
Abstract
Background:
Despite recognition of the integral relationship between healthcare worker (HCW) safety and patient safety, few studies have evaluated practices that improve safety for both groups. We undertook a scoping meta-review including only systematic reviews (SRs) to determine the extent to which existing literature identifies practices likely to benefit both HCW safety/well-being and patient safety and remaining research questions.
Methods:
Literature searches were conducted for SRs and meta-analyses from 2011 to 2020 that reported outcome measures related to improving HCW safety/well-being or organizational safety culture as well as patient safety. After multi-stage screening, studies were classified as relationship/association or focused on a specific practice. Among practice-focused, those that found positive outcomes for both HCW/organizations and patients were considered potentially promising practices. Information was extracted on topic area, interventions, care settings, HCW type, outcomes measured and improvements.
Findings:
Of 1,619 abstracts, 114 reviews met all inclusion criteria. Major topic groups were Worker Safety/Well-being (n = 33), Operational Practices (n = 34), Organization Safety Culture (n = 24), and Patient Safety/Quality (n = 23). Of 78 reviews addressing specific practices, 48 described practices likely to benefit both groups. Practices/interventions targeting how work is organized were most promising (subtopics staffing/human resources; structure, policies/procedures; human factors engineering). Practices addressing teamwork and engagement suggest opportunities to enhance safety climate.
Conclusions/Application to Practice:
A wide range of practices and topic areas may directly and/or indirectly improve safety for both HCWs/organizations and patients, suggesting an integrated approach to examining interventions and operational practices. Occupational health/safety and patient safety leaders should consider collaborating to implement promising practices.
Background
The US Surgeon General stated “the nation’s health depends on the well-being of our health workforce” (U.S. Department of Health and Human Services, 2022). The long-standing view of healthcare worker self-sacrifice for the patient’s benefit was challenged in part by the COVID-19 pandemic experience and factors contributing to the “great resignation” (Abbasi, 2022; Nigam et al., 2023; Shen et al., 2024).
Growing awareness of the inter-relationships between patient and worker safety has motivated many efforts to improve healthcare worker (HCW) well-being (Agency for Healthcare Research and Quality [AHRQ], 2024b; Grime, 2021; Hodkinson et al., 2022; National Academy of Medicine, 2022; National Steering Committee for Patient Safety, 2020; The Joint Commission, 2012). These efforts recommend a systems approach to improving safety (National Steering Committee for Patient Safety, 2022). Historically, safety efforts have been siloed to address either HCWs (Anger et al., 2024; Panagioti et al., 2017; Sinsky et al., 2020; West et al., 2016) or patients (K. K. Hall et al., 2020; Zegers et al., 2016). Few studies examine practices that improve safety for both HCWs and patients; examples include workplace violence (Lipscomb & El Ghaziri, 2013) and safety culture (Morello et al., 2013; Occupational Safety and Health Administration, n.d.; Weaver et al., 2013).
We undertook a scoping meta-review (ScMR) to identify promising, evidence-based practices that improve safety for both HCWs and patients. A ScMR is a novel variation of a scoping review used for high-level mapping of a new field based on evidence solely from systematic reviews (SRs; Sarrami-Foroushani et al., 2015). We defined safety as “freedom from exposure to danger and protection from the occurrence or risk of injury or loss” (National Library of Medicine, 1991). The term “healthcare worker” included paid employees, volunteers, licensed practitioners and contractors, and “patient” included setting-preferred terms such as clients, nursing home residents, and customers. The primary research aim was to determine the extent to which the literature identifies practices that improve safety for both HCWs and patients. The secondary aim was to identify research gaps and remaining questions to be addressed. We did not intend to evaluate the effectiveness of specific practices (as done in SRs) but rather to assess the range and breadth of topics that affect safety for both groups and the types of outcomes used for evaluation.
Conceptual Framework
The most widely used work systems model in healthcare is Systems Engineering Initiative for Patient Safety (SEIPS). This human factors engineering-based model describes four interactive components: people; tasks, tools, and technologies; the physical environment; and organizational conditions (Carayon et al., 2020; Xie & Carayon, 2015). These components have also been applied to examining worker safety (Carayon et al., 2015; Zink et al., 2024). Organizational conditions, such as safety culture and leadership, greatly influence both well-being for workers and patient safety. Leaders and managers often determine operational policies, practices, and also unit-level safety culture (Sfantou et al., 2017; Shanafelt et al., 2015; Swensen et al., 2013).
We used a conceptual framework that integrates safety concerns for both groups: (a) the HCW and/or their organization and (b) patients (Figure 1). We focused on one SEIPS model component—practices/interventions implemented by the healthcare organization to improve safety. In the integrated model, organizations can take different paths to improve safety depending on their short- and long-term goals. Efforts targeted to one group may also affect the other, since organizational safety culture and operational practices can have bi-directional effects. For example, organizational efforts to improve safety culture, infection prevention, and workplace violence prevention may directly or indirectly affect both HCWs and patients.
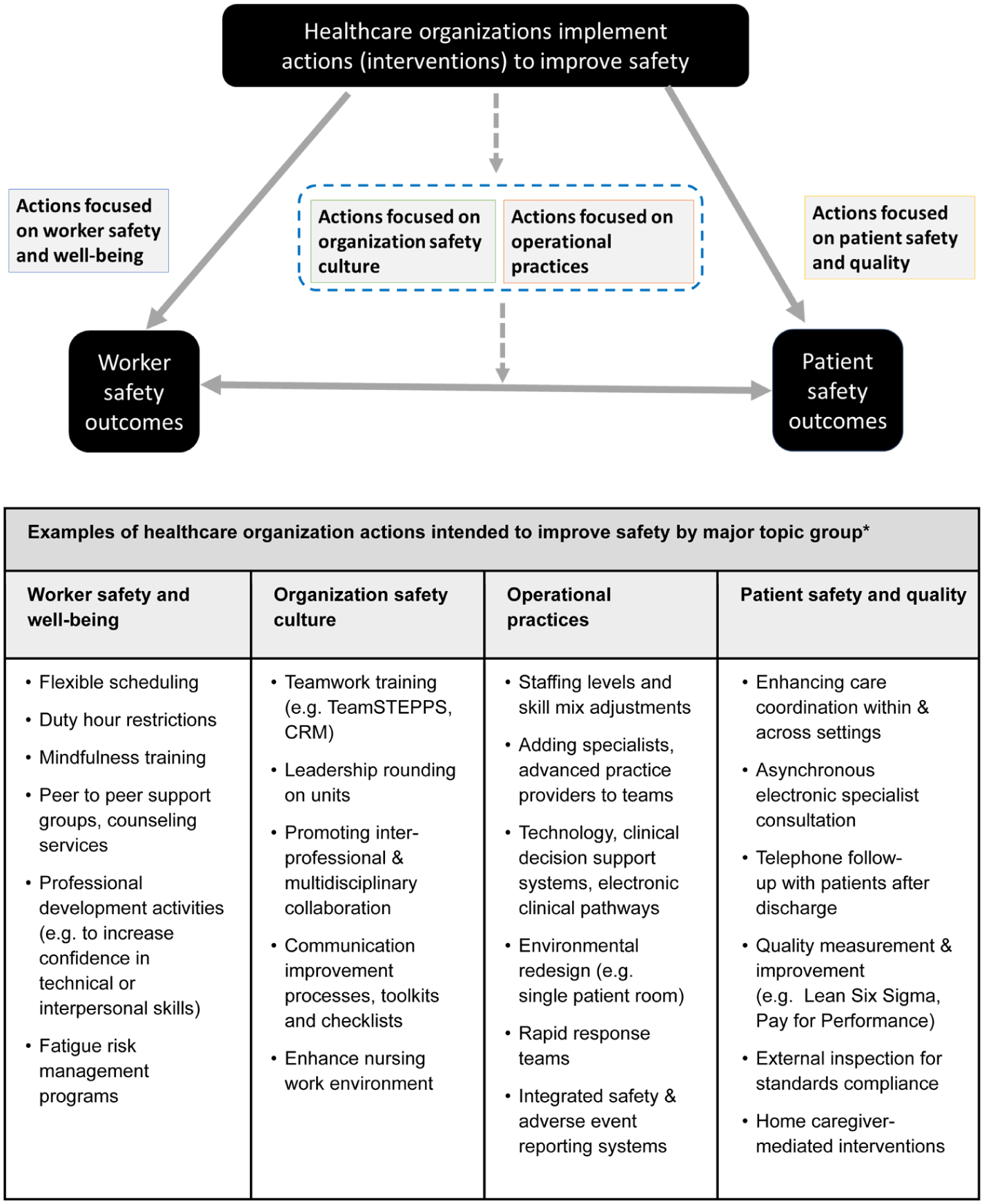
Actions to improve healthcare safety can be targeted toward workers, organizations, and/or patients
Methods
Scoping reviews examine the extent, range, and nature of existing research activity in a broad topic area, contextualize the current state of understanding, and recommend next steps for types of research needed (Morris et al., 2016; Peters et al., 2024). We followed methodology recommended by scoping meta-review developers, limiting article types searched to SRs and meta-analyses (Sarrami-Foroushani et al., 2015) as well as the Joanna Briggs Institute (JBI) guidance for conducting scoping reviews and the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR; Pollock et al., 2023; Tricco et al., 2018). This activity was reviewed by CDC, deemed research not involving human subjects, and conducted consistent with applicable federal law and CDC policy. No a priori review protocol was specified and evaluation of SRs quality was not done.
Data Sources and Searches
A medical librarian searched PubMed (MEDLINE), APA PsycINFO, CINAHL, and Cochrane Database of Systematic Reviews for SRs and meta-analyses published between 2011 and 2020 using keywords and MeSH terms related to HCWs, patients, safety/well-being, and organizational safety culture. See Supplemental Table 1 for detailed search terms and supplemental searches with additional keywords generated through relevant results. We operationally defined HCW well-being to include topics related to staff burnout, wellness, fatigue, psychological distress, second victim phenomenon, resilience, job satisfaction, disclosure perceptions, and medical resident duty hour limitations.
The article inclusion criteria were: (1) a systematic review or meta-analysis, (2) addresses actions or associations related to improving HCW safety, well-being or organization culture and patient safety, (3) reports outcome measures for both HCW/organizations and patients, and (4) primary focus is on both HCW/organizational safety and patient safety. Measures of culture were considered organizational outcomes because they aggregated worker responses for relevant domains. SRs evaluating HCW educational and training efforts were included if the outcomes addressed work environment satisfaction, stress, burnout, turnover intent, attitudes, perceptions, confidence, self-efficacy, etc. All project team members contributed to developing the inclusion/exclusion criteria and screening processes.
We excluded SRs that (1) only reported process of care measures (e.g., guideline adherence, medication errors) without outcomes, (2) measured outcomes for only one group, (3) narrative reviews due to selection bias potential (Uman, 2011), and (4) only included studies which originated from countries with very dissimilar income levels or healthcare systems from those found in western nations.
Data Selection and Extraction
The team used DistillerSR® to perform four-level screening of abstracts and articles (Evidence Partners, 2022). DistillerSR® distributed each abstract to two of four team members who independently screened each title and abstract (Level 1). Conflicts were resolved at Level 2 by a third team member. At Level 3, each full-text SR was evaluated against the inclusion criteria independently by two reviewers and discrepancies were resolved by consensus at weekly meetings.
Patient safety categories were partially based on the AHRQ’s topic taxonomy (AHRQ, 2024a). When multiple inter-related topics were identified, we applied simple hierarchical rules to improve consistency. Three members (MB, EU, BB) focused on data mapping at Level 4, for which we assessed abstractor consistency by having 12 articles mapped by at least two abstractors. (A detailed guidance document for abstracting 26 data elements is available from the authors).
The project was funded in part by the CDC National Institute for Occupational Safety and Health (NIOSH) Contract # 75D30120P08556. The NIOSH co-authors were engaged in study design, conduct and in contributing to this report but not in data collection and analysis.
Data Synthesis and Analysis
We classified SRs into two groups: (1) “Relationship-focused” studies that examined an association or correlation between two factors (e.g., associations between clinician burnout and patient adverse events) or (2) “Practice-focused” studies which examined the effectiveness of a specific intervention or practice (e.g., teamwork training). For SRs evaluating specific practices, we examined authors’ findings and conclusions for evidence of improvements in safety for HCWs and patients. When the authors reported positive impact for both, we classified the SR as having practices likely to benefit both groups referred to as “promising practices.”
We assigned one of 14 primary subtopics to the problem addressed, then grouped subtopics into four major topic areas: (1) Worker Safety and Well-being, (2) Organization Safety Culture, (3) Operational Practices, and (4) Patient Safety and Quality.
We identified research gaps by considering topics for which there were few included SRs, SRs with outcomes for only one group, and those without positive impact due to lack of interventions or major methodological weaknesses. We calculated aggregate frequencies for categorical variables and means (SD) for continuous variables using Microsoft Excel.
Results
We screened 1,619 abstracts, of which 428 moved directly to full-text review (Level 3). Additionally, 214 moved to full-text review after conflict resolution. As shown in Figure 2, of 642 articles receiving full-text review, 528 were excluded, leaving 114 SRs that met all inclusion criteria. (A table listing excluded studies lacking both outcome measures is available upon request).
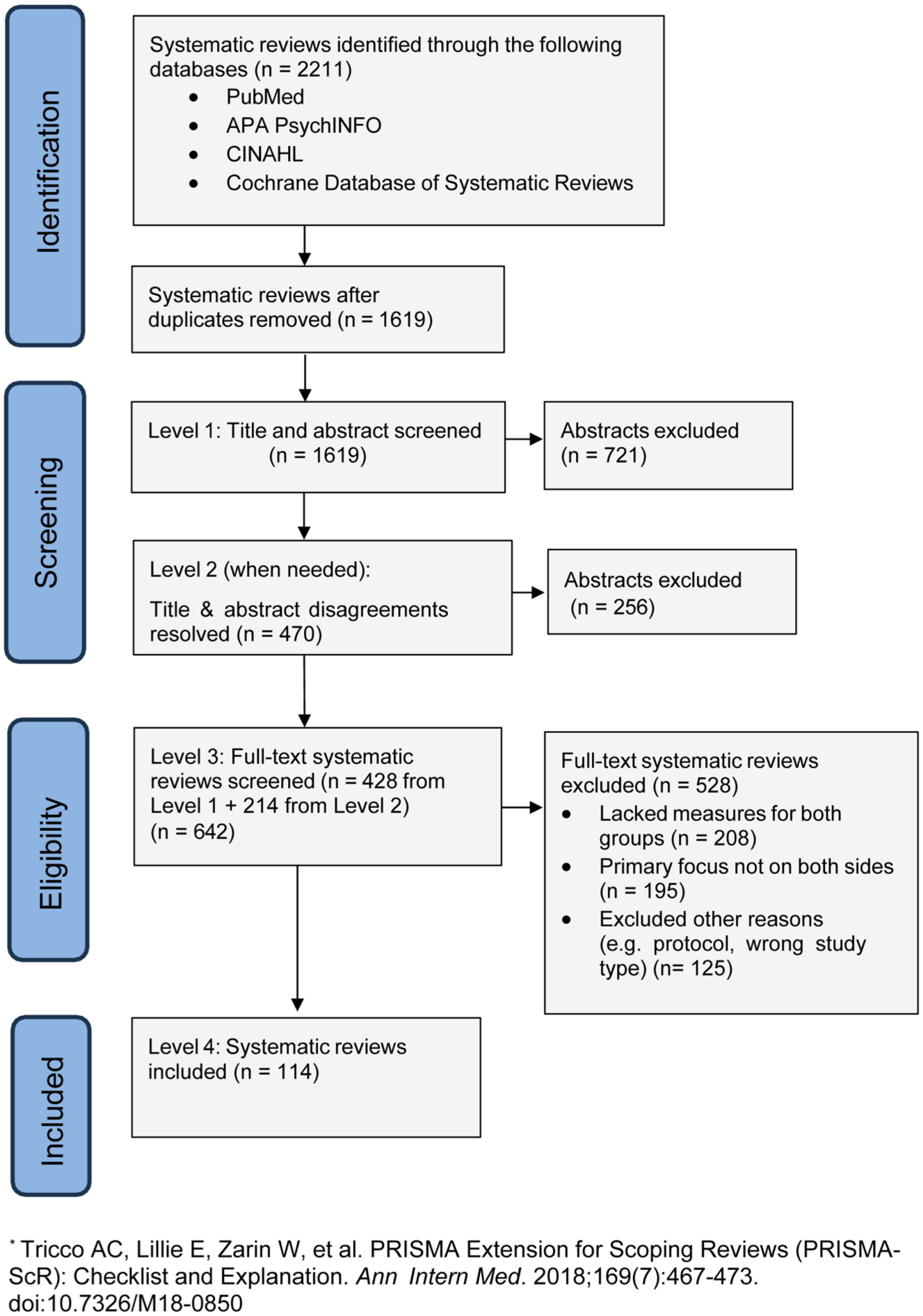
PRISMA-ScR flow diagram
Aggregated Findings Across Included Reviews
Overall, 36 (31.6%) focused on relationships between variables while most (n = 78, 68.4%) focused on a specific practice. Table 1 lists relationship-focused reviews and brief findings. Table 2 lists all practice-focused reviews. Among the SRs that examined specific practices, 48 (61.5%) were considered to have promising practices likely to benefit both HCWs/organizations and patients.
Systematic Reviews Focused on Relationships and Associations
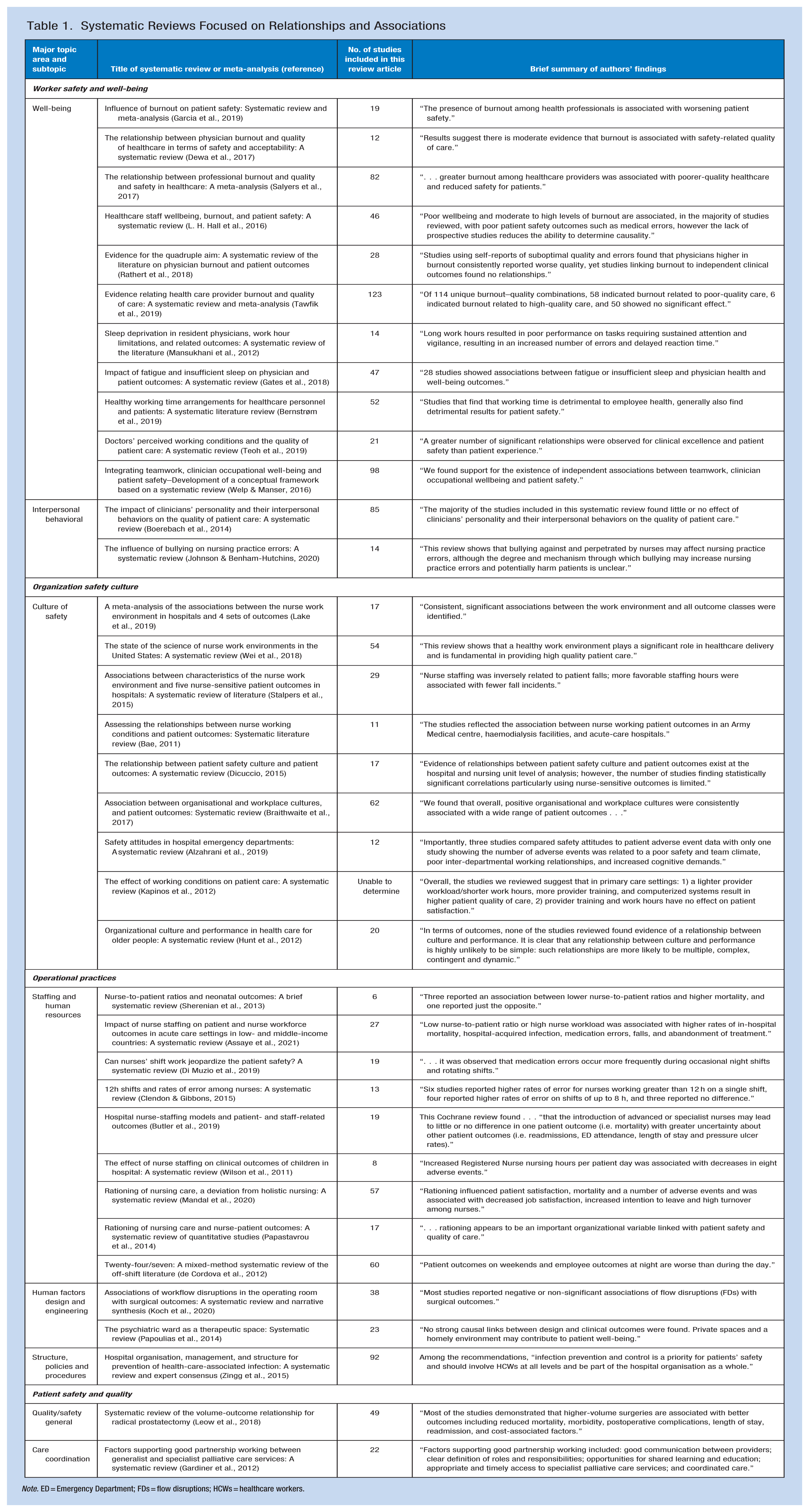
Note. ED = Emergency Department; FDs = flow disruptions; HCWs = healthcare workers.
Systematic Reviews Focused on a Specific Practice
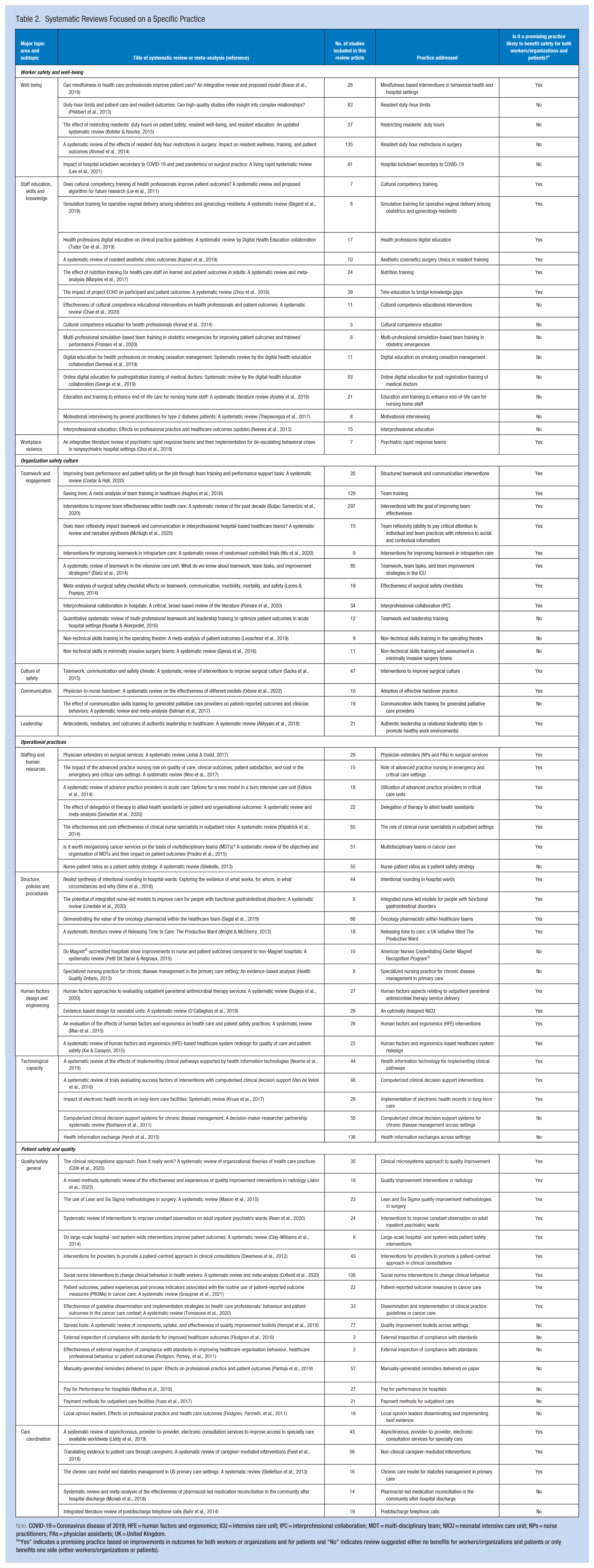
Note. COVID-19 = Coronavirus disease of 2019; HFE = human factors and ergonomics; ICU = intensive care unit; IPC = interprofessional collaboration; MDT = multi-disciplinary team; NICU = neonatal intensive care unit; NPs = nurse practitioners; PAs = physician assistants; UK = United Kingdom.
“Yes” indicates a promising practice based on improvements in outcomes for both workers or organizations and for patients and “No” indicates review suggested either no benefits for workers/organizations and patients or only benefits one side (either workers/organizations or patients).
Most included reviews were SRs (n = 89, 78.1%), however, six (5.3%) were meta-analyses, and 19 (16.7%) were classified as both (National Library of Medicine, 2025). The total number of articles across included SRs was 4,171, with mean studies per review of 36.9 (SD = 38.9, range 2–297).
The SRs were published in 76 different journals across several disciplines: medicine (n = 25); evidence synthesis (n = 18); nursing (n = 16); quality/patient safety (n = 13); interdisciplinary studies (n = 10); healthcare administration/policy/research (n = 10); surgery (n = 8); informatics (n = 4); pharmacy (n = 3); occupational/environmental health (n = 2); and other (n = 5). Most reviews (n = 79, 69.3%) were written by author teams affiliated only with organizations outside the U.S. Most SRs (n = 97, 85.1%) evaluated the quality of their included studies using an objective tool such as GRADE (Guyatt et al., 2011) or JBI critical appraisal tool (JBI, n.d.).
Supplemental Table 2 summarizes the outcome measures reported, settings included, and types of HCW involved. Most reviews described multiple types of outcomes and HCWs, often physicians (n = 81, 71.1%), and nurses (n = 75, 65.8%). Common settings were hospitals (n = 101, 88.6%) and ambulatory care (n = 48, 42.1%).
Findings for the Four Major Topic Areas
Within major topic areas, the number of included studies was Worker Safety and Well-being (n = 33), Organization Safety Culture (n = 24), Operational Practices (n = 34), and Patient Safety and Quality (n = 23) (Figure 3). Examples of subtopics comprising the four major topic areas are listed at the bottom of Figure 1. Because of the variation in practices and outcomes, in the sections below we summarize studies that found associations within subtopics, first for relationship-focused studies then for practice-focused studies. Detailed information about practices, measures, and findings for each study is provided in Supplemental Tables 3 to 6.
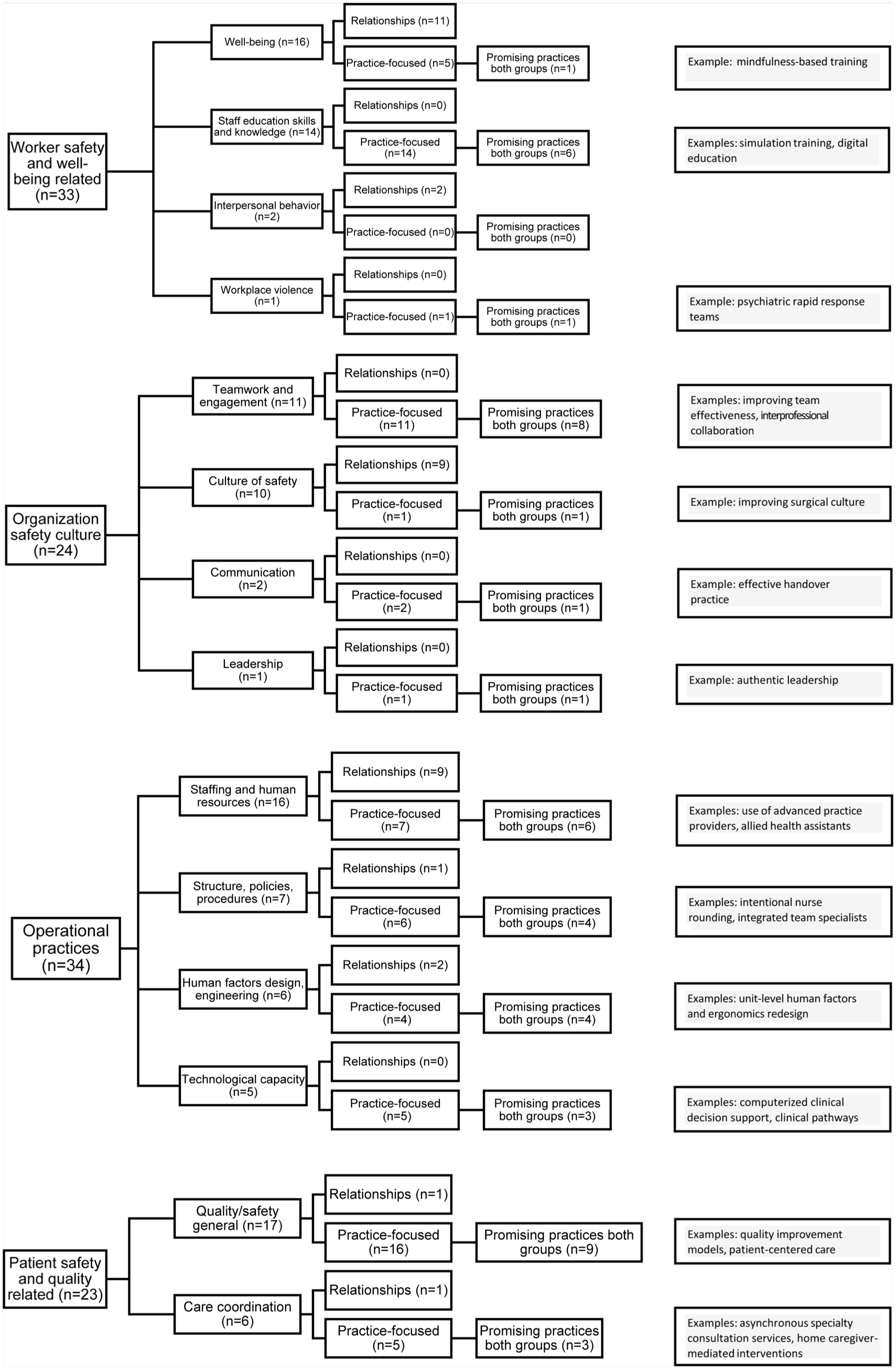
Frequency of included review subtopics and promising practices within major topic areas
Worker Safety and Well-Being Focused Topics
Within this topic area, four subtopics were addressed: well-being (n = 16), staff education, skills, and knowledge (n = 14), interpersonal behavior (n = 2), and workplace violence (n = 1). Thirteen focused on relationships and 20 addressed specific practices. Supplemental Table 3 provides additional detail about each SR, listing first those found to be a promising practice for both, then relationship-focused then those not found to be promising for both.
Among 13 relationship-focused reviews (Table 1), six examined burnout, of which four (Dewa et al., 2017; Garcia et al., 2019; L. H. Hall et al., 2016; Salyers et al., 2017) associated burnout with decreased patient safety and two (Rathert et al., 2018; Tawfik et al., 2019) yielded mixed results. One found fatigue was associated with decreased patient safety (Mansukhani et al., 2012) while another found no clear differences in patient outcomes between sleep-deprived and non-sleep-deprived physicians (Gates et al., 2018). One examined adverse work schedule arrangements and found an association with decreased patient safety (Bernstrøm et al., 2019). Another found better working conditions for physicians was associated with clinical excellence and patient safety (Teoh et al., 2019). One found independent associations between teamwork, clinician well-being, and patient safety (Welp & Manser, 2016). Another examined clinicians’ personality and interpersonal behaviors but found little effect on outcomes (Boerebach et al., 2014). Finally, one found that bullying influenced nursing practice errors and patient outcomes (Johnson & Benham-Hutchins, 2020).
Among 20 practice-focused SRs (Table 2), eight were considered to have promising practices. Examples of promising practices include simulation and tele-education (Bligard et al., 2019; Marples et al., 2017; Tudor Car et al., 2019; Zhou et al., 2016), and surgical resident rotations in aesthetic (cosmetic) surgery clinics (Kaplan et al., 2019). Also promising were mindfulness-based interventions (Braun et al., 2019) and team-based rapid response to workplace violence (Choi et al., 2019).
Three SRs examined medical resident duty hour restrictions but did not show benefits for patient outcomes (Ahmed et al., 2014; Bolster & Rourke, 2015; Philibert et al., 2013). Three SRs examined cultural competency training (Chae et al., 2020; Horvat et al., 2014; Lie et al., 2011), one of which was considered promising (Lie et al., 2011).
Organization Safety Culture Focused Topics
Reviews within this topic area addressed four subtopics: teamwork and engagement (n = 11), culture of safety (n = 10), communication (n = 2), and leadership (n = 1). Nine were classified as relationship SRs and 15 addressed specific practices. Supplemental Table 4 provides additional details about each SR.
All relationship-focused reviews were on the subtopic of culture of safety (Table 1). Four examined nurse work environments and generally found positive associations with patient outcomes (Bae, 2011; Lake et al., 2019; Stalpers et al., 2015; Wei et al., 2018). Two examined workplace culture across settings and found a positive association between culture and patient outcomes (Braithwaite et al., 2017; Dicuccio, 2015). Three examined associations within specific populations with mixed results: safety attitudes of ED staff (Alzahrani et al., 2019); primary care workplace conditions (Kapinos et al., 2012), and organizational culture and performance (activity and outcomes) for older people (Hunt et al., 2012).
Among the 15 practice-focused SRs, 11 were considered to have promising practices for both groups (Table 2). Examples of promising practices include training and interventions to improve teamwork and team effectiveness (Buljac-Samardzic et al., 2020; Costar & Hall, 2020; Dietz et al., 2014; Hughes et al., 2016; Wu et al., 2020), communication (McHugh et al., 2020; Odone et al., 2022), and inter-professional collaboration (Pomare et al., 2020). Also promising were surgery-specific checklists (Lyons & Popejoy, 2014), interventions to improve culture (Sacks et al., 2015) as well as relational (authentic) leadership style (Alilyyani et al., 2018).
Operational Practices Focused Topics
This topic area addressed four subtopics: staffing and human resources (n = 16); structure, policies, and procedures (n = 7); human factors design and engineering (n = 6); and technological capacity (n = 5). Twelve were classified as relationship studies and 22 addressed specific practices. Supplemental Table 5 provides additional detail about each SR.
Among 12 relationship SRs (Table 1), several examined nurse staffing practices such as staffing ratios (Assaye et al., 2021; Sherenian et al., 2013), shift length (Clendon & Gibbons, 2015; Di Muzio et al., 2019), and staffing models (Butler et al., 2019; Wilson et al., 2011) and found associations with specific adverse events. Two examined rationing of nursing care and found associations with negative outcomes (Mandal et al., 2020; Papastavrou et al., 2014). One examined the impact of night/weekend/holiday shift work and found negative associations with specific patient outcomes (de Cordova et al., 2012). Other reviews showing mixed results examined workflow disruptions in the operating room (Koch et al., 2020), design of psychiatric wards (Papoulias et al., 2014), and hospital management and structure for prevention of healthcare-associated infections (Zingg et al., 2015).
Among 22 practice-focused SRs, 17 were considered to have promising practices for both groups (Table 2). Examples of promising operational and clinical staffing models include use of advanced practice clinicians in surgical, emergency, and critical care services (Edkins et al., 2014; Johal & Dodd, 2017; Woo et al., 2017), clinical nurse specialists in outpatient roles (Kilpatrick et al., 2014), integrated nurse-led models for people with functional gastrointestinal disorders (Linedale et al., 2020), incorporating oncology pharmacists on teams (Segal et al., 2019), use of multidisciplinary teams for cancer care (Prades et al., 2015), and use of allied health assistants (Snowdon et al., 2020). Other nursing-related practices included intentional rounding (Sims et al., 2018) and increasing time to provide direct care (Wright & McSherry, 2013). Four SRs addressed human factors and ergonomic interventions (Bugeja et al., 2020; Mao et al., 2015; O’Callaghan et al., 2019; Xie & Carayon, 2015). Three addressed use of health information technology and computerized clinical decision support (Kruse et al., 2017; Neame et al., 2019; Van de Velde et al., 2018). Two others with mixed results were related to health information technology (Hersh et al., 2015; Roshanov et al., 2011).
Patient Safety and Quality Focused Topics
Within this topic area, two subtopics were addressed: quality/safety general (n = 17) and care coordination (n = 6). Two were classified as relationship studies and most (n = 21, 91%) addressed specific practices. Additional details are available in Supplemental Table 6.
Among the relationship studies (Table 1), one found positive associations between surgical volume and outcomes (Leow et al., 2018); the other examined partnerships between generalist and specialist palliative care services and patient/family experience of care with mixed results (Gardiner et al., 2012).
Among 21 practice studies (Table 2), 12 were considered promising, examples of which include quality improvement and performance measurement-related approaches for specific services and settings (Clay-Williams et al., 2014; Côté et al., 2020; Graupner et al., 2021; Jabin et al., 2022; Mason et al., 2015). Also promising were actions directed at changing clinician behavior (Cotterill et al., 2020; Dwamena et al., 2012; Tomasone et al., 2020) and asynchronous, provider-to-provider, electronic consultation services for specialty care (Liddy et al., 2019). Other practices include the chronic care model for diabetes management in primary care (Stellefson et al., 2013), interventions to improve constant observation on inpatient psychiatric wards (Reen et al., 2020), and interventions targeted at family and other non-clinical caregivers (Fiest et al., 2018). Community pharmacist-led medication reconciliation (McNab et al., 2018) and post-discharge telephone calls (Bahr et al., 2014) had mixed results.
Research Gaps
Regarding the secondary research aim to identify gaps, we noted several observations. The literature showed few SRs with explicit goals to measure outcomes for both groups and few prospective controlled designs. Many SRs included a preponderance of correlational analyses within cross-sectional studies and differential attention to either the HCW or patient. Almost all reviews identified the need for more rigorous study designs (controls or comparison groups) and longitudinal data. Among practice-focused SRs, 13 did not identify promising practices for either group; in six of these, authors did not draw any conclusions because the quality of evidence was too weak.
Several included SRs (n = 17) reported promising practices only for one group, suggesting opportunities for further research in these topic areas. Many seemingly relevant SRs were excluded because they only reported outcome measures for one group. These topic areas are ripe for additional research measuring outcomes for both groups with rigorous designs.
Rarely found were common worker safety and well-being topics including task-specific processes (e.g., workflow), physical environment changes (e.g., exposure to hazards, built environment design), and injuries related to safe patient handling and fall prevention. Finally, the lack of objective outcome measures for HCWs, such as loss-time injuries, hazard exposures, work attendance, turnover, etc. suggests a gap in outcome measurement for occupational health research.
Discussion
This scoping meta-review aimed to determine the extent to which existing research identifies promising, evidence-based practices that improve safety for both HCWs/organizations and patients and to identify research gaps. Overall, 114 reviews met the inclusion criteria and were classified as either relationship studies (n = 36) or practice-focused studies (n = 78), of which 48 practices were considered promising, defined as likely to benefit both workers and patients.
The findings revealed that safety for HCWs and patients can potentially be improved through promising practices and actions directed toward either or both groups. Similarly, a wide range of topic areas can be addressed that directly or indirectly impact worker safety, organizational culture, operational practices, and patient safety. Examples of promising practices included team-based strategies to improve performance, technological skills, quality improvement and patient-centered care, actions that foster leadership engagement in safety culture, and increased attention to human factors and systems design.
The Intersection of Topic Areas and Promising Practices
Though separated for analysis purposes, many interrelationships exist among the four major topic areas. For example, operational practices (e.g., staffing patterns) set by leadership will affect staff perceptions of culture as will responses to adverse events (Tawfik et al., 2023). In three of four major topic areas, more than 50% of practice-focused reviews were considered promising for both groups, highlighting the interactive relationships in healthcare settings.
Actions targeting how work is designed and organized may offer the most benefits to both workers and patients. The Operational Practices topic area had the highest yield of promising practices within the subtopics of staffing and human resources, structure, policies and procedures, and human factors design and engineering.
The Organization Safety Culture subtopic of teamwork and engagement yielded 73% promising practices, suggesting greater uptake of these practices may enhance safety climate (Rotenstein et al., 2024). Arguably, teamwork and engagement may be thought of as an attribute of an organization’s safety culture, as it relates to “the way we do things around here,” which is often used as a commonplace definition of organizational culture (Grissinger, 2014). The high proportion of reviews finding teamwork likely to benefit both groups may be in part because some training strategies have been formally evaluated in nationwide studies (Buljac-Samardžić et al., 2021; Chen et al., 2019; Dinh et al., 2020).
Reviews focused on Patient Safety and Quality frameworks for improvement were also likely to benefit both groups. Such efforts typically target important parameters of patient care (e.g., patient centeredness) and direct attention to operational processes and interactions, which can also enhance worker participation, horizontal integration, and overall engagement (AHRQ, 2020; Plsek, 1999; Simpson, 2009). For example, Aiken reported that clinicians preferred improvements in staffing and work environments for enhancing their well-being over clinician wellness and resilience programs (Aiken et al., 2023).
Reviews related to Worker Safety and Well-being relationships showed that burnout, fatigue, and bullying were consistently associated with adverse effects on both patients and HCW. However, reviews addressing the impact of medical resident duty hour restrictions on patient outcomes did not document patient benefit (Ahmed et al., 2014; Bolster & Rourke, 2015; Philibert et al., 2013) and one SR suggested increased complication rates in high-acuity surgical patients (Ahmed et al., 2014).
Reviews focusing on the more abstract concept of safety culture showed few promising practices but yielded several relationships. This is unsurprising as safety culture is challenging to measure and harder to change (Schein, 2010). Similarly, fewer promising practices in the Worker Safety and Well-being topic area may be due to the design of the SR’s included studies, which often measure outcomes like burnout and fatigue but do not feature initiatives designed to alleviate these outcomes. Also, the databases searched comprised more medical care journals than occupational health journals, the latter of which may be less likely to address patient outcomes than the converse.
Nevertheless, few promising practices in subtopic areas do not imply these relationships are unimportant. Strong and consistent associations across SRs provide important signals demanding further attention and evaluation of specific interventions. Similarly, lack of supportive evidence for a practice does not necessarily mean it is ineffective, that is, “absence of evidence of effect need not imply evidence of absence of effect.” (Boerebach et al., 2014). Lack of evidence could be due to reasons such as few evaluation studies, weak or underpowered study designs, and/or publication bias.
Strengths and Limitations
To our knowledge, this is the first ScMR to take a systems-level, integrated approach to considering practices that can improve both worker and patient safety. The integrated approach, broad inclusion criteria, and general definition of safety enabled the wide range of topics and available SRs. All included SRs reported actual outcome measures for both groups, not just process of care measures. Reliability was enhanced through two-person screening of all abstracts and full-text articles with team discussion to resolve disagreements.
However, several limitations exist. Importantly, our findings are limited to publications through 2020. Many reviews have given this area increased attention after the pandemic (Li et al., 2024; Tawfik et al., 2023). The breadth of topics, study designs, and heterogeneity of outcomes precluded assessing the quality and extent of SR bias. We searched widely in peer-reviewed literature but not gray literature. Excluding SRs measuring only care processes without outcomes may have led to missing some relevant studies.
A review of reviews makes it impracticable to know the details of individual studies within the SRs; some data elements may have been missed or misclassified. Terminology challenges existed; few authors differentiated between measures of quality of care and patient safety, partly because patient safety-related outcomes are rare events and inconsistently defined (AHRQ, 2019; Mitchell, 2008; Shahian et al., 2016). Safety culture was another poorly defined term used differently among SRs (Guldenmund, 2000). Given the preponderance of studies by non-U.S. authors, we may have misinterpreted specific terms.
Finally, identifying promising practices from SR authors’ conclusions sometimes required judgment, as authors’ conclusions varied by their included study designs (e.g., only controlled studies); evaluation of study quality; outcome measures reported; and the sensitivity of the outcomes to the intervention. In some cases, authors had a worker or patient safety research perspective which influenced interpretations and conclusions. Related challenges occurred when findings from both groups were not explicitly mentioned in conclusions, when a SR addressed multiple interventions, or when the primary focus group was unclear.
Implications for Research
We found several major research gaps. Methodologically stronger designs with outcomes for both groups are required for evaluating practices. The dearth of SRs evaluating interventions related to burnout and safety culture suggests a critical area for future research. Valid and reliable measures exist for assessing burnout and culture, but future research could focus on developing and testing interventions (e.g., workplace policies and programs) that aim to reduce adverse outcomes. Also, researchers may wish to focus on fewer topic areas and evaluate the quality of the included reviews. Our breadth in topic areas made categorization challenging.
The wide variety of outcome measures for workers, organizations, and patients across SRs can be useful for those evaluating the impact of practice on multiple groups. Reviews often included both objective and subjective measures, which sometimes yielded inconsistent findings about a particular practice. Mixed method evaluation may support the feasibility of collecting outcome data sensitive to the expected mechanism of effect. Per Tawfik et al. (2019), “further research is needed to determine the appropriate balance between insensitivity of objective quality metrics and potential for recall bias with subjective quality metrics.” Proxy outcomes are sometimes needed when measuring actual outcomes for both groups is unethical. For example, one cannot prospectively assess the impact of sleep deprivation on surgical patient outcomes using intentionally sleep-deprived surgeons, however, simulators can be used to measure performance (Whelehan et al., 2020).
We were surprised to find that most included studies were done by teams of authors, all of whom were from outside the U.S. National healthcare systems may be better positioned to examine changes that impact both worker and patient safety than systems tied to private and public insurance. This suggests more research is needed to enhance generalizability across countries.
Implications for Practice
These findings strengthen the case for organizations to consider an integrated, non-siloed approach to improving safety that assesses the impact of interventions to both HCWs and patients. As recommended by Benishek et al. (2023) “If clinician well-being is not considered as part of the patient safety equation, we risk losing buy-in for future interventions, burning out the workforce, fueling turnover, and ultimately reducing the efficiencies and care quality we have fought so hard to improve. However, if it is done right and a human-centered mindset is adopted, well-being to clinicians can be restored through an enhanced work environment and to patients through improved care quality.” Since healthcare settings comprise interactive systems, it seems only logical to consider safety for both workers and patients together.
Before adopting or adapting any of the identified promising practices, readers are strongly encouraged to examine the referenced SRs and source articles therein to ascertain the quality of each study and appropriateness of the authors’ conclusions. Reviews led by evidence synthesis organizations (e.g., Cochrane Collaboration or JBI) often had very stringent inclusion criteria. It is important to consider the context of the SRs’ included studies and the need for and readiness of one’s own organization for implementing the practice.
Similarly, this report does not conclusively demonstrate directionality or causation regarding the promising practices. Most studies included in the SRs were not randomized controlled trials and are subject to confounding factors and biases (Weinberger et al., 2001). For example, one cannot easily determine that strengthening safety culture caused better patient outcomes or that enhancing patient care coordination increased worker satisfaction. Instead, one must acknowledge that associations may be direct or indirect. As described by Tawfik et al. (2019), “whether curtailing burnout improves quality of care, or whether improving quality of care reduces burnout, is not yet known, and adequately powered and designed randomized trials will be indispensable in answering these questions.” Similarly, we did not address the magnitude of improvement when identifying promising practices. In some cases, the effect size of improvements when reported was large, but in many cases the differences in outcomes were quite small.
Conclusion
This scoping meta-review identified a wide range of practices and topic areas that can be addressed to directly and/or indirectly improve safety for both HCWs/organizations and patients. It is important for healthcare leaders and managers to consider adopting an integrated approach to evaluating the impact of safety improvement interventions and operational practice changes on both patients and workers to enhance the effectiveness and value of efforts to improve safety.
Implications for Occupational Health Practice
Efforts to improve healthcare worker safety have traditionally been viewed as separate and unrelated to patient safety. This study identified synergies between worker and patient safety and calls for an integrated approach to intervention and operational practice design. Occupational health, safety, and patient safety leaders should consider working collaboratively to implement promising practices that improve both worker and patient safety in healthcare settings.
In Summary
Because few studies have evaluated practices that improve safety for both workers and patients, this scoping meta-review (including only systematic reviews) was conducted to determine the extent to which existing literature identifies practices that improve outcomes for both groups.
After multi-stage screening of 1,619 abstracts and 642 full texts, 114 reviews met the inclusion criteria and addressed 4 major topic areas: Worker Safety and Well-being (n = 33), Operational Practices (n = 34), Organization Safety Culture (n = 24), and Patient Safety and Quality (n = 23).
Of 78 systematic reviews addressing specific practices, 48 reported evidence of being likely to benefit both workers and patients and are described in Table 2 and Supplemental Tables 3 to 6.
Occupational health/safety and patient safety leaders should consider working collaboratively to implement promising practices that improve both worker and patient safety.
Supplemental Material
sj-docx-1-whs-10.1177_21650799261446613 – Supplemental material for Improving Healthcare Workforce and Patient Safety: A Scoping Meta-Review
Supplemental material, sj-docx-1-whs-10.1177_21650799261446613 for Improving Healthcare Workforce and Patient Safety: A Scoping Meta-Review by Barbara I. Braun, Michele R. Bozikis, Megan L. Casey, David N. Weissman, Katherine J. Orze, Annette Riehle and David M. DeJoy in Workplace Health & Safety
Supplemental Material
sj-docx-2-whs-10.1177_21650799261446613 – Supplemental material for Improving Healthcare Workforce and Patient Safety: A Scoping Meta-Review
Supplemental material, sj-docx-2-whs-10.1177_21650799261446613 for Improving Healthcare Workforce and Patient Safety: A Scoping Meta-Review by Barbara I. Braun, Michele R. Bozikis, Megan L. Casey, David N. Weissman, Katherine J. Orze, Annette Riehle and David M. DeJoy in Workplace Health & Safety
Supplemental Material
sj-docx-3-whs-10.1177_21650799261446613 – Supplemental material for Improving Healthcare Workforce and Patient Safety: A Scoping Meta-Review
Supplemental material, sj-docx-3-whs-10.1177_21650799261446613 for Improving Healthcare Workforce and Patient Safety: A Scoping Meta-Review by Barbara I. Braun, Michele R. Bozikis, Megan L. Casey, David N. Weissman, Katherine J. Orze, Annette Riehle and David M. DeJoy in Workplace Health & Safety
Supplemental Material
sj-docx-4-whs-10.1177_21650799261446613 – Supplemental material for Improving Healthcare Workforce and Patient Safety: A Scoping Meta-Review
Supplemental material, sj-docx-4-whs-10.1177_21650799261446613 for Improving Healthcare Workforce and Patient Safety: A Scoping Meta-Review by Barbara I. Braun, Michele R. Bozikis, Megan L. Casey, David N. Weissman, Katherine J. Orze, Annette Riehle and David M. DeJoy in Workplace Health & Safety
Supplemental Material
sj-docx-5-whs-10.1177_21650799261446613 – Supplemental material for Improving Healthcare Workforce and Patient Safety: A Scoping Meta-Review
Supplemental material, sj-docx-5-whs-10.1177_21650799261446613 for Improving Healthcare Workforce and Patient Safety: A Scoping Meta-Review by Barbara I. Braun, Michele R. Bozikis, Megan L. Casey, David N. Weissman, Katherine J. Orze, Annette Riehle and David M. DeJoy in Workplace Health & Safety
Supplemental Material
sj-docx-6-whs-10.1177_21650799261446613 – Supplemental material for Improving Healthcare Workforce and Patient Safety: A Scoping Meta-Review
Supplemental material, sj-docx-6-whs-10.1177_21650799261446613 for Improving Healthcare Workforce and Patient Safety: A Scoping Meta-Review by Barbara I. Braun, Michele R. Bozikis, Megan L. Casey, David N. Weissman, Katherine J. Orze, Annette Riehle and David M. DeJoy in Workplace Health & Safety
Footnotes
Acknowledgements
We are most grateful to Mushira Khan PhD, Ethalle Ukeka MPH, Meghann Adams MPH, and Haley Jordan Seaman BA for project coordination, data collection, and/or editorial assistance.
Author Contributions
Conceptualization—BB, DD, MC, DW; Methodology—BB, DD, MC, DW, MB, KO, AR; Software—KO; Validation—BB, MB, DD, AR; Formal Analysis—BB, MB, DD; Investigation—BB, DD, MB, KO, AR; Data curation—MB, KO, BB; Writing—Original Draft—BB, MB, DD; Writing Review & Editing—DD, MC, AR, DW; Visualization—BB, MB.
Conflict of Interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded in part by the CDC National Institute for Occupational Safety and Health under contract # 75D30120P08556.
Ethical Considerations
This activity was reviewed by CDC, deemed research not involving human subjects, and conducted consistent with applicable federal law and CDC policy. No a priori review protocol was specified and evaluation of systematic review quality was not done.
Disclaimer
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the National Institute for Occupational Safety and Health, Centers for Disease Control and Prevention or The Joint Commission. No AI was utilized in manuscript preparation.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.