
Abstract
Background:
It is well known that healthcare workers experience poor outcomes associated with workplace stress and secondary trauma from on-the-job events. In order to respond, healthcare systems must evolve. Yet it is unknown how trauma-informed approaches (TIAs) may effectively address system-level factors within healthcare settings. The aim of this study was to: (1) map out the existing knowledge about TIAs integrated within healthcare organizations and (2) map out the reported health impact of TIA integration on healthcare workers.
Methods:
A scoping review was conducted using Fink’s five-step approach for systematic reviews, with scoping review modifications based on Joanna Briggs Institute guidelines.
Results:
A total of 6,162 participants from 17 articles published between 2018 and 2024 were included in the retained sample. Key findings indicate: (1) TIA support for healthcare workers is insufficient, necessitating systemic organizational change led by effective leadership, and; (2) TIA integration may protect healthcare workers from trauma and burnout, fostering resilience and well-being.
Conclusion:
TIAs within healthcare were associated with well-being among healthcare workers. Leadership plays an integral role in establishing trauma-informed organizational climates. Further work must be conducted with a large sample of healthcare workers to explore the perceived impact of trauma-informed system-level efforts aimed at promoting hospital staff’s well-being.
Keywords
Trauma is an event or circumstance resulting in physical, emotional, or life-threatening harm (Substance Abuse and Mental Health Services Administration [SAHMSA], 2014). Frequent exposure to distressing and traumatic situations such as human suffering, death, disease, and violence, places healthcare workers (HCWs) at a disproportionate risk for secondary trauma and adverse mental health consequences (National Institute for Occupational Health and Safety, 2022; Yu et al., 2022). Nearly 38% of HCWs reported experiencing post-traumatic stress disorder, 47.5% reported secondary traumatic stress, and up to 80% reported developing vicarious trauma and compassion fatigue due to prolonged exposure to traumatic events (Data|CBHSQ, 2000; Hendrickson et al., 2022; Orrù et al., 2021; SAMHSA, 2023). This cumulative trauma can lead to the experience of chronic stress, severe burnout, and untreated anxiety and can exacerbate trauma-related symptoms and disorders (Jun et al., 2021; Xue et al., 2023). In addition to these negative outcomes for HCWs, other consequences include negative job performance, workplace attrition, decreased patient safety, and reduced quality of patient care (Jun et al., 2021; Xue et al., 2023). Despite numerous efforts to combat poor mental health and burnout among HCWs, their limited impact highlights the need for healthcare organizations to address systemic issues at an organizational level (Bright et al., 2023). In 2022, the U.S. Surgeon General placed a call to action for systems-oriented, organizational-level solutions targeting burnout and building healthy workforces (Office of the Surgeon General, 2022).
Trauma-Informed Approaches Integrated Within Healthcare Organizations
Healthcare settings encompass the wide range of environments in which healthcare services are delivered, including acute care hospitals, physician offices and primary care clinics, urgent care centers, rehabilitation facilities, nursing homes and other long-term care facilities, specialized outpatient services, ambulatory surgery centers, and community- or home-based care sites (Christensen & Fagan, 2019). HCWs are those who deliver care and services to clients either directly, such as nurses, doctors, and nurse assistants, or indirectly, through administrative roles, leadership positions, and educators. The Trauma-Informed Approach (TIA) is a framework designed to understand, recognize, and respond to the effects of trauma on individuals, including HCWs, and provides the foundation for establishing trauma-informed organizational climates. TIA is guided by six key principles: safety; trustworthiness and transparency; peer support; collaboration and mutuality; empowerment; and recognition of cultural, historical, and gender issues that support individuals who have experienced trauma (SAMHSA, 2014).
An umbrella review of 14 systematic reviews across educational, social service, behavioral health, and criminal justice settings found that trauma-informed approaches are associated with improvements in patient functioning, service quality, and access, as well as staff safety and burnout. However, the overall evidence-base remains mixed and of low methodological quality (Mahon, 2024). The review also identified 62 different trauma-informed frameworks and models that varied in how they were defined, what components they included, how they were implemented, and how outcomes were measured. These inconsistencies limited the ability to draw definitive conclusions about effectiveness (Mahon, 2024). Nevertheless, evidence from other human service sectors suggests that TIA integration may improve workforce well-being, reduce burnout and secondary traumatic stress, and enhance organizational culture, highlighting its potential relevance for healthcare settings (Mahon, 2024; SAMHSA, 2014).
While the TIA framework outlines key principles for establishing a trauma-informed organizational climate (SAMHSA, 2014), the specific ways these principles are put into practice within healthcare systems remain poorly defined. As a result, we still do not fully understand the extent to which TIAs impact HCWs. These findings further highlight the critical importance of conducting this scoping review so we can better understand the application of TIAs in healthcare settings and the impact on HCWs. As to our knowledge, no literature reviews have been conducted on this topic to date.
Purpose
This scoping review addresses two research questions:
What is known about the integration of TIAs within healthcare organizations?
What is the health impact of TIA integration on HCWs?
Contribution to Nursing Science
Understanding the health impact of TIAs within healthcare organizations may cultivate positive system-level changes benefiting HCWs. A comprehensive understanding of TIAs and the health impact may provide a foundation for establishing supportive work environments that contribute to the overall well-being of HCWs affected by work-associated stress and trauma. The experience of trauma among HCWs and the resulting mental and physical health consequences are a serious issue which impact not only patients, but the U.S. Healthcare System overall, and requires a systemic, organizational-level strategy (Menschner & Maul, 2016; Sutton et al., 2022).
Methods
A scoping review was selected to address key gaps in the literature related to TIAs in healthcare organizations. Current evidence is limited by a lack of synthesis of TIA implementation and outcomes in healthcare settings, variability in how TIAs are defined and operationalized, and limited understanding of their impact on healthcare workers’ well-being, role stress, and burnout. A scoping review is appropriate for mapping existing evidence, clarifying concepts, and identifying gaps in emerging fields (Munn et al., 2018). Consistent with scoping review methodology, no formal quality assessment was conducted, as the primary aim was to characterize the breadth of existing literature rather than evaluate study quality (Grant & Booth, 2009).
Inclusion and Exclusion Criteria
The inclusion criteria were peer-reviewed articles that: (1) were written in English, (2) discussed TIAs within a healthcare organization, (3) addressed the health impact of TIAs on HCWs and (4) were published between 2018 and 2024 to provide current literature while capturing pre-and-post Covid-19 pandemic studies. The review initially covered articles from the past 5 years; however, the timeframe was extended by an additional year to incorporate updates made during the manuscript revision process (2018–2024). The primary screening tool was developed to support implementation (Table 1).
Primary Screening Tool
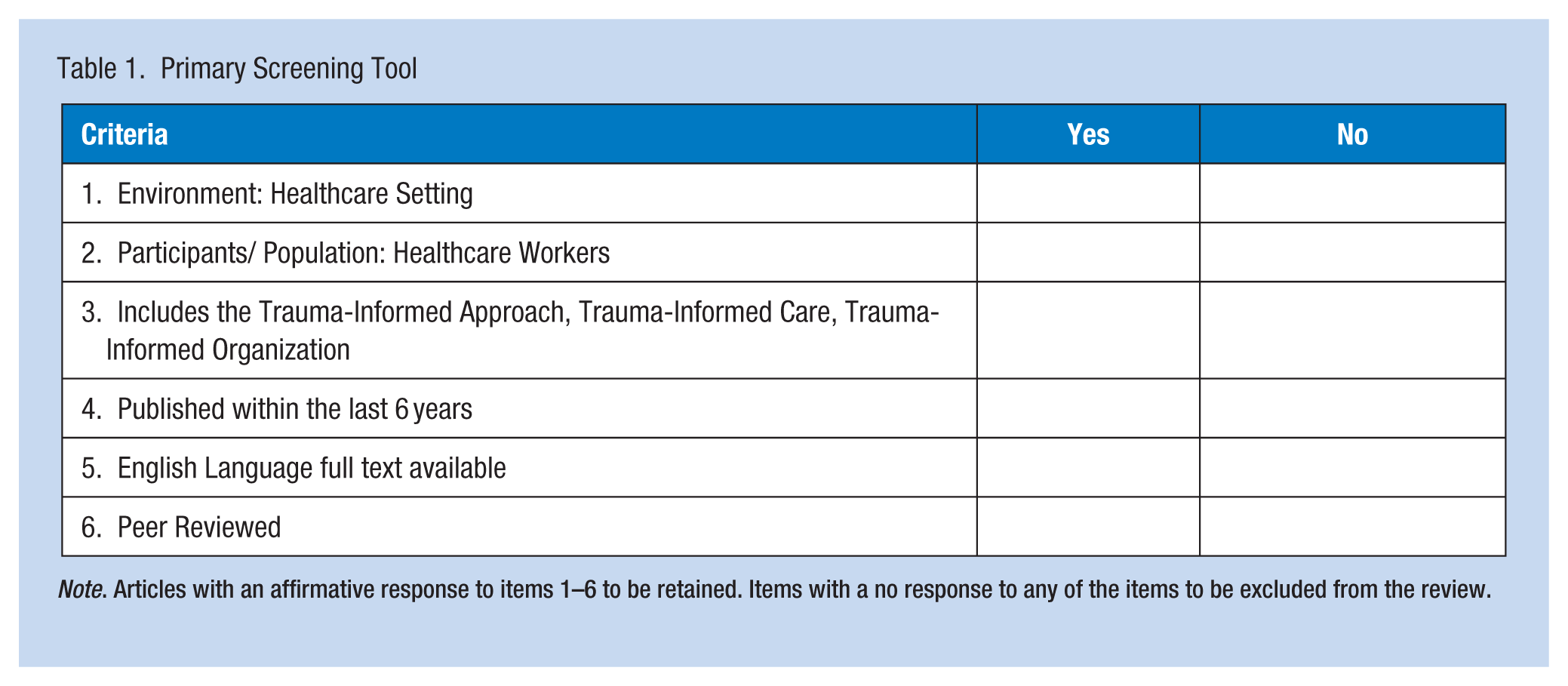
Note. Articles with an affirmative response to items 1–6 to be retained. Items with a no response to any of the items to be excluded from the review.
Exclusion criteria included: (1) any study conducted where direct care services were not performed, such as academic, social service, or criminal justice settings and (2) studies focused on patient outcomes and/or patient care. While posters, blogs, websites, editorials, and conference abstracts were excluded to maintain methodological rigor, peer-reviewed commentaries and perspective articles were included to capture conceptual and implementation-focused insights relevant to TIA, given the emerging nature of the field.
Databases and Search Strategies
A consultation was conducted with the university’s health profession librarian to identify relevant databases and to establish a systematic, rigorous literature search process (Fink, 2020). Bibliographic databases and websites were selected to identify publications related to health, nursing, and professional development within healthcare organizations, including PubMed, Primo Library Services (PRIMO), and a multi-database search conducted through the EBSCOhost platform (EBSCOhost), including American Psychological Association (APA) PsycArticles, APA PsycInfo, and the Cumulative Index to Nursing and Allied Health Literature (CINAHL).
Comprehensive search terms relevant to the topic were developed through consultation among the study authors and a university librarian. The search was initially conducted in September 2023, in an iterative process and an updated search was conducted in September 2024. There is a critical opportunity for standardizing language in TIA research for consistency and clarity (SAMHSA, 2014), so we took into consideration the variety of ways TIAs have been addressed in the literature based on clinical and academic knowledge. We began with various search terms such as the “trauma-informed approach,” “trauma-informed organizational climate,” and “trauma-informed care” to broaden the search and capture any relevant practices in this emerging field (Menschner & Maul, 2016). Next, we refined the search strategy to include a combination of the following keywords: “trauma-informed OR trauma-informed care OR trauma-informed approach” AND “healthcare organization or hospital or healthcare facility or care center” AND “nurse OR health personnel or health provider or healthcare worker or health professional.”
To enhance study rigor and thoroughness, a secondary search strategy was implemented which was a hand search. A hand search is performed by carefully reviewing the reference sections of all retained articles in order to capture additional articles relevant to the research questions (Vassar et al., 2016). Any articles identified from the hand search were then added to the Principles of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) diagram (Moher et al., 2009) and included in the screening process (Figure 1).
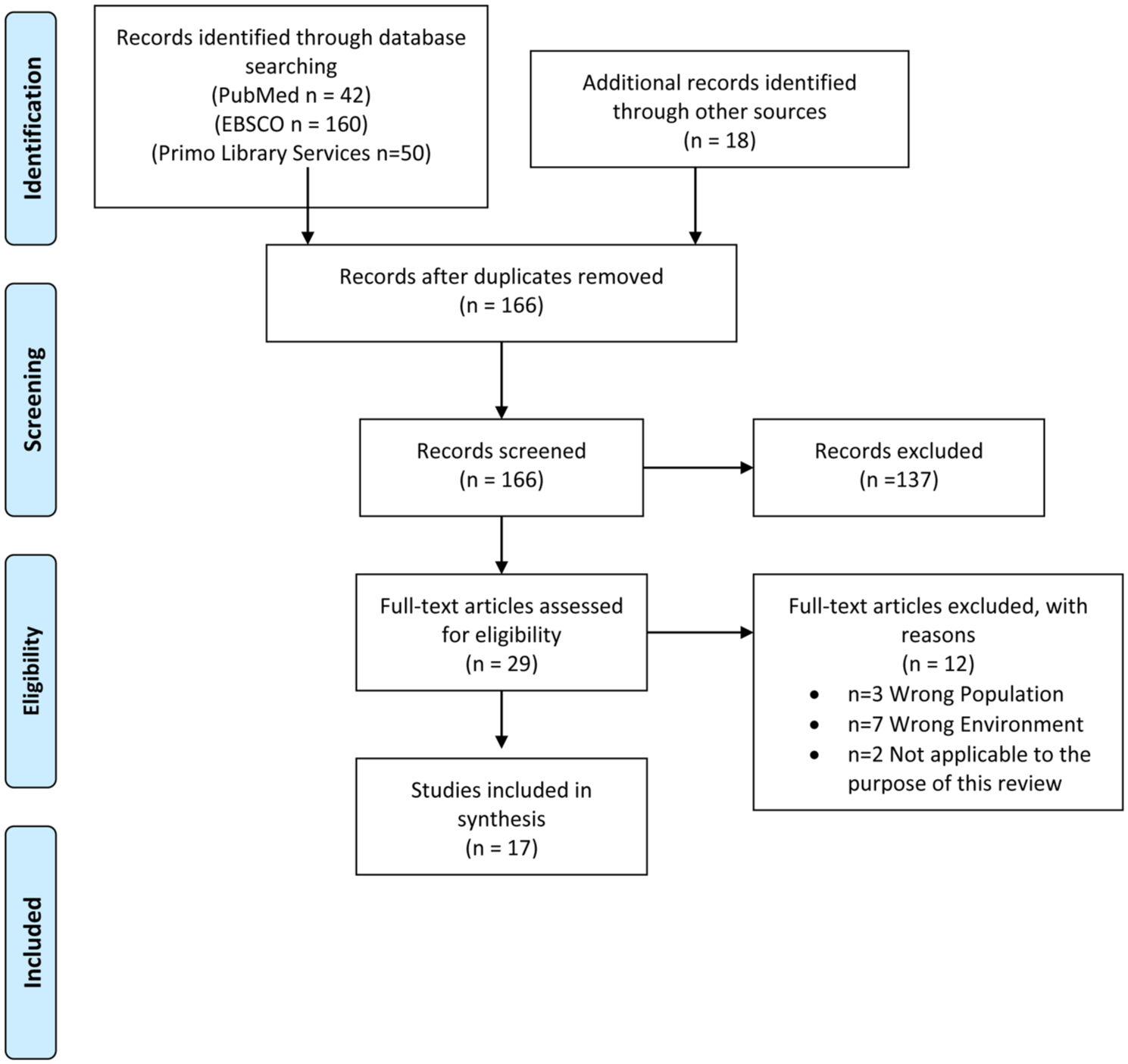
PRISMA 2009 flow diagram
Practical Screening
A practical screen was conducted using the author-developed practical screening tool (Table 1). Rayyan, an online software that supports the process of organizing articles and removing duplicates based on inclusion or exclusion criteria, was utilized (Ouzzani et al., 2016). During the practical screening process collaborative discussion between the authors occurred.
The practical screen was followed by a two-reviewer methodological screen. The rigorous methodological screening process provided the most relevant articles applicable to the selected research questions. The PRISMA guidelines were used to report the results. A total of 270 records were identified through database searching. After removal of 104 duplicates, 166 records were screened, of which 137 were excluded based on title and abstract review. Twenty-nine full-text articles were assessed for eligibility, and 12 were excluded for reasons including non–healthcare worker populations, non-healthcare settings, or lack of relevance to trauma-informed approaches. A final sample of 17 studies was included in the review.
DataExtraction
A data extraction table was developed by the authors based on Cochrane (2019) guidelines and was utilized by both authors, who served as independent reviewers for all articles meeting inclusion criteria following the methodological screening stage. The reviewers independently extracted data and met to resolve any discrepancies through discussion. The data extraction table facilitated the summarization of pertinent information from each article (Table 2). No discrepancies between reviewers were identified; however, a third reviewer was available for consultation if needed.
Retained Articles in Scoping Review of Trauma Informed Approaches Applied in Healthcare Alphabetical Order (2018–2024)
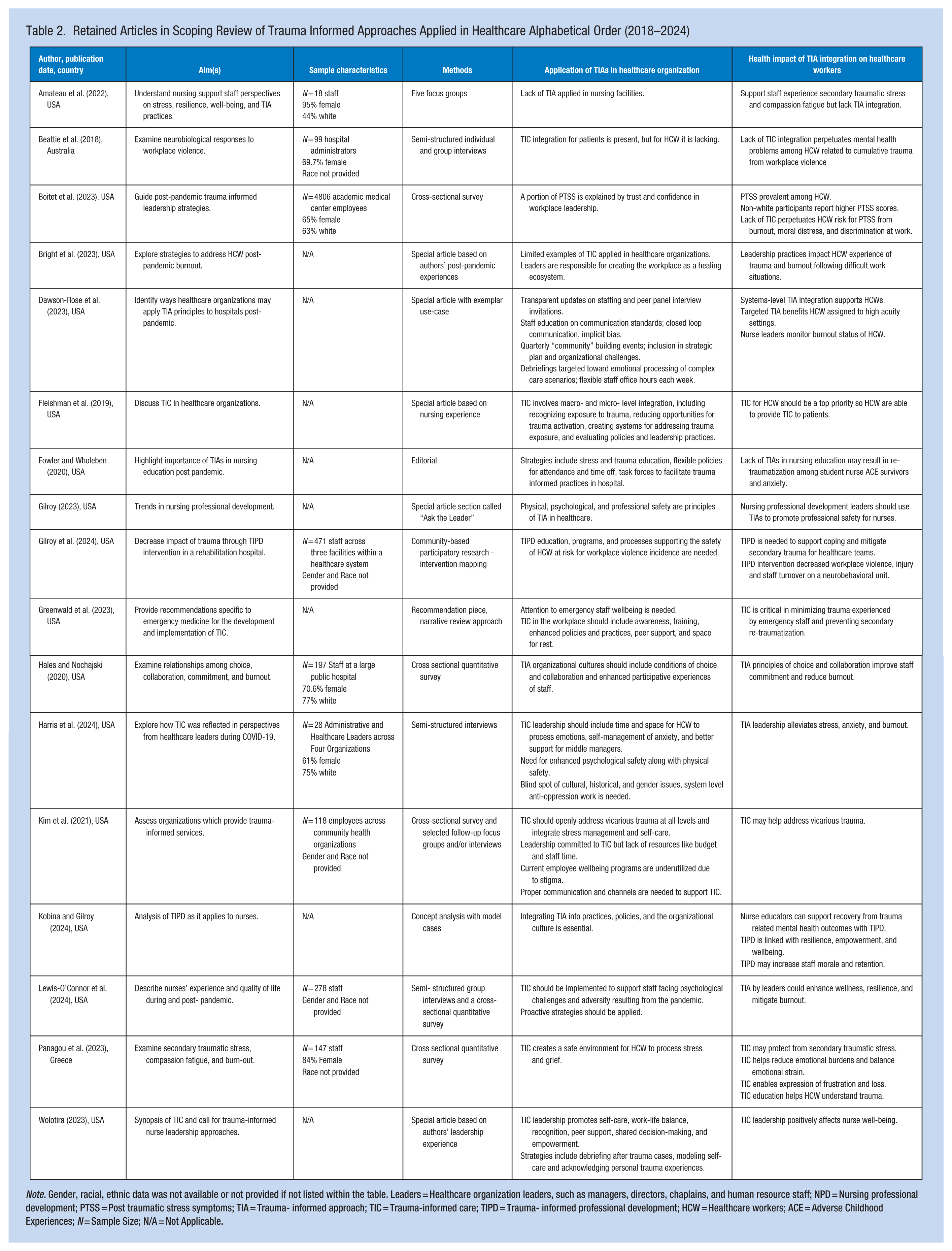
Note. Gender, racial, ethnic data was not available or not provided if not listed within the table. Leaders = Healthcare organization leaders, such as managers, directors, chaplains, and human resource staff; NPD = Nursing professional development; PTSS = Post traumatic stress symptoms; TIA = Trauma- informed approach; TIC = Trauma-informed care; TIPD = Trauma- informed professional development; HCW = Healthcare workers; ACE = Adverse Childhood Experiences; N = Sample Size; N/A = Not Applicable.
Results
A total of 17 articles (N = 17) met the inclusion criteria and were included in the final scoping review, representing 6,162 participants. The studies spanned a range of healthcare settings, including nursing homes, hospitals, and other institutions, as well as diverse hospital units such as emergency departments, behavioral health units, and pediatric intensive care units. Most studies originated from the United States with publication years ranging from 2018 to 2024.
Study designs varied and included quantitative (n = 3), qualitative (n = 3), mixed-methods (n = 3), review articles (n = 2), case studies (n = 1), and opinion pieces authored by clinical experts (n = 5). Sample populations of HCWs included both direct and indirect care staff, such as nurses, physicians, support staff, nursing professional development educators, administrators, health scientists, nurse practitioners, trainees, and other clinicians. The studies with sample demographics (Amateau et al., 2022; Beattie et al., 2018; Boitet et al., 2023; Hales & Nochajski, 2020; Harris et al., 2024; Panagou et al., 2023), had a higher proportion of female participants than male participants, and most participants were white (Table 2).
Integration of Trauma-Informed Approaches in Healthcare Organizations
The most widely reported strategies for implementing TIAs were trauma awareness and education (82%, n = 14/17) and the cultivation of safe and supportive environments (82%, n = 14/17), each appearing in the majority of reviewed articles. Other strategies reported with high frequency included policy assessments (76%, n = 13/17), peer support opportunities (71%, n = 12/17), and transparent communication with routine check-ins, such as scheduled team huddles, leadership rounding, or structured updates to share information and address concerns (65%, n = 11/17). Self-care and stress management resources (53%, n = 9/17) and debriefing sessions following critical incidents (41%, n = 7/17) were also described. The formation of dedicated task forces to oversee trauma-informed initiatives was also reported (12%, n = 2/17). Figure 2 illustrates the frequency of reported strategies for implementing TIAs within healthcare organizations.
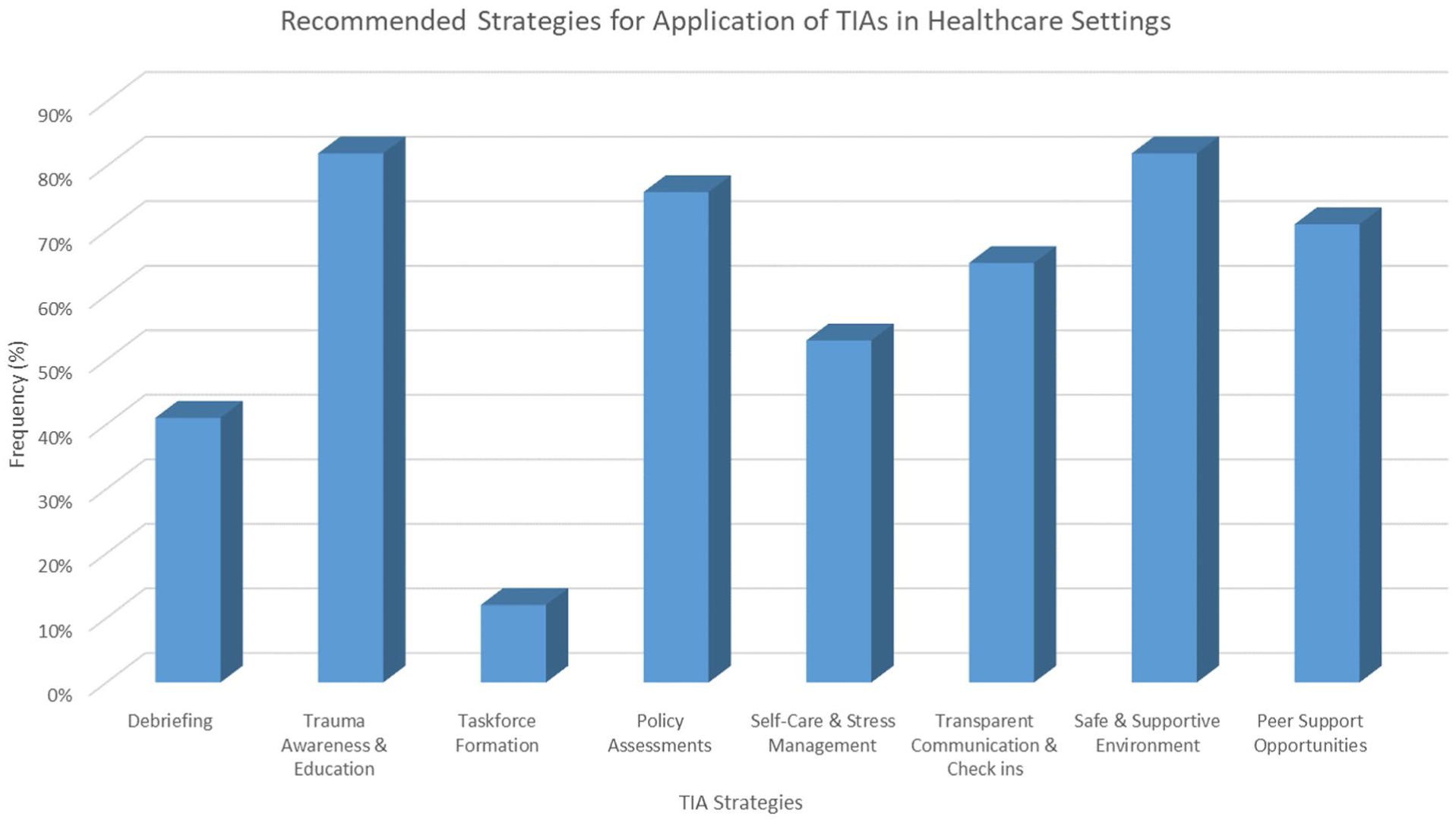
Strategies for application of TIAs based on frequency
Health Impacts of Trauma-Informed Approaches on Healthcare Workers
Reported health impacts of TIAs on HCWs included enhanced protective factors (82%, n = 14/17), lower burnout (88%, n = 15/17), improved mental health (88%, n = 15/17), and greater trauma recovery or healing (88%, n = 15/17). Decreased emotional exhaustion (76%, n = 13/17) and lower compassion fatigue (76%, n = 13/17) were also commonly noted. Balancing psychological strain related to job demands was reported in 65% (n = 11/17) of the articles, while increased job satisfaction was reported less often (35%, n = 6/17). Figure 3 presents the frequency of reported health impacts related to TIA implementation.
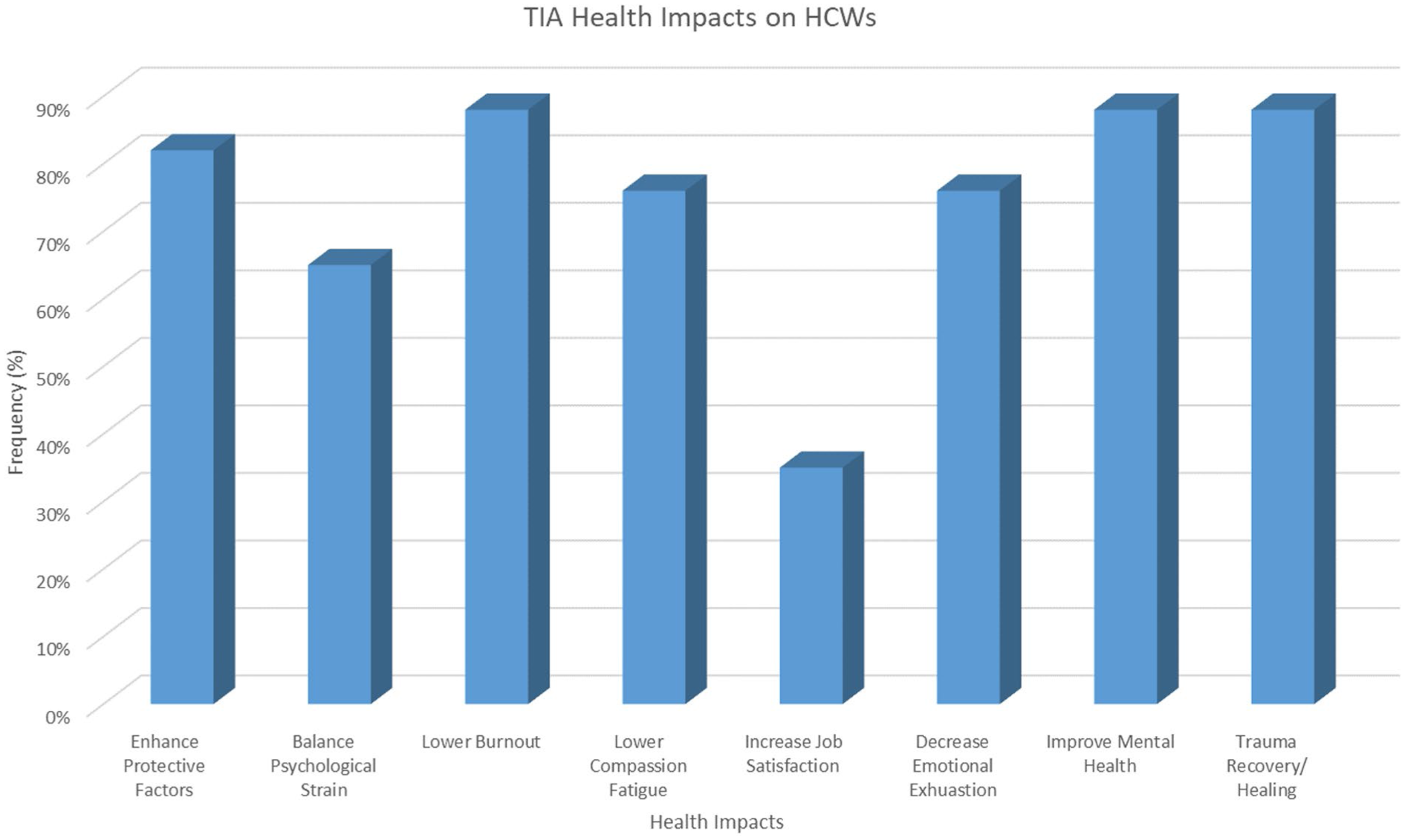
TIA health impacts based on frequency
Discussion
This scoping review mapped the existing literature on the integration of TIAs within healthcare organizations and the reported health impacts of TIA integration on HCWs. Across the included literature, TIA integration was frequently associated with improvements in HCW well-being, including resilience, job satisfaction, engagement, and retention, which may ultimately support improved patient care. These findings align with prior systematic reviews conducted in other human service systems, such as substance use treatment settings, where similar workforce outcomes have been reported following TIA implementation (Mahon, 2024).
Our review expands the literature by examining how TIAs have been integrated across diverse healthcare environments and how these efforts are reported to influence burnout, secondary traumatic stress, and other mental health challenges experienced by HCWs. Across the included studies, TIA initiatives were implemented in a variety of healthcare settings, including emergency departments, medical centers, and public hospitals. However, the literature suggests that many TIA initiatives remain primarily patient-focused, with comparatively limited attention directed toward supporting the well-being of healthcare staff (Amateau et al., 2022; Beattie et al., 2018).
Several organizational strategies for TIA integration were commonly reported in the literature. These included increasing trauma awareness and education, cultivating safe and supportive work environments, conducting organizational policy assessments, promoting peer support opportunities, and implementing transparent communication practices with routine staff check-ins (Gilroy et al., 2024; Panagou et al., 2023). Structural mechanisms such as trauma-informed task forces and ongoing policy evaluation were also described as approaches to sustain TIA initiatives, particularly in high-risk clinical settings such as emergency departments and intensive care units (Fowler & Wholeben, 2020; Greenwald et al., 2023).
Leadership engagement emerged as an important facilitator of trauma-informed organizational climates. Across several studies, leaders who modeled self-care, communicated transparently, and created psychologically safe environments for staff discussion were reported to support recovery from workplace trauma and reinforce cultures of trust and collaboration (Bright et al., 2023; Dawson-Rose et al., 2023). However, multiple barriers to implementation were identified across the literature, including limited organizational resources, insufficient workforce training, stigma surrounding mental health, and underutilization of employee well-being programs (Amateau et al., 2022; Kim et al., 2021). Addressing broader cultural, historical, and gender-related considerations and promoting anti-oppressive practices, were also identified as important for advancing trauma-informed leadership in healthcare organizations (Harris et al., 2024).
Across the included studies, the integration of TIA principles such as autonomy, collaboration, and peer support was frequently associated with reductions in burnout, emotional exhaustion, compassion fatigue, and secondary traumatic stress among HCWs (Fleishman et al., 2019; Gilroy et al., 2024). Improvements in coping, resilience, psychological safety, and overall staff well-being were also commonly reported. These organizational supports were described as contributing to greater workforce stability, including improved retention and staff satisfaction (Kobina & Gilroy, 2024; Wolotira, 2023).
Consistent with previous reviews, the findings of this scoping review highlight the importance of organizational and leadership commitment to successfully enculturate trauma-informed principles within healthcare systems (Lewis et al., 2023; Mahon, 2022; Mahon, 2024). Additional research involving larger samples of healthcare workers is needed to further explore the perceived impact of system-level trauma-informed initiatives on workforce well-being and organizational outcomes.
Lastly, we found existing studies relied heavily on expert opinions which align with prior review findings (Lewis et al., 2023; Mahon, 2024; Oral et al., 2020). There is a need for more robust studies applying well-established measurement tools for TIA effectiveness (Lewis et al., 2023; Mahon, 2024; Oral et al., 2020).
Implications for Future Research
Future research should aim to better understand TIA perceptions in settings more susceptible to trauma such as emergency rooms, intensive care units, and behavioral health units. Focusing on specific healthcare disciplines, particularly nurses working in high-risk areas, may also provide valuable insights into best practices for addressing the unique challenges faced in these environments. Furthermore, since the impact of integrating TIAs within healthcare settings is still in the early stages, qualitative research is necessary with a larger sample of HCWs to explore the perceived effects of trauma-informed system-level initiatives aimed at promoting well-being.
Implications for Occupational Health Practice
Occupational health nurses can promote safety and foster physical, mental, and social well-being of staff by applying TIA strategies within their practice. Occupational health programs that incorporate TIA can help create safer work environments, reducing workplace injuries while further enhancing the overall well-being of staff. Occupational health nurses often respond to serious injuries, including burns and falls, and help stabilize workers before additional help arrives. Witnessing these traumatic events may predispose occupational health nurses to post traumatic stress disorder and secondary traumatic stress. Strategies may be incorporated into occupational healthcare workplaces such as creating safe spaces and holding debriefings to facilitate emotional processing of complex care scenarios, peer support programs, and enhanced training on cultural and gender anti-oppression work (Dawson-Rose et al., 2023; Fowler & Wholeben, 2020; Gilroy et al., 2024; Greenwald et al., 2023; Harris et al., 2024).
Limitations
A limitation of this study is that it is a scoping review, meaning a wide net was cast to incorporate the most recent literature on TIAs in healthcare organizations in relation to HCWs, and therefore it is not intended to determine clinical practice decisions. One notable aspect of a scoping review is the lack of a quality assessment. Due to this, recommendations from this literature are only meant to map out the next steps in this area of research to further develop the science.
Another limitation is the potential for incomplete evidence synthesis due to inconsistent and evolving terminology used within trauma-informed research. The lack of standardized language may have affected the comprehensiveness of the search strategy, increasing the possibility that relevant search terms, databases, or recently published studies were not captured. To mitigate this limitation, the first author collaborated with a university librarian at the start of the study to develop a comprehensive search strategy intended to minimize the inadvertent exclusion of relevant search terms or databases. Despite these efforts, the inclusion and exclusion criteria may still introduce selection bias that could influence the results. A comprehensive electronic database search was recently reconducted (Fall 2024) to capture any additional studies that may have been published in the past 12 months.
A third limitation is that the practical screening stage was conducted by a single author, while the methodological screening was conducted by both authors, which introduces the potential for reviewer bias or inconsistent evaluation of articles. However, both reviewers have expertise in trauma-informed approaches in healthcare organizations and in conducting systematic scoping reviews using Fink’s process (2020), which supports the rigor of the review. The authors met at study conception to establish the practical screening plan and maintained communication throughout the study to promote consistency in the screening process.
Conclusion
This review aimed to examine what is known about TIAs integrated within healthcare organizations and their health impact on HCWs and this was met. A scoping review was conducted to investigate the literature, identify gaps for future research, and provide insight for healthcare organizations to consider when establishing initiatives to improve the well-being of their healthcare teams.
Applying TIAs within healthcare organizations demonstrates promise toward more inclusive, supportive, and healing environments that mitigate the poor mental health outcomes and burnout afflicting the healthcare workforce. This review suggests that integrating TIAs within healthcare can serve as a system-oriented, organizational level solution for addressing burnout and building healthy workforces, yet more work must be done to better understand HCWs’ perceived effectiveness of TIA strategies.
In Summary
TIAs were frequently associated with improved retention and decreased burnout, but most of the studies were special articles or qualitative in nature
While leadership disengagement and systemic barriers pose as threats to cultivating a trauma-informed organizational climate, they may equally be the anchor points for promoting healthcare worker retention and well-being.
Footnotes
Author Note
The authors used ChatGPT and Grammarly for language editing and clarity improvements. Authors declare that the content, ideas, results, discussion, and conclusions presented are the sole responsibility of the author.
Author Contributions
Both authors made substantial contributions to the manuscript conception, and analysis and interpretation of data. Both authors were involved in drafting the manuscript, revising it critically for important intellectual content, and giving final approval of the version to be published.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.