
Abstract
Objective:
Dressing changes after digit replantation can trigger pain, anxiety, and local wound cooling, yet the clinical impact of cleansing solution temperature remains unclear. This study evaluated whether warmed saline irrigation improves patient experience and physiological stability during wound care after digit replantation.
Approach:
In this single-center, parallel-group randomized controlled trial, 149 patients undergoing digit replantation were randomized to receive warmed or room-temperature saline irrigation during postoperative dressing changes. Primary outcomes were pain and digit temperature assessed before, during, and after dressing changes. Secondary outcomes included anxiety, comfort, complications, and digit survival. Analyses followed the intention-to-treat principle using linear mixed-effects models. Reporting adhered to CONSORT guidelines.
Results:
Compared with room-temperature saline, warmed saline significantly reduced pain and anxiety and improved patient comfort over time (all p < 0.001). Warmed saline maintained peri-wound temperature during dressing changes, whereas room-temperature saline induced transient cooling. No between-group differences were observed in complication rates, C-reactive protein, or digit survival. Clinically meaningful improvements in pain, anxiety, and comfort were more frequent in the warmed-saline group. Exploratory analyses suggested greater benefit in younger patients and during colder seasons.
Innovation:
This trial provides preliminary randomized evidence in a microsurgical population demonstrating that warmed saline irrigation, a simple and low-cost modification, can improve patient-reported outcomes without compromising safety.
Conclusion:
Warmed saline irrigation offers a safe and practical strategy to enhance comfort and reduce distress during wound care after digit replantation. These findings highlight thermal management as an underutilized, patient-centered component of postoperative care and support its integration into routine practice.
INTRODUCTION
Maintaining microvascular stability is the central challenge in digit replantation, and postoperative wound temperature is a critical determinant of success. 1 Approximately 10–30% of patients experience postoperative vascular crises. 2 Among these crises, vasospasm and thrombosis are the most prevalent and detrimental complications. 3 Notably, the replanted digits are particularly vulnerable to cold exposure, which can trigger pathological vasospasm and compromise digital perfusion. 4 Therefore, postoperative management of the wound temperature is critical for preventing complications and promoting healing.
Lijun Lu, MS

Warmed saline irrigation has been regarded as an effective tool for wound care because it helps maintain an optimal local wound temperature and supports cellular healing processes. Clinical studies have demonstrated that dressing changes themselves significantly exacerbate wound cooling. McGuinness et al. 5 reported that the mean wound temperature decreased to 32.6°C after dressing removal. When room-temperature (29.9°C) normal saline was subsequently used for irrigation, wound temperature declined by an additional 2.4°C and required approximately 23 min to return to the pre-procedure level. Maintaining a periwound temperature ≥33°C is a prerequisite for preserving the physiological activity of key cells involved in wound repair. Neutrophils, fibroblasts, and epithelial cells are known to be temperature-sensitive during the early phases of healing, and appropriate thermal conditions effectively sustain their functional activity. 6 Furthermore, previous studies have shown that warm irrigation helps reduce cold-induced vasoconstrictive responses and maintain local thermal stability.7,8 These effects support stable microcirculatory perfusion during wound care. 9 It also reduces noxious stimuli associated with microcirculatory impairment, thereby improving patient comfort.10,11 These combined physiological and psychomodulatory actions make warmed saline irrigation a potentially beneficial option for postoperative wound care in patients undergoing digit replantation (Fig. 1A).
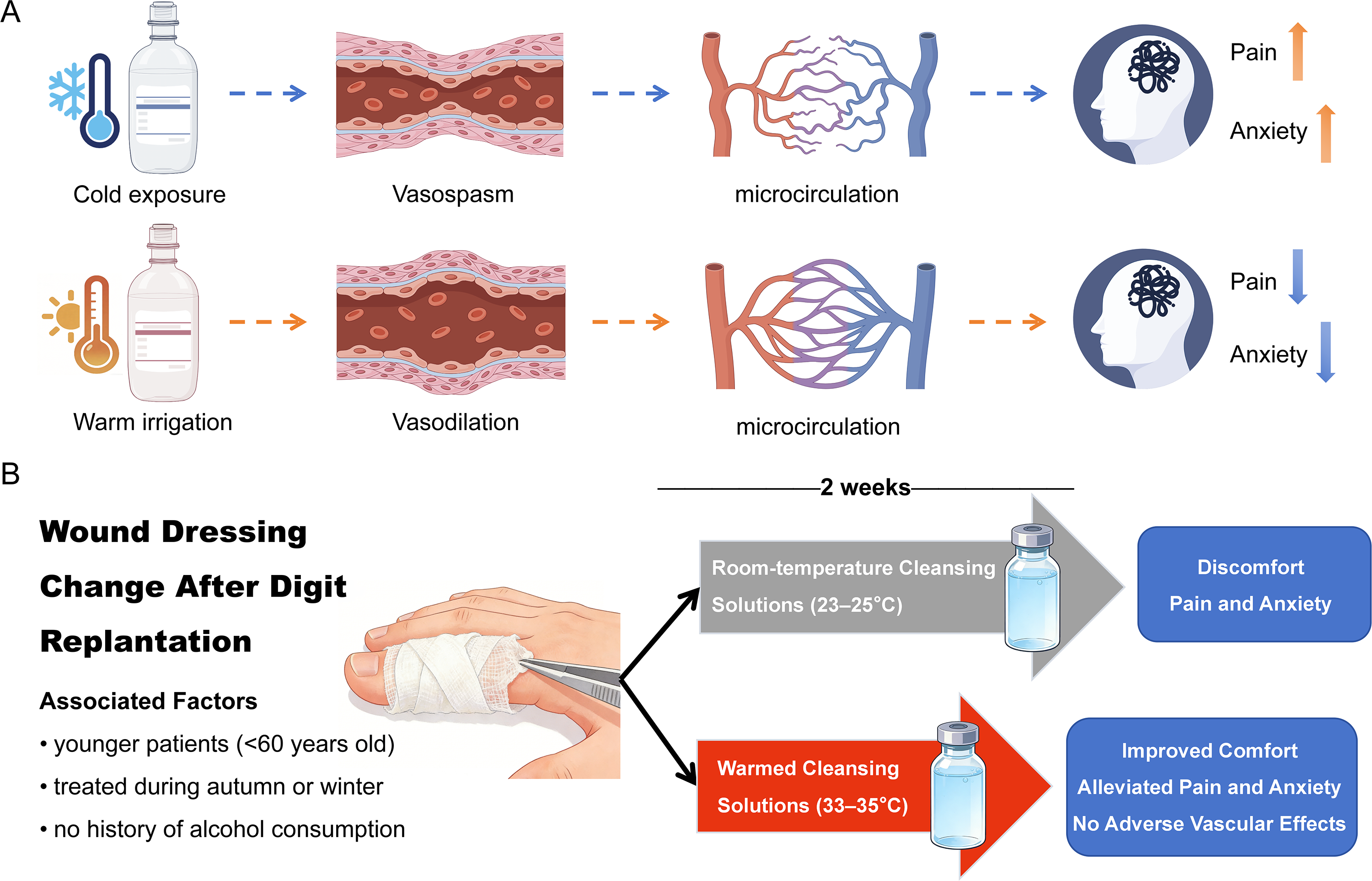
Hypothesized mechanisms and effects of warmed saline irrigation during dressing changes after digit replantation.
To date, evidence regarding the effects of warmed saline irrigation in digit replantation wound care remains limited. Existing studies have mainly focused on microvascular anastomosis techniques and perioperative blood flow management,12,13 while evidence regarding the impact of cleansing solution temperature on patient experience and local physiological responses in digital replantation remains limited.
CLINICAL PROBLEM ADDRESSED
Although increasing evidence from chronic wound care14,15 supports the use of warmed saline irrigation to mitigate heat loss during dressing changes, whether the benefits observed in chronic wound care can be translated to the unique microvascular environment of digit replantation remains unknown. Unlike chronic wounds, replanted digits rely on a fragile microvascular anastomotic network. This network is particularly sensitive to temperature fluctuations. Cold exposure may induce vasospasm and compromise perfusion. 16 Therefore, the effects of warmed saline irrigation may differ from those observed in chronic wounds. We hypothesized that, compared with room-temperature saline, warmed saline irrigation during postoperative dressing changes helps improve digit replantation patient comfort, reduce dressing change–related pain and anxiety without adversely affecting vascular outcomes (Fig. 1B). To test this hypothesis, we conducted a randomized controlled trial to evaluate the effects of warmed saline irrigation on digital replantation wounds during postoperative dressing changes. The findings provide evidence for reducing dressing change–related distress and supporting patient-centered wound care.
MATERIALS AND METHODS
Trial design
This CONSORT-compliant, two-arm parallel-group randomized controlled trial with blinded outcome assessment analyzed all patients on an intention-to-treat (ITT) basis. The trial was prospectively registered with the Chinese Clinical Trial Registry (ChiCTR2500100037). Ethical approval was obtained from the Wuxi Ninth People’s Hospital Ethics Committee (KS2025014). Electronic laboratory notebook was not used.
Participants
This single-center study was conducted at Wuxi Ninth People’s Hospital, a tertiary referral hospital specializing in hand and microsurgery. Eligible postoperative patients who underwent digit replantation surgery were consecutively recruited between April 10 and November 10, 2025.
Inclusion criteria were having undergone digit replantation surgery; being in stable general condition at the time of enrollment; being conscious and able to comply with study procedures; and providing written informed consent. Exclusion criteria included: postoperative necrosis of the replanted digit; severe or unstable systemic diseases; comorbid psychiatric disorders or cognitive impairment; extensive and severe injuries to other limbs; and coagulation disorders.
Intervention
Preheating procedure
Saline was prewarmed to 33°C–35°C 8 approximately 30 min before dressing changes using a medical fluid warming bag (Xianwei Ltd., Dongguan, China) and stored in a portable insulated container (Kegu Ltd., Guangzhou, China) with real-time temperature monitoring. Before irrigation, the temperature of the solution bag was rechecked using a digital thermometer, and irrigation was initiated only when the temperature was confirmed to be ≥33°C.
Irrigation protocol (both groups)
Dressing removal was preceded by saline-moistened gauze application to enable atraumatic detachment. Wound irrigation was performed using 20 mL saline delivered via syringe (1 mL/s, 0.5 cm above wound) in a circular motion, 17 repeated three to four times until wound cleanliness was achieved. Following irrigation, the periwound skin was disinfected with povidone-iodine, and the wound was covered with sterile gauze. Dressing changes lasted 10–20 min and were repeated every 3–5 days based on exudate levels until wound healing.
Group-specific conditions
In the intervention group, saline was maintained at 33°C–35°C; in the control group, room-temperature saline (23°C–25°C) was used with ambient temperature maintained at 25°C via air conditioning.
All procedures were performed by trained nurses following a standardized protocol. Both groups received standardized health education on nutrition, personal hygiene, and activity precautions.
Outcome measures
The primary outcomes were pain and replanted digit temperature, as the intervention was designed to maintain local temperature and reduce discomfort during dressing changes. These measures are sensitive to short-term thermal and nociceptive changes and serve as proximal indicators of microcirculatory stability and patient tolerance. In contrast, clinical outcomes such as wound survival and infection are more appropriate for evaluating longer-term effects and were therefore included as secondary outcomes. Pain was assessed using the Visual Analog Scale (VAS) at corresponding time points: immediately before the dressing change, immediately after irrigation, and immediately after completion. The scale ranges from 0 to 10, with higher scores indicating greater pain intensity. Skin temperature of the replanted digit was measured at three predefined time points: immediately before dressing removal, immediately after irrigation, and immediately after completion of the dressing change, using a Shanghai Lulin WMY-01 digital thermometer (range 0°C–50°C). Measurements were taken at the distal pulp of the replanted digit, with the probe applied gently to the skin surface until a stable reading was obtained. A photograph of the digital thermometer used for digit temperature measurement is provided in Supplementary Figure S1. Measurements were taken after removing the warming lamp, at a fixed site, and at consistent time points. A 2-week follow-up period was employed because vascular compromise and other acute complications are most likely to occur during the early postoperative phase following digital replantation. 4
The secondary outcomes included comfort, anxiety during dressing changes, incidence of complications, digit survival, and C-reactive protein (CRP) levels. Dressing change comfort was measured via the Postoperative Patient Comfort Scale (PPCS) before the first dressing change and at 1 and 2 weeks postoperatively. Fan Yaling et al. 18 developed this measure in 2021 to assess patients’ comfort during the postoperative recovery period. It consists of 10 items categorized into four dimensions: pain, physical function status, sleep and mental status, and social and emotional status. The higher the scores, the higher the patient’s comfort level.
Patient anxiety during dressing changes was evaluated via the Hospital Anxiety and Depression Scale (HADS) 19 before the first dressing change and at 1 and 2 weeks postoperatively. Zigmond and Snaith developed the HADS in 1983 to screen for anxiety and depression symptoms in hospitalized patients. The scale consists of 14 items, with seven items assessing depression and seven items assessing anxiety. Scores range from 0 to 21, with higher scores indicating greater severity of anxiety and depressive symptoms.
Digit survival was recorded within 2 weeks postoperatively. Complications, including vascular crisis, infection, and chills, were observed and recorded within the same period. Vascular crisis was defined as a replanted digit temperature >2°C lower than that of the contralateral healthy digit under the same ambient conditions, accompanied by delayed capillary refill (>3 s), pale or purplish discoloration, and abnormal tissue turgor.8,20 Postoperative CRP levels were extracted from patient medical records within 2 weeks.
The demographic and clinical information form was developed by the researchers based on a literature review, clinical practice, and expert consultation. Sociodemographic data included sex, age, ethnicity, marital status, education level, occupation, and place of residence. Clinical data included smoking history, comorbidities, alcohol consumption, type of digit injury, amputated digit, amputation plane, completeness of amputation, and ischemia time.
Sample size calculation
The sample size was calculated based on a two-sample comparison of means, with pain intensity defined as the primary outcome. A two-sided significance level of 0.05 and a statistical power of 90% were specified. Based on prior literature, 11 an expected between-group mean difference of 0.64 and a variance of 1.20 were assumed, yielding a required sample size of 124 participants. Allowing for an anticipated attrition rate of 10%, a total of 138 participants (69 per group) was considered sufficient to ensure adequate statistical power.
Randomization
Stratified randomization was performed by a researcher responsible for sequence generation. Stratification factors included the completeness of digit amputation (complete versus incomplete), warm ischemia time of the amputated digit (≤6 h versus >6 h), and smoking history (yes versus no). Within each stratum, random sequences were generated using SPSS version 26.0, and participants were assigned to either the intervention or control group according to the sequence. Patients in the intervention group received wound cleansing with a prewarmed solution maintained at 33°C–35°C, whereas patients in the control group received wound cleansing with a solution at room temperature (24°C–26°C). The study followed an open-label design with blinded outcome assessment. Due to the nature of the intervention, participants and care providers could not be blinded; however, outcome assessors remained blinded throughout the study. To minimize potential performance bias, irrigation solutions were prepared in a separate room, and temperature-related information was not disclosed to participants throughout the study.
Statistical methods
Statistical analyses were conducted according to the ITT principle, including all randomized participants. A detailed assessment of missing data was conducted before statistical analysis. Missing data occurred only at the end of the follow-up period (2 weeks later). Therefore, missingness was limited to HADS, PPCS, digit survival rate, and complication incidence.
Data were analyzed using IBM SPSS Statistics version 26.0. The normality of continuous variables was evaluated using the Shapiro–Wilk test. Continuous variables were summarized as mean ± SD for normally distributed data. Variables that did not follow a normal distribution were presented as median (interquartile range). Categorical variables were summarized as frequencies and percentages. Between-group differences were assessed using independent-samples t-tests or chi-square tests. The primary analyses were prespecified and conducted using linear mixed-effects models (LMMs) for repeated continuous outcomes. Time was treated as a categorical variable and included as a fixed effect along with treatment group and the group × time interaction. Baseline HADS score was included as a covariate to adjust for baseline imbalance. Model parameters were estimated using restricted maximum likelihood, which allows inclusion of all available data under the missing at random assumption. A random intercept was specified for each participant to account for within-subject correlation. Given the limited number of measurement time points and the absence of a priori assumptions regarding the correlation structure, an unstructured covariance matrix was used to flexibly model correlations between repeated measures. Baseline HADS scores were included as covariates to adjust for baseline imbalance. Binary outcomes were analyzed using logistic regression models.
To explore potential heterogeneity in treatment response, descriptive subgroup analyses were performed within the intervention group according to several a priori-selected stratification factors, including sex, age, smoking, alcohol consumption, diabetes mellitus, and season. Treatment response was operationalized as the change score from pre-dressing change to during dressing change. These analyses were post hoc and exploratory in nature, and the study was not designed or powered for formal interaction testing. Multiple comparisons were adjusted using the Bonferroni correction by multiplying each raw p value by the number of comparisons (m = 6). A two-sided p value <0.05 was considered statistically significant.
The proportion of patients achieving clinically meaningful change was assessed at each follow-up assessment. For digit pain, clinically significant worsening was defined as an increase of ≥10 mm on the VAS during dressing changes, based on the established minimal clinically important difference (MCID). 21 The responder analysis, therefore, assessed the proportion of patients whose pain increase remained below this threshold, indicating acceptable tolerability during the procedure. For the HADS, the established MCID of 3 points was applied, consistent with the validation study by Puhan et al. 22 For the PPCS, for which no anchor-based MCID has been established, a distribution-based approach was applied, using 0.5 standard deviation as an approximate threshold for clinically meaningful change. 23
The per-protocol (PP) population comprises participants who adhered to the study protocol without major deviations and completed the trial. The PP analysis was performed using repeated measures analysis of covariance and chi-square tests for the PP group. The assumption of sphericity was assessed using Mauchly’s test. When sphericity was violated, the Huynh–Feldt correction was applied if ε ≥ 0.75, whereas the Greenhouse–Geisser correction was used if ε < 0.75 to adjust the degrees of freedom. Effect sizes were interpreted as small, medium, and large for Cohen’s d values of 0.2, 0.5, and 0.8, respectively, and for partial η2 values of 0.01, 0.06, and 0.14, respectively. 24
RESULTS
A total of 149 patients were enrolled and randomly assigned to the intervention (n = 73) or control (n = 76) group. During follow-up, one participant (1.4%) in the intervention group and two participants (2.6%) in the control group were lost to follow-up (Fig. 2). Reasons for attrition included study withdrawal (n = 2) and hospital transfer (n = 1).
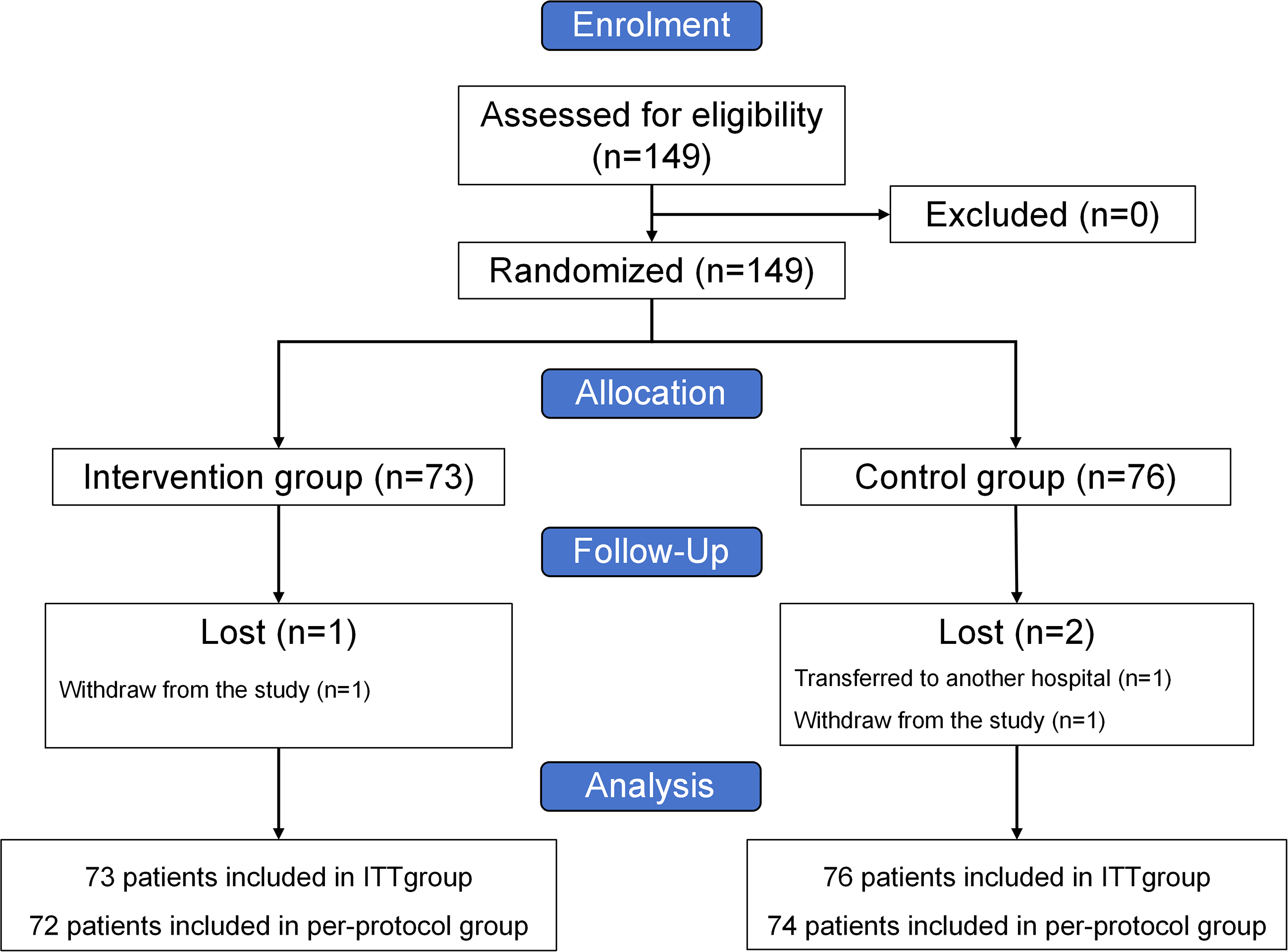
Flowchart of the study.
Participants’ ages ranged from 17 to 70 years, with a mean of 43.8 ± 12.6 years, and 64.4% were male. Baseline characteristics were comparable between groups, including age, sex, marital status, education level, smoking and alcohol consumption, income, insurance status, ischemia time of the amputated digit, type of digit injury, and amputated digit (Table 1).
Baseline patient characteristics
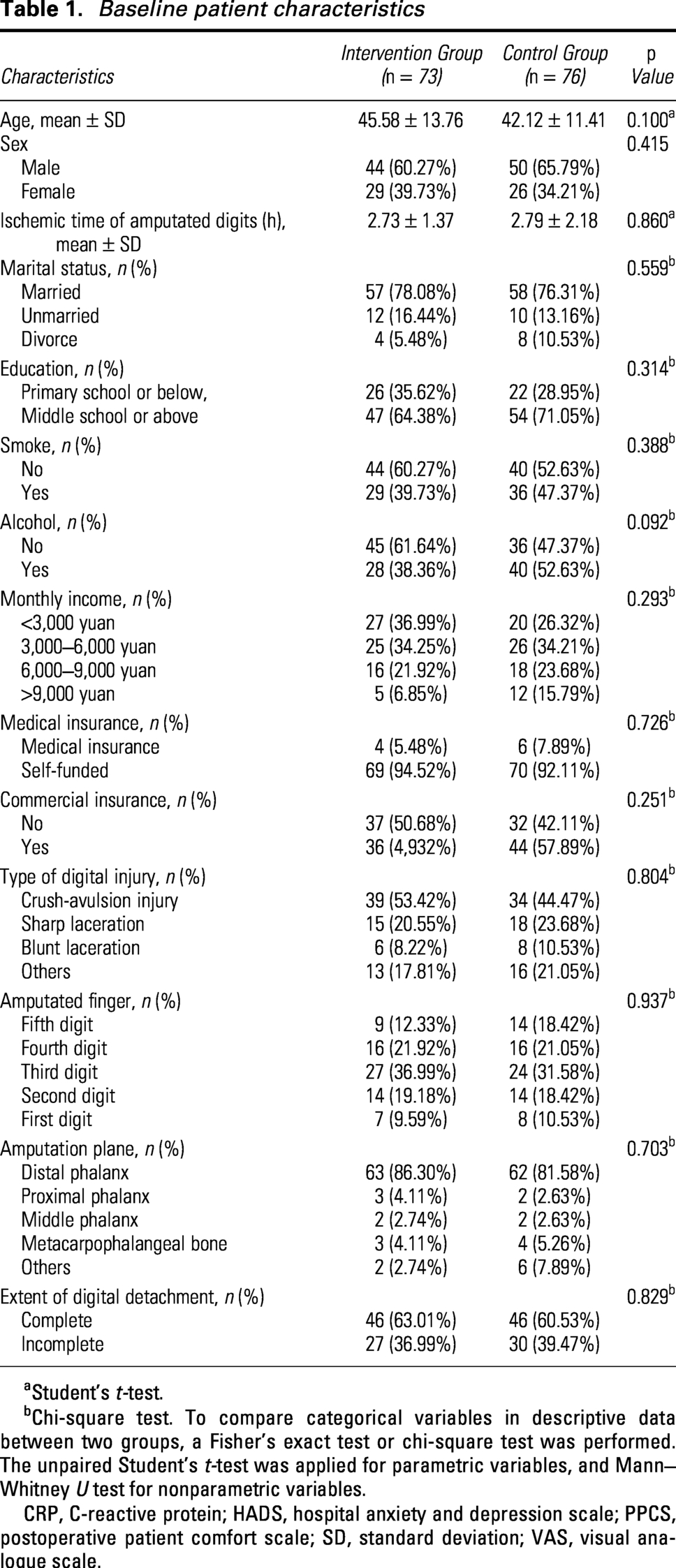
aStudent’s t-test.
bChi-square test. To compare categorical variables in descriptive data between two groups, a Fisher’s exact test or chi-square test was performed. The unpaired Student’s t-test was applied for parametric variables, and Mann–Whitney U test for nonparametric variables.
CRP, C-reactive protein; HADS, hospital anxiety and depression scale; PPCS, postoperative patient comfort scale; SD, standard deviation; VAS, visual analogue scale.
Primary outcomes
Pain intensity
Pain scores increased during dressing changes and declined thereafter in both groups; however, the intervention group exhibited a smaller rise in pain during the procedure and lower final pain scores compared with the control group. LMMs analysis revealed a significant group × time interaction (F = 20.27, p < 0.001). Baseline between-group difference was small and not statistically significant (Cohen’s d = 0.21, 95% CI: [−0.14, 0.60]), but moderate effects were observed during and after dressing change (Cohen’s d = −0.70, 95% CI: [−1.38, −0.51]; Cohen’s d = −0.72, 95% CI: [−1.40, −0.52]), suggesting a clinically meaningful benefit (Table 2).
Comparisons of outcomes between the two groups using linear mixed models
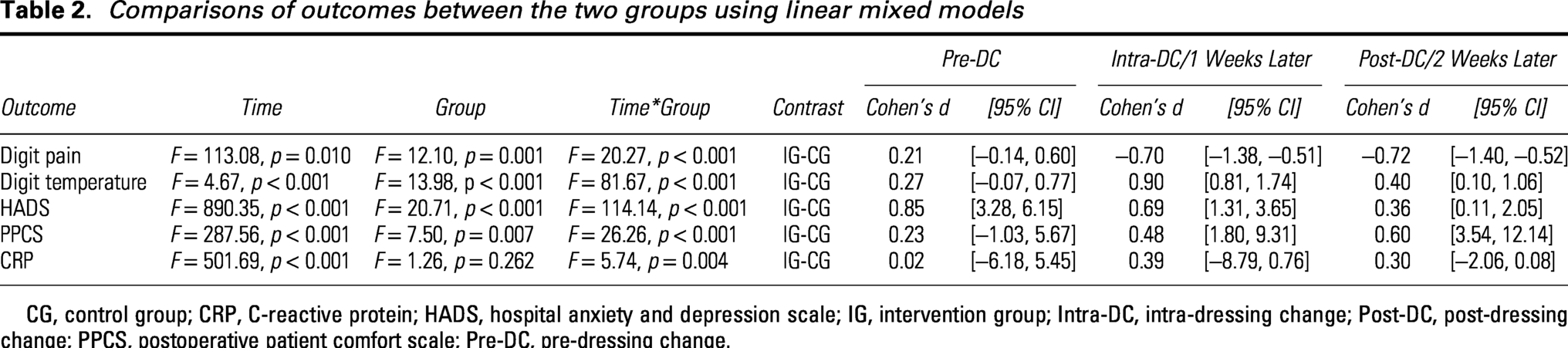
CG, control group; CRP, C-reactive protein; HADS, hospital anxiety and depression scale; IG, intervention group; Intra-DC, intra-dressing change; Post-DC, post-dressing change; PPCS, postoperative patient comfort scale; Pre-DC, pre-dressing change.
Digit temperature
Warmed solutions increased digit temperature during dressing changes; room-temperature solutions decreased digit temperature before later recovering (Fig. 3). LMMs analysis revealed a significant group-by-time interaction (F = 81.67, p < 0.001), indicating differential changes between groups over time (Table 2). Baseline between-group difference was small and not statistically significant (Cohen’s d = 0.27, 95% CI: [−0.07, 0.77]), while a large between-group effect was observed during dressing change (Cohen’s d = 0.90, 95% CI: [0.81, 1.74]), which persisted at a smaller effect post-procedure (Cohen’s d = 0.40, 95% CI: [0.10, 1.06]).
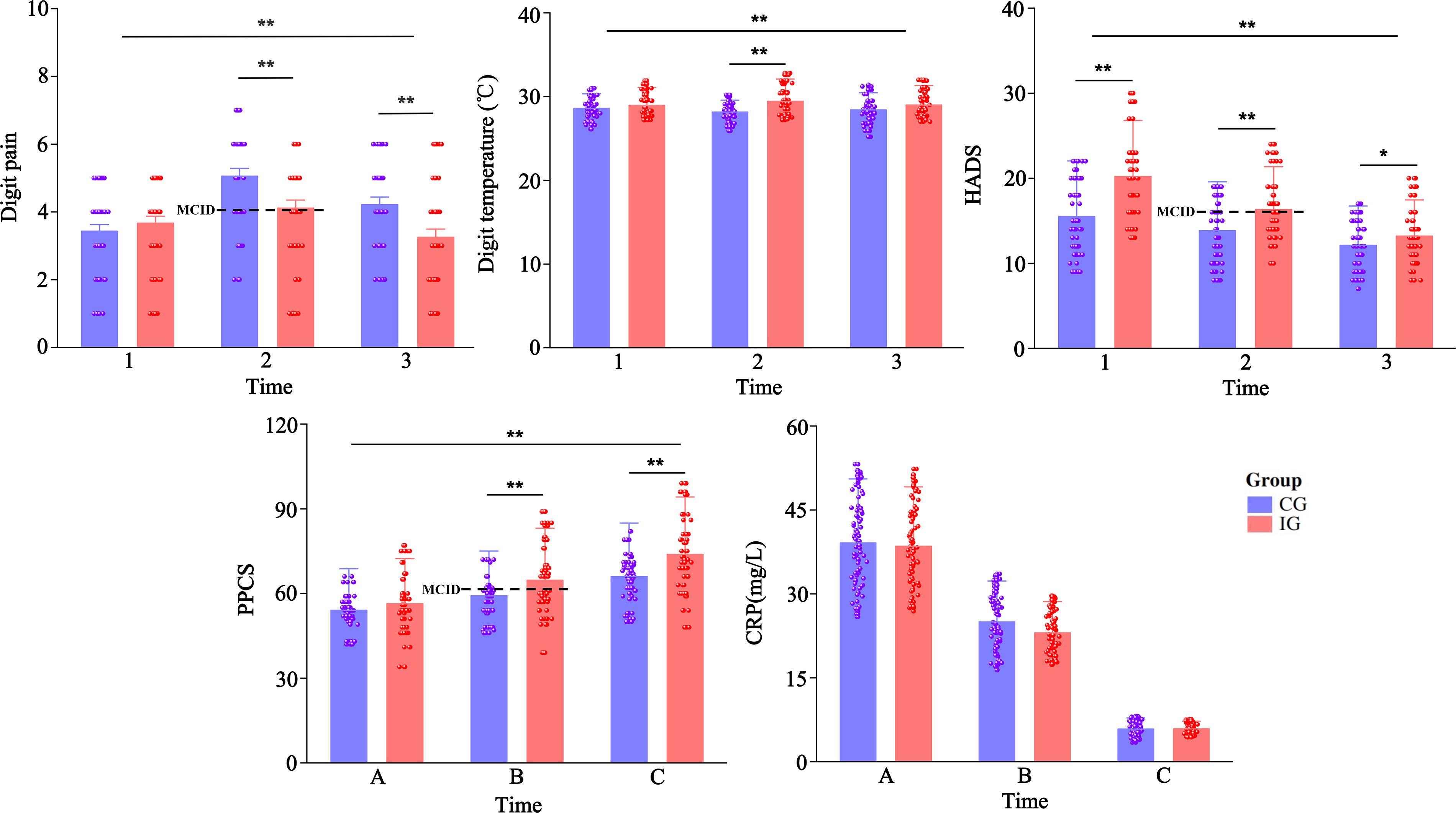
Changes in outcomes over time in the intervention and control groups. Digit pain (0, no pain; 1–3, mild pain; 4–6, moderate pain; 7–10, severe pain), the dashed horizontal line represents the minimal clinically important difference (MCID);PPCS, postoperative patient comfort scale, higher scores indicate greater comfort, scores ≥ 70 denote comfort; HADS, hospital anxiety and depression scale, higher scores indicate higher levels of anxiety and depression (0–7, no symptoms; 8–10, suspected anxiety or depression; 11–21, definite anxiety or depression); CRP, C-reactive protein, <3 mg/L under normal health conditions; Time 1/A, pre-dressing change; Time 2, intra-dressing change; Time 3, post-dressing change; Time B, 1 week later; Time C, 2 weeks later; IG, intervention group; CG, control group.
Secondary outcomes
Anxiety
HADS scores decreased over time in both groups with a significant group × time interaction (F = 114.14, p < 0.001). The intervention group showed lower scores at baseline, corresponding to a large between-group effect (Cohen’s d = 0.85, 95% CI: [3.28, 6.15]). Although the magnitude of the difference gradually diminished over time, a moderate between-group effect remained at Week 1 (Cohen’s d = 0.69, 95% CI: [1.31, 3.65]), while a small effect at Week 2 (Cohen’s d = 0.36, 95% CI: [0.11, 2.05]). Independent t-tests further indicated a significantly greater reduction in anxiety scores in the intervention group after dressing changes (p < 0.001; Supplementary Table S1).
Comfort
PPCS scores improved in both groups over time, with consistently higher values in the intervention group. A significant group-by-time interaction (F = 26.26, p < 0.001) was observed. Baseline comfort levels were comparable between groups, with a negligible between-group effect (Cohen’s d = 0.23, 95% CI: [−1.03, 5.67]). Subsequently, the intervention was associated with progressively larger effects on comfort over time, ranging from small to moderate in magnitude (Cohen’s d = 0.48, 95% CI: [1.80, 9.31]; Cohen’s d = 0.60, 95% CI: [3.54, 12.14]; Table 2).
Inflammatory marker
CRP levels gradually decreased over time in both groups. No significant between-group difference was observed (F = 1.26, p = 0.262), and effect sizes were small across all time points (Cohen’s d = 0.02–0.39; Table 2).
Digit survival and complications
No statistically significant differences were observed between the intervention and control groups in digit survival or the incidence of complications within 2 weeks postoperatively (p = 0.211, OR = 2.449; p = 0.069, OR = 0.327; Table 3).
Binary logistic regression analysis of digit survival and complications within 2 weeks between the two groups
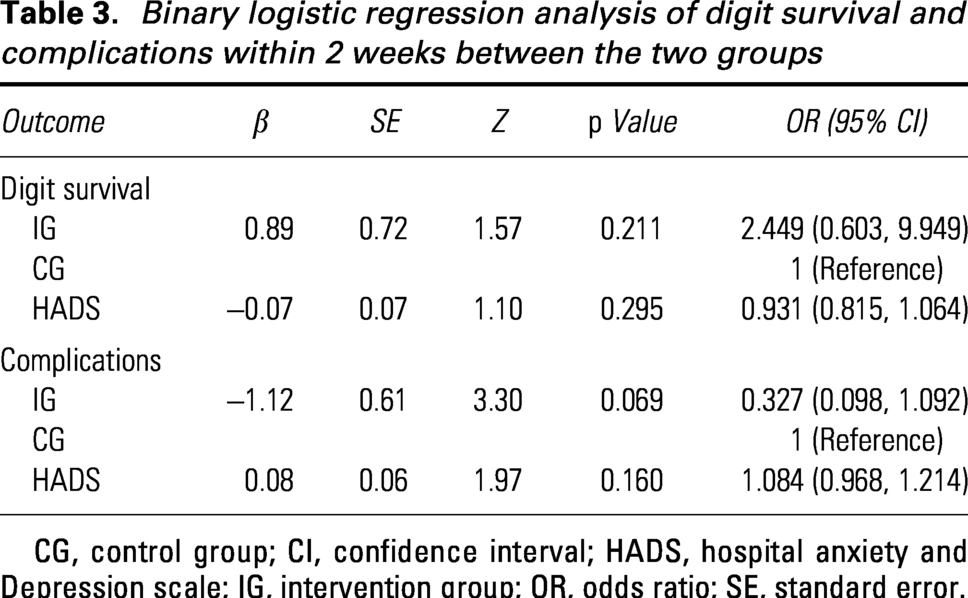
CG, control group; CI, confidence interval; HADS, hospital anxiety and Depression scale; IG, intervention group; OR, odds ratio; SE, standard error.
Sensitivity and subgroup analyses
After excluding three participants lost to follow-up, repeated outcomes for the PP population were assessed. Results from the PP population (Supplementary Tables S2 and S3) were consistent with those observed in the ITT population (Table 2; Table 3).
Exploratory subgroup analyses within the intervention group indicated that the magnitude of intervention effects on pain and digit temperature varied by patient characteristics (Supplementary Table S4): young and middle-aged patients (MD = −0.97, 95% CI: [−1.37, −0.57], p < 0.001), patients with diabetes (MD = −0.92, 95% CI: [−1.60, −0.24], p = 0.009), and those underwent surgery in the autumn/winter (MD = 0.36, 95% CI: [0.01, 0.72], p = 0.049) experienced smaller pain exacerbations following dressing changes. Patients with no history of alcohol consumption exhibited greater temperature increases after the intervention than those with a history (MD = 0.26, 95% CI: [0.02, 0.51], p = 0.033).
MCID Responder analysis
Responder analysis based on MCID thresholds revealed that a significantly higher proportion of patients in the intervention group experienced clinically acceptable pain increases compared with the control group (56.16% versus 14.67%, p < 0.001; OR = 7.45, 95% CI: [3.39, 16.41]). Similarly, a greater proportion of patients in the intervention group reached the MCID for HADS (71.23% versus 14.67%, p < 0.001; OR = 14.41, 95% CI: [6.37, 32.58]). As no validated MCID exists for the PPCS, a distribution-based estimate (0.5 SD = 5.15) was applied; the intervention group showed a higher responder rate on this criterion (76.71% versus 48.00%, p < 0.001; OR = 3.57, 95% CI: [1.76, 7.24]; Supplementary Table S5).
DISCUSSION
This study demonstrated that warmed saline irrigation improved the patient experience during dressing changes after digit replantation. Compared with room-temperature saline, warmed saline reduced pain and anxiety and increased patient comfort. Importantly, these benefits were achieved without compromising digit survival or increasing postoperative complications. These findings support the use of warmed saline irrigation as a simple, low-cost, and nonpharmacological strategy to improve patient-centered outcomes during postoperative wound care.
Regarding the primary outcomes, warmed irrigation demonstrated benefits in both digit temperature and pain relief. However, the absolute difference in digit temperature between groups during irrigation was <1°C, a magnitude unlikely to directly alter tissue metabolism or microcirculatory dynamics. 25 While physiological effects on microcirculation appear modest, the consistent and clinically meaningful improvements in patient-reported pain, anxiety, and comfort are highly relevant to practice. A substantial proportion of patients achieved the MCID for these outcomes, suggesting that these benefits may be mediated through psychosocial pathways. Warmed irrigation may reduce cold-induced sympathetic activation and psychological tension. 26 This interpretation is consistent with the observations of Ernst et al., 27 who reported that warm saline was perceived as more comfortable and relaxing during laceration irrigation. In contrast, Galdino-Júnior et al. 11 found that 37°C saline did not provide analgesic effects in patients with chronic wounds. This discrepancy likely reflects differences in wound types and patient populations, as acute replantation wounds may be more sensitive to thermal-induced nociceptive and microcirculatory changes. Given that procedural pain can affect rehabilitation adherence, anxiety, and patients’ willingness to undergo repeated wound care, these improvements carry substantial clinical value for enhancing the overall perioperative experience of digit replantation patients. 28
Furthermore, the applicability of these findings may extend beyond digit replantation. Dressing-change-related pain and cold-induced discomfort are common challenges across a range of acute surgical wounds. Procedures involving exposed tissue or temperature-sensitive wounds, such as hand trauma, flap reconstruction, and open fracture management, may also benefit from temperature management during wound care. However, whether these findings are generalizable to other surgical populations requires further studies.
With respect to safety, warmed saline irrigation improved comfort during dressing changes without compromising digit survival or increasing postoperative complications. The CRP analysis also showed no significant intergroup difference. As a systemic inflammatory marker, CRP may not be sensitive enough to detect the localized effects of peri-wound warming.29,30 For clinical implementation, the intervention requires saline to be preheated approximately 30 min before dressing changes and maintained at 33°C–35°C using a medical warming device and an insulated container. This intervention is low-cost, nonpharmacological, and easy to implement. It requires minimal additional time and resources. The approach may be particularly valuable in high-volume dressing-change settings. It can improve patient comfort without disrupting routine clinical workflows. To facilitate clinical implementation, a detailed implementation protocol is provided in Supplementary Table S6.
Subgroup analyses revealed that the benefits of warmed saline irrigation varied by patient characteristics. Compared with older patients, young and middle-aged patients experienced greater pain relief. These differences may be related to age-associated physiological changes, as older patients may derive less analgesic benefit because of reduced temperature sensitivity and impaired pain modulation. 31 In addition, patients treated during colder seasons (autumn and winter) appeared to benefit more from warmed saline irrigation, possibly because cooler ambient temperatures heighten cold-induced discomfort and peripheral vasoconstriction. 32 Notably, patients with concomitant diabetes exhibited a smaller increase in pain after the intervention compared with those without complications. This counterintuitive finding may be attributable to peripheral sensory impairment and microcirculatory dysfunction. 33 Overall, these subgroup differences suggest that the effects of warmed cleansing vary by patient characteristics and may support more individualized application. Clinicians should consider prioritizing warmed irrigation for younger patients in colder environments or seasons and for patients reporting high dressing-change discomfort. However, these subgroup findings remain exploratory and require validation in larger prospective studies.
This study has several limitations. First, blinding was challenging because the intervention involved different irrigation fluid temperatures, and the influence of patient expectations cannot be completely excluded. Second, baseline differences in HADS scores and minor variations in irrigation technique may have affected the results. Third, subgroup analyses were exploratory and should be interpreted with caution. In addition, the 2-week follow-up captured early postoperative outcomes but did not assess long-term functional recovery. Finally, the single-center design may limit the generalizability of the findings. Future multicenter studies with longer follow-up are warranted.
In conclusion, the use of warmed saline irrigation during postoperative dressing changes for digit replantation improves patient-reported pain, anxiety, and comfort without adversely affecting early clinical outcomes. This simple and cost-effective intervention should be considered for routine use in wound care after digit replantation. However, further studies are needed to evaluate long-term outcomes and the underlying mechanisms.
INNOVATION
The effects of warmed saline irrigation during postoperative dressing changes have not previously been evaluated in microsurgical populations such as patients undergoing digit replantation. This randomized controlled trial is among the first to evaluate a simple but underexplored peri-wound thermal intervention using both patient-reported outcomes and real-time physiological indicators. The findings demonstrate that warmed saline irrigation improves patient-reported pain, anxiety, and comfort without compromising vascular outcomes. These findings provide preliminary evidence supporting the incorporation of warmed saline irrigation into postoperative microsurgical wound management protocols.
Supplemental Material
sj-docx-1-wnd-10.1177_21621918261466878 — Supplemental material for Does Warmed Saline Irrigation Improve Comfort During Dressing Changes After Digit Replantation? A Randomized Controlled Trial
Supplemental material, sj-docx-1-wnd-10.1177_21621918261466878 for Does Warmed Saline Irrigation Improve Comfort During Dressing Changes After Digit Replantation? A Randomized Controlled Trial by Fengxia Lai, Feng Huang, Yunyi Sheng, Fanghui Guo, Hui Xia, Ye Dong, Suming Wei, Lan Mo, Leiyin Mao, and Lijun Lu
Footnotes
ACKNOWLEDGMENTS AND FUNDING SOURCES
This work was funded by the Wuxi Association for Science and Technology [Grant Number
AUTHORS’ CONTRIBUTIONS
F.L., F.H., Y.S., and F.G. collected the data; F.H. carried out the randomization; F.L., H.X., and Y.D. analyzed the data; F.L. and L.M. drafted the article; L.L. and L.M. provided edits to the article; L.L., F.L., and L.M. designed the study.
AUTHOR DISCLOSURE AND GHOSTWRITING
The authors declare no financial interests or conflicts of interest to disclose. No ghostwriters were employed.
ABOUT THE AUTHORS
Abbreviations and Acronyms
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.