
Abstract
The current study examines two developmental risk pathways (an academic/economic pathway and a delinquency/interpersonal pathway) linking cumulative socioeconomic adversity to subsequent depressive symptoms and the interplay between these pathways and depressive symptoms using path analysis with a sample of 14,563 respondents from the National Longitudinal Study of Adolescent to Adult Health over a 13-year period. Minority youth comprised 49% of this nationally representative sample, including 21% Blacks, 16% Hispanics, 6% Asians, 2% Native Americans, and 4% multiracial youth. Cumulative socioeconomic adversity appears to initiate an adverse life course process involving depressive symptoms, academic/economic difficulties, and delinquency/interpersonal incompetency. It appears that mediating life experiences partially explain the persistent influence of socioeconomic adversity and the continuity of depressive symptoms over the early life course. A deeper understanding of this dynamic process provides insight into the prevention of emotional problems in these early life stages.
Previous studies document that depression is a major public health problem from adolescence (13–19 years) through young adulthood (Kessler et al., 1994; Kessler & Walters, 1998). Also, these studies show significant continuity in early depressive symptoms across adolescence, emerging adulthood (19–25 years), and young adulthood (25–40 years; Costello, Mustillo, Erkanli, Keeler, & Angold, 2003; Wickrama, Conger, Lorenz, & Jung, 2008). The continuity in depressive symptoms is associated with more serious conditions, including clinically high levels of depressive symptoms and depressive disorders (Insel & Fenton, 2005) as well as with failures in social, cognitive, and behavioral developmental pathways over this period (Rudolph, Flynn, Abaied, Groot, & Thompson, 2009).
Furthermore, longitudinal studies on developmental pathways suggest that developmental experiences during adolescence (e.g., academic failures and delinquency) stemming from childhood/adolescent cumulative socioeconomic adversity predict failures during the transition to young adulthood (e.g., low economic attainment and poor romantic relationship quality) and, ultimately, elevated depressive symptoms among young adults (Wickrama et al., 2008). However, previous research has not adequately investigated whether the persistent influence of socioeconomic adversity on young adult depressive symptoms is mediated by these risk pathways. Also, we know little about the interplay between these developmental pathways and depressive symptom continuity through adolescence and into young adulthood.
The current study focuses specifically on depressive symptoms because past research suggests that this internalizing problem may play a more prominent role in overall psychopathology compared to other internalizing symptoms. For example, previous studies show that youth with high levels of depressive symptoms tend to have comorbid high levels of anxiety symptoms more often than those with high levels of anxiety symptoms exhibit comorbid high levels of depressive symptoms (Merikangas & Avenevoli, 2002; Ollendick, Shortt, & Sander, 2005). Additionally, depressive disorders are generally more related to proximal stressors than anxiety disorders (Phillips, Hammen, Brennan, Najman, & Bor, 2005), which makes the investigation of depressive symptoms and stressful developmental processes over time of particular interest.
Furthermore, it is important to investigate this continuous developmental process from adolescence through young adulthood because the incidence of depression increases from adolescence to young adulthood (Keenan, Feng, Hipwell, & Klostermann, 2009). Adolescents with subdiagnostic levels of depressive symptoms show higher rates of depression in early adulthood and report adverse psychological and social functioning (Aalto-Setälä, Poikolainen, Tuulio-Henriksson, Marttunen, & Lönnqvist, 2002; Harrington, Fudge, Rutter, Pickles, & Hill, 1990; Lewinsohn, Rohde, Klein, & Seeley, 1999). High levels of depressive symptoms early in life are predictive of a depressive disorder diagnosis in later years even after taking into account comorbidity with other disorders (Costello et al., 2003; Keenan et al., 2009).
From a prevention perspective, identifying early, and ongoing, predictors of increasing and/or continually high depressive symptoms over the early life course is important because early high levels of depressive symptoms are the best known predictor of later depression (Keenan et al., 2009). Identifying those at risk can facilitate interventions that reduce the continuity of depressive symptoms before a chronic course of symptoms is established. Prospective longitudinal research offers the best design for identifying these early predictors (Harrington et al., 1990; Lewinsohn et al., 1999).
Furthermore, longitudinal studies on developmental pathways suggest that life experiences during adolescence (e.g., academic failures and delinquency in adolescence) stemming from childhood/adolescent cumulative socioeconomic adversity predict failures during the transition to young adulthood (e.g., low economic attainment and relationship dissatisfaction) and, ultimately, poor well-being among young adults (Bird, 2007; Bradley & Corwyn, 2002; Featherman & Hauser, 1978; Wickrama et al., 2008). The cascade model provides a framework for understanding how risks proliferate and compound over adolescence and emerging adulthood in a successively contingent manner creating a “chain of insults” (O’Rand & Hamil-Luker, 2005) involving the continuity of depressive symptoms well into young adulthood. In this process, one hardship may continue while another appears, forming a cascading sequence of stress or risks (Hatch, 2005). This is a type of life course process whereby multiple smaller effects combine over time to exert a cumulative effect (Hatch, 2005).
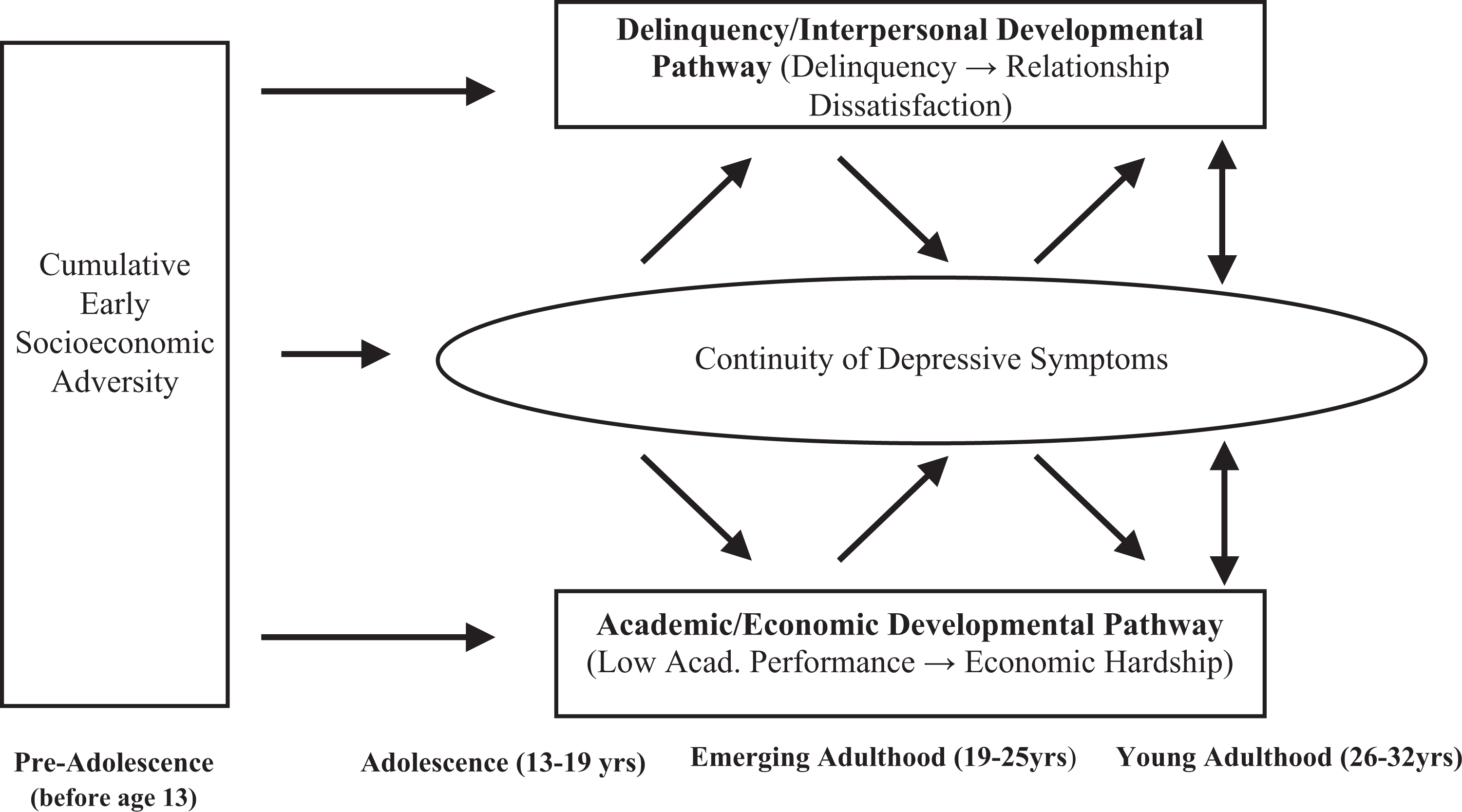
The present study will examine two risk pathways (i.e., an academic/economic pathway and a delinquency/interpersonal pathway) from cumulative socioeconomic adversity to young adult depressive symptoms and the interplay of these two pathways with depressive symptoms from adolescence into young adulthood (see Figure 1). These risk pathways are examined using prospective data over a 13-year period from a national sample of over 12,000 adolescents who participated in the National Longitudinal Study of Adolescent to Adult Health (Add Health).
Theoretical framework.
Socioeconomic Adversity
Socioeconomic adversity can entail both family and community adversities, and these adversities put youth at risk for emotional problems. Family risk factors include family poverty, low parental education, and related aspects of the family context (parents’ marital status, family conflict and aggression, and poor parenting practices; Conger, Conger, & Martin, 2010). Family poverty may lead adolescents to feel trapped, angry, hopeless, and frustrated (Prawitz, Kalkowski, & Cohart, 2013). For instance, it places limits on participation in extracurricular educational activities (Broh, 2002) and makes non-essentials, such as specific clothing and concert tickets, out of reach for adolescents whose families have limited funds, which may hinder their perceptions of being able to “fit in” (Orr, 2003). Reduced access to healthy, positive adolescent activities may decrease the opportunity cost of their time and, consequently, increase the likelihood of involvement in nonproductive or delinquent activity (Upchurch, Levy-Storms, Sucoff, & Aneshensel, 1998). In contrast, affluent parents are able to invest more in the development of their children (Schoeni & Ross, 2005), leading to greater educational attainment, increased employment prospects, and more advanced cognitive, problem-solving, and technological skills (Youniss & Ruth, 2002).
Lower levels of parent education are another family risk factor that may proliferate into several risk factors, such as ineffective parenting, parental negligence, and parental rejection. One reason for this proliferation may be that parents who have attained less education have unfavorable job characteristics (e.g., less work control) and less access to the social and psychological resources, skills, and information associated with child protection and the facilitation of child development (Clougherty, Souza, & Cullen, 2010).
In addition, adolescents from disrupted, fragile, unstable, and/or single-parent families are at greater risk for emotional problems, such as depressive symptoms (Fomby & Cherlin, 2007; Sweeney, 2007). In particular, stressful circumstances for single caregivers, combined with the absence of a caring and supportive co-parent, often result in stress-related ineffective parenting practices, such as parental rejection and a lack of parental warmth, which have detrimental consequences for youths’ well-being (Conger & Donnellan, 2007).
More broadly, socioeconomically disadvantaged families are, essentially, families under stress (Repetti, Taylor, & Seeman, 2002). Stressful family environments strain the stress-responsive biological regulatory systems of children (Barker et al., 1993) and disrupt their development and psychosocial functioning (Hertzman & Power, 2005). The accumulation of these risks results in biobehavioral system disruptions known to be associated with childhood/adolescent neurocognitive, neurobehavioral, and physiological impairments (“biological programming”), including educational failures, poor mental health, behavioral problems, impaired emotional processing, and social incompetence. These risks often continue into young adulthood (Repetti et al., 2002).
In addition to family risk factors, adverse community conditions also put youth at risk for emotional problems. Community risk factors include a lack of physical and/or social resources and opportunities, deteriorated normative community environment, high crime rates, poor housing, and physical hazards. The lack of resources and opportunities in adverse communities may generate feelings of hopelessness and frustration among youth (Ross, Reynolds, & Geis, 2000), and these negative feelings place youth living in deprived neighborhoods at increased risk for developing emotional and behavioral problems (Wheaton & Clarke, 2003). Community studies have identified adverse community processes, including the deterioration of the physical, social, and normative community environments, through which structural community adversity is associated with residents’ well-being (Cutrona et al., 2003). Ambient stress (i.e., “community stress”) associated with exposure to adverse community conditions also predisposes adolescents to depressive symptoms (Ross & Mirowsky, 2009).
The Cumulative Risk of Family and Community Socioeconomic Adversity
Because family and community adverse socioeconomic circumstances often co-occur, children and adolescents often contend with constellations of developmental risk factors rather than isolated instances of adverse circumstances (Conger et al., 2010). Previous research provides robust findings related to the differential effects of multiple and single risk exposures (Sameroff, 2006) and has noted that exposure to multiple socioeconomic adversities in childhood and/or adolescence has more severe consequences for youth development than exposure to a single socioeconomic adversity (Evans & Kim, 2010). That is, socioeconomic adversities may cumulatively undermine adjustment from adolescence into young adulthood.
For example, in an examination of overall child wellness, the buildup of multiple hardships negatively affected child well-being (Frank et al., 2010). Moreover, using a composite index of multiple family risk indicators, such as current unemployment, single-parent family structure, inadequate income, and adverse community characteristics, studies demonstrate that adolescents experiencing a high level of cumulative socioeconomic risk are more likely to have elevated depressive symptoms, less educational attainment, and physical health problems than adolescents who encounter low levels of cumulative socioeconomic risk (Brody et al., 2013).
Based on these findings, we anticipate that cumulative socioeconomic adversity, as captured by a composite index, will be negatively associated with youths’ developmental outcomes. There are several advantages of formulating indices of multiple risk factor exposures into a composite score. These advantages include enhancing the validity of the measure by more fully capturing the meaning of the construct of interest and reducing potential co-linearity among individual risk factors in a regression analysis (Jankowski, 2015).
Cumulative Adversity and the Academic/Economic Risk Pathway
As previously discussed, socioeconomic adversity can curtail adolescents’ performance through a lack of educational resources, facilities, and ineffective parental practices as well as through impaired cognitive development. Education helps individuals develop abilities and skills, or human capital (Becker, 1965). In school, youth not only learn to read and write but also learn to solve problems, employ critical thinking skills, develop ideas, and implement plans (Kingston, Hubbard, Lapp, Schroeder, & Wilson, 2003). Education also develops the competencies, skills, and behaviors necessary for socioeconomic attainment, including dependability, judgment, motivation, and effort (Benson et al., 2006). Additional research suggests that education may promote positive physiological functioning, which may enhance these competencies (e.g., the development of neural connections; Conroy, Sandel, & Zuckerman, 2010).
Furthermore, educationally competent youth may more effectively utilize family economic resources (e.g., family income) and noneconomic resources (e.g., parental education and family relationships/support) to successfully transition to young adulthood. Conversely, a lack of educational attainment and poor academic performance may lead to an unsuccessful transition to young adulthood, particularly in the form of economic difficulties.
Cumulative Adversity and the Delinquency/Relational Risk Pathway
Adolescents’ behavioral problems (delinquent behavior, in particular) may reflect an externalized reaction to family and community adversity that exists parallel to an internalized reaction to risk and stress exposure in the form of depressive symptoms (Kubzansky & Kawachi, 2000). Consequently, it is important to consider delinquency as a response to the hopelessness adolescents from disadvantaged families and communities may feel due to the lack of resources and opportunities (Browning & Cagney, 2003). Wilson (1996) argued that social disorganization in adverse communities undermines adolescents’ bonds to community organizations, such as schools, and reduces the ability of communities to enforce normative control over adolescent risky and delinquent behavior.
Adolescents’ delinquency can lead to the development of a pattern of aggressive behavior in young adulthood. This pattern of aggressive behavior may extend to other social settings, including romantic relationships. There is a significant association between adolescents’ delinquency and the likelihood that young adults display aggressive behaviors toward a romantic partner (White & Widom, 2003). Accordingly, we propose that delinquency in adolescence will be associated with relationship dissatisfaction in young adulthood.
Interplay Between Depressive Symptoms and Academic/Economic and Delinquency/Interpersonal Pathways
Adolescents’ depressive symptoms have the potential to disrupt their healthy development from adolescence into young adulthood. For instance, depressive symptoms in adolescence may impede the normative development of social, psychological, cognitive, academic, and behavioral competencies necessary for a successful transition to adulthood (Wickrama et al., 2008). At the same time, depressive symptoms are prone to persist from adolescence into young adulthood (Wickrama, Conger, Lorenz, & Martin, 2012). We expect that cumulative socioeconomic adversity occurring before and during adolescence will lead to later disadvantages in a continuous and cumulative manner, specifically through early academic failures and behavioral problems, such as delinquency (O’Rand & Hamil-Luker, 2005). Furthermore, this cycle is expected to persist with depressed mood also selecting young adults into stressful life circumstances (e.g., failures in relationships and low economic attainment; Conger & Donnellan, 2007).
More specifically, we propose that adolescent academic failures will be linked to young adult economic failures, and both of these failures will mediate the association between early and later depressed mood (i.e., the academic/economic pathway). Depressed adolescents may have low educational and socioeconomic expectations and may experience difficulty developing knowledge, psychological/cognitive capabilities, and other skills necessary for educational and occupational attainment (Fergusson & Woodward, 2002). Also, depressed adolescents may not receive sufficient social support, which is a valuable resource that increases the likelihood of emerging adults’ success in advanced educational or career endeavors (Miech, Caspi, Moffitt, Wright, & Silva, 1999). Social and educational failures during this key transitional stage can have substantial mental health consequences (Benson et al., 2006).
Additionally, because depressed individuals often behave in a manner that elicits social rejection and avoidance from others (Rudolph et al., 2009), their lack of interpersonal skills and the related negative responses from others may hinder their development of close relationships. As previously discussed, delinquency is often an adolescent’s response to depressive feelings stemming from their experiences in disadvantaged families and communities (Browning & Cagney, 2003). Not only is this pattern of aggressive behavior problematic in adolescence, but it may extend to problematic romantic relationships in young adulthood, which have emotional consequences. Thus, we propose that adolescent delinquency and young adult relationship dissatisfaction will mediate the relationship between early and later depressed mood, representing a delinquency/interpersonal risk pathway.
The Current Study and Hypotheses
Drawing from the findings of previous studies, we identified two developmental risk pathways stemming from cumulative socioeconomic adversity, as components of a life course cascade model (Figure 1). These pathways include an academic/economic pathway and a delinquency/interpersonal pathway, and these pathways are hypothesized to exist parallel to emotional development (i.e., the continuity/discontinuity in depressive symptoms). The academic/economic pathway refers to the cascade of educational and financial failures, whereas the delinquency/interpersonal pathway involves delinquency and relationship dissatisfaction.
As depicted in Figure 1, the present research has three main objectives. First, this study examines the relationship between cumulative socioeconomic adversity (including family and community adversity before and during adolescence) and the level of, and continuity in, depressive symptoms across adolescence, emerging adulthood, and young adulthood. Second, this study examines the persistent influence of cumulative socioeconomic adversity on young adults' depressive symptoms through youths’ academic/economic and delinquency/interpersonal developmental risk pathways. Third, this study examines the interplay between two distinct risk pathways and depressive symptom continuity from adolescence to young adulthood.
Method
Sample
Data for this study came from a nationally representative sample of adolescents participating in the Add Health study. In 1995, baseline (Wave 1) data were derived from a complex stratified cluster sampling of middle and high school students, yielding 20,745 respondents (M age = 15.5 years and range = 13–19 years at baseline) from 134 middle and high schools. To ensure diversity, the sample was stratified by region, urbanicity, school type (public vs. private), racial composition, and size. The second, third, and fourth waves of data were collected in 1996, 2001, and 2008 (N 2 = 14,738; N 3 = 15,100, and N 4 = 15,701). Respondents’ ages ranged from 14–20 at Wave 2 (1996), 19–25 at Wave 3 (2001), and 26–32 at Wave 4 (2008). Racial/ethnic minorities were oversampled. More information about the Add Health study is available at http://www.cpc.unc.edu/projects/AddHealth
We used in-home interview data from parents who participated in Wave 1 and adolescents who participated in Waves 1 (adolescence), 3 (emerging adulthood), and 4 (young adulthood). Thus, the final study sample size was comprised of 14,563 respondents who participated in the three waves of data collection of interest in the current study. The average number of missing cases for each study variable was 14.18%, with a range from 0.30% for economic problems at Wave 4 to 21.90% for academic problems at Wave 1 (see Table 1). The final sample consisted of approximately 53% women, and 49% of respondents reported a minority racial/ethnic status with the largest percentages reported for Black (21%), Hispanic (16%), Asian (6%), Native American (2%), and multiracial youth (4%), respectively. Attrition and missing data analysis showed that adolescents who participated in all four waves were slightly younger but otherwise confirmed that there was little difference between adolescents with missing data in our study sample and those with complete data.
Descriptive Statistics and Correlations Among Study Variables.

Note. DEP = depressive symptoms; CSA = cumulative socioeconomic adversity; DELQ = delinquency; ACP = academic problems; RELDIS = relationship dissatisfaction; and ECONP = economic problem.
***p < .001.
Measures
Depressive symptoms
Depressive symptoms were measured at Wave 1 (1995; adolescence), Wave 3 (2001; emerging adulthood), and Wave 4 (2008; young adulthood) using 8 items from the Center for Epidemiological Studies of Depression Scale (CES-D; Radloff, 1977) to assess feelings of distress (e.g., “felt depressed and sad”) in the past week. Scale responses ranged from 0 = never or rarely to 3 = most of the time or all of the time. Positive affect items were reverse coded before summing all items. This resulted in an index of depressive symptoms ranging from 0 to 24. The scale had adequate internal reliability (α = .80 or higher at all three waves).
Cumulative socioeconomic adversity
We constructed a composite index for cumulative socioeconomic adversity by summing dichotomous indicators capturing different dimensions of adversity (Brody et al., 2013). These indicators included low parental education, high family economic hardship, low parental marital stability, and high community adversity. Except for marital stability (already a dichotomous measure), dichotomous indicators were created by mean splitting the following measures. Mean splitting was employed because all of the indicators do not have intuitively meaningful cut points to differentiate high and low adversity. Mean splitting allowed us to use a single strategy to consistently identify socioeconomic adversity across all of the variables included in the composite score while maintaining relatively meaningful cut points for variables, when applicable (i.e., parent education mean = 5.49, which is slightly above a high school diploma; economic hardship mean = 1.49, which identifies families who received just over one form of assistance). Each indicator is described in more detail in the paragraphs that follow.
Parental education
The responding parent reported both parents’ highest level of education obtained at Wave 1 (1995). Responses ranged from 1 = never went to school to 10 = professional training beyond 4-year college or university degree. Mothers’ and fathers’ educational levels were summed to create an index of parental education. For single-headed families (n = 79) with no available data from fathers, maternal education served as the indicator of parental education.
Economic hardship
Five dichotomous items (0 = no and 1 = yes) assessed whether any member of the household received the following social service benefits in the past month: social security, supplemental security income, aid to families with dependent children, food stamps, or housing subsidies at Wave 1 (1995). Responses to these 5 items were summed to create an index of economic hardship with a range of 0–5.
Parents’ marital stability
A binary variable was used to differentiate parents who had been consistently married to their spouse (or in a marriage-like relationship) for at least 15 years (1) from other parents (0). Fifteen years were selected as the cutoff because the average age of respondents at Wave 1 was 15 years. Thus, for most respondents this variable represents their parents’ continuous marriage for the duration of the child’s life.
Community adversity
Community adversity was assessed by summing four indicators corresponding to census tract information from the 1990 U.S. Census. The indicators included (a) the proportion of families living in poverty, (b) the proportion of single-parent families, (c) the proportion of adults employed in service occupations, and (d) the proportion of unemployed men.
Adolescent measures (Add Health Wave 1; ages 13–19)
Delinquency
Twelve items from Wave 1 (1995) were used to assess delinquent behavior in the past 12 months. This composite scale included items such as whether and how often the respondent “engaged in a serious physical fight” and “deliberately damaged property that did not belong to them.” Responses for each item ranged from 0 = never to 3 = five times or more. Sum scores were computed (possible range of 0–36), with higher scores indicating more delinquent behavior. The scale had good internal consistency (α = .78).
Academic problems
At Wave 1 (1995), adolescent respondents reported their recent letter grades in school mathematics, social studies, and science classes. These letter grades were transformed into a 4-point numerical scale (1 = A, 2 = B, 3 = C, and 4 = D). Sum scores were computed, with higher scores indicating more academic problems.
Young adult measures (Add Health Wave 4; ages 26–32)
Relationship dissatisfaction
A sum score was created from respondents’ reports of the quality of their current (or most recent) romantic relationship at Wave 4 (2008). These 7 items capture specific dimensions of overall relationship dissatisfaction, such as conflict resolution (“I am satisfied with the way we handle our problems and disagreements”), communication (“My partner listens to me when I need someone to talk to”), trust/commitment (“I trust my partner to be faithful to me”), sexual satisfaction (“I am satisfied with our sex life”), and closeness (“My partner expresses love and affection to me”; Wickrama & O’Neal, 2015). In total, 92.9% of this study’s sample responded to these items (n = 11,543 respondents). Item responses ranged from 1 = strongly agree to 5 = strongly disagree, creating a scale ranging from 7 to 35. The items had adequate internal consistency (α = .90).
Economic problems
At Wave 4 (2008), 7 dichotomous items assessed respondents’ economic hardship in the previous year. For example, respondents reported if in the past 12 months there was “a time when you worried whether food would run out before you would get money to buy more” (0 = no and 1 = yes). Responses were summed with a range of 0–7 to create an index of economic hardship.
Covariates
Race/ethnicity
Previous studies have shown that being a racial/ethnic minority has a persistent detrimental influence on mental health, including depressive symptoms, beginning in childhood and continuing across the life course regardless of income and education (Spencer, 2001). Thus, we incorporated race/ethnicity as a control variable. At Wave 1, adolescents reported their race/ethnicity. Dichotomous (mutually exclusive) variables were then created to assess Black, Hispanic, Asian, Native American, White, and multi- (i.e., youth indicating more than one race/ethnicity) racial/ethnic statuses. The dichotomous variables for each of the minority statuses were included as independent variables in the regression equation resulting in regression coefficients that can be interpreted with reference to Whites (reference group = Whites).
Sex
Previous research has documented that females experience higher levels of depressive symptoms from adolescence into young adulthood (Ge, Lorenz, Conger, Elder Jr., & Simons, 1994). Thus, we incorporated sex as a control variable. Sex was coded as man (0) or woman (1).
Analysis Plan
We tested the theoretical model as a path analysis using Mplus (Version 7.2). In order to preserve the nationally representative nature of the sample, individual sample weights from Wave 1 were used in the analysis. We used the TYPE = COMPLEX command to adjust for potential bias in standard errors and χ2 computation due to the lack of individual independence between observations within schools in the Add Health data. Furthermore, in order to test two competing pathways (an academic/economic developmental pathway and a delinquency/interpersonal developmental pathway), the current study employed a multiple mediator model approach with 1,000 bootstraps (CI = 95%; Preacher & Hayes, 2008). Because our focus is young adults’ depressive symptoms, when estimating the contribution of the developmental pathways to the explained variance of young adult depressive symptoms, we assumed directional associations from young adults’ relationship dissatisfaction and economic problems to their depressive symptoms. Missing data were accounted for using the full information maximum likelihood (FIML) procedure. FIML does not impute missing values; rather, it estimates model parameters and standard errors from all available data, which minimize potential age-related bias that would have influenced the results (Enders, 2001). We used the comparative fit index (CFI ≥ .95) and root mean square error of approximation (RMSEA ≤ .06) to evaluate model fit.
Results
Descriptive statistics and correlations among all study variables are shown in Table 1. The mean of depressive symptoms was 4.81, 3.89, and 4.46 for Waves 1, 3, and 4, respectively. Using the cut point of 6.4 (based on the usual cut point of 16 for 20 items), 25% of young adults (21 and 29% of men and women, respectively) in Wave 4 showed clinically significant depressive symptomology (Radloff, 1977). These percentages are compatible with the prevalence rates documented in other studies (Reisner et al., 2009).
Overall, the path analysis model (see Figure 2) accounted for 20% of the variance in young adults’ depressive symptoms, and the model fit the data well (CFI = 1.00, RMSEA = .01), χ2(df) = 10.47(6), p = .10.
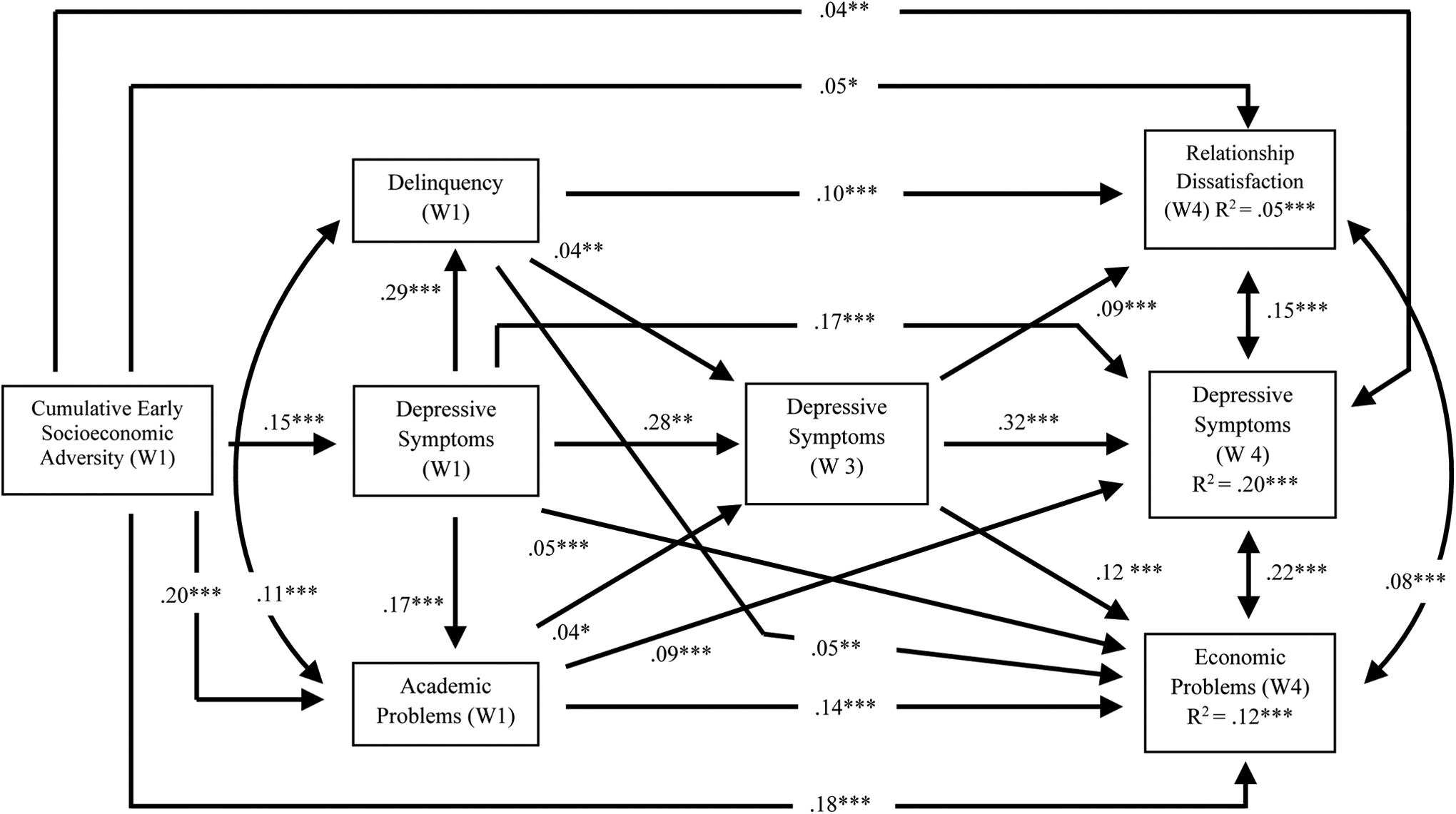
The results of the current study. Standardized regression coefficients are shown; nonsignificant pathways are not shown; Compared to Whites (reference group), Blacks experienced more relationship dissatisfaction (.13***) and more economic problems (.08***); Hispanics reported more delinquency (.03*) and less economic problems (−.04***); Asians experienced fewer academic problems (−.04**) and fewer economic problems (−.05***); multiracial youths reported more depressive symptoms during adolescence and young adulthood (.02* and .03**, respectively) as well as more delinquency (.03**) and more economic problems (.03*). Women reported more depressive symptoms than men at Wave 1 (.14***), Wave 3 (.08***), and Wave 4 (.05***). Women also reported more economic problems (.07***), but they experienced fewer academic problems (−.11***), less delinquency (−.17***), and less relationship dissatisfaction (−.06***). χ2(df) = 10.47 (6); Comparative fit index (CFI)/Tucker-Lewis index (TLI) = 1.00/.99; root mean square error of approximation = .01. *p < .05. **p < .01. ***p < .001.
Findings Related to Cumulative Socioeconomic Adversity and Depressive Symptoms Over Time
On average, adolescents experiencing more cumulative socioeconomic adversity reported higher levels of depressive symptoms during adolescence than those with less cumulative socioeconomic adversity (Wave 1, 1995; β = .15), suggesting that cumulative socioeconomic adversity is directly related to adolescents’ depressive symptoms. Also, there was statistically significant continuity in depressive symptoms from adolescence to emerging adulthood (β = .28) and from emerging adulthood to young adulthood (β = .32). These findings suggest a moderate level of continuity in the rank order of depressive symptoms across these life stages even after accounting for the influence of covariates. However, these stabilities are smaller than the zero-order correlations between these constructs (r = .31 and .38, respectively; see Table 1). Therefore, the zero-order correlations appear to be partly spurious due to the influence of covariates included in the model.
Findings Related to the Hypothesized Academic/Economic Developmental Risk Pathway
Adolescents with higher levels of depressive symptoms reported poorer academic performance compared to less depressed adolescents (β =.17), and poor academic performance was associated with the presence of more depressive symptoms in emerging adulthood (Wave 3 and β = .04). The chain of insults continued with depressive symptoms in adolescence and emerging adulthood explaining variation in young adults’ economic problems (β = .05 and .12), which, in turn, was related to experiencing more depressive symptoms in young adulthood (standardized coefficient = .22). Cumulative socioeconomic adversity was also directly related to adolescents’ academic problems (β = .20) and young adults’ economic problems (β = .18). Additionally, poor academic performance was also associated with increased economic problems in young adulthood (β = .14).
Findings Related to the Hypothesized Academic/Economic Developmental Risk Pathway
The findings also supported the existence of a delinquency/interpersonal developmental risk pathway. Those with more depressive symptoms as adolescents reported more delinquency than adolescents with fewer depressive symptoms (β = .29). In turn, delinquency was associated with emerging adults’ reports of their depressive symptoms (β = .04), and depressive symptoms in emerging adulthood were associated with relationship dissatisfaction (β = .09). Relationship dissatisfaction was more prevalent among young adults with high levels of depressive symptoms (standardized coefficient = .15). The model also revealed cumulative socioeconomic adversity and delinquency were associated with relationship dissatisfaction in young adulthood (β = .05 and .10, respectively).
Interplay Between the Two Hypothesized Pathways
There also appears to be interplay between the academic/economic and delinquency/interpersonal pathways. Adolescents with higher levels of delinquency also generally reported more academic struggles (standardized coefficient = .11) and more young adult economic problems (β = .05) than individuals with lower levels of delinquency. Moreover, there was a statistically significant association between young adults’ relationship dissatisfaction and their economic problems (standardized coefficient = .08).
Indirect Effects
Next, indirect effects were examined (see Table 2). There was a statistically significant indirect effect of early cumulative socioeconomic adversity on young adults’ depressive symptoms. The proportion of variance explained by the indirect pathways out of the total variance explained was calculated (see MacKinnon, Fairchild, & Fritz, 2007). Approximately 23% of the explained variance in young adults’ depressive symptoms was attributed to the academic/economic pathway examined. This is notably larger than the 4% of explained variance in young adults’ depressive symptoms that was attributed to the delinquency/interpersonal pathway.
Results of Indirect Tests for the Hypothesized Model.
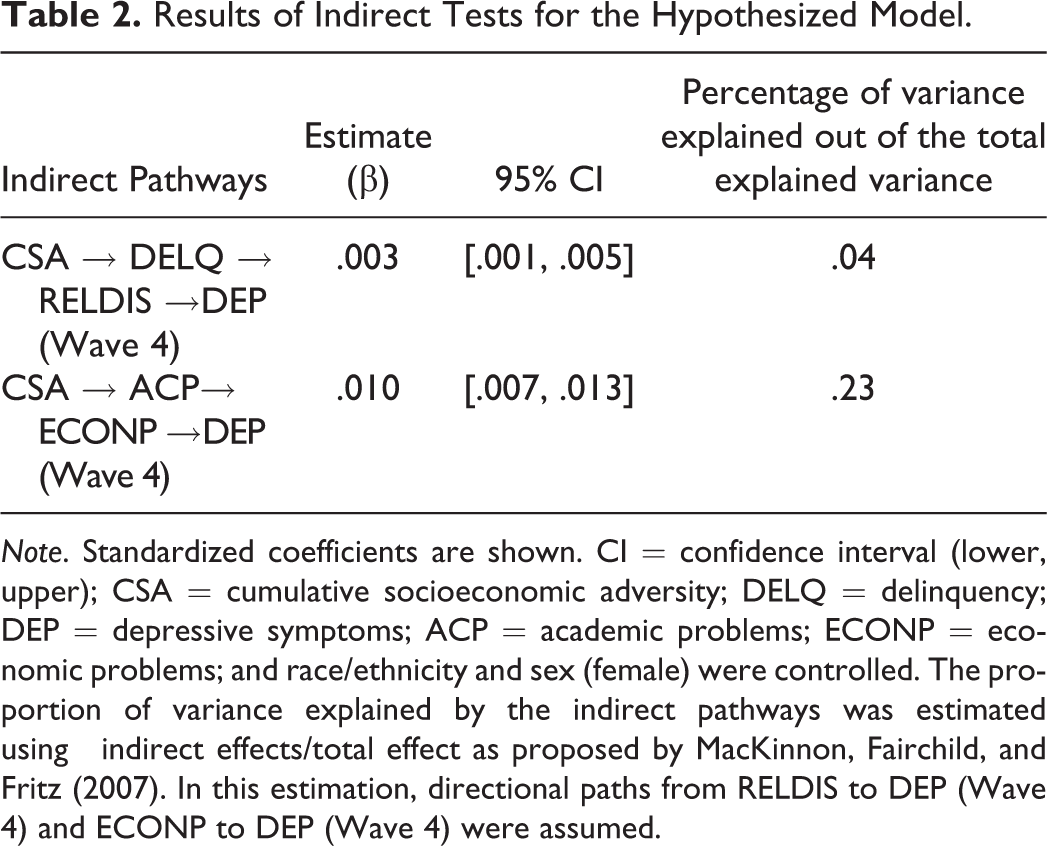
Note. Standardized coefficients are shown. CI = confidence interval (lower, upper); CSA = cumulative socioeconomic adversity; DELQ = delinquency; DEP = depressive symptoms; ACP = academic problems; ECONP = economic problems; and race/ethnicity and sex (female) were controlled. The proportion of variance explained by the indirect pathways was estimated using
Discussion
The primary goal of this study was to examine the influence of two developmental risk pathways stemming from cumulative socioeconomic adversity on the continuity and discontinuity of depressive symptoms from adolescence into young adulthood. Existing literature is fragmented with respect to theoretical and analytical models. To our knowledge, previous research has not utilized a single analytical framework to assess diverse life experiences as developmental pathways from adolescence into young adulthood in examinations of young adults’ depressed mood. Thus, the present study responded to this paucity of research by examining a life course cascading model that explored two developmental pathways linking cumulative socioeconomic adversity occurring before and/or during adolescence to young adults’ depressive symptoms.
In the present investigation, we captured cumulative socioeconomic adversity by generating a composite adversity index summing dichotomous indicators of low parental education, low family income, parents’ marriage instability, and community adversity. These various stressful circumstances are thought to combine to exert a unique effect that is considerably stronger than the independent effect of individual stressors (Brody et al., 2013). Thus, we expected that adolescents experiencing high levels of cumulative adversity were more vulnerable to depressive symptoms than adolescents experiencing low levels of socioeconomic adversity. Our delinquency/interpersonal developmental pathway included two developmental behavioral outcomes that are important for the specific life stages during which they were assessed: behavioral problems (delinquency) in adolescence and romantic relationship problems (relationship dissatisfaction) in young adulthood. Similarly, our academic/economic developmental pathway included behavioral outcomes that are particularly relevant for the specific life stages: educational underperformance (academic problems) in adolescence and lack of socioeconomic attainment (economic problems) in young adulthood.
In general, the results illustrated that early cumulative socioeconomic adversity initiates an adverse life course process. This is consistent with the findings of recent research focusing on early adversity and child/youth development (Evan & Kim, 2010). More specifically, cumulative socioeconomic adversity was associated with adolescents’ depressive symptoms. The stability of depressive symptoms over the early life course was statistically significant across life stages, including from adolescence to emerging adulthood and from emerging adulthood to young adulthood, and it appears that mediating life experiences associated with early socioeconomic adversity only partially explain the continuity of depressive symptoms. In addition, depressive symptoms in adolescence (1995) directly contributed to depressive symptoms in young adulthood (2008), bypassing depressive symptoms in emerging adulthood. Thus, early depressive symptoms appear to have long-term mental health consequences regardless of individuals’ life experiences during emerging adulthood. These findings are in line with previous research documenting strong homotopic continuity in depressive symptoms from adolescence into young adulthood (Carballo et al., 2011).
Furthermore, the results showed that cumulative socioeconomic adversity was directly associated with the academic/economic pathway (low grade point average in adolescence and economic stress in young adulthood) and the behavioral pathway (relationship dissatisfaction in adulthood), and these two pathways were implicated in young adults’ levels of depressive symptoms. In addition, adolescent depressive symptoms stemming from cumulative socioeconomic adversity were also associated with both delinquency/interpersonal and academic/economic developmental pathways leading to depression in young adulthood. This is consistent with the notion of a “kindling effect,” which suggests that the consequences of depression increase the likelihood of later depression (Rudolph et al., 2009). It appears that, although stressful experiences during adolescence are linked to failures during young adulthood as a chain of insults with one stressor relating to another subsequent stressor, one failure/hardship may also continue while another appears, forming a cascading sequence of stress, or a stress “convoy” (Hatch, 2005). For example, academic problems during adolescence were directly associated with young adults’ depressive symptoms, even after accounting for the influence of young adults’ economic problems. Also, relationship dissatisfaction in young adulthood was associated with depressive symptoms in adolescence (Wave 1, 1995), even after controlling for the influence of depressive symptoms in emerging adulthood (Wave 3, 2001). This cascading sequence of stressful experiences from adolescence to young adulthood is consistent with the life course “cascade model” (Brody, Chen, & Kogan, 2010).
More importantly, as shown in Figure 2, cumulative socioeconomic adversity was directly related to young adults’ socioeconomic attainment over and above the risks accounted for at earlier stages of the life course. This is consistent with the intergenerational transmission of socioeconomic adversity hypothesis. It seems that there are other social, psychological, and cognitive pathways, not specified in the present analysis, through which socioeconomic adversities impact young adults’ lives. These mediating pathways may involve various resources, such as parental support, self-esteem, mastery, self-control, self-regulation, and future orientation (Melby, Conger, Fang, Wickrama, & Conger, 2008; Wickrama & O’Neal, 2013).
Although findings from the present study are generally consistent with the hypothesized model, several factors potentially limit the scope and generalizability of the results. First, future replications should involve alternative, more objective measures. Use of objective measures will reduce potential self-report biases (e.g., teacher reports of grades, observational measures of young adult relationship dissatisfaction, and tax returns for socioeconomic attainment). For instance, the use of self-reported relationship dissatisfaction may bias the results because individuals with higher levels of depressive symptoms may be more likely to view their romantic relationships negatively. It should also be noted that those with high levels of depressive symptoms may be less likely to have a romantic relationship. For example, in the study sample, the average level of depressive symptoms in young adults without a romantic relationship was significantly higher (M = 4.92 and SD = 3.75) than the average level of depressive symptoms in young adults with a romantic partner (M = 4.35 and SD = 3.61; t = 7.32, df = 14,561, and p < .001). Consequently, the study findings do not apply to individuals without a romantic partner. Second, although, in many instances, the use of longitudinal data is a strength of the current study, in some instances the temporal ordering of available data was not ideal and limited our ability to draw temporal conclusions. For instance, while we hypothesized a directional effect with cumulative socioeconomic adversity leading to delinquency, delinquency and cumulative socioeconomic adversity were both assessed at Wave 1. Furthermore, the delinquency measure assessed the previous 12 months, whereas at least one indicator of socioeconomic adversity (family economic hardship) captured only the preceding month. Similarly, while we hypothesized that academic problems and delinquency are an outgrowth of adolescent depressive symptoms, all three of these constructs were measured at Wave 1. Third, potential confounding variables may exist that were not considered in the present study, such as a disrupted adolescent transition (e.g., dropping out of school and teenage pregnancy), which may influence depressive symptoms both during adolescence and during young adulthood, causing a spurious association.
Despite these limitations, the present study makes a valuable contribution to existing research by elucidating how early life contexts contribute to academic/economic and delinquency/interpersonal pathways leading to different depressive symptom outcomes in young adults. The results demonstrate that, although there is a substantial and persistent association between early life experiences and young adult depressive symptoms through mediating pathways, there is significant continuity in depressed mood over the early years.
This study demonstrated that early social disadvantage significantly contributes to adolescents’ elevated depressive symptoms, delinquency, and academic failure. These findings emphasize the possibility of detecting emotional problems early in life and the need for federal, state, and local policies and programs designed to reduce childhood adversity. In addition, the findings emphasize the need for programs that promote characteristics that convey resilience in coping with adolescent developmental risks. The results of the present study also suggest that an improved understanding of the reciprocities between depressive symptoms, behavioral problems, such as delinquency, and academic/economic failure may lead to more effective interventions that are able to address these mutual influences. The interplay found between depressive symptoms, delinquency, and academic/economic failure also highlights the need for multifocused mental health programs as there is significant continuity between these risks. Consequently, identifying youth who experience early risk factors, such as academic problems or delinquency, may facilitate interventions that are able to reduce the continuity of depressive symptoms before a chronic course of depressive symptomatology is established. Furthermore, the continuity of depressive symptoms from adolescence into young adulthood emphasizes the need for ongoing psychological care for depressed adolescents. For many adolescents exhibiting depressive symptoms, these symptoms should be conceptualized and treated as a chronic condition that will likely persist over multiple life stages. While the treatment of these symptoms is not “hopeless,” treatment that takes a long view rather than attempting a “quick fix” may be most beneficial.
Footnotes
Authors’ Note
Acknowledgments
This research uses data from Add Health, a program project directed by Kathleen Mullan Harris and designed by J. Richard Udry, Peter S. Bearman, and Kathleen Mullan Harris at the University of North Carolina at Chapel Hill, and funded by grant P01-HD31921 from the Eunice Kennedy Shriver National Institute of Child Health and Human Development, with cooperative funding from 23 other federal agencies and foundations. Special acknowledgment is due Ronald R. Rindfuss and Barbara Entwisle for assistance in the original design. Information on how to obtain the Add Health data files is available on the Add Health website (![]() ). No direct support was received from grant P01-HD31921 for this analysis. We are thankful to Jennifer Tanner for her constructive comments on an earlier draft of this manuscript.
). No direct support was received from grant P01-HD31921 for this analysis. We are thankful to Jennifer Tanner for her constructive comments on an earlier draft of this manuscript.
Authors' Contribution
Kandauda A. S. Wickrama contributed to conception and design, contributed to analysis and interpretation, drafted the manuscript, critically revised the manuscript, gave final approval, and agrees to be accountable for all aspects of work ensuring integrity and accuracy. Catherine Walker O'Neal contributed to conception and design, contributed to analysis and interpretation, drafted the manuscript, critically revised the manuscript, gave final approval, and agrees to be accountable for all aspects of work ensuring integrity and accuracy. Tae Kyoung Lee contributed to conception and design, contributed to analysis and interpretation, critically revised the manuscript, gave final approval, and agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.