
Abstract
Background:
The aim of this study is to investigate the relationship between various types of burnout, coping strategies, and resilience among healthcare professionals through a transactional model of stress and coping framework.
Methods:
A sample of healthcare professionals (HCPs; N = 647) from various hospitals across China responded to an online questionnaire survey, and Partial Least Squares Structural Equation Modeling (PLS-SEM) was used to test the proposed interaction model.
Results:
Emotional exhaustion and reduced personal accomplishment negatively predicted resilience, while depersonalization positively predicted resilience. Emotional exhaustion and depersonalization positively predicted emotion-oriented strategies, and depersonalization negatively predicted problem-oriented strategies. Reduced personal accomplishment negatively predicted problem-oriented and avoidance-oriented strategies. Emotion-oriented strategies negatively predicted resilience, while problem-oriented and avoidance-oriented strategies positively predicted resilience. Mediation analysis revealed that emotion-oriented strategies significantly mediated the relationships between emotional exhaustion, depersonalization, and resilience; avoidance-oriented strategies significantly mediated the relationships between depersonalization, reduced personal accomplishment, and resilience; and problem-oriented strategies mediated the relationships between reduced personal accomplishment and resilience.
Conclusions/Applications to Practice:
The conclusions of this study may enhance the effectiveness of interventions for HCPs by providing insights into the specific effects of different burnout coping strategies. Particular attention should be given to HCPs experiencing a high level of reduced personal accomplishment burnout, and interventions for this subtype should emphasize problem-oriented strategies and the moderate adoption of avoidance strategies to best promote resilience.
Introduction
Healthcare professionals (HCPs) worldwide are experiencing burnout at increasing frequency and severity (Yue et al., 2022). Research has found that the rate of burnout among HCPs is approximately twice that of the general population, and this negative psychological state persists throughout their careers (Grow et al., 2019). A survey by the British Medical Association (2019) revealed that 80% of doctors in the United Kingdom were at high or very high risk of burnout, while a recent study in China has reported that 65.8% of HCPs have experienced burnout related to their work (Yin et al., 2023).
Burnout among HCPs not only negatively impacts their physical and mental health but also exacerbates the burden on the healthcare system. Some studies have found that burnout makes HCPs more prone to anxiety and depression (Grow et al., 2019), increases their turnover intention (G. Chen et al., 2024), and can lead to a higher risk of suicide (Grow et al., 2019). Previous research has also indicated that HCPs with a higher level of burnout exhibited poorer attitudes toward patients and had less effective communication with them (Argentero et al., 2008). As a result of the impact of HCP burnout on patient treatment outcomes, the likelihood of medical errors has been found to increase, leading to more malpractice claims and additional healthcare costs for medical institutions (Grow et al., 2019). In the United States, the annual cost associated with physician turnover and reduced clinical hours due to burnout has been estimated to be about $4.6 billion (Han et al., 2019).
In light of the serious effects of severe burnout among HCPs, more effective measures to enhance HCPs resilience, to help them better combat burnout and maintain their overall well-being are essential (Baskin & Bartlett, 2021; Dossett et al., 2021). The Transactional Model of Stress and Coping (TMSC) provides an insightful theoretical framework for exploring how HCPs cope with burnout to maintain their resilience. According to the TMSC, when individuals encounter stressful events or situations, they employ different coping strategies to manage the stress. Their subsequent quality of mental health and adaptability depends on the extent to which they adopt effective coping strategies (Lazarus & Folkman, 1984). By examining the different impacts of the coping strategies HCPs adopted in response to various types of burnout on their resilience, this study extends the application of the TMSC in the field of HCP resilience. Furthermore, this study aimed to identify HCPs preferred coping strategies when facing different types of burnout, in an effort to provide insights for the development of future interventions to help them enhance their resilience in the face of burnout.
Background and Hypothesis Development
The Impact of Burnout on Resilience
Burnout is defined as extreme exhaustion from prolonged work hours and high intensity work situations (Maslach et al., 2001). Healthcare professionals frequently encounter stress related to the healthcare system, as well as experiencing threats to their physical and mental well-being (McGarry & O’Connor, 2024). Factors such as high-pressure administrative management, burdensome digital record-keeping, a culture of perfectionism, and excessive integration of work and life all contribute to increasing HCP burnout (Grow et al., 2019). The person experiencing burnout expresses a hostile or indifferent attitude toward work, lack of empathy, and a diminished sense of work value. Typically this is divided into three dimensions: emotional exhaustion, depersonalization, and reduced personal accomplishment (Maslach et al., 2001). Emotional exhaustion refers to feeling emotionally drained and excessively fatigued due to overwhelming work stress; depersonalization is characterized by a cold and detached attitude toward work-related individuals or colleagues, marked by a loss of empathy and increased feelings of alienation; reduced personal accomplishment refers to a decline in work achievement and efficiency, accompanied by feelings of helplessness and failure (Maslach et al., 1997).
Resilience refers to an individual’s ability to effectively adapt to and recover from stress, challenges, or adversity (Campbell-Sills & Stein, 2007). Research has shown that resilience can significantly enhance HCPs’ ability to cope with setbacks and difficulties in their work, allowing them to handle the psychological impacts and stress caused by negative occupational events more calmly (Dossett et al., 2021).
Burnout is widely recognized as a significant factor that undermines resilience among HCPs, with studies indicate that high levels of burnout negatively impact HCPs’ capacity to adapt to stress and recover from challenges, diminishing their overall resilience (Montgomery & Patrician, 2022). Research findings have shown that a high level of emotional exhaustion can decrease HCP resilience, reducing their ability to cope with stress. For example, Fiabane et al. (2021) found that emotional exhaustion was associated with lower resilience among Italian HCPs, making them more likely to feel fatigued and helpless when facing stress, thus weakening their ability to recover. On the other hand, depersonalization, although it can be considered a defense mechanism for HCPs to cope with work-related stress (Moradi et al., 2021), often diminishes their perceived professional support, making it more difficult for HCPs to adapt to work-related stress, thereby reducing their resilience (Bredicean et al., 2021). Previous studies have also shown that reduced personal accomplishment is associated with lower HCP resilience (Zhang et al., 2021), as a decline in personal accomplishment may decrease HCPs’ self-efficacy and confidence, further lowering their resilience. Therefore, based on the above research evidence, the following hypotheses were proposed:
Coping With Burnout for Resilience: A TMSC Perspective
According to the TMSC, stress is a dynamic interaction between individuals and their environments, assessed as depleting or exceeding the existing coping resources of the individual, thereby endangering their well-being (Lazarus & Folkman, 1984). When these resources are insufficient, stress may manifest as burnout, a common response to prolonged work-related stress. The TMSC further explains that individuals faced with stress engage in a cognitive appraisal of whether the stressor poses a significant threat to them and whether they have coping resources available, and based on the results of this assessment, they will adopt corresponding strategies to cope with the stress (Lazarus & Folkman, 1984). The coping process of individuals is defined as one’s cognitive and behavioral efforts to manage internal or external demands perceived as exceeding personal capacities (Lazarus & Folkman, 1984). Previous research has shown that coping strategies are a crucial protective factor for resilience, and successful coping patterns enhance individuals’ adaptability to withstand adversity (Wright & Masten, 2005). Endler and Parker (1999) have identified three coping strategies that people use when faced with stressful situations: problem-oriented, which centers on solving the encountered problem; emotional-oriented, which concentrates on the emotions caused by specific issues (such as anxiety or anger); and avoidance-oriented, which involves attempting to avoid the problem.
When HCPs experience burnout in the workplace, they may adopt various coping strategies to alleviate their burnout and psychological stress, and to help them better adapt to their environment. Research increasingly suggests that HCP burnout is associated with specific coping strategies, and that resilience can be considered a positive psychological outcome of adopting effective burnout-coping strategies. HCPs experiencing one of the three aforementioned types of burnout—emotional exhaustion, depersonalization, and reduced personal accomplishment—tend to adopt emotion-oriented coping strategies rather than problem-oriented strategies (Howlett et al., 2015). Masiero et al. (2018) found that emergency department HCPs experiencing emotional exhaustion and a sense of professional inefficacy are more inclined to adopt avoidance-oriented strategies. Similarly, SunnyHu and Cheng (2010) showed that individuals with emotional exhaustion, depersonalization, and reduced personal accomplishment burnout types are more likely to employ avoidance-oriented coping strategies. Meanwhile, some studies have indicated that the different coping strategies of HCPs may have varying impacts on their resilience. For example, problem-oriented coping strategies can positively predict resilience among Alzheimer’s caregivers, whereas emotion and avoidance strategies may negatively affect their resilience (Wilks et al., 2011). Avoidance-oriented strategies used by cancer nurses are associated with lower levels of resilience (Cadorin et al., 2024), while problem-oriented coping among Romanian doctors during the COVID-19 pandemic was confirmed to positively predict resilience (Crișan et al., 2024).
Still, few studies to date have explored the relationships between the different types of burnouts, different coping strategies, and resilience among HCPs. A deeper understanding of these relationships is crucial for the development of more targeted interventions to better maintain the psychological health of HCPs. Based on the existing literature, then, this study proposed the following hypotheses:
The Study
The aim of this study is to investigate the relationships between different types of burnout, coping strategies, and resilience among HCPs.
Ethical Considerations
All research procedures in this study were approved by the institutional IRB of the Academic Committee of Beijing Hospital of Traditional Chinese Medicine, Capital Medical University (Approval Number: 2024BL02-017-01). All participants provided their informed consent, and retained the right to withdraw from the study at any time. This study implemented strict measures to protect participants’ privacy and the confidentiality of their data, with all data collected in this study anonymized.
Methodology
Design
An online cross-sectional survey was conducted from January to March 2024, targeting HCPs from various hospitals across China.
Data Collection
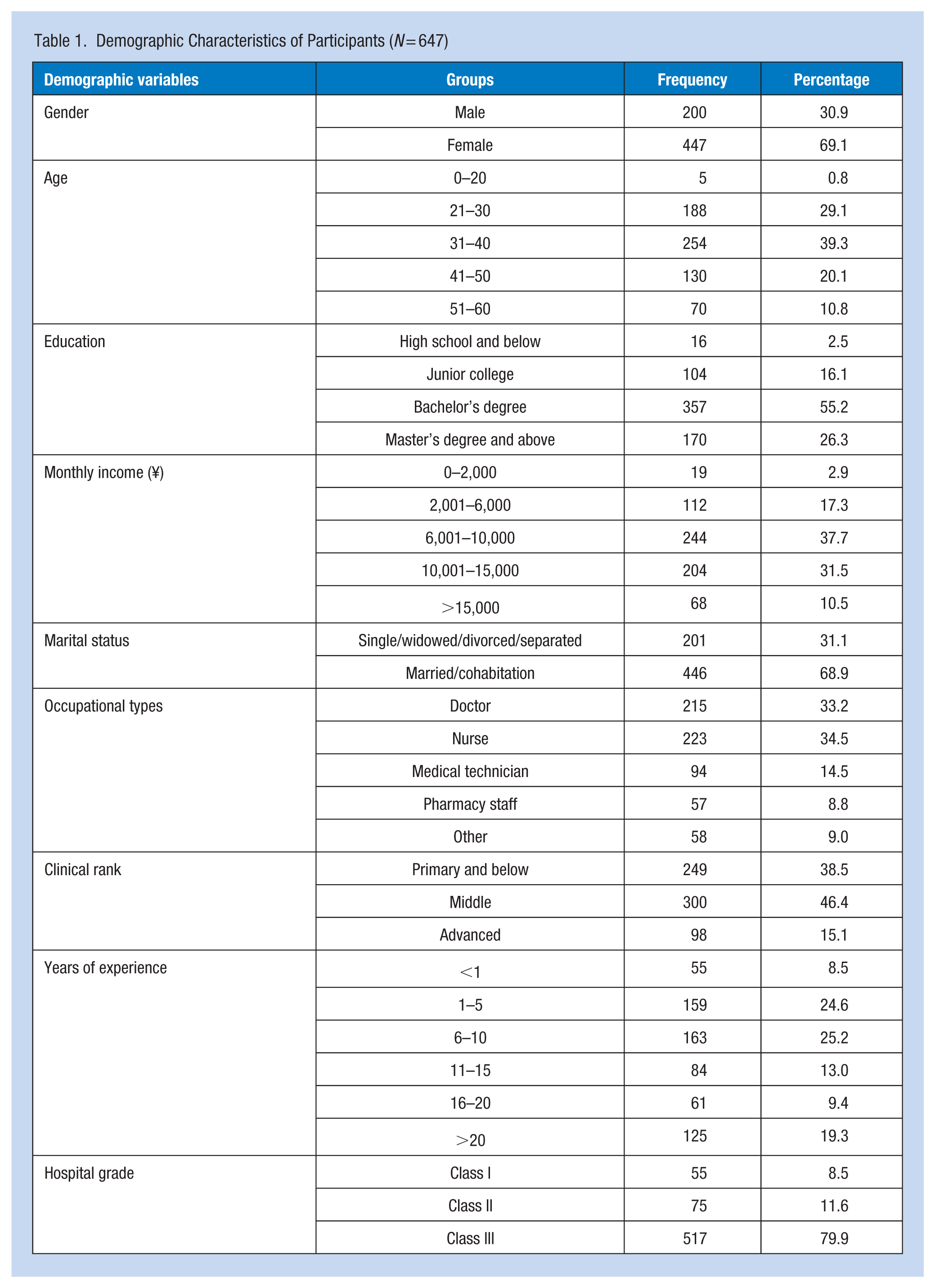
A snowball sampling method was used to recruit a sample of HCPs from various grades of hospitals in China to respond to the online questionnaire survey developed for this study. The sample of HCPs included doctors, nurses, and medical technicians. All participants agreed freely to participate in the study and sign an informed consent form before completing the survey. Involuntary participants, non-medical professionals, and those who had left the medical profession were excluded from the study sample. The online questionnaire system incorporated a program to prevent duplicate responses, to further ensure the accuracy of our research data. In the end, based on the inclusion and exclusion criteria, 647 valid questionnaires were retained for further analysis, accounting for 89.95% of all returned questionnaires. Detailed participant characteristics are shown in Table 1.
Demographic Characteristics of Participants (N = 647)
Measures
Burnout was measured using the Maslach Burnout Inventory (Maslach et al., 1997). This instrument consists of 22 items which assess the three core dimensions of burnout: Emotional exhaustion, depersonalization, and reduced personal accomplishment. Responses are rated on a 7-point Likert scale, ranging from 1 (never) to 7 (every day). Emotional exhaustion is measured using nine items, such as, “I feel emotionally drained by my work” (Cronbach’s α = .838); depersonalization is measured using five items, such as, “I’ve become more insensitive to people since I took this job” (Cronbach’s α = .899); Reduced personal accomplishment (RPA) is measured using eight items, such as, “I look after my patients’/clients’ problems very effectively” (Cronbach’s α = .846). According to Maslach et al. (1997), a higher score on the original personal accomplishment subscale indicates a lower level of burnout. Therefore, this subscale was reverse-coded in this study so that higher scores represented a greater reduced personal accomplishment.
Coping strategies were measured using the Coping Inventory for Stressful Situations-short form (CISS-21; Endler & Parker, 1999). This instrument includes three subscales: emotion-oriented, avoidance-oriented, and problem-oriented coping strategies. Responses are rated on a 5-point Likert scale ranging from 1 (never) to 5 (always), with higher scores indicating a greater tendency to adopt the corresponding coping strategy. Emotion-oriented is measured with seven items, such as, “Blame myself for having gotten into this situation” (Cronbach’s α = .867); avoidance-oriented is measured with seven items, such as, “Take some time off and get away from the situation” (Cronbach’s α = .851); and problem-oriented is measured with seven items, such as, “Focus on the problem and see how I can solve it” (Cronbach’s α = .926).
Resilience was measured using the Connor-Davidson Resilience Scale (Campbell-Sills & Stein, 2007). This scale consists of 10 items (e.g., “Able to adapt to change”) and uses a 5-point Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree). Higher overall scores indicate a higher level of resilience. In this study, the Cronbach’s α for this scale was .946.
This study also collected demographic information on HCPs’ gender, age, education, monthly income, marital status, clinical rank, years of experience, and hospital grade, which were all considered as control variables.
Data Analysis
SmartPLS 4.1 software was used to perform partial least squares structural equation modeling (PLS-SEM) for the data analysis and model testing. In this study, the PLS-SEM algorithm was employed to test the reliability and validity of the measurement instruments, and the bootstrapping procedure was used for path analysis and mediation effect testing. Following Hayes’ (2009) recommendations, bootstrapping was repeated at least 5,000 times during mediation path testing, and a 95% confidence interval (CI) for the indirect effect that did not include zero indicated the presence of a mediation effect.
Results
Common Methods Bias (CMB)
Considering the potential risk of common method bias (CMB) in self-reported cross-sectional surveys, this study employed Harman’s single-factor analysis to test for the presence of CMB. The results showed that the first factor explained 14.78% of the total variance, which is below the acceptable threshold of 50% (Hair et al., 2019). Additionally, the results from the multicollinearity diagnostics revealed that the variance inflation factor for all measured items in this study did not exceed 5 (Hair et al., 2019). These findings suggest that CMB was not present in this study.
Validity and Reliability
Analysis results indicated that the Cronbach’s α, Dijkstra-Henseler’s ρA, and composite reliability for the instruments in this study all exceeded 0.7, suggesting that the internal reliabilities of the research tools were satisfactory. Additionally, the factor loadings for all items surpassed the expected value of 0.7, and the average variance extracted (AVE) ranged from 0.525 to 0.713, exceeding the acceptable threshold of 0.5 (Hair et al., 2019). These findings confirmed the convergent validity of the measurement instruments.
The study employed the Heterotrait-Monotrait (HTMT) ratio to evaluate the discriminant validity of the instruments. Results showed that the HTMT ratios ranged from 0.211 to 0.73, with all below the threshold of 0.85 (Henseler et al., 2015). Furthermore, according to the Fornell-Larcker criterion, Table 2 shows that the correlation coefficients between any two variables in this study were all below 0.8, and the square roots of the AVEs for all variables were greater than the correlation coefficients between the variables (Henseler et al., 2015). These findings indicated that the measurement instruments all passed the discriminant validity test.
The Square Root of the AVE and Correlation Coefficient Between Variables
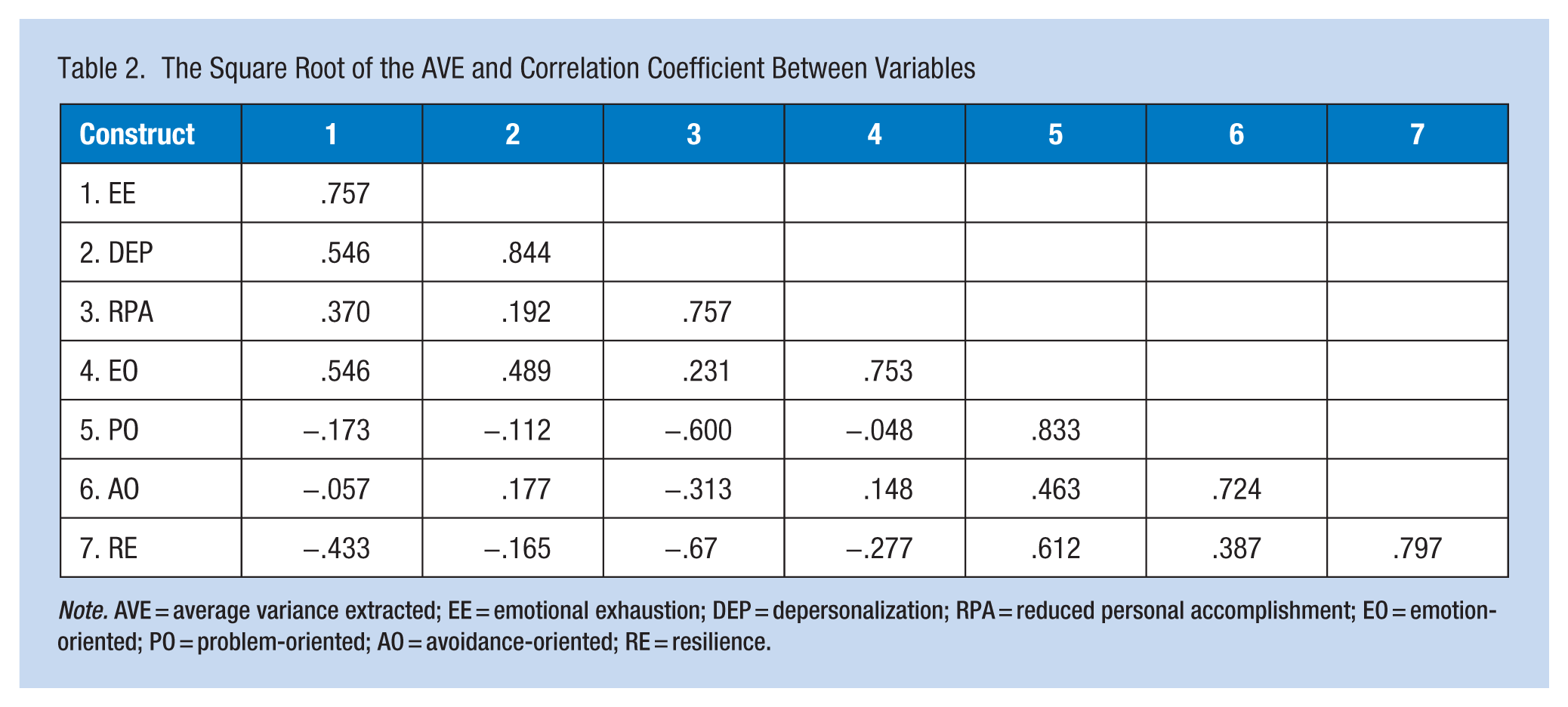
Note. AVE = average variance extracted; EE = emotional exhaustion; DEP = depersonalization; RPA = reduced personal accomplishment; EO = emotion-oriented; PO = problem-oriented; AO = avoidance-oriented; RE = resilience.
Path Analysis
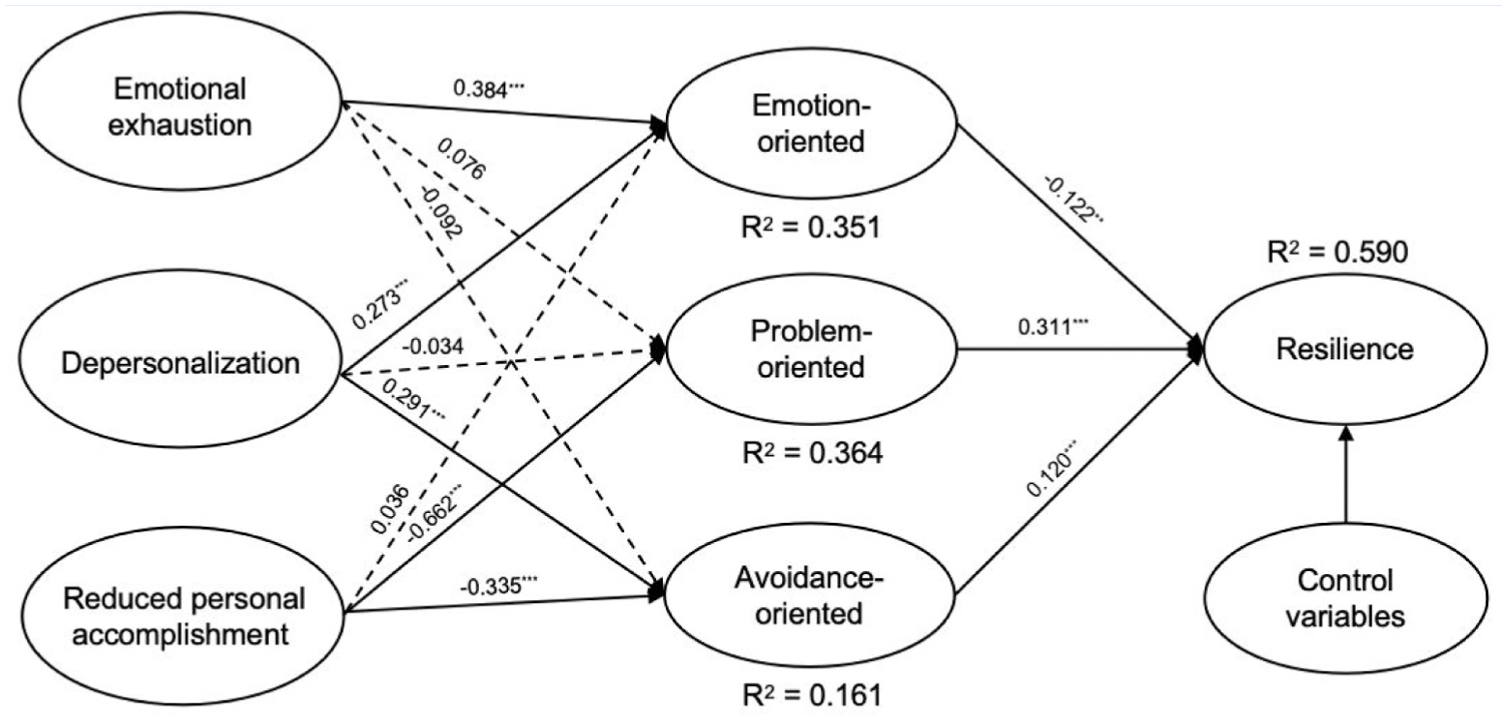
Table 3 and Figure 1 show the results of the model path analysis, which indicated that emotional exhaustion (β = −.231, p < .001) and reduced personal accomplishment (β = −.352, p < .001) negatively predicted resilience, while depersonalization (β = .102, p < .001) positively predicted resilience. Thus, H1a and H1c were supported, while H1b received contradictory support. Additionally, emotional exhaustion positively predicted emotion-oriented strategies (β = .384, p < .001), and depersonalization positively predicted both emotion-oriented strategies (β = .273, p < .001) and avoidance-oriented strategies (β = .291, p < .001). Reduced personal accomplishment negatively predicted both problem-oriented strategies (β = −.622, p < .001) and avoidance-oriented strategies (β = −.335, p < .001). Thus, H2a, H2b, and H3b were supported, while H3c and H4c received contradictory support. Emotion-oriented strategies negatively predicted resilience (β = −.122, p = .003), while problem-oriented strategies (β = .311, p < .001) and avoidance-oriented strategies (β = .120, p < .001) positively predicted resilience. Thus, H5a and H6 were supported, while H5b received contradictory support.
Results of Hypothesis Tests
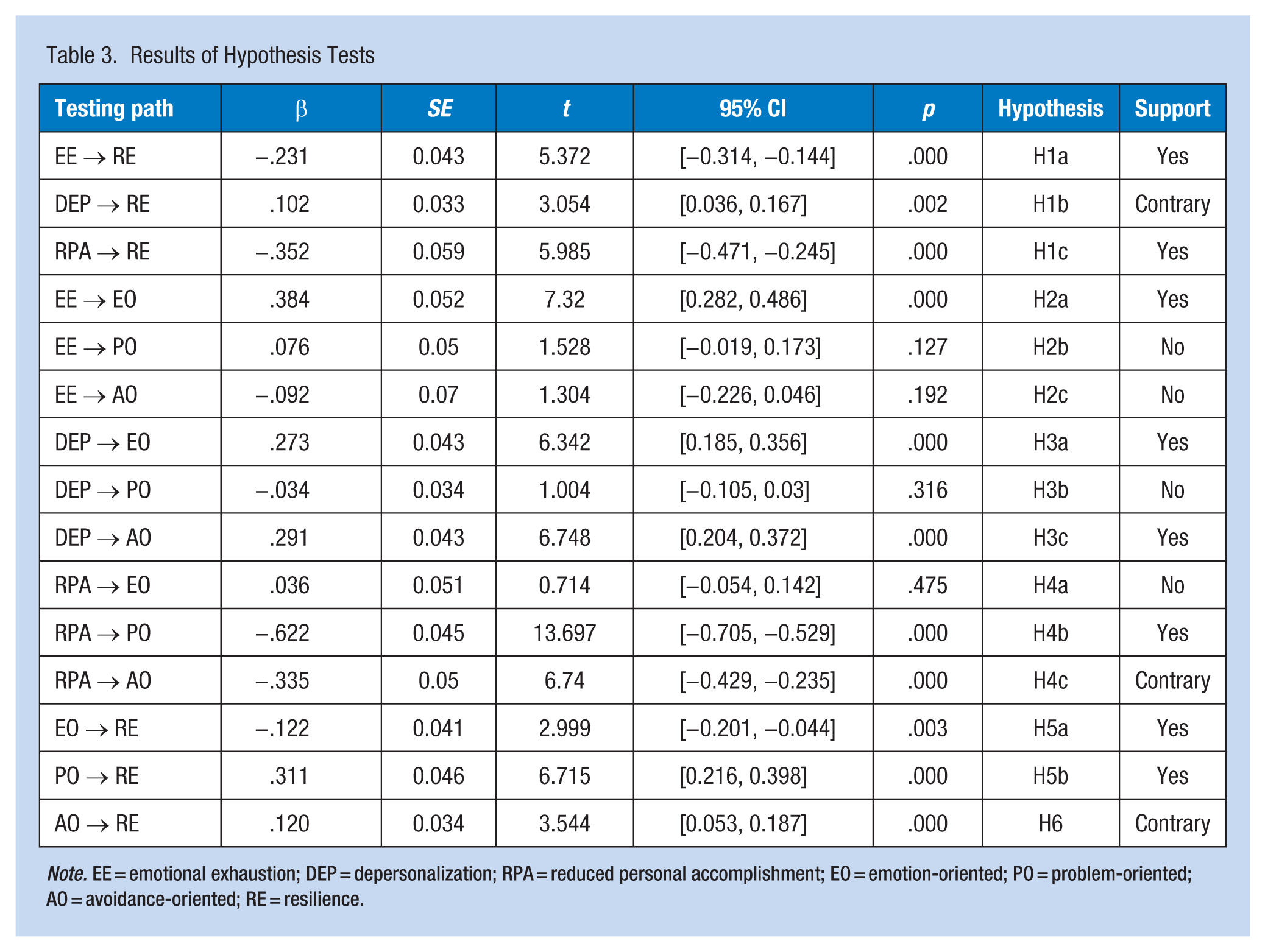
Note. EE = emotional exhaustion; DEP = depersonalization; RPA = reduced personal accomplishment; EO = emotion-oriented; PO = problem-oriented; AO = avoidance-oriented; RE = resilience.
Results of hypothesis tests
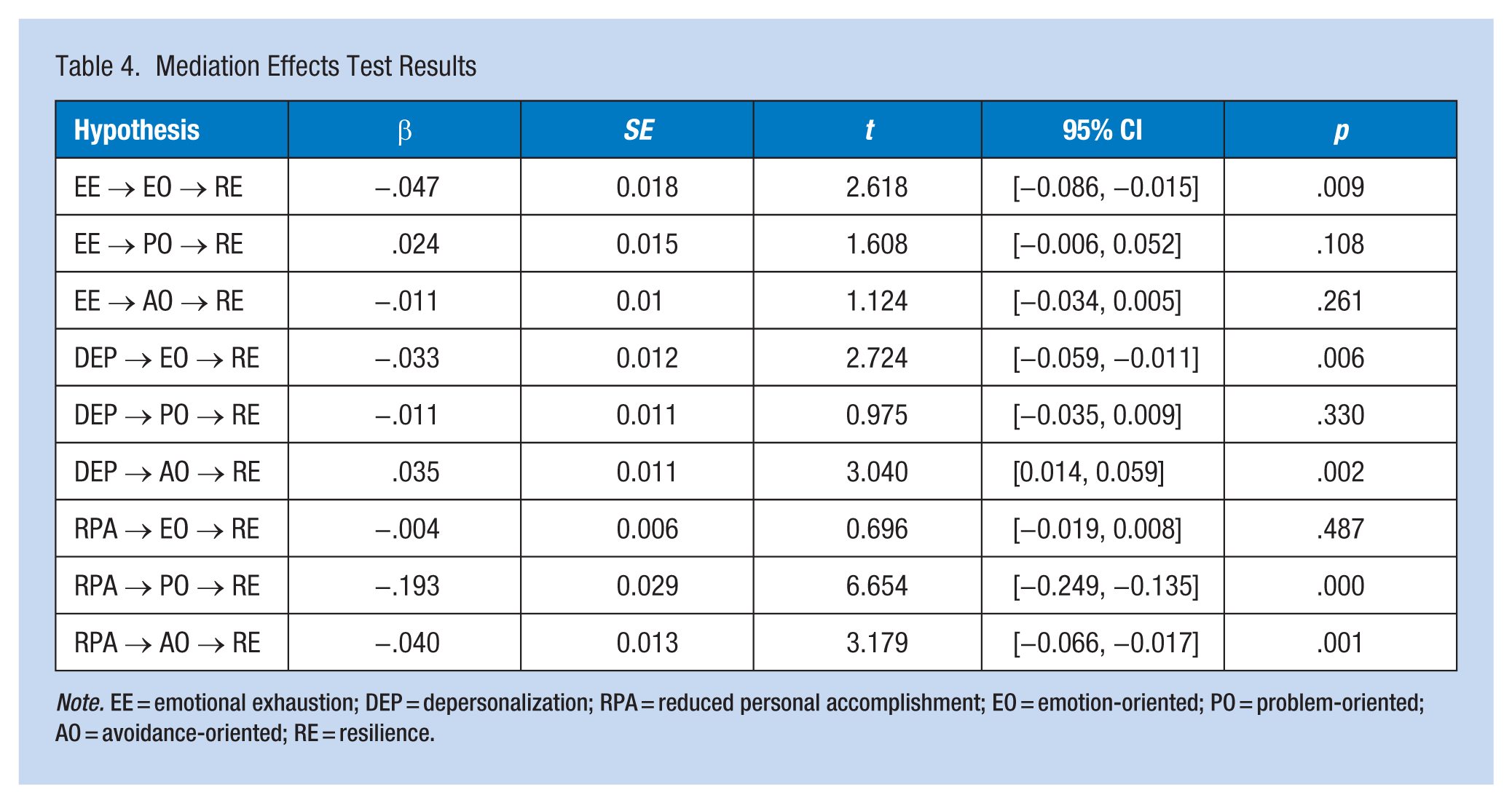
The results of the mediation effects analysis (see Table 4), revealed that emotion-oriented strategies significantly mediated the relationship between emotional exhaustion (β = −.047, 95% CI [−0.086, −0.015], p = .009), depersonalization (β = −.033, 95% CI [−0.059, −0.011], p = .006), and resilience, respectively. Avoidance-oriented strategies significantly mediated the relationship between depersonalization (β = .035, 95% CI [0.014, 0.059], p = .002), reduced personal accomplishment (β = −.040, 95% CI [−0.066, −0.017], p = .001), and resilience, respectively. Problem-oriented strategies (β = −.193, 95% CI [−0.249, −0.135], p < .001) mediated only the relationship between reduced personal accomplishment and resilience.
Mediation Effects Test Results
Note. EE = emotional exhaustion; DEP = depersonalization; RPA = reduced personal accomplishment; EO = emotion-oriented; PO = problem-oriented; AO = avoidance-oriented; RE = resilience.
Discussion
This study is the first to explore the relationships between various types of burnout, coping strategies, and resilience among HCPs. By revealing the roles of different coping strategies within the context of various burnout subtypes and their outcomes in terms of resilience, this study provides insight into how to better support HCP resilience. Using the TMSC model as its theoretical base while considering HCP resilience as a psychological outcome of coping strategies adopted in response to experiencing burnout as they work to maintain balance with their surrounding environment, this study also extends the application of TMSC in the field of resilience research among HCPs. By identifying these complex relationships, this study provides a reference for future research, and contributes to a deeper understanding of how HCPs use different coping strategies to maintain their mental health while working in high-pressure occupational environments.
Emotional exhaustion and reduced personal accomplishment were found to negatively predict resilience, which supported H1a and H1c. These results are consistent with previous research findings that have confirmed that the burnout subtypes of emotional exhaustion and reduced personal accomplishment are negatively associated with resilience among HCPs (Fiabane et al., 2021; Zhang et al., 2021). Contrary to H1b, however, depersonalization positively predicted resilience, which is not consistent with prior findings (Bredicean et al., 2021). It could be that depersonalization, typically manifested as interpersonal and emotional detachment between individuals and their colleagues in a work context, may serve as a self-regulation psychological mechanism for HCPs when faced with work-related stress. The positive correlation between depersonalization and resilience did not imply that depersonalization constitutes a desirable psychological state, but rather revealed it as a short-term adaptive strategy developed by medical staff to preserve resilience amid sustained high-pressure and trauma-exposed healthcare environments. Consequently, this study posits that the state of depersonalization may be regarded as a self-protection mechanism through which healthcare professionals actively reduce the depth of emotional involvement to prevent deeper emotional exhaustion in high-stress work contexts. However, it must be emphasized that persistent depersonalization burnout may further exacerbate interpersonal detachment, resulting in a decline in empathy among HCPs. This may not only weaken their quality of work, it may also negatively impact patient outcomes, and in the long term, this condition becomes detrimental to career development and poses potential risks to HCPs’ physical and mental health. The true value of resilience should be directed toward facilitating recovery and growth under stress, rather than fostering prolonged reliance on emotional detachment. Paradoxically, this positive correlation reveals a complex manifestation of defense mechanisms within healthcare professionals’ resilience under extreme stress, rather than indicating that depersonalization burnout serves as a positive source for resilience maintenance.
The findings also revealed that HCPs experiencing the burnout subtypes of emotional exhaustion and depersonalization tended to use emotion-oriented strategies to cope with burnout, supporting H2a and H2b. Following the dual-process theory (Kahneman & Frederick, 2002), when HCPs are confronted with excessive emotional burden from patients and their families, they may struggle to engage in rational and logical thinking. Consequently, they become more likely to rely on emotional venting or emotional rumination (e.g., overfocusing on negative emotional states such as anxiety or sadness) as burnout coping strategies. Moreover, HCPs experiencing depersonalization burnout often exhibit indifferent and distant attitudes toward their patients and colleagues, which has been considered to be a self-protective behavior (Moradi et al., 2021). This makes them more likely to adopt emotion-oriented strategies, such as self-blame, to cope with burnout. It is possible, however, that when HCPs are continuously exposed to high-intensity work and patients’ suffering, their negative emotions may become difficult to suppress fully. Instead, these negative emotions begin to accumulate subconsciously, leading HCPs to focus inadvertently on these emotions during their self-regulation process. Furthermore, emotion-oriented strategies were found to negatively predict resilience, which supports H5a and is consistent with previous research findings (Wilks et al., 2011). Emotion-oriented coping strategies can potentially cause individuals to focus excessively on their negative emotions, which can lead to further emotional depletion and hindering their ability to cope effectively with adversity (Smith et al., 2016). Mediation analysis further revealed that emotion-oriented strategies significantly mediated the relationships between emotional exhaustion, depersonalization, and resilience. For HCPs experiencing emotional exhaustion and depersonalization burnout subtypes, a higher degree of reliance on emotion-oriented strategies was associated with lower levels of resilience. In short, adopting emotion-oriented burnout coping strategies may have more negative effects on HCPs’ mental health, thereby reducing their resilience.
Additionally, positive correlations were found between depersonalization and avoidance-oriented coping strategies, which supports H3b. HCPs experiencing depersonalization may be inclined to distance themselves from their emotionally-draining work environment, thereby preventing psychological fatigue from excessive emotional involvement, which might explain why HCPs experiencing this type of burnout are more inclined to use avoidance-oriented strategies. However, contrary to previous research conclusions (Cadorin et al., 2024), this study found that avoidance-oriented strategies positively predicted resilience, meaning that H6 received contradictory support. According to the conservation of resources theory (S. Chen et al., 2015), individuals in stressful situations strive to preserve their existing resources to cope with stress. Although avoidance-oriented coping is generally considered a negative strategy, it could, to some extent, prevent the rapid depletion of resources in HCPs, thereby preserving their personal psychological resources in the short term. This resource conservation mechanism may help HCPs reduce their overreactions to external pressures and gradually develop their adaptability and resilience to ongoing stress. Therefore, while avoidance-oriented strategies may not be the most effective long-term coping methods, they may contribute to the enhancement of resilience among HCPs through short-term resource conservation and emotional buffering (Lazarus & Folkman, 1984). Further mediation analysis indicated that avoidance-oriented strategies significantly mediated the relationship between depersonalization and resilience. This suggests that, for HCPs experiencing depersonalization as a burnout subtype, a greater tendency to use avoidance-oriented coping strategies may promote their resilience. Nevertheless, prolonged reliance on avoidance-oriented strategies for stress coping may have potential adverse effects on the overall physical and mental health of healthcare professionals. This is because behaviors aimed at avoiding negative emotions and occupational challenges are not direct means of addressing stressors; rather, they represent a passive defensive mechanism. Excessive dependence on avoidance strategies may gradually erode the foundation of healthcare professionals’ psychological resilience, thereby compromising their overall well-being and professional confidence (Rossi et al., 2023).
Reduced personal accomplishment was shown to be negatively associated with problem-oriented and avoidance-oriented coping strategies, supporting H4b and conversely supporting H4c. It could be that when HCPs experience a higher level of reduced personal accomplishment, their sense of self-efficacy in completing their medical tasks and making a positive impact on patients may decrease, leading them to reduce their use of problem-oriented strategies. Furthermore, the more reduced accomplishment that HCPs experience, the more likely they are to feel a loss of control over their environment, which in turn will lead to either increased adoption of passive coping mechanisms, or a complete abandonment of coping efforts. In other words, HCPs experiencing reduced personal accomplishment may develop a sense of helplessness, leading them to believe that no coping strategy will improve the situation, possibly resulting in them ceasing to take any proactive actions at all, including avoidance strategies. Consistent with previous research (Wilks et al., 2011), problem-oriented strategies were shown to positively predict HCP resilience, which supports H5b. Previous study results have suggested that problem-oriented strategies are associated with a higher sense of control and high levels of self-efficacy, and that these positive beliefs can enhance individuals’ ability to overcome difficulties, thereby promoting their resilience (Peñacoba et al., 2021). In this study, mediation analysis results showed that problem-oriented and avoidance-oriented strategies played significant mediating roles in the relationship between reduced personal accomplishment and resilience. This suggests that HCPs frequently experiencing reduced personal accomplishment burnout may be less inclined to adopt problem-oriented or avoidance-oriented strategies, potentially creating a vicious cycle that continuously diminishes their resilience. The path coefficient of the negative impact of reduced personal accomplishment on HCP resilience was also found to be the largest. These findings suggest that particular attention should be given to the burnout subtype of reduced personal accomplishment among HCPs, as it may lead to more severe psychological consequences. The path coefficient results showed a stronger correlation between reduced personal accomplishment and problem-oriented strategies. Problem-oriented strategies, compared to others, were also shown to be more effective in promoting HCP resilience. This implies that helping HCPs develop problem-oriented strategies to cope with burnout can be crucial for improving their resilience.
Strengths and Limitations of the Study
This study has several strengths and limitations that need to be considered. First, this is the first study to address the relationship between different burnout subtypes, coping strategies, and resilience among HCPs across various grades of hospitals in China, thus enriching the established literature on HCP resilience. Second, this study integrated the TMSC model in its theoretical framework, thereby providing insight into how HCPs cope with burnout to enhance their resilience, which can then contribute to the development of more targeted interventions on HCP burnout. Nevertheless, this study also has some limitations. First, the cross-sectional survey used in this study cannot reveal causal relationships between the variables. Future research should employ longitudinal tracking surveys targeting HCPs to further test the conclusions of this study, and to better understand the long-term effects of various coping strategies. Second, most of the HCPs in this study sample were from tertiary hospitals in China. Since these are the highest-grade hospitals in the country, HCPs working in these hospitals are more likely to endure higher work intensity and stress, which may have enhanced the statistical testing power of the current study model to some extent. Nevertheless, we still recommended that future research adopt more comprehensive and scientific sampling methods (e.g., stratified sampling) to improve the representativeness of the HCP samples. Finally, although this study considered three main strategies for coping with burnout and their impacts on resilience, additional coping strategies (e.g., behavioral and mental disengagement; Carver et al., 1989) and individual characteristic variables (e.g., personality traits) might also influence these relationships. Therefore, future research should explore the effects of additional coping strategies on the relationship between burnout and resilience, as well as the boundary conditions of these relationships.
Implications for Occupational Health Practice
First, emotion-oriented strategies may decrease HCP resilience against experiencing emotional exhaustion and depersonalization. Therefore, HCPs should reduce their reliance on emotion-oriented coping strategies (e.g., excessive focus on negative emotions such as anxiety or anger). Healthcare institutions should provide support in terms of emotional management and regulation techniques to help HCPs identify and manage their negative emotions. For example, cognitive behavior therapy or establishing social support networks could help HCPs develop more effective coping mechanisms and alleviate emotional stress. Second, for HCPs experiencing depersonalization burnout subtypes, avoidance-oriented coping strategies may help them increase their resilience to some extent. As prior research has indicated that avoidance-oriented coping strategies only offer short-term benefits (Smith et al., 2016), the moderate adoption of avoidance-oriented strategies should be encouraged to help HCPs enhance their resilience. For instance, hospitals could develop more scientific time management and work adjustment plans, such as work rotation or more appropriate vacation arrangements, to help HCPs avoid excessive stressors and reduce burnout. Finally, HCPs with higher levels of reduced personal accomplishment may be less likely to adopt positive coping strategies to deal with burnout, suggesting the importance of focusing on this particular burnout subtype moving forward. Furthermore, problem-oriented strategies were found to have the most positive effect on maintaining resilience. Therefore, healthcare organizations should offer HCPs experiencing reduced personal accomplishment additional resources and support, and focus on helping them cope with burnout more effectively, especially by strengthening problem-oriented strategies to avoid long-term burnout cycles. The provision of more specialized training courses and team collaboration platforms for HCPs can help encourage them to share problem-solving experiences. Additionally, managers should regularly provide positive feedback and recognition to HCPs, to help them feel a sense of professional value and achievement and thereby strengthen their resilience.
Applying Research to Occupational Health Practice
This study, grounded in the transactional model of stress and coping, explored how various coping strategies, as employed by HCPs experiencing different burnout subtypes, influence resilience. The conclusions of this study may enhance the effectiveness of interventions for HCPs by providing insights into the specific effects of different burnout coping strategies. Particular attention should be given to HCPs experiencing a high level of reduced personal accomplishment burnout, and interventions for this subtype should emphasize problem-oriented strategies and the moderate adoption of avoidance strategies to best promote resilience.
Footnotes
Acknowledgements
The authors are grateful to all participants in this study, as well as to the medical administrator working in hospitals who were involved for assistance.
Conflict of Interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Humanities and Social Sciences Youth Foundation, Ministry of Education of China (No. 20YJCZH010) awarded to Shuang Chen; Tsinghua University Initiative Scientific Research Program (No. 2024THZWWH02) awarded to Shuang Chen; Tsinghua Lab Research Program on Computational Communication and Intelligent Media (No. 2026TSJCLAB001) awarded to Shuang Chen; Tsinghua University Undergraduate Education Innovation Grants (No. DX08_06) awarded to Shuang Chen.
Ethical Approval Statement
Research ethics approval was obtained by the Academic Committee of Beijing Hospital of Traditional Chinese Medicine, Capital Medical University in 2024, and the ethical review approval number is: 2024BL02-017-01.
Consent to Participate
Informed consent was obtained from all individual participants included in the study.
Consent to Publish
Not applicable. This study does not include data from individual persons (including individual details, images, or videos etc.).
Data Availability Statement
Data are available upon request from the corresponding author.*