
Abstract
The Wound Healing Foundation (WHF) previously organized consensus panels on the management of chronic wounds (2022), acute wounds (2024), and diabetic wounds (2025). This WHF consensus statement, authored by a global interdisciplinary panel of clinicians and researchers, focuses on the management of infected wounds. The panel members reviewed the literature and reached consensus on elements of an evidence-based approach to infected wounds. Using a structured format, this statement progresses from discussing how wound infections develop, how to diagnose them, how to provide the most appropriate antimicrobial and surgical treatment, how to assess response to treatment, and how to further investigate instances of unsuccessful treatment.
Nicolás Cortés-Penfield
INTRODUCTION
Acute and chronic wound infections cause a high global burden of morbidity, frequently leading to source control procedures, amputations, antimicrobial therapy-associated complications, and sometimes mortality. In the United States, annual direct costs of diabetes-related foot wound care (mainly infections) approach $80 billion, compared with approximately $190 billion for all U.S. cancer care combined.1,2 Despite this, wound infection research is poorly funded and medical and nursing curricula provide limited training in their evaluation and management. The Wound Healing Foundation (WHF), an international organization of clinicians, researchers, and patient advocates passionate about wound care, previously formed expert panels to draft consensus guidance for wound care. These documents overview key topics, emphasize clinical decision-making, and are aimed at wound care professionals in all types of practice. Prior WHF consensus statements focused on the management of acute wounds, chronic wounds, and diabetic wounds.3–5 This document, updating and building on the comprehensive wound infection guidance published by the International Wound Infection Institute (IWII) in 2022 6 and the expertise of its members, offers a focused review of the management of infected wounds. Of note, we eschewed reviewing noninfectious aspects of wound care, as these were addressed in preceding WHF consensus documents.3–5
The consensus panel on infected wounds was organized by a steering committee (E.E., N.C-P., B.A.L., R.T., P.L., I.U., L.K.S.P., and, in its earliest stages, the late professor Gregory S. Schultz) that outlined the major topics to be covered and then recruited the other panelists. They sought clinicians and/or scientists who had nationally recognized expertise studying and treating various types of wound infection and who represented a broad range of geographic regions (North America, Europe, and Asia/Oceania) and specialties (surgical subspecialties, microbiology, infectious diseases, wound care nursing, pharmacy, and basic science). The panelists divided into workgroups, each tasked with performing literature reviews of each of their assigned major subsections, then drafting a brief review of the topics and proposing consensus recommendation statements.
The novel contribution of this work lies in its multidisciplinary construction and format. Each aspect of infected wound management, from diagnosis to medical and surgical treatments to assessment of treatment response (Fig. 1), has been authored and reviewed with input from primary wound care specialists, as well as experts from across the disciplines with whom they collaborate in caring for patients. Similarly, we deliberately constructed a consensus panel comprised of authorities with broad global representation so as to lessen the risk of enshrining regional practice preferences as standards of care where they do not reflect optimal evidence-based medicine.
The full consensus panel convened virtually on November 9, 2024. During a day-long meeting, all members reviewed each of the proposed consensus statements and their supporting evidence, then serially modified them until a final statement was accepted by ≥80% of the panelists. None of the authors received any payment or other compensation for any part of this work.
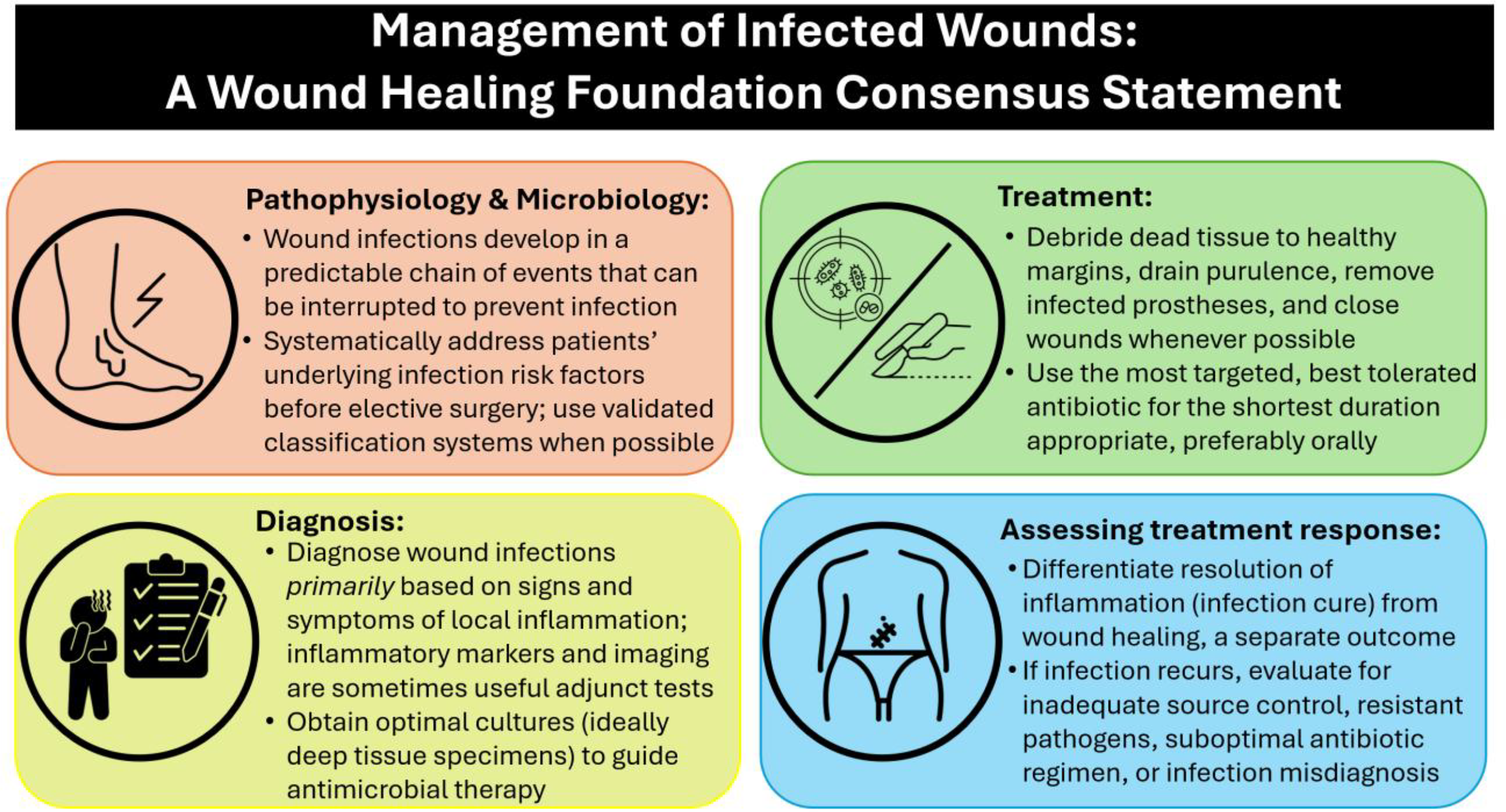
Conceptual approach to wound infection.
CLINICAL PROBLEM ADDRESSED
The goal of the WHF infected wound consensus was to develop concise evidence summaries describing how wound infections arise, are diagnosed, and should be treated, then produce practice consensus guidance that was relevant (falling within the scope of the wound care professions and/or helping them understand the contributions of their multidisciplinary team colleagues), evidence-based (wherever possible, referencing well-designed comparative clinical studies rather than opinion or historical standards of practice), and helpful (focusing on actionable recommendations and common areas of confusion and uncertainty for clinicians).
PATHOPHYSIOLOGY AND MICROBIOLOGY
How wound infections develop
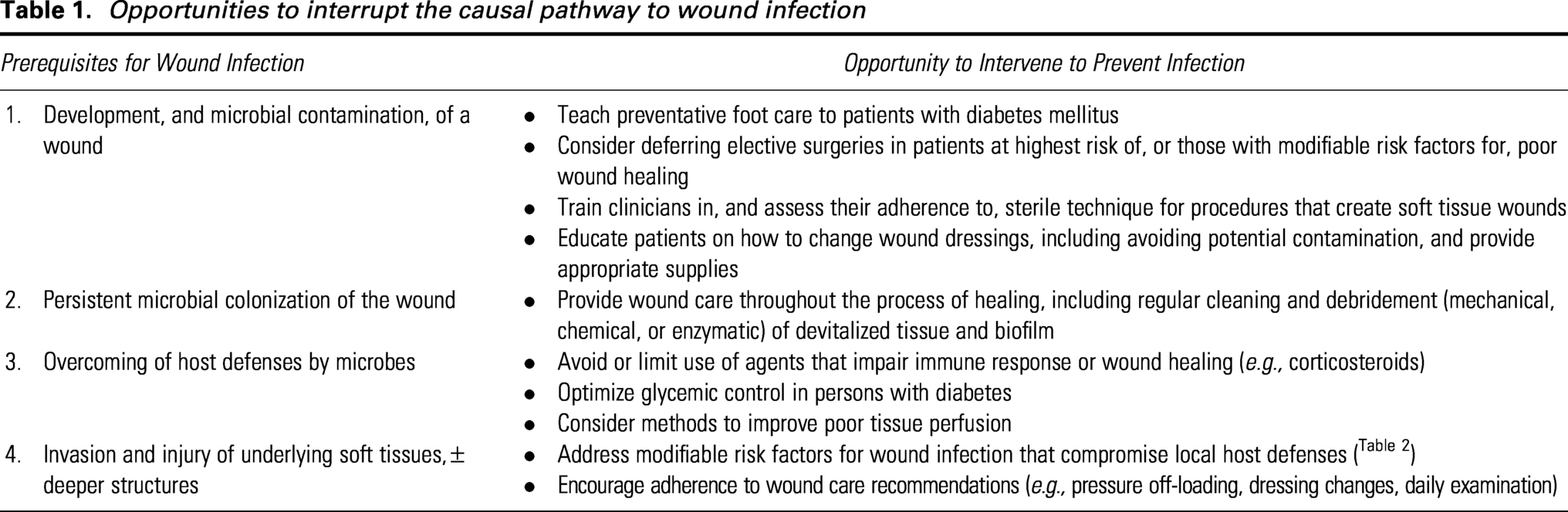
By disrupting skin integrity, wounds inherently compromise the first major host defense against infection. While virtually all open wounds become contaminated with microorganisms, not all become infected. Infection requires (1) successful microbial replication, leading to persistent colonization; (2) that overcomes the host’s immune defenses; (3) leading to invasion from the wound surface into at least the surrounding skin and soft tissues; and (4) causing tissue injury from direct bacterial destruction and/or the host’s own inflammatory response. Understanding this chain of events is critical to identifying opportunities to both prevent and treat wound infection (Table 1).
Recommendations
Systematically evaluate and address each patient’s underlying risk factors for wound infection, in addition to providing wound care, antimicrobials, and surgery, as appropriate.
Use validated risk stratification tools (where available) to assess and manage patients with infected wounds.
Opportunities to interrupt the causal pathway to wound infection
Risk factors for wound infection
Observational studies have identified a variety of risk factors for wound infection, including prolonged wound duration and colonization with pathogens possessing inherent virulence or propensity to develop biofilm. Host risk factors for wound infection can be broadly categorized as those that (1) compromise immune defenses, (2) impair wound healing, or (3) impede patient access or adherence to wound care. Some risk factors span several of these categories; for example, chronic hyperglycemia in uncontrolled diabetes leads to a dysregulated inflammatory response that compromises host defenses, 7 as well as to microvascular disease and local tissue hypoperfusion that impairs wound healing.
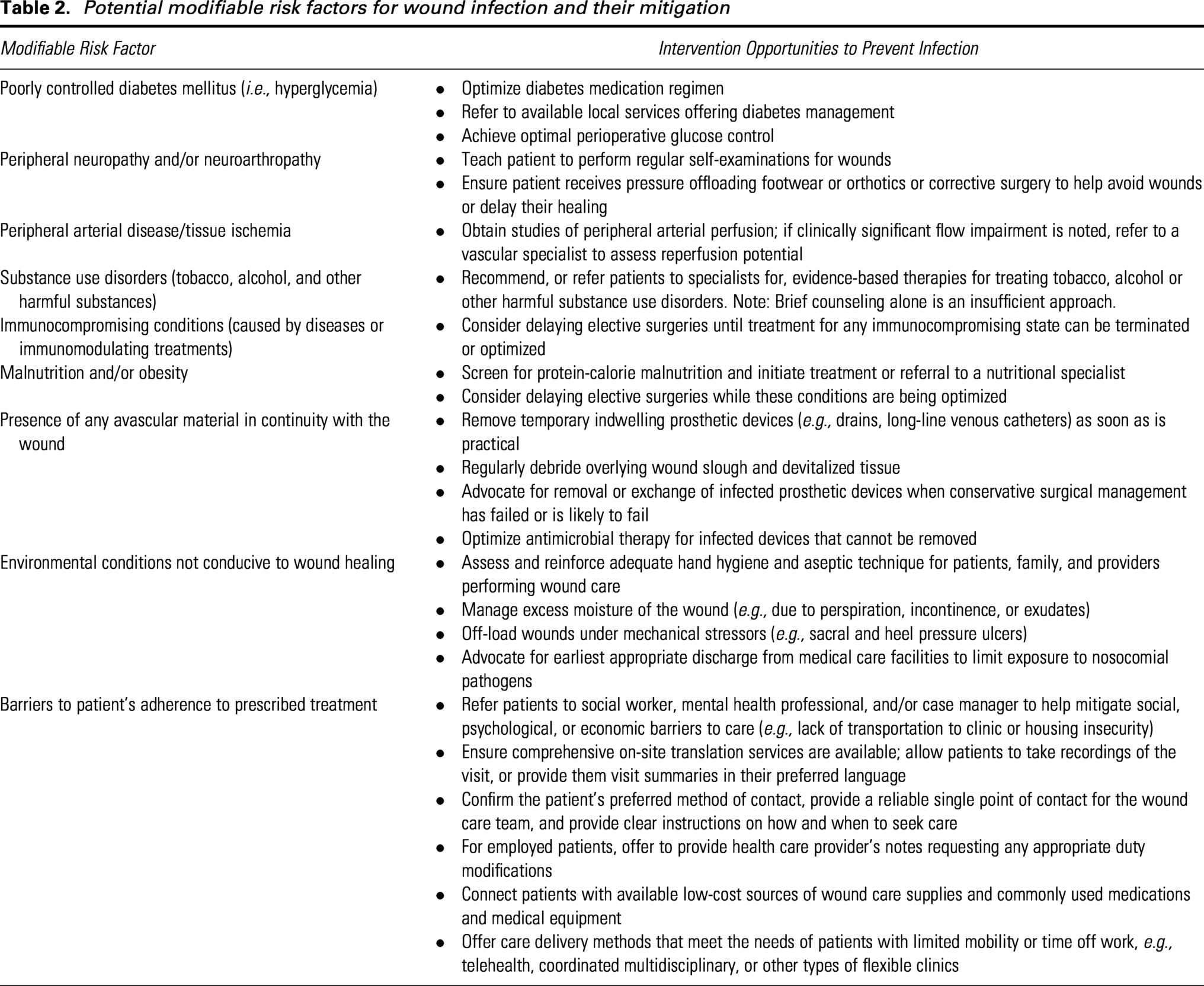
Clinicians should systematically investigate and mitigate modifiable risk factors (Table 2) in patients who have or are at elevated risk for wound infection. Multiple studies suggest that a standardized wound management approach implemented via an interdisciplinary team can address patients’ barriers to care, improve the quality of the diagnostic workup, and optimize clinical outcomes.8–13
Some risk factors for wound infection are not modifiable, such as advanced age, treatment with certain medications (e.g., chemotherapy), prior local trauma (e.g., radiation therapy), or major medical comorbidities (e.g., end-stage kidney or liver disease). Nonmodifiable features of existing wounds include large size, great depth, gross contamination, or anatomical location proximate to sites of contamination (e.g., the perineum). Clinicians should consider these factors when evaluating a patient’s candidacy for elective surgery and deciding whether to pursue a standard or alternative (e.g., minimally invasive) surgical approach.
Potential modifiable risk factors for wound infection and their mitigation
Classifying wound infections
No single system has been universally adopted for classification of either wounds or wound infections. One common method to categorize wounds is by duration, with acute generally meaning occurring within the past few days, and chronic usually defined as not having closed within a month of the initial injury. Some experts have noted that time-based criteria have been inconsistently applied in the chronic wound literature and suggested that these be instead defined by pathophysiology, with a chronic wound being one occurring in a patient who has one or more underlying comorbidities that contribute to either insidious onset or delayed healing.14,15
Microbiologically, wounds can be characterized on a spectrum from asymptomatic colonization to overt clinical infection. Proliferating microorganisms can contribute to poor wound healing through local tissue injury and the inflammatory response it induces. However, this does not mean that every patient with a poorly healing wound has a covert or “subclinical” infection, and critically, there is a lack of evidence demonstrating that treating wounds without classical signs of infection with systemic antibiotics aids wound healing or prevents infection.16–18 On the other hand, inappropriately prescribed antibiotic therapy often promotes colonization (and likely eventual infection) with multidrug-resistant organisms (MDROs), and infection with MDROs is associated with increased treatment costs, treatment failure, and mortality.19–22 We urgently need studies to help delineate what findings or tests may help identify patients with a poorly healing, but not yet overtly infected, wound who can be managed with topical antiseptics (antimicrobial substances applied to living skin or tissue to destroy or inhibit the growth of microorganisms) and wound care alone versus benefiting from adding topical or systemic antibiotic therapy, or indeed other treatment modalities (e.g., surgical procedures).
Some wound infections treated nonoperatively have a poor outcome despite receiving topical or systemic antimicrobial therapy (drugs and other agents that kill or inhibit the growth of microorganisms) and appropriate wound care, which generally includes surgical excisional, nonsurgical mechanical, enzymatic, or other means of debridement of devitalized and unhealthy tissue, application of appropriate wound dressings to manage moisture and stimulate wound healing. In select cases, wound care may also involve adjunctive treatments such as negative pressure wound therapy and hyperbaric oxygen. While not all hard-to-heal wounds require surgery, those more likely to require a source control procedure in addition to antibiotic treatment and local wound care: (1) involve deeper tissues, especially bone or visceral structures; (2) are associated with an undrained abscess or phlegmon; (3) occur in the context of peripheral vascular disease; or (4) are complicated by implanted prosthetic material or devices.23–25
Finally, whenever possible, clinicians should assess wound infections using clinically validated staging systems with proven prognostic value (Table 3). Perhaps the best-established example of such a system is the wound, ischemia, and foot infection (WIfI) score, which provides prognostic information on both the risk of amputation and potential benefit of revascularization in patients with infected foot wounds related to diabetes or peripheral arterial disease (PAD).26–30 The WIfI score can be determined using only clinical examination and noninvasive vascular studies, and several free online resources (e.g., the Society for Vascular Surgery’s iPG mobile phone app; www.mdcalc.com) allow rapid bedside calculation and interpretation. The Infectious Disease Society of America (IDSA)/International Working Group for the Diabetic Foot (IWGDF) classification system also has demonstrated management and prognostic value in patients with diabetes and an infected foot ulcer, and this classification system forms the basis of the “foot infection” component of the WIfI system. 31 Unfortunately, there are no equivalent scoring systems proven to optimize the management or predict the outcome of most other wound infections. Developing and validating such systems, and ensuring they are easy to calculate using simple bedside assessments and noninvasive tests, should be a priority for the next decade of wound infection research.
Clinically validated diagnostic classification systems for wound infections
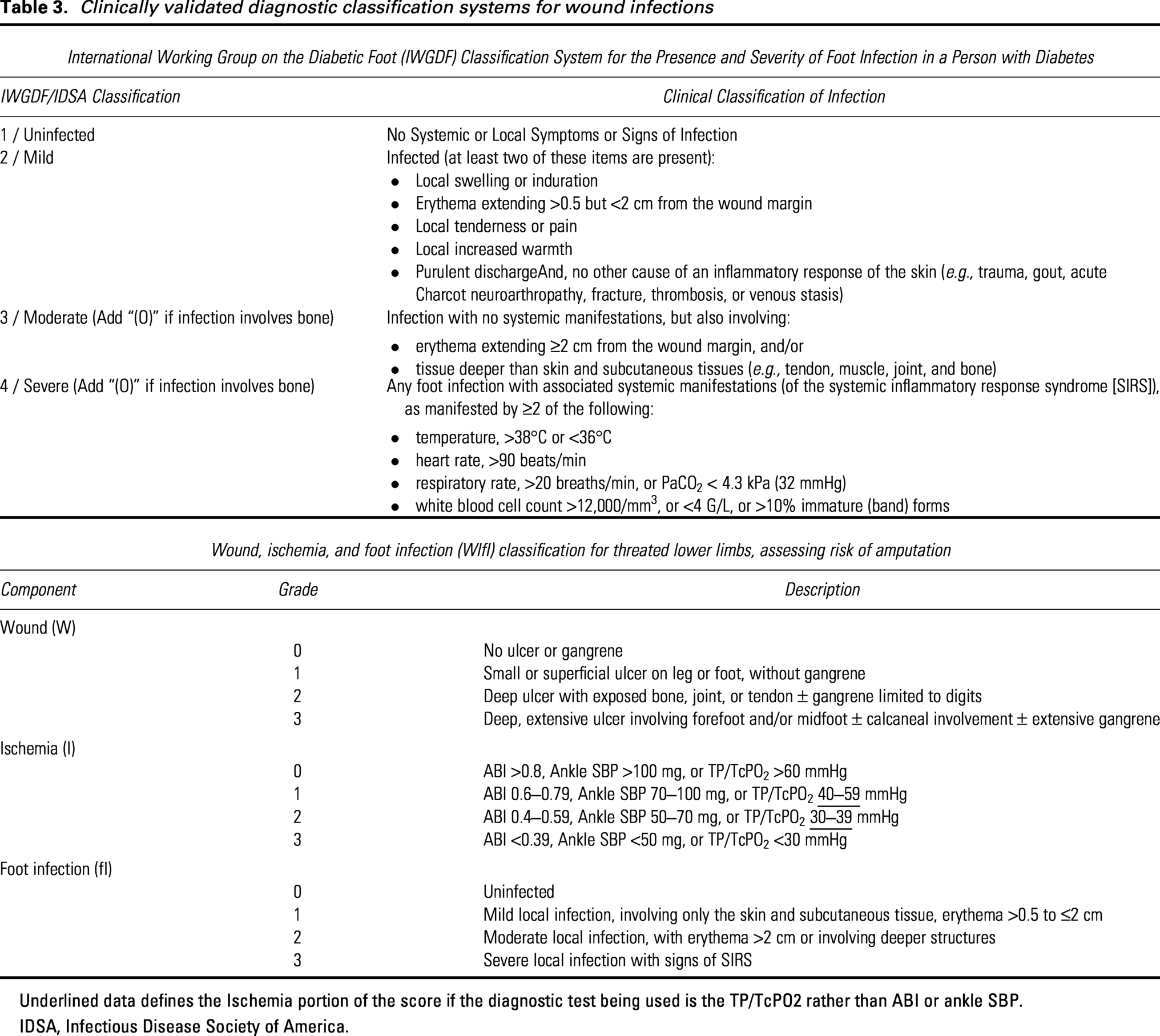
Underlined data defines the Ischemia portion of the score if the diagnostic test being used is the TP/TcPO2 rather than ABI or ankle SBP.
IDSA, Infectious Disease Society of America.
Role of biofilm in wound infections
Biofilms are microscopic communities of bacteria and/or fungi that aggregate and envelop themselves within an extracellular matrix of DNA, proteins, polysaccharides, and other small molecules. 32 Microorganisms inside this biofilm become less susceptible to both host immune defenses and antimicrobials. Biofilms can propagate on avascular surfaces in or on the body within days of inoculation and can become a nidus of recurrent infections until removed. This is a key reason patients who develop implant-related infections often fare poorly with simple debridement and antibiotic therapy, rather than complete device removal or exchange.
Biofilms develop in most chronic wounds 33 and can delay or prevent healing by causing a dysregulated local inflammatory immune response. This manifests via degradation of granulation tissue that compromises wound healing biomechanics, suppression of vascular epithelial growth factor expression, and ultimately increasing tissue necrosis and the development of slough.34–36 While clinicians often attribute a particular affinity for biofilm formation to certain types of bacteria (e.g., staphylococci), most bacterial and fungal pathogens form biofilms under suitable conditions. In fact, biofilms frequently involve polymicrobial communities, and preclinical studies suggest that interspecies interactions within these biofilms may contribute to increased antibiotic resistance and greater impairment of wound healing.37–39
Wound care techniques focused on identifying and eradicating biofilm have been associated with improved wound healing, even in the absence of infection.40–43 One clinical trial found that serial debridements guided by wound blotting with a nitrocellulose membrane followed by chemical staining of the membrane to visualize fragments of transferred biofilm resulted in greater reductions in wound depth and severity over a 3 week period, compared with debridement not guided by wound blotting. 42 Topical antiseptics can reduce wound biofilm burden and, notably from the antimicrobial stewardship perspective, may be an attractive alternative to systemic antimicrobials for nonhealing wounds without clinical evidence of overt infection. 44
Unfortunately, the overall level of evidence supporting the effectiveness of topical treatment modalities for biofilm in infected wounds is poor. More studies demonstrate that various approaches can reduce biofilm burden than that this translates to clinical benefit. One recent meta-analysis identified 13 randomized clinical trials that spanned a wide range of interventions aimed at biofilm in wounds, of which 85% were at high risk of bias. It found that only two studies reported wound healing outcomes in infected wounds, with neither demonstrating improvement in either resolution of symptoms of infection or complete wound closure. 45 Nonetheless, findings from in vitro, animal model, and observational clinical data, as well as consensus clinical experience, support the notion that bacterial biofilms commonly form in chronic wounds (infected or not) and they contribute to impaired wound healing. Thus, we believe that to optimize wound healing after the acute infection has been addressed. Patients who develop wound infection in a chronic wound should receive thorough wound cleansing and debridement, as well as other available means to address residual biofilm at the treating clinician’s discretion.
Many types of specific topical antiseptics and antibiotic treatments and dressings have been proposed to treat wound infections. Further discussion of this complex topic is beyond the scope of this document, but has been addressed in some detail in the prior WHF consensus statements on the management of acute, chronic, and diabetic wounds.3–5
Microbiology of wound infections
Acute wound infections are often monomicrobial, whereas chronic wound infections are usually polymicrobial. Wounds are most commonly colonized by the surrounding skin microbiota, with common but virulent skin pathogens (e.g., Staphylococcus aureus) being the most frequent causes of infection across various wound etiologies.46–49 Beyond this, the microbiology of any specific wound infection varies by the type of wound, 50 anatomical site, 51 geographic region, 52 patient comorbidities, 53 and the impact of changes in microenvironment from prior care50,53,54 (e.g., replacement of the normal microbiome by nosocomial or MDROs after repeated or prolonged antibiotic exposures or hospitalizations) (Table 3).
Nonbacterial (e.g., fungal, mycobacterial, or parasitic) wound infections are rare in the developed world, except in specific clinical scenarios, such as a nonhealing or recurrent surgical wound infection that has been treated with multiple courses of broad-spectrum antibiotics, or as part of a polymicrobial infection in a wound bed contaminated with either environmental debris (e.g., soil or water) or gastrointestinal contents. 55 In these cases, fungi, especially Candida species, sometimes supersede the original causative bacteria as pathogens, often with a poor outcome. Patients with deep inoculation of soil or vegetative matter may develop chronic draining wounds due to infection with atypical pathogens, such as nontuberculous mycobacteria, Sporothrix spp., Actinomyces spp., or Nocardia spp.56–59 To diagnose infection caused by these unusual pathogens, clinicians must first consider them in characteristic circumstances, then identify them by skin or deep tissue biopsy processed with special microbiologic stains and cultures.
Wound infections caused by fungi other than Candida are uncommon, 55 except perhaps in certain highly immunocompromised hosts (e.g., those who have recently undergone solid organ or stem cell transplant) or high-burden inoculations (e.g., thermal burns, deep penetrating injuries involving wood or soil). Single positive wound cultures with organisms, such as Penicillium spp., Aspergillus spp., Alternaria spp., or Mucorales spp., usually reflect laboratory culture contamination, rather than infection. Thus, in the absence of risk factors, we recommend against routine testing, or empiric treatment, for fungi or mycobacteria in wound infections, as this is likely a low-value practice. 60 Parasitic and other tropical cutaneous infections can also mimic bacterial wound infection, but mostly occur in patients who have lived in or visited endemic areas. These infections are beyond the scope of this review.
Clinically summary
Wound infections develop via a typical chain of events and share common risk factors, many of which are modifiable and thus can be proactively addressed to disrupt the chain. 46 Wounds exist on a spectrum from asymptomatically colonized with bacteria to overtly infected, but there is limited evidence to support the notion that poor wound healing alone indicates infection. Wound infections can be categorized as acute or chronic, with chronic wounds typically having insidious onset or delayed resolution driven by host comorbidities.14,15 The presence of biofilm frequently complicates chronic wound infections, can contribute to poor wound healing when present, and should be controlled (e.g., by surgical debridement and/or local wound care strategies) to increase the likelihood of cure.35,40,42 Clinically validated scoring systems for foot infections predict treatment outcomes, including risk of amputation and potential benefit from revascularization24,26,29,61; such well-validated classification tools are sorely needed for other types of wound infection.
DIAGNOSIS
Clinical signs and symptoms
International guidelines addressing how to diagnose a wound infection vary, but they agree on the importance of clinical signs and symptoms.6,31,62 Many guidelines classify these findings as either “classical” (i.e., pain/tenderness, warmth, erythema, induration, purulence) or “secondary” (e.g., malodor, friable granulation, poor healing). While all are limited by poor interobserver agreement, the classical signs of local inflammation have largely been validated over time, and we recommend using them as the standard for diagnosing a wound infection. When assessing for signs and symptoms of infection, clinicians should be attentive to potential confounding factors, such as the patient’s natural skin tone, the impact of common comorbidities (especially ischemia or neuropathy), and immunocompromising conditions that may lead to reduced inflammatory findings. Dependent rubor due to vascular compromise can be particularly difficult to distinguish from erythema due to cellulitis. Elevating the limb to see if the erythema diminishes (more likely with the former than the latter) can help make this distinction.
For patients with open infected foot wounds in which underlying osteomyelitis is suspected, we suggest doing the probe-to-bone test—gently inserting a sterile blunt metal probe into the foot wound to feel for the hard, gritty structure of cancellous bone. This test requires limited training, is rapid, inexpensive, relatively harmless, and reasonably accurate in experienced hands.
Recommendations:
The key findings for diagnosing infection in a wound are clinical signs and symptoms of inflammation.
When signs and symptoms are insufficient or too equivocal to make the diagnosis of infection, results of selected laboratory tests (white blood cell count [WBC], erythrocyte sedimentation rate [ESR], C-reactive protein [CRP], or procalcitonin [PCT]) can be helpful in evaluating if a wound is infected. Several newer biomarkers have not yet been adequately studied to determine when and how they might be useful.
Microbiological studies are not used to diagnose wound infection but are central to optimally selecting their treatment. They facilitate timely initiation of targeted antimicrobial therapy, thereby improving patient outcomes and minimizing the adverse effects associated with unnecessarily broad-spectrum antimicrobial regimens.
When possible, it is best to obtain viable tissue specimens for wound cultures as they more accurately identify pathogens than swabs. Properly obtained deep swab specimens can also reasonably serve as alternatives for culture.
Molecular microbiology techniques often identify more bacteria from soft tissue samples than standard cultures, but the clinical relevance of these additional organisms remains unclear. Clinicians should continue to request conventional culture and sensitivity testing for wound specimens.
Consider using imaging procedures to characterize the extent of a wound infection, particularly when underlying bony involvement is suspected.
Biomarkers
Several studies have examined the utility of serum biomarkers in diagnosing various infections. The most widely used biomarker is the WBC, elevation of which (≥11,000 cells/µL) in the setting of an infected diabetes-related foot wound and without any other inflammatory pathology (e.g., active gout) usually suggests at least a moderately severe infection. Other commonly used biomarkers are the ESR, CRP, and PCT.63,64 A recent systematic review and meta-analysis of the diagnostic accuracy of various inflammatory markers found that the serum CRP most effectively distinguished infected from noninfected diabetes-related foot ulcers (DFUs), followed by PCT, ESR, and WBC. 65 Highly elevated values of these markers suggest osteomyelitis may be complicating an infected wound, particularly of the diabetic foot.66,67 For ESR, using a cutoff of approximately 50 mm/h, the sensitivity and specificity for detecting osteomyelitis in an infected DFU are each about 0.8; for CRP, using a cutoff of approximately 8 mg/L, sensitivity is about 0.7 and specificity about 0.6. However, the diagnostic utility of these markers for osteomyelitis underlying foot wounds appears to be limited in patients without diabetes. 68 The limited published sensitivity of these markers highlights that they should not be used alone to rule out bone involvement, particularly in patients suspected of having chronic osteomyelitis, for which local inflammatory responses are often attenuated. Assessing a composite of several biomarkers, in conjunction with clinical assessment and imaging, likely provides the greatest diagnostic utility.
Less commonly used tests that might be available in some centers include those for (1) host-specific biomarkers (chemicals and enzymes released during infection and healing, e.g., calprotectin, presepsin, lysozyme, myeloperoxidase); (2) bacteria-specific biomarkers (chemicals and enzymes produced by invading bacteria, e.g., proteases, pyocyanin, homoserine lactone, β-lactamase); and (3) bacterial volatile organic compounds (gas-phase biomarkers or volatile compounds). 69 Host-specific biomarkers may offer information about the health of a wound while those that are bacteria-specific are more likely to help diagnose infection, but none of these have yet been well-studied clinically or have established a clear role in wound infection management. Other novel methods of detecting wound infection still in development include autofluorescence (which identifies the presence and density of various bacteria on the wound surface), wound blotting (which stains and maps biofilm in a wound), leukocyte esterase detecting devices, and medical sensors that assess a wound’s odor, temperature, or pH. 69
Microbiologic cultures
Infection should not be diagnosed solely by the isolation of microorganisms from a wound, as these may represent colonizers or contaminants. However, establishing the microbiologic etiology of wound infections to optimize antimicrobial treatment is crucial to achieving cure while minimizing antibiotic-associated harms and cost. 70 Undertaking this process is referred to as antibiotic stewardship, which focuses on selecting the right drug, correct dose, appropriate drug-route, suitable duration, and timely de-escalation (the 5Ds). 71 Reliably obtained and processed culture data can facilitate this work by allowing clinicians to confidently opt for antibiotic regimens that use orally administered, narrower-spectrum, cheaper, and better-tolerated agents, rather than unnecessarily broad-spectrum parenteral empiric regimens. 72
When clinicians suspect infection in a wound based on clinical findings, they should promptly collect a high-quality wound specimen for culture,6,31,73 that is, deep purulence or infected tissue, or a swab culture obtained via the Levine technique, rather than a more haphazardly collected superficial specimen that may be contaminated with superficial colonizing organisms. Thus, in most cases, the best specimen is aseptically collected wound tissue, ideally obtained via biopsy. Tissue specimens have the added advantage of providing both quantitative information (the bioburden) and qualitative data, such as histopathology. Several studies demonstrate that tissue samples may be both more sensitive and more specific than swabs in identifying pathogens in wound infections.74–76 However, obtaining tissue biopsies may require local anesthesia (in non-neuropathic wounds) and some specialized training, can cause discomfort or exacerbate wound damage, and is more expensive and less expedient than obtaining swab cultures. 77
Clinicians more routinely collect wound swabs than tissue specimens for culture because they are noninvasive and performing them requires no specialized training. If sampling is done by swab, it should be performed after wound cleansing and sharp debridement by applying mechanical pressure with swab rotation (Levine technique). This can detect organisms within deeper tissue layers, and studies indicate that such specimens produce microbiological results that correlate well with tissue biopsies.78,79 Moreover, a recent study demonstrated that assessment of wound infection by experts does not differ when they are provided results of swabs versus biopsies, albeit with substantial interobserver variability. 80 These data support a role for obtaining a deep swab culture (after cleansing and debridement and using aseptic technique) when acquiring tissue cultures is not feasible or they cannot be obtained in a timely and cost-effective manner.
Molecular studies
Molecular tests, such as DNA polymerase chain reaction (PCR) and next-generation sequencing (NGS), are based on microbial DNA/RNA extractions from clinical samples. These methods overcome key limitations of culture techniques, including poor recovery of some fungi and obligate anaerobes as well as decreased sensitivity for senescent bacteria in mature biofilms. 81 Molecular methods also potentially offer faster turnaround times, with multiplex PCR technology allowing simultaneous identification of multiple pathogens within hours. 82
Unfortunately, while clinically validated PCR diagnostics have been developed for other infection syndromes (e.g., meningitis, bacteremia), no commercially available molecular test has yet demonstrated its usefulness for diagnosing or improving the management of wound infections generally. 81 The key limitations of molecular diagnostic methods are that they do not distinguish live from dead microorganisms and do not always provide accurate information on antibiotic susceptibility phenotype (e.g., a bacteria may test positive for a carbapenem resistance gene, but then demonstrate susceptibility to carbapenems in culture, or conversely, harbor resistance to an antibiotic via a mechanism not tested on the PCR panel). 83 Most critically (and as we have learned from recent changes in approach to Clostridioides difficile colitis diagnosis), PCR tests cannot distinguish colonizing from infecting pathogens, and their ability to detect bacteria at lower, clinically insignificant levels may drive overtreatment. 84 Data from a recent prospective study of infected DFUs demonstrated that while molecular techniques detected a broader microbial spectrum, including fastidious anaerobes, its low concordance with standard cultures and lack of antibiotic sensitivity data limit its current suitability to supplant cultures. 85
Imaging
Many imaging modalities can aid in diagnosing, classifying, and managing wound infection. Understanding each test’s relative advantages and disadvantages is important for determining its role in delivering optimal and cost-effective care.86–89
Plain X-rays are widely available, relatively inexpensive, and can be obtained and read quickly (often by the ordering clinician). They are useful for identifying radiopaque foreign bodies or chronic osteomyelitis, but are insensitive for early osteomyelitis and non-gas-forming soft tissue infections.90,91 Computed tomography (CT) with intravenous (IV) contrast, also widely available and relatively inexpensive, offers more detailed cross-sectional views, making it much more sensitive than plain X-rays for abscesses and deep soft tissue infection. 91 Ultrasound (placing the probe adjacent to, not into, the wound bed) is a noninvasive, inexpensive, and increasingly available bedside imaging method that can identify abscesses and help guide drainage procedures. 92 Magnetic resonance imaging (MRI) can provide highly detailed images of almost any type of tissue and is particularly useful for detecting osteomyelitis in the early stages. 92 However, compared with plain X-ray and CT, MRI is more expensive, often less readily available, and contraindicated in patients with certain implanted devices.
Nuclear medicine studies, like tagged-WBC scans and bone scans, use various radiolabeled white blood cells or radionuclides that concentrate in certain body tissues to detect infection or inflammation. Bone scans are highly sensitive for osteomyelitis, but can have limited specificity. 93 [18F]fluorodeoxyglucose positron emission tomography assesses metabolic activity in tissues, which may optimally distinguish infectious from noninfectious inflammatory processes (i.e., diagnosing early postoperative wound infection when postoperative inflammation is still active), but is costly and often not readily available.94,95
Clinically summary
Wound infections are primarily diagnosed clinically by the presence of local inflammatory changes. Leukocytosis and elevated inflammatory markers can help diagnose wound infection in equivocal cases, and imaging can be useful to identify or characterize the extent of a deeper infection, such as underlying abscess or osteomyelitis. Microbiologic studies—principally cultures, although molecular studies are increasingly being adopted—are critical for selecting optimal antimicrobial therapy for wound infections and rely on properly collected tissue or swab samples for optimal and accurate diagnostic yield.
ANTIMICROBIAL TREATMENT
General principles of treatment
Antimicrobials used for treating wound infections include antiseptic (topical) and antibiotic (topical and systemic) agents. These are powerful tools for treating wound infection—so much so that clinicians are often overreliant on them, neglecting other aspects of wound care, such as debridement, dressings, pressure off-loading, revascularization, and reducing immune-suppressive medications. Clinicians should be aware, and impress upon their patients, that while antimicrobials are effective in resolving infection, they do not heal wounds per se. 96 The efficacy of antimicrobial therapy is greatest in acute soft tissue infections, but often more limited (and sometimes negligible) in chronic nonhealing wounds without signs of acute infection. 96
Empiric therapy: when and how to select
When treating wound infections, antimicrobial therapy should almost always be accompanied by debridement, which is aimed at removing necrotic and purulent material, diminishing the microbial load, and collecting tissue samples for culture (preferably before administering antimicrobials).31,47,72,97,98 While awaiting culture results, clinicians should select an empiric antibiotic regimen based on the available clinical and microbiological information that may help suggest the likeliest pathogens. This typically includes the history of the presentation and appearance of the wound, results of recent cultures, and any microorganisms (and neutrophils) seen on a Gram-stain smear of a wound specimen. 73 If microbiological data are not available, base the regimen on the most frequent microorganisms known to be responsible for the specific type of wound infection, while also considering local antibiotic susceptibility data and other relevant clinical or epidemiological factors (e.g., recent antibiotic therapy, drug allergies, immune status, renal insufficiency).
Empiric antibiotic therapy should usually include coverage for S. aureus and beta-hemolytic streptococci, which are common (and virulent) pathogens across nearly all types of wound infections. 99 Whether to use agents also active against aerobic gram-negative bacteria depends on several key factors, including the site of infection, the presence of wound ischemia or maceration, or any recent antimicrobial exposure.73,100–102 The regional microbiology is also important; for example, diabetes-related foot infections (DFIs) in subtropical regions are frequently caused by Pseudomonas aeruginosa, while this is a relatively uncommon pathogen in temperate climates.31,103 Empiric therapy aimed at obligate anaerobic bacteria is usually unnecessary except for acute, severe, or rapidly spreading infections, those accompanied by sepsis, or those presenting with necrosis or a foul odor (of note, foul wound odor may be improved with topical metronidazole gel, though evidence this directly hastens infection resolution is more limited). 104 For cases of severe wound infection, we recommend initial therapy with a broad-spectrum parenteral antibiotic regimen. 73 Table 4 provides common characteristics of a wound infection that can help guide antimicrobial therapy and Table 5 provides our suggestions for empiric regimens.
Characteristics of wound infection that may inform the likely causative pathogen(s)
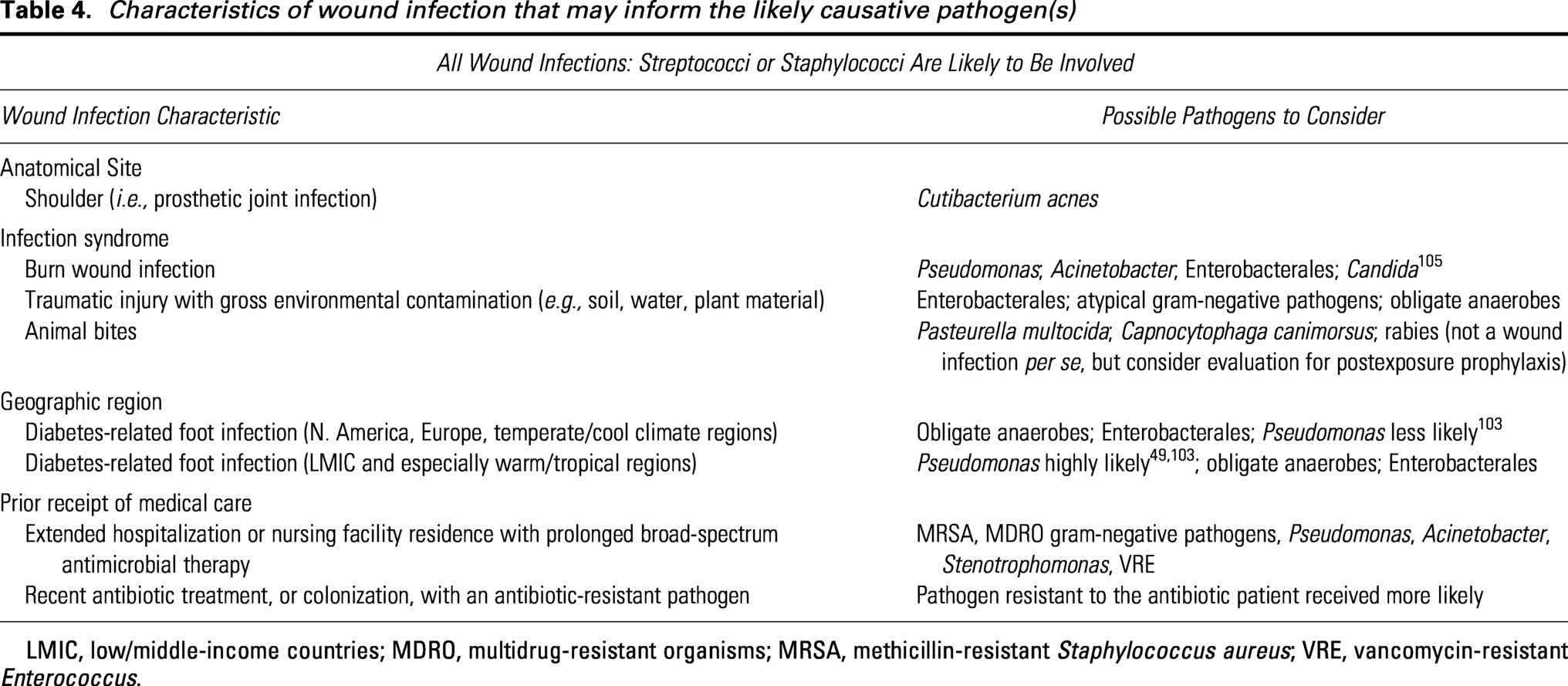
LMIC, low/middle-income countries; MDRO, multidrug-resistant organisms; MRSA, methicillin-resistant Staphylococcus aureus; VRE, vancomycin-resistant Enterococcus.
Possible empirical antibiotic agents/regimens for polymicrobial wound infections
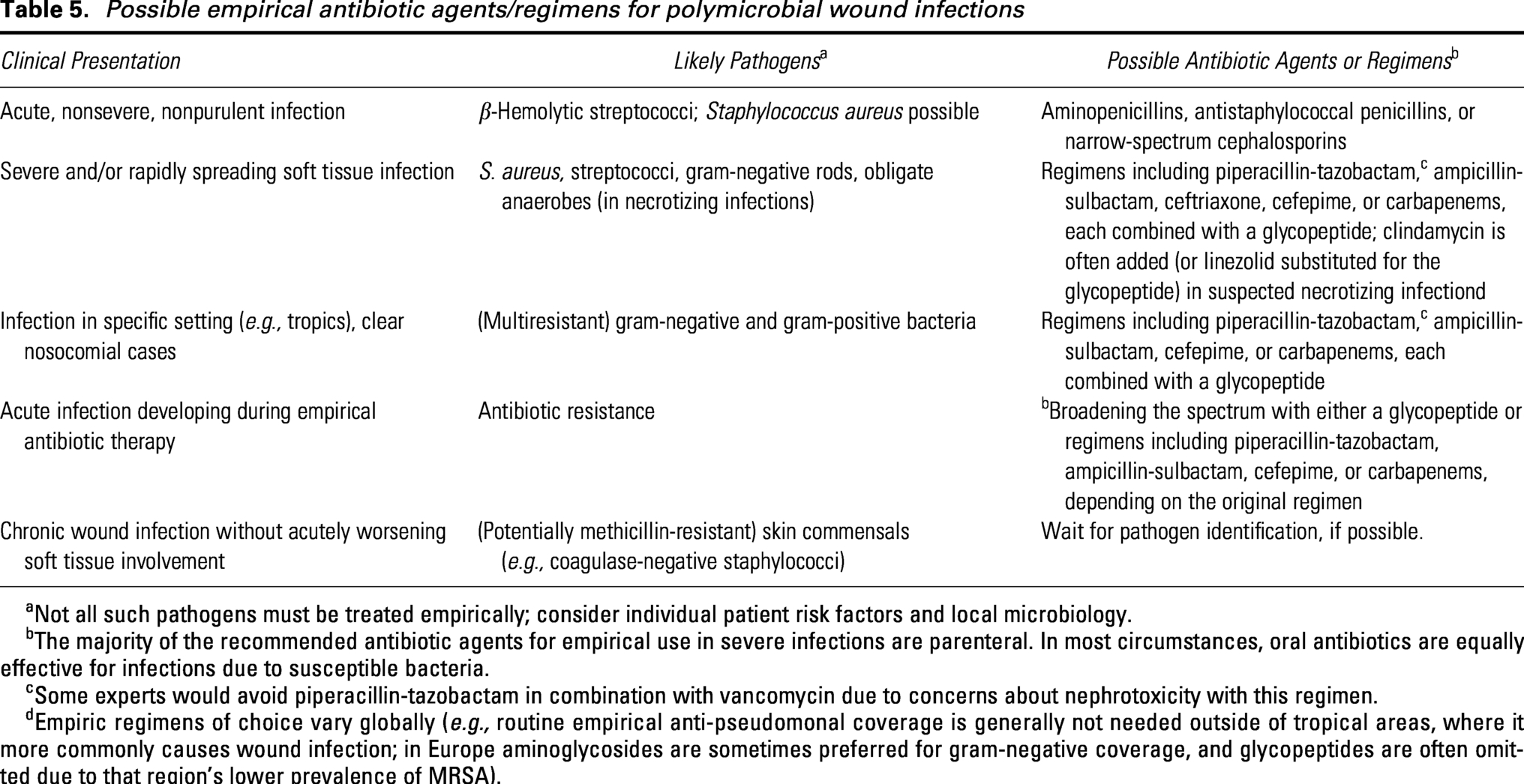
Not all such pathogens must be treated empirically; consider individual patient risk factors and local microbiology.
The majority of the recommended antibiotic agents for empirical use in severe infections are parenteral. In most circumstances, oral antibiotics are equally effective for infections due to susceptible bacteria.
Some experts would avoid piperacillin-tazobactam in combination with vancomycin due to concerns about nephrotoxicity with this regimen.
Empiric regimens of choice vary globally (e.g., routine empirical anti-pseudomonal coverage is generally not needed outside of tropical areas, where it more commonly causes wound infection; in Europe aminoglycosides are sometimes preferred for gram-negative coverage, and glycopeptides are often omitted due to that region’s lower prevalence of MRSA).
Selecting agents for empiric therapy for chronic infections can be challenging, as these are frequently polymicrobial, with the microbiology often influenced by recent antibiotic treatment. 98 This problem is now compounded by the increased proliferation of MDRO pathogens. Importantly, clinicians are not obliged to target every possible pathogen previously or currently isolated from a chronic wound culture. For treating infections that are mild and superficial, particularly if a first episode, it is reasonable to initially target just the most likely pathogens.
Definitive systemic antibiotic therapy
When cultures have identified the pathogen(s) and their antibiotic sensitivities, clinicians should evaluate the empiric antibiotic regimen and consider switching to the narrowest appropriate spectrum using the fewest agents, preferably given by the oral route.106–108 When wound cultures are negative or not available, if the patient is improving and tolerating the initial empiric regimen, continuing it is usually reasonable. In general, no single antibiotic agent, or combination, has been demonstrated to be clearly preferable to others for treating bacterial wound infections. 109 Nor have pharmacokinetic issues like bactericidal (versus bacteriostatic) activity been clearly associated with clinical outcomes. 110 Thus, other factors, such as the agent’s tolerability, safety, cost, or other antibiotic stewardship considerations, may take precedence in choosing antibiotic therapy. When possible, give preference to regimens that require fewer daily doses to improve treatment adherence. 111
Route of therapy
Antibiotic therapy given parenterally rapidly provides high serum levels, but it is often associated with longer hospitalizations, higher costs, and increased risk of catheter-related adverse events, such as venous thrombosis or IV catheter-associated infections. 112 Recent studies have shown that properly selected oral antimicrobial regimens reduce treatment cost, are at least as effective as IV therapy, 113 avoid IV catheter-related complications, and are less burdensome. 108 While not all patients (or pathogens) are suitable for a switch from IV to oral regimens, it should be the default route for definitive antimicrobial therapy in most cases. 112 Long-acting antimicrobials given by a single infusion, while often more costly, can also be pragmatically useful alternatives to daily IV therapy in select circumstances.114,115
Nonsevere localized wound infections can usually be treated with oral antimicrobials from the start. For initial therapy, there are no strict criteria for when to choose the IV route, nor for any minimum duration. 112 Patients presenting with critical illness or a rapidly spreading soft tissue infection may benefit from the higher and more rapidly achieved therapeutic levels associated with initial empiric IV beta-lactam and/or lipoglycopeptide therapy. 97 Once they have been stabilized, however, a switch to oral antibiotic therapy is usually appropriate.
In patients with a wound infection that has caused secondary bacteremia, clinicians can usually still switch from an IV to an oral regimen once the patient is clinically improving. 107 For bacteremia due to select virulent or difficult-to-treat pathogens (e.g., S. aureus), we generally prefer to continue IV antibiotics as supportive evidence for oral therapy is more limited. 116 Likewise, a suboptimal response of an infected wound to initial IV therapy is not a reason to avoid oral agents; rather, it is a call to investigate other causes of treatment nonresponse, such as failure to achieve source control at the infection site.
Duration of systemic antibiotic therapy
Most nonsurgical wound infections limited to soft tissue can be effectively treated with 5–10 days of systemic antibiotic therapy.73,117 Even in cases accompanied by bacteremia (other than with S. aureus), 7 days usually suffice in hemodynamically stable patients.118,119 For superficial wounds, therapy can be discontinued once the patient demonstrates a good clinical response, rather than requiring a minimum duration. For postsurgical wounds, the duration of therapy depends on the type of surgery and the adequacy of source control; national and international societies vary in several aspects of their respective guidelines for postsurgical infection management.31,120
Wound infections complicated by underlying infected bone that has not been completely eradicated surgically should be treated with 4–6 weeks of antibiotic therapy.121–123 Observational studies, and a small controlled trial, 124 suggest that shorter durations (e.g., 3 weeks) may be sufficient when no foreign material is present. Confirmatory trials of shorter duration therapy for osteomyelitis are underway. Wound infections involving retained implanted prosthetic materials (e.g., orthopedic prostheses or fixation hardware) also require prolonged therapy, with clinical trials suggesting that up to 12 weeks may be optimal.125,126
Safety and efficacy of local antimicrobials
Local antimicrobials are generally divided into antiseptics, nonselective local-administered agents with a wide spectrum of activity, and antibiotics, which usually target specific sites within only certain bacterial cells.127,128 Local antibiotics are usually applied to infected skin or soft tissue, but some can also be administered intraosseously. 129 They may be used alone or combined with systemic antibiotic therapy. The topical route of therapy has several potential advantages for treating wound infections: application is easy; most agents are relatively inexpensive; they attain a high local concentration in infected tissue 130 ; and the negligible systemic absorption limits the potential for organ toxicity and disturbance of the gut microbiome. Downsides of topical agents include their potential for local irritation or allergic contact dermatitis; like systemic antibiotics, they can contribute to the development of antimicrobial resistance.
Studies on the efficacy of topical antimicrobials in non-burn-wound infection are sparse and largely translational. While low-certainty evidence suggests that the use of antimicrobials, compared with non-antimicrobials, wound dressings might improve wound healing in patients with DFUs, it is insufficient to recommend routine use of topical therapies in infected wounds.31,131,132 Topical antimicrobials are also frequently prescribed as prophylaxis in clinically uninfected wounds, but other than for burn wounds,133–135 there is little supportive evidence for this practice. One Cochrane systematic review suggests that the use of antimicrobial versus non-antimicrobial wound dressings in DFUs may lead to a better rate of wound healing, albeit with a low certainty of evidence. 132 Topical antimicrobials may have a role as a sole agent for treatment of selected, mild, superficial infections. 136
Potential indications for antimicrobial prophylaxis or suppressive therapy
Antibiotic prophylaxis is primarily useful when administered as short-duration, narrow-spectrum therapy given immediately preceding invasive surgical procedures.137–141 This is usually a single dose of an IV beta-lactam (e.g., cefazolin), which may optimally prevent surgical site infection (SSI), but the choice of prophylaxis can vary depending on the type of procedure, its duration, local microbiological epidemiology, and patient factors (e.g., drug allergies, comorbidities). 142 No strong data support administering antibiotic prophylaxis for several days in patients with an uninfected open wound.
A key issue is when the skin barrier will be re-established, either by surgical closure or secondary intention. Prolonged antibiotic therapy predisposes to colonization with organisms resistant to the agents used, increasing the risk for wound infection with difficult-to-treat pathogens.143,144 We believe that for most invasive procedures, giving antibiotic prophylaxis beyond the immediate postoperative period is more likely to result in harm than benefit and advocate for limiting this practice to situations where it is supported by high-quality data.
Antimicrobial stewardship: key role and basic principles
The practice of antimicrobial stewardship is gaining momentum in wound management, following increasing recognition that clinically important antibiotic-related adverse events (i.e., those necessitating therapy modifications) occur in 5–20% of cases.145,146 Numerous retrospective and prospective studies have shown the potential for stewardship interventions, compared with standard prescribing practices, to reduce the prescribed antibiotic-related spectrum, duration of treatment, reliance on IV administration, antibiotic-related adverse events, proliferation of MDR organisms, and costs, without increasing the risk of clinical failure. 147
The best stewards of antimicrobial therapy first aim to avoid prescribing antibiotics when they are not clearly needed. When they are, the steward chooses the most targeted-spectrum regimen appropriate, preferably given by the oral (or occasionally topical) route, for the shortest duration likely to be effective. 99 In wound infection, a key stewardship principle is that antibiotic treatment duration is based on resolving the infection, not closing the wound, which usually takes considerably longer. 96
Antimicrobial stewardship in wound care is best provided by an interdisciplinary team, optimally including internists, infectious diseases and microbiology experts, wound care specialists, surgeons, pharmacists, and nurses. 99 There are two main types of antibiotic stewardship interventions: persuasive methods, which are aimed at educating health care providers by advising about antimicrobial therapy and giving constructive feedback, and restrictive methods, which administratively constrain how clinicians may prescribe (e.g., by limiting specific agents or instituting automatic stop orders for antibiotics). 99 Ideally, before being adopted, those instituting stewardship interventions should solicit input from health care authorities, clinician colleagues, patients, and other stakeholders.
Novel antimicrobial strategies
While the traditional approaches described above remain the cornerstones of management of wound infections, several emerging novel approaches are garnering interest. The use of bacteriophages to target specific bacteria offers a potential alternative for multidrug-resistant or refractory infections. 148 The main difficulties regarding phage therapy for wound infections are their tendency to be polymicrobial and to have iterative change in their microbiology, especially during antimicrobial therapy. We know of no convincing, large epidemiological studies showing a benefit of phage therapy for wound infection, but it might be considered in exceptional circumstances where chronic infections due to MDRO pathogens have failed traditional therapies. 149
Other novel antimicrobial strategies being investigated for treating wound infections include biofilm disrupting chemical substances (e.g., polypeptides and surfactants),150,151 newer drug delivery systems (e.g., polymers,152,153 liposomes, 154 hydrogels, 155 bone cement, 156 and metal chelation 157 ), and physical therapies (e.g., cold atmospheric plasma 158 and photodynamic therapy 159 ). Hyperbaric oxygen therapy has been used to manage wounds for decades, and studies suggest it accelerates wound healing, especially in ischemic areas.160,161 For infections, it is currently approved for treating clostridial myositis/necrosis, necrotizing soft tissue infection (NSTI), and refractory osteomyelitis, but its role in helping resolve infection in wounds remains unclear.99,113
Clinically summary
Empiric antibiotic therapy should target likely pathogens and should be rapidly changed based on culture data to the most targeted and well-tolerated regimen appropriate, ideally given orally, for the shortest appropriate duration (typically no more than 7–10 days unless deeper bony structures and/or implanted foreign materials are involved). Prophylactic antibiotics should be limited to short, targeted perioperative use. These preferences reflect antimicrobial stewardship—using antimicrobials judiciously to protect patients from the excess cost, drug toxicities, and poor outcomes associated with infections due to drug-resistant pathogens.
MANAGEMENT OF SPECIFIC INFECTIONS
Soft tissue wound infections usually require a combination of surgical and antimicrobial treatment. While enzymatic or hydro-excision debridement may suffice for superficial necrosis and contamination, most wound infections require surgical debridement to healthy tissue with irrigation and drainage of deep-seated purulence. When a wound is acceptably clean, it should be closed by suturing, skin graft, or a flap if possible; early and adequate closure of acute wounds is key to preventing chronic wounds. Below we discuss treatment considerations specific to individual wound infection syndromes.
Recommendations
Track each SSI by type of procedure, hospital area, and performing surgeon, and provide regular feedback on their rates to the relevant hospital areas and clinicians.
Standardize surgical site preparation, surgical technique, and postoperative wound management in accordance with the most recent validated recommendations.
To diagnose burn wound infection, use consensus definitions, such as those of the American Burn Association (ABA).
In burn wounds, early surgical excision is the mainstay of infection prevention and treatment. Reserve systemic antimicrobial therapy for patients who have clinical signs of infection (i.e., purulence, inflammation/invasion of adjacent healthy tissues, graft loss, or sepsis).
Debride wounds that have heavy microbial contamination or extensive soft tissue destruction/devitalization up to viable tissue.
When infection develops at the site of implanted material, presume the implant is involved and treat accordingly, until evidence suggests otherwise.
Surgical site infection
One of the universal considerations of the surgical team is to minimize avoidable surgical complications, particularly SSI. Rates of SSI vary from 2.5% in wounds characterized as “clean” to 11.8% in those considered “dirty.” 162 A landmark study of 62,000 patients at a Calgary hospital elucidated the primary risk factors for intraoperatively acquired SSI, which have been confirmed in many subsequent studies. 163 These include whether the index surgery occurs at clean site (versus clean-contaminated or dirty), the adequacy of preoperative skin preparation, adherence to optimal sterile surgical practices, and the durations of both surgery and preoperative hospitalization. 163 Core strategies for minimizing SSI include optimizing the patient’s preoperative condition (e.g., improving glucose control in patients with diabetes); deferring nonemergency procedures to an optimal time, when possible; employing minimally invasive (e.g., endoscopic) surgical approaches; matching the most difficult operations with the most skilled/experienced surgeons; and providing feedback about local SSI data to the relevant departments, teams, and/or individual surgeons. Future advances in SSI prevention will likely involve the use of predictive modeling to more effectively risk-stratify patients and identify those for whom surgery should be deferred, delayed, or performed with enhanced precautions.164,165
Clinicians who manage wounds should be aware that polymicrobial NSTI (sometimes called Meleney’s gangrene or progressive bacterial synergistic gangrene) is a rare but dire complication. 166 This infection, caused by polymicrobial flora often including S. aureus and/or beta-hemolytic streptococci, usually arises 1–2 weeks after surgery or trauma. Because it typically spreads rapidly and destroys surrounding tissues, quick recognition and treatment with both extensive debridement and systemic antibiotic therapy are required to avoid major amputation or mortality. Consider NSTI in patients with pain out of proportion to findings on examination, wound crepitus, rapidly developing tissue necrosis, or systemic symptoms after surgery.
Burn wounds
Deep-, partial-, and full-thickness burns (formerly called second and third degree, respectively) may become covered by an eschar, which is a layer of coagulated dead skin often colonized by bacterial skin (and potentially oral or fecal) flora. In small burns (less than about 5% of body surface area), local tissue and systemic host defenses can usually contain this contamination, and the dead skin will loosen and slough. In larger burns, purulent infections may develop under the eschar as host defenses are overwhelmed, producing sheet-like abscesses that can lead to life-threating sepsis if not promptly removed. Thus, burn wound treatment is directed toward eschar removal, followed by skin grafting. This is usually done with mesh autografts, but if sufficient amounts are not available, allo- or xeno-grafts can serve as temporary skin replacements.
Prevention of burn wound infection is critical for optimizing outcomes in burn patients. In addition to wound cleansing, treating patients with large burns with universal infection control precautions and in isolation rooms when performing procedures may help prevent infection. 167 Early excision (within 1–7 days) and wound closure are among the greatest advances in burn care.168,169 Recently, enzymatic debridement with bromelain-based topical agents has been shown to help remove eschar and potentially reduce the incidence of infection.168,170,171 Enzymatic debridement is an alternative to surgical excision in selected patients for whom the latter approach is not available or desirable. Routine prophylactic systemic antibiotic therapy is not recommended for burn wounds and may increase the risk of antibiotic resistance. 172 Burn wounds should initially be cleansed and then covered with an antimicrobial cream or dressing. While topical antimicrobials do not reliably prevent burn wound infection, they can be useful to buy time to allow for burn eschar debridement and mesh grafting, which is the preferred method of infection prevention.
A central challenge to advancing burn wound care is that there is no single, widely accepted, and validated definition of an infected burn wound. 173 The 2007 ABA consensus on burn wound infection suggests categorizing burn wounds as colonized or infected, based on quantitative cultures (>105 colony-forming units/gram of tissue defined as infected), with a third category of “invasive infection,” which refers to suppurative separation of eschar, tissue graft loss, invasion of adjacent unburned tissue, or sepsis. 174 Unfortunately, quantitative cultures are unavailable at many centers and take days to complete, and the benefit of treating wounds based on cultures alone is unproven. Practically speaking, clinical signs and symptoms are the most useful method for diagnosing infection of a burn wound at the bedside. Specifically, a change in wound color or conversion from a partial thickness to a full thickness wound is correlated with infection. 173 Biopsies for tissue histopathology and culture, where feasible, can be useful in selected cases to confirm or further characterize burn wound infections.
The microbiology of infected burn wounds varies by wound location and duration. Immediately after injury, burn wounds typically harbor few bacteria, but they invariably become colonized over the following days to weeks. Observational data suggest gram-negative bacteria predominate in infected wounds. 175 In large burns (>20% of total body skin area), which can be associated with significant immunosuppression, fungi and molds may also colonize wounds and can result in invasive infections.
Appropriate treatment of infected burn wounds may include topical antimicrobials, systemic antibiotics, or surgical excision, depending on the type of infection and the wound depth. Infected burn wounds should be cleaned, debrided, and dressed, usually including with topical antimicrobials. Surgeons should excise eschar to healthy tissue, and re-excisions are often necessary when patients have invasive infection, particularly if caused by fungi. Patients with fever, leukocytosis, or signs of sepsis should be treated with systemic antibiotics; so too should those with a large or spreading area of cellulitis surrounding a burn. Whenever possible, antimicrobial therapy should be directed toward a specific organism rather than being unfocused or broad-spectrum. Wound swab cultures, while not ideal, can help guide treatment when quantitative culture of a tissue sample or histopathology is not available.
Foot infections in people with diabetes
The combination of peripheral neuropathy (leading to reduced protective sensation and musculoskeletal foot deformities) and PAD (leading to poor perfusion) makes diabetic patients particularly prone to developing foot ulcers. These, coupled with diabetes-related impaired immune responses, frequently lead to infection. 31 Infection is defined by clinical findings of inflammation, which can be supported by laboratory testing (WBC, ESR, CRP, PCT) and imaging (plain X-rays to start, moving to advanced studies if necessary). Ulcer infections generally begin with mild severity (defined by only limited lateral spread and depth) but are often not detected until the severity is moderate (characterized by attaining subcutaneous depth or extensive spread) or severe (being accompanied by findings suggesting systemic infection). The two higher levels of severity are often accompanied by contiguous osteomyelitis.
Treatment starts with wound cleansing, debridement of devitalized and infected tissue, and collecting specimens (preferably tissue and bone when osteomyelitis is suspected) for culture; the IWII’s recent guidance paper on wound and skin cleansing addresses these topics in greater detail. 176 Assessing the extent of infection is critical in formulating a strategy and determining its efficacy. Next, clinicians should select an empiric antibiotic regimen based on the severity of infection, review any current or recent antibiotic therapy, the local microbiologic epidemiology, and any relevant patient comorbidities. The latest IWGDF/IDSA guidelines on DFIs and a recent systematic review and meta-analysis offer more detailed guidance on evidence-based empiric and definitive antibiotic treatment.31,109
In every case, the clinician should consider if surgical treatment of a DFI is required, and nonsurgeons should seek surgical consultation if in doubt. In recent years, surgeons have moved toward using more “conservative” (less-aggressive or destructive) surgical procedures in an effort to avoid or limit the level of any required amputations and preserve tissue to improve patient mobility. When amputation is necessary, early wound closure, achieved primarily with a graft, or flap, can help control infection and hasten healing.
Infections complicating PAD
Patients with a foot ulcer or dry gangrene complicated by both infection and PAD have a greatly increased risk of limb loss. 177 Multidisciplinary evaluation by both a foot specialist and vascular specialist is best for determining the optimal timing for surgical drainage, debridement, and/or revascularization.
The severity of both ischemia and infection should be evaluated using a verified classification system, such as the Society for Vascular Surgery Wound, Infection, Ischemia (WIFi) classification system.24,61 In patients with falsely elevated ankle-brachial index due to medial calcinosis, evaluate PAD severity with noninvasive assessments, such as the toe-brachial index, transcutaneous tissue oxygen tension (TcPO2), or skin perfusion pressure (SPP). Toe pressure ≥30 mmHg, TcPO2 ≥25 mmHg, and SPP ≥40 mmHg are associated with higher rates of healing.177,178 Perform vascular assessments in patients with no palpable pedal pulses, those with gangrene, or when an ulcer fails to improve despite adequate infection control and drainage.31,178
Surgical timing should be guided by whether infection or ischemia is the dominant presentation. In patients with severe foot infection (including abscesses), prioritize incision and drainage for source control, followed by revascularization and any required definitive foot procedure. 31 In patients with severe ischemia and no immediate need for drainage, perform revascularization first, optimizing perfusion for wound healing before the podiatric procedure. 178
Infections in pressure ulcers
Pressure ulcers occur mainly in patients with paralysis or who are bedridden for prolonged periods. Old age, inadequate level of support for activities of daily living at home, and malnutrition are also contributing factors. Ulceration typically follows pressure on the skin overlying bony prominences that reduces blood flow, especially when accompanied by friction, shear, or moisture. As pressure continues over time, skin changes progress from nonblanchable erythema, to partial thickness skin loss, to full thickness skin loss, to necrosis in deeper tissues and eventually bone. 179 Open wounds quickly become contaminated and then colonized by polymicrobial flora, often followed by local infection, which can then become deep (involving and eventually eroding the bone surface) or systemic. 180
Treatment consists of pressure off-loading, cleansing, and debriding the wound, and, if possible, flap closure when the wound is acceptably clean. Routine application of topical antimicrobials, especially as prophylaxis for uninfected wounds, is not recommended. Systemic antibiotics should generally only be given for acute soft tissue or deep wound infections, judiciously and briefly (generally for ≤1 week), preferably based on deep tissue culture results.179,181 Diagnosing and treating osteomyelitis underlying a pressure ulcer is generally useful only after the wound has been surgically debrided and closed. When the infection has spread to the medullary canal and necrotic bone or sequestrae are present, surgical debridement is typically necessary for cure. In other cases of pressure ulcer-related osteomyelitis, prolonging antimicrobial therapy beyond what is needed to treat any acute soft tissue component of infection does not clearly improve long-term outcome and may cause antibiotic-associated harms.181–183 Infected soft tissue in pressure ulcers often heal with an appropriate short course of antibiotic therapy followed by appropriate wound care, but closure typically takes weeks to months.
Implant-related wound infections
Orthopedic implant-related wound infections
Differentiating between superficial and deep infections at the site of orthopedic implants is crucial, but difficult in practice. Multiple studies have found that patients diagnosed with a “superficial” postoperative infection overlying an implant are often later diagnosed with deep infection.184,185 Implant-related infections may initially present with only superficial signs, such as localized erythema, edema, and warmth. Other clinical signs that suggest an implant-related infection include delayed wound healing, late wound dehiscence or breakdown, formation of local sinuses or abscess, and recurrent episodes of “superficial” infection. The European Bone and Joint Infection Society categorizes suspected implant-related infections as “infection confirmed,” “infection likely,” or “infection unlikely,” based on established periprosthetic joint infection definitions. 186 In cases of fracture-related infections, the diagnosis may be supported by either confirmatory or suggestive criteria, as defined in a recent international orthopedic consensus. 187
Select antibiotic therapy for orthopedic implant-associated infections based on the results of deep tissue or synovial fluid cultures. When an infected implant will be retained, prolonged antimicrobial therapy (12 weeks, or more as a suppressive approach) may be required. 125 Surgical treatment options encompass a range of strategies, including debridement, antibiotics, and implant retention; one- or two-stage revision (exchange) procedures; complete removal of the implant without later replantation; or amputation. The optimal surgical approach is based on multiple factors, including the integrity of the surrounding bone and soft tissues, stability of the fracture construct (for fracture-related infections), the overall health of the host, and the specific characteristics of the causative microorganisms.188,189 Importantly, infections around endoprosthetic or joint replacement implants differ from fracture implants in that the former are intended to last the lifetime of the patient. Even low-grade infections often cause chronic pain and eventually implant loosening and failure. 190 Thus, wound issues in the postoperative period often require aggressive treatment with surgical debridement, sometimes with partial or complete implant exchange, and culture-directed antibiotic therapy.
Other implant-related wound infections
Risk factors for nonorthopedic-implant-related infections are similar to those for infections in other types of operations and include smoking, obesity, prior local radiation therapy, prior same-site surgeries, and longer operative times. Treatment of implant-associated infections, in addition to antibiotic therapy, generally consists of removal of the implanted material if feasible, along with irrigation and open drainage. The wound may sometimes be closed after implant removal and irrigation, but it often takes days to weeks before the infection clears sufficiently to allow closure.
Clinically summary
The treatment of wound infections varies considerably by the specific syndrome, but common themes include the need to drain purulence, debride dead and poorly viable tissue, and close wounds quickly to address infections and prevent recurrence. When wound infections complicate underlying tissue healing comorbidities (e.g., open pressure ulcers, peripheral vascular disease, or the sequelae of uncontrolled diabetes), controlling these is paramount to durably curing the superimposed infection. For implant-related wound infections, it is most critical to determine whether there is deep infection involving the implant, and if so the most appropriate surgical management of said infected implant.
Recommendations
Define successful treatment of an infected wound by resolution of the signs and symptoms used to diagnose the infection. Wound healing is an important clinical outcome that is related to, but separate from, resolution of infection.
Differentiate recurrences of infection in an initially successfully treated wound as either a relapse (failure to eradicate the initial pathogens) or reinfection (caused by introduction of a different pathogen).
When a satisfactory clinical response is not possible (e.g., inability to achieve source control), establish a treatment plan, such as expectant management with symptom control, antibiotic retreatment, or antibiotic suppression, based on available resources and patient/family preferences.
DEFINING TREATMENT RESPONSE
Diagnosis of infection in a wound requires identifying specific clinical signs or symptoms, so it is logical to define a response to treatment by the resolution of the findings used for its diagnosis. In assessing the clinical response to therapy, clinicians should separate evidence of resolution of wound infection from that of wound healing, usually defined as complete epithelial closure. Wounds that appear clinically uninfected after a course of therapy are often not yet healed; conversely, a wound may fully re-epithelialize despite having persistent evidence of infection. 191 When confronted with a persistently nonhealing wound despite successful treatment for infection, the clinician should consider what noninfectious factors might be contributing to the poor healing.
Inadequate medical or surgical therapy may lead to persistent or recurrent wound infection. If a wound infection is correctly diagnosed and treated with an appropriate antibiotic regimen, the expected result is clearance of the pathogen(s), leading to resolution of clinical evidence of infection. Poor response of an infection to targeted therapy may have many causes, including inadequate source control (e.g., unresected necrotic tissue, undrained abscess), infection with an antibiotic-resistant pathogen, therapy with an antimicrobial regimen with inadequate dosing or duration, or patient nonadherence (e.g., with taking antibiotics, wound off-loading, or wound care). When a wound fails to respond to antibiotic therapy, has negative cultures, worsens with surgical debridement, or has atypical features (e.g., violaceous border, undermined edges, chronic painless course), clinicians should also consider misdiagnosis of other conditions masquerading as an infected wound (e.g., pyoderma gangrenosum, Marjolin’s ulcer, hidradenitis suppurativa, or calciphylaxis).192,193 When confronted with a wound that has responded poorly to treatment, clinicians should consider reinvestigating for missed or inadequately treated deeper infection; this usually begins with obtaining new optimal-quality cultures, and questioning the original diagnosis (Fig. 2).
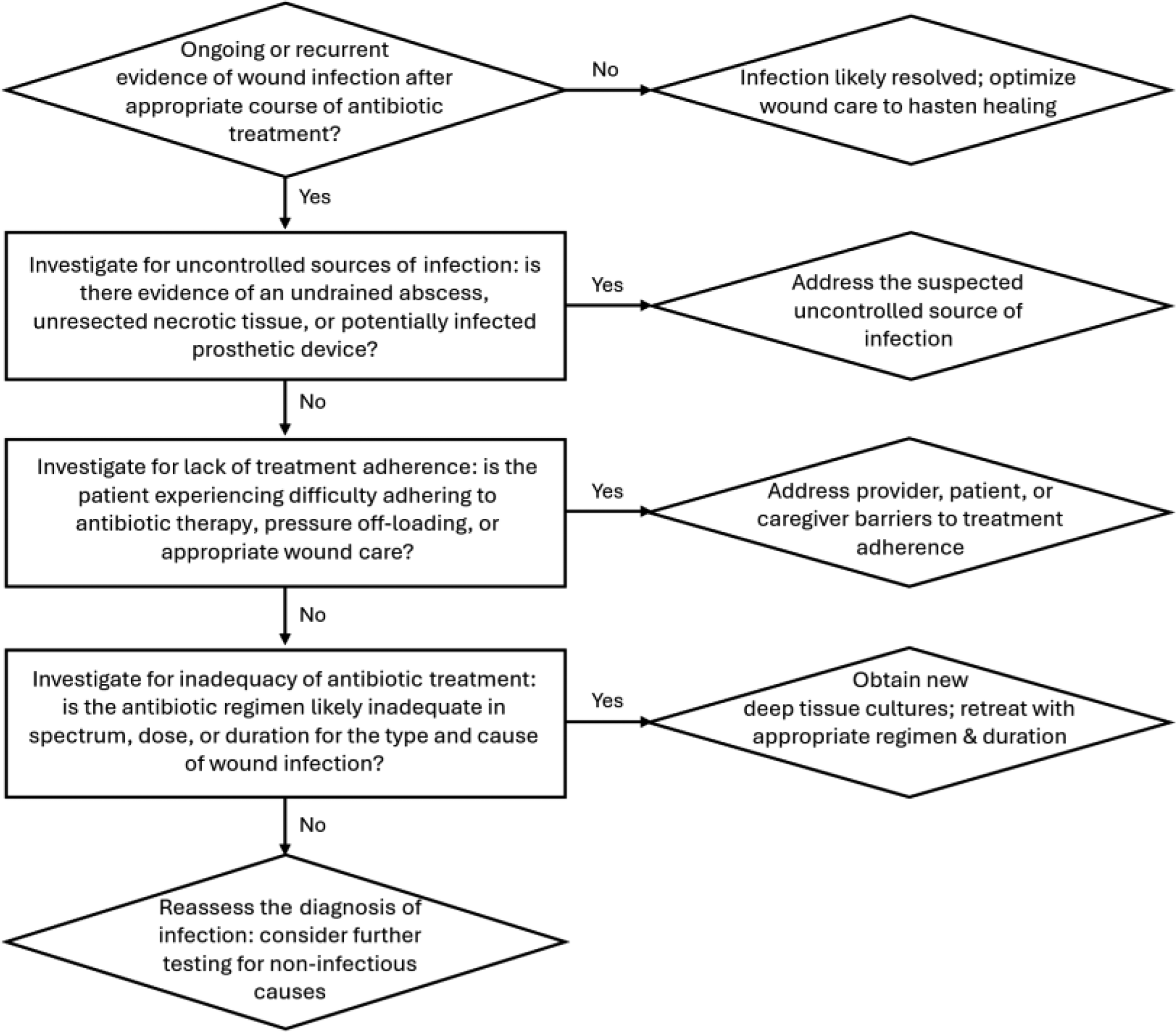
Systematic workflow for evaluating antibiotic treatment failure in wound infection.
Infection recurrences (onset of new clinical findings after apparent resolution of an infection) can be further divided into those that represent a relapse (caused by a failure to eradicate the initial pathogen[s]) or reinfection (caused by introduction of a different pathogen in the same wound site). This distinction is important because the former usually suggests inadequate source control or deeper infection than was originally diagnosed.
In some instances, a wound infection may appear to be unlikely to be eradicated, or the consequences of trying to do so may be worse than the infection. In such situations, the treating clinicians must devise a strategy to try to relieve troublesome symptoms and prevent further complications. This should be individualized to the patient’s specific scenario and account for (via shared decision-making) the preferences and values of the patient and their caregivers. Such plans may include local approaches (e.g., debridement, wound care, topical antimicrobial therapy), suppressive systemic antibiotic treatment, 194 or surgical extirpation of as much necrotic and infected material as possible, up to and including amputation.
Clinically summary
Successful treatment of a wound infection is defined by the resolution of the inflammatory signs that led to its diagnosis, but importantly, not by wound healing per se—wounds whose infections have resolved often remain unhealed, and wounds may heal during antibiotic therapy despite underlying uncontrolled infection. When wound infections fail to respond to initial treatment, clinicians should consider whether the patient has not had adequate source control, has a drug-resistant pathogen, or has not had adequate drug exposure (e.g., due to suboptimal dosing or incomplete medication adherence); if none of these complicating factors are present, they ought to consider whether they might be dealing with a wound infection mimic, such as malignancy or pyoderma gangrenosum. In some instances (e.g., infection of orthopedic hardware that cannot be safely removed), it may not be possible to eradicate deep-seated wound infection; such cases require an individualized approach using alternative approaches ranging from chronic suppressive antibiotic therapy up to surgical amputation.
CONCLUSIONS AND FUTURE DIRECTIONS FOR WOUND CARE RESEARCH
The intention of this consensus document was to succinctly distill the most clinically important aspects of a large and complex topic. We have summarized our main conclusions, based on our review of the literature and collective personal experiences, in the recommendations provided in each section.
Many fundamental questions and presumptions within wound infection management are based on expert opinion, in vitro or animal model data, or a limited body of unreplicated and oft-conflicting observational studies. These include such examples as the importance of biofilm and biofilm-based treatment strategies in determining rates of infection recurrence and wound healing, and the utility of local antiseptics and antibiotics alone versus in combination with systemic antibiotics for infected wounds. Therefore, much of the dogma of wound infection care should be subjected to testing in comparative, prospective, and randomized studies. Below, we outline what we believe are major unresolved issues and open questions that need to be addressed to move the field of treatment of infected wounds ahead.
Beginning with diagnosis, we need to develop internationally accepted consensus definitions for each major subtype of wound infection; these should be easy to use, readily applicable in the clinic or at the bedside, and objective enough to ensure high interrater reliability. Retrospective data could be collected to help build scoring systems that predict the risk of treatment failure and need for unplanned surgical intervention in as yet inadequately studied types of wound infections (e.g., sacral pressure or burn wounds). These systems should then be subjected to prospective studies to assess their validity. particularly how well they identify patients likely to benefit from early invasive interventions (e.g., revascularization, surgical debridement, removal versus retention of implanted prosthetic material). In addition to benefiting patient care, such tools could standardize and greatly improve the generalizability of future wound infection research.
A problem in building wound infection scoring systems is that there is currently no reference criterion standard for determining when a wound is infected. Nor is there even universal consensus on what defines a “healthy” (presumably uninfected and moving toward healing) versus a “subclinically infected” wound or if this is a clinically meaningful distinction. To ensure higher-quality future studies to facilitate approval of new drugs and other therapies for wound infection, we must develop a rigorous and clinically useful reference standard for their diagnosis. Specially, retrospective observational data from a large wound care center cohort using natural language processing methods to extract data from clinical documentation might identify whether specific physical examination findings traditionally associated with “subclinical infection” are associated with progression to overt infection or failure of wound healing. If so, a prospective randomized study could evaluate whether patients with such findings (but no signs of overt infection) achieve better clinical outcomes when systemic antibiotics are added to local wound care and topical antimicrobial therapies.
Also, in the realm of diagnostics, we need further research to define the proper role of molecular microbiological testing in identifying pathogens, including obligate anaerobes, and informing antimicrobial treatment for wound infections. Most molecular diagnostic tests have been used for diagnosing infections occurring in normally sterile sites, such as multiplex PCR panels for bacteremia and meningitis, where positive results for virulent organisms almost always reflect true disease. For wound infections, which are typically polymicrobial and exist on a spectrum from colonization to infection, this will not be the case. Prospective randomized studies in which patients undergo both traditional culture and PCR-based testing for their wound infection, then receive antibiotics solely based on the culture results versus also based on the PCR results, could clarify the utility and/or potential harms of PCR-based treatment.
Regarding treatment strategies, we need more rigorous, well-designed, randomized clinical trials to assess the most appropriate therapies for wound infection. Specifically, rather than relying on more industry-sponsored trials of new proprietary wound dressings and treatments, we need studies aimed at definitively addressing basic questions in wound infection management. These include randomized comparative studies of topical versus systemic antibiotic therapy for localized (nonsystemic) wound infections, trials evaluating shorter durations of therapy for various wound infection subtypes, and studies evaluating the efficacy of lower-cost treatment strategies for the millions of patients dealing with wound infections in low-resource settings. Finally, we need large observational or quasi-experimental pre/postintervention studies to define which antimicrobial stewardship interventions (e.g., reducing empiric anti-pseudomonal, anti-anaerobic, or anti-MRSA coverage in treatment regimens) best produce clinical value—that is, reducing antibiotic-related adverse events, improving treatment-related quality of life, providing better clinical outcomes, and lowering treatment-related costs.
National and international societies whose members are interested in managing issues related to wound infection should codevelop recommendations for future research and funding in this area. These recommendations could identify important topics for which consensus is lacking, focus on new and inadequately studied agents and technologies for diagnosing and treating infected wounds, and incorporate input from wound infection advocacy groups and patients.
AUTHOR DISCLOSURE AND GHOSTWRITING
The following authors report relevant disclosures: L.K.S.P. previously consulted with Pathnostics. P.K. reports associations with UrgoMed Inc. and Solventum Inc. All remaining authors: nothing to disclose. No ghostwriting services were used.
ABOUT THE AUTHORS
Footnotes
ACKNOWLEDGMENTS AND FUNDING DISCLOSURES
None of the authors received financial or other compensation for this work. Publication-related costs were funded by the WHF. This consensus effort was coconceived with, and is posthumously dedicated to, Dr. Gregory Schultz, a prolific researcher and mentor who devoted his career to advancing our understanding of how wound infections arise and how best to treat them. The work is also dedicated to Dr. Paul Liu, who coauthors posthumously.