
Abstract
Evidence indicates that conducting research, especially within the health sector, is associated with numerous challenges, notably those related to individual participation. This study aimed to identify the barriers affecting stakeholder participation in healthcare research. This cross-sectional study was conducted in 2025 employing a mixed-methods design comprising two distinct phases: a systematic review of reviews and an exploratory qualitative interview approach. During the initial phase, multiple databases were systematically searched. In the subsequent phase, 17 unstructured interviews were conducted with university faculty members. Data analysis was performed in accordance with the Boyatzis framework for thematic analysis. The systematic review resulted in the inclusion of 20 studies. The findings indicated that multiple thematic barriers hinder individual participation in healthcare research projects, including Communication Barriers, Attitudinal Barriers and Motivational Deterrents, Structural and Institutional Challenges, Awareness and Knowledge-Related Challenges, and Research and Methodology-Related Challenges. The interview data corroborated approximately 77% of the findings reported in previously published studies within the literature. Overall, Structural and Institutional Challenges emerged as the most frequently cited barriers impeding beneficiary participation in healthcare projects. The study’s findings identified multiple thematic barriers restricting individual participation in healthcare research projects. These findings can be leveraged by relevant stakeholders within the context to promote participation in such projects through an evidence-based approach.
Plain Language Summary
This study addresses a critical issue in health services research’ the challenges associated with individual and stakeholder participation in healthcare research projects. Despite the increasing need for inclusive and representative research, participation barriers often remain overlooked and inadequately addressed. Our investigation utilized a robust, mixed-methods approach, combining a systematic review of twenty relevant studies with qualitative insights drawn from seventeen in-depth interviews with university faculty members. By applying the Boyatzis framework for thematic analysis, we identified and categorized barriers into five key themes: Communication Barriers, Attitudinal and Motivational Challenges, Structural and Institutional Challenges, Knowledge and Awareness Deficits, and Methodology-Related Issues. Importantly, our findings highlight Structural and Institutional Challenges as the most frequently reported obstacles, underscoring the need for systemic changes to foster meaningful engagement. These insights offer valuable evidence to guide stakeholders, policymakers, and researchers in designing strategies to enhance beneficiary participation in healthcare research.
Keywords
Background
Research, or scientific inquiry, is defined as a systematic investigation designed to develop or contribute to generalizable knowledge (ORI, 2026). In the healthcare domain, research often involves studies conducted on human subjects in order to better understand diseases and to develop diagnostic and therapeutic interventions (Çaparlar & Dönmez, 2016). In such context, there has been a significant increase in research related to digital medicine, utilizing artificial intelligence and telemedicine (online consultations; Zhang et al., 2024). Countries such as Germany, the United States, and China are leading the way through extensive international collaborations (Badareu et al., 2025).
The beneficiaries in health research encompass a broad range of individuals and organizations. In this regard, research participants are among the most significant stakeholders; these individuals are typically subject to more intensive monitoring and gain access to specialized healthcare that may otherwise be unavailable to them. They may also have access to novel treatments that have not yet been made widely available (NHS, 2020). Another group of beneficiaries includes future generations within society, as health research greatly contributes to the development of new diagnostic tests, treatments, and healthcare service processes that may benefit generations to come (NHS, 2020). Overall, the general public also stands to benefit from health research; by addressing health inequalities through targeted research initiatives, society benefits from improved public health outcomes and more equitable access to healthcare services (NHS England, 2023). Additionally, healthcare organizations such as hospitals involved in research activities are important beneficiaries. These hospitals often report lower mortality rates and deliver higher quality care. Moreover, participation in research enhances staff satisfaction, improves recruitment and retention, and fosters a culture of innovation within hospitals (Holliday et al., 2023). Beyond those already mentioned, researchers and institutions investing in research projects are also beneficiaries in health research. In this context, research can lead to cost savings for services by improving efficiency, and it may generate commercial revenue through intellectual property associated with project outcomes (Holliday et al., 2023).
Evidence indicates that conducting research, particularly studies conducted in the health sector, is associated with numerous challenges, including the presence of complex and time-consuming planning processes. Complicated administrative procedures for developing research projects represent another significant obstacle to health research. Additionally, the lack of appropriate infrastructure—including technological tools and sufficient financial resources—constitutes a fundamental problem. Moreover, recruiting healthcare professionals is challenging due to a shortage of training and experience in scientific writing, as well as competitive clinical demands. The translation of research knowledge or the application of research findings into practice also faces barriers. Furthermore, weak collaboration between universities and healthcare services is an additional challenge (Bonfim et al., 2023). In addition to the aforementioned issues, complex ethical and regulatory systems have created multiple problems in the process of health research. Limited funding for conducting clinical trials is cited as one of the greatest obstacles, as securing adequate financial support is extremely difficult. Recruiting patients to participate in clinical trials is also fraught with challenges, often due to a lack of awareness or mistrust regarding research. Furthermore, a shortage of specialized personnel to manage clinical trials is considered a serious concern (Varse et al., 2019).
The literature has identified various barriers that influence individuals’ participation in research projects. In this regard, financial constraints often present a barrier to participation in research. In this context, the availability of funding can significantly influence the level of engagement in clinical research (Jacobson et al., 2008; Lloyd et al., 2004). The lack of experienced professionals to serve as mentors or supervisors is another important obstacle, particularly for students or novice researchers (Adebisi, 2022). Time constraints associated with conducting research, a lack of knowledge and expertise, insufficient motivation, and a shortage of equipment and resources are additional challenges to participation in health research (Adebisi, 2022; Doulani & Hossaini, 2024; Jacobson et al., 2008).
A previously published review of reviews exists in the literature examining barriers to individual participation in healthcare research, indicating a sufficient body of review studies to support conducting such overviews. In this regard, the study synthesized 26 systematic reviews to identify psychosocial factors affecting participation in health research. The study presented that the barriers varied by context. Some factors, such as participant information and social influences, functioned as both barriers and facilitators. These were mainly linked to Motivation and Opportunity in the Theoretical Domains Framework (TDF) (Sheridan et al., 2020). The TDF is a robust, theory-informed framework developed to integrate and streamline numerous psychological and organizational theories that explain behavior change, particularly within healthcare and implementation research (Atkins et al., 2017; Michie et al., 2005). It originally consolidated constructs from a wide range of behavioral and behavior-change theories into broader, conceptually coherent domains, synthesizing 128 explanatory constructs into 12 domains that collectively encompass cognitive, social, affective, and environmental determinants of behavior (Francis et al., 2012; Michie et al., 2005). However, a subsequent validation and refinement study resulted in a revised version of the TDF, comprising 14 domains and 84 constructs (Cane et al., 2012). As a single theory, the TDF principal applications include identifying barriers and enablers to behavior change, guiding both qualitative and quantitative analyses of behavioral determinants, and informing the design of targeted interventions by aligning identified determinants with suitable change strategies (Atkins et al., 2017; French et al., 2012; Richardson et al., 2019). Consequently, the TDF serves as an appropriate and effective framework for examining data related to the barriers affecting beneficiaries’ participation in healthcare research projects.
Given the mature topic and substantial existing literature, conducting a systematic review of reviews to comprehensively compile and integrate available evidence is more appropriate than performing a primary review of original research. In such context, identifying the barriers that influence beneficiary participation in healthcare research offers numerous advantages. Policymakers and health sector managers, by accessing data related to these barriers, can formulate and implement evidence-based policies and interventions to enhance individual participation in research. Furthermore, researchers—and particularly patients—who provide their opinions and perspectives to higher authorities for the purpose of increasing research engagement help to advance the development of personalized services. Ultimately, this leads to increased satisfaction among beneficiaries, a greater number of health-related research projects, and, in the long term, an improvement in the overall quality of healthcare services.
Methods
This cross-sectional study was conducted in 2025 using a mixed-methods design, which encompassed two distinct phases: a systematic review methodology and an exploratory qualitative interview approach. In the initial phase, study data were reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines for review studies (Page et al., 2021). In the subsequent phase, data reporting adhered to the Consolidated Criteria for Reporting Qualitative Research (COREQ) Checklist for qualitative research (Tong et al., 2007).
We decided to conduct a systematic review of reviews because numerous review studies on the original research already exist in the literature. Consequently, undertaking additional review studies of original research was considered unnecessary. Instead, providing a comprehensive and synthesized overview of the existing data from these reviews was regarded as highly valuable. Furthermore, we chose to employ qualitative interviews to obtain additional first-hand insights and to update the data by capturing information not addressed in the existing reviews.
Research Questions
The primary research question of this study was: “What are the barriers to beneficiary participation in healthcare research?” Additionally, several secondary research questions were addressed through the analysis of the study data, including: “What are the most frequently cited categories of barriers to beneficiary participation in healthcare research?” and “What solutions exist to overcome the barriers to beneficiary participation in healthcare research?”
Data Collection
Phase One: Systematic Review of Reviews
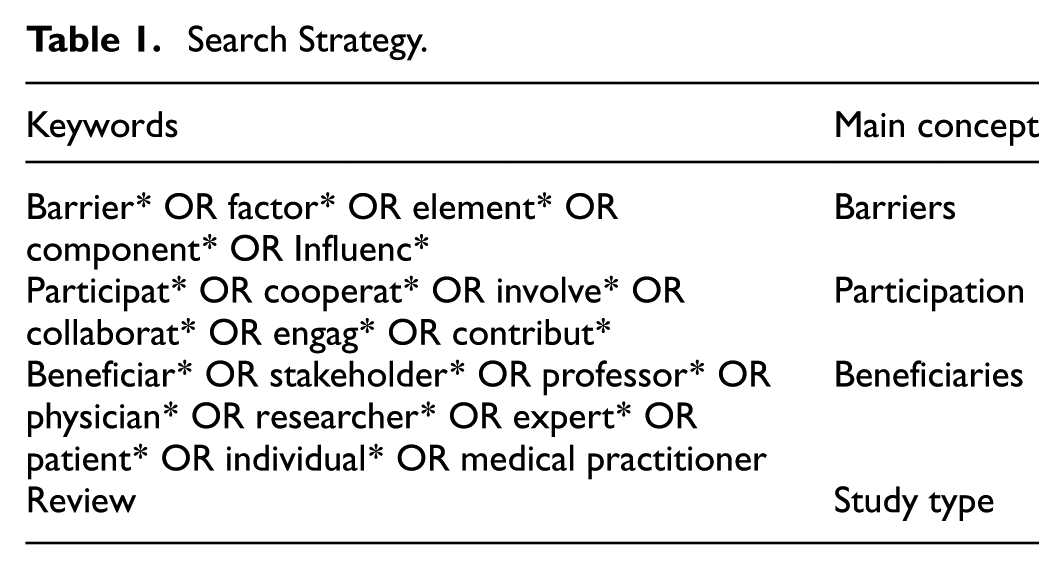
The databases examined included PubMed, Scopus, ProQuest, and the Cochrane Database of Systematic Reviews. The Boolean operators “AND” and “OR” were utilized to enhance the precision and accuracy of the studies retrieved from the search. The default search strategy is presented in Table 1.
Search Strategy.
Inclusion criteria:
Full-text access to English-language articles.
Publication between the years 2000 and 2025.
Publication as a review study.
Qualitative and quantitative studies containing components relevant to the research objectives.
Exclusion criteria:
Conference proceedings, letters to the editor, and protocols.
Inability to access the full text of articles.
Data collection and extraction in this phase were carried out using a pre-designed data collection table in Microsoft Office Word. The table included details such as author names, study title, year of publication, publishing journal, and the inhibiting factors to research participation reported in the study results. During this process, one researcher screened the titles and abstracts of the references obtained from the database searches. After screening for relevant studies, the researcher reviewed the full texts of the remaining studies. Finally, data from the studies that passed the screening stage were recorded in the aforementioned data extraction table. To ensure validity and minimize bias in the data collection process, a second researcher reviewed and verified the accuracy of the data collection.
Phase Two: Exploratory Qualitative Interviews
The second phase of the study was based on conducting a number of unstructured interviews, which were carried out in 2025 at a healthcare university located in Iran. This interview approach was chosen to provide participants with the opportunity to freely express their views regarding the research question. Data collection was guided by the COREQ framework, which was originally published in 2007. This comprehensive checklist, consisting of 32 items, assists researchers in more effectively collecting and reporting data, particularly in interview-based studies (Booth et al., 2014).
The interviews began with a broad question concerning the factors that inhibit the stakeholder participation in research projects. The question was: “Have you previously participated in a health research project? What factors have reduced your willingness or prevented you from participating in research?” Throughout the interview process, efforts were made to allow participants to freely express their opinions so that all relevant challenges could be articulated without restriction. The duration of each conversation varied depending on the participant’s interest in discussing the research questions.
The interviews were conducted in person by one of the researchers, adhering to the ethical principles of qualitative, conversation-based research. In this regard, participant privacy was safeguarded by anonymizing their personal information during the data collection process. Moreover, individuals who were considered to have any conflicts of interest related to the study outcomes were excluded to minimize the risk of bias in the collected data. Informed consent was also obtained from the study participants, and any individual who wished to withdraw from the study at any time was permitted to do so. These measures upheld the ethical standards of the study and helped prevent any potential harm to individuals, particularly the study participants. These measures eliminated any potential risks to the study participants, and, furthermore, the outcomes of the study provided several benefits to the relevant beneficiaries within the context discussed earlier in the article. Consequently, the benefits of the research outweighed any potential harms, even though such harms had already been addressed and mitigated as previously described. Data extraction was performed using a pre-designed table in Microsoft Office Word 2016, which included fields for gender, age, educational level, and the inhibiting factors for research participation. The entire data collection process was carried out by one researcher and subsequently reviewed by another. One researcher was responsible for reviewing and recording the relevant data in the designated table, while another researcher reviewed the process to ensure validity and minimize bias in data collection.
The sample size for the interviews varied according to the point of data saturation. The interview process commenced with two general questions regarding the research objectives, as described previously. Sampling was conducted purposively among faculty members at a healthcare university in Iran. This group of individuals was exclusively included in the study sample, as they represented the primary beneficiaries of research projects within the healthcare context. The inclusion of additional beneficiary groups was precluded due to limitations in the time and resources available to the study researchers.
Inclusion criterion:
Employment as a faculty member at the university.
A minimum of three months’ employment at the university.
Exclusion criterion:
Inability to participate in an in-person interview.
Data Analysis
At this stage of the research, the data collected during both of the study phases were categorized by two researchers simultaneously and independently, using a thematic analysis approach. Any discrepancies between the two researchers during the thematic analysis were resolved through the involvement of a third researcher, who provided the final decision. The thematic analysis was performed using Microsoft Office Word 2016. The factors inhibiting beneficiary participation in research were presented in a single table. The analysis of extracted information was conducted in accordance with the Boyatzis framework (Boyatzis, 1998).
The Boyatzis framework is a structured method for identifying, analyzing, and reporting themes in qualitative data. This framework involved the following key steps: familiarization with the data, generation of initial codes, formation of themes, review of themes, and finally, definition and naming of themes. In this regard, the authors initially familiarized themselves with the data extracted from the texts of the included studies in the review. Subsequently, they generated codes from the data that corresponded to the research question. After thorough analysis of the initial codes, the authors decided to consider these codes as sub-themes. These sub-themes were then categorized according to their context and nature, drawing upon the authors’ analytical expertise. The generated themes were reviewed multiple times to identify and correct any potential issues or misclassifications throughout the process. Finally, the authors named and defined the themes. The Boyatzis framework was particularly effective in studies requiring the integration of qualitative findings, enabling researchers to develop a deeper understanding of participants’ experiences and perspectives by identifying overarching patterns. Furthermore, emphasis on precision in coding, theme development, and maintaining a systematic coding process enhanced the validity and reliability of the qualitative research results (Braun & Clarke, 2024; Hemming et al., 2021; Thomas & Harden, 2008).
To ensure validity and reliability in the thematic analysis, the criteria proposed by Lincoln and Guba were applied. These criteria included credibility, transferability, dependability, and confirmability. The credibility criterion emphasized the accuracy of the findings; in this regard, the study researchers endeavored to ensure that the results genuinely reflected participants’ views and experiences. The transferability criterion referred to the applicability of the findings to other contexts or settings. To address this, researchers provided detailed descriptions of the study context to allow readers to assess the extent to which the results might be applicable to their own circumstances. The dependability criterion involved evaluating the consistency of the data over time and under varying conditions. Accordingly, the researchers carefully documented interview processes to enable others to replicate the study if desired. Finally, the confirmability criterion ensured that the findings were not influenced by the researcher bias. To enhance these qualities, techniques such as triangulation (using multiple data sources or collection methods) and reflexivity (self-reflection regarding research biases) were employed (Guba, 1981; Morse, 2015).
Results
Phase One: Systematic Review of Reviews
The database search retrieved a total of 17,711 references, of which 3,734 were identified as duplicates. Following the removal of duplicates and subsequent screening of the remaining references, 20 review studies were included in the analysis (Figure 1). In this regard, the average publication year of the studies was 2021. The earliest reference dated back to 2002, whereas the most recent was published in 2025.
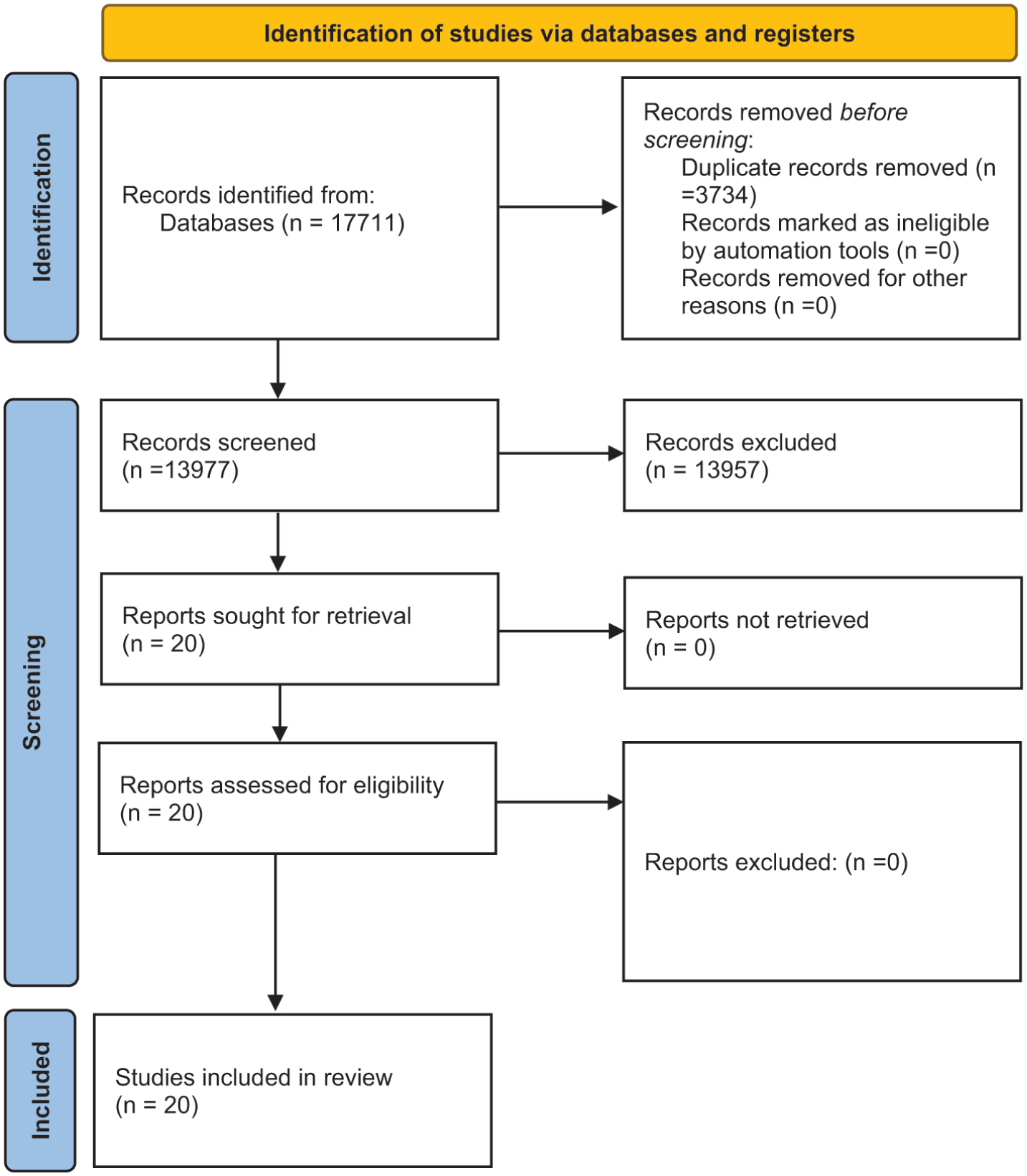
PRISMA flow diagram of the search within the databases.
Phase Two: Exploratory Qualitative Interviews
The study data saturation was achieved after conducting interviews with 17 individuals. The participants comprised individuals holding diverse academic positions. Assistant professors constituted the largest demographic, representing approximately 53% of the sample. This was followed by full professors at 24%, associate professors at 18%, and one individual holding a Master’s degree, accounting for 6%. Regarding gender distribution, females comprised the majority of the sample at approximately 65%, with males representing the remaining 35%. Expertise in health education and promotion accounted for nearly 24% of the participants, environmental health engineering for approximately 18%, cellular medicine for about 12%. The remaining fields of expertise among the study participants included social health and welfare, biotechnology, biological statistics, epidemiology, immunology, mycology, medical parasitology, and medical bacteriology.
Data Analysis
The thematic analysis of the data gathered from the two phases of the study revealed five main themes and 21 sub-themes. These themes included Communication Barriers, Attitudinal Barriers and Motivational Deterrents, Structural and Institutional Challenges, Awareness and Knowledge-Related Challenges, and Research & Methodology-Related Challenges (Table 2).
Thematic Analysis of Data.

Communication Barriers
This theme encompassed obstacles related to the transmission of information and the physical or logistical ability of beneficiaries to participate. The sub-themes included geographical Barriers, Time Constraints, and Cultural and Language Barriers.
Geographical Barriers
The data presented by the literature reported that the participants, especially those from rural or remote areas and individuals with mobility issues, faced considerable logistical challenges in attending meetings or accessing research sites, with greater travel distances correlating to lower retention rates. Factors such as unemployment, housing insecurity, and transportation difficulties further hindered involvement, particularly among caregivers with substance use disorders (Anderst et al., 2020; Corr et al., 2024; Domecq et al., 2014; Gao et al., 2024; Werner et al., 2025; Zibrowski et al., 2021).
Time Constraints
The data presented by the literature revealed that both researchers and participants faced significant challenges that have limited meaningful engagement in healthcare research projects. Researchers frequently encountered competing demands, including heavy clinical workloads, teaching responsibilities, and institutional requirements such as ethics approvals, which often conflicted with the timelines necessary for participatory research. Similarly, participants were burdened by busy personal schedules, including parenting, work commitments, and diverse family obligations, which restricted their availability. The engagement process itself required additional time for activities such as training, meetings, and travel, further increasing the time burden on all parties involved. Limited protected time for research activities, coupled with organizational issues including funding shortages, logistical difficulties, and gatekeeping by institutional boards, compounded these constraints. Insufficient financial, staff, and training resources has also hindered the capacity of both researchers and public partners to participate fully. These time-related challenges led to perceptions of research projects as overly time-consuming and burdensome, contributing to higher withdrawal rates (Anderst et al., 2020; Bowness et al., 2024; Brodeur et al., 2025; Chen et al., 2025; Corr et al., 2024; Domecq et al., 2014; Flynn et al., 2019; Gao et al., 2024; Sahin et al., 2014; Warraitch et al., 2024; Wearn et al., 2025).
The interview data revealed that one of the primary barriers to healthcare researchers’ participation in research projects was the limitation imposed by short project timelines. Participants reported that the durations allocated for their research activities were insufficient, often resulting in barely enough time to complete data collection, with minimal or no opportunity for thorough data analysis. This misalignment between the project timeline and the scope of the research significantly hindered their ability to engage fully and effectively in the research process. In this regard, one participant quoted:
The duration allocated for the research was so short that we barely had time to finish the data collection, let alone analyze it properly. The timeline was simply not aligned with the scope of the project.
Cultural and Language Barriers
The data within the literature revealed that differences in language, cultural norms, and values significantly impeded the recruitment and retention of diverse participants in healthcare research projects. A prominent issue was the linguistic mismatch between researchers and participants, compounded by the scarcity of bilingual staff and translated materials, which limited accessibility and understanding of research goals, procedures, and benefits. Communication gaps were further widened by jargon-heavy explanations and insufficient translation support, fostering misunderstandings and mistrust. The lack of minority researchers, particularly those matching the racial or ethnic backgrounds of participants, intensified suspicion and cultural misalignment, undermining participants’ willingness to engage. Factors, including difficulty accessing culturally relevant recruitment sites and networks, exclusion of underrepresented groups such as disabled or low-income youth, and tokenistic approaches to engagement, also contributed to these barriers (Gao et al., 2024; Khan et al., 2024; Torres & Tajima, 2024; Vincent et al., 2022; Warraitch et al., 2024; Zibrowski et al., 2021).
The interview data presented lack of shared terminology and mutual understanding among reviewers as a significant barrier. In this regard, researchers experienced challenges when their specialized concepts or methodological approaches were not recognized or valued by reviewers, leading to misunderstandings that adversely impacted the evaluation and acceptance of their work. This disconnection hindered effective communication and often resulted in the rejection of articles, ultimately affecting the overall quality and progress of their research contributions. One participant noted:
For example, I say that adding a flexibility factor to the two-stage model has a significant effect, but for the reviewers, this is not a priority at all. This lack of understanding can lead to my articles being rejected, and it severely affects the quality of my research work.
Attitudinal Barriers and Motivational Deterrents
This theme explored the internal perceptions and motivations of beneficiaries that influenced their willingness to participate. The sub-themes included Perceived Risk and Usefulness, Personal Motivation and Interest, and Mistrust and Attitudinal Barriers.
Perceived Risk and Usefulness:
The data derived from the literature highlighted a complex interplay between motivations and concerns influencing beneficiary participation in healthcare research projects. Participants recognized that involvement could lead to improved patient outcomes, enhanced quality of practice, and advancement of the healthcare profession, which served as key motivators. However, financial inequities, such as unpaid or underpaid roles, and insufficient compensation presented significant deterrents. Among clinicians and researchers, skepticism about consumer involvement was prevalent; some viewed it as politicizing the process or undermining professional expertise, expressing concern that participant input might challenge the legitimacy of professional knowledge. Perceived risks also included fears of physical harm or unknown consequences from experimental interventions, alongside broader suspicions regarding research motives and potential misuse of data. Gatekeepers—such as institutional or clinical authorities—sometimes prioritized their own workload or preferences over participant interests, further restricting access. Additionally, financial disincentives and the absence of tangible benefits or incentives for participants contributed to reluctance. Specific populations, such as individuals with intellectual and developmental disabilities (IDD), were often presumed incapable of consenting or benefiting from research, resulting in exclusion (Boote et al., 2002; Brodeur et al., 2025; Domecq et al., 2014; Gao et al., 2024; Limkakeng et al., 2014; Matheson et al., 2025; Sahin et al., 2014; Torres & Tajima, 2024; Zibrowski et al., 2021).
The interview data highlighted concerns among healthcare researchers regarding their personal credibility, reputation, and academic standing as barriers to participation in research projects. Some researchers were cautious about endorsing work they did not fully understand, fearing potential damage to their professional reputation. Additionally, there was a perception among certain colleagues that research could be exploited for personal financial gain or treated as a business, which was met with disapproval by others who valued research integrity over profit. These attitudes collectively influenced researchers’ willingness to engage fully in projects. One participant remarked:
I told, if I don’t approve this, it’s because I don’t want to risk my reputation. I can’t approve something I don’t know well.
Another participant also stated:
Some colleagues see research as a business and try to profit from it. This approach might be useful for some, but personally, I don’t agree with it.
Personal Motivation and Interest
Intrinsic motivation, including a genuine curiosity about research and an interest in scientific inquiry, was identified within the literature as a strong driver for engagement. Participants who possessed personal interest and enthusiasm for research were more likely to commit and contribute meaningfully. However, motivational deterrents were notable, particularly the lack of robust peer support and research networks, which fostered feelings of isolation and reduced collaborative opportunities. Variations in participants’ skills and training needs, especially among adolescents with competing priorities such as school, also affected motivation. Additionally, emotional burdens related to participating in sensitive research topics sometimes discouraged sustained involvement. Limited prior exposure to research concepts often resulted in hesitation or disinterest, highlighting the importance of education and familiarization to build motivation. These findings align with broader evidence indicating that intrinsic, altruistic, and intellectual motivations significantly influence research participation, while absence of community support and perceived emotional costs can undermine it (Chen et al., 2025; Matheson et al., 2025; Sahin et al., 2014; Torres & Tajima, 2024; Warraitch et al., 2024; Wearn et al., 2025; Zibrowski et al., 2021).
The interview data demonstrated that low motivation among healthcare researchers was a significant barrier to their participation in research projects, primarily due to the absence of effective incentives or recognition systems. Researchers expressed frustration over the lack of feedback or acknowledgment from their departments, which diminished the perceived value of their work and consequently dampened their motivation. Furthermore, the need for continuous professional development and self-empowerment was emphasized, as researchers struggled with inadequate access to workshops and training sessions necessary to keep pace with evolving research methodologies. Additionally, a tendency to prioritize individual goals over collective academic advancement was noted, with some colleagues focusing predominantly on personal publications and promotions rather than collaborative efforts or shared progress. In this regard, one participant quoted:
When I publish something, there’s no feedback or recognition from the department. It feels like my work doesn’t matter, and that kills my motivation.
Another participant stated:
I often feel like I’m lagging behind. There are no proper workshops or training sessions, and it’s hard to keep up with new research methods.
Another participant narrated:
Some colleagues only care about their own publications and promotion. There’s no real interest in collaborative work or shared progress.
Mistrust and Attitudinal Barriers
According to the literature, a pervasive mutual distrust existed between advocates and researchers, often fueled by perceptions that researchers disregarded participants’ input or priorities, leading to frustration and disengagement. Historical and socio-political factors, notably within minority and underserved communities, contributed significantly to pervasive skepticism toward research motives and fears of exploitation or misuse of data. Participants frequently expressed concerns about being treated as “guinea pigs” and questioned the legitimacy of researchers’ intentions, which was compounded by feelings of being marginalized as “guest researchers” or token participants, further eroding trust and confidence. The role of gatekeepers and institutional actors sometimes manifested in dismissive or negative attitudes toward public partners, undermining mutual respect and collaborative relationships. Additionally, high staff turnover disrupted continuity, impairing trust-building efforts over time. Emotional burnout from repeatedly sharing lived experiences diminished willingness to engage, while tokenistic engagement approaches devalued patient contributions and deepened mistrust. These dynamics resulted in a lack of genuine collaboration, with some participation driven instrumentally by access to healthcare rather than authentic partnership. This complex interplay of distrust, skepticism, and attitudinal barriers significantly limited equitable research participation and underscored the need for intentional strategies to foster respect, transparent communication, sustained relationship-building, and culturally sensitive engagement to rebuild trust and enhance inclusivity in healthcare research (Baralt & McCormick, 2010; Brodeur et al., 2025; Domecq et al., 2014; Flynn et al., 2019; Khan et al., 2024; Limkakeng et al., 2014; Matheson et al., 2025; Torres & Tajima, 2024; Vincent et al., 2022; Wearn et al., 2025; Werner et al., 2025; Zibrowski et al., 2021).
The interview data indicated that discouragement caused by low peer engagement and lack of support represented a significant barrier to the participation of healthcare researchers in research projects. Multiple participants experienced emotional distress, including feelings of discouragement, frustration, and a diminished sense of self-worth, often intensified by interpersonal conflicts and personality differences among colleagues. These challenges were compounded by a lack of attentive communication, with some researchers describing instances where their contributions were met with indifference or opposition from peers, further undermining their sense of value within the research environment. Such dynamics not only created emotional obstacles but also hindered collaborative interactions essential for productive research work. One Participant described his experiences as follows:
This is very discouraging and I feel that my work is not properly valued, and this is problematic for me.
Another participant remarked:
One reason I couldn’t connect well with some colleagues was our personality and attitude differences. When I present an idea and feel I face opposition, it becomes very heavy and strange for me.
A third participant shared:
For example, imagine I am explaining a formula, and my colleague in his office is silent and pays no attention to my words. This is very discouraging.
Structural and Institutional Challenges
This theme highlighted systemic issues within research institutions and policies that hindered beneficiary involvement. The sub-themes included Lack of Clear Policies and Guidelines, Underreporting and Poor Evaluation, Logistical Challenges, Lack of Resources, Rigid and Unsupportive Institutions, and Weak Leadership Support.
Lack of Clear Policies and Guidelines
Many organizations lacked explicit policies or strategic frameworks to support effective consumer involvement, resulting in limited guidance or established best practice standards for engagement. This absence of clarity extended to unclear role definitions and expectations for public partners, which often led to confusion, frustration, and dissatisfaction, as exemplified by early projects like the Long Island Breast Cancer Study Project. Institutional constraints—including bureaucratic hurdles, rigid protocols, and insufficient training for both researchers and participants—further complicated efforts to organize and sustain participatory activities. Restrictive policies notably excluded certain groups, such as individuals with intellectual and developmental disabilities, from research opportunities, undermining inclusivity. Additionally, the absence of systematic evaluation of consumer involvement policies created uncertainty about their effectiveness and hindered continuous improvement. Transparency deficits in decision-making and unresolved power hierarchies between academic and patient partners weakened trust and collaboration. The scarcity of mentorship and guidance limited participants’ capacity to contribute meaningfully throughout research design, execution, and dissemination (Anderst et al., 2020; Baralt & McCormick, 2010; Boote et al., 2002; Brodeur et al., 2025; Chen et al., 2025; Gao et al., 2024; Matheson et al., 2025; Wearn et al., 2025; Werner et al., 2025; Zibrowski et al., 2021).
The interview data revealed that conflicting regulations regarding teamwork and authorship contributions posed a considerable barrier to healthcare researchers’ participation in research projects. Researchers expressed confusion and frustration over discrepancies between official policies promoting teamwork and the practical realities of authorship credit and performance evaluations. For example, although teamwork was encouraged in principle, the existing point allocation system penalized projects with multiple authors by distributing fewer points per author, thereby discouraging collaborative efforts. This inconsistency between regulations and evaluation criteria led to difficulties in advancing research and fostered a climate where individuals prioritized personal interests over collective progress. A participant articulated these challenges by stating:
When I reach the research deputy, I don’t understand the priorities. Disclosing the model or theory I present doesn’t seem to matter much, and this causes me trouble.
Another participant noted:
There are contradictions in the regulations related to teamwork. For example, while it is claimed that teamwork is important, in the calculation of points, the more authors there are, the fewer points each author receives.
A third participant quoted:
The contradictions in regulations and evaluation systems make progress in research and universities difficult, and people think more about their own interests.
Underreporting and Poor Evaluation
Many research publications failed to explicitly report consumer and community engagement (CCE) activities, partly due to a lack of formal requirements from journals, resulting in underrepresentation of engagement efforts in the literature. Furthermore, there was a notable absence of ongoing, systematic evaluation of the collaborative processes themselves, limiting the ability to identify challenges and improve engagement practices in real time. Where reporting did occur, it was often of poor quality, characterized by minimal measurement of engagement impact and inconsistent documentation. These deficiencies were exacerbated by the complexity and burden of data collection and reporting requirements, which discouraged comprehensive evaluation. The lack of robust evaluation mechanisms hindered the understanding of how consumer engagement influences research quality, relevance, and outcomes (Anderst et al., 2020; Baralt & McCormick, 2010; Domecq et al., 2014; Sahin et al., 2014).
The interview data highlighted that ineffective, non-transparent, and potentially biased evaluation systems were significant barriers to healthcare researchers’ participation in research projects. Researchers expressed confusion and dissatisfaction regarding the criteria used for promotions and assessments, observing that high-quality research efforts often received low scores, while others advanced without commensurate work. This perceived lack of clarity and fairness in evaluation processes undermined researchers’ trust in the system and negatively impacted their motivation and engagement. One participant encapsulated this experience by stating:
Sometimes I don’t even understand based on what criteria people get promoted. You do quality research and still get low scores, while others get ahead without serious work.
Logistical Challenges
Participants experienced difficulties attending meetings and accessing research sites due to limited transportation options, and mobility issues. Studies consistently identified lack of local infrastructure, and workforce shortages created significant obstacles, often leading to lower enrollment and retention rates among rural populations. Additional logistical barriers included the complexity and time demands associated with multiple site-specific approvals and fragmented governance frameworks, which delayed research initiation and continuity. Rural residents also faced social stigma and privacy concerns in small communities, deterring engagement in sensitive health research. Structural issues such as inadequate organizational support, lack of digital infrastructure, and limited integration of research activities within primary care further restricted access (Anderst et al., 2020; Domecq et al., 2014; Khan et al., 2024).
The interview data indicated that overly complex and time-consuming ethical approval processes, combined with administrative errors and poor managerial decision-making, significantly hindered healthcare researchers’ participation in research projects. Researchers described the ethics approval procedures as complicated and prolonged, creating substantial delays that impeded timely progress. This complexity was exacerbated by administrative mistakes and ineffective management judgments which not only wasted valuable time but also jeopardized the success of entire projects and institutions. One participant specifically highlighted the issue, stating:
For my field, we need an ethics code, but this process is very complicated and time-consuming,
Another participant quoted:
We spent 3 or 4 months on this project, and in the end, our university was deprived due to managerial mistakes.
Lack of Resources
The literature underscored that lack of time, funding, and organizational support critically hindered meaningful consumer and researcher participation in healthcare research projects. Both researchers and participants faced significant time constraints, with competing clinical, teaching, and personal responsibilities limiting availability for engagement activities. Funding shortages were pervasive, restricting the ability to sustain participatory efforts, provide adequate compensation, and cover necessary training or logistical costs. Institutional challenges—including bureaucratic gatekeeping, limited staff, and inadequate infrastructure—further exacerbated these issues, creating obstacles particularly notable when attempting to involve specific populations such as adolescents or underrepresented groups. Resource deficiencies also contributed to power imbalances, with insufficient investment in public partner support undermining meaningful involvement. Busy personal schedules, including parenting and work commitments, alongside perceptions of research as too time-consuming or burdensome, led to higher withdrawal rates. Moreover, weak leadership support and underfunded health systems limited the capacity to build a robust culture of engagement (Anderst et al., 2020; Bowness et al., 2024; Brodeur et al., 2025; Chen et al., 2025; Corr et al., 2024; Domecq et al., 2014; Flynn et al., 2019; Gao et al., 2024; Khan et al., 2024; Matheson et al., 2025; Torres & Tajima, 2024; Vincent et al., 2022; Warraitch et al., 2024; Wearn et al., 2025; Werner et al., 2025).
The interview data underscored several financial and resource-related barriers impeding healthcare researchers’ participation in research projects, notably limited access to data and resources due to international sanctions, insufficient institutional funding, inadequate financial compensation for specialized academic work, and overall limited financial resources for research-related expenditures. Researchers reported feeling undervalued, as their analytical and specialized work, such as programming and questionnaire design, often lacked appropriate financial support or recognition. The sanctions exacerbated isolation, forcing some researchers to work independently without collaboration or access to laboratory resources. Further, disparities in funding and compensation were highlighted, with some colleagues receiving fractional support while others received none, adding to perceived inequities. Participants expressed frustration that these financial constraints diminished the perceived worth of their contributions and hindered research productivity. One participant quoted:
As my work is analytical, I have to work alone in my office, and the costs related to my work are not properly covered. I feel that my work is not properly valued, and this is problematic for me,
Another participant stated:
Due to sanctions, access to data and resources is limited. I don’t collaborate with anyone working in the lab, and the nature of my work is such that I have to research alone.
Rigid and Unsupportive Institutions
The literature reported that even in projects with formal structures, such as the Breast Cancer and the Environment Research Centers (BCERCs), advocates and public partners were often excluded from early research design and key decision-making processes, reflecting persistent hierarchies between academic researchers and patient communities. Institutional environments were characterized by inflexible academic and administrative formats, rigid protocols, and bureaucratic hurdles that constrained adaptability and responsiveness to community input. These structural inequalities were compounded when external funders controlled research agendas, reducing local ownership and relevance. Unsupportive institutional cultures frequently failed to provide adequate organizational backing, resources, and infrastructure necessary to facilitate participatory research activities. Negative attitudes within institutions and poorly addressed power imbalances further marginalized consumer voices (Baralt & McCormick, 2010; Bowness et al., 2024; Khan et al., 2024; Matheson et al., 2025; Vincent et al., 2022; Zibrowski et al., 2021).
The interview data identified institutional undervaluation and a lack of recognition for research activities as critical barriers to healthcare researchers’ engagement in research projects. Researchers reported that teaching and administrative duties received more acknowledgment and prestige than scientific research, leading to feelings that their scholarly work was underappreciated. Furthermore, the scoring systems used for performance evaluations discouraged collaborative efforts, as shared authorship in multi-author publications resulted in reduced individual scores. This punitive approach to teamwork impeded collaboration, with some researchers preferring to work alone to maximize their evaluation outcomes. One participant expressed this dilemma:
There’s more recognition for teaching or administrative duties than for actual research. It makes you feel your scientific work is not valued,
Another participant noted:
I often avoid collaborating with others because shared authorship reduces my score in evaluations. It’s just not worth the cost.
Weak Leadership Support
The literature revealed that a lack of strong institutional backing significantly hampered resource allocation and the development of a supportive culture for healthcare research and engagement activities. Leadership challenges included insufficient commitment from institutional leaders, bureaucratic hurdles, and rigid organizational protocols that limited flexibility and responsiveness to participatory research needs. The absence of robust mentorship and professional networks further constrained confidence-building and skill development among researchers and public partners. Effective leadership was identified as crucial for fostering a collaborative environment, securing adequate resources, and overcoming structural barriers in healthcare settings. Studies underscore that well-trained, supported leaders who foster open communication, teamwork, and shared decision-making can enhance workforce capacity, reduce turnover, and align organizational efforts toward inclusive engagement. However, inadequate leadership development and weak executive support remain persistent obstacles, impeding progress and limiting meaningful participation (Chen et al., 2025; Gao et al., 2024; Matheson et al., 2025).
The interview data revealed that the participation of healthcare researchers in research projects was hindered by the use of non-expert reviewers and superficial, hierarchical peer review mechanisms. Researchers reported that reviewers were sometimes not from their specific field, leading to misjudgment of the core ideas and a focus on irrelevant details rather than substantive evaluation. Additionally, the peer review process was occasionally described as perfunctory, conducted merely to fulfill procedural requirements without genuine engagement with the research content. These shortcomings undermined the quality of peer assessments and impeded fair recognition of research contributions. One participant stated:
Sometimes the reviewer doesn’t even belong to the same field. They miss the core idea completely and focus on irrelevant points.
Another participant noted:
Sometimes reviews are done just to check a box. There’s no in-depth engagement with the research content.
Awareness and Knowledge-Related Challenges
This theme addressed the lack of understanding and preparedness among beneficiaries and researchers regarding research processes and engagement. The sub-themes included Lack of Research Skills and Competencies, Limited Training, Limited Awareness and Preparation, and Differences in Paradigms.
Lack of Research Skills and Competencies
The literature reported that many professionals reported feeling insufficiently trained and lacking confidence in research methodologies, which limited their engagement in research projects and reduced their ability to contribute effectively. This lack of familiarity with research processes extended to public partners as well, with some feeling unprepared to participate fully without adequate training and support. Studies highlighted that limited research knowledge, skill deficits, and inadequate institutional training opportunities undermine professionals’ research involvement and capacity-building efforts. Additional barriers tied to this included insufficient mentorship, limited access to statistical expertise, and uncertainties navigating ethics and regulatory procedures. Conversely, positive attitudes toward research and motivation to develop skills were identified as enablers, especially when supported by organizational culture and mentorship programs (Brodeur et al., 2025; Chen et al., 2025; Sahin et al., 2014; Torres & Tajima, 2024; Wearn et al., 2025).
The interview data indicated that a lack of adequate training in research design and methodologies was a significant barrier preventing healthcare researchers from effectively engaging in research projects. Researchers reported insufficient mastery of essential research models and statistical concepts, which hampered their ability to plan, conduct, and analyze studies confidently. This gap in skills and knowledge underscored the need for targeted educational programs and workshops. For instance, one participant admitted:
I don’t have much mastery over models and statistical issues.
Limited Training
Many advocates possessed insufficient scientific training, which undermined their confidence and ability to engage fully in technical discussions, limiting their influence and contribution to research processes. Similarly, researchers often expressed frustration over advocates’ lack of familiarity with research methods, which hindered effective communication and collaboration. The burden of training, combined with logistical challenges such as transportation and attendance requirements, further impeded advocates’ involvement. Additionally, inadequate orientation and preparation for patients and families restricted their effective participation. The scarcity of mentorship and guidance compounded these challenges, leaving advocates without essential support to navigate research design, execution, and dissemination. Research also highlighted insufficient training for researchers in participatory methods and cultural humility, which adversely impacted mutual understanding and engagement quality. Furthermore, poor reporting transparency regarding participatory methods diminished accountability and learning opportunities (Baralt & McCormick, 2010; Bowness et al., 2024; Chen et al., 2025; Domecq et al., 2014; Flynn et al., 2019; Khan et al., 2024; Zibrowski et al., 2021).
The interview data presented that healthcare researchers experienced significant challenges when required to adapt to interdisciplinary or non-laboratory research formats. Individuals with strong laboratory-based backgrounds often felt uncomfortable and uncertain about their roles in conceptual or cross-disciplinary projects, which differ markedly from familiar laboratory environments. This discomfort inhibited their confidence and willingness to contribute, highlighting a need for targeted support and skill development to facilitate smoother transitions into diverse research settings. One participant reflected this barrier by stating:
My background is very lab-based, so when it comes to conceptual or interdisciplinary research, I often feel out of place and unsure how to contribute.
Limited Awareness and Preparation
The literature revealed that a pervasive lack of knowledge and understanding among researchers, gatekeepers, and potential participants significantly hindered effective consumer and community engagement (CCE) in healthcare research. Many researchers were unaware of the benefits of CCE or uncertain about how to engage consumers meaningfully, while gatekeepers often lacked sufficient information about research projects or the capabilities of prospective participants. Misconceptions and misinformation about research risks, especially regarding vulnerable groups such as individuals with intellectual and developmental disabilities (IDD), further impeded participation. Many members of communities, including the Fanconi Anemia (FA) community, were unfamiliar with research processes and the potential advantages of involvement. Poor communication, inconsistent terminology (e.g., patient engagement, participation, involvement), and unclear roles and expectations generated confusion and mistrust. Insufficient training and orientation for patients and families limited their readiness to contribute effectively. This lack of clarity often reduced participants to token roles rather than genuine co-researchers involved throughout all research phases (Anderst et al., 2020; Boote et al., 2002; Brodeur et al., 2025; Flynn et al., 2019; Gao et al., 2024; Torres & Tajima, 2024; Warraitch et al., 2024; Werner et al., 2025).
The interview data presented that insufficient rationale and strategic planning in research proposals was a major barrier affecting healthcare researchers’ participation in projects. Many proposals were reported to be hastily prepared solely to meet submission deadlines, lacking clear justification, coherent research questions, or well-defined strategic directions. This rushed approach resulted in proposals that failed to adequately articulate the significance or purpose of the research, often missing essential elements such as focused problem statements, sound methodology, and meaningful objectives. Such deficiencies diminished the proposals’ quality and chances of approval, ultimately impeding researchers’ ability to secure funding and support. One participant summarized this challenge by stating:
Many proposals are written in a hurry, just to submit something before the deadline. There’s often no clear rationale or strategic direction.
Differences in Paradigms
The literature highlighted fundamental disparities between advocates and scientists regarding the scientific inquiry process, research priorities, and desired outcomes, which posed significant challenges to effective collaboration in healthcare research. Researchers typically concentrated on biomedical and epidemiological data, aiming to advance scientific knowledge, while advocates emphasized broader public health outcomes and policy changes that directly impacted their communities. These divergent perspectives often resulted in misunderstandings and frustration on both sides, as patients raised concerns and priorities that were personally or community-relevant but not always aligned with the scientific goals or feasibility of the research. This misalignment occasionally led to scope creep, where the inclusion of community issues extended beyond the original research objectives, potentially rendering studies impractical or unmanageable. Balancing patient priorities with the constraints and aims of rigorous scientific inquiry remained a persistent challenge, underscoring the need for transparent communication, mutual respect, and negotiation to integrate diverse perspectives effectively (Baralt & McCormick, 2010; Domecq et al., 2014; Flynn et al., 2019; Vincent et al., 2022).
The interview data presented that healthcare researchers faced difficulty in establishing meaningful and sustainable collaborations due to the absence of institutional structures that support long-term teamwork. While researchers might collaborate on isolated occasions, there were no mechanisms or frameworks in place to maintain and nurture ongoing collaborative relationships. This lack of sustained partnership limited opportunities for collective advancement and continuity in research efforts. One participant expressed this challenge succinctly:
There’s no structure that supports long-term collaboration. We might work together once, but there’s nothing to keep the team going.
Research and Methodology-Related Challenges
This theme focused on issues inherent within the research design and ethical considerations that created barriers. The sub-themes included Research Ethical Concerns, Methodological Barriers, Power Imbalance, Risk of Tokenism, and Ineligibility and Recruitment Challenges.
Research Ethical Concerns
The literature highlighted multiple challenges when involving vulnerable populations, such as children, adolescents, and socially disadvantaged groups, in healthcare research. Ethical issues included power imbalances between researchers and participants, risks to confidentiality, and safeguarding participant safety, particularly regarding emotional distress. Ensuring informed consent proved difficult, especially in time-sensitive or emergency contexts, raising doubts about participants’ autonomy and true understanding of research implications. Additionally, concerns about data privacy, potential misuse, and ethical compromises—such as the suppression of discussions on systemic inequities to maintain research flow—further deterred participation. Vulnerable populations often face heightened risks due to social and structural determinants, necessitating a delicate balance between protecting participants and ensuring equitable inclusion. Ethical guidelines emphasize that vulnerable groups should not be excluded solely because of their status; rather, fair inclusion based on scientific rationale and appropriate safeguards is essential. Researchers must navigate competing ethical principles—respect for persons, beneficence, and justice—while addressing contextual factors influencing vulnerability. Moreover, public involvement with vulnerable groups requires transparent communication, accessible information, and mitigation of burden to empower rather than exploit participants (Flynn et al., 2019; Gao et al., 2024; Limkakeng et al., 2014; Vincent et al., 2022).
Methodological Barriers
The literature presented traditional methodologies, which often prioritize biomedical and epidemiological data collection, can be difficult to reconcile with the inclusive, collaborative principles central to participatory research. Integrating consumer perspectives introduced epistemological challenges that required rethinking knowledge production and validation processes to accommodate diverse stakeholder inputs meaningfully. Recruitment and retention complexities were common, especially when attempting to ensure inclusivity of marginalized or hard-to-reach groups. Participatory research demands flexibility in method selection and design, as collaborative decision-making between researchers and community partners influences every phase of the research cycle—from defining research questions to data collection and dissemination—allowing methods to be tailored to the priorities and contexts of all stakeholders. These methodological adaptations are critical but time-intensive and require negotiating differing expectations and power dynamics (Boote et al., 2002; Bowness et al., 2024; Warraitch et al., 2024).
Power Imbalance
Despite formal participatory frameworks, power sharing is often limited, with researchers retaining predominant control over core aspects such as research questions, methodology, and decision-making processes. This imbalance fosters feelings among participants of being undervalued, ignored, or tokenized, especially for vulnerable groups like children or marginalized communities. The shift toward involving consumers represents a challenge to traditional hierarchies, often resisted by professionals accustomed to entrenched academic authority. Historical and structural inequities, including wealth disparities and colonial legacies, further exacerbate these power differentials, reinforcing marginalization and exclusion (Anderst et al., 2020; Baralt & McCormick, 2010; Boote et al., 2002; Bowness et al., 2024; Flynn et al., 2019; Vincent et al., 2022; Warraitch et al., 2024; Wearn et al., 2025; Werner et al., 2025; Zibrowski et al., 2021).
The interview data presented that pressure to approve or support research proposals based on personal relationships constituted a notable barrier amidst healthcare researchers. Participants described how decisions were sometimes influenced by friendships or social closeness rather than objective evaluation, leading to preferential treatment or biased support. The relational dynamic created sensitivities and ethical dilemmas, wherein researchers felt compelled to adjust their judgments to benefit acquaintances, which compromised the fairness and integrity of the review process. One participant explained:
Unfortunately, it’s become very relationship-based. For example, someone is my friend, you have to be close. Sometimes you become close to certain people and become sensitive. That’s how it is.
Another reflected on the ethical tension:
A colleague called and said, for example, give this a minor revision, do something, but don’t reject it so they can pass. Honestly, I did this for the student. I did this. But for a close colleague, for example, for promotion, I didn’t do this.
Risk of Tokenism
The literature revealed a significant challenge in consumer and community engagement within healthcare research, where involvement is often perceived as superficial or symbolic rather than meaningful and influential. Many researchers expressed concerns that consumer participation might be reduced to a formality without genuine decision-making power, leading to patient input being undervalued and dismissed. This tokenistic engagement undermines trust between researchers and participants, diminishes motivation, and compromises the quality and relevance of research outcomes. Tokenism manifests as inclusion for appearance’s sake, lacking substantive influence on research design, implementation, or dissemination. Such practices risk alienating participants and perpetuating disillusionment with the research process, particularly among marginalized or vulnerable groups (Anderst et al., 2020; Domecq et al., 2014; Flynn et al., 2019; Khan et al., 2024; Warraitch et al., 2024; Wearn et al., 2025; Zibrowski et al., 2021).
Ineligibility and Recruitment Challenges
The literature revealed multifaceted and persistent barriers that impede effective and inclusive participant enrollment, especially among underrepresented populations such as Fanconi Anemia (FA) communities. Recruitment processes are often lengthy, demanding, and can lead to patient frustration, particularly when frequent or invasive visits, rigid eligibility criteria, and inflexible protocols increase participant burden. Geographic dispersion and lack of targeted outreach contribute to the underrepresentation of FA and other rare disease communities, while stigma and misconceptions—such as assumptions about cognitive impairment in psychiatric populations—further undermine engagement. Studies frequently rely on convenience sampling rather than systematic or randomized approaches, which may limit diversity and generalizability. Recruitment efforts often prioritize meeting short-term enrollment targets over building equitable, trusting partnerships, resulting in exclusion of key stakeholders like careers from crucial stages of research. Access barriers, including the absence of safe and inclusive environments and ineffective outreach methods, particularly affect hard-to-reach groups (Bowness et al., 2024; Corr et al., 2024; Domecq et al., 2014; Khan et al., 2024; Torres & Tajima, 2024; Vincent et al., 2022; Werner et al., 2025; Zibrowski et al., 2021).
Discussion
As outlined in the preceding section, the study’s findings were categorized into several overarching themes. These themes encompassed Communication Barriers, Attitudinal Barriers and Motivational Deterrents, Structural and Institutional Challenges, Awareness and Knowledge-Related Challenges, and Research and Methodology-Related Challenges. Notably, Structural and Institutional Challenges, comprised the greatest number of sub-themes. In contrast, Communication Barriers and Attitudinal Barriers and Motivational Deterrents contained the fewest sub-themes.
Comparing the study findings with the TDF, a theory that was introduced and described in detail in the initial section of this study, revealed that several barriers identified in the research aligned with the domains of the framework. In this regard, barriers such as communication challenges (including geographical, temporal, and cultural/language factors), attitudinal and motivational deterrents (such as perceived risk, personal motivation, and mistrust), structural and institutional obstacles (including lack of clear policies, limited resources, and inadequate leadership support), deficiencies in awareness and knowledge (limited research skills, training, and preparation), and concerns related to research methodology (ethical issues, power imbalances, and recruitment difficulties), correspond closely with the key domains of the TDF. These include Environmental Context and Resources, Social Influences, Knowledge and Skills, Beliefs about Consequences and Emotion, and Behavioral Regulation. The thematic analysis further highlighted geographical barriers and nuanced social justice issues, such as tokenism and power imbalances, with greater specificity than the broader categories encompassed by the TDF. Overall, while the thematic findings provided more detailed and context-specific insights, they remain broadly consistent with the psychosocial constructs and behavioral determinants outlined in the TDF (Zhou et al., 2024). This presents the pivotal role of psychosocial constructs and behavioral determinants in influencing the participation of beneficiaries in healthcare research projects.
The study findings indicated that the interview data corroborated approximately 77% of the information reported in previously published studies within the literature. This underscores the positive impact of conducting the interview phase subsequent to the initial review of existing literature. In such context. the interviews provided more localized data that is specifically relevant to the context of the study’s beneficiaries. In this regard, Structural and Institutional Challenges were cited more frequently by the study participants, whereas Communication Barriers and Research- and Methodology-Related Challenges were less commonly reported. These findings provide valuable insights for beneficiaries within the local context of the study as well as in comparable international settings.
Although multiple reviews had examined the factors influencing individuals’ participation in healthcare research projects, the existing literature provides comparatively less information on the barriers to such participation than on the facilitators (Brandon & Bagnall, 2024; Dobra et al., 2023; Matheson et al., 2025; Ross et al., 1999). Accordingly, our study, which solely focused specifically on identifying the barriers to participation among beneficiaries using a detailed approach, offered significant insights on this subject that have not been extensively addressed in previous research.
As demonstrated by the study findings, Structural and Institutional Challenges emerged as the most frequently cited barriers inhibiting beneficiaries’ participation in healthcare projects. This underscores the significance of this category of barriers, which warrants thorough examination. Accordingly, this section of the study is dedicated to a detailed discussion of the challenges related to this theme. Such analysis provides valuable insights for stakeholders—including healthcare policymakers, administrators, and researchers—who seek to enhance individual participation in healthcare research projects. In this regard, the study results highlighted that managerial and organizational issues constitute the primary obstacles to such participation, and that addressing Structural and Institutional factors has the potential to substantially improve the engagement in healthcare research initiatives.
Consistent with the findings of our study, existing literature on the establishment of public and patient panels for research in organizational science and management principles within healthcare highlights the pivotal role of management expertise. Specifically, management proficiency facilitates member recruitment, sustains active involvement, and supports the co-production of charters that ensure participant engagement throughout all stages of the research process (Harnett et al., 2022). In such context, management creates enabling conditions that foster participation, such as cultivating supportive practice environments and securing understanding and backing from leaders and colleagues. Healthcare professionals engaged in research acquire enhanced confidence and knowledge, thereby contributing meaningfully to both research endeavors and the advancement of practice (Laustsen et al., 2021). Researchers’ project management experience improved organization, communication, and collaboration, ensuring timely completion and goal achievement, thereby indirectly enhancing participant involvement through a more cohesive research environment (Payne et al., 2011). Furthermore, collaborative efforts between healthcare managers and researchers serve to augment the relevance, quality, and capacity of research by capitalizing on managers’ contextual insights, optimizing recruitment strategies, and improving dissemination mechanisms. This collaboration, grounded in management expertise, effectively bridges the gap between research and practice, thereby enhancing the overall efficacy of participant engagement (Bullock et al., 2012).
Several key measures have been proposed to enhance management science knowledge in healthcare research centers. Creating a supportive organizational culture is essential for facilitating knowledge sharing, learning, and adaptation. Aligning organizational structure by clarifying roles related to knowledge processes improves knowledge flow and management effectiveness. Regular performance evaluations and the effective use of information technology systems also strengthen knowledge management through efficient storage, retrieval, and dissemination of information (Ayatollahi & Zeraatkar, 2020).
The organization of training programs and professional development activities aimed at enhancing knowledge management competencies among healthcare managers and researchers has been identified as a crucial strategy (Bonfim et al., 2023; Karsikas et al., 2022). Additionally, the effective management of human resources and capital within health research centers is recognized as essential (Amiri et al., 2016). Moreover, the application of multifaceted implementation strategies—including educational meetings, dissemination of materials, reminders, academic detailing, and audit with feedback—has been demonstrated to effectively facilitate the adoption of knowledge products and management guidelines in both clinical and research environments (Uwizeye et al., 2022).
As identified in the study findings, attitudinal barriers and motivational deterrents constituted a significant group of obstacles impeding beneficiary participation in healthcare research projects. These included perceived risk and doubts regarding the usefulness of the research, levels of personal motivation and interest, as well as mistrust and various attitudinal reservations held by potential participants (Boote et al., 2002; Brodeur et al., 2025; Chen et al., 2025; Domecq et al., 2014; Gao et al., 2024; Limkakeng et al., 2014; Matheson et al., 2025; Sahin et al., 2014; Torres & Tajima, 2024; Warraitch et al., 2024; Wearn et al., 2025; Zibrowski et al., 2021). In this regard, it is presented that addressing ethical concerns and implementing rigorous research governance are essential for fostering participant confidence and alleviating fears (McElfish et al., 2019). Promoting positive attitudes through transparent communication about the benefits and risks associated with participation is crucial to mitigating perceived risks and skepticism about the research’s value (Matheson et al., 2025). Furthermore, enhancing transparency and cultivating trust by sharing study results with participants effectively addresses mistrust and related attitudinal barriers (McElfish et al., 2019). Providing targeted education and training serves to improve participants’ understanding, motivation, and engagement in the research process (Gholipour et al., 2023). Finally, the provision of appropriate incentives and resources can further diminish obstacles and encourage greater participation (Bakken et al., 2009).
Another category of barriers affecting beneficiary participation in healthcare research projects, as identified in the study findings, pertains to challenges related to research and methodology. These include ethical concerns surrounding research conduct, methodological obstacles, power imbalances, risks of tokenism, and difficulties associated with participant eligibility and recruitment (Anderst et al., 2020; Baralt & McCormick, 2010; Boote et al., 2002; Bowness et al., 2024; Corr et al., 2024; Domecq et al., 2014; Flynn et al., 2019; Gao et al., 2024; Khan et al., 2024; Limkakeng et al., 2014; Torres & Tajima, 2024; Vincent et al., 2022; Warraitch et al., 2024; Wearn et al., 2025; Werner et al., 2025; Zibrowski et al., 2021). In this regard, it is reported that early engagement and meaningful collaboration with communities and stakeholders are essential for balancing power dynamics and mitigating the risks of tokenism. This approach fosters equitable partnerships and ensures that diverse community perspectives are authentically represented (Gholipour et al., 2023). Furthermore, the implementation of flexible and inclusive recruitment strategies tailored to the specific needs and characteristics of diverse populations effectively addresses challenges related to participant eligibility and enrollment, thereby enhancing participation rates (Heffernan et al., 2023).
Limitations and Implications
This study had some limitations to address. The study sample, which was exclusively drawn from a single healthcare university, may be regarded as a limitation. Accordingly, future research is encouraged to undertake similar investigations across multiple universities to significantly address and mitigate this limitation. Moreover, as the study’s primary aim was to identify a comprehensive list of barriers to participation among diverse beneficiaries in healthcare research, without distinguishing the specific barriers unique to each group; given that these barriers likely differ across beneficiary categories, the study did not explore these variations due to limitations in time and resources. Future research can address this gap by examining the distinct barriers faced by each type of beneficiary.
The study carried several important implications. It offered comprehensive data on the barriers that hindered participation in healthcare research projects. This information held significant relevance for key stakeholders—including healthcare policymakers, administrators, and researchers—who sought to improve participant engagement in such projects. The data can effectively be utilized to develop strategic and operational plans aimed at increasing participation over both short- and long-term horizons. Furthermore, it can serve as an evidence-based foundation for designing interventions to overcome the identified barriers. In addition, the findings can inform the creation of evaluation checklists to assess adherence to these strategies within research initiatives, thereby identifying strengths and weaknesses in efforts to enhance individual participation. Notably, the study identified structural and institutional challenges as the most frequently cited barriers, corroborated by both literature and participant interviews. These findings had significant implications for beneficiaries in both local and international contexts. This underscored the critical importance of organizational and managerial knowledge in fostering greater participation in healthcare research. In this regard, the study also proposed several strategies to improve management knowledge among healthcare research centers and investigators.
Conclusions
The study findings identified several thematic barriers impeding individual participation in healthcare research projects. Among these, structural and institutional challenges were the most frequently cited barriers, as corroborated by both the literature and participant interviews. Within this context, the study underscored the critical importance of organizational and managerial knowledge in promoting increased participation in healthcare research. Consequently, it proposed strategies aimed at enhancing management knowledge among researchers. The findings may be utilized by relevant stakeholders within the context to enhance participation in healthcare research projects through an evidence-based approach.
Footnotes
Ethical Considerations
An ethical approval was obtained from the Birjand University of Medical Sciences Ethics Committee with the code IR.BUMS.REC.1404.018. All stages of the analysis were conducted by researchers who had no conflict of interest regarding the subject of the research. According to the specific ethical considerations form, the data analysis was performed in such a manner that the personal information of none of the participants was disclosed, and all information was kept confidential. Furthermore, in accordance with ethical principles, not only was consent obtained from participants upon their entry into the study, but they were also granted the necessary authority to withdraw from the study at any time if they so desired.
Consent for Participation
Informed consent was taken from all of the study participants.
Author Contribution
MK and RI conducted the review, and performed the thematic analysis. MK wrote the text of the manuscript. ZZ and NJ conducted the interviews and collaborated in the thematic analysis. RI and ZZ revised the text of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The research data can be accessed by contacting the corresponding author of the article.*