
Abstract
Background:
Despite awareness of night shift work’s mental health risks, its long-term effects, especially sex differences, remain underexplored. The aim of the study was to investigate the association between night shift work and mental health outcomes using multivariable regression models and to assess sex differences in these associations.
Methods:
We analyzed data from 9,057 participants (mean age = 22.08 years, 52.6% females) who participated in Waves III (2001–2002), IV (2008–2009), and V (2016–2018) of the National Longitudinal Study of Adolescent Health (Add Health) in the USA. Associations between night shift work and mental health outcomes were assessed using binomial generalized linear models to estimate relative risks (RR; 95% CIs). We tested night shift with sex interactions and performed sex-stratified analyses when significant.
Findings:
Night shift work for 17 years (4.6% of the participants), was associated with an increased risk of suicidal ideation (RR = 2.30, 95% CI [1.35, 3.90]) and depression (RR = 1.46, 95% CI [1.02, 2.09]) in women, but not in men. Depressive symptoms including feeling unhappy (RR = 1.69, 95% CI [1.15, 2.46]) and “shake blue/feeling blue” (RR = 2.04, 95% CI [1.01, 4.12]) were significantly associated with night shift work in men. In women, feeling sad (RR = 1.79, 95% CI [1.05, 3.07]) and “shake blue/feeling blue” (RR = 1.87, 95% CI [1.02, 3.43]) were also significantly linked to night shift work.
Conclusions/Application to Practice:
Long-term night shift work was associated with suicidal ideation and depression among women, but not men, reflecting sex-specific susceptibility to adverse mental health outcomes. Our findings suggest the need for sex-specific interventions to address the mental health risks of night shift work, particularly in women.
Introduction
Shift work is defined as “any work schedule that falls outside the hours of 7 am and 6 pm (. . .) which can include evening, night, and early morning shifts, as well as fixed or rotating schedules” (U.S. Bureau of Labor Statistics, 2020). Night shifts, in particular, has long been essential for sustaining critical services and enhancing industrial efficiency (Guénel & Léger, 2023). However, today it remains indispensable, not only for essential services but also across other industries like information technology, logistics, tourism, and entertainment. As a result, non-standard work schedules have become a defining feature of the modern workforce, with significant portions of workers in both the U.S. and Europe engaged in night shifts or irregular work patterns (European University Institute, n.d.; U.S. Bureau of Labor Statistics, 2020).
Nevertheless, night shift work has been linked to a range of adverse health outcomes. Shift work, particularly at night, is associated with increased risks of chronic conditions such as type 2 diabetes (Romero-Parra et al., 2025), cancer (Dun et al., 2020), or sleep disorders (Kerkhof, 2018). Additionally, night shift work is increasingly recognized as a risk factor for mental health problems (Zhao et al., 2019). The impact on mental health is particularly concerning given the global rise in mental health disorders and the critical role of mental well-being in overall health-related quality of life (Moitra et al., 2023).
Night shift work disrupts circadian rhythms, resulting in chronic sleep deprivation and subsequent physiological and psychological stress (Boivin et al., 2022). These disruptions are believed to significantly elevate the risk of mental health issues (Walker et al., 2020). Although research on this topic is limited, existing studies indicate that the impact of night shifts on mental health may vary by sex. For example, a study involving workers at an electronics manufacturer, found that women engaged in shift work had a significantly higher risk of depression, whereas this risk was not significantly elevated for men (Kang et al., 2017). In contrast, previous studies revealed a significant association between shift work and suicidal ideation among men, while the association was not significant for women (Kim et al., 2019; H. Park et al., 2022; Takusari et al., 2011).
Despite increasing awareness of the mental health risks associated with night shift work, its long-term effects on the general workforce, particularly with respect to sex differences, remain underexplored. Moreover, previous studies have often been limited by cross-sectional designs (Kang et al., 2017; Takusari et al., 2011), short follow-up periods and a narrow focus on specific occupational groups such as nurses (Bildt & Michélsen, 2002) or industrial workers (Kang et al., 2017; Son & Lee, 2021). To address these gaps, this prospective cohort study aims to investigate the long-term relationship between night shift work and mental health outcomes, including depression and suicidal ideation, in a U.S. population, using multivariable regression models and assessing sex differences.
Methods
Population Sample and Study Design
This study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines (Von Elm et al., 2007), and used data from the National Longitudinal Study of Adolescent to Adult Health (Add Health) study, a nationally representative sample of adolescents in grades 7 to 12 in the U.S. followed from adolescence through adulthood (Harris et al., 2019). The baseline sample (Wave I) was recruited in 1994 to 1995 using a multistage, stratified cluster sampling design, with students initially surveyed in-school and a stratified subsample selected for in-home interviews. The Wave I in-home interview achieved a response rate of approximately 79%. In this study, we used data from Waves III (2001–2002; response rate 77.4%), IV (2008–2009; response rate 80.3%), and V (2016–2018; response rate 72%), during which information on work shift type was collected via interviewer-administered in-home questionnaires. Retention relative to the original Wave I cohort was approximately 73.2% at Wave III, 75.7% at Wave IV, and 68.8% at Wave V. Participants were eligible for inclusion if they completed these waves and provided information on night shift work and mental health outcomes. Individuals with missing data on key exposure or outcome variables were excluded. A participant flow diagram is provided in Figure 1.
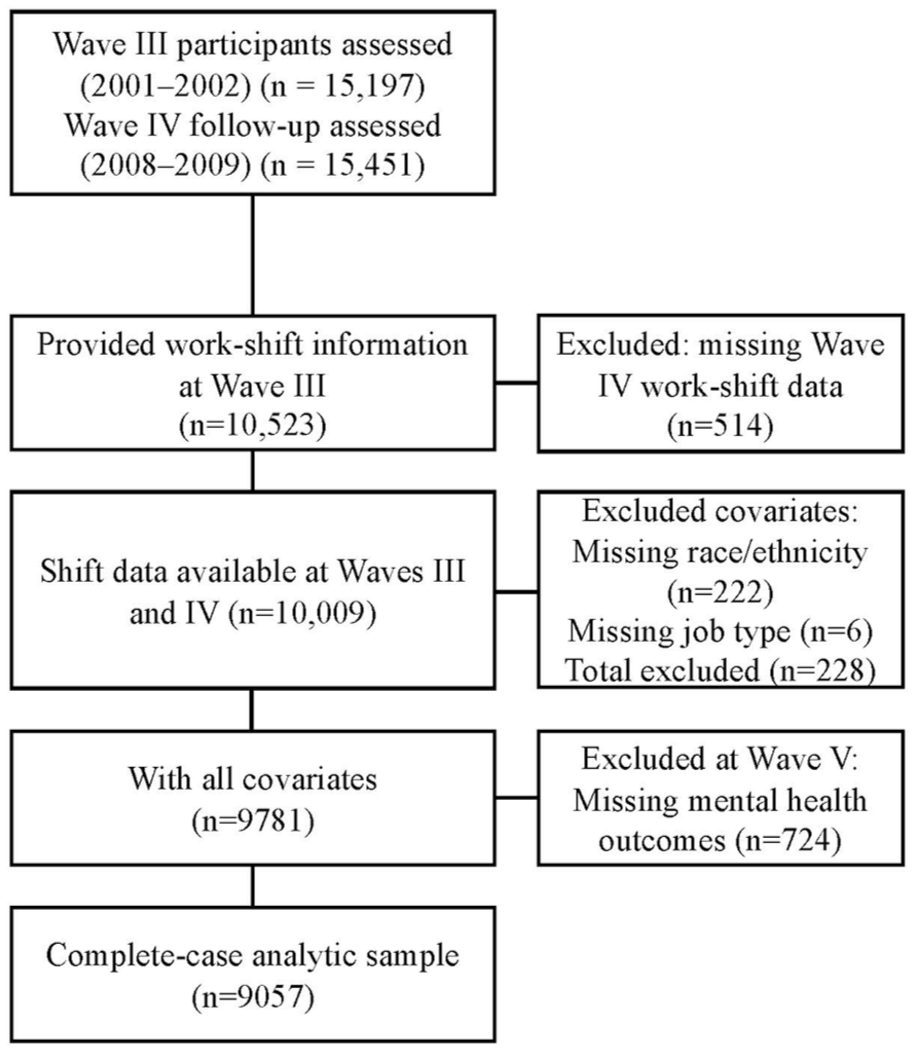
Flowchart of the study cohort
The Add Health study was approved by the Institutional Review Board (IRB) at the University of North Carolina at Chapel Hill. The permission to conduct secondary analyses was obtained by the Ethics Committee of the University Hospital of Navarra (PI_2020/143).
Shift Work (Independent Variable)
Shift work information was gathered for individuals who were employed using a simple question: 1) “Which of these categories best describes the hours you work at this job?” with the response categories “regular day shift,” “regular evening shift,” “regular night shift,” “shift rotates” (i.e., changes periodically from day to evening or night), “split shift” (i.e., two distinct periods each day), “irregular schedule or hours.” For the present analyses, work schedule was dichotomized as follows: (1) Regular daytime shift (“regular day shift”), and (2) Night Shift (“regular night shift” or “shift rotates”). Participants reporting “regular evening shift,” “split shift,” or “irregular schedule or hours” were excluded from the analytics sample, as these schedules do not necessarily imply night work and could lead to exposure misclassification. In this study, we considered participants to be night shift workers only if they reported working night shifts (“regular night shift” or “shift rotates”) at both Wave III and IV. Work-shift schedule was assessed at Waves III and IV. Wave IV data were used to confirm exposure status over time; participants were classified as long-term night shift workers only if they reported “night shift” or “rotating shift” at both waves. Participants without Wave IV shift information were not eligible for exposure classification.
Depression Symptoms (Dependent Variable)
Adults were categorized as having depression if they had self-reported history of depression (“Has a doctor, nurse, or other health care provider ever told you that you have or had depression?”) and/or any prescription medication-use for depression in the past 4 weeks. Also, adults at Wave V were asked in the prior 7 days how often they experienced the following symptoms: “felt depressed,” “felt sad,” “felt happy” (reverse coded), “could not shake off the blues,” and “felt that life was not worth living.” Responses to each item ranging from 0 to 3: 0 = “never or rarely,” 1 = “sometimes,” 2 = “a lot of the time,” 3 = “most of the time or all the time.” For the purposes of analysis, symptoms were categorized as present if respondents reported any level of symptom experience (numeric value ≥1, i.e., “sometimes,” “a lot of the time,” or “most of the time or all of the time”).
Suicidal Ideation (Dependent Variable)
Suicidal ideation was assessed by a single question with a dichotomic yes/no response option: “During the past 12 months, did you ever seriously think about committing suicide?” Suicidal attempts were assessed by a single item: “During the past 12 months, how many times did you attempt suicide?” This question included the following response options: “zero,” “one,” “two,” “three,” and “four or more.” We categorized this variable as dichotomous, coding 0 attempts (“zero”) as no, and ≥1 attempt (“one,” “two,” “three,” or “four or more”) as yes.
Covariates
Information on sociodemographic factors, such as age, race/ethnicity (operationalized as a four-level: White, Black, Native American, and Asian), hours worked per week, and type of job, was collected through in-home questionnaires at Wave III.
Statistical Analysis
We described the analytic sample, including tests to identify significant differences based on night shift work. Descriptive data are presented as frequencies and percentages for categorical variables, and as means and standard deviations for continuous variables. Model specification and convergence were checked for all generalized linear models. When analyzing the interaction between night shifts and sex with various dependent variables (e.g., history of depression p < .001), we observed a significant interaction between the two factors. Consequently, the analyses were conducted separately for men and women.
Generalized linear models with a binomial distribution were used to assess the risk of a history of depression, depression symptoms, and suicidal ideation in relation to night shifts compared with regular daytime shifts. For each outcome, we first estimated unadjusted models, followed by models adjusted for age, race/ethnicity, hours worked per week, and type of job, all measured at Wave III.
All analyses were conducted in R (Version 4.3.2) and RStudio (Version 2023.09.1+494). Statistical significance was set at two-sided p < .05.
Results
Table 1 shows descriptive statistics for the full sample at Wave III. The study sample comprised 9,057 participants (mean age = 22.08 years, 52.6% females). Of these, 8,642 worked in regular day shifts, and 415 worked in night shifts or night rotating shifts. Racial composition was predominantly White (73.9%), followed by Black or African American (19.3%), Asian or Pacific Islander (5.9%), and a small fraction identifying as American Indian or Alaska Native (0.9%). The participants worked an average of approximately 37 hours per week across various occupations. Among night shift workers, the most common occupational categories were personal care and service (20.7%), protective service (15.9%), and installation, maintenance, and repair (10.6%). For interpretation, occupations related to personal care and healthcare (i.e., personal care and service, healthcare practitioners and technical, and healthcare support) were considered together, as they represent service-oriented roles involving direct care of individuals. At Wave V, 24.2% of participants were diagnosed with depression, and 6.2% reported suicidal thoughts. Regarding depressive symptoms, 20.5% reported feeling depressed, 11.9% felt sad, 27.7% reported being unable to shake off the blues, 21.0% reported feeling unhappy, and 21.8% felt that life was not worth living.
Demographic Characteristics of the Participating Subjects During Wave III According to Job Shift
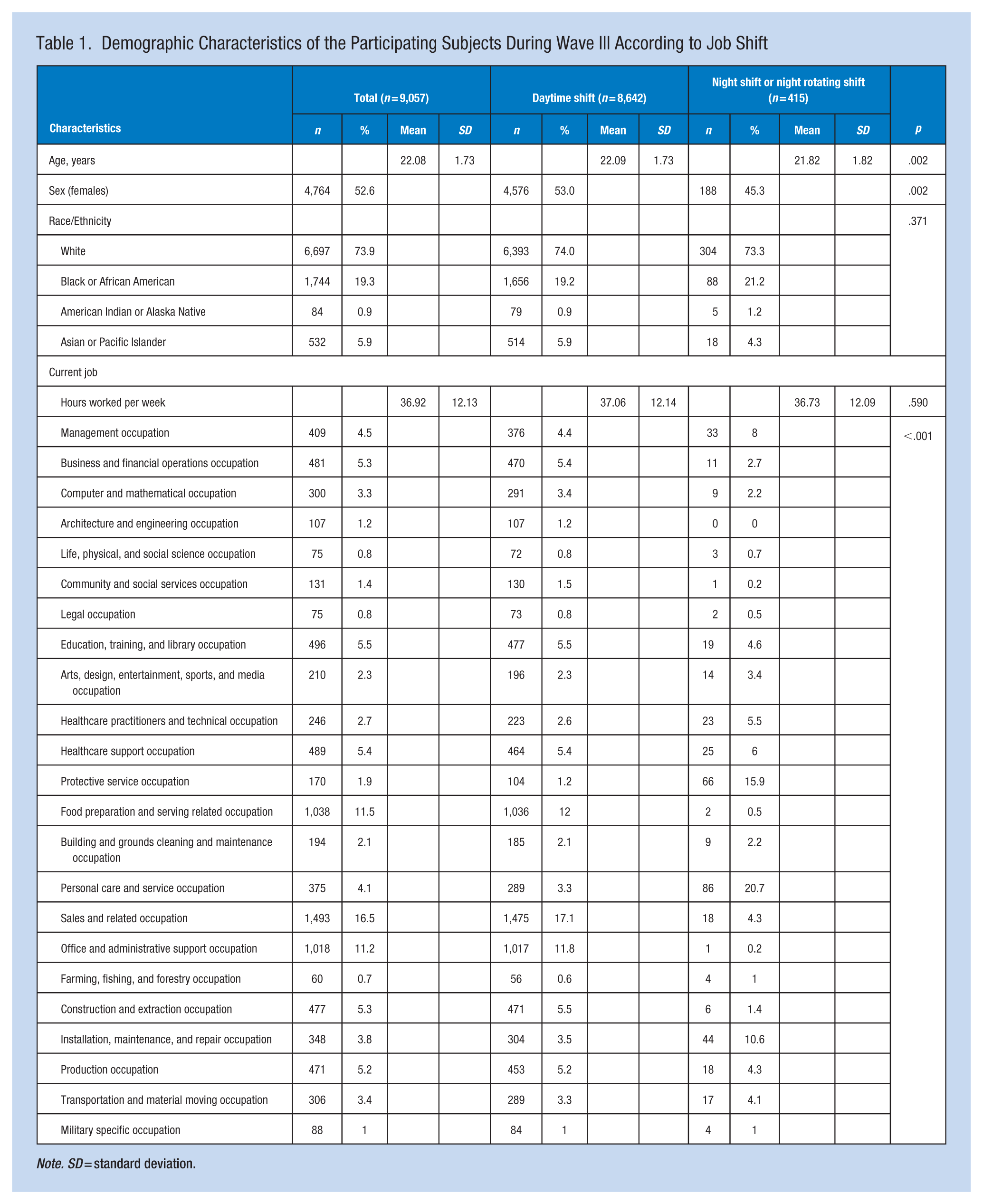
Note. SD = standard deviation.
The relative risk (RR) and 95% confidence interval (CI) for suicidal ideation, diagnosis of depression, and depression symptoms among night shift workers, divided by sex, is shown in Table 2. Regarding suicidal ideation, men night shift workers showed a non-significant RR of 1.71 (95% CI [0.98, 2.98], p = .059), which decreased to 1.52 (95% CI [0.84, 2.74], p = .163) in the adjusted model. In the case of women night shift workers, the crude model indicated a significant RR of 2.51 (95% CI [1.50, 4.20], p < .001), with the adjusted model showing a slightly lower yet significant RR of 2.30 (95% CI [1.35, 3.90], p = .002). Suicide attempts were rare in the study population (1.1% among men and 1.5% among women). Due to the very small number of events, stratified regression analyses yielded unstable estimates with wide confidence intervals; therefore, suicide attempts were not included in Table 2.
Relative Risks (RR) and 95% Confidence Intervals (CI) for Mental Health Outcomes at Wave V Among Night Shift Workers Compared With Day Shift Workers, Stratified by Sex
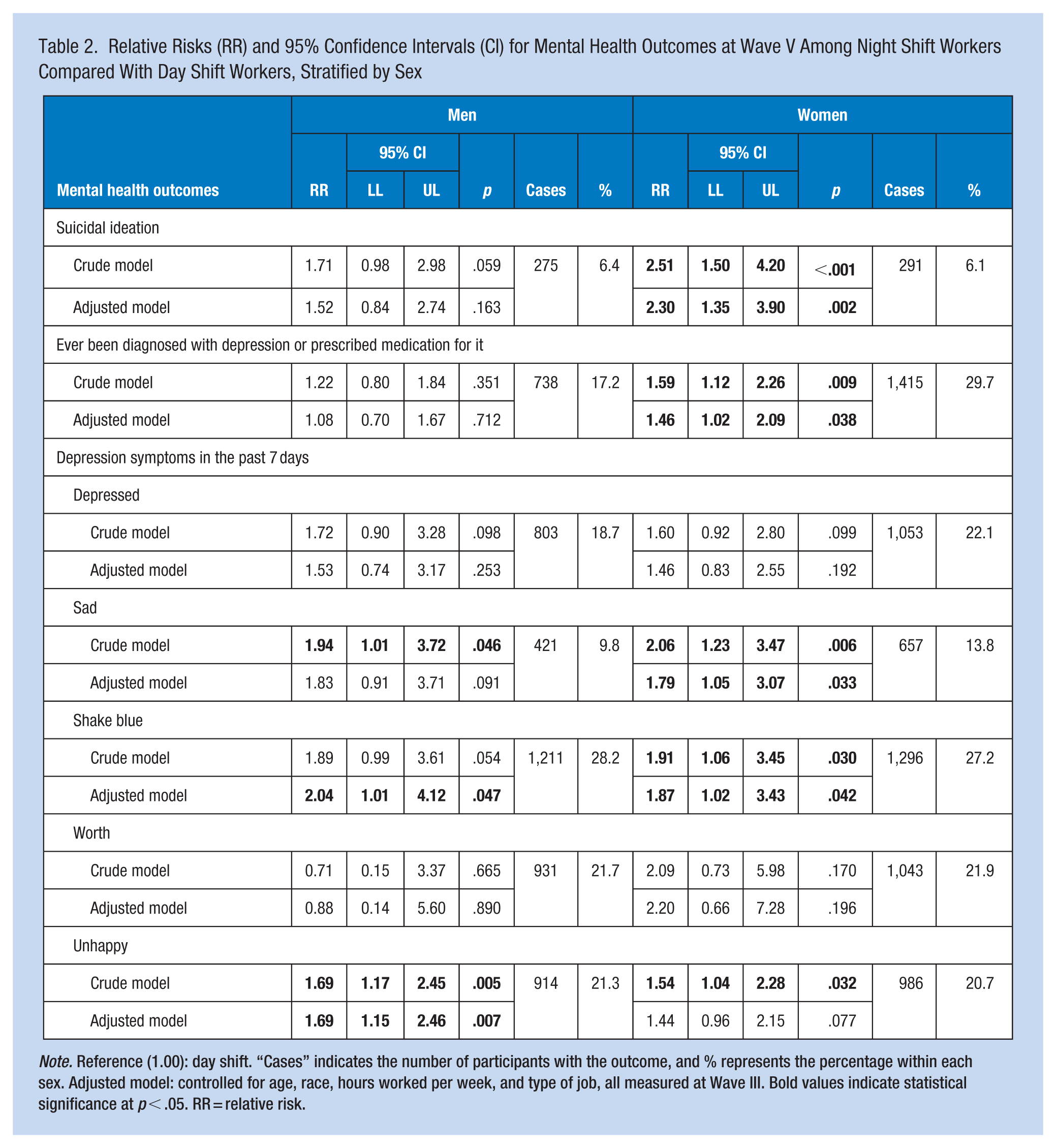
Note. Reference (1.00): day shift. “Cases” indicates the number of participants with the outcome, and % represents the percentage within each sex. Adjusted model: controlled for age, race, hours worked per week, and type of job, all measured at Wave III. Bold values indicate statistical significance at p < .05. RR = relative risk.
The risk for being diagnosed with depression or having prescribed medication for it, was not significant among men, where RR was 1.08 (95% CI [0.70, 1.67], p = .712) in the adjusted model. However, this risk was significant for women (adjusted model: RR of 1.46 [95% CI [1.02, 2.09], p = .038]).
Regarding depression symptoms in the past 7 days, night shift work was associated with feeling unhappy (RR = 1.69 [95% CI [1.15, 2.46], p = .007]) and feeling so depressed that nothing could cheer you up (“shake blue”) among men (RR = 2.04 [95% CI [1.01, 4.12], p = .047]). In women, feeling sad (RR = 1.79 [95% CI [1.05, 3.07], p = .033]) and “shake blue” (RR = 1.87 [95% CI [1.02, 3.43], p = .042]) were significantly associated with night shift work.
Discussion
This study examined the association between night shift work and mental health outcomes, focusing on depression and suicidal ideation among young adults. Our findings indicate that night shift work is significantly associated with an increased risk of depression and suicidal ideation, particularly among women. Our results highlight the importance of considering sex-specific factors when assessing the mental health risks associated with night shift work.
The disruption of circadian rhythms, a critical regulator of sleep-wake cycles and mood, is a well-documented consequence of night shift work (Boivin et al., 2022). Shift workers operate during hours that are misaligned with their natural physiological and social rhythms, leading to poor sleep quality, melatonin suppression, and increased risks of mood disorders (Lim et al., 2020). The occupational distribution of night shift workers should also be considered, as these participants were more commonly employed in care-related, protective service, and maintenance occupations. Such jobs often involve high job strain, emotional demands, and irregular schedules, which may exacerbate circadian disruption and contribute to poorer mental health outcomes. Our findings showed that women who worked night shifts were significantly more likely to experience depressive symptoms compared to their counterparts who had day work. These findings are consistent with previous studies, which have linked night shift work to subclinical depression in female nurses (Okechukwu et al., 2023), and depressive disorder in women from the general workforce (Torquati et al., 2019). These results could be attributable to several factors. For instance, from a biological point of view, the naturally shorter circadian rhythms of women, including melatonin release and body temperature, which are naturally set earlier than men (Walton et al., 2022), could make them more prone to disruption from night shifts. Additionally, although chronotype was not assessed in our study, women tend to prefer morning activities and are more likely to be “morning types” (Randler & Engelke, 2019), which may further amplify the negative impact of working during night hours. Likewise, hormonal differences, such as fluctuations in estrogen and progesterone, may make women more vulnerable to the detrimental effects of disrupted sleep and circadian misalignment (Haufe & Leeners, 2023) and could exacerbate the impact on mood regulation. Other explanations may involve the fact that women often face a higher burden of work-life conflict, particularly when balancing night shifts with family responsibilities (Tucker et al., 2021). This dual pressure can amplify stress levels and contribute to mental health issues. Social and cultural expectations may also play a role, as women are frequently expected to fulfill caregiving responsibilities even after working demanding shifts (Cakan & Yildiz, 2020), further intensifying their stress and emotional exhaustion. Similarly, the unconventional hours of night shifts could also lead to social isolation, reducing opportunities for social interaction and support. For women, who tend to rely heavily on social networks for emotional support (Shin & Park, 2023), this isolation could be a critical factor in the development of depressive symptoms.
Similarly, our findings also revealed that women who worked night shifts were significantly more likely to experience suicidal ideation, aligning with previous studies (Son & Lee, 2021; Yoon et al., 2015), which reported similar associations in women. Many of the pathways already discussed in the association between night shift work and depression may also help explain these results, given that depression is a strong predictor of suicidal ideation (Dugas et al., 2012). Moreover, although we did not measure individual factors, it is likely that elements such as psychiatric disorders, substance abuse, a history of trauma or abuse, chronic physical illness or pain, financial difficulties, interpersonal conflicts, and previous suicide attempts could have contributed to these findings (Groves et al., 2023; H. Park & Lee, 2022; Riera-Serra et al., 2024; Smith et al., 2004). Regarding occupational factors, while the duration of each shift was not measured in our study, existing research indicates that long working hours and shift work may increase suicidal ideation (Yoon et al., 2015). Chronic sleep deprivation could disrupt emotional regulation and increase feelings of hopelessness, key risk factors for suicidal thoughts. Additionally, other occupational factors like low pay, job insecurity, and the risk of injury may further contribute to increased suicide risk (Greiner & Arensman, 2022). Certain professions might also provide easier access to lethal means of suicide (Agerbo et al., 2007), potentially influencing the observed outcomes.
Regarding men, we observed a significant association between night shift work and depressive symptoms, such as feeling unhappy and being unable to shake off the blues. However, despite these symptoms, male participants did not appear to be at a higher risk for developing depression or suicidal ideation compared to those working regular day shifts. This could suggest that men may physiologically adapt more effectively to the circadian disruptions caused by night shift work (Dorsey et al., 2021). Research indicates that hormonal responses to sleep deprivation differ between sexes, potentially offering men some protection against the adverse effects (Dorsey et al., 2021). Additionally, societal norms often place less emphasis on men’s domestic responsibilities, which may alleviate the strain between work and home life. Furthermore, men are generally less likely to report mental health struggles, as societal norms around masculinity discourage help-seeking behaviors (Galdas et al., 2005), potentially leading to underreporting. However, our results contrasts with previous studies, which have reported stronger associations between night shift work and anxiety or depression in men (Bara & Arber, 2009; J. N. Park et al., 2016), or night shift associated with suicidal ideation (H. Park et al., 2022; Takusari et al., 2011), while failed to find the same associations in women working in night shifts, with the latter findings originating from studies conducted in South Korea and Japan. These discrepancies could be attributable to cultural differences, such as the more rigid and hierarchical work environments often found in Asian countries, where long working hours and high job demands are common, compared to the more flexible work routines in US, which may emphasize work-life balance (Le et al., 2020). Additionally, lifestyle factors such as diet, physical activity, and social support systems can vary significantly between these regions, potentially influencing the outcomes of these studies.
Strengths and Limitations
Strengths of this study include its large sample size and prospective design with a long-term follow-up of 17 years, which allowed us to track changes in mental health over time and establish temporal relationships between night shift work and mental health outcomes. However, several limitations must be acknowledged. First, the reliance on self-reported data may introduce reporting bias, particularly in the measurement of mental health conditions. Depression was assessed using self-reported history of diagnosis and/or depression-related medication use, without validated symptom scales or information on specific medications, which may have led to non-differential misclassification. Additionally, dichotomizing symptom responses may have misclassified some participants and reduced the specificity of the data. Moreover, the “ever diagnosed with depression” outcome does not allow clear temporal ordering between depression onset and night shift work. Analyses using recent depressive symptoms (past 7 days), which better align with temporality assumptions, showed largely similar risk estimates for females and males; therefore, sex-stratified findings based on lifetime diagnosis should be interpreted with caution. Second, the temporal spacing of assessments limits our ability to capture the precise timing and latency of mental health effects associated with night shift work, which may manifest over shorter or longer intervals than those assessed between study waves. Third, while the study adjusted for several potential confounders, unmeasured variables, such as the occupational environment (i.e., lighting, temperature, noise levels, break areas), type of work (i.e., physical demands, cognitive load, autonomy, safety-critical roles), individual coping mechanisms (i.e., sleep hygiene, nutrition, exercise, social support, the chronotype of participants, stress management), the duration of night shift work or other factors that may influence the deleterious effects of night shifts, may still influence the observed associations. In addition, although urbanicity was available at earlier waves, it was not included because it was not measured at Wave V and may have changed substantially over time. To ensure consistency and temporal comparability across covariates, we restricted adjustment to variables measured at Wave III. Furthermore, although smoking behavior was positively associated with mental health outcomes, its inclusion in sensitivity analyses did not materially change the RR estimates for night shift work and therefore it was not retained in the final models. Fourth, shift work exposure was self-reported and assessed using predefined categories. In the Add Health questionnaire, the category “rotating shift” includes schedules that may rotate between day and evening shifts and/or include night shifts, without further distinction. Therefore, some participants classified as rotating shift workers may not have been exposed to night work. This potential non-differential misclassification could have attenuated the observed associations, biasing results toward the null. Finally, the generalizability of our findings may be limited to similar populations, as the study sample was from the U.S. workforce and predominantly White and relatively young.
Future studies should explore the mechanisms underlying the sex differences observed in this study and identify which workers are most vulnerable to shift work-related health issues. Research could also examine the impact of interventions aimed at mitigating the mental health risks of night shift work. Prior work has emphasized a multi-level approach to fatigue risk management, including work scheduling strategies that ensure adequate opportunities for sleep, training and educational programs to support effective use of recovery time, and organizational or technological measures to detect and manage fatigue-related risks (Wong et al., 2019). Additionally, investigating whether individuals with an eveningness chronotype, those who naturally prefer later hours, experience the same negative effects of night shift work as those with a morningness chronotype could be crucial. Understanding the role of circadian preference as a moderator in the relationship between shift work and mental health would be a particularly valuable area of study. Furthermore, more research is needed to understand the long-term mental health effects of night shift work across different demographic groups and occupational settings.
Implications for Occupational Health Practice
Our study highlights the significant association between night shift work and mental health conditions, with women particularly at risk. These findings underscore the need for screening, targeted interventions and workplace policies to address the mental health challenges faced by night shift workers, considering sex-specific factors and occupational contexts. Given the increasing prevalence of non-standard work schedules in modern economies, it is imperative that employers and policymakers take proactive steps to safeguard the mental well-being of these workers.
Applying Research to Occupational Health Practice
This study highlights the long-term mental health risks associated with night shift work, particularly among women. Over a 17-year follow-up, women who worked night shifts showed a higher risk of suicidal ideation and depression compared with women who worked regular daytime shifts. In addition, night shift work was associated with specific depressive symptoms in both men and women: feeling unhappy and being unable to shake off the blues in men, and feeling sad and being unable to shake off the blues in women. These findings emphasize the importance of integrating mental health screening and support programs for night shift workers. Occupational health professionals should advocate for workplace interventions, including flexible scheduling, mental health resources, and stress management strategies tailored to shift workers. Given the sex-specific differences observed, a gender-sensitive approach is essential in developing policies to protect workers’ mental well-being. Addressing these risks proactively can improve employee health, reduce absenteeism, and enhance overall workplace productivity.
Footnotes
Author Contributions
MR-P contributed to the conceptualization, methodology, and wrote the original draft. AG-H was responsible for data curation, formal analysis, and supervision. JFL-G also assisted with data curation and contributed to the review & editing process. JP-H contributed to the methodology. CR-D contributed to the review & editing. RY-S contributed to the conceptualization. YE contributed to the conceptualization and the review & editing, and supervision.
Conflict of Interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The National Longitudinal Study of Adolescent to Adult Health (Add Health study) was approved by the Institutional Review Board (IRB) at the University of North Carolina at Chapel Hill. The permission to conduct secondary analyses was obtained by the Ethics Committee of the University Hospital of Navarra (PI_2020/143).
Availability of Data and Materials
Due to our data protection agreements with the participating cohort study, we are unable to share individual-level data with third parties. According to Add Health’s data access policy, researchers can submit data requests to the steering committee. These requests will be reviewed promptly for confidentiality, data protection, and intellectual property considerations, and will not be unreasonably denied. Researchers registered with Add Health can apply for access to its database by submitting an application (![]() ).
).