
Abstract
There is a consensus among addictions researchers and clinicians that mental health concerns and substance use problems are often interrelated. It is less clear to what extent the general public, and university students in particular, understand connections between substance use and mental health. The current study aimed to understand university students’ perceived links between substance use and mental health by conducting three semistructured focus groups (N = 24 participants, 67% female). Thematic analysis of the data yielded five themes: (1) Students use substances to cope with mental health issues, (2) substance use can lead to mental health problems, (3) links between mental health and substance use are cyclical, (4) substance use is an aspect/indicator of mental health, and (5) substance use and mental health are not always linked. Findings provide insight into the understudied area of perceived links between substance use and mental health and have implications for campus programming.
There is a broad consensus among addictions researchers and clinicians that mental health concerns and substance use problems are often interrelated. According to a national U.S. epidemiologic study by Grant et al. (2004), 20% of respondents with a substance use disorder experienced comorbid mood/anxiety disorders, whereas proportions in the general population are closer to 5% for generalized anxiety disorder and depression (Kessler et al., 2005; Pratt & Brody, 2008). A national Australian survey yielded estimates closer to 30% for alcohol use disorders that were comorbid with at least one other mental disorder (Burns & Teesson, 2002). In the same way, individuals with mental illnesses exhibit a high lifetime prevalence of substance use disorders (Cuffel, 1996). Indeed, strong co-occurrences have been documented between a range of psychopathologies and various forms of substance use and abuse. This (nonexhaustive) list includes alcohol use disorder comorbid with social anxiety and depression (Grant et al., 2004; Hasin & Grant, 2002; Stewart, Morris, Mellings, & Komar, 2006); cannabis use disorder comorbid with psychosis, anxiety, and depression (Degenhardt, Hall, & Lynskey, 2003; Hall, 1998; Linszen, Dingemans, & Lenior, 1994; Patton et al., 2002); and hallucinogen and stimulant use disorders comorbid with psychosis (Curran, Byrappa, & McBride, 2004; Geyer & Vollenweider, 2008; González-Maeso et al., 2008).
Interrelations between substance use/abuse and mental health problems (i.e., thought, behavior, or emotion patterns that are distressing or impairing) can be grouped into four primary themes, according to the scientific literature. (1) Individuals use substances to self-medicate or cope with preexisting mental health problems (Dawson, Grant, Stinson, & Chou, 2005; Hasin, Goodwin, Stinson, & Grant, 2005; Khantzian, 1985, 1997; Lasser et al., 2000; Stewart, Grant, Mackie, & Conrod, 2016). (2) Mental health problems represent direct (e.g., drug-induced symptoms) or indirect (e.g., symptoms brought on by drug-related interpersonal or financial problems) outcomes of substance use (Dawson et al., 2005; Grant et al., 2004; Patton et al., 2002; Ross, 1995; Stewart et al., 2016). (3) Mental health problems and substance use co-occur due to other interrelated factors (e.g., social, biological, and contextual factors), which confer vulnerability for both mental health problems and substance (ab)use (Menezes et al., 1996; Patton et al., 2002; Stewart et al., 2016). (4) Mental health problems and substance abuse may also exist in a vicious cycle, whereby individuals experience comorbidity through mechanisms (1) or (2), but a bidirectional cycle maintains both disorders (Stewart & Conrod, 2007). The relative value of each of these accounts in explaining the relation between mental illnesses and substance use seemingly depends on a number of factors including individual traits, the type of substances being used/abused, and the type of mental health problem or psychopathology in question (Bowers & Swigar, 1983; Kushner, Sher, & Beitman, 1990; Patton et al., 2002; Stewart, Zvolensky, & Eifert, 2001). Nonetheless, as a whole, the extant research provides evidence for the presence of a reliable (albeit complex) relation between substance misuse and mental health problems.
Clinicians and mental health researchers appear to be well aware of associations between substance use and mental health, based on the growing body of research in this area, as well as the routine screening of comorbid mental health and substance use disorders in clinical practice (de Beurs et al., 2011). What is less clear is the degree to which the general public understands connections between substance use and mental health. Research on lay perceptions has focused almost exclusively on conceptions of substance use or mental health, but not associations between the two (e.g., Phelan, Link, Stueve, & Pescosolido, 2000; Rhodes, 2000). For instance, Kuppin & Carpiano (2008) examined adults’ lay appraisals of causal factors and treatment options for mental health and substance use problems but did not assess beliefs regarding comorbidity. In a related study, Martin, Pescosolido, and Tuch (2000) compared stigma toward individuals with mental health problems and stigma toward individuals with substance use problems in the general U.S. adult population but did not examine attitudes toward individuals with a dual diagnosis. Clearly, research on lay perceptions of relations between substance use and mental health is lacking. One exception is a study by Link, Phelan, Bresnahan, Stueve, and Pescosolido (1999) who analyzed respondents’ responses to vignettes in a nationwide American social survey, revealing that less than half of the respondents recognized alcohol or drug abuse as a mental health issue. However, this study was solely quantitative and, thus, did not present participants’ own personal accounts of links between substance use and mental health. Given the capacity of qualitative research to shed light on the intricacies of lay perceptions, a lack of qualitative research on the topic represents a notable gap in the literature.
Assessing lay understanding of links between substance use and mental health is crucial for several reasons. Namely, personal beliefs about substance use and mental health have the potential to shape individual and community responses to these issues for the better or worse. Lay appraisal of mental health and addictions issues occurs long before professional help is ever sought (Link, Phelan, Bresnahan, Stueve, & Pescosolido, 1999; Mann, Hosman, Schaalma, & de Vries, 2004), and so an early responsibility lies with the individual and the members of their social circles. Indeed, misinformation regarding connections between substance use and mental health could potentially influence the prevalence and severity of comorbid problems. A lack of awareness of substance-related mental health problems may place individuals at risk of developing substance-induced psychosis, anxiety, or other problems. In the same way, misconceptions about self-medication with substances may lead to increased rates of addictions problems resulting from using substances as a coping mechanism. As such, it is necessary to gauge general knowledge of links between mental health and substance use, so that misperceptions can be corrected through public campaigns.
One population that may warrant special consideration in evaluating perceived links between mental health and substance use is university students, considering that emerging adulthood is a time of heightened risk of substance use and misuse (Chen & Jacobson, 2012; Schulenberg & Maggs, 2002) as well as mental health problems (Patel, Flisher, Hetrick, & McGorry, 2007). For instance, in a population of university students surveyed about their mental health and help-seeking, 30% reported a perceived need for treatment for a mental or emotional problem in the past year (Eisenberg, Golberstein, & Gollust, 2007). Results from the U.S. National Comorbidity Study indicate that the average age of onset for most mental health problems is between 18 and 25 years of age (Kessler et al., 2005). More specifically, substance use disorders had a median age of onset of 20, whereas the median age of onset for anxiety and mood disorders varied from 10 to 30, depending on the disorder (Kessler et al., 2005). As such, the university years represent a centermost time of onset for both mental health problems and substance use problems. Indeed, findings from the National College Health Assessment Survey (Kwan, Faulkner, Arbour-Nicitopoulos, & Cairney, 2013) indicate high levels of binge drinking and mental health problems among Canadian University students. In fact, university students exhibit higher levels of alcohol intake than age-matched peers who do not attend university (O’Malley & Johnston, 2002).
Despite the high rates of both substance use and mental health problems among university students, relatively little research has examined university students’ perceptions of substance abuse and mental health problems. Moreover, work that has been conducted has investigated students’ experiences or opinions involving specific substances (Howard, Griffin, Boekeloo, Lake, & Bellows, 2007; Levy, O’Grady, Wish, & Arria, 2005; Young, Morales, McCabe, Boyd, & d’Arcy, 2005) or mental health concerns (Davies et al., 2000; Eisenberg et al., 2007). As is the case with research in the general population, there remains a need to investigate university students’ conceptions of substance use and mental health problems in tandem.
This population also has much to gain from campaigns that address attitudes toward mental health and substance use, given that many campuses have properties (e.g., tight-knit communities, student-led events, university-centered media, and advertising outlets) that lend well to far-reaching mental health initiatives. Indeed, many universities are devoting increased attention to these issues by providing students with mental health promotion and addiction prevention programming (DeJong, 2002; Glassman & Braun, 2010). However, campus programs and services tend to maintain segregation between issues of mental health and substance use, despite an awareness in the professional mental health community that these issues often co-present (Cuffel, 1996; Grant et al., 2004). Hence, research on students’ views of the overlap and links between mental health and substance use will be crucial in advising campus campaigns and resources.
Therefore, the current study aimed to provide insight into university students’ perceived links between substance use and mental health in hopes of identifying strengths and gaps in their understanding and providing guidance to future campus mental health and harm reduction initiatives. This research was conducted under the auspices of the Caring Campus Project, a Movember funded initiative.
Method
Focus Groups
Three focus groups were conducted in a private university meeting room within the university’s psychology department to obtain qualitative data about students’ perceptions of links between substance use and mental health. Participants were recruited by advertisements placed around campus and on social media sites. The focus group discussions were based on a semistructured, open-ended interview, centered on students’ beliefs about links between substance use and mental health. Mental health was not defined for participants but, rather, left open to their interpretation. Focus groups were facilitated by two trained researchers, one of whom was a postdoctoral fellow with expertise in university substance use culture, links between addiction and mental health in young people, and youth-targeted prevention initiatives, and the other was a research coordinator with training in mental health first aid for emerging adults. Both facilitators were White females, similar to the majority of focus group participants. Facilitators prompted participants, when necessary, used probing questions in attempt to get participants to elaborate, and shared the duty of keeping the discussion on topic. Questions were developed by the facilitators as well as by two primary investigators. Questions are presented in the Appendix.
Upon arrival to the focus group location, participants gave written informed consent. Confidentiality was maintained by asking participants to avoid repeating what was shared in the focus groups with others and by assuring participants that they would not be identified by name or any other identifying information during transcription or data analysis. Participants were informed that quotes from the focus groups may be published and consented to this during the informed consent process. At the end of the focus groups, participants were debriefed and compensated US$20 for their time. All focus group sessions were audio recorded and were transcribed verbatim at a later time. The transcriber did not assign participant identification numbers, as she could not be sure who was speaking in the recordings.
Focus Group Characteristics
A total of 24 participants took part in the three focus groups on links between substance use and mental health (nfocusgroup1 = 9, nfocusgroups2 = 9, and nfocusgroups3 = 6). Focus group participants ranged from 18 to 23 years of age, and the mean age of participants was 18.9 years (SD = 1.2). Most participants were first-year university students (66%), and the remainder were second- (28%) and third-year students (6%). Sixty-seven percent were female. Most participants lived in university residences (54%), followed by apartments or houses shared with friends (25%), family (13%), and alone (8%). Participants represented a range of degree programs including science (33%), health professions (25%), arts and social sciences (17%), computer science or business (8%), and other programs that were not specified (17%). Thirteen percent of focus group participants were international students. All students were attending a single public, urban university. Participants were required to have drank alcohol at least once in the past month to be eligible to participate, as we were interested in how students’ use of alcohol and other substances related with their perceived mental health. Students reported on their drinking quantity, in terms of the average number of drinks consumed on one occasion, and drinking frequency. On average, students drank twice a month and drank approximately five drinks in one sitting. These statistics are comparable to those reported in the Canadian National College Health Assessment Survey (Kwan et al., 2013), where over half of the students drank five or more alcoholic drinks in a single occasion within the past 15 days.
Data Analysis
We followed standard guidelines for thematic analysis (see Braun & Clarke, 2006), which involve studying all data items, generating organizational codes, identifying and reviewing themes, and defining and naming themes. Data items were not associated with any identifying information. One researcher divided the transcripts into data items such that each data item contained only one idea. All data items were assigned codes by the same researcher to summarize participant responses. After all preliminary coding had taken place, the coder met with another researcher to review and revise codes and then organize codes into theoretically meaningful themes and subthemes. Any disagreements were discussed until a consensus was reached. In order for saturation to be achieved, Krueger and Casey (2009) and Morgan (1998) recommend focus groups consist of 6–10 participants and three focus group sessions. After preliminary analysis of the three focus groups, theoretical saturation of the data was reached with significant repetition of themes emerging. Thematic analysis was an appropriate analytic technique, given that it dually enables exploration of the data along with determination of how the data corresponds with theory. Therefore, in the current study, thematic analysis permitted an examination of how students’ perceptions of links between substance use and mental health correspond with predominant themes in the scientific literature.
Results/Discussion
Participants reported four main ways in which substance use and mental health can be related: (1) Students use substances to cope with mental health issues, (2) substance use can lead to mental health problems, (3) links between mental health and substance use are cyclical, and (4) substance use is an aspect or indicator of mental health. A fifth theme was also observed, which centered on the notion that (5) substance use and mental health are not always linked. For Themes 1 and 2, several subthemes were identified, which are described below. Sample items are presented to illustrate participant quotes that correspond with each theme. 1 To quantify each of the respective response categories, and provide an estimate of relative importance to students, the number of responses assigned to each theme and subtheme was recorded, and the proportion of total responses associated with each (sub)theme was calculated. The majority of participants’ responses centered on Theme 1, whereby substance use was seen as a coping mechanism for dealing with stressors and other mental health issues (79 items in total). This finding emphasizes the role that students ascribe to substance use as a way of coping with life stressors and mental health problems. Comments regarding the effects of substance use on mental health (Theme 2) were less common (20 items). Several comments explained circumstances where substance use and mental health were cyclically linked (15 items; Theme 3), were overlapping (9 items; Theme 4), or were conditionally linked (15 items; Theme 5). A variety of substances emerged in the commentary, with alcohol being the most common (42 items), followed by cannabis (14 items), prescription drugs (6 items), caffeine (4 items), over-the-counter medications (3 items), cigarettes (1 item), heroin (1 item), and cocaine (1 item). The remainder of comments included mention of substances more generally (80 items). A summary of themes, subthemes, and descriptions of those (sub)themes is presented in Table 1.
Themes and Subthemes From Focus Groups on Links Between Substance Use and Mental Health.
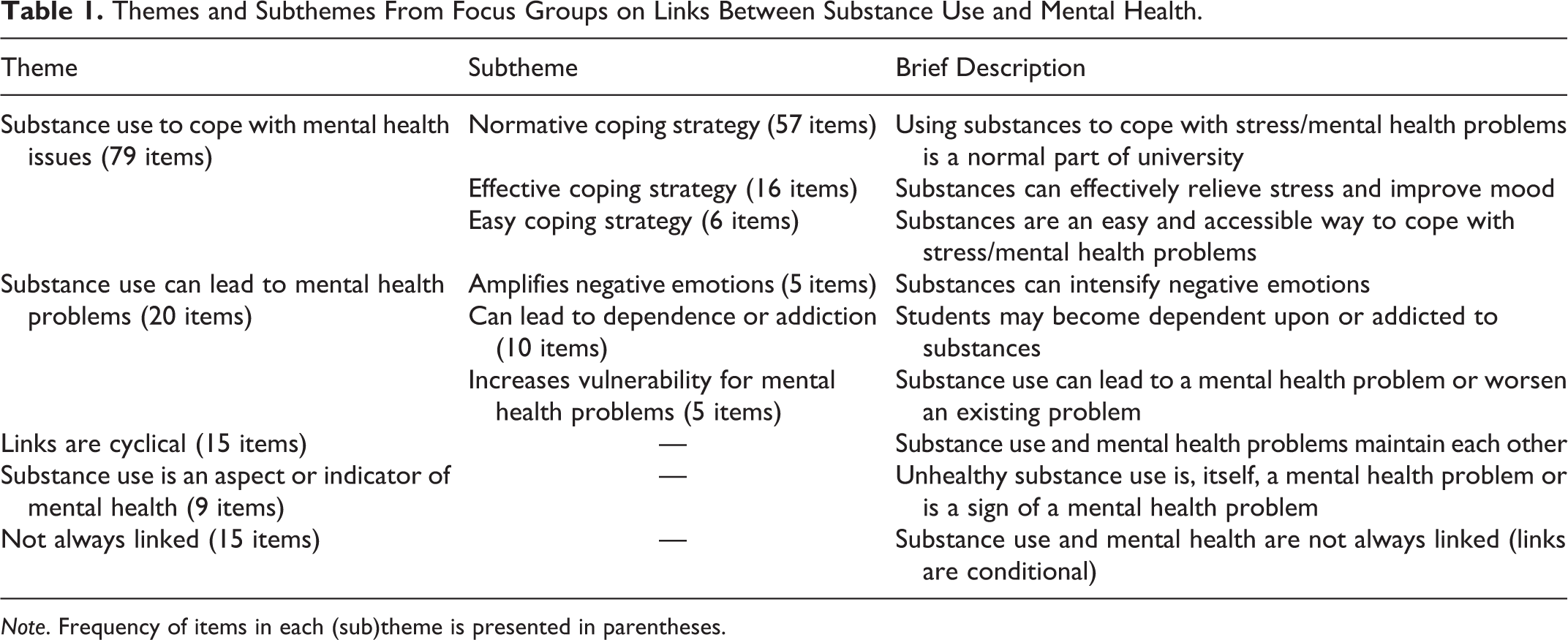
Note. Frequency of items in each (sub)theme is presented in parentheses.
Theme 1: Students Use Substances to Cope With Mental Health Issues
Students outlined a number of ways in which mental health can influence substance use. This theme fits well with a self-medication theory of substance abuse, which posits that individuals use substances to relieve affective and mental health problems (Khantzian, 1985, 1997). In this way, stress and other mental health concerns are viewed as factors that precede and elicit substance use. Three subthemes were apparent in students’ responses, revolving around the notions that using substances to cope is normative, easy, and effective.
Using substances to cope is normative
Many students agreed that drinking alcohol and using other substances was a normal part of university life—something that was bound to happen due to the stressors that they face in university. Students noted that drinking alcohol to deal with breakups, exams, and other stressful things in their lives was a popular and socially acceptable coping mechanism among their peer groups. Students also believed that drinking alcohol was a common way of coping with life stressors across cultures and age groups, based on their own personal experiences. Participants estimated that anywhere from 70% to 100% of students have used substances to get over a negative mood at some point. Of all of the substances discussed, alcohol was deemed to be the most common and most socially acceptable substance to use to cope with life problems. Other substances that were touched on included marijuana, cigarettes, over-the-counter medications, prescription drugs, caffeine, and “substances” more generally. For a lot of people who can’t cope well with the stress of university or with mental health [problems], alcohol and substance use is a coping mechanism. Especially in the university setting, where we’re very stressed out all the time about tests and assignments and stuff like that, individuals increase their use. I know that some people use alcohol, or other drugs as well, as kind of an escape from mental health issues that they’re experiencing. I see a lot of people smoking [marijuana] at noon so that they can get through the rest of the day because it’s been a bad week.
Using substances to cope is easy
Students explained this widespread use of substances to cope as arising, in part, due to ease of access. Students also expressed that using substances was an easier way to deal with mental health issues, such as stress and negative mood, than to seek help. One participant noted that in circumstances where students need an immediate fix for their bad mood or problem, they are likely to take the easiest way out (i.e., alcohol and other substance use). It’s a lot easier to go to the liquor store [than to deal with stress in other ways]. So, of course, you’re gonna take the easier way out. Exactly…if somebody really needs something, they’re gonna go get a coffee or a glass of wine.
Using substances to cope is effective
Students also noted that substances are sometimes used as an adaptive coping behavior. Students described caffeine as having a positive effect on mood, and prescription drugs as enabling students with mental health problems to function. In terms of alcohol use, students viewed alcohol as relieving feelings of being overwhelmed, if only temporarily, and of offering a well-deserved break from the demands of university life. The benefit of alcohol is that it suppresses that feeling of being overloaded. So, in a way, it’s effective in changing the mental state of how you feel, or how stress affects you. I find you sometimes need those nights off of being stressed from work and need those nights of fun. I think some people do successfully self-medicate when they can’t access, or are barred from accessing mental health resources on campus. And it can work, it can be effective. If you’ve finished all of your work and you just want to relax, it [marijuana] is a good thing for that. If you’re gonna take a night off and you’ve done everything, then drinking that night isn’t necessarily a bad thing. You’re relaxed, you have some fun with your friends, and then the next day, y’know, you stick to your plan and you do some work.
Theme 2: Substance Use Can Lead to Mental Health Issues
Several students also indicated that substance use can have harmful consequences, noting that substance use can be an antecedent to mental health problems. A few comments revolved around the notion that substance use can make an individual more susceptible to mental health problems or can exacerbate existing problems. Other comments were made concerning the tendency of substances, and in particular alcohol, to intensify negative emotions. In this way, uncontrolled negative feelings, including anxiety, anger, and stress, were conceptualized as mental health concerns. Finally, several participants discussed a risk of developing substance dependence or addiction with continued use. Across these subthemes, substance use that interfered with daily functioning or that continued despite negative consequences was framed as problematic.
Substance use increases vulnerability for mental health problems
Students defined ways in which substance use could precipitate a mental health problem or exacerbate an existing problem. Students emphasized how substances, and alcohol in particular, may sometimes cause or worsen depression and can reduce students’ abilities to cope with stress. One student also communicated that substance use increased stress by making life problems worse. I also find [I go] downhill after a day or a night of drinking. I always feel…not always but a lot of the time…. I feel depressed the day after drinking a lot. It [alcohol] sets you in a place where you may lose control, y’know what I mean? It’s fine for one minute, and then the stress gets so, so high that suddenly you need to go back to where you were, but you cannot. [Alcohol] affects your brain so it could predispose you to developing mental illnesses.
Substance use can lead to addiction
Students expressed concerns about how substance use that was currently not problematic could, downstream, lead to psychopathology in the form of substance dependence or addiction. One student identified a risk of coming to rely on substances as a crutch to get through the day. This notion of loss of control with continued use fits with the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM 5; American Psychiatric Association, 2013) criteria for a substance use disorder and suggests that students have some knowledge regarding the progression from substance use to a substance use disorder. Once it becomes a crutch, I think that’s the point where it really starts to negatively impact you…when you can’t function properly without offloading stress in that manner. If you’re used to having a glass of wine when you’re stressed, then maybe after university, you’d be more likely to develop an addiction. My Dad told me before I left for school, he said I don’t really care if you drink or anything but if you start to find yourself saying, you’re stressed, “I need a drink,” that’s an addictive behavior and that’s when it becomes a problem.
Substance use amplifies negative emotions
Students reported instances where alcohol reduced their ability to cope with emotions or their control over their emotions. The idea that alcohol amplifies negative emotions was illustrated when participants shared experiences, where alcohol made them feel more anxious, angry, or upset than they would have felt when sober. In turn, a couple of students offered cautionary advice about drinking when facing difficulties in life, stating that it was wise to be in the right state of mind to drink. Or like, I’ve had nights when I’ve been drunk and remembered what’s going on in my life that isn’t good, and that’s when my anxiety’s been really bad. I’ve gotten really scared on those sorts of nights, and it doesn’t happen all the time, but when the two things mix, you feel worse than you would’ve when sober. It’s really bad for you to drink when you’re really stressed out, or something tragic just happened, or you’re really angry, cause that’s just gonna amplify those emotions, so you need to be mentally prepared to drink.
Theme 3: Links Between Mental Health and Substance Use Are Cyclical
One interesting, though relatively less popular, theme that emerged was the view that mental health and substance use are reciprocally related. Students described using substances to cope with stress and mental health issues, and experiencing stress and negative emotions as a result of their substance use, in a cyclical manner. A paradoxical effect was described, in which students assumed that alcohol and other substances would improve their mood or reduce their stress but, instead, had the opposite result. Several examples within this theme involved a cycle in which alcohol was used as an ineffective coping strategy that inadvertently increased stress by way of hindering academic performance, which in turn motivated more coping-oriented drinking. In many cases, these comments captured the idea of short-term relief of stress through substance use, but long-term worsening of stress and other mental health symptoms. I think it [alcohol] helps you get away from it [stress] for a little bit, but then almost doubles it [stress] as soon as you’re done getting away. I find, if you have things to do, then it [drinking] hinders your ability to do those things the day after, because you just feel gross and you just don’t want to get out of bed. Then I find that leads to stress because you have things to do, you always have things to do, and you just can’t get them done. You just forget about it [stress]. You’re able to relax [while drinking]. And then once you come back to reality, it’s like “Ok, let’s go back,” know what I mean? So it just comes into this cycle and it’s a vicious cycle and some people just get really consumed.
Theme 4: Substance Use Is an Aspect or Indicator of Mental Health
Several students believed that substance misuse is an element or a signal of a mental health problem. For instance, according to one participant, student use of substances out of peer pressure or reliance on substances to establish and maintain social relationships is, in itself, a problem. Several other students expressed concerns about friends who overuse substances, specifying that they could use their friends’ substance use as a type of barometer or indicator of their friends’ current mental health. In other words, they felt that if they or their peers were using alcohol, other substances, or even caffeine excessively, that it was a reflection of another type of problem. One student stated that noticing changes in one’s substance use can make one aware of an underlying mental health problem that one may not have otherwise acknowledged. Experiencing a substance use issue might bring your awareness to the mental health issue that you didn’t see before. …if you know your friend is taking three caffeine pills every day to get through the day, they’re probably not at healthy stress levels.
Theme 5: Substance Use and Mental Health Are Not Always Linked
Although students noted that substance use and mental health are often linked, they also recognized that they are not always linked. Many students felt that substance use was not associated with mental health issues for everyone but rather depended on the individual, the type and quantity/frequency of use, and reasons for use. Students’ awareness of these moderating factors represents a high level of understanding, given that individual differences and the motives underlying one’s substance use have been described as determinants of substance use outcomes in the empirical literature (Stewart et al., 2001; von Sydow, Lieb, Pfister, Höfler, & Wittchen, 2002; Woicik, Stewart, Pihl, & Conrod, 2009). Students’ knowledge of the dependent nature of links between substance use and mental health suggests that some of them are aware of the complexities of this relationship. I think it [substance use] has the potential to help someone, or to harm them, or do nothing depending on what they’re doing and what substance they’re using and why they’re using it. I don’t think you can make a blanket statement about substance use and stress. I think if you’re abusing any stimulant that’s helping you study to an extreme extent, that’ll be a very different response than if you just put off your studying and get drunk and forget about it.
General Discussion
The current study provided insight into university students’ perceptions of links between substance use and mental health problems by conducting a short series of focus groups. Using thematic analysis, five main themes were identified, four of which described distinct ways in which substance use and mental health can be related, and a fifth, which centered on the idea that substance use and mental health are not always linked.
As noted in the Introduction section, research suggests that interrelations between substance use and abuse and mental health are 4-fold. (1) Individuals (ab)use substances to cope with preexisting mental health problems (Dawson et al., 2005; Hasin et al., 2005; Lasser et al., 2000; Stewart et al., 2016). (2) Mental health problems represent outcomes of substance use (Dawson et al., 2005; Grant et al., 2004; Patton et al., 2002; Ross, 1995; Stewart et al., 2016). (3) Mental health problems and substance use and abuse co-occur due to other factors, which increase risk of both mental health problems and substance abuse (Menezes et al., 1996; Patton et al., 2002; Stewart et al., 2016). (4) Mental health problems and substance use exist in a vicious cycle (Stewart & Conrod, 2007). Although students’ knowledge of explanations (Themes 1, 2, and 4) was evident in their responses, and the overarching themes, students did not explicitly touch on this third explanation in which other factors (biological predispositions, social disadvantage, personality risk factors, etc.) dually put individuals at risk of mental health problems as well as substance use problems. Improving understanding in this area may be a worthy focus of future campus campaigns. Ideally, campus mental health and substance use programs will disseminate information regarding common vulnerability factors (Whiteford et al., 2013; World Health Organization, 2010).
Comments that fell within the “students use substances to cope with mental health issues” theme occurred more frequently than items falling under any other theme. According to our focus group participants, using substances to cope is easy, common, and a normal part of university life. Students’ emphasis on the positive aspects of using substances to cope is concerning and suggests that they may not have a balanced and informed view of the probable adverse consequences of using substances as a coping strategy. 2 Research consistently demonstrates links between coping motives for substance use and substance-related problems (Grant, Stewart, O’Connor, Blackwell, & Conrod, 2007; Simons, Correia, Carey, & Borsari, 1998). Therefore, future campus substance use initiatives would do well to focus on presenting students with accurate information on the risks of using substances to cope. For instance, harm reduction interventions could inform students that self-medication/coping-motivated substance use is related to heavier use, substance dependence, and substance-related problems (Carpenter & Hasin, 1999; Grant et al., 2007). Such initiatives could also improve access to and awareness of “dry activities” that promote well-being and reduce stress. In addition, substance use was discussed as an alternative to professional help that was used when barriers to help-seeking were encountered. Hence, an important goal for future work involves determining how barriers (e.g., time constraints and privacy concerns) can be eliminated, so that self-medication can be minimized and effective professional care can be sought. Importantly, the normative use of substances to cope with stress and mental health issues reported by students highlights a need to make mental health and self-care interventions a regular component of substance abuse prevention programs.
Although many comments revolved around the benefits of using substances in dealing with mental health issues, several students also recognized potential adverse consequences of substance use, including mental health concerns, negative emotions, and addiction or substance dependence. However, students made far fewer comments on pathways from substance use to mental health problems than vice versa, suggesting that they may be less familiar with the concept of developing or exacerbating mental health issues as a result of substance use. This knowledge gap represents a notable target for campaigns aimed at promoting mental health awareness and reducing harmful substance use on campus. Although campus campaigns aimed at increasing awareness of substance misuse and mental health issues have become prominent over recent years, published literature reviews suggest few have incorporated content related to substance-related mental health problems (DeJong, 2002; Glassman & Braun, 2010).
Students also conceptualized substance use as an aspect or indicator of mental health or illness. Students’ recognition of the overlap between mental health and substance use problems was reassuring, yet surprising. Traditionally, campus mental health and substance use problems have been treated with a silo mentality. Indeed, campus services, programs, and campaigns tend to target one issue or the other, and communication and overlap between services is often limited. Given the high levels of comorbidity between substance use disorders and other mental health problems (Cuffel, 1996; Grant et al., 2004), and considering the DSM-5’s recognition of substance use disorders as mental disorders (American Psychiatric Association, 2013), future initiatives would do well to take an integrated approach in their mental health and substance use education programming.
Comments in the “substance use and mental health are not always linked” theme qualified the consequences of substance use. Outcomes were said to depend on a number of things including frequency, quantity, and duration of use, as well as individual characteristics of the person and the type of substance being used. Although the notion of differential vulnerability for addiction and dependence seemed to be common knowledge, there was no specification of what confers vulnerability (i.e., personality risk factors, family history, and life circumstances). Campus programming that improves awareness of risk factors for substance use problems may be helpful in addressing this knowledge gap and in helping students to correctly self-appraise personal risk. Research suggests that individuals, and particularly adolescents and young adults, often recognize a potential for negative consequences of others’ behaviors but are less likely to see themselves as being at risk—a phenomenon known as the personal fable (Alberts, Elkind, & Ginsberg, 2007). As such, teaching students to identify risk factors for substance abuse and to recognize these within themselves may prove to be a valuable harm reduction strategy in campus communities.
As noted, it is common for campus campaigns and services devoted to mental health and substance use to operate independently from one another, despite an acceptance by mental health professionals that these issues are intricately related (Cuffel, 1996; Grant et al., 2004). As seen throughout our focus group themes, university students themselves recognize that mental health and substance use are linked in notable ways. As such, mental health and substance use campaigns will need to be combined if they are to reflect professional opinions, as well as students’ perceptions, of those matters. Reviews of the literature question the efficacy of current campus mental health and substance use initiatives—particularly those that are educational or informational programs (Larimer & Cronce, 2002; Moreira, Smith, & Foxcroft, 2009). From health-literacy and help-seeking perspectives, one barrier to effectively reaching students may reside in educational campaigns’ inattention to the various social determinants of health for university students (Eisenberg et al., 2007; Nutbeam, 2000). Substance use programs that are more engaging and harm reduction–oriented have achieved better results, in terms of awareness of the adverse effects of substance misuse and willingness to engage in protective behaviors (e.g., It takes less than you think—University of Alabama, The Stupid Drink—Syracuse University, and You Know. Be There—George Washington University). Still, these have emphasized substance misuse alone and have not addressed mental health problems that may contribute to substance misuse. This represents a key area for consideration for campus wellness and harm reduction initiatives going forward.
Across themes, students identified criteria for distinguishing adaptive and maladaptive substance use. Indicators of problematic use included impaired daily functioning, being unable to enjoy a social event without using substances, an absence of non-substance-related coping strategies, experiencing relationship problems due to substance use, and feeling addicted to substances. This student-composed list paints student understanding of substance abuse in an encouraging light, given its convergence with professional standards for diagnosing a substance use disorder. For instance, the DSM-5 (American Psychiatric Association, 2013) criteria for a substance use disorder include loss of control, craving, interference with daily life activities, continued use despite harm, relationship difficulties, tolerance, and withdrawal, among other symptoms. Accurate identification of the signs of a substance use problem is essential if students are to recognize problematic use and seek help in a timely manner.
Findings should be framed within the context of some noteworthy study limitations. First, the focus groups consisted primarily of noninternational first-year female students. This raises the question of whether the attitudes and perceptions documented here are generalizable to other university populations. Second, it is possible that our selected questions for the focus group interviews primed students to give certain responses. Had questions been worded differently, participant responses and corresponding themes that emerged in analysis may have been altered. However, care was taken to ensure that questions were not leading when the interview guide was designed. Third, we were unable to calculate the proportion of participants who made comments within the various themes, as no participant identification numbers were assigned to transcripts because the transcriber could not be sure who was speaking. However, we did attempt to provide quantitative information by calculating the frequency of items within each theme and subtheme. Because transcripts and participant identifying information were unmatched, we were also unable to conduct any form of gender analyses or examine differences by age or year of study. Likewise, focus group numbers were not retained when coding the transcripts. Fourth, we did not collect information on participant ethnicity, although students did report on their status as international students. Future work may aim to address similar discussion questions, but with students from more diverse ethnic backgrounds. On a similar note, focus group participants were primarily female first-year students, and so future research should examine perceived links between substance use and mental health problems in more varied university populations. As noted, all students were self-declared drinkers, and so it would be interesting to pose focus group questions to students with different substance use backgrounds including abstainers. Last, we did not record information regarding students’ mental health statuses or experiences (i.e., family histories of mental health problems).
In summary, our findings pinpoint both strengths and weaknesses in students’ understanding of links between substance use and mental health and identify potential targets for future mental health and harm reduction campus initiatives. Namely, future campus campaigns should (1) address the knowledge gap of substance-related mental health problems, (2) emphasize the risks of using substances as a coping strategy, (3) educate students about common vulnerability factors for both mental health and substance use problems, and (4) seek to integrate programs and services targeting mental health and substance use issues.
Footnotes
Appendix
Conclusion: Did we miss anything? Is there anything we should have talked about and didn’t?
Author Contributions
Amanda Hudson contributed to analysis, interpretation, analysis, and interpretation; critically revised the manuscript; gave final approval; and agreed to be accountable for all aspects of work ensuring integrity and accuracy. Kara Thompson contributed to conception, design, and acquisition; critically revised the manuscript; gave final approval; and agreed to be accountable for all aspects of work ensuring integrity and accuracy. Parnell D. MacNevin contributed to conception, design, and acquisition; critically revised the manuscript; gave final approval; and agreed to be accountable for all aspects of work ensuring integrity and accuracy. Meredith Ivany contributed to analysis and interpretation, critically revised the manuscript, gave final approval, and agreed to be accountable for all aspects of work ensuring integrity and accuracy. Michael Teehan contributed to conception and design, critically revised the manuscript, gave final approval, and agreed to be accountable for all aspects of work ensuring integrity and accuracy. Heather Stuart contributed to conception and design, critically revised the manuscript, gave final approval, and agreed to be accountable for all aspects of work ensuring integrity and accuracy. Sherry H. Stewart contributed to conception and design, critically revised the manuscript, gave final approval, and agreed to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Caring Campus Project was funded by Movember Canada (Grant # 35361), H. Stuart, S.-P. Chen, T. Krupa, K. Dobson, S. Stewart, and M. Teehan.