
Abstract
Background:
The Recovery Friendly Leader (RFL) Training Program (TP) developed an instructor-led, 2-day training: Addressing Substance Use & Demonstrating Inclusion (ASDI), which was piloted virtually under the Zoom platform.
Methods:
The pilot evaluation employed pre- and post-training surveys administered online via Qualtrics to registered participants. Quantitative responses were examined using a right-tailed Welch’s t-test to determine statistically significant improvements in participants’ knowledge and confidence from pre- to post-training. Eleven participants completed the pre-training survey and of those, eight also completed the post-training survey.
Findings:
The training program significantly improved participants’ knowledge and confidence in addressing workplace substance use (p < .05), with high engagement and strong intent to implement recovery-supportive strategies.
Conclusions/Application to Practice:
Analysis revealed the training was effective in increasing participant knowledge and confidence for identifying and addressing employee substance use and supporting recovery. Workplace policies ought to include structured, stigma-reducing leadership training programs to proactively support employee recovery and foster a recovery-supportive organizational environment.
Background
Substance use challenges among employees remain a significant concern for the U.S. workforce. Data from the Substance Abuse and Mental Health Services Administration (2014) indicate that approximately 10% of full-time and 8% of part-time employees meet the criteria for a substance use disorder (SUD). Complementary findings from the Centers for Disease Control and Prevention (2024) and the National Safety Council (NSC) reveal that although 75% of employers report observable impacts of substance use among employees, only 17% consider themselves sufficiently prepared to address employee substance-use challenges and offer support. In 2020, the economic burden associated with employee problematic substance use, including absenteeism, diminished productivity, and elevated healthcare costs, was estimated at $696 billion, reflecting both organizational and societal-level consequences (National Opinion Research Center (NORC) at the University of Chicago, n.d.).
Recognizing the growing impact of substance use on the workforce, the U.S. government articulated a key objective in its 2022 National Drug Control Strategy: to increase by 75% the number of states implementing a “Recovery-ready Workplace Initiative” also known as a “Recovery Friendly Workplace Initiative,” by 2025 (Office of National Drug Control Policy [ONDCP], 2022; Recovery Friendly Workplace Institute, 2024). These initiatives aim to support employers in adopting policies that prevent substance use, promote help-seeking behaviors, provide reasonable accommodations, and foster recovery-supportive workplace cultures (U.S. Department of Labor, n.d.). Empirical evidence suggests that recovery-supportive environments and leadership practices contribute to measurable improvements in employee health, safety, and productivity, as well as organizational cost savings (Narine, 2021). For instance, employees in recovery are absent an average of 13.7 fewer days per year than those not in recovery and 3.6 fewer days than the general workforce. Being in recovery translates to an estimated $8,500 in savings per employee annually due to reduced absenteeism, turnover, and lost productivity (NORC, n.d.).
In response to the growing challenges associated with substance use in the workplace, the Recovery Friendly Leader (RFL) Training Program (TP) was developed to enhance workplace leadership capacities in identifying, addressing, and supporting employees experiencing problematic substance use and facilitating ongoing recovery opportunities, while keeping the workplace safe, healthy, and productive (Narine, 2024; NORC, n.d.; ONDCP, 2022). Drawing on prior research, extensive community input, and the nationwide recovery-friendly workplace movement, the RFL TP was designed to equip leaders with practical strategies and stigma-reduction techniques that enhance recovery-supportive work environments (Narine, 2021, 2022; ONDCP, 2022; U.S. Department of Labor, n.d.).
A well-designed program requires careful planning, rigorous experimental design, and precise execution to achieve high-quality outcomes (Morin, 2023). Conducting a pilot study in the form of an initial, smaller-scale investigation helps assess feasibility and refine the approach before undertaking a full-scale trial (Morin, 2023). The RFL TP developed an initial RFL Educational Workshop: Introduction to Substance Use, Addiction, and Recovery (ISAR)—a 90-minute educational workshop that provides a foundational overview of key concepts related to substance use, addiction, and recovery in the workplace. The ISAR was designed to set the stage for more in-depth training, and a pre-pilot program was conducted in September 2024 to assess effectiveness in increasing leaders’ knowledge of substance use and recovery in the workplace and elicit participant feedback regarding training content format and delivery. The evaluator designed a pre- post-training survey, administered it to all participants, and used the respondents’ feedback to refine both the training content and its delivery.
Building on the ISAR foundation, including lessons learned from piloting, the RFL TP developed the RFL 2-Day Training: Addressing Substance Use & Demonstrating Inclusion (ASDI) to provide workplace leaders with practical strategies to address problematic substance use and foster a culture of inclusion. The ASDI (Figure 1) was delivered over two-half days (totaling 7 hours) and offered in-depth guidance on recognizing early warning signs of substance use, appropriately addressing related performance or behavioral concerns, and adopting leadership practices that are inclusive, non-stigmatizing, and supportive of employee recovery. These practices emphasize psychological safety, equitable support for all employees, and the intentional creation of a workplace culture that encourages help-seeking and sustained recovery.
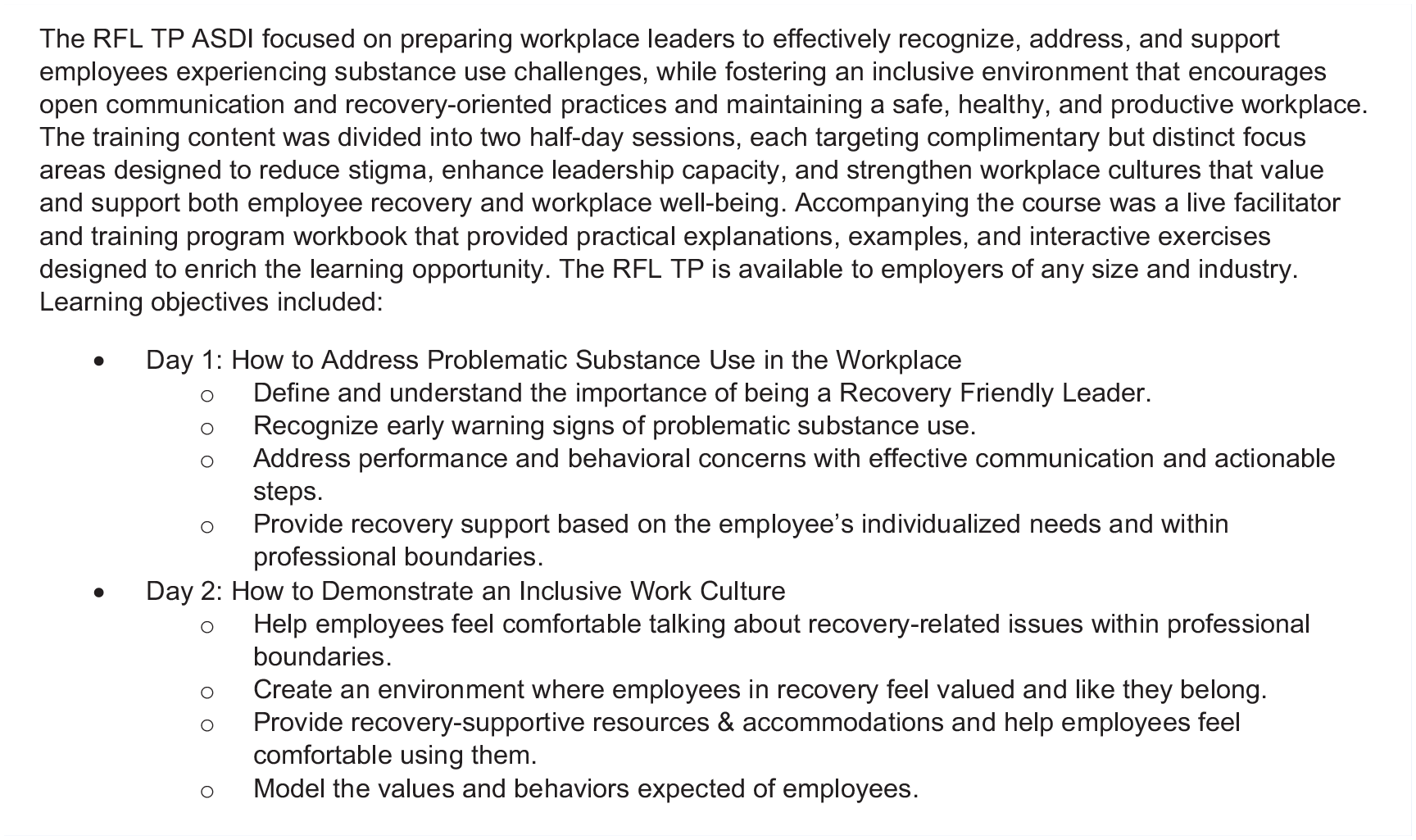
RFL 2-day training: Addressing substance use & demonstrating inclusion training description
The aim of this evaluation was to assess the effectiveness of the ASDI pilot training program in increasing leaders’ self-reported capacity, knowledge, and skills in identifying and addressing problematic substance use, as well as in enhancing environments where employees can access recovery support. The evaluator proposed two hypotheses (H): H1, that the RFL training program is effective in increasing leaders’ knowledge and confidence in identifying and addressing problematic substance use among employees; and H2, the training would enhance the leaders’ ability to foster an environment in the workplace to facilitate recovery opportunities consistently. This evaluation reports the results of the ASDI pilot training.
Methods
This pilot evaluation employed a mixed-methods, pre-post intervention design to evaluate the effectiveness of the ASDI pilot training in enhancing leaders’ capacity (knowledge and confidence) to identify and respond to substance use impacts in the workplace and foster recovery-supportive environments.
Study Population, Recruitment, and Sampling
Participants were recruited utilizing a convenience/voluntary sampling method. Initial outreach targeted attendees of the prior ISAR training and community members who had expressed interest in workplace recovery support training. Recruitment was conducted via email invitations that described the training objectives, outlined required materials (e.g., training workbook), and specified technology requirements (e.g., internet and Zoom access). A Doodle Poll link was provided to coordinate scheduling and confirm availability for both sessions. Subsequently, a calendar invitation for the Zoom sessions was remitted and accepted by each participant, and the training workbook (to be utilized during training) was mailed and confirmed received by each participant.
Instrument
All survey instruments were developed by the author in consultation with evaluation experts at the Centers for Health, Work, and Environment, Colorado School of Public Health, ensuring each survey item reflected the learning objectives of the training (Figure 1). The pre-training survey included demographic items (age range, gender, race/ethnicity, organizational role) and 11 self-report items measuring baseline capabilities, knowledge, and skills for addressing employee substance use and supporting recovery (Table 2). Each item employed a 5-point Likert scale, and a final open-ended question asked participants to describe their expectations for the training. To evaluate change and impact, the post-training survey re-administered the same 11 core items from the pre-training survey. Additionally, participants were asked to report their intended application of learned knowledge and skills (Table 3) and to provide feedback about the training experience, including plans for supporting employee recovery.
Intervention
The ASDI online curriculum described earlier (Figure 1) was delivered via Zoom and totaled 7 hours, divided into two sessions of 3.5 hours each. In the first session, participants received instructions for addressing problematic substance use in the workplace. The content included strategies to identify warning signs of problematic substance use, initiate constructive conversations about performance or behavioral concerns, and tailor supportive interventions to individual employee circumstances. The second session comprised a lecture on cultivating an inclusive work culture. The content incorporated methods for establishing and maintaining supportive relationships with employees in recovery, reducing stigma, providing equitable resources and accommodations, and demonstrating inclusive leadership behaviors. Both sessions were reinforced through interactive learning activities such as discussion questions, role-playing scenarios, and break-out group exercises that enabled participants to practice applying concepts and communication strategies. Instructional materials included PowerPoint slides and a training workbook mailed to participants in advance.
Data Collection
All study activities were conducted remotely in February 2025. Electronic informed consent was obtained via Qualtrics, and all study participation was voluntary. Data were collected through two online surveys pre- and post-training, administered via Qualtrics. To maintain confidentiality and allow linkage of pre- and post-training survey responses without collecting personally identifying information, participants generated a unique code. Participants who had not completed the pre-training survey were prompted to answer demographic items in the post-training survey.
Data Analysis
Qualitative data from open-ended survey responses were exported to Microsoft Excel, where the authors independently conducted an inductive thematic analysis. Pre-training survey responses, wherein participants were asked to provide their training expectations (e.g., “I hope to learn more effective . . . ways to interact with any employees who may be returning to use and how to address this with compassion and clarity”), were coded into themes that aligned with the ASDI’s learning objectives (e.g., “Address performance and behavioral concerns with effective communication and actionable steps”). Post-training survey responses where participants provided feedback on their training experience (e.g., “I had some confusion . . . this really helped clear those questions”) were categorized into emergent themes.
Quantitative data were analyzed using Statistics Kingdom, a web-based statistical platform, and summarized in Microsoft Excel. Descriptive statistics were calculated for demographic variables and Likert-type item scores: frequencies and percentages for categorical variables and means and standard deviations for continuous variables. To evaluate changes (increases) between the 11 core items in the pre- and post-survey measurements and given unequal sample sizes (pre-training N = 11; post-training N = 8), a right-tailed Welch’s t-test was conducted (West, 2021). The nine application-focused items in the post-training survey were described using frequencies and percentages only. All results were synthesized and presented in tables that display pre- and post-training means, standard deviations, and p-values to facilitate comprehensive evaluation and interpretation.
Results
A total of 11 individuals registered and attended the ASDI training, with 9 participants on Day 1 and 9 on Day 2. Notably, two participants who attended Day 1 did not attend Day 2, while two different participants attended Day 2 only. Eleven individuals completed the pre-training survey, and eight completed the post-training survey.
Based on self-reported demographics, the sample (N = 11) consisted of two Front-line Supervisors/Team Leads, two Mid-level Managers, five Senior-level or Directors, and two Executive-level/C-suite. Respondents represented Orange County, FL, and Adams, Boulder, Denver, Garfield, and Jefferson counties in Colorado. Participants spanned several industries, including public sector/administration (n = 7; e.g., government, non-profit, conservation, advocacy), construction (n = 1), educational services (n = 1), healthcare and social assistance (n = 1), and professional, scientific, and technical services (n = 1).
Among the participants, six worked in organizations that had signed The Colorado Recovery Friendly Workplace Initiative™ Pledge/Letter of Intent—a written commitment made by Colorado employers to create a workplace that supports employees experiencing substance use challenges, educate employees about the dangers of substance misuse, and reduce stigma related to SUD (Colorado Recovery Friendly Workplace Initiative, 2024). Four participants expressed interest in learning more about the initiative, and one was unsure of the organization’s involvement.
Regarding lived experience, five participants identified as being in personal recovery from substance use, while six did not. Seven participants reported supporting someone with lived experience. Additionally, nine participants indicated awareness of employees in recovery or with a history of substance use challenges in their organizations, whereas two participants were not aware. Among those who reported awareness, the average organization size was 921 employees, with an average of 94 known to be in recovery (10.2%).
In the pre-training survey, participants were asked about their prior education and training in substance use, addiction, and recovery. Seven participants had attended the ISAR pre-pilot training. Participants who reported additional training or education listed: Certified Recovery Peer Specialist “CRPS” (Florida Certification Board “FCB”), Certified Professional Recovery Coach Program “CPRC” (International Association of Professional Recovery Coaches “IAPRC”), Certified Facilitator Addiction Awareness for Human Resources “CFAA-HR” (Developer and Trainer), Work and Health Links, as well as personal family experience and peer support specialist training.
Participants were asked to describe what they hoped to gain from the training related to supporting employee recovery. As shown in Table 1, their responses aligned with at least one of the training’s learning objectives, confirming strong congruence between participants’ needs and the RFL curriculum. Themes included: (1) role modeling and recovery-friendly workplace advocacy, (2) foundation knowledge and tools, (3) effective intervention and support strategies, and (4) resource provision and encouragement. The themes underscore both Day 1’s focus on problematic substance use identification and intervention and Day 2’s emphasis on culture, providing resources, and role modeling (prevention strategies).
Training Expectations – Qualitative Results
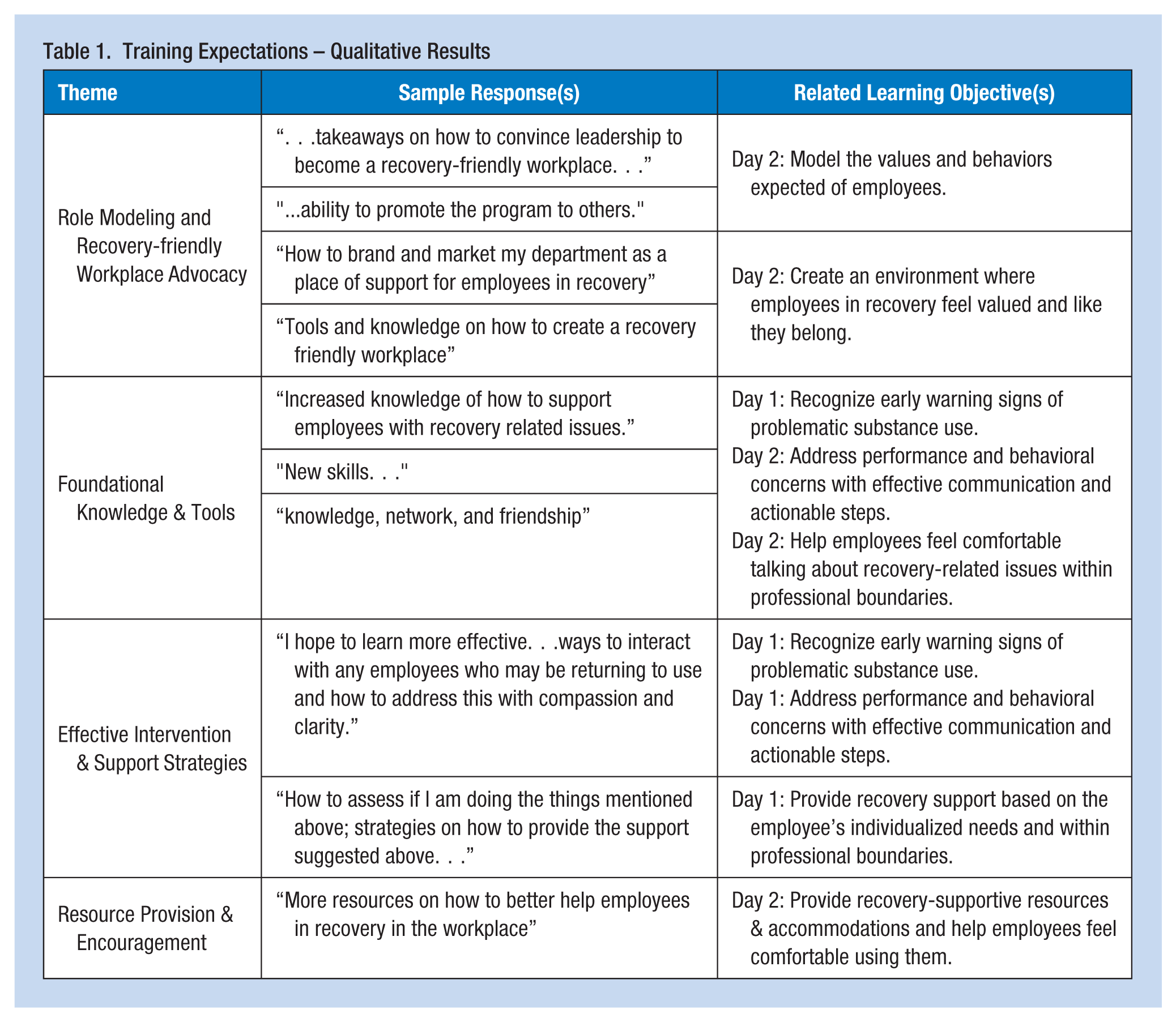
Table 2 illustrates participants’ pre- and post-training levels of agreement on items assessing capability, knowledge, and skills, including the percent changes observed between the two time points. All three items related to participants’ capability demonstrated percentage increases from pre- to post-training; however, none of these changes achieved statistical significance (p < .05). In contrast, seven of the eight items related to knowledge and skills exhibited statistically significant improvements (p < .05).
Capability, Knowledge, and Skills Assessment—Participant Group Responses
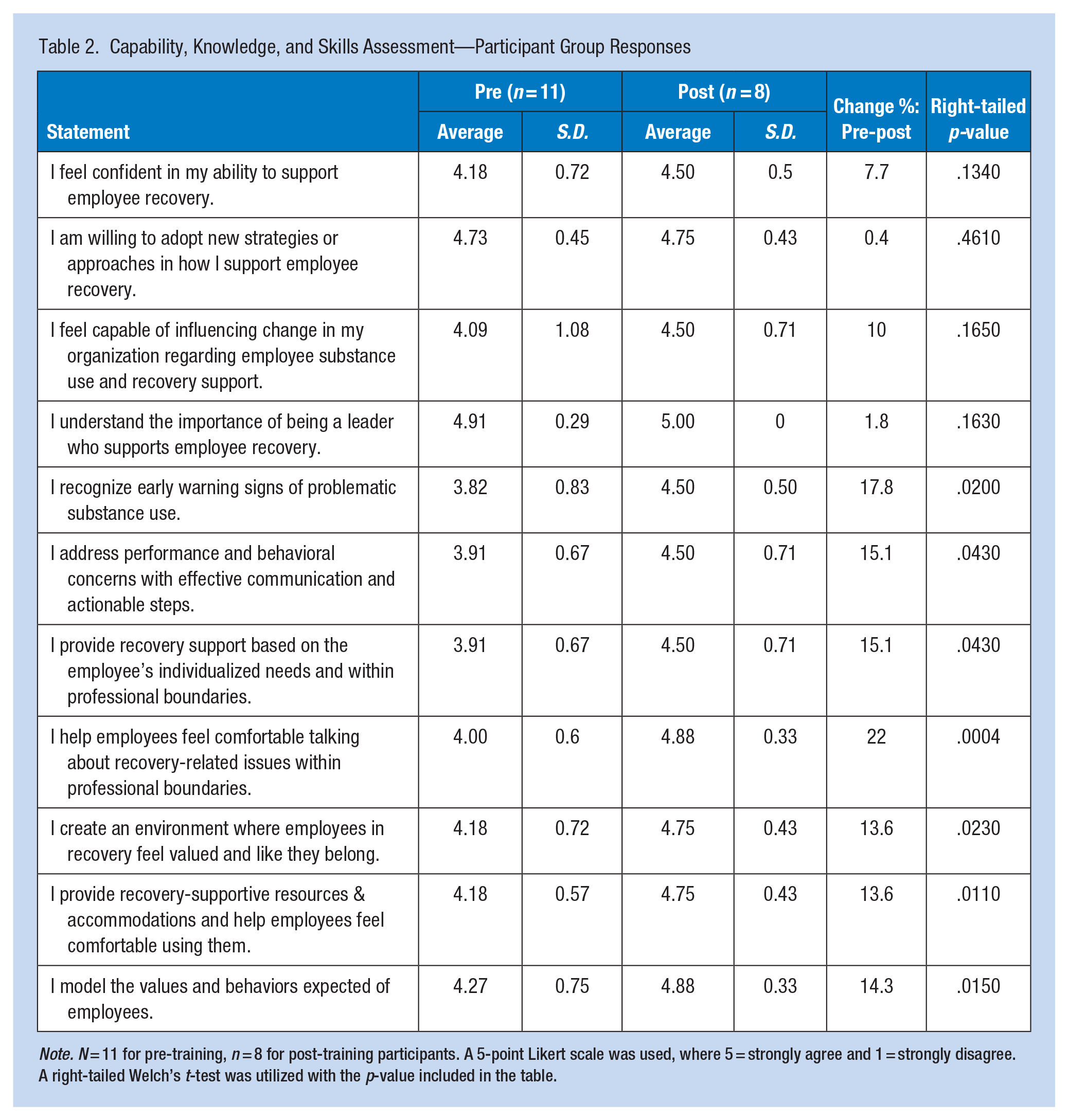
Note. SD = standard deviation; N = 11 for pre-training, n = 8 for post-training participants. A 5-point Likert scale was used, where 5 = strongly agree and 1 = strongly disagree. A right-tailed Welch’s t-test was utilized with the p-value included in the table.
Participants were asked to indicate the actions they planned to undertake to support employee recovery following the training. All participants (n = 11) reported intentions to perform eight out of the nine (88%) listed activities: for example, actively reducing stigma and bias surrounding recovery, connecting employees with relevant supportive resources, advocating for policy changes, and scheduling a follow-up coaching session. Table 3 provides a comprehensive list of all activities presented to the participants and their self-reported planned actions. Additionally, participants provided feedback on training effectiveness using a 5-point Likert-type scale (5 = strong agreement; 1 = strong disagreement) in terms of content delivery (5.0), clear training materials (5.0), knowledge gap addressed (4.75), and training recommended to others (5.0).
Post-Training Actions Planned—Participant Group Responses
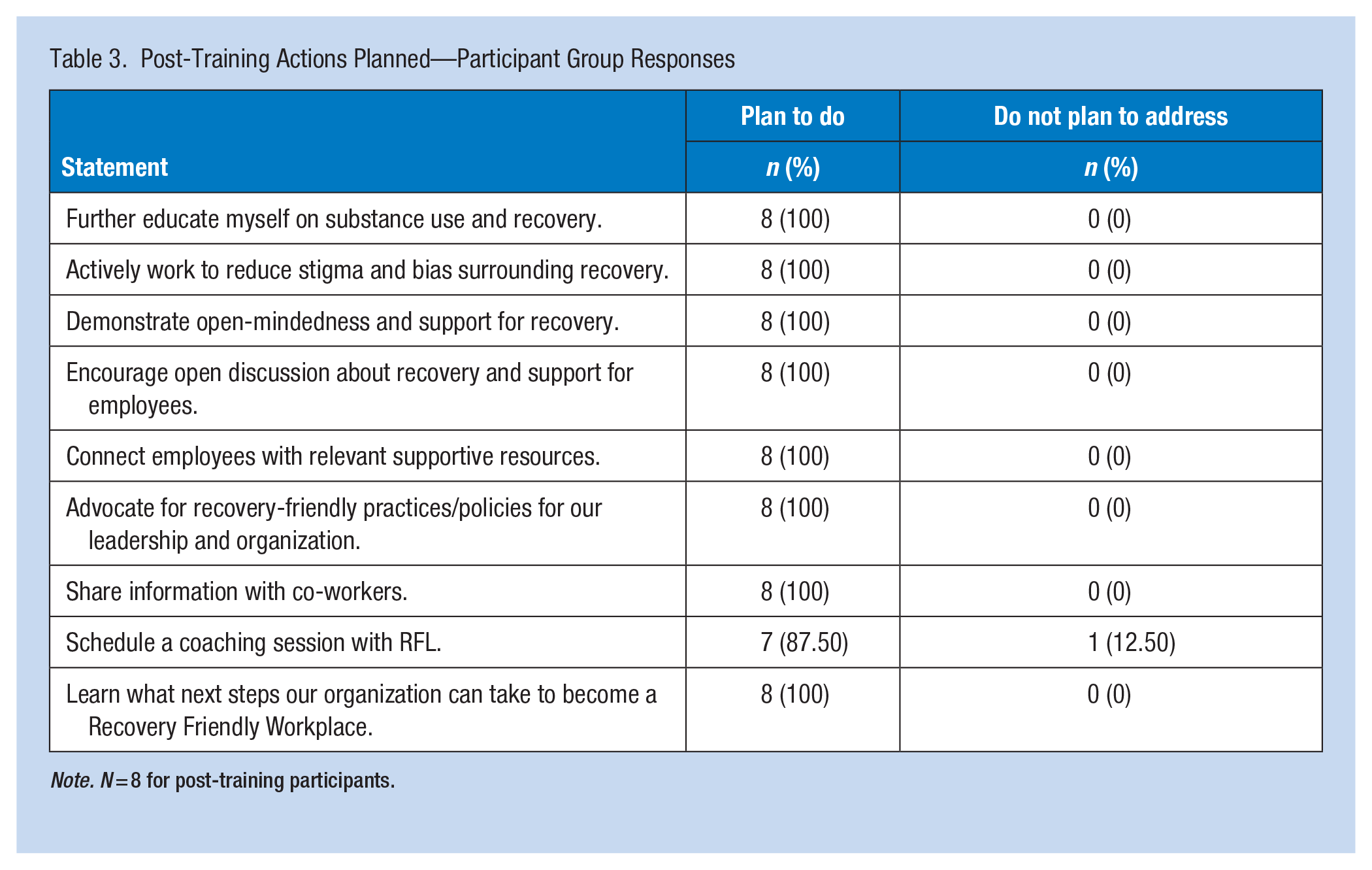
Note. N = 8 for post-training participants.
Discussion
The findings from this pilot program evaluation support the two hypotheses (H) proposed: H1, that the RFL training program is effective in increasing leaders’ knowledge and confidence in identifying and addressing problematic substance use among employees; and H2, the training would enhance the leaders’ ability to foster an environment in the workplace to facilitate recovery opportunities consistently. Statistically significant increases in seven out of the eight knowledge- and skill-focused measures indicated that participants acquired practical competencies for vital recovery-supportive skills such as recognizing early warning signs of substance use, engaging in effective communication to address performance or behavioral concerns, and providing individualized employee support within professional boundaries.
These outcomes have important implications for practice. By demonstrating rapid improvements in critical skill areas, this pilot evaluation suggests that incorporating the RFL TP in leadership training can enable workplace leaders to better identify employees experiencing substance-use challenges and create environments in which employees have better opportunities to access support. Leaders who consistently apply these skills may lay the groundwork for improved workplace cultures, reduced absenteeism, fewer safety and health incidents related to substance use, and high levels of employee engagement, productivity, and retention (Narine, 2022; NORC, n.d.; U.S. Department of Labor, n.d.).
Participant feedback also highlighted the training’s effectiveness in providing actionable strategies for supporting employee recovery. Nearly all participants reported intentions to actively implement strategies post-training, such as resource connection, policy advocacy, and reducing stigma, a practice known to increase levels of help-seeking from those with mental health needs (Song et al., 2023). Furthermore, seven of the eight participants planned to schedule follow-up coaching, suggesting that the RFL TP was well-received and likely to foster momentum for future organizational change.
Limitations
Several limitations must be considered when interpreting these findings. Of utmost importance is the small sample size, which limits generalizability. While the organizational and geographical demographics of the sample remained diverse, a larger sample size would increase generalizability as effects may differ in other industries, organizational sizes, or regions.
All capability-related items showed increased directional change; however, these improvements did not reach statistical significance, potentially due to high baseline agreement on leadership self-efficacy. This ceiling limits the capacity to detect meaningful change in those domains. Nevertheless, initial high agreement levels regarding confidence in abilities, willingness to adopt new approaches, and perceived capability to influence organizational change for recovery reflect positively on participant readiness. RFL TP can therefore reinforce and incrementally build upon pre-existing strengths.
Unmatched pre- and post-survey responses prevented the utilization of a paired-sample t-test that could have improved statistical power and the ability to detect significant changes by accounting for within-subject variability (Field, 2024). Future evaluations may strive to match and link responses while maintaining confidentiality. Finally, reliance on self-reported measures restricts confirmation that knowledge gains translate into sustained behavioral change. Therefore, subsequent studies ought to integrate objective metrics (e.g., observed manager-employee interactions and employee productivity rates) to validate behavioral outcomes.
To build on these preliminary results, future evaluations should consider a longitudinal assessment to gauge sustained knowledge application and long-term impact on organizational practices, policy, and employee well-being outcomes. This would clarify whether knowledge and skill gains persist and influence workplace practices over time. As such, the evaluator has developed a 3-month post-training survey for the RFL TP, which is designed to investigate leadership actions implemented and observable changes in organizational practices, culture, safety, employee wellbeing, and behavior since training. Moreover, future studies ought to consider including a control group to strengthen the inference on whether observed changes are directly attributed to the RFL TP or from other external influences.
Despite these limitations, this pilot evaluation provides encouraging evidence that RFL TP can quickly enhance managers’ knowledge and confidence for supporting employee recovery and fostering the ability to advance recovery-friendly environments. While actual behavior and culture change remain to be demonstrated, these initial gains in capacity represent a critical first step toward embedding recovery-supportive practices across workplaces in any industry.
Implications for Occupational Health Practice
Findings from this evaluation suggest that structured, recovery-supportive leadership training can enhance organizational capacity to address substance use in the workplace. Since employees spend much of their time within the organizational setting, recovery support must extend beyond external services and be embedded in organizational policy and day-to-day leadership practices. To create an environment that supports employee recovery, organizations should adopt policies that define confidentiality expectations, legal protections, reasonable accommodations, access to recovery resources, and safety protocols for employees who disclose substance use concerns. These policies establish a critical foundation for support.
Policy adoption alone is not sufficient, as effective intervention implementations depend on leaders who understand the nature of SUD, recovery, and are equipped to cultivate stigma-free, inclusive workplace cultures (Kelloway, 2017; Narine, 2021). Specialized training for these “recovery-friendly leaders” ensures they can recognize early signs of substance use challenges, connect employees with appropriate services, implement accommodations, and reinforce a culture of safety and support.
Organizations can strengthen these efforts by participating in a state or national Recovery Friendly Workplace Initiative and partnering with specialized providers, such as the RFL TP, to support leadership development and ongoing coaching. Such structured and sustained interventions are essential for fostering a supportive workplace environment conducive to both sustainable employee recovery and beneficial organizational outcomes.
Applying Research to Occupational Health Practice
The virtual RFL TP ASDI pilot program equips organizational leaders with practical knowledge and actionable strategies to effectively support employee recovery while maintaining a safe, healthy, and productive organization. Pre- and post-training survey analyses revealed statistically significant gains in participants’ self-reported knowledge and confidence for strategies such as recognizing warning signs, initiating supportive conversations, and implementing accommodations for employees facing substance use challenges. These findings highlight the value of structured leadership development within occupational health practice. By pairing recovery-supportive policies, such as confidentiality guidelines, employee legal protections, and resource access, with specialized training for workplace leaders, organizations can proactively reduce stigma, enhance early intervention, and foster inclusive cultures that encourage prevention and long-term recovery. This model can be adopted across industries through partnerships with a recognized Recovery Friendly Workplace Initiative or training providers, such as the RFL TP, embedding sustainable, research-based interventions into existing health and safety programs to improve both employee well-being and organizational outcomes.
Footnotes
Acknowledgements
The authors thank Nick Williams, Cheryl Brown Merriwether, Tim Wackenreuter, Marcie Phillis, Stephen Rotter, David Shapiro, Dr. Carol Brown, Dr. Robert C. Voigt, and Dr. Eric Persaud for their review and thoughtful feedback throughout the study.
Author Contributions
All author(s) substantially contributed to the conception of the study, interpretation of the data, and construction of the manuscript.
Conflict of Interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Narine is the founder and executive director of Recovery Friendly Leader, a 501(c)(3) organization that administers the RFL TP outlined in this study. To mitigate this potential conflict of interest, the author recruited one independent co-author and one independent peer reviewer who had no prior personal or professional relationship with the author, their body of work, or the RFL TP to perform an objective evaluation of the data, interpretation of the findings, and manuscript.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.