
Abstract
Objective:
Burn injuries affect millions globally, with increasing survival rates due to advances in acute care. However, long-term cardiovascular outcomes including major adverse cardiovascular events (MACE), venous thromboembolism (VTE), and mortality in burn survivors remain under-investigated.
Approach:
We conducted a retrospective propensity score–matched cohort study using the TriNetX US Collaborative Network. Individuals aged 18 years or older who had an emergency department visit or hospitalization with a diagnosis of burn injuries occurring between January 1, 2014, and January 1, 2019, were identified and matched 1:1 to nonburn controls who were selected based on similar demographics, comorbidities, and medications. The primary outcomes were the hazard ratios (HRs) and absolute risk differences (ARDs) of MACE, VTE, and mortality occurring between 3 months and 5 years after the index date. Secondary cardiovascular and thromboembolic endpoints included the HRs and ARDs of coronary artery disease (CAD), cerebrovascular disease (CVD), pulmonary embolism (PE), and deep vein thrombosis (DVT).
Results:
A total of 71,426 propensity score–matched pairs of burn survivors and nonburn controls were included. Burn survivors had significantly elevated risks of MACE (HR 1.95, 95% confidence intervals [CI] 1.84–2.07; ARD 0.9%), VTE (HR 1.99, 95% CI 1.80–2.19; ARD 0.4%), and all-cause mortality (HR 2.29, 95% CI 2.10–2.49; ARD 0.7%) compared with controls. Increased risks were also observed for CAD (HR 1.85, 95% CI 1.72–1.98; ARD 0.5%), CVD (HR 2.05, 95% CI 1.88–2.24; ARD 0.5%), PE (HR 2.09, 95% CI 1.77–2.47; ARD 0.1%), and DVT (HR 1.96, 95% CI 1.69–2.27; ARD 0.1%).
Innovation:
We demonstrate that burn injury is associated with sustained long-term cardiovascular and thromboembolic risks up to 5 years after injury.
Conclusions:
These findings establish burn injury as a chronic condition, requiring routine cardiovascular screening and targeted prevention in long-term care.
Sheng-Hsiang Ma, MD

Cian-Hao Ye, MD

INTRODUCTION
Burn injury is a major global public health concern, affecting millions of people each year. In 2019 alone, approximately 9 million individuals worldwide suffered burn injuries, with roughly 111,000 associated deaths. 1 Advances in acute burn care over recent decades have significantly improved survival rates.2,3 As a result, an increasing number of burn patients survive the initial trauma, and emerging evidence indicates that many of these survivors experience chronic complications long after the burn injury.4–6 The shift in epidemiology has brought greater attention to the long-term consequences and comorbidities faced by burn survivors. 7 These include persistent pain, pruritus, hypertrophic scarring, functional impairments, neuropsychiatric disorders, as well as metabolic dysregulation, increased risk of infections and cardiovascular diseases.5,8–11
Among these long-term sequelae, cardiovascular complications have gained increasing attention in recent years, with studies suggesting that burn survivors may be at elevated risk for major adverse cardiovascular events (MACE), such as myocardial infarction and stroke, as well as venous thromboembolism (VTE).12–14 Severe burns trigger a systemic inflammatory cascade and a hypermetabolic state that can persist for months or even years during recovery. 15 This prolonged inflammatory stress state is accompanied by high circulating levels of catecholamines and cytokines, which can induce endothelial dysfunction, oxidative injury, and cardiac remodeling.16,17 Emerging evidence suggests that severe injuries, including burns, may predispose individuals to increased long-term cardiovascular risk. In a large population-based cohort study from Western Australia, Duke et al. found that adult burn survivors had significantly elevated rates of ischemic heart disease, cerebrovascular events, and heart failure compared with noninjured individuals. 18 Regarding VTE, burn patients exhibit all components of Virchow’s triad—vascular injury, stasis due to immobilization, and a hypercoagulable state—contributing to an increased risk of thromboembolic events. 12 While the acute-phase risks are well-documented, the long-term incidence of VTE in burn survivors remains unresearched.12,19,20
Despite these observations, an important knowledge gap remains in distinguishing the burden of acute hospitalization-related complications from the subsequent incidence of new cardiovascular and thromboembolic events occurring months to years after discharge. Although previous studies have characterized inpatient readmissions, acute cardiovascular complications, and burn-associated coagulopathy, the longer-term risk of incident MACE and VTE among burn survivors after the acute care period remains poorly quantified. Moreover, burn survivors are not typically considered a distinct population for long-term cardiovascular risk surveillance. Given these associations, it is imperative to investigate whether burn survivors are at increased long-term risk of these serious cardiovascular outcomes. The findings from this study aim to guide long-term surveillance strategies and preventive interventions to optimize cardiovascular health in burn survivors.
Clinical problem addressed
While advances in acute burn care have significantly improved survival, the chronic cardiovascular and thromboembolic consequences of burn injury remain poorly understood. Because existing research predominantly focuses on short-term outcomes, burn survivors are not routinely integrated into long-term cardiovascular risk assessments, leaving clinicians without data to guide postdischarge surveillance and preventive care. This study addresses this critical gap by quantifying the long-term risks of MACE, VTE, and mortality using real-world data, delivering actionable evidence for targeted survivorship care.
METHODS
Data source and acquisition
This retrospective cohort study utilized the TriNetX database, a global federated health research network that aggregates de-identified electronic health records (EHRs) from participating health care organizations, including academic medical centers and community hospitals. The network comprises longitudinal data from over 130 million patients, primarily in the United States. The platform seamlessly aggregates real-time, longitudinal clinical data directly from these integrated EHR systems. The types of data captured encompass patient demographics, clinical diagnoses, medical procedures, prescribed medications, laboratory values, and vital status. The study cohort was constructed and analyzed using the TriNetX Analytics platform, which provides access to demographics, diagnoses, medications, laboratory values, and procedures. Diagnoses were identified using International Classification of Diseases, 10th Revision, Clinical Modification (ICD-10-CM) codes, while medications were classified using standardized RxNorm codes. All data processing and analysis were conducted using the TriNetX built-in query builder and proprietary algorithms. The study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for reporting. Data collection and analysis were performed in April 2025 using the US Collaborative Network. The TriNetX platform adheres to strict data governance standards to ensure patient privacy and data integrity. TriNetX is certified to the ISO 27001:2013 standard for Information Security Management Systems (ISMS) and is fully compliant with the Health Insurance Portability and Accountability Act (HIPAA) Security Rule. All data presented in this study were de-identified and aggregated, which received a waiver of informed consent from the Western Institutional Review Board. 21 The Institutional Review Board of Far Eastern Memorial Hospital approved the study and deemed it exempt from further ethical review. Electronic laboratory notebook was not used.
Subject selection
A burn cohort was constructed using the TriNetX platform. Eligible participants were adults (≥18 years) who had an emergency department (ED) visit or hospitalization with a diagnosis of burn injuries (ICD-10-CM T20-T32) during the period between January 1, 2014, and January 1, 2019. Exclusion criteria included individuals younger than 18 years and those with a prior diagnosis of MACE or VTE before the index date. The index date for burn patients was defined as the date of their first recorded diagnosis. Detailed ICD-10 codes are provided in Table 1. A control cohort was then constructed, comprising individuals without a history of burn injury, MACE, or VTE during the same period. Patients in both cohorts were excluded if they had experienced any predefined outcomes of interest.
ICD-10-CM codes used for cohort definition, propensity score matching covariates, and outcome identification
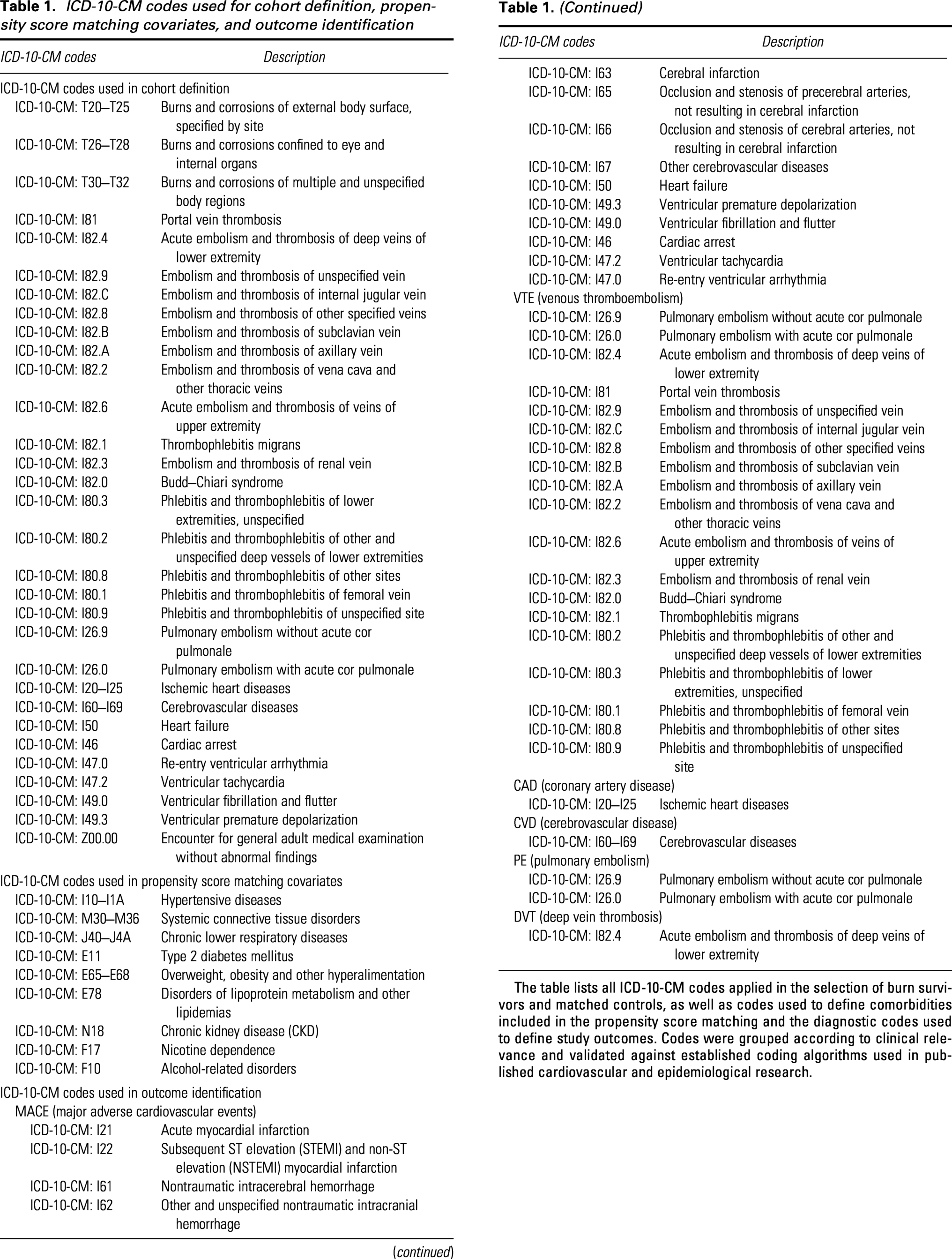
The table lists all ICD-10-CM codes applied in the selection of burn survivors and matched controls, as well as codes used to define comorbidities included in the propensity score matching and the diagnostic codes used to define study outcomes. Codes were grouped according to clinical relevance and validated against established coding algorithms used in published cardiovascular and epidemiological research.
Covariates
To account for potential confounding in the association between burn injury and the composite outcome, we incorporated a range of covariates into the propensity score models. These included age, sex, race, comorbidities, and concomitant medication use. Specifically, the research team adjusted for hypertensive diseases (ICD-10-CM I10–I1A), systemic connective tissue disorders (ICD-10-CM M30–M36), chronic lower respiratory diseases (ICD-10-CM J40–J4A), type 2 diabetes mellitus (ICD-10-CM E11), disorders of lipoprotein metabolism and other lipidemias (ICD-10-CM E78), overweight and obesity (ICD-10-CM E65-E68), nicotine dependence (ICD-10-CM F17), chronic kidney disease (ICD-10-CM N18), and alcohol-related disorders (ICD-10-CM F10). In addition, medication-related covariates included hormone therapy (VA Class HS900), antilipemic agents (VA Class CV350), platelet aggregation inhibitors (VA Class BL117), anticoagulants (VA Class BL110), and immunosuppressants (VA Class IM600). A comprehensive list of covariates and their definitions is provided in Table 1.
Outcomes
The primary endpoints were the composite incidence of MACE, VTE, and overall mortality occurring between 3 months and 5 years after the index date. To distinguish long-term systemic sequelae from the immediate physiological impact of thermal injury, we implemented a 3-month blanking period following the index event. This exclusion criterion ensures the subsidence of acute recovery phases and transient inflammatory or thrombotic effects associated with initial resuscitation. Furthermore, it serves to mitigate peri-hospitalization confounding and surveillance bias, preventing the misclassification of preexisting conditions that might be incidentally diagnosed during the index admission. Secondary outcomes included deep vein thrombosis (DVT), pulmonary embolism (PE), cerebrovascular disease (CVD), and coronary artery disease (CAD) within the same time frame. A comprehensive list of outcomes and their definitions is provided in Table 1.
Subgroup and sensitivity analyses
Subgroup analyses were conducted to evaluate the risk of MACE, VTE, and overall mortality in specific burn patient groups compared with the control cohort. These analyses were stratified by age (>65 years vs. 18–65 years), race, sex, and burn severity. Burn severity was assessed using medical visit access as an indicator of the severity of illness, based on the premise that patients with greater severity require higher levels of medical care. Those who visited the ED without subsequent hospitalization were categorized as the “ED-only” group; those who required inpatient admission were classified into the “Inpatient” group; and those whose inpatient records included critical care services within 7 days of admission were categorized as the “Critical care” group. To assess the robustness of our findings, we conducted sensitivity analyses as follows: (1) varying the outcome period by redefining the follow-up windows to 6 months to 5 years and 1–5 years after the index date, (2) expanding generalizability by using the Global Collaborative Network, (3) refining the control cohort by requiring patients to have at least three medical visits during the study period, and (4) excluding patients with documented bedridden status or limited mobility following burn injury. Finally, to evaluate the external validity of our findings across different ethnic backgrounds, a post hoc sensitivity analysis was conducted specifically for patients of Hispanic/Latino ethnicity.
Statistical analyses
All statistical analyses were performed using the TriNetX platform. Categorical variables were compared using chi-square tests, while continuous variables were analyzed using independent-sample t-tests. To reduce confounding, propensity score matching (PSM) was applied using a 1:1 greedy nearest-neighbor matching method with a caliper of 0.1 pooled standard deviations of the logit of the propensity score. Matching variables included demographic characteristics, comorbidities, and concomitant medication use (Table 1). Postmatching balance between groups was assessed using standardized differences (SDs), with SD < 0.1 indicating adequate balance. Survival outcomes were analyzed using Kaplan–Meier curves, and differences between groups were assessed with the log-rank test. The association between burn injury and clinical outcomes was evaluated using Cox proportional hazards models, which estimated hazard ratios (HRs) and 95% confidence intervals (CIs). The proportional hazards assumption was evaluated using the generalized Schoenfeld approach available within the TriNetX platform. In instances where this assumption was violated, we addressed the issue by calculating HRs separately for distinct time intervals. In addition to HRs, absolute risk differences (ARDs) and corresponding 95% CIs were calculated based on the cumulative incidence of each outcome during the predefined follow-up period. Cumulative incidence curves were generated to visualize the time-dependent risk of mortality and cardiovascular outcomes. All statistical tests were two-tailed.
RESULTS
Participant characteristics
Initially, the study identified 71,429 eligible burn patients and 4,439,760 controls. Following PSM, 71,426 patients were included in the burn cohort, matched 1:1 with 71,426 controls. The demographic characteristics, comorbidities, and concomitant medication profiles of both cohorts, before and after PSM, are detailed in Table 2. Among the participants in the burn cohort, the mean age was 36.8 years; 39,573 (55.4%) were male, and 31,848 (44.6%) were female. The major race was Caucasian (58.8%). Before matching, significant differences were observed in demographic characteristics, comorbidities, and the use of concomitant medications between burn patients and controls. Postmatching, these differences were minimized, indicating well-balanced cohorts. Among the 71,426 burn survivors included in the matched cohort, ED-only, inpatient, and critical care groups represented distinct levels of health care utilization at the index encounter. Short-term mortality demonstrated a clear severity gradient across these categories, with 3-month mortality rates of approximately 0.1% in the ED-only group, 1.1% among patients requiring inpatient admission, and 5.5% among those receiving critical care. This stepwise increase supports the use of health care utilization as a clinically meaningful surrogate for burn severity in the absence of detailed injury characteristics. Figure 1 presents a graphical summary of the study.
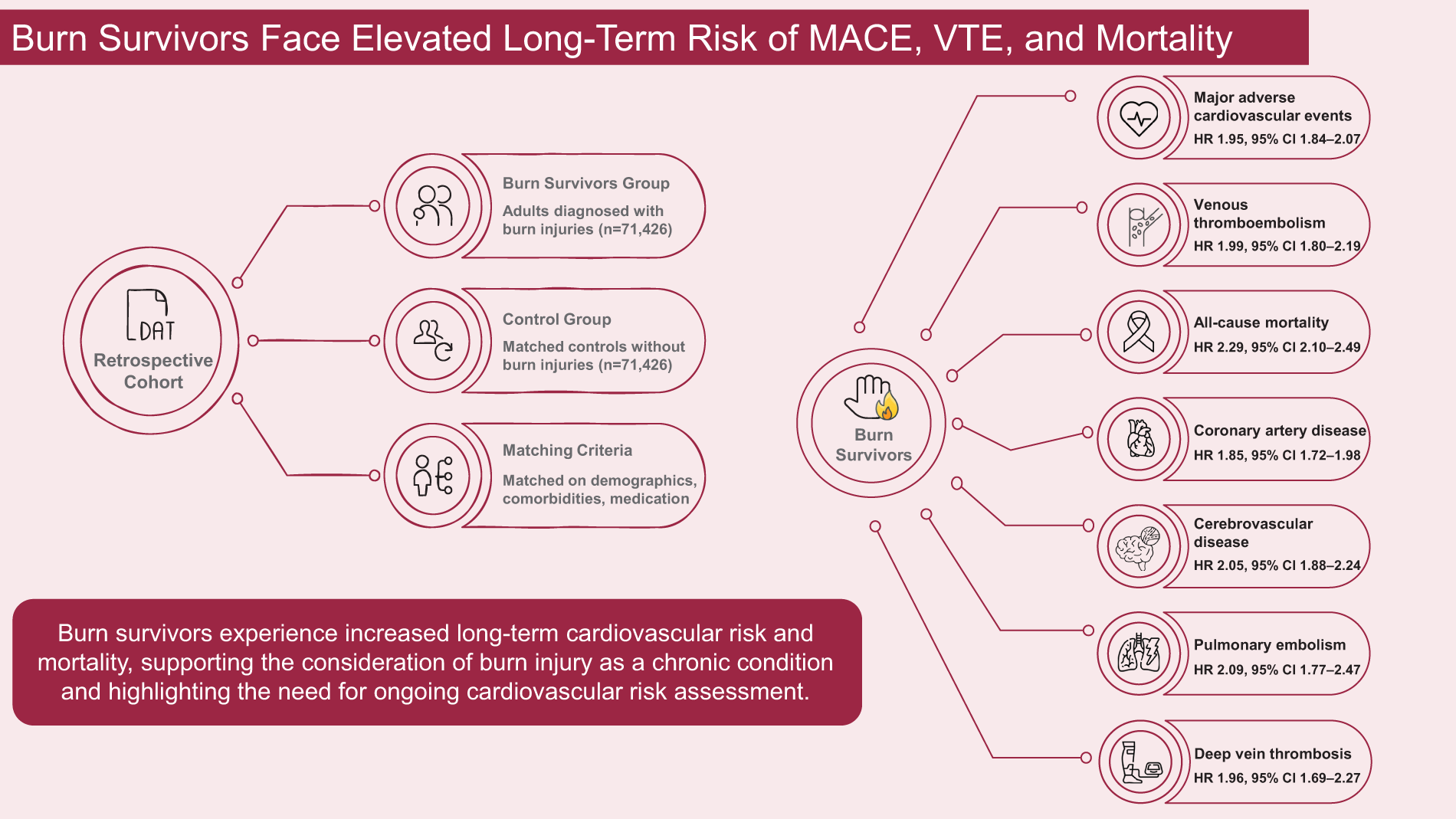
Summary graphic illustration. A propensity score–matched cohort study demonstrating increased long-term cardiovascular, thromboembolic, and mortality risks among adult burn survivors compared with nonburn controls during 3 months to 5 years of follow-up.
Baseline characteristics of study participants before and after propensity score matching
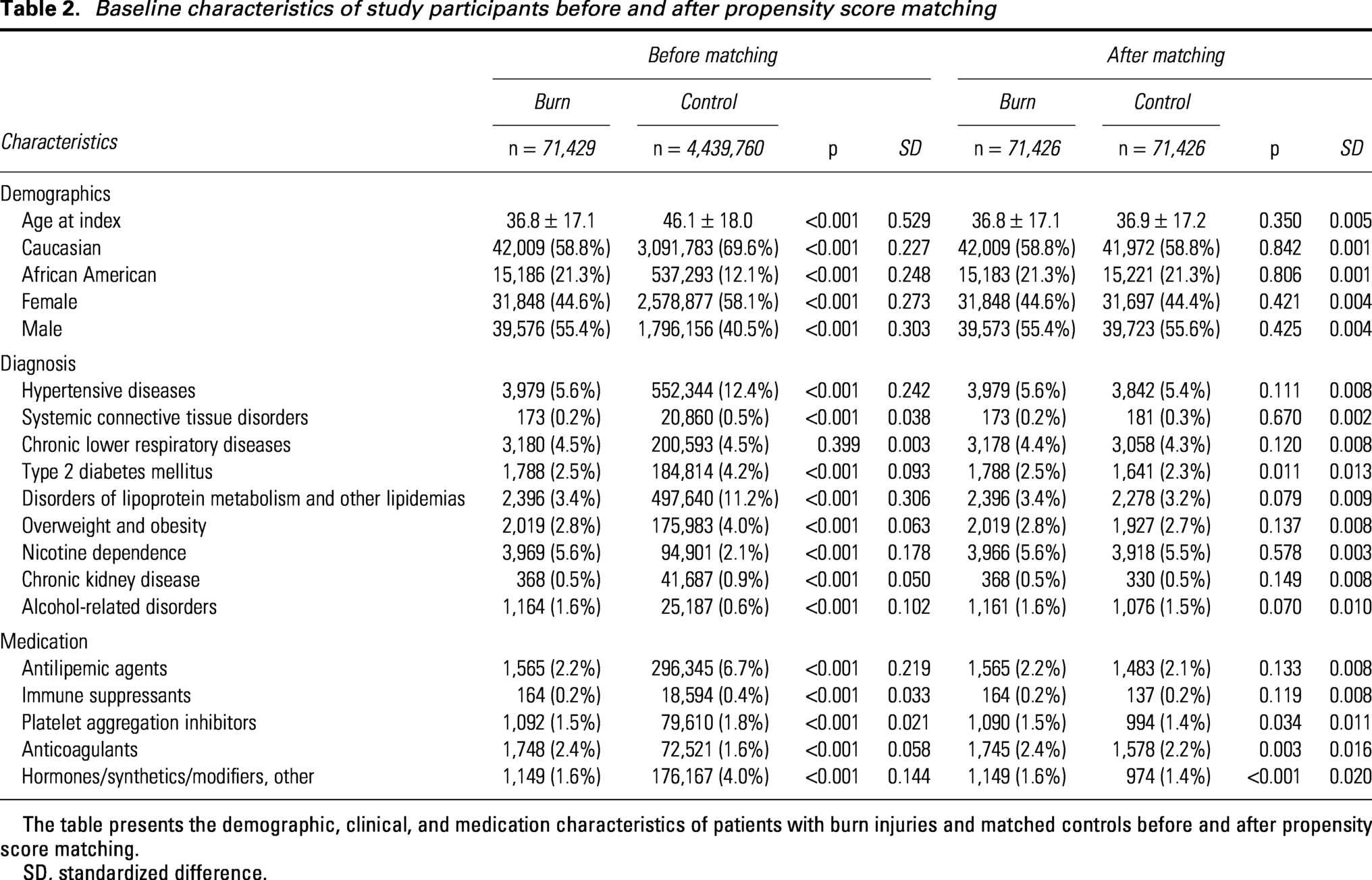
The table presents the demographic, clinical, and medication characteristics of patients with burn injuries and matched controls before and after propensity score matching.
SD, standardized difference.
Primary and Secondary Outcomes
Figure 2 presents the number and percentage of patients experiencing each outcome in both cohorts, together with the ARDs and corresponding HRs over the 3-month to 5-year follow-up period. Burn survivors demonstrated significantly higher risks of MACE (HR 1.95, 95% CI 1.84–2.07; ARD 0.009, 95% CI 0.007–0.011), VTE (HR 1.99, 95% CI 1.80–2.19; ARD 0.004, 95% CI 0.002–0.005), and all-cause mortality (HR 2.29, 95% CI 2.10–2.49; ARD 0.007, 95% CI 0.006–0.008). Elevated risks were also observed for CAD (HR 1.85, 95% CI 1.72–1.98; ARD 0.005, 95% CI 0.004–0.007), CVD (HR 2.05, 95% CI 1.88–2.24; ARD 0.005, 95% CI 0.004–0.006), PE (HR 2.09, 95% CI 1.77–2.47; ARD 0.001, 95% CI 0.001–0.002), and DVT (HR 1.96, 95% CI 1.69–2.27; ARD 0.001, 95% CI 0.001–0.002). Given that outcomes including MACE and CAD violated the proportional hazards assumption, we divided the follow-up period into 12-month intervals (Table 3). This approach provided a more accurate assessment of the temporal relationship between burn injury and the outcomes of interest. The results consistently demonstrated a significant elevation in HRs across these intervals in all outcomes, with a slight downward trend over longer durations. Cumulative incidence curves of mortality and cardiovascular outcomes during the study period are presented in Supplementary Fig. S1.
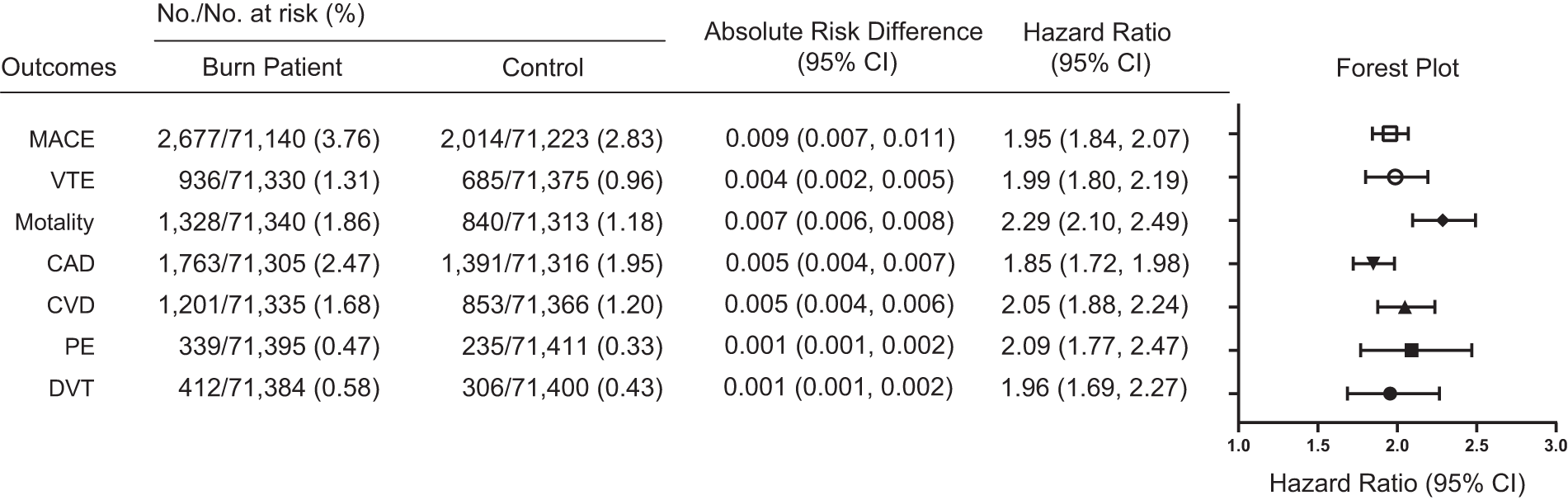
Relative and absolute risks of cardiovascular and thromboembolic outcomes among burn patients compared with matched controls. Forest plot showing hazard ratios (HRs) and 95% confidence intervals (CIs) for major adverse cardiovascular events (MACE), venous thromboembolism (VTE), all-cause mortality, coronary artery disease (CAD), cerebrovascular disease (CVD), pulmonary embolism (PE), and deep vein thrombosis (DVT) among burn patients compared with propensity score–matched controls during a follow-up period of 3 months to 5 years. HRs were estimated using Cox proportional hazards models. All p-values for the presented hazard ratios and log-rank tests were <0.001.
Time-varying hazard ratios of adverse outcomes across different follow-up periods
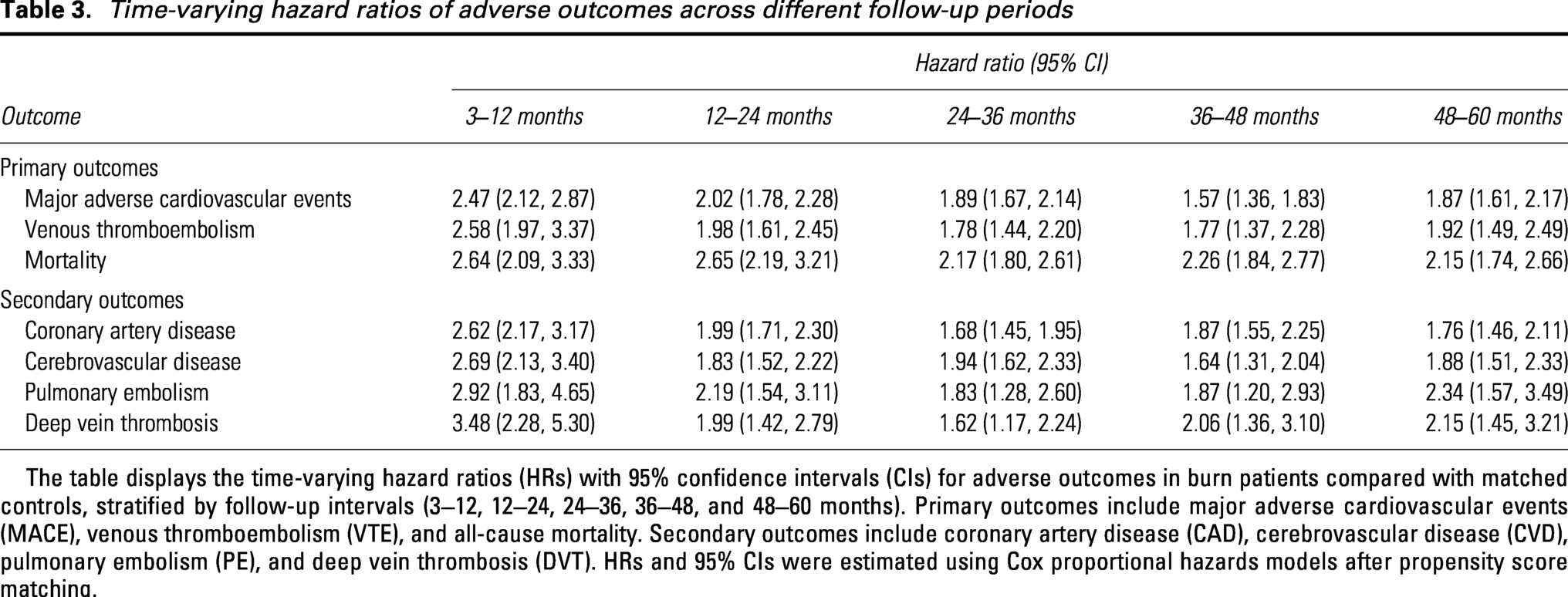
The table displays the time-varying hazard ratios (HRs) with 95% confidence intervals (CIs) for adverse outcomes in burn patients compared with matched controls, stratified by follow-up intervals (3–12, 12–24, 24–36, 36–48, and 48–60 months). Primary outcomes include major adverse cardiovascular events (MACE), venous thromboembolism (VTE), and all-cause mortality. Secondary outcomes include coronary artery disease (CAD), cerebrovascular disease (CVD), pulmonary embolism (PE), and deep vein thrombosis (DVT). HRs and 95% CIs were estimated using Cox proportional hazards models after propensity score matching.
Subgroup and Sensitivity Analyses Results
We conducted subgroup analyses based on various factors, including sex, race, age groups (18–65 years and >65 years), and burn severity. Subgroup analyses revealed consistently elevated risks of MACE, VTE, and mortality in burn patients compared with matched controls across various demographic and clinical stratifications (Table 4).
Subgroup analyses of hazard ratios for cardiovascular, thromboembolic, and mortality outcomes
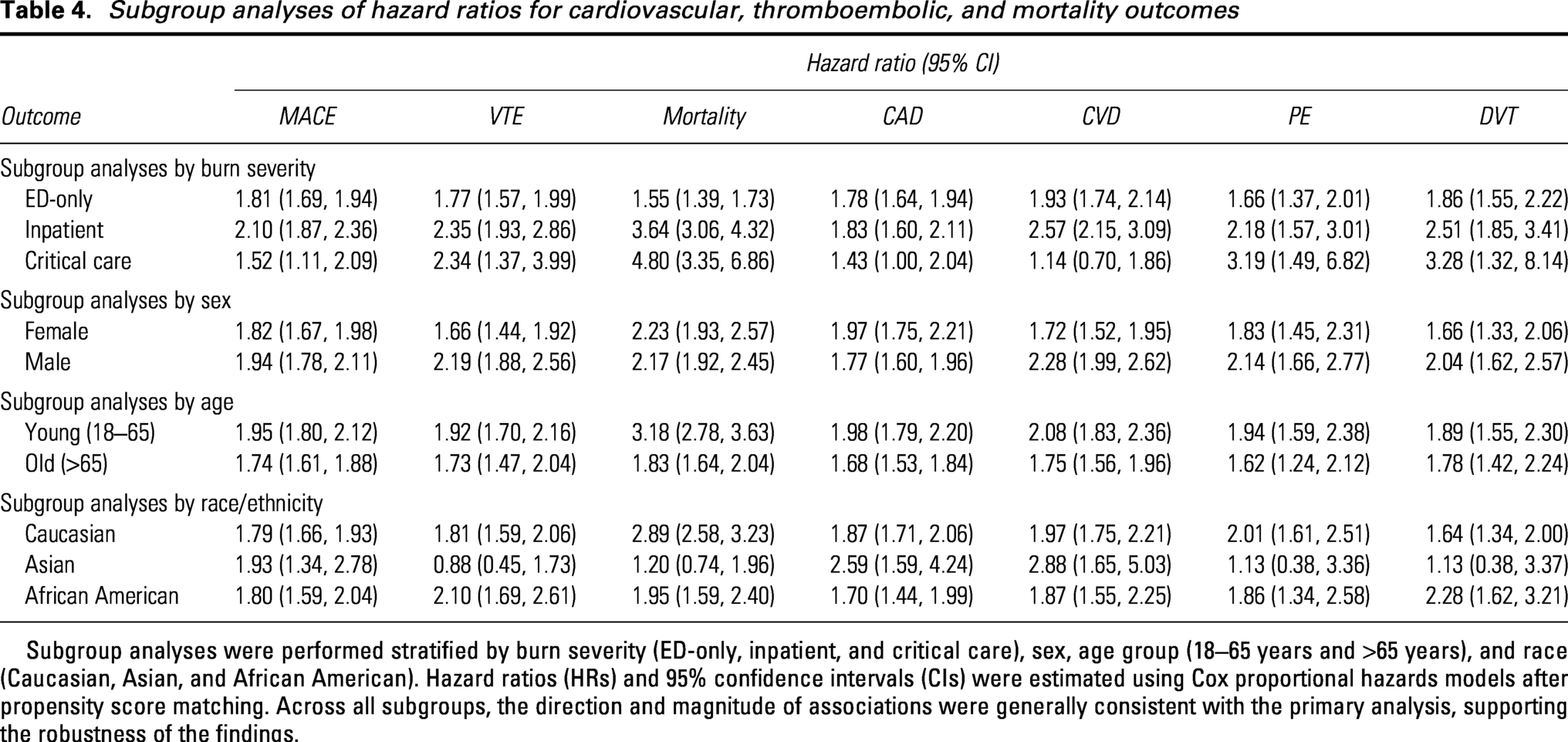
Subgroup analyses were performed stratified by burn severity (ED-only, inpatient, and critical care), sex, age group (18–65 years and >65 years), and race (Caucasian, Asian, and African American). Hazard ratios (HRs) and 95% confidence intervals (CIs) were estimated using Cox proportional hazards models after propensity score matching. Across all subgroups, the direction and magnitude of associations were generally consistent with the primary analysis, supporting the robustness of the findings.
For MACE, burn survivors had a significantly increased overall risk (HR 1.95, 95% CI 1.84–2.07). A severity-dependent pattern was observed, with higher risk among patients requiring inpatient admission (HR 2.10, 95% CI 1.87–2.36), while those receiving critical care also demonstrated elevated risk (HR 1.52, 95% CI 1.11–2.09). Increased risks were observed across sex and age groups. In race-stratified analyses, elevated risks were noted among Caucasian (HR 1.79) and African American patients (HR 1.80), as well as among Asian patients (HR 1.93).
For VTE, the overall HR was 1.99 (95% CI 1.80–2.19). Risks were higher among patients with more severe burns, including those requiring inpatient admission (HR 2.35, 95% CI 1.93–2.86) and critical care services (HR 2.34, 95% CI 1.37–3.99). Elevated risks were observed across sex and age groups. In race-stratified analyses, the association was significant among Caucasian (HR 1.81) and African American patients (HR 2.10), whereas the association among Asian patients was not statistically significant (HR 0.88, 95% CI 0.45–1.73).
For all-cause mortality, burn survivors exhibited a markedly increased overall risk (HR 2.29, 95% CI 2.10–2.49), with a pronounced gradient by burn severity. Mortality risk was highest among patients requiring critical care (HR 4.80, 95% CI 3.35–6.86), followed by those requiring inpatient admission (HR 3.64, 95% CI 3.06–4.32). Elevated mortality risks were observed across sex and age groups. In race-stratified analyses, increased mortality risk was observed among Caucasian patients (HR 2.89) and African American patients (HR 1.95), while the association among Asian patients was not statistically significant (HR 1.20, 95% CI 0.74–1.96).
Similar patterns were observed for secondary outcomes, including CAD, CVD, PE, and DVT. Detailed subgroup estimates and forest plots are presented in Table 4 and Supplementary Fig. S2.
Sensitivity analyses demonstrated that the associations between burn injury and adverse cardiovascular, thromboembolic, and mortality outcomes were robust across multiple analytic specifications (Table 5). When the observation window was varied to exclude early events (6 months to 5 years and 1–5 years), HRs for MACE, VTE, and all-cause mortality remained significantly elevated and were comparable in magnitude to the primary analysis. Similarly, analyses modifying study population definitions, including restriction to the Global Collaborative Network, requiring controls to have at least three health care visits, and exclusion of bedridden or limited-mobility patients, yielded consistent results across all outcomes. Although modest attenuation of effect estimates was observed after excluding bedridden or limited-mobility patients, the direction and statistical significance of associations were preserved. In the Hispanic/Latino subgroup, the risks of all-cause mortality and MACE mirrored the primary cohort, showing robust and statistically significant elevations. However, the association with VTE was mildly attenuated; while the composite VTE risk remained elevated, the individual endpoints of DVT and PE did not reach statistical significance. Forest plots of the sensitivity analyses are presented in Supplementary Figures S3, S4, S5, S6, and S7. Collectively, these findings support the soundness of the observed long-term cardiovascular, thromboembolic, and mortality risks among burn survivors.
Sensitivity analyses of hazard ratios for cardiovascular, thromboembolic, and mortality outcomes
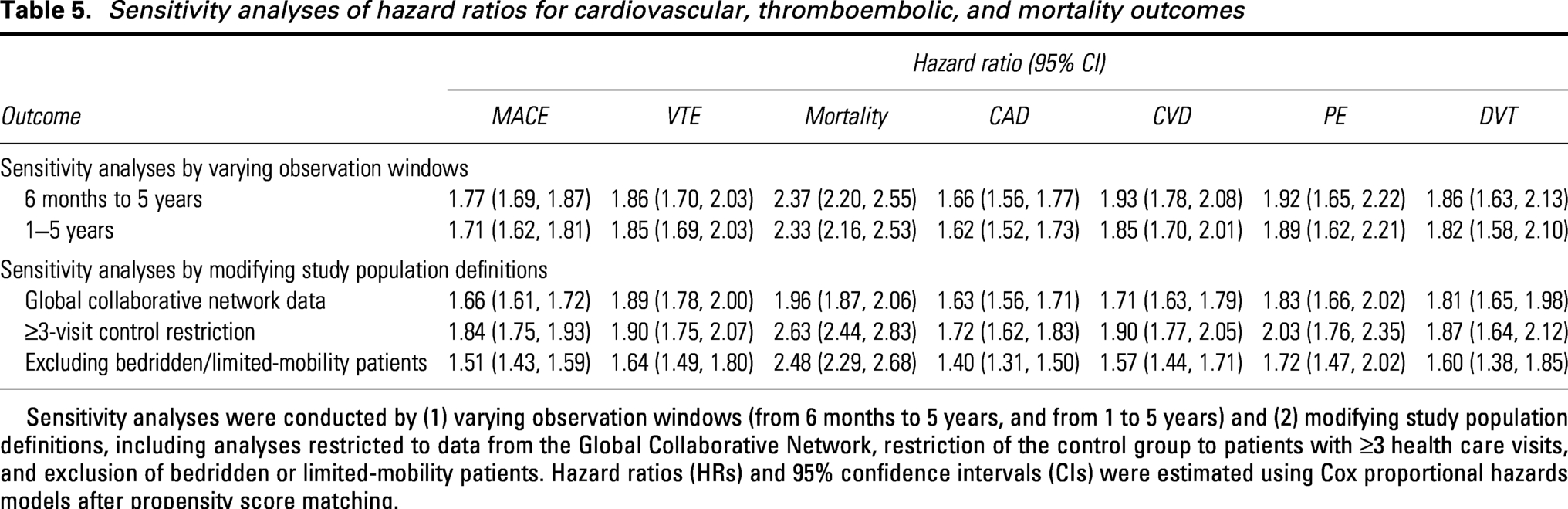
Sensitivity analyses were conducted by (1) varying observation windows (from 6 months to 5 years, and from 1 to 5 years) and (2) modifying study population definitions, including analyses restricted to data from the Global Collaborative Network, restriction of the control group to patients with ≥3 health care visits, and exclusion of bedridden or limited-mobility patients. Hazard ratios (HRs) and 95% confidence intervals (CIs) were estimated using Cox proportional hazards models after propensity score matching.
DISCUSSION
In this large cohort study of adult burn survivors, we observed significantly elevated long-term risks of MACE, VTE, and all-cause mortality compared with matched nonburn controls. The HRs for MACE and VTE were approximately two, indicating that burn injury survivors face a twofold increased risk of serious cardiovascular and thromboembolic events over time. These findings reinforce the concept that burn injury is not merely an acute trauma but can lead to chronic physiological changes.4,22,23
Severe burns initiate chronic inflammation in which sustained catecholaminergic drive and excessive production of pro-inflammatory cytokines disrupt cardiometabolic and vascular homeostasis for years. 24 This persistent systemic stress provides biological credibility for long-term cardiovascular risk through multiorgan effects on the myocardium, vasculature, and hemostatic system. 15 Mechanistically, experimental studies indicate that activation of β-adrenergic receptors along with these cytokines may contribute to cardiac mitochondrial injury with reactive oxygen species excess and perturbed cGMP–PKG signaling.16,25,26 In parallel, pro-inflammatory cytokines also cause endothelial injury with chronic impairment of nitric oxide-mediated signaling. 27 These vascular injury pathways may provide a mechanistic link between burn injury and the subsequent risks of both atherothrombotic events and VTE. Human data in well-healed burn survivors show impaired vasodilator function, supporting the presence of long-lasting endothelial dysfunction after burn injury. 28 At the level of endothelial injury and coagulation regulation, endotheliopathy in burn patients is evidenced by endothelial glycocalyx shedding (elevated circulating syndecan-1) and reduced anticoagulant tone (lower tissue factor pathway inhibitor) in previous cohorts.29,30 Moreover, burn survivors exhibit persistent disturbances in lipid metabolism with an increased level of triglycerides and a decreased level of high-density lipoprotein. 31 Finally, emerging evidence links burns to sustained platelet activation. A recent murine model study demonstrated sustained platelet hyperreactivity after burn injury. 32 Despite these insights, mechanistic evidence is largely limited to the acute phase and small, heterogeneous cohorts. Longitudinal studies incorporating standardized burn severity metrics, serial biomarker assessments, and adjudicated cardiovascular outcomes are needed to elucidate causal pathways and preventive targets.33,34
Our findings are in line with emerging evidence from population-based studies of burn survivors. Duke et al. reported that burn patients had significantly higher rates of cardiovascular-related hospitalizations and longer cumulative hospital stays for circulatory diseases compared with uninjured controls. 8 Notably, compared with nonburn trauma patients, the burn cohort had higher adjusted rates of CVD admissions and longer CVD hospital stays. 18 Similarly, Mason et al. conducted a matched cohort study that followed 1,965 burn survivors and 8,671 matched controls over a median follow-up of 5 years. 35 The study found a significantly higher 5-year mortality rate among burn survivors (11%) compared with controls (4%). 35 The risk was greatest during the first year after discharge and gradually decreased over time. 35 We similarly observed a more than twofold increase in all-cause mortality risk among burn survivors. Moreover, this study provides significant incremental contributions. By utilizing the TriNetX network, we enhance the study’s global generalizability and account for ethnic heterogeneity. We also explicitly capture the enduring VTE risk. Importantly, our utilization-based stratification demonstrates that even outpatient-managed burn survivors face significant, long-term atherothrombotic hazards.
Our observation of elevated long-term mortality provides a complementary perspective to the findings of Weissman et al., who reported no significant difference in life expectancy in an Israeli cohort. 36 This divergence is likely attributable to distinct study designs and population characteristics. Methodologically, Weissman et al. compared burn survivors with minor trauma patients using multivariate regression for adjustment. In contrast, our study leveraged a larger sample size and employed 1:1 PSM to strictly pair burn survivors with nonburn controls. This matching process ensures a balanced distribution of baseline comorbidities prior to analysis. Furthermore, regional disparities in baseline health profiles are notable. Our US-based cohort operates within a distinct health care insurance system and likely exhibits a higher prevalence of cardiovascular risk factors (e.g., obesity, metabolic syndrome) compared with the Israeli population. 37 Finally, our follow-up extended into the COVID-19 pandemic, a period when burn survivors with compromised physiological reserve may have been disproportionately vulnerable compared with the prepandemic era of the referenced study. 38
One area where our study extends the literature is in documenting long-term VTE risk. Prior burn studies have primarily focused on cardiovascular disease and mortality, while the long-term risk of VTE has received comparatively little attention.12,19,20,39 Only recently has a 5-year retrospective study begun to explore this burden. 12 We found nearly a twofold hazard of VTE in burn survivors, which aligns with the known prothrombotic state following burns. 40 These findings suggest a prothrombotic tendency that persists well beyond wound healing, extending prior evidence of high in-hospital DVT/PE rates and the need for prophylactic anticoagulation in severe burns.19,20,41 However, it is noteworthy that this susceptibility appears to be modulated by race/ethnicity. Our subgroup analysis observed an attenuated VTE risk in Asian and Hispanic burn survivors, aligning with global epidemiological data on the prevalence of VTE among different racial/ethnic groups.42–44 Therefore, incorporating race/ethnicity alongside validated risk assessment models (e.g., Caprini score) could facilitate a more precise, risk-stratified approach. 45 Continuous risk assessment and tailored prophylaxis are crucial for the long-term management of burn survivors.
In our subgroup analyses, patients who required critical care services had the highest long-term mortality risk but comparatively lower risk of MACE than patients requiring inpatient admission. This may be explained by several factors. First, this observation highlights a classical competing-risk phenomenon. Despite surviving the acute phase, critically ill burn survivors face a profound burden of fatal noncardiovascular complications, with sepsis and multiple organ failure consistently identified as leading causes of mortality.46,47 In these patients, persistent immune dysregulation, barrier disruption, recurrent wound or nosocomial infections, and ongoing organ vulnerability may sustain a prolonged period of competing fatal risk.15,34 Consequently, the most severely injured patients frequently succumb to these competing etiologies before long-term atherothrombotic complications can clinically manifest. Second, during their initial hospitalization, these patients likely received intensive cardiovascular and thromboprophylactic management, potentially mitigating their long-term MACE and VTE risks. Moreover, cause-of-death misclassification or underreporting may have contributed to an underestimation of MACE and VTE events in this group.
In this study, while relative risks were substantially elevated, the ARDs for individual outcomes remained modest, directly reflecting the inherently low baseline incidence of these cardiovascular events in the general population. These findings therefore strongly argue against universal intensive screening and instead support a targeted, risk-stratified approach to survivorship care. Burn survivors with more severe injuries, particularly those requiring inpatient hospitalization or critical care, represent the most appropriate candidates for cardiovascular risk assessment and preventive strategies.
Translating these findings into practice requires reframing burn injury as a chronic systemic condition rather than an isolated acute trauma. Routine outpatient visits and dressing changes provide accessible opportunities for wound care teams to incorporate cardiovascular and thromboembolic vigilance into postburn follow-up. Because excess risks persisted for up to 5 years after injury, we propose a risk-stratified surveillance framework based on acute health care utilization (Fig. 3), within which surveillance intensity scales with the level of care required at the index injury. Patients managed exclusively in the ED (Tier 1: Standard Vigilance) may warrant annual cardiometabolic review, including assessment of blood pressure, body mass index, and lipid and glucose profiles as clinically indicated. Survivors requiring inpatient admission (Tier 2: Targeted Monitoring) may benefit from semiannual metabolic monitoring during the first 3 years and individualized postdischarge VTE risk assessment using validated tools such as the Caprini score; severe burn history may further be considered a risk-enhancing factor when estimating atherosclerotic cardiovascular disease risk, consistent with the 2019 ACC/AHA primary prevention guideline. 48 Survivors requiring critical care (Tier 3: Intensive Surveillance) should be considered for early multidisciplinary comanagement with primary care and cardiology, with a low threshold for echocardiography when dyspnea, edema, persistent tachycardia, reduced exercise tolerance, or abnormal ECG findings are present. Future studies incorporating cumulative incidence curves and individualized risk prediction models may further refine these surveillance strategies.
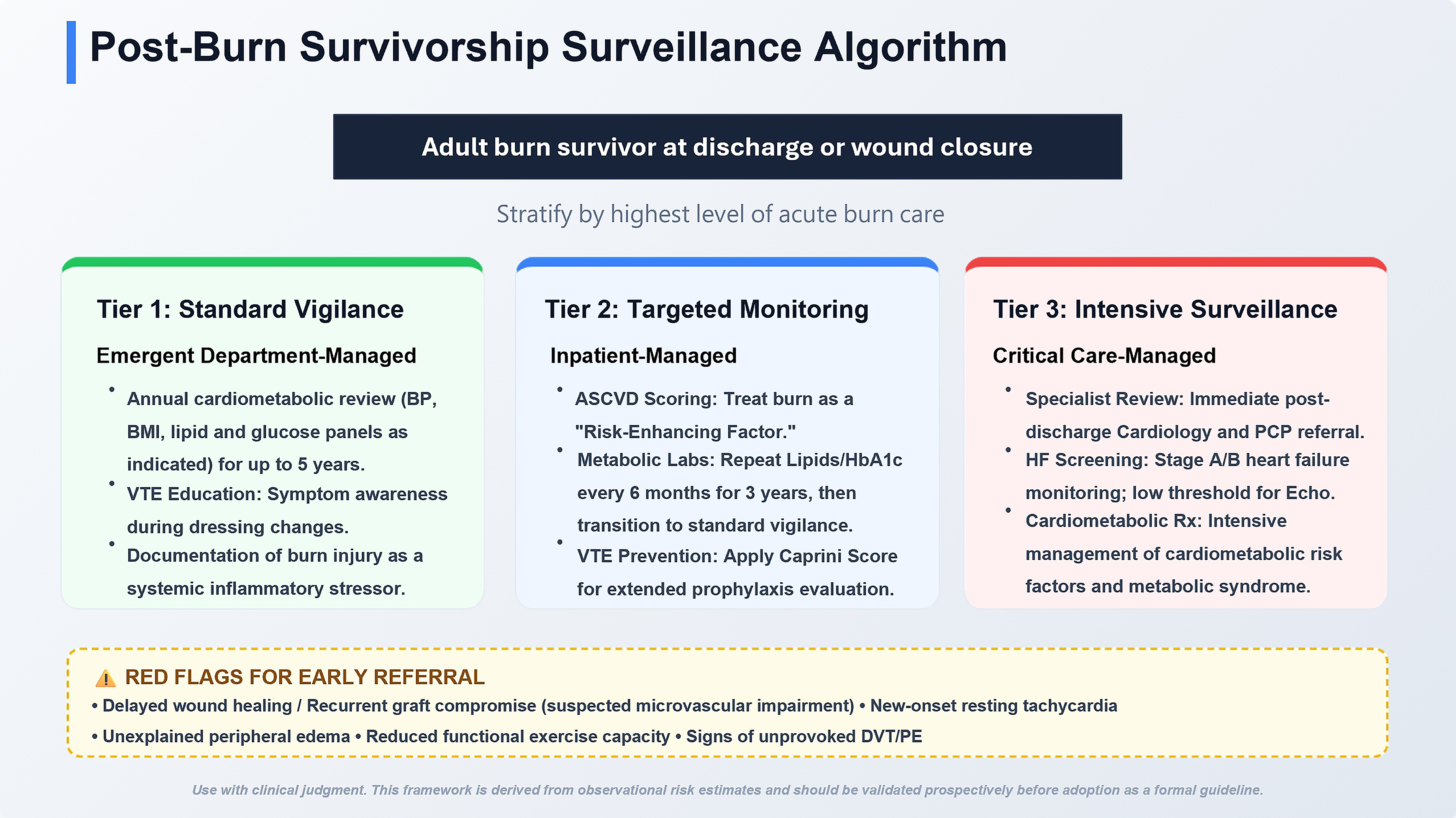
Proposed risk-stratified postburn survivorship surveillance algorithm. Adult burn survivors are stratified at discharge or wound closure according to the highest level of acute care received during the index injury: emergency department management, inpatient admission, or critical care admission. Tier 1 (Standard Vigilance) applies to emergency department–managed survivors and includes annual cardiometabolic review covering blood pressure, body mass index, and lipid and glucose profiles as clinically indicated, alongside venous thromboembolism symptom education and documentation of burn injury as a systemic inflammatory stressor. Tier 2 (Targeted Monitoring) applies to inpatient-managed survivors and includes atherosclerotic cardiovascular disease risk assessment, semiannual lipid and hemoglobin A1c testing for 3 years, and individualized evaluation for extended venous thromboembolism prophylaxis using validated tools such as the Caprini score. Tier 3 (Intensive Surveillance) applies to survivors who required critical care and includes early postdischarge referral to primary care and cardiology, monitoring for stage A/B heart failure or subclinical myocardial stress, and aggressive cardiometabolic risk factor management. Across all tiers, delayed wound healing, recurrent graft breakdown, new-onset resting tachycardia, unexplained peripheral edema, reduced functional exercise capacity, or signs of unprovoked deep vein thrombosis or pulmonary embolism should prompt early multidisciplinary referral. This framework is derived from observational risk estimates and should be applied with clinical judgment pending prospective validation.
Beyond systemic monitoring, clinicians should remain alert to cutaneous findings that may reflect impaired perfusion or broader vascular dysfunction. Persistent postburn endothelial dysfunction, microvascular alterations, and hypermetabolic stress may impair tissue perfusion and repair, lowering the threshold for delayed wound healing, recurrent graft compromise, or chronic ulceration.49,50 Rather than treating these findings solely as localized wound failures, clinicians should consider them potential indicators of underlying cardiovascular and thromboembolic risk, prompting broader systemic assessment and timely specialist referral. Representative clinical scenarios illustrating the application of the proposed surveillance tiers in outpatient burn survivorship care are provided in Supplementary Box S1.
Several limitations of this study warrant consideration. First, we used the TriNetX EHR database, which relies on clinical coding and data entry across many centers. As a result, there is potential for incomplete or missing data and misclassification of variables. To mitigate this limitation, we focused on well-defined and coded outcomes and performed the sensitivity analysis by requiring patients to have at least three medical visits during the study period. Second, although we applied PSM to balance baseline characteristics between burn survivors and controls, residual confounding cannot be fully excluded. Covariate balance before and after matching was assessed using standardized mean differences, with all matched variables achieving an absolute SD < 0.1, indicating adequate balance; detailed balance diagnostics are presented in the main text (Table 2). Nevertheless, important factors such as socioeconomic status, diet, physical activity, and environmental exposures are not comprehensively captured in EHRs. To partially address these unmeasured confounders, we incorporated clinically relevant proxy variables into the PSM framework, including chronic lower respiratory diseases as a proxy for smoking exposure and alcohol-related disorders as a proxy for alcohol use. Third, the external validity of this study warrants consideration. The study population was predominantly composed of individuals identified as Caucasian, reflecting the demographic composition of participating health care systems within the TriNetX US Collaborative Network. To address this concern, we conducted a sensitivity analysis using data from the Global Collaborative Network. The direction and magnitude of associations between burn injury and cardiovascular, thromboembolic, and mortality outcomes were consistent with those observed in the primary analysis (Table 5), supporting the robustness of our findings across different health care systems. Fourth, bedridden status or reduced mobility following burn injury is a potential confounder. Accordingly, we performed a sensitivity analysis excluding patients with documented bedridden or limited-mobility status after burn injury. The findings paralleled the primary results, with a mild attenuation of the estimated effect. Fifth, a major limitation is the absence of detailed burn injury characteristics in the dataset. Key prognostic factors like total body surface area burned, burn depth, surgical procedures, length of hospital stay, intensive care unit stay duration, and specific acute nutritional interventions (e.g., high-calorie/high-protein diets) were not available at the patient level. Also, due to the reliance on ICD-10 coding in administrative data, specific burn mechanisms (e.g., electrical injury) and concomitant conditions like inhalation injury or acute respiratory distress syndrome appeared to be underreported in the database. Consequently, we were unable to perform reliable subgroup analyses on these specific etiologies. To partially address these gaps, we used health care utilization patterns (e.g., emergency visits, inpatient admissions, and critical care services) as a proxy for burn severity. The validity of this stratification was supported by a stepwise increase in 3-month mortality. Because severe injury mechanisms like electrical burns or profound respiratory complications inherently necessitate intensive monitoring and mechanical ventilation, these high-risk phenotypes are implicitly captured within our critical care cohort. While this approach provides a pragmatic surrogate for burn severity, we explicitly acknowledge that this utilization-based proxy is susceptible to confounding by institutional practice patterns, variations in local admission criteria, and noninjury-related factors (e.g., baseline comorbidities or socioeconomic status). Hence, the interpretation of our severity-stratified findings should remain cautious. In addition, it is crucial to explicitly acknowledge the heterogeneity of our study population. The ICD-10-CM codes utilized for cohort identification (T20–T32) encompass a broad spectrum of injury types and severities. Future studies incorporating standardized clinical scoring systems or registry-based severity metrics are warranted. Finally, residual surveillance bias cannot be excluded. Burn survivors frequently require prolonged health care engagement for scar management, reconstructive evaluations, and physical rehabilitation and may therefore undergo more frequent medical scrutiny than noninjured controls.
In conclusion, this large-scale real-world cohort study demonstrates that burn survivors have significantly increased long-term risks of MACE, VTE, and all-cause mortality compared with matched nonburn controls. These findings support a shift in postburn care from episodic wound-focused management toward structured survivorship care that recognizes burn injury as a chronic systemic condition. Wound care practitioners should use routine follow-up visits as opportunities to screen for cardiovascular and thromboembolic risk, while high-risk survivors should be co-managed by burn surgeons, primary care providers, and cardiologists. Incorporating risk-stratified surveillance into postdischarge care may provide opportunities for earlier detection of systemic complications, timely preventive intervention, and improved long-term outcomes for burn survivors.
INNOVATION
Long-term cardiovascular and thromboembolic risks after burn injury remain underrecognized, with prior studies largely limited to acute outcomes or short-term follow-up. This study leverages large-scale real-world data to quantify sustained risks up to 5 years after burn injury using both relative and absolute risk measures. By integrating a pragmatic burn severity proxy, comprehensive subgroup analyses, and extensive sensitivity testing, this work advances the conceptualization of burn injury as a chronic systemic condition. These findings provide a framework for risk-stratified survivorship care and inform future efforts toward targeted cardiovascular prevention in burn survivors.
AUTHORS’ CONTRIBUTIONS
All authors confirm that they have made substantial contributions to the conception and design of the study, data analysis and interpretation, and drafting or critical revision of the article. All authors have approved the final version of the article and agree to be accountable for all aspects of the work. All authors have full access to all the data in the study and take responsibility for the integrity of the data and accuracy of the data analysis. Concept and design: All authors. Acquisition, analysis, or interpretation of data: all authors. Drafting of the article: Y.-C.W. and Y.-H.L. Critical revision of the article for important intellectual content: all authors. Statistical analysis: Y.-C.W. and Y.-H.L.
KEY FINDINGS
Burn survivors face a nearly twofold increased risk of major adverse cardiovascular events (MACE) and venous thromboembolism (VTE) that persists for up to 5 years after injury. Mortality remains significantly elevated long after wound closure, supporting the recognition of burn injury as a chronic systemic condition rather than an isolated acute trauma. Even survivors managed exclusively in the emergency department have significantly elevated long-term risks, indicating that outpatient-managed burns should not be considered risk-free after wound healing. These findings support integrating long-term cardiovascular and thromboembolic risk assessment into routine postburn survivorship care, particularly for patients requiring inpatient or critical care management.
DATA SHARING STATEMENT
Data are available on the TriNetX platform; however, due to Health Insurance Portability and Accountability Act (HIPAA) regulations, the data cannot be made publicly accessible.
Footnotes
ACKNOWLEDGMENTS AND FUNDING SOURCES
The authors sincerely thank the Yen Tjing Ling Medical Foundation for their support and Far Eastern Memorial Hospital for their assistance with this research project. The authors acknowledge the financial support from the Yen Tjing Ling Medical Foundation (CI-114-28) and Taipei Veterans General Hospital (V115B-024). The funding sources played no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the article; or the decision to submit the article for publication.
AUTHOR DISCLOSURE AND GHOSTWRITING
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this article. No professional medical writers, ghostwriters, or editorial assistance were involved in the preparation of this article.
ABOUT THE AUTHORS
Supplemental Material
Abbreviations and Acronyms
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.