
Abstract
Objective:
To benchmark zero-shot generative pre-trained transformer (GPT)-based multimodal large language models (MLLMs) for pressure injury (PI) staging from photographs and quantify the effects of prompt strategy, structured outputs, and clinically meaningful label granularity.
Approach:
We performed a retrospective observational benchmark using 1,091 public, de-identified PI photographs labeled Stage I–IV. In the standardized analysis, all 10 model/prompt conditions were evaluated using a standardized, resume-safe application programming interface pipeline with per-image logging. We evaluated exact four-class staging, three-class staging (I/II/III–IV), skin-break screening (I vs. II–IV), and an advanced-intervention threshold (I–II vs. III–IV). Reporting followed Strengthening the Reporting of Observational Studies in Epidemiology and artificial intelligence/machine learning guidance; metrics included accuracy, Wilson 95% confidence intervals, F1 scores, weighted kappa, and threshold sensitivity/specificity.
Results:
All conditions yielded parsed predictions for all 1,091 images. The best accuracy was 93.77% for skin-break screening (GPT-5.2 structured JavaScript Object Notation [JSON]), 90.28% for the advanced-intervention threshold (GPT-5.1 full prompt, low reasoning), 83.78% for three-class staging (GPT-5.1 full prompt, low reasoning), and 65.08% for exact four-class staging (GPT-5.2 structured JSON). The best advanced-intervention condition achieved sensitivity 96.72%, specificity 83.79%, and negative predictive value 96.19%. Stage IV undercalling remained safety-relevant; GPT-5.2-pro had Stage IV recall 8.79% and false-negative rate 91.21%.
Innovation:
This prompt-transparent benchmark shows how outcome granularity, prompting, and structured outputs affect GPT-based PI staging and adds ordinal, threshold-based, and safety metrics.
Conclusion:
GPT-based MLLMs may support clinician-supervised triage and prioritization, but image-only autonomous exact staging is not clinically ready.
Toshiaki Takahashi, RN, PhD

INTRODUCTION
Pressure injuries (PIs) are localized damage to the skin and/or underlying soft tissue and are staged according to standardized criteria. 1 PIs remain prevalent across acute and long-term care settings and impose substantial clinical and economic burden, as supported by systematic reviews and cost analyses.2–6 Because PI stage reflects the depth of tissue involvement, accurate staging is essential for clinical communication and documentation, informs reimbursement, and guides treatment selection and urgency—including timely escalation of care to prevent deterioration and recurrence. 1 In addition, PI prevention and management require sustained multidisciplinary effort: evidence syntheses have identified a broad set of patient-level and care-process risk factors (e.g., immobility, impaired perfusion, nutritional compromise), and studies consistently emphasize the need for ongoing clinician education and competency maintenance to support prevention and early identification.7,8
A persistent barrier to consistent PI management is variability in visual assessment and staging. Studies evaluating staging agreement—particularly those using photographs—have reported only moderate interrater reliability, with disagreement most pronounced for early-stage lesions and for differentiation of pressure-related lesions from moisture-associated skin damage.9–15 This variability has practical consequences: staging inconsistency can lead to delayed escalation of preventive measures, misalignment of treatment intensity with true injury depth, and challenges in quality monitoring and benchmarking across care settings. To mitigate gaps in access to expertise and to standardize assessment, technology-enabled decision-support approaches, including telehealth-based monitoring and consultation, have been explored to extend specialist input into routine care workflows. 16
Concurrently, computer vision and deep learning methods have been increasingly applied to wound and PI image analysis.17–33 Prior work includes algorithmic pipelines for wound segmentation and measurement,21,22 as well as automated PI detection and staging classification using a range of deep learning architectures and clinical deployment contexts.23–32 Although these approaches demonstrate feasibility, their performance and generalizability can be strongly influenced by dataset composition, labeling procedures, and imaging conditions, and the field continues to converge on the need for transparent reporting and clinically meaningful evaluation frameworks.18–20 In particular, guidelines such as Checklist for Artificial Intelligence in Medical Imaging (CLAIM) and Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) underscore the importance of clear reporting of dataset provenance, labeling standards, evaluation design, and limitations to support reproducibility and translation to clinical settings.19,20
Multimodal large language models (MLLMs) that jointly interpret images and text represent a new class of foundation models with potential advantages for wound care: they can be prompted with explicit staging definitions, requested to provide human-readable rationales, and evaluated without task-specific model training. Early reports suggest that vision-enabled chatbots may assist with PI interpretation and that multimodal systems can support fine-grained wound-related classification tasks; however, rigorous benchmarking across model generations and prompt strategies—and transparent documentation of prompt-level design choices—remain limited.33–37 Moreover, practical deployment requires careful characterization not only of accuracy but also of how performance changes when labels are collapsed into clinically motivated groupings (e.g., triage-oriented binary thresholds vs. full four-stage staging).
Therefore, we benchmark generative pre-trained transformer (GPT)–based MLLMs (GPT-4o, GPT-4.1, GPT-5.1, GPT-5.2, and GPT-5.2-pro) for PI staging using a public image dataset and quantify performance across clinically relevant label granularities (four-class, three-class, and two-class). We further evaluate prompt strategies that vary in the degree of embedded domain knowledge (concise vs. definition-rich prompts) and output structuring, with the goal of providing a prompt-transparent, clinically interpretable baseline for subsequent method development and validation.
CLINICAL PROBLEM ADDRESSED
PIs require timely recognition and escalation, yet specialist wound expertise is not uniformly available, particularly in remote or resource-limited settings. In practice, management decisions often depend less on an exact National Pressure Injury Advisory Panel (NPIAP) stage than on whether the lesion is superficial (Stages I–II; typically managed with offloading and local care) versus a deeper injury (Stages III–IV; often prompting debridement, infection evaluation, and possible surgical consultation). Accordingly, we benchmarked zero-shot MLLMs on PI photographs across clinically motivated granularities, including a triage-oriented threshold (Stages I–II vs. III–IV) alongside conventional four-stage staging.
MATERIALS AND METHODS
Study design and reporting
This was a retrospective observational benchmarking study of model outputs on a labeled public image dataset. Reporting followed relevant guidance for observational studies and artificial intelligence (AI)–focused evaluations, including STROBE and CLAIM, and supplementary reporting was aligned with recent AI/machine learning (ML) rigor guidance for health care and clinical research. 39 An AI/ML reporting crosswalk is provided in Supplementary Appendix A3. Electronic laboratory notebook was not used.
Dataset
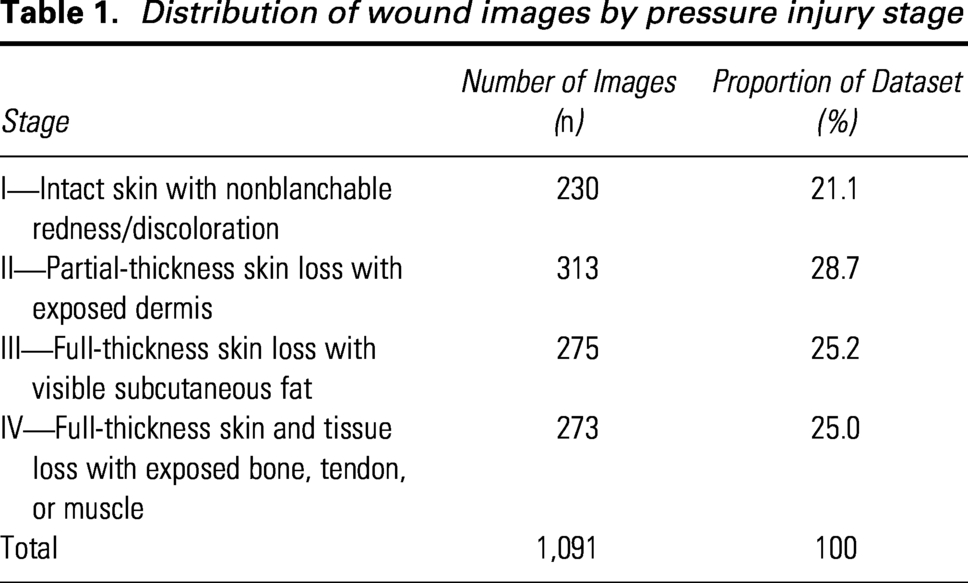
We analyzed the Pressure Injury Images Dataset (PIID), a publicly accessible dataset of de-identified clinical photographs of PIs. The released PIID repository describes the dataset as 1,091 red–green–blue (RGB) color images of 299 × 299 pixels. The released stage distribution was Stage I (n = 230), Stage II (n = 313), Stage III (n = 275), and Stage IV (n = 273). We used all images available in the released dataset and did not apply additional study-specific exclusions after dataset retrieval. Each image had a source-distributed stage label assigned according to NPIAP definitions. We used the provided labels as the operational reference standard and performed no relabeling, lesion segmentation, or data augmentation. The PIID images were accessed via the dataset repository maintained by the dataset authors and were used solely for research purposes; we did not redistribute the image files as a dataset.
The local analysis copies used for the standardized analysis were verified in the image manifest as 224 × 224 RGB images for all 1,091 files. No additional preprocessing, filtering, lesion segmentation, or augmentation was performed before application programming interface (API) submission beyond encoding the fixed local image file for model input. The source release did not provide structured metadata on care setting, body site distribution, camera/device type, skin-tone representation, dressing status, contaminant status, or other image-acquisition descriptors. The source publication also did not report whether labels were assigned by a single or multiple raters, whether adjudication was performed, or whether interrater agreement statistics were available for the released labels. A source-available dataset datasheet summarizing available and unavailable metadata is provided in Supplementary Table S1. Because the dataset was publicly accessible and de-identified, this study constitutes secondary analysis of nonidentifiable data and did not require institutional review board review or informed consent, consistent with prior work using public PI image datasets.
Models, zero-shot definition, and prompt conditions
We evaluated five GPT-based MLLMs capable of image understanding: GPT-4o, GPT-4.1, GPT-5.1, GPT-5.2, and GPT-5.2-pro. We describe these as GPT-based MLLMs to distinguish the scope of this benchmark from non-GPT commercial or open-source vision-language models. All models were used in inference-only mode without task-specific fine-tuning, reinforcement learning, or parameter updates. We use “zero-shot” to mean that no labeled PI image exemplars or task-specific few-shot examples were included in the prompt; definition-rich prompts did contain textual staging definitions and decision rules.
Ten model/prompt conditions were evaluated in the standardized analysis: GPT-4o full prompt/no reasoning; GPT-4.1 full prompt/no reasoning; GPT-4o simple prompt/no reasoning; GPT-4.1 simple prompt/no reasoning; GPT-5.1 full prompt/no reasoning; GPT-5.1 full prompt/low reasoning; GPT-5.1 structured JavaScript Object Notation (JSON)/no reasoning; GPT-5.1 structured JSON/low reasoning; GPT-5.2 structured JSON/no reasoning; and GPT-5.2-pro structured JSON/xhigh reasoning. The simple prompt requested a single-stage label with minimal task context. The full prompt embedded concise NPIAP-aligned staging definitions and decision rules. Structured-output conditions requested a constrained JSON object containing a single-stage label and a short rationale. The exact prompts and JSON schemas are provided in Supplementary Appendix SA1.
Standardized API-based inference and execution
All 10 model/prompt conditions were evaluated using a standardized, resume-safe Python API pipeline with per-image logging. Each condition was run on the full analytic set of 1,091 images. All conditions produced analyzable parsed outputs for all 1,091 images, yielding a uniform N = 1,091 for every reported condition. The runner wrote one row per image per condition and recorded the condition identifier, image identifier, source label, parsed prediction, raw model output, rationale when available, parse status, model string, prompt style, output mode, reasoning setting, requested and applied generation parameters, API response identifier, finish status, attempt count, timestamps, latency, and token counts when available.
The resolved API model strings were gpt-4o, gpt-4.1, gpt-5.1, gpt-5.2, and gpt-5.2-pro. Temperature was set to 0 when supported by the model. For reasoning-effort conditions in which the API did not support temperature, the unsupported parameter was detected during smoke testing and omitted; this behavior was documented in the parameter support log. Top-p was not specified. Maximum output tokens were set to 600 for all conditions except GPT-5.2-pro with xhigh reasoning, for which 3,000 output tokens were allowed. Reasoning effort was omitted for no-reasoning conditions, set to low for the GPT-5.1 low-reasoning conditions, and set to xhigh for GPT-5.2-pro. Model execution parameters, support checks, runtime summaries, and token summaries are reported in Supplementary Table S9. The standardized analysis was performed from May 21 to May 24, 2026.
Output parsing and quality control
Outputs were parsed using a prespecified normalization protocol. The primary parsed value was a single integer stage label from 1 to 4. Structured-output conditions were parsed directly from the JSON schema when available. For prompt-JSON conditions, the parser extracted the stage label from the model output and, when needed, normalized explicit textual stage expressions such as “Stage III” to the corresponding numeric stage. Outputs that could not be resolved to a single stage label after normalization would have been treated as nonparseable and incorrect; however, in the standardized analysis, all 10 conditions produced valid parsed stage labels for all 1,091 images. For GPT-4o, a small number of rows required text-based parsing rather than direct structured parsing, but all were resolved to valid stage labels. The full parsing rules and examples are provided in Supplementary Appendix SA2. Prediction-output integrity for the standardized analysis is summarized in Supplementary Table S2.
Classification tasks and clinical endpoint definitions
We evaluated four outcome formulations. First, the four-class task required exact prediction of Stage I, II, III, or IV and reflects standard clinical staging. Second, the primary three-class task grouped labels as Stage I, Stage II, and Stage III/IV combined. We specified this as the primary endpoint because it preserves clinically meaningful distinctions between intact skin, partial-thickness skin loss, and advanced full-thickness injury while acknowledging the limited reliability of photo-only discrimination between Stage III and Stage IV. Third, we retained a skin-break screening threshold defined as Stage I versus Stages II–IV, corresponding to the distinction between intact skin injury and visible skin loss or deeper tissue involvement. Fourth, to improve clinical actionability, we evaluated an advanced-intervention threshold defined as Stage I–II versus Stage III–IV, intended to approximate a clinically meaningful distinction between lower-stage injuries typically managed with pressure relief and local care versus advanced full-thickness injuries that may require specialist wound review, debridement, infection assessment, or surgical consultation. These binary thresholds should be interpreted as triage-oriented decision-support endpoints, not as autonomous treatment recommendations.
Evaluation metrics and statistical analysis
For each condition and outcome task, we calculated accuracy with 95% Wilson confidence intervals (CIs). To address the ordinal and class-imbalanced nature of PI staging, we also calculated macro F1, weighted F1, and Cohen’s quadratic weighted kappa. For binary thresholds, we calculated sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and false-negative rate, treating the higher-severity class as the positive class. Stage IV safety metrics included Stage IV precision, recall, specificity, NPV, false-negative rate, and the proportion of true Stage IV images undercalled as Stage III.
Because the standardized analysis produced predictions for all 1,091 images in every condition, paired statistical comparisons were performed on the common full-image set. We used Cochran’s Q test to evaluate whether correct/incorrect patterns differed across multiple conditions for each outcome task. Pairwise McNemar tests were used for selected condition comparisons, with Holm adjustment for multiple testing. These statistical tests were interpreted as exploratory because model outputs were generated from API-based systems and because the public dataset labels may contain unquantified label uncertainty.
To assess the potential impact of uncertain ground-truth labels, we conducted a post hoc label-noise sensitivity analysis. We simulated adjacent-stage perturbations at 5%, 10%, and 15% label-noise rates by randomly moving labels to an adjacent stage where possible, repeated the simulation, and recalculated performance metrics. This analysis was not intended to estimate the true label-error rate in PIID; rather, it bounded how modest adjacent-stage label uncertainty could affect apparent performance, particularly for exact four-class staging.
Reproducibility, data management, and software
The standardized analysis used a fixed image manifest, run manifest, prompt files, JSON schema files, prediction CSVs, progress logs, parameter support logs, and file checksums. Each prediction CSV contains 1,091 rows and 1,091 unique image identifiers. Checksums were generated for prediction files, manifests, logs, and reports. Statistical analyses were performed in Python using pandas, NumPy, SciPy, and scikit-learn; exact package versions and run details are reported in Supplementary Table S9. Raw PIID images are not redistributed. Selected images reproduced as representative misclassification examples are included with permission from the dataset author and with citation to the source PIID publication.
RESULTS
Dataset characteristics and standardized analysis integrity
The PIID dataset contained 1,091 labeled PI images (Stage I: n = 230, 21.1%; Stage II: n = 313, 28.7%; Stage III: n = 275, 25.2%; Stage IV: n = 273, 25.0%). The combined Stage III/IV class comprised 548 images for the primary three-class analysis and for the advanced-intervention threshold analysis. All 10 model/prompt conditions were evaluated using a standardized, resume-safe API pipeline with per-image logging. All conditions produced parsed predictions for all 1,091 images, with no failed predictions, no duplicate image identifiers, and identical stage distributions across condition files (Supplementary Table S2). Table 1 presents the dataset stage distribution, Table 2 summarizes the standardized-analysis performance metrics, and Fig. 1 summarizes the study design and key findings.
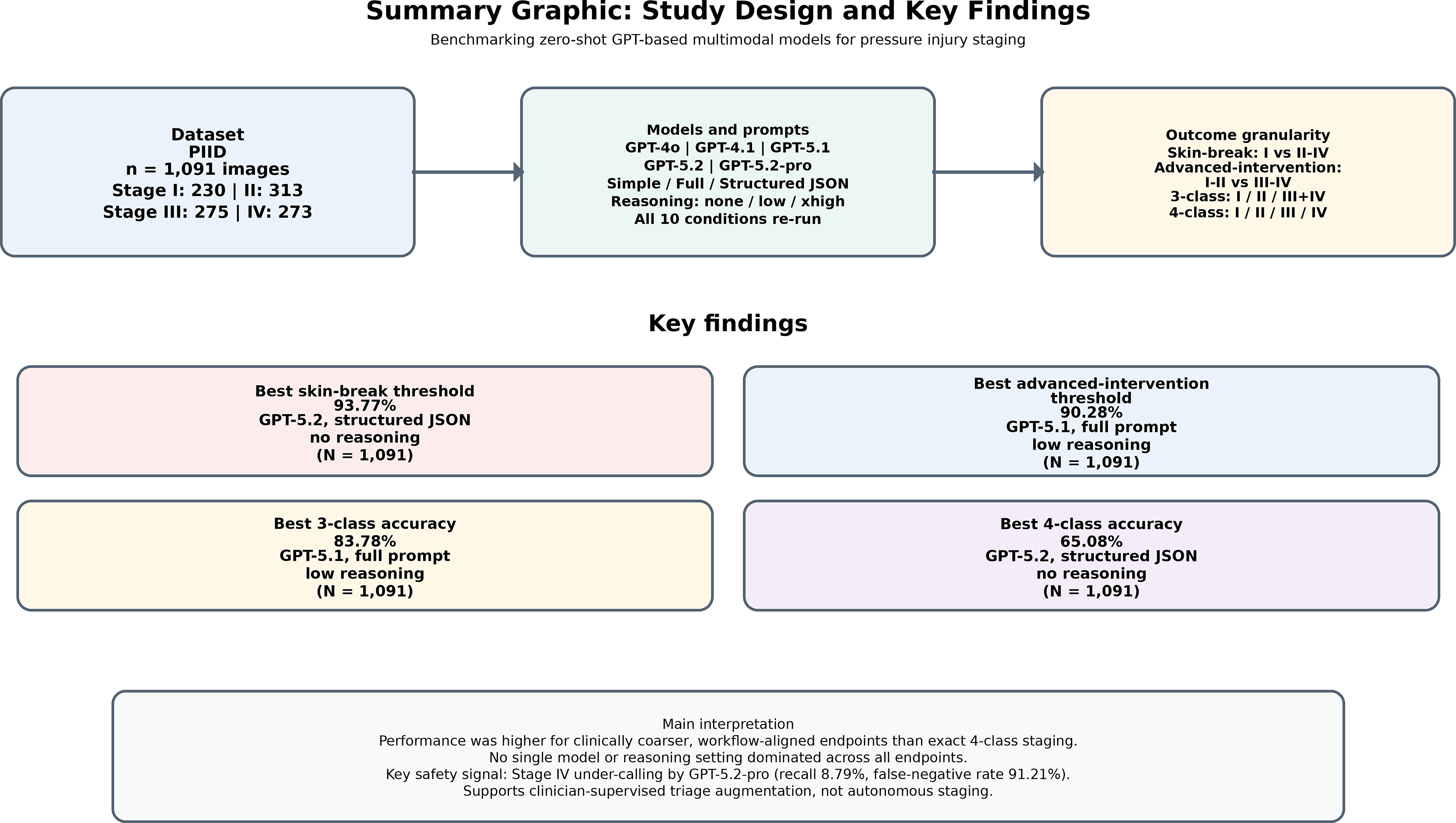
Summary graphic of the standardized full-rerun study design and key findings. The figure summarizes the PIID dataset (N = 1,091), evaluated zero-shot GPT-based multimodal model conditions, outcome definitions, and key performance/safety findings from the standardized rerun. The revised two-class endpoints distinguish the skin-break screening threshold (Stage I vs. Stage II–IV) from the advanced-intervention threshold (Stage I–II vs. Stage III–IV). GPT, generative pretrained transformer; PIID, Pressure Injury Images Dataset.
Distribution of wound images by pressure injury stage
Standardized full-rerun performance across model and prompt conditions
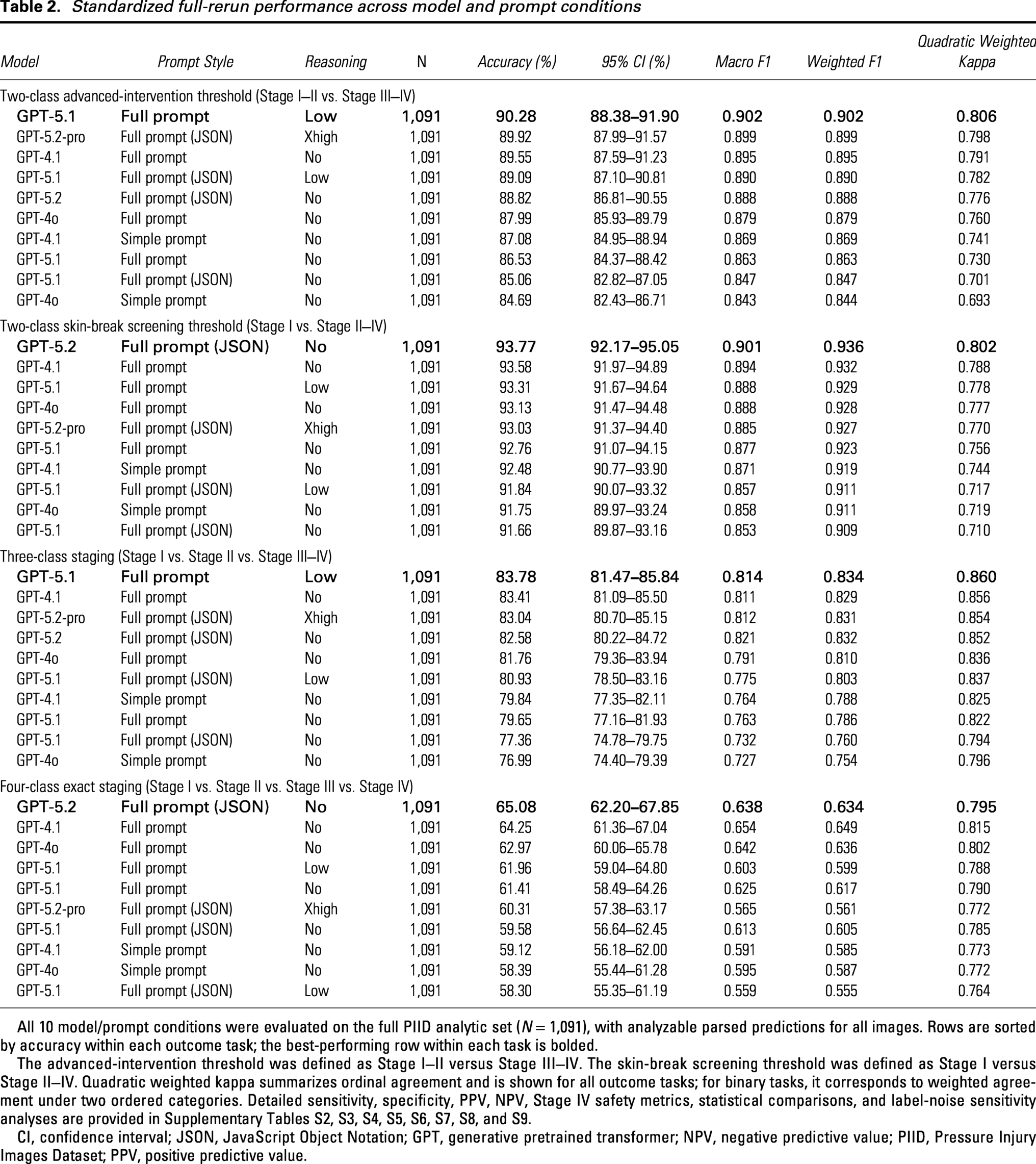
All 10 model/prompt conditions were evaluated on the full PIID analytic set (N = 1,091), with analyzable parsed predictions for all images. Rows are sorted by accuracy within each outcome task; the best-performing row within each task is bolded.
The advanced-intervention threshold was defined as Stage I–II versus Stage III–IV. The skin-break screening threshold was defined as Stage I versus Stage II–IV. Quadratic weighted kappa summarizes ordinal agreement and is shown for all outcome tasks; for binary tasks, it corresponds to weighted agreement under two ordered categories. Detailed sensitivity, specificity, PPV, NPV, Stage IV safety metrics, statistical comparisons, and label-noise sensitivity analyses are provided in Supplementary Tables S2, S3, S4, S5, S6, S7, S8, and S9.
CI, confidence interval; JSON, JavaScript Object Notation; GPT, generative pretrained transformer; NPV, negative predictive value; PIID, Pressure Injury Images Dataset; PPV, positive predictive value.
Primary outcome: Three-class staging performance
For the primary three-class task (Stage I vs. Stage II vs. Stage III/IV), the top-performing condition was GPT-5.1 with the full prompt and low reasoning, with an accuracy of 83.78% (95% CI: 81.47–85.84), macro F1 of 0.814, weighted F1 of 0.834, and quadratic weighted kappa of 0.860 (Table 2). GPT-4.1 with the full prompt performed similarly (accuracy 83.41%; 95% CI: 81.09–85.50; quadratic weighted kappa 0.856), followed by GPT-5.2-pro with structured JSON and xhigh reasoning (accuracy 83.04%; 95% CI: 80.70–85.15; quadratic weighted kappa 0.854) and GPT-5.2 with structured JSON and no reasoning (accuracy 82.58%; 95% CI: 80.22–84.72; quadratic weighted kappa 0.852). The row-normalized confusion matrix for this best-performing three-class condition is shown in Fig. 2.
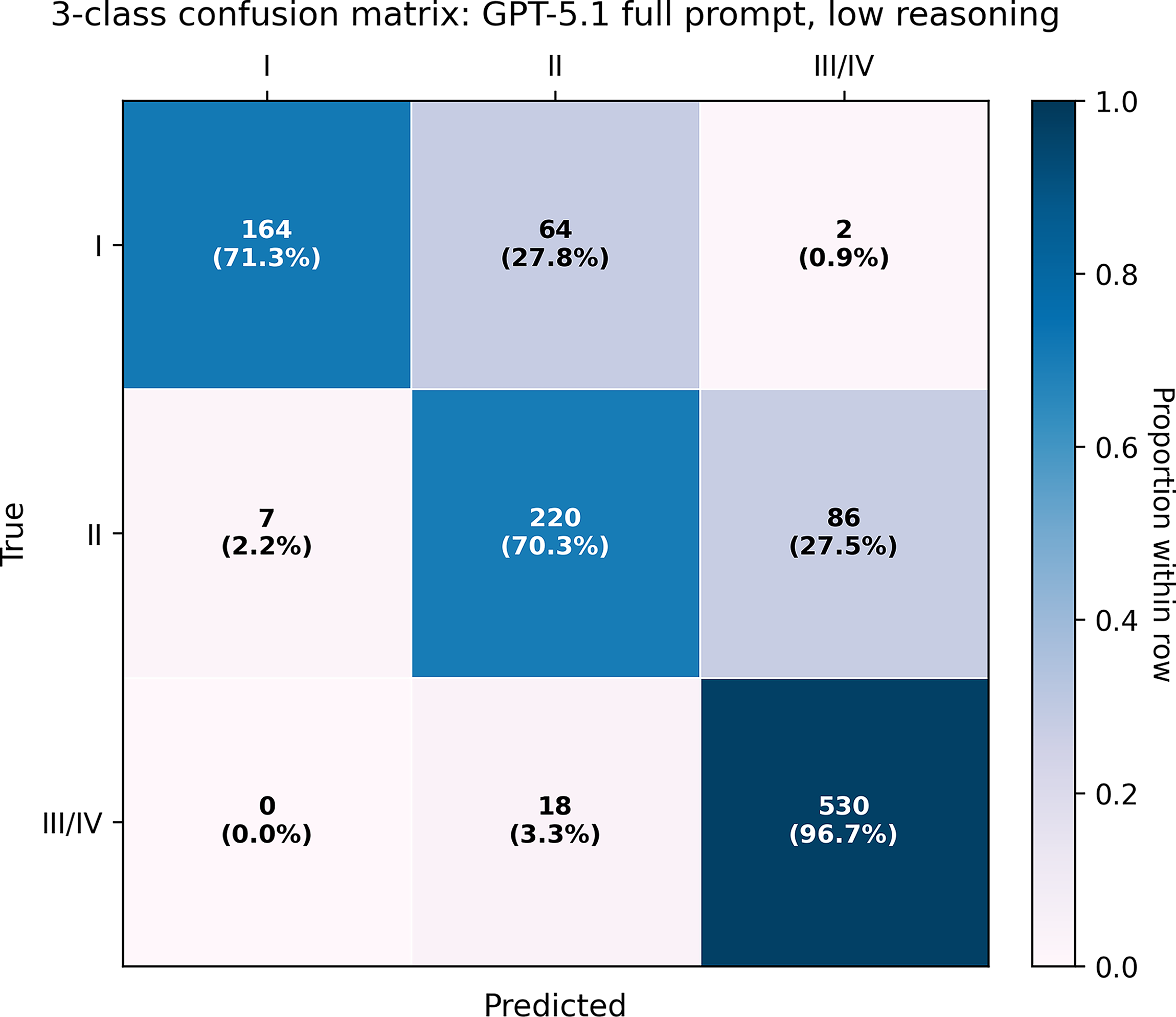
Three-class confusion matrix for the best-performing primary three-class condition: GPT-5.1 with full prompt and low reasoning. Rows indicate true labels, and columns indicate predicted labels for Stage I, Stage II, and combined Stage III/IV. Each cell reports the raw count and row percentage; shading indicates the proportion within each true-stage row.
Across all 10 conditions, three-class accuracy ranged from 76.99% to 83.78%. Cochran Q testing on the common image set (N = 1,091 for all conditions) indicated statistically significant heterogeneity in the paired correctness patterns across conditions (p < 0.001; Supplementary Table S7A). Pairwise McNemar tests with Holm adjustment are provided in Supplementary Table S7B and should be interpreted as exploratory because multiple related model/prompt conditions were compared.
Secondary outcome: Exact four-class staging
For exact four-class staging (Stage I vs. Stage II vs. Stage III vs. Stage IV), overall performance remained modest. The highest exact-stage accuracy was observed for GPT-5.2 with structured JSON and no reasoning (65.08%; 95% CI: 62.20–67.85), with macro F1 of 0.638, weighted F1 of 0.634, and quadratic weighted kappa of 0.795. GPT-4.1 with the full prompt achieved 64.25% accuracy (95% CI: 61.36–67.04) and the highest quadratic weighted kappa among the exact-stage conditions (0.815), indicating that ordinal agreement can remain relatively high even when exact-stage accuracy is limited. GPT-4o with the full prompt achieved 62.97% accuracy (95% CI: 60.06–65.78). The row-normalized exact-stage confusion matrix for the best-performing four-class condition is shown in Fig. 3.
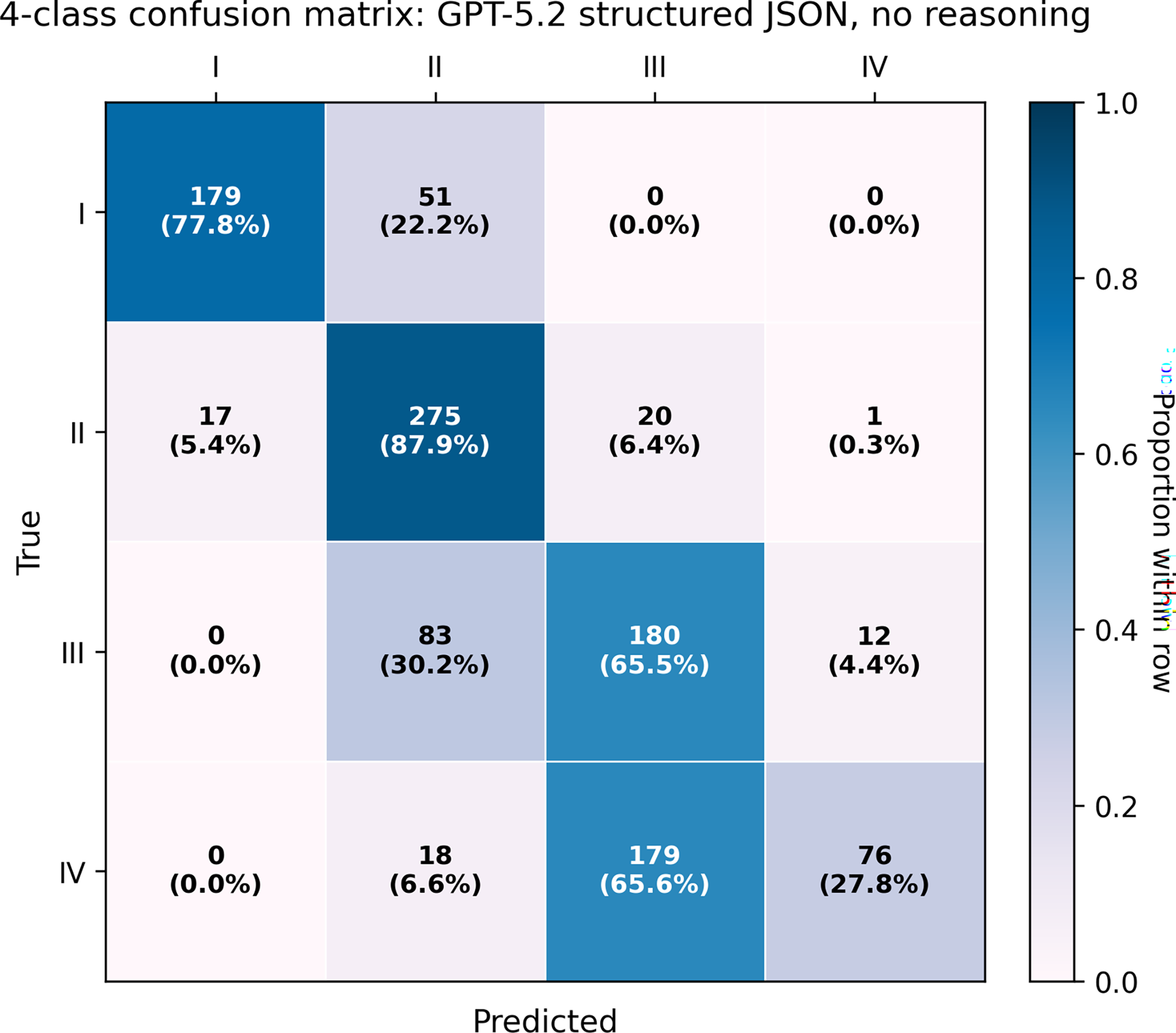
Exact four-class confusion matrix for the best-performing exact-stage condition: GPT-5.2 with structured JSON output and no reasoning. Rows indicate true labels, and columns indicate predicted labels for Stages I–IV. Each cell reports the raw count and row percentage; shading indicates the proportion within each true-stage row. JSON, JavaScript Object Notation.
Across all conditions, four-class accuracy ranged from 58.30% to 65.08%, and Cochran Q testing again showed significant heterogeneity across conditions (p = 3.44 × 10−9; Supplementary Table S7A). These results reinforce that exact four-stage assignment from photographs remains substantially more difficult than clinically coarser triage-oriented tasks.
Clinically actionable binary thresholds
For the original skin-break screening threshold (Stage I vs. Stage II–IV), performance was high across conditions. The best condition was GPT-5.2 with structured JSON and no reasoning, with accuracy of 93.77% (95% CI: 92.17–95.05), macro F1 of 0.901, weighted F1 of 0.936, and quadratic weighted kappa of 0.802. Sensitivity for Stage II–IV was 98.03%, specificity for Stage I was 77.83%, PPV was 94.30%, and NPV was 91.33% (Supplementary Table S3).
To evaluate a more clinically actionable management threshold, we also evaluated an advanced-intervention threshold defined as Stage I–II versus Stage III–IV. For this endpoint, the best-performing condition was GPT-5.1 with the full prompt and low reasoning, with accuracy of 90.28% (95% CI: 88.38–91.90), sensitivity of 96.72%, specificity of 83.79%, PPV of 85.76%, NPV of 96.19%, macro F1 of 0.902, weighted F1 of 0.902, and quadratic weighted kappa of 0.806. Across conditions, this threshold yielded accuracies ranging from 84.69% to 90.28%, supporting its use as a clinically interpretable triage endpoint for distinguishing lower-stage injuries from injuries more likely to require advanced wound intervention or specialist review.
Stage IV safety and adjacent-stage error patterns
Stage IV undercalling remained the most safety-relevant error pattern. In exact four-class staging, Stage IV recall varied widely across conditions, from 8.79% for GPT-5.2-pro with structured JSON and xhigh reasoning to 48.35% for GPT-5.1 with structured JSON and no reasoning (Supplementary Table S5). GPT-5.2-pro was highly specific for Stage IV (specificity 99.63%) and had high Stage IV precision (88.89%), but its false-negative rate was 91.21%, with 245 of 273 true Stage IV images (89.74%) predicted as Stage III. This pattern indicates that the model rarely selected Stage IV unless overt features were present and would be unsafe as an autonomous exact-stage classifier. The exact-stage confusion matrix for GPT-5.2-pro is shown in Fig. 4 to visualize this Stage IV undercalling pattern.
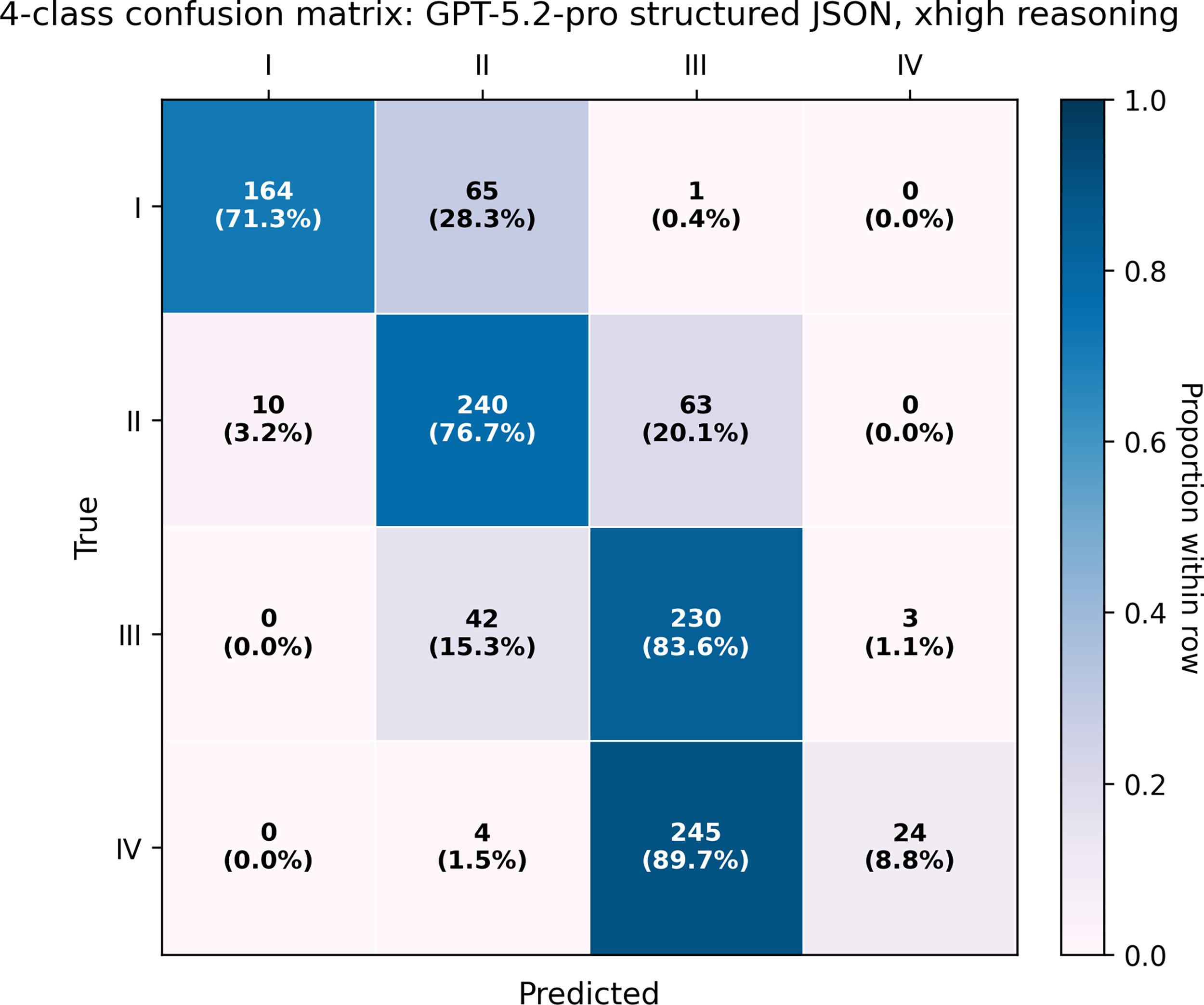
Exact four-class confusion matrix for GPT-5.2-pro with structured JSON output and xhigh reasoning. This condition is shown because it illustrates the safety-relevant Stage IV undercalling pattern: many true Stage IV images were predicted as Stage III. Each cell reports the raw count and row percentage; shading indicates the proportion within each true-stage row.
Most exact-stage errors were adjacent-stage errors. Depending on the condition, adjacent errors accounted for 95.0% to 99.8% of all exact-stage errors (Supplementary Table S6). Stage II overcalling into Stage III/IV ranged from 6.7% of true Stage II images for GPT-5.2 structured JSON to 50.2% for GPT-4o simple prompt. Stage IV undercalling as Stage III ranged from 51.6% to 89.7% of true Stage IV images. Representative examples of the dominant misclassification patterns are shown in Fig. 5.
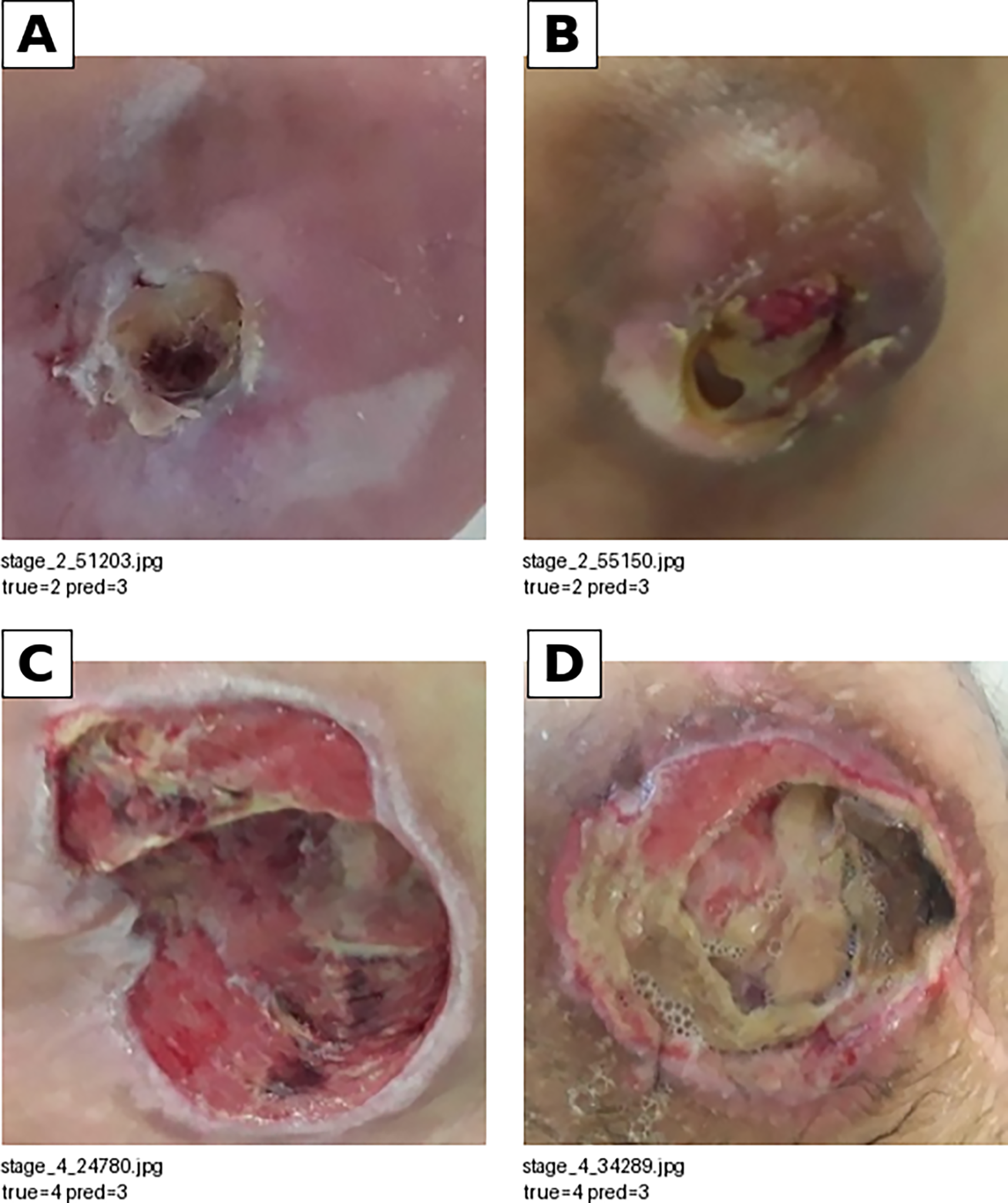
Representative misclassification examples from the PIID dataset. Panels (
Label-noise sensitivity analysis
Because the PIID source labels were used as the operational reference standard and the dataset did not report rater count, adjudication, or interrater agreement statistics, we performed a post hoc adjacent-label-noise sensitivity analysis (Supplementary Table S8). For the best exact four-class condition (GPT-5.2 structured JSON, no reasoning), simulated adjacent-stage label perturbation shifted mean accuracy from the observed 65.08% to 63.39% under 5% adjacent-label noise, 61.15% under 10% noise, and 59.68% under 15% noise. For the best three-class condition (GPT-5.1 full prompt, low reasoning), mean accuracy under simulated label perturbation was 81.89%, 80.10%, and 78.49% for 5%, 10%, and 15% adjacent-label noise, respectively. These simulations do not estimate the true label-error rate in PIID; rather, they illustrate that modest adjacent-stage uncertainty could materially affect apparent performance, particularly for exact four-class staging.
Implementation and reproducibility summaries
All 10 standardized analysis conditions were executed with per-image logging and analyzable predictions for all 1,091 images. Model execution parameters, run dates, latency, token summaries, and retry-related information are summarized in Supplementary Table S9. GPT-5.2-pro with xhigh reasoning had the longest mean latency and the largest reasoning-token burden, whereas other conditions completed substantially faster. These data contextualize the practical implementation trade-off between extended reasoning and throughput.
DISCUSSION
In this standardized benchmark using the PIID, we evaluated 10 GPT-based multimodal model/prompt conditions on the same 1,091 Stage I–IV PI images, with analyzable parsed outputs for every image in every condition. The principal finding is that model performance depended strongly on outcome formulation. The best exact four-class accuracy remained modest at 65.08% (GPT-5.2 structured JSON, no reasoning; quadratic weighted kappa, 0.795), whereas the primary three-class task achieved 83.78% accuracy (GPT-5.1 full prompt, low reasoning; quadratic weighted kappa, 0.860). The clinically actionable Stage I–II versus Stage III–IV threshold achieved 90.28% accuracy, 96.72% sensitivity, and 96.19% negative predictive value under the best condition (GPT-5.1 full prompt, low reasoning). These findings support the interpretation that photo-based GPT model outputs are more suitable for triage-oriented risk stratification than for autonomous exact staging.
Because the original binary task (Stage I vs. Stage II–IV) does not fully reflect escalation-oriented clinical decision-making, we distinguish two binary thresholds in the current analysis. The skin-break threshold (Stage I vs. Stage II–IV) captures the transition from intact skin to skin loss or deeper tissue involvement and may be relevant for early documentation and screening. In contrast, the advanced-intervention threshold (Stage I–II vs. Stage III–IV) better corresponds to escalation toward specialist wound review, debridement assessment, infection evaluation, and possible reconstructive or advanced wound intervention. This latter threshold is clinically more actionable than the skin-break grouping and is therefore reported as a major secondary analysis.
The three-class task remains justified as the primary endpoint because it preserves clinically meaningful distinctions while acknowledging the limits of photograph-only staging. Stage I represents intact skin injury; Stage II represents partial-thickness skin loss; and the combined Stage III–IV category represents advanced full-thickness injury requiring escalation. This grouping is also aligned with known staging uncertainty: differentiating Stage III from Stage IV often depends on features such as exposed bone, tendon, or muscle, undermining, tunneling, and wound depth, which may not be visible or reliably inferable from a single two-dimensional photograph. Therefore, the three-class endpoint is not merely a mathematically easier task; it is a clinically motivated compromise between oversimplified binary screening and exact staging that may exceed what photographs alone can support.
A central safety finding is that severe-stage false negatives remain clinically important even when global performance appears acceptable. In the standardized analysis, GPT-5.2-pro with structured JSON and xhigh reasoning showed high Stage IV precision (88.89%) but very low Stage IV recall (8.79%), corresponding to a Stage IV false-negative rate of 91.21%; 245 out of 273 true Stage IV cases (89.74%) were undercalled as Stage III. Other conditions had higher Stage IV recall, but Stage IV false-negative rates remained clinically meaningful. This pattern illustrates the asymmetry of wound-staging errors: understaging a Stage IV injury may delay urgent escalation, debridement consideration, infection evaluation, or surgical consultation, whereas overstaging an early injury may primarily increase review burden. Consequently, accuracy alone is insufficient for clinical interpretation; safety-relevant metrics such as Stage IV recall, false-negative rate, and NPV must be reported and monitored.
Most four-class errors occurred between adjacent stages, which supports both the clinical plausibility of the error pattern and the need for ordinal metrics. For example, adjacent-stage errors accounted for the great majority of exact-staging errors across conditions, and Stage II to Stage III/IV overcalling and Stage IV to Stage III undercalling were prominent patterns. Reporting quadratic weighted kappa, macro F1, weighted F1, threshold-based sensitivity/specificity, and false-negative rates provides a more clinically informative interpretation than accuracy alone. The exploratory Cochran Q analyses also showed statistically significant differences in paired correctness patterns across the 10 conditions for all evaluated tasks, although pairwise comparisons should be interpreted cautiously because effect sizes were modest and multiple comparisons were performed.
Ground-truth uncertainty remains a major determinant of the apparent performance ceiling. The PIID release does not report whether stage labels were assigned by a single evaluator, multiple raters, or consensus adjudication, nor does it provide interrater agreement statistics for the released labels. This limitation is important because PI staging is subjective, especially for Stage II versus Stage III and Stage III versus Stage IV boundaries. Published studies of PI classification, particularly photograph-based assessments, have reported only moderate interrater reliability and substantial boundary ambiguity.9–15 In the label-noise sensitivity analysis, simulated adjacent-stage label perturbations of 5%, 10%, and 15% materially shifted apparent accuracy and quadratic weighted kappa, especially for exact four-class staging. These simulations do not establish the true label error rate; rather, they demonstrate that observed model accuracy is jointly determined by model capability, label quality, and inherent staging ambiguity.
The clinical realism of image-only inference is also limited. Comprehensive PI assessment is multimodal and includes wound depth, undermining, tunneling, exudate, odor, surrounding skin, perfusion, infection signs, pain, anatomical site, offloading status, and longitudinal change. A single two-dimensional photograph cannot reliably capture all of these features. The current benchmark also excludes deep tissue injury (DTI), unstageable PIs, mucosal PIs, and mixed-etiology lesions. Therefore, the findings apply only to visible Stage I–IV categories represented in PIID and should not be generalized to the full spectrum of PI diagnosis or wound-care decision-making. A clinically realistic workflow would likely require an initial image-quality and category-screening step, followed by human review for unstageable, deep tissue, infected, ischemic, or otherwise uncertain wounds.
The present study should also be positioned relative to prior wound AI systems, but Table 3 should not be interpreted as a direct performance ranking across model families. In particular, supervised convolutional neural network (CNN) and transfer-learning models, including the original PIID study by Ay et al., were trained and tested using labeled PIID split data, whereas the present GPT-based models used no PIID images or labels for task-specific training, fine-tuning, reinforcement learning, or few-shot prompting. Thus, higher in-dataset supervised CNN performance is expected to reflect, at least in part, target-dataset training exposure, whereas the zero-shot GPT setting evaluates a different deployment premise: prompt-based inference without local model training. Conversely, supervised train/test split estimates may be optimistic when cross-validation and external validation are limited. Other wound-care systems and research pipelines emphasize wound measurement, segmentation, tissue composition, infection risk, or longitudinal monitoring rather than direct PI staging. Commercial and research-stage wound platforms such as digital wound measurement and documentation tools are therefore not direct equivalents to the present zero-shot GPT benchmark. The contribution of this study is not that GPT-based MLLMs outperform supervised wound models; rather, it provides a prompt-transparent, inference-only baseline showing what general-purpose GPT-family vision-language models can and cannot do without task-specific training. Table 3 provides a contextual comparison to clarify differences in task, training paradigm, data requirements, and clinical output.
Contextual comparison with prior pressure injury and wound-artificial intelligence systems
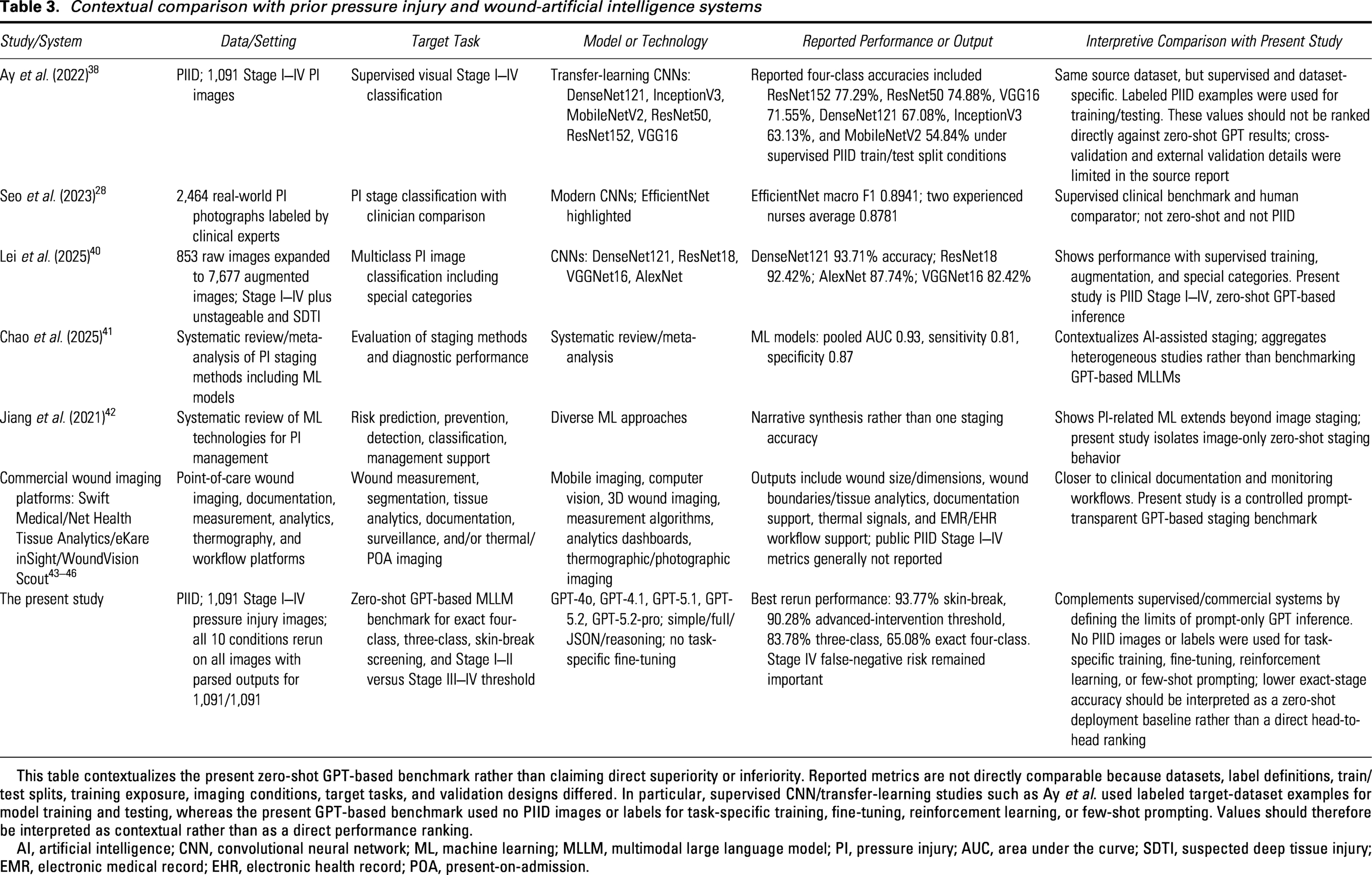
This table contextualizes the present zero-shot GPT-based benchmark rather than claiming direct superiority or inferiority. Reported metrics are not directly comparable because datasets, label definitions, train/test splits, training exposure, imaging conditions, target tasks, and validation designs differed. In particular, supervised CNN/transfer-learning studies such as Ay et al. used labeled target-dataset examples for model training and testing, whereas the present GPT-based benchmark used no PIID images or labels for task-specific training, fine-tuning, reinforcement learning, or few-shot prompting. Values should therefore be interpreted as contextual rather than as a direct performance ranking.
AI, artificial intelligence; CNN, convolutional neural network; ML, machine learning; MLLM, multimodal large language model; PI, pressure injury; AUC, area under the curve; SDTI, suspected deep tissue injury; EMR, electronic medical record; EHR, electronic health record; POA, present-on-admission.
The zero-shot design is both a strength and a limitation. We define zero-shot here as the absence of labeled PI image exemplars or task-specific few-shot examples in the prompt; definition-rich prompts may still contain textual staging criteria and decision rules. This design isolates the performance of general-purpose models under transparent prompting, but it is not necessarily the optimal clinical deployment strategy. In real-world wound assessment, domain adaptation, supervised fine-tuning, retrieval-augmented reference examples, few-shot prompting, or specialized open-source vision-language models may improve performance and calibration. Because this study evaluated only GPT-family models, it should be framed as a GPT-based benchmark rather than a comprehensive evaluation of all multimodal foundation models. Non-GPT models, open-source VLMs, supervised CNN/transformer baselines, and fine-tuned wound-specific systems remain important comparators for future work.
From a workflow perspective, the most defensible near-term use case is clinician-supervised triage augmentation rather than autonomous staging. In remote monitoring or nursing screening workflows, model outputs could be used to flag images likely to represent Stage III–IV injury, prioritize cases for specialist review, or prompt standardized reassessment when deterioration is suspected. However, such use would require explicit governance: low-confidence or high-severity predictions should trigger mandatory clinician review; suspected Stage III–IV or unstageable cases should be escalated regardless of exact-stage assignment; and false-negative patterns, especially Stage IV undercalling, should be audited after deployment. Model outputs should support—not override—wound clinician judgment.
Generalizability and fairness require particular caution. This was a single-dataset benchmark using images without structured metadata on care setting, anatomical site, camera device, lighting, dressing status, or skin tone. The absence of skin-tone annotation precludes stratified fairness assessment, even though erythema and early PI appearance can differ across skin tones. External validation across diverse care settings, body sites, skin tones, image-acquisition protocols, and clinical categories is therefore essential before clinical adoption.
In summary, the standardized analysis strengthens the reproducibility and interpretability of this benchmark by eliminating analyzable-N inconsistencies and enabling per-image paired analyses and expanded clinical metrics. The results suggest that GPT-based MLLMs can support coarse triage-oriented PI assessment, especially for Stage I–II versus Stage III–IV prioritization, but remain insufficient for autonomous exact Stage I–IV classification. Future studies should compare GPT models against supervised and open-source baselines, evaluate domain-adapted and few-shot strategies, include DTI and unstageable categories, incorporate uncertainty and calibration, and prospectively test human–AI workflow safety in clinical wound-care settings.
KEY FINDINGS
Across all models, performance improved substantially when the task was simplified from exact four-class staging to clinically coarser three-class or two-class formulations. A standardized analysis of 10 GPT-based model/prompt conditions produced parsed outputs for 1,091/1,091 images in every condition, enabling common-sample comparisons across all conditions. Clinically coarser tasks outperformed exact staging: best accuracies were 93.77% for Stage I versus II–IV, 90.28% for Stage I–II versus III–IV, 83.78% for three-class staging, and 65.08% for exact four-class staging. The advanced-intervention threshold (Stage I–II vs. III–IV) showed high sensitivity and NPV in the best condition (96.72% and 96.19%), supporting supervised triage/prioritization rather than autonomous staging. Stage IV undercalling remained safety-relevant, especially for GPT-5.2-pro (recall 8.79%; false-negative rate 91.21%), requiring clinician oversight and escalation safeguards. The exact-stage confusion matrix for GPT-5.2-pro is shown in Fig. 4 to visualize this Stage IV undercalling pattern.
INNOVATION
AI-based PI image analysis has largely relied on supervised deep learning, whereas prompt-transparent evaluation of general-purpose GPT-based MLLMs remains limited. In a standardized analysis of 10 conditions, all outputs were analyzable for 1,091 images. We show that clinically coarser thresholds achieved higher performance than exact staging: 93.77% for skin-break screening, 90.28% for Stage I–II versus III–IV, and 65.08% for exact four-class staging. By adding weighted kappa, F1, sensitivity/specificity, and Stage IV false-negative metrics, this work defines a safer triage-oriented role for MLLMs.
ACKNOWLEDGMENTS AND FUNDING INFORMATION
This work was supported by the
Supplemental Material
sj-docx-1-wnd-10.1177_21621918261465916 — Supplemental material for Benchmarking Zero-Shot Generative Pre-Trained Transformer-Based Multimodal Large Language Models for Pressure Injury Staging
Supplemental material, sj-docx-1-wnd-10.1177_21621918261465916 for Benchmarking Zero-Shot Generative Pre-Trained Transformer-Based Multimodal Large Language Models for Pressure Injury Staging by Toshiaki Takahashi, Kengo Miyo, and Nao Tamai
Supplemental Material
sj-docx-2-wnd-10.1177_21621918261465916 — Supplemental material for Benchmarking Zero-Shot Generative Pre-Trained Transformer-Based Multimodal Large Language Models for Pressure Injury Staging
Supplemental material, sj-docx-2-wnd-10.1177_21621918261465916 for Benchmarking Zero-Shot Generative Pre-Trained Transformer-Based Multimodal Large Language Models for Pressure Injury Staging by Toshiaki Takahashi, Kengo Miyo, and Nao Tamai
Supplemental Material
sj-docx-3-wnd-10.1177_21621918261465916 — Supplemental material for Benchmarking Zero-Shot Generative Pre-Trained Transformer-Based Multimodal Large Language Models for Pressure Injury Staging
Supplemental material, sj-docx-3-wnd-10.1177_21621918261465916 for Benchmarking Zero-Shot Generative Pre-Trained Transformer-Based Multimodal Large Language Models for Pressure Injury Staging by Toshiaki Takahashi, Kengo Miyo, and Nao Tamai
Supplemental Material
sj-docx-4-wnd-10.1177_21621918261465916 — Supplemental material for Benchmarking Zero-Shot Generative Pre-Trained Transformer-Based Multimodal Large Language Models for Pressure Injury Staging
Supplemental material, sj-docx-4-wnd-10.1177_21621918261465916 for Benchmarking Zero-Shot Generative Pre-Trained Transformer-Based Multimodal Large Language Models for Pressure Injury Staging by Toshiaki Takahashi, Kengo Miyo, and Nao Tamai
Supplemental Material
sj-docx-5-wnd-10.1177_21621918261465916 — Supplemental material for Benchmarking Zero-Shot Generative Pre-Trained Transformer-Based Multimodal Large Language Models for Pressure Injury Staging
Supplemental material, sj-docx-5-wnd-10.1177_21621918261465916 for Benchmarking Zero-Shot Generative Pre-Trained Transformer-Based Multimodal Large Language Models for Pressure Injury Staging by Toshiaki Takahashi, Kengo Miyo, and Nao Tamai
Footnotes
AUTHOR DISCLOSURE AND GHOSTWRITING
The authors declare no competing financial interests relevant to this work. No ghostwriters were used in the preparation of this article.
ABOUT THE AUTHORS
Abbreviations and Acronyms
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.