
Abstract
Effective self-report screening tools for emerging adults are understudied. The present study examined the latent structure of the Depression, Anxiety, and Stress Scales (DASS-21) with U.S. undergraduates. Data were collected from 1,413 undergraduates surveyed online. Three models were tested: (a) a one-factor model, (b) the original correlated three-factor model, and (c) a bifactor model that included a general negative affectivity factor and three specific factors of depression, anxiety, and stress. The bifactor model with three specific orthogonal factors yielded the best fit. All items loaded onto the general negative affectivity factor. This study provides an important evaluation of alternative models of the latent structure of the DASS among U.S. undergraduates, with results supporting it as an assessment of general distress for emerging adults.
Depressive and anxiety disorders often emerge during late adolescence and emerging adulthood, yet the majority of this population does not receive treatment (Downs, Boucher, Campbell, & Dasse, 2013; Judd, 1997). Approximately 70% of 18- to 22-year-olds in the United States attend college (U.S. Bureau of Labor Statistics, 2015), and during the school year, typically more than 50% report overwhelming anxiety and almost a third experience severe depression that interferes with their functioning (American College Health Association, 2014). College counseling centers across the United States employ a wide range of measures for screening and assessing mental health distress in students. However, the disproportionate rates of mental health problems and service utilization among U.S. college students emphasize that it is essential to improve identification of students in need of services (Downs et al., 2013).
Many assessments currently used in college counseling centers were not developed specifically for a college population, for example, the Beck Depression Inventory (Beck, Ward, Mendelson, Mock, & Erbaugh, 1961) or the Outcome Questionnaire-45 (Lambert et al., 1996). Some measures were created for college students, but evidence of their reliability and validity is limited, or they are too lengthy for widespread use or monitoring progress (Locket et al., 2011). Another challenge is that some measures are symptom-specific scales, while others are more focused on a global measure of distress. In particular, the extent to which depression and anxiety can be measured as distinct constructs is limited, as these highly comorbid psychopathological symptoms often occur in the context of underlying, shared etiological and maintenance processes (Andrews et al., 2009; Kessler, Berglund, & Demler, 2005). Given this high comorbidity, Clark and Watson (1991) called for a tripartite model that considered three factors: depression, hyperarousal, and general distress—a nonspecific component described as negative affectivity (Watson & Clark, 1984). Whether distinct factors hold for emerging adults, and their applicability in measurement has implications for being able to identify appropriate, reliable, and easy to administer screeners that provide opportunities for earlier identification of risk and more targeted interventions.
The Depression, Anxiety, and Stress Scales (DASS) was originally developed to individually assess for both anxiety and depression, but initial validation efforts pointed to a third “negative affectivity” factor that was termed the Stress subscale. The DASS was first validated among a nonclinical sample aged 17–69 years (Lovibond & Lovibond, 1995), with the purpose of indicating a need for further assessment rather than providing a specific diagnosis (Byrd & Alschuler, 2009; Kessler, 2009).
Despite its wide use of the DASS-21, there are continuing questions as to whether it measures distinct latent features or one general factor (Watson & Clark, 1984). For example, a parallel analysis of adolescent data concluded that the DASS-21 is unidimensional (Patrick, Dyck, & Bramston, 2010). Other studies using confirmatory factor analysis (CFA) have found support for a bifactor structure. Other research offers support for a bifactor model including a general negative affectivity factor and the expected three specific factors of depression, anxiety, and stress with both general adult (Bottesi et al., 2015; Henry & Crawford, 2005) and college student samples (Osman et al., 2012).
Research on the use of the DASS and its psychometrics within an undergraduate population remains limited. Osman and colleagues (2012) conducted the only study (known to these authors) supporting a bifactor model of the DASS-21 with U.S. undergraduates. Their sample was relatively homogenous (70% were White and 78% were in Year 1 postsecondary school), and the authors note the need to examine the DASS-21 bifactor structure with diverse samples of U.S. undergraduates. Thus, the current study evaluated the factor structure of the DASS-21 (Lovibond & Lovibond, 1995), including U.S. undergraduate from an ethnically diverse campus, and including all school years, to consider its potential as a mental health screener.
Method
Participants
A total of 1,413 (35.3% response rate; 36.0% male, 63.4% female, 0.5% other) undergraduates (Mage = 20.0 years, SD = 1.8) completed an online survey (Year 1 = 24.8%, Year 2 = 19.0%, Year 3 = 28.3%, and Year 4 = 27.9%) administered by the campus Research Office. The Research Office recruited participants by e-mailing a random sample of 4,000 of all 20,200 enrolled undergraduates. The ethnicities of the participants were as follows: White 45.3%, Asian American 27.7%, Latino 25.1%, Middle Eastern 3.4%, South Asian 3.1%, African American 3.0%, Pacific Islander 2.5%, Alaskan/Native American 1.7%, and other ethnic identification 3.1%.
Measures
Adaptation of DASS-21 for U.S. college students
The DASS-21 (Lovibond & Lovibond, 1995) is a 21-item measure and includes three scales—depression, anxiety, stress—that each contains 7 items. Respondents rate (0 = did not apply to me at all to 3 = applied to me most of the time) the extent to which each item has applied to them over the past week. Previous studies reported high α coefficients (depression α = .97, anxiety α = .92, stress α = .95; Antony, Bieling, Cox, Enns, & Swinson, 1998), with strong convergent validity with other measures of depression and anxiety (r = .79, r = .68, and r = .68, respectively; Antony et al., 1998).
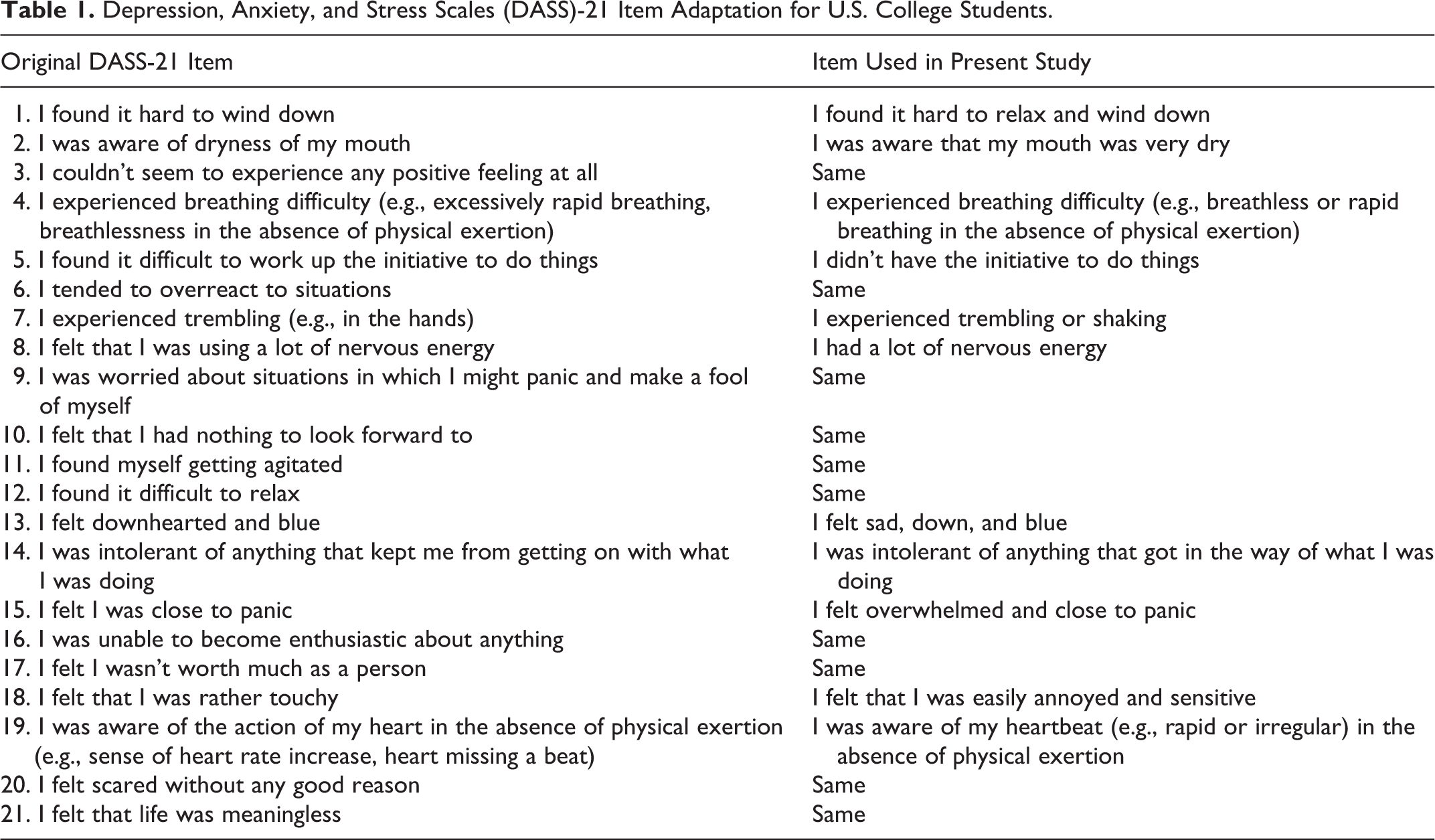
Because the DASS-21 was developed in Australia and previous studies have identified items with possible poor fit, we slightly modified the DASS-21 item wording. We collected data from 32 undergraduate students who completed the original scale and answered questions about the ease of understanding, commonality of words/phrases used, and relevance of items to the U.S. college students’ experiences. Item revisions were determined based on these data and consensus of three of this study’s investigators. Table 1 shows the minor wording adaptations.
Depression, Anxiety, and Stress Scales (DASS)-21 Item Adaptation for U.S. College Students.
Statistical Analyses
Data screening and descriptive analyses were performed using SPSS Version 23. Mplus Version 7.2 (Muthén & Muthén, 2013) was used to examine the factor structure of the DASS-21 using weighted least squares with mean and variance adjustment estimation for ordinal indicator variables (Rhemtulla, Brosseau-Liard, & Savalei, 2012). To evaluate the fit of the tested models, the following fit indices were examined: χ2 test of model fit, comparative fit index (CFI; Bentler, 1990), Tucker–Lewis Index (TLI), and root mean square error of approximation (RMSEA; Steiger & Lind, 1980). Good model fit was indicated by CFI and TLI values greater than .95 and RMSEA values less than .05; adequate fit was indicated by CFI and TLI values between .90 and .95 and RMSEA values between .05 and .08 (Hu & Bentler, 1999).
Three models were tested including a one-factor model (Model 1; e.g., Patrick et al., 2010), the original correlated three-factor model (Model 2; Lovibond & Lovibond, 1995); a bifactor model specifying general negative affectivity and orthogonal specific factors of depression, anxiety, and stress (Model 3; e.g., Henry & Crawford, 2005; Osman et al., 2012). To choose the best among three competitive models, model fit indices were used. Notably, the determination of best fitting model was based on ΔCFI, when the differences in CFI values between models were less than .002 (Meade, Johnson, & Braddy, 2008)—this showed the stable results under various conditions (i.e., sample size, number of factors and items).
Results
Descriptive Statistics and Scale Intercorrelations
The correlations for the total sample (N = 1,413) among the three DASS-21 subscale scores ranged from .66 to .72 (compared to .53 to .67 reported by Osman et al., 2012). The average subscale scores (range = 0–21) were as follows: depression (M = 4.1, SD = 4.3), anxiety (M = 3.9, SD = 3.6), and stress (M = 6.0, SD = 4.1). The DASS-21 combined total score (0–63) was comparable to previous findings (Osman et al., 2012) at a mean of 14.1 (SD = 10.6). Coefficient ω values for the total score, depression, anxiety, and stress subscales were .96, .94, .87, and .89, respectively, indicating strong reliability. A correlation matrix (Online Appendix 1) shows all interitem and subscale correlations and item response means.
Alternative Latent Trait Model Testing
Table 2 presents the fit statistics for each of the three tested models. Model 1 yielded poor fit, whereas Model 2 yielded adequate fit. Furthermore, the increase in CFI values was .06 (larger than cutoff = .002) for this comparison, indicating better fit in Model 2 than 1. Model 3 indicated better fit than Models 1 and 2. The increase in CFI (.026) supported Model 3. Based on these indicators, the bifactor model with three specific factors (Model 3) exhibited the best fit. For the bifactor model with three specific factors (Model 3), loadings of the items onto the general and specific factors (see Table 3) indicate strong to very strong relations between each item and the general factor, with these relations consistently being stronger than those of items with a specific factor. A majority of the specific loadings of items on the anxiety and stress factors are negligible with two of the items on the anxiety factor yielding nonsignificant loadings.
Fit Statistics for Each of the Tested Models.
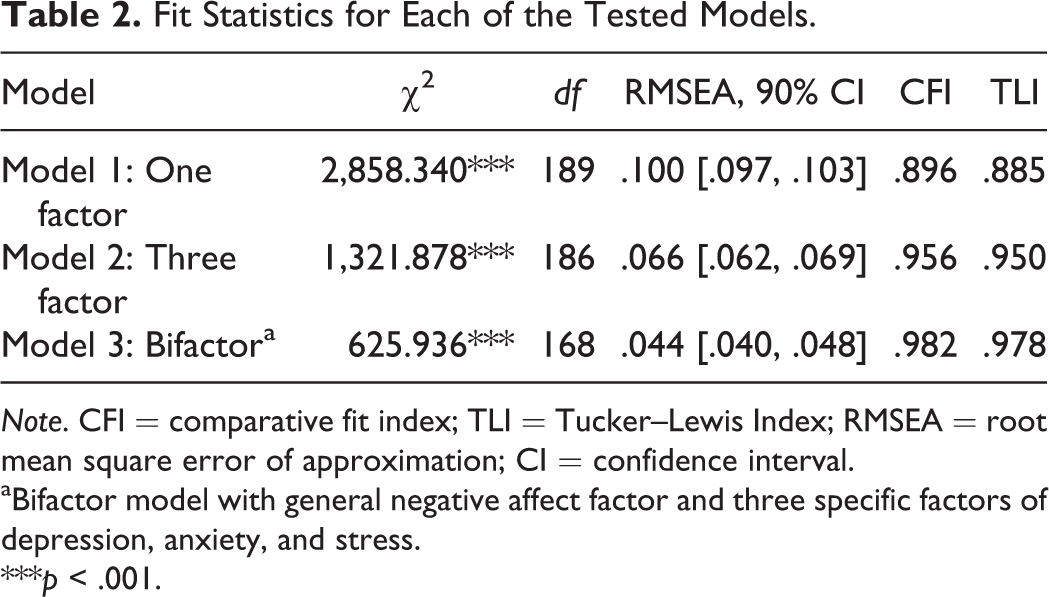
Note. CFI = comparative fit index; TLI = Tucker–Lewis Index; RMSEA = root mean square error of approximation; CI = confidence interval.
aBifactor model with general negative affect factor and three specific factors of depression, anxiety, and stress.
***p < .001.
Standardized Factor Loadings.
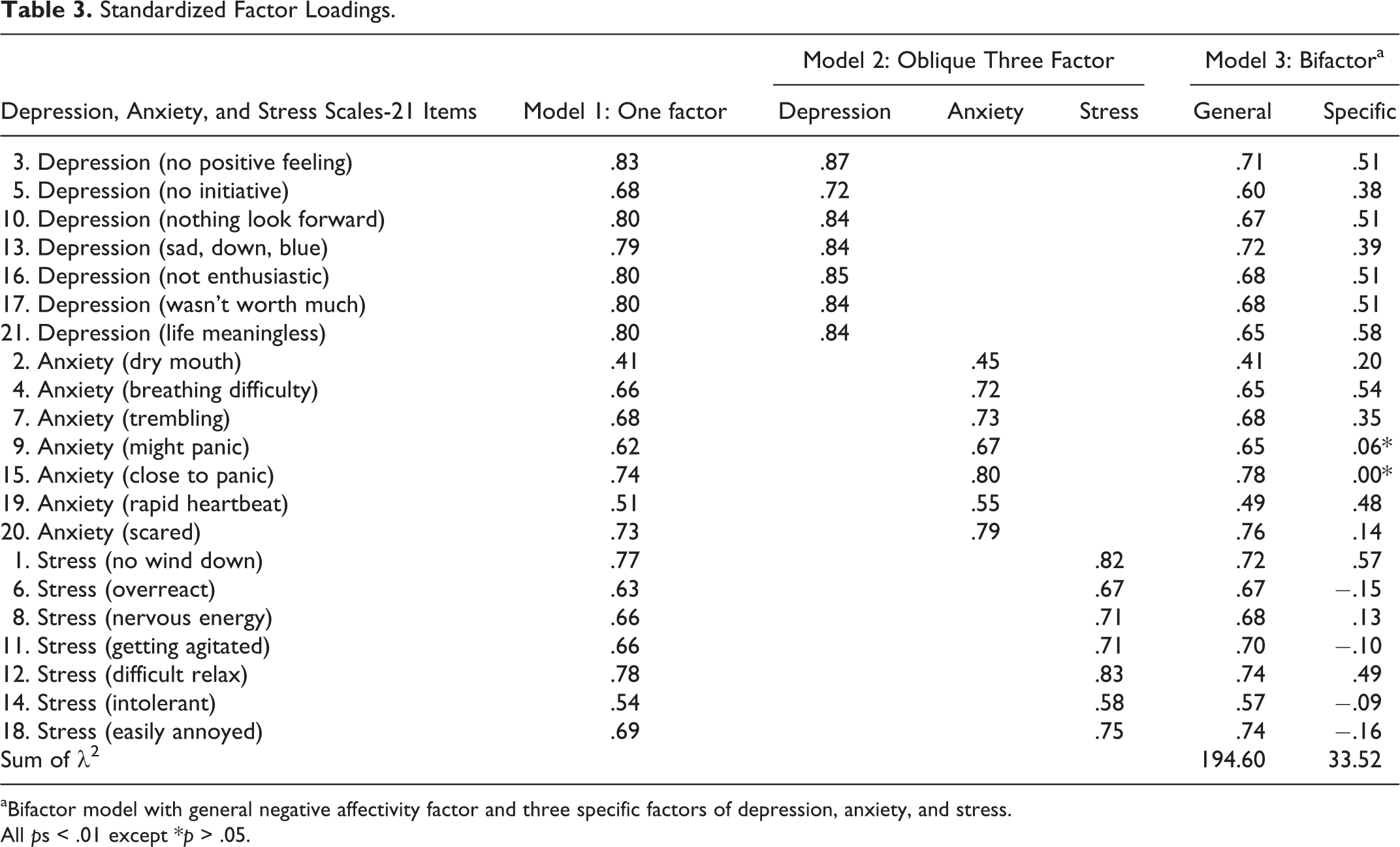
aBifactor model with general negative affectivity factor and three specific factors of depression, anxiety, and stress.
All ps < .01 except *p > .05.
When examining reliability of general and specific factors, ω coefficients are recommended to exceed .50, but .75 is preferable (Reise, 2012; Reise, Bonifay, & Haviland, 2012). Although the ω hierarchical coefficient exceeds this criteria, ω h = .89, the ω subscale coefficients for the depression (ωs = .32), anxiety (ωs = .12), and stress (ωs = .02) factors, which control for the influence of the general factor, were well below the recommended criteria. Thus, support is offered for a strong general factor. The explained common variance (ECV) further confirms the presence of a strong general factor (ECV = .76). In a summed total score of the DASS-21 items, 89% of the variance in the total score would be attributed to the general factor.
Discussion
This study evaluated the latent structure of the DASS-21 among U.S. undergraduates, providing empirical evidence for its utility as a mental health screener for emerging adults. Results suggest that a bifactor model with three specific orthogonal factors of depression, anxiety, and stress had the best fit. Although the three-factor structure proposed in the development of the DASS-21 exhibited adequate fit, Model 3 bifactor results and computed ω coefficients support a strong general factor, called negative affectivity in accordance with a tripartite or quadripartite structure.
Whereas higher order models specify the relation between the general factor and individual items to be fully mediated by the first-order factors (Morgan, Hodge, Wells, & Watkins, 2015; Murray & Johnson, 2013), bifactor models acknowledge both the general factor and specific factors as having a direct impact on items. Similarly, working within a tripartite model of internalizing conditions, both a general negative affectivity dimension and specific features associated with each of depression and anxiety are theorized to contribute to these internalizing syndromes (Clark & Watson, 1991). That is, physiological hyperarousal or anhedonia (i.e., low positive affect) unique to anxiety and depression, respectively, is believed to contribute to these conditions in addition to negative affectivity—each exerts influence, and negative affectivity’s impact is not fully mediated by the unique features of anxiety and depression. In addition, bifactor models, but not higher order models, allow for empirical examination of the viability of the use of total and subscale scores when data are believed to be multidimensional. Given that the DASS-21 was intended to provide subscale scores associated with severity of depression, anxiety, and stress symptoms (Lovibond & Lovibond, 1995), but also that a total score indicative of general distress may also be useful within screening contexts and early identification frameworks, we wished to examine the appropriateness of a total score. Bifactor models further allow for examination of the adequacy of subscale scores, given the use of a total score. Therefore, testing bifactor models in addition to other previously supported CFA structures was deemed most appropriate.
In particular, in this study, all items exhibited strong loadings on the general factor, each of which was consistently stronger than the item loadings on the specific factors. In addition, the item loadings on the specific factors within the bifactor model, accounting for shared variance across all items, are consistently stronger than the item loadings of the oblique three-factor solution, indicating that item variance is largely associated with the general underlying construct rather than specific variance (Reise et al., 2012). Further, examination of ω hierarchical and subscale coefficients and ECV further confirmed a majority of DASS-21 item variance to be attributed to a common construct associated with the scale’s items with minimal remaining variance associated with constructs specific to depression, anxiety, and stress.
There is building evidence that the DASS-21 includes a general factor explaining the bulk of its shared interitem variance (Daza, Novy, Stanley, & Averill, 2002; Sinclair et al., 2012). In the current study, a general factor explained a majority of the variance (89%) of the total score. This finding is consistent with Osman and colleagues (2012), indicating that, with U.S. college students, there is insufficient evidence to warrant the use of the DASS-21 subscales as latent measures. Additionally, Osman and colleagues’ (2012) research suggests that the DASS-21 might be efficiently measured with 4 items per subscale. Findings from the current study were generally consistent with this work by also identifying three matching depression (3, 13, and 17) and stress (11, 12, and 18) items as strong indicators of general negative affectivity. Inconsistent with the Osman and colleagues’ past work, however, there was only one Anxiety item (7) among the strongest bifactor general items. There was also one Anxiety item (2) asking participants to report the sensation of a “dry mouth,” which loaded poorly across models and ostensibly may not be an adequate measure of anxiety to include. A notable result of this study was that all 21 items had acceptable loadings (>.30) on the general factor; it is possible that a balanced combination of DASS-21 items, when there is an interest to use fewer items, would produce similar results. It may be useful for future research to examine briefer versions of the scale.
Although the stress items had low specificity in the bifactor model analysis, they nonetheless retained higher loadings on the general factor. Although the stress items do not directly measure mental distress symptoms, they are meaningful with college samples because of the common stressors (i.e., balancing academic tasks with work schedules, healthy social engagement, etc.). Hence, these items have implications regarding assessment and treatment delivery.
The current findings also contribute to the theoretical models (e.g., Clark & Watson, 1991), and literature on common factors underlying emotional disorders, providing empirical support for a strong general factor of negative affectivity. In addition to provide evidence to guide researchers and clinicians in their screening practices, this research aligns with clinical efforts to implement a transdiagnostic approach in treatment (Newby, McKinnon, Kuyken, Gilbody, & Dalgleish, 2015). The results of this study can directly inform applied use of the DASS-21 with college students. In particular, scoring is important to consider. Subscale scores reflect a combination of common and unique variance associated with negative affectivity and each of the three subscales of depression, anxiety, and stress. Little variance in each composite subscale score reflects variance unique to depression, anxiety, or stress. Thus, for use as a screening tool, clinicians may utilize a DASS-21 total score that provides a more reliable measure of unique variance associated with an individual’s score and is indicative of internalizing symptoms that can be further assessed and treated. Having access to a short screening tool that incorporates mental health issues common to college student populations, the DASS-21 has the potential to readily be streamlined into college and university health system assessments.
Limitations
This study included an undergraduate sample attending a West Coast University, who completed an online survey at a single time point. The potential generalization of these findings is thereby limited, given the restricted sample and the 35% response rate. It is helpful to note that prior research suggests survey response rates as low as 5–10% are reliable when drawn from a sampling frame of at least 500 college students (Fosnacht, Sarraf, Howe, & Peck, 2017). Although procedures were taken to carefully reword items to be more meaningful for U.S. participants, the reliability, construct validity, and general psychometrics of the revised items created in this study remain in question and should be examined in future research. Future research longitudinally examining the predictive ability of negativity affectivity in regard to student psychopathology as well as socioemotional health is also warranted.
Conclusion
The current findings have implications for assessment in prevention and intervention during emerging adulthood. Results support use of the DASS-21 as part of an efficient universal monitoring assessment of college students’ mental health and well-being. In particular, as a robust measure of general distress with strong psychometric properties, the DASS-21 can help to quickly assess mental health in college counseling centers and college health clinics and, with growing attention to empirically assessing quality of care, to monitor the effects of campus wellness programs (Sinclair et al., 2012).
Supplemental Material
Online_Appendix - Structural Validity of the Depression, Anxiety, and Stress Scales-21 Adapted for U.S. Undergraduates
Online_Appendix for Structural Validity of the Depression, Anxiety, and Stress Scales-21 Adapted for U.S. Undergraduates by Maryam Kia-Keating, Unkyung No, Stephanie Moore, Michael J. Furlong, Sabrina Liu, and Sukkyung You in Emerging Adulthood
Footnotes
Author’s Note
This research was conducted under approval by the University of California, Santa Barbara, Office of Research, institutional review board. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants included in the study.
Author Contributions
Maryam Kia-Keating contributed to conception, design, acquisition, analysis, and interpretation; drafted the manuscript; critically revised the manuscript; gave final approval; and agrees to be accountable for all aspects of work ensuring integrity and accuracy. Unkyung No contributed to analysis and interpretation, drafted the manuscript, critically revised the manuscript, gave final approval, and agrees to be accountable for all aspects of work ensuring integrity and accuracy. Stephanie Moore contributed to interpretation, drafted the manuscript, critically revised the manuscript, gave final approval, and agrees to be accountable for all aspects of work ensuring integrity and accuracy. Michael J. Furlong contributed to conception, design, acquisition, analysis, and interpretation; drafted the manuscript; critically revised the manuscript; gave final approval; and agrees to be accountable for all aspects of work ensuring integrity and accuracy. Sabrina Liu contributed to interpretation, drafted the manuscript, critically revised the manuscript, and agrees to be accountable for all aspects of work ensuring integrity and accuracy. Sukkyung You contributed to analysis and interpretation.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.