowering life stories (Bećirović, 2021); (b) CBT-based mindfulness to enhance present-moment awareness and reduce rumination (Antoniou et al., 2022); and (c) Neuro-Linguistic Programming (NLP) to restructure maladaptive thought patterns and foster psychological flexibility (Stein-Rubin & Adler, 2024).
The present study aims to evaluate the effectiveness of the Si-Konseling program in reducing psychological distress (anxiety, depression, stress) and enhancing well-being among abuse survivors through a randomized controlled trial. While preliminary studies support its feasibility (Suranata et al., 2020; Suranata et al., 2021), rigorous efficacy testing is needed to validate its impact across diverse populations.
Method
Participants
Of the 629 individuals invited to participate, 182 met the inclusion criteria and were enrolled in the study. Participants were recruited from three Indonesian provinces: West Sumatra (n = 192), Bali (n = 230), and East Nusa Tenggara (n = 207). The online screening survey was conducted between May 10 and June 10, 2024. After screening, 182 eligible participants were randomly assigned to either the experimental group (n = 91) or the waiting-list control group (n = 91). Six participants in the experimental group discontinued the intervention for personal reasons, resulting in a final sample of 85 participants in the experimental group and 91 in the control group for analysis. Participants’ ages ranged from 18 to 25 years (M = 20).
Inclusion criteria were: (a) Experience of violence: Participants must have experienced at least one form of abuse (verbal, physical, mental, or other); and (b) Severe psychological distress: Participants must have scored at least one severe indicator on the DASS-21. Those who did not meet these criteria or failed to complete the pre-screening survey were excluded.
Design
A randomized controlled trial (RCT) design was employed, considered the gold standard for evaluating intervention efficacy (Gill, 2021). Participants were assigned to groups using block randomization to ensure balanced distribution across key variables (White, 2013). Figure 1 illustrates the participant flow.
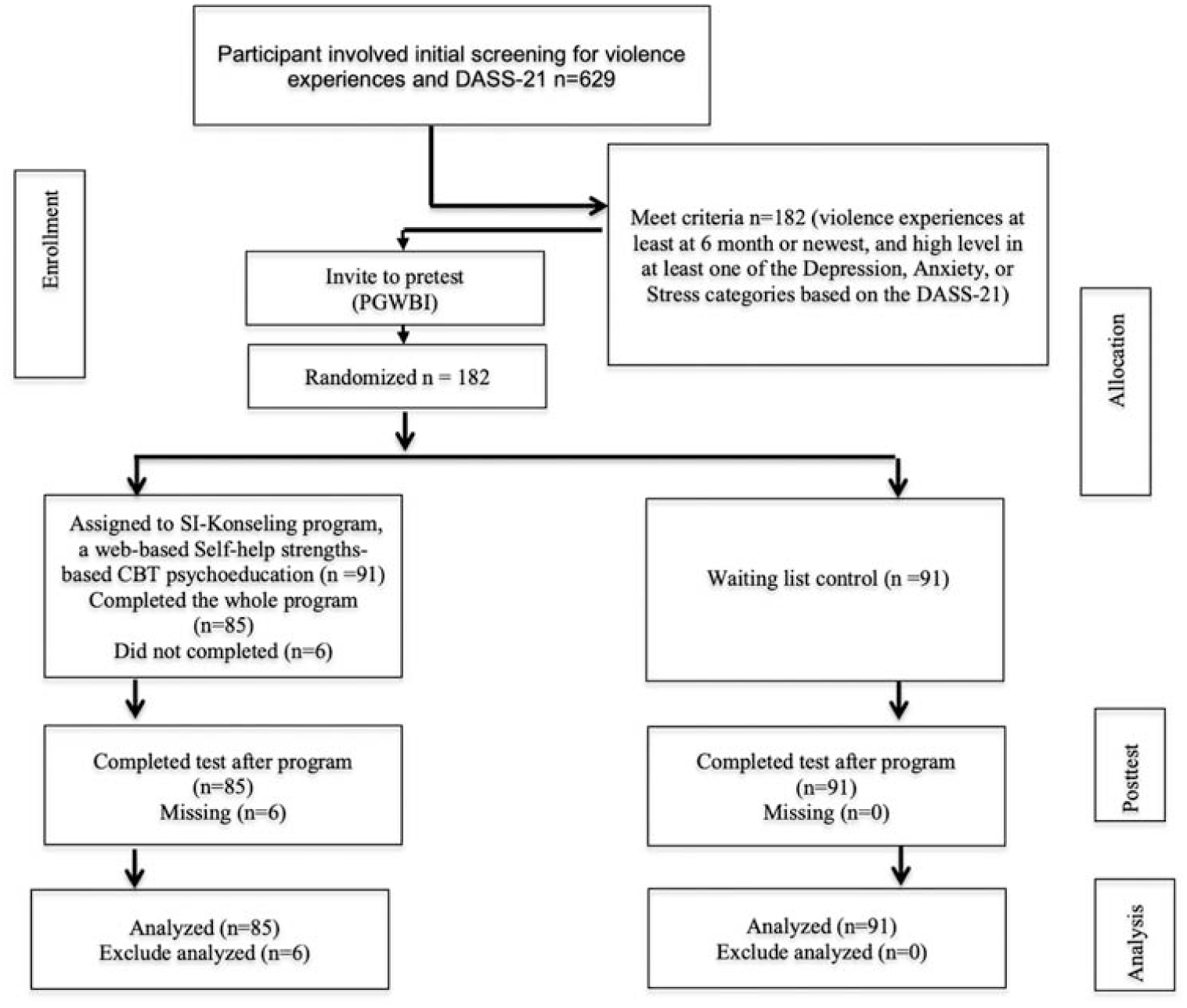
Participant flow.
Intervention Protocol
The experimental group received a self-help psychoeducation program delivered via the Si-Konseling platform, grounded in strengths-based CBT (Nickerson & Fishman, 2013; Padesky & Mooney, 2012). The platform integrates three core modules: Narrative Therapy, Mindfulness, and Neuro-Linguistic Programming (NLP), each delivered through virtual counselor-guided audio-video tutorials.
The intervention protocol followed seven sequential steps (see Figure 2): (1) Participant login; (2) Orientation tutorial; (3) Access to main menu; (4) Pre-assessment using DASS-21 and PGWBI; (5) Completion of structured sessions: Narrative Therapy (3 sessions × 50 min), Mindfulness (5 sessions × 50 min), and NLP (3 sessions × 50 min); (6) On-demand communication with virtual counselors for guidance; and (7) Post-intervention assessment. Participants were given 4 weeks to complete the program at their own pace. Internet access costs were subsidized for the experimental group. The control group received the full intervention after post-test completion.
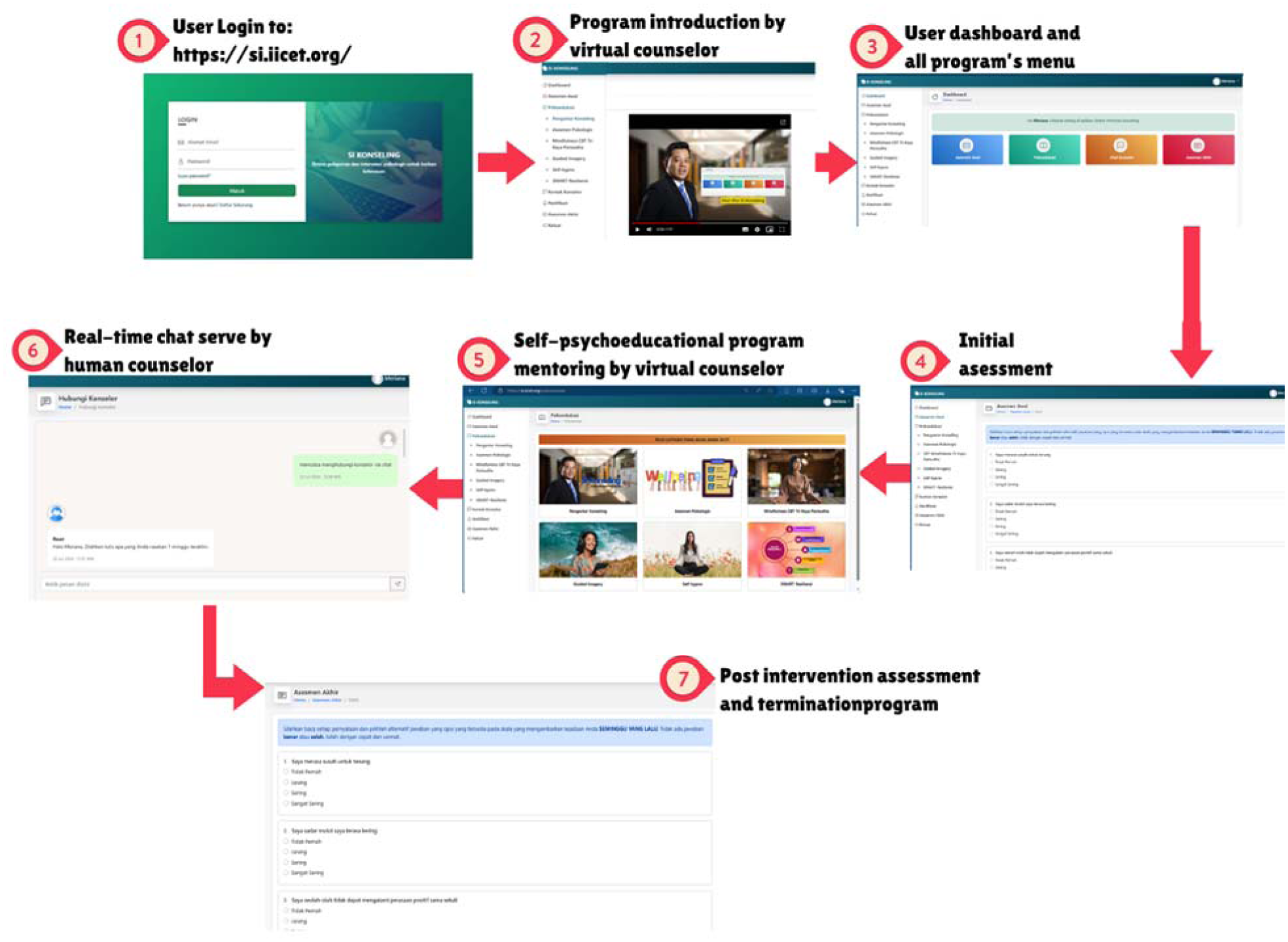
SI-Konseling program flow procedure illustration.
Ethical Approval and Informed Consent
This study received ethical approval from the Research Ethics Committee of Universitas Pendidikan Ganesha (Approval No. 008/UN48.16.04/PT/2025) on April 29, 2025, in accordance with the Declaration of Helsinki. All participants provided written informed consent before enrollment. For minors under 18 years of age, written assent was obtained in addition to parental/guardian consent. Participation was voluntary, and participants were informed of their right to withdraw at any time without penalty. Data were anonymized to ensure confidentiality, and procedures were designed to minimize psychological risk, including access to on-demand counseling support during the intervention.
Measures
Psychological outcomes were measured using the Depression Anxiety Stress Scale-21 (DASS-21; Kraska et al., 2023) and the Psychological General Well-being Index (PGWBI; Ifdil et al., 2023). The DASS-21 is a 21-item self-report measure assessing depression, anxiety, and stress, with each subscale comprising seven items rated on a 4-point Likert scale (0 = did not apply to me at all; 3 = applied to me very often or most of the time). Higher scores indicate greater psychological distress. The Indonesian version has demonstrated strong psychometric properties, including acceptable reliability (composite α = .806–.917) and a bifactor structure (Muttaqin & Ripa, 2021).
The PGWBI-22 is a 22-item scale measuring overall psychological well-being across six dimensions: anxiety, depression, positive well-being, self-control, general health, and vitality (Ay et al., 2010). Items are rated on a 6-point scale, with higher scores reflecting better well-being. The Indonesian version exhibits excellent internal consistency (α = .96; Ifdil et al., 2023).
Statistical Analysis
Multivariate Analysis of Variance (MANOVA) was used to assess the intervention’s effect on the combined dependent variables (depression, anxiety, stress, well-being), with Pillai’s Trace as the test statistic due to its robustness to assumption violations (Ntumi, 2021). Assumptions of homogeneity of covariance matrices (Box’s M-test, p > .05) and multivariate normality (Shapiro-Wilk, p > .05) were confirmed. Post hoc ANOVAs with Bonferroni correction examined individual effects. Analyses were performed using JASP (Goss-Sampson, 2020) at α = .05.
Results and Discussion
Baseline characteristics between the experimental and waiting-list control groups were highly comparable, confirming successful randomization. As shown in Table 1, pre-intervention scores for anxiety (Mexp = 14.26, SD = 2.65 vs. Mctrl = 14.30, SD = 2.63), stress (Mexp = 13.20, SD = 2.38 vs. Mctrl = 13.45, SD = 2.48), and well-being (Mexp = 38.89, SD = 6.72 vs. Mctrl = 39.00, SD = 7.30) were nearly identical, indicating equivalent levels of psychological distress and functioning at baseline. Although the control group reported slightly higher pre-depression scores (M = 14.08 vs. M = 13.38), this difference was statistically negligible and well within the margin of measurement error.
The Depression, Anxiety, Depression, and Well-Being Among Groups in Pre and After Intervention.
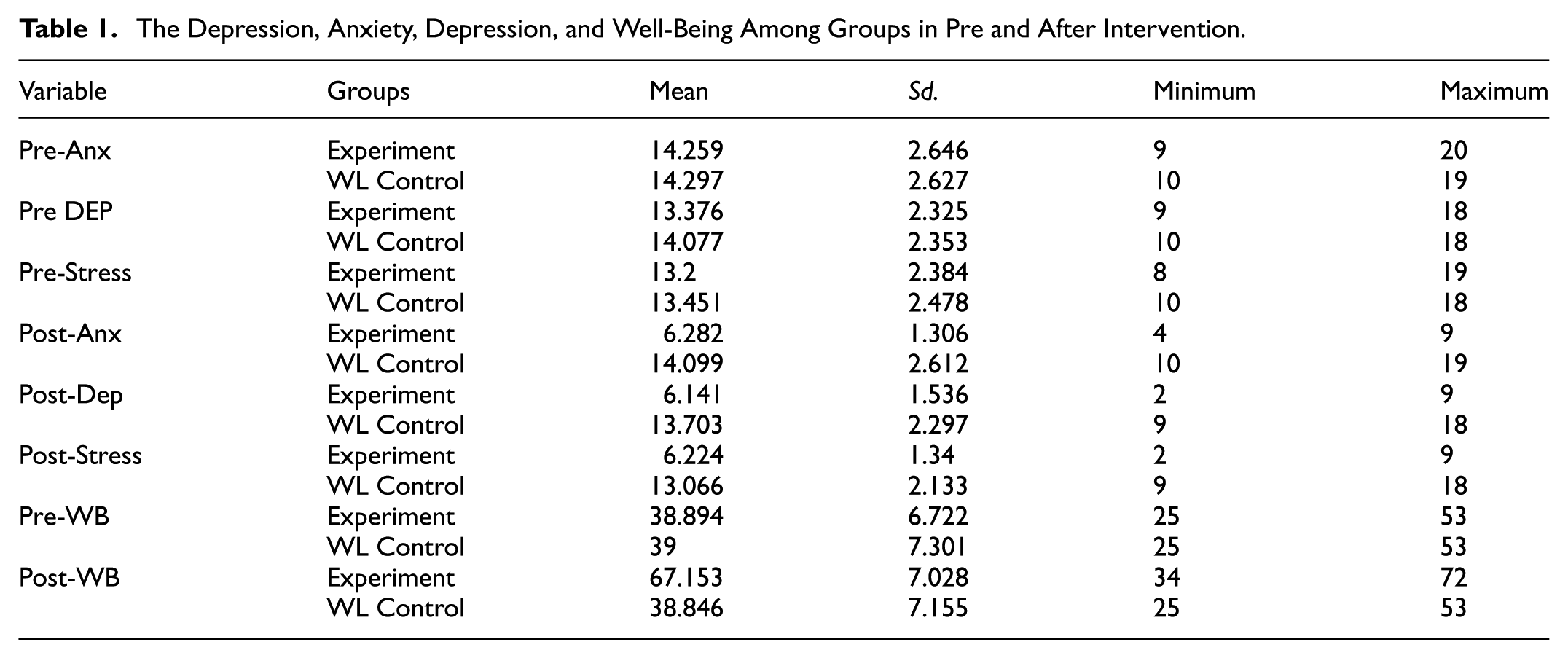
Following the 4-week intervention, the experimental group exhibited clinically and statistically significant improvements across all outcomes. Post-intervention anxiety scores dropped from 14.26 to 6.28, a 56% reduction, placing the majority of participants below the clinical threshold for moderate anxiety (typically DASS-21 Anxiety ≥ 8; Lovibond & Lovibond, 1995). Similarly, depression scores declined from 13.38 to 6.14 (54% reduction), and stress levels fell from 13.20 to 6.22 (53% reduction), indicating a substantial reduction in chronic psychological tension and hyperarousal.
In stark contrast, the control group showed no meaningful change, with post-assessment scores remaining virtually identical to baseline. Most notably, well-being in the experimental group increased by 73%, from a mean of 38.89 to 67.15, approaching the upper range of the PGWBI scale (where scores > 65 reflect high life satisfaction and emotional regulation), whereas the control group remained stable (M = 38.85).
These divergent trajectories are visually summarized in Figure 3, which illustrates the marked post-intervention improvement in the experimental group across all four domains, while the control group’s scores remained flat.
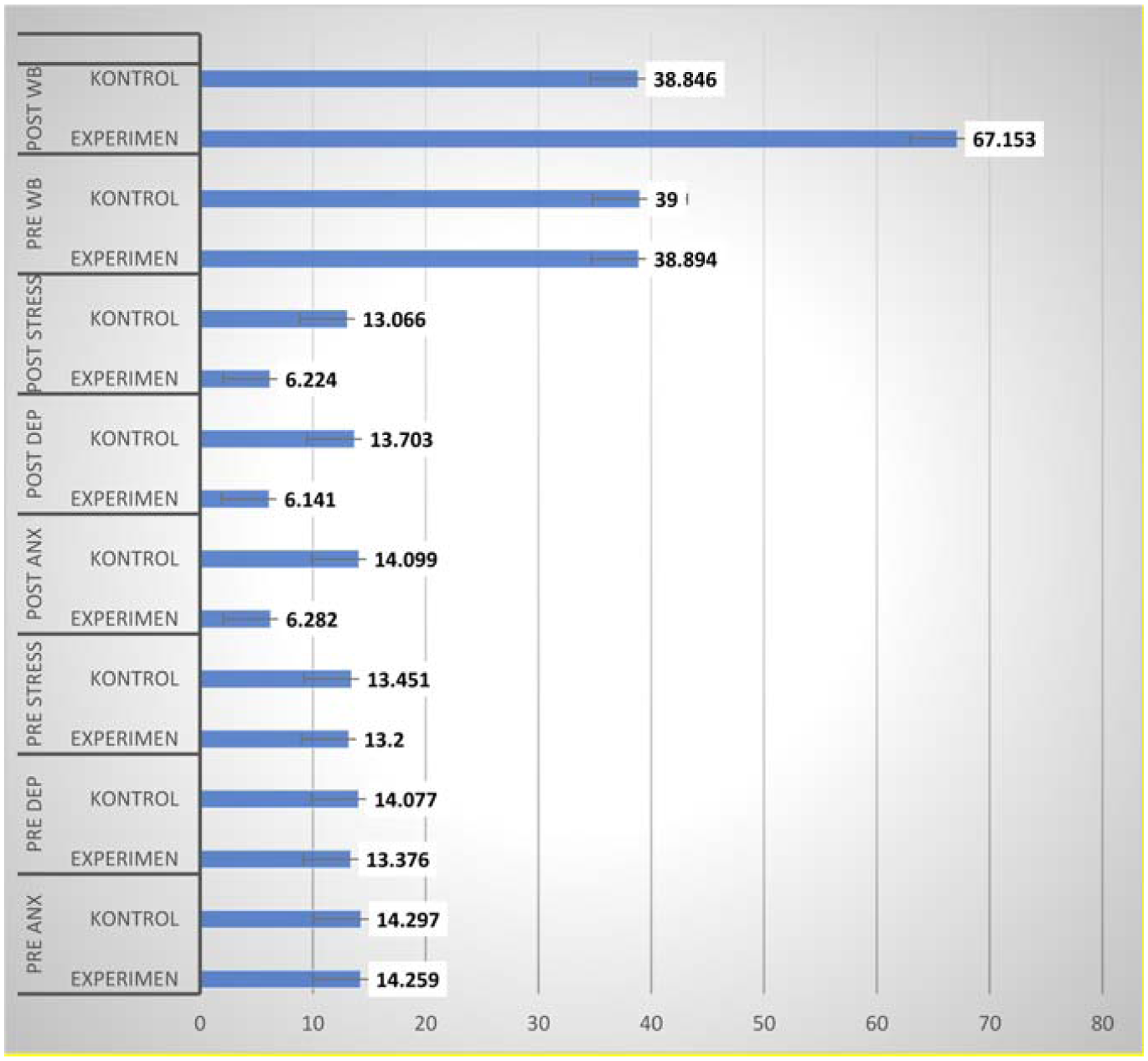
Histogram depression, anxiety, depression, and well-being among groups in pre and after-intervention.
To statistically validate these observations, a MANOVA was conducted. As reported in Table 2, the assumptions of homogeneity of covariance matrices (Box’s M:χ2 = 60.90, p = .061) and multivariate normality (Shapiro-Wilk: W = 0.98, p = .054) were satisfied. The MANOVA revealed a robust multivariate effect of group assignment, Pillai’s Trace = 0.891, F(4, 171) = 347.81, p < .001, indicating that the intervention explained 89.1% of the variance in mental health outcomes.
MANOVA Analysis Results for Depression, Anxiety, Depression, and Well-Being.
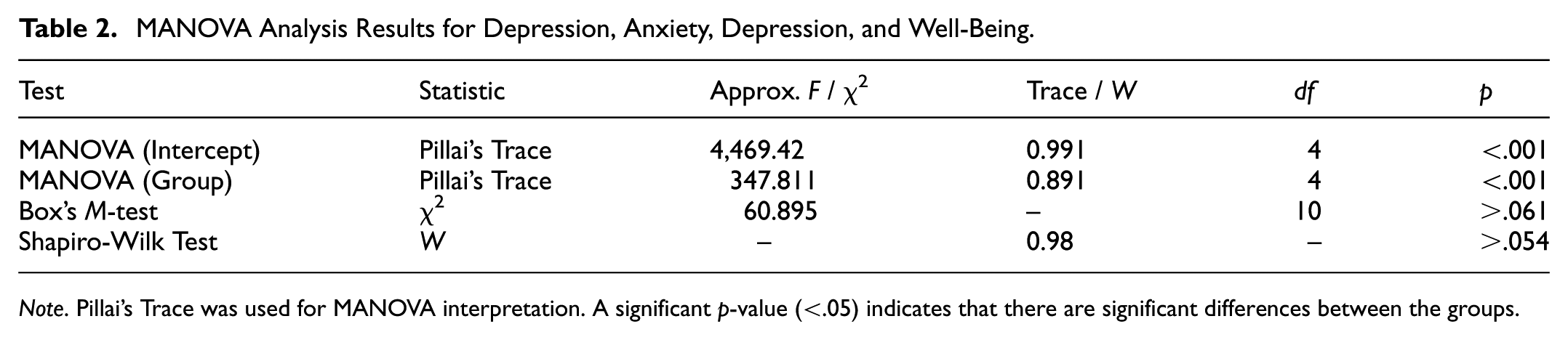
Note. Pillai’s Trace was used for MANOVA interpretation. A significant p-value (<.05) indicates that there are significant differences between the groups.
Post-hoc ANOVA analyses (see Table 3) confirmed large and statistically significant differences between the experimental and waiting-list control groups across all four outcome measures. Participants in the experimental group reported a substantial reduction in anxiety symptoms, with a mean difference of −8.01 (η2 = .187). Similarly, depression scores decreased significantly, showing a mean difference of −7.76 (η2 = .190). Stress levels also declined markedly, with a mean difference of −7.60 (η2 = .222), representing the largest effect size among the distress indicators. In contrast, psychological well-being demonstrated a pronounced increase, with the experimental group scoring, on average, 30.82 points higher than the control group (η2 = .217). All effect sizes exceeded Cohen’s (1988) threshold for a large effect (η2 ≥ .14), underscoring the clinical meaningfulness of the intervention’s impact on both symptom reduction and positive psychological functioning.
Post-Hoc ANOVA Anxiety, Depression, Stress, and Well-Being.

All effect sizes exceeded Cohen’s (1988) benchmark for large effects (η2 ≥ .14), and the mean differences surpassed the minimal clinically important difference (MCID) for DASS-21 subscales (typically 5–6 points), underscoring the clinical relevance of the findings.
Discussions
The present study provides robust evidence for the efficacy of Si-Konseling, a web-based strengths-based CBT program, in significantly reducing psychological distress and enhancing well-being among survivors of abuse. With large effect sizes (η2 = .187–.222) and an 89.1% variance explained by group assignment (Pillai’s Trace = 0.891), the intervention demonstrates not only statistical significance but also clinical relevance, exceeding minimal clinically important differences (MCID) for DASS-21 subscales. These findings confirm that digital interventions can achieve substantial therapeutic impact, even in resource-constrained settings.
These results align with and extend the growing body of literature on digital strengths-based interventions. For instance, Severo et al. (2025) reported significant improvements in resilience and emotional well-being from an online strengths-based CBT model in hospitalized patients, while Mireau and Inch (2009) demonstrated the effectiveness of brief solution-focused counseling in community mental health services. Our findings confirm that these benefits are replicable beyond clinical or Western contexts, particularly in culturally diverse, high-stigma environments like Indonesia, where traditional care is often inaccessible due to social norms and logistical barriers (Kaul et al., 2024; Rodríguez et al., 2009).
Crucially, Si-Konseling goes beyond symptom reduction by actively cultivating psychological well-being, a core tenet of strengths-based CBT (Flückiger et al., 2023; Padesky & Mooney, 2012). The 73% increase in PGWBI scores (ΔM = +30.8) surpasses typical gains in conventional CBT trials (Δ ≈ 10–15), suggesting that integrating narrative therapy, mindfulness, and neuro-linguistic programming within a strengths framework amplifies therapeutic outcomes. This supports a paradigm shift from a “deficit-reduction” to a “resource-building” model in trauma recovery (Yan et al., 2020; Zhou et al., 2024), positioning well-being not as the absence of distress, but as a distinct, cultivatable state.
The success of Si-Konseling underscores the critical role of virtual counselors and immersive technology in creating safe, engaging therapeutic spaces. As Cooper et al. (2019) and Park et al. (2023) have shown, avatar-mediated counseling enhances rapport, presence, and user satisfaction, key factors for engagement among trauma survivors who fear judgment or retraumatization. In our sample, the platform’s anonymity and self-paced design likely contributed to high adherence and low dropout (only 6 out of 91 discontinued), addressing a persistent challenge in digital mental health (Paalimäki-Paakki et al., 2022).
This innovation resonates with emerging research on AI and digital equity. Al-Worafi et al. (2024) demonstrated that ChatGPT, when guided by educators, can generate high-quality educational content, validating our design philosophy: structured, scalable, and culturally adapted psychoeducation delivered via digital interfaces can be as effective as face-to-face care in contexts of resource scarcity. Similarly, Ting et al. (2024) showed that big data mining can mediate academic performance and crime prevention among youth, reinforcing that data-driven, personalized interventions like Si-Konseling are especially relevant for young populations navigating trauma and stigma.
Moreover, the platform’s success across three Indonesian provinces, such as West Sumatra, Bali, and East Nusa Tenggara, echoes findings by Firdaus et al. (2024) and Soon et al. (2025), who emphasized the importance of technology acceptance models (TAM) and inclusive digital infrastructure in low-resource settings. Our results suggest that Si-Konseling’s self-paced, anonymous interface reduces barriers related to gender norms and social judgment, aligning with TAM principles that highlight perceived usefulness and ease of use as key drivers of adoption.
Josephng et al. (2025) argue that generative AI and encryption technologies can revolutionize cybercrime mitigation, a parallel to how Si-Konseling mitigates the “cyber-social crime” of stigma and exclusion. By leveraging encrypted communication and AI-guided tutorials, the platform protects user identity while maintaining clinical fidelity, making it a model for ethical digital mental health delivery in vulnerable communities.
Despite its strengths, challenges remain. While digital interventions offer scalability and cost-efficiency (Venkatesan et al., 2020), they risk impersonal delivery if not designed with emotional intelligence and cultural sensitivity. Our platform’s integration of Balinese values (e.g., Tri Kaya Parisudha) and localized narratives may explain its high acceptability, a lesson for future adaptations in other cultural contexts.
Ultimately, this study positions Si-Konseling not merely as a local innovation, but as a model for SDG-aligned digital public health infrastructure. It directly contributes to: (a) SDG 3.4: Reducing premature mortality from mental health conditions through scalable, low-cost intervention; (b) SDG 5.2: Eliminating gender-based violence by providing accessible, culturally safe recovery pathways; (c) SDG 9.1: Building resilient infrastructure for digital health services in underserved regions; and (d) SDG 10.2: Promoting social and political inclusion through equitable access to psychosocial support.
These results offer a compelling reference for practitioners, policymakers, and researchers seeking to innovate in mental health service delivery. Si-Konseling provides a viable, low-cost, and scalable model for extending high-quality psychosocial support to underserved communities, particularly in low-resource settings with significant cultural barriers. Future research should focus on replicating these findings with larger, more diverse samples and evaluating the long-term sustainability of the intervention’s benefits.
In conclusion, strengths-based digital interventions like Si-Konseling represent a vital component of the global mental health innovation movement, demonstrating that technology, when thoughtfully designed and implemented, can be a powerful catalyst for healing, empowerment, and equitable access to care for some of society’s most marginalized individuals.
Limitations and Future Directions
First, the sample was limited to ages 18 to 25 and excluded male survivors. Future studies should test Si-Konseling with diverse age groups, genders, and trauma types. Second, the 4-week follow-up precludes conclusions about long-term efficacy. Third, the active components (e.g., NLP vs. mindfulness) were not isolated; dismantling trials are needed to identify essential mechanisms.
Practical Implications
Given its success across three Indonesian provinces (West Sumatra, Bali, East Nusa Tenggara), Si-Konseling is a strong candidate for integration into national mental health systems, particularly within Dinas Sosial and Rumah Berdaya networks. It also offers a model for LMICs seeking scalable, stigma-free support for violence survivors.
Conclusion
In conclusion, the results of this study provide robust evidence that Si-Konseling, a web-based self-help psychoeducation program grounded in the strengths-based CBT paradigm, is highly efficacious in improving mental health outcomes and enhancing overall well-being among survivors of violence. The intervention demonstrated large effect sizes across all key domains, reducing anxiety, depression, and stress while simultaneously boosting psychological well-being, thereby addressing not only symptom reduction but also fostering positive psychological growth.
This finding underscores the transformative potential of technology-enabled, strengths-focused interventions. By leveraging digital platforms to deliver culturally sensitive, user-centered care, Si-Konseling directly addresses critical barriers to access faced by vulnerable populations, including cultural stigma, logistical constraints, and systemic gaps in service provision. As such, it aligns with and advances Sustainable Development Goal 3 (Good Health and Well-being), particularly targets 3.4 (reduce premature mortality from non-communicable diseases, including mental health conditions) and 3.8 (achieve universal health coverage). It also contributes to SDG 5 (Gender Equality) by offering a scalable, stigma-reducing pathway for women and girls who are disproportionately affected by gender-based violence.
The success of Si-Konseling highlights the critical role of virtual counselors and immersive technology in creating safe, engaging therapeutic spaces. This innovation resonates with recent findings on avatar-mediated therapy, which demonstrate enhanced rapport, presence, and satisfaction among users (Cooper et al., 2019; Park et al., 2023). Furthermore, its integration of narrative therapy, mindfulness, and neuro-linguistic programming reflects a holistic, multi-modal approach that empowers users to reframe their experiences, cultivate resilience, and build personal agency, core tenets of the strengths-based model (Flückiger et al., 2023; Zhou et al., 2024).
These results offer a compelling reference for practitioners, policymakers, and researchers seeking to innovate in mental health service delivery. The Si-Konseling program provides a viable, low-cost, and scalable model for extending high-quality psychosocial support to underserved communities, particularly in low-resource settings or regions with significant cultural barriers. Future research should focus on replicating these findings with larger, more diverse samples and evaluating the long-term sustainability of the intervention’s benefits.
Ultimately, this study positions strengths-based digital interventions like Si-Konseling as a vital component of the global mental health innovation movement, demonstrating that technology, when thoughtfully designed and implemented, can be a powerful catalyst for healing, empowerment, and equitable access to care for some of society’s most marginalized individuals.
Footnotes
Author Note
This manuscript has not been submitted to a preprint server prior to submission to SAGE Open. The authors confirm that the work described is original research, has not been published previously, and is not under consideration for publication elsewhere, in whole or in part. All listed authors have reviewed and approved the final manuscript. This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and analyzed during the current study are available from the corresponding author* on reasonable request. Due to ethical and privacy considerations related to sensitive mental health and personal trauma data, the full dataset is not publicly deposited in an open repository. However, anonymized data and analysis scripts can be shared upon formal request for research purposes, contingent upon approval of a data sharing agreement and adherence to confidentiality protocols.