
Abstract
Emerging adults with chronic health conditions (CHCs) face additional challenges compared to their peers during this transitional period, which can exacerbate their symptoms and negatively impact their quality of life (QoL). This study assessed the impact of CHC status and the potential protective factor of perceived health competence (PHC) on QoL. Nine hundred twenty-nine emerging adults, aged 18–25 years (M age = 22.19, SD = 1.95; 55% female), participated in the current study as part of a larger online survey. Results showed that those with a CHC reported significantly lower QoL than those without a CHC. Additionally, higher PHC was associated with higher QoL for both groups of emerging adults. Although the current study identified some factors that may differentially impact this positive association, the results consistently suggest that promotion of emerging adults’ PHC may play a key role in improving their QoL during this transitional period, regardless of CHC status.
It is estimated that one in four children and adolescents in the United States are currently living with a chronic health condition (CHC; Van Cleave et al., 2010), and approximately 40% of these children and adolescents have two or more conditions (Gerteis et al., 2014; National Survey of Children’s Health, 2011/2012). CHCs, regardless of type, can result in comparable stressful experiences for children and adolescents, including academic setbacks, social isolation or withdrawal, functional limitations, and poor psychosocial functioning (Compas et al., 2012; Perrin et al., 2012). Stein and Jessop (1982, 1989) proposed the noncategorical approach to CHCs, which posits that children and adolescents with CHCs face many common challenges and changes due to their conditions and that these experiences are more similar across conditions than they are different. The noncategorical approach defines a CHC as having a biological, cognitive, or psychological basis and resulting in one or more of the following consequences: limitations in daily function, dependence on compensatory mechanisms, and need for services beyond routine care (Stein et al., 1993, 2000). Within this broad conceptualization, some of the more common CHCs among children and adolescents include allergies, asthma, developmental disabilities, frequent or persistent headaches, obesity, and recurrent abdominal pain (Compas et al., 2012; Torpy et al., 2010; Van Cleave et al., 2010).
Advancements in technology have allowed for more accurate diagnoses and more effective and efficient treatment options, resulting in more children and adolescents with CHCs thriving well into adulthood (Halfon & Newacheck, 2010; Mokkink et al., 2008). Consequently, millions of individuals in their late teens and early 20s are currently living with CHCs in the United States (Blum et al., 1993; Compas et al., 2012). The transition from adolescence to adulthood is already a tumultuous experience, characterized by increased autonomy, discovery and development of one’s personal identity, and potentially establishing independent living (Arnett, 2018; Dornbusch, 2000; Goldscheider & Goldscheider, 1999). The presence of a CHC may further complicate this transition (Blum et al., 1993; Zhou et al., 2016). Emerging adults with CHCs are required to assume a greater amount of responsibility regarding their self-care as they transition into adulthood and seek more independence from their parents (Dovey-Pearce & Christie, 2013; Heath et al., 2017). For example, emerging adults often are expected to take primary responsibility for the self-management of their condition by scheduling their own appointments or procedures, following treatment regimens as directed, and carefully monitoring the status of their condition, when previously they could rely on their parents to complete or remind them to complete these tasks. The greater assumed responsibility may be associated with increased stress, which is known to exacerbate the symptoms and worsen the prognosis of CHCs (e.g., Compas et al., 2012).
The adverse effects of CHCs and their management have been shown to place individuals with CHCs at risk for lower quality of life (QoL) in comparison to their healthy peers (e.g., Bai et al., 2017; Centers for Disease Control and Prevention [CDC], 2009; Megari, 2013; Rothrock et al., 2010). The greater the number of diagnosed CHCs an individual is being treated for, the more detrimental the impact is on their QoL (Rothrock et al., 2010). Additionally, individuals who perceive their condition as more severe have been shown to have poorer psychosocial well-being and QoL than individuals who perceive their condition as less severe (Leung et al., 1997). Research has shown that higher QoL is associated with better coping skills, better health prognosis, and more satisfaction with life (e.g., CDC, 2009; Megari, 2013), which highlights the importance of promoting QoL, especially for individuals with CHCs.
Perceived health competence (PHC), or the degree to which one feels capable of effectively managing their health outcomes (Smith et al., 1995), is a potentially important protective factor against the negative impacts of living with a CHC during emerging adulthood. PHC is a form of self-efficacy, which is broadly defined as one’s perception of their own abilities (Bandura, 1997). Self-efficacy is an important cognitive factor affecting general health status (O’Leary, 1985), and research suggests that lower self-efficacy is associated with poorer coping skills, poorer disease management, and lower QoL for individuals with CHCs (Hoffman, 2014; Luszczynska et al., 2005). Additionally, individuals with lower self-efficacy are at a higher risk of experiencing distress and negative emotions (e.g., anxiety and depression) in response to stressful situations (Hoffman, 2014; Luszczynska et al., 2005). Emerging evidence suggests that low PHC may be associated with an increased risk for less adaptive coping skills and lower QoL among individuals with CHCs (Bachmann et al., 2016; Cramm et al., 2013).
Previous research has focused on emerging adults with CHCs as they transition from pediatric to adult health care services (e.g., Blum et al., 1993; Scal et al., 1999; Zhou et al., 2016); however, there is a paucity of research on how to support a less stressful transition to adulthood for emerging adults with CHCs outside of the medical context, as they begin to engage in more independent self-management. The current study aimed to further assess the impact of PHC and CHC status on QoL in a community sample of emerging adults. It was hypothesized that emerging adults who reported having one or more CHCs would have lower QoL than their healthy peers. It was also hypothesized that emerging adults with higher PHC would demonstrate higher QoL. Further, it was hypothesized that CHC status would moderate the proposed relationship between PHC and QoL. Specifically, it was hypothesized that emerging adults with CHCs would demonstrate a greater increase in QoL with higher PHC in comparison to emerging adults without CHCs. Post hoc analyses investigated the influence of comorbidity of conditions and type of condition (i.e., only physical health conditions, only mental health conditions, or both physical and mental health conditions) on the relationship between PHC and QoL.
Method
Participants
Over the course of four academic semesters, 929 emerging adults between the ages of 18 and 25 years (M age = 22.19 years, SD = 1.95) participated in the current study as part of a larger online survey. The majority of participants were female (55%), Caucasian/White (73%), and single, never married (93%). Eighty-five percent of emerging adults had at least some college education, and 59% were currently full- or part-time college students. Almost three fourths of participants reported living outside the family home (72%), while the remainder lived with roommates (37%), with a spouse or romantic partner (17%), alone (13%), or with another family member (not parent; 4%). Demographic data for all participants are presented in Table 1.
Participant Demographic Information.
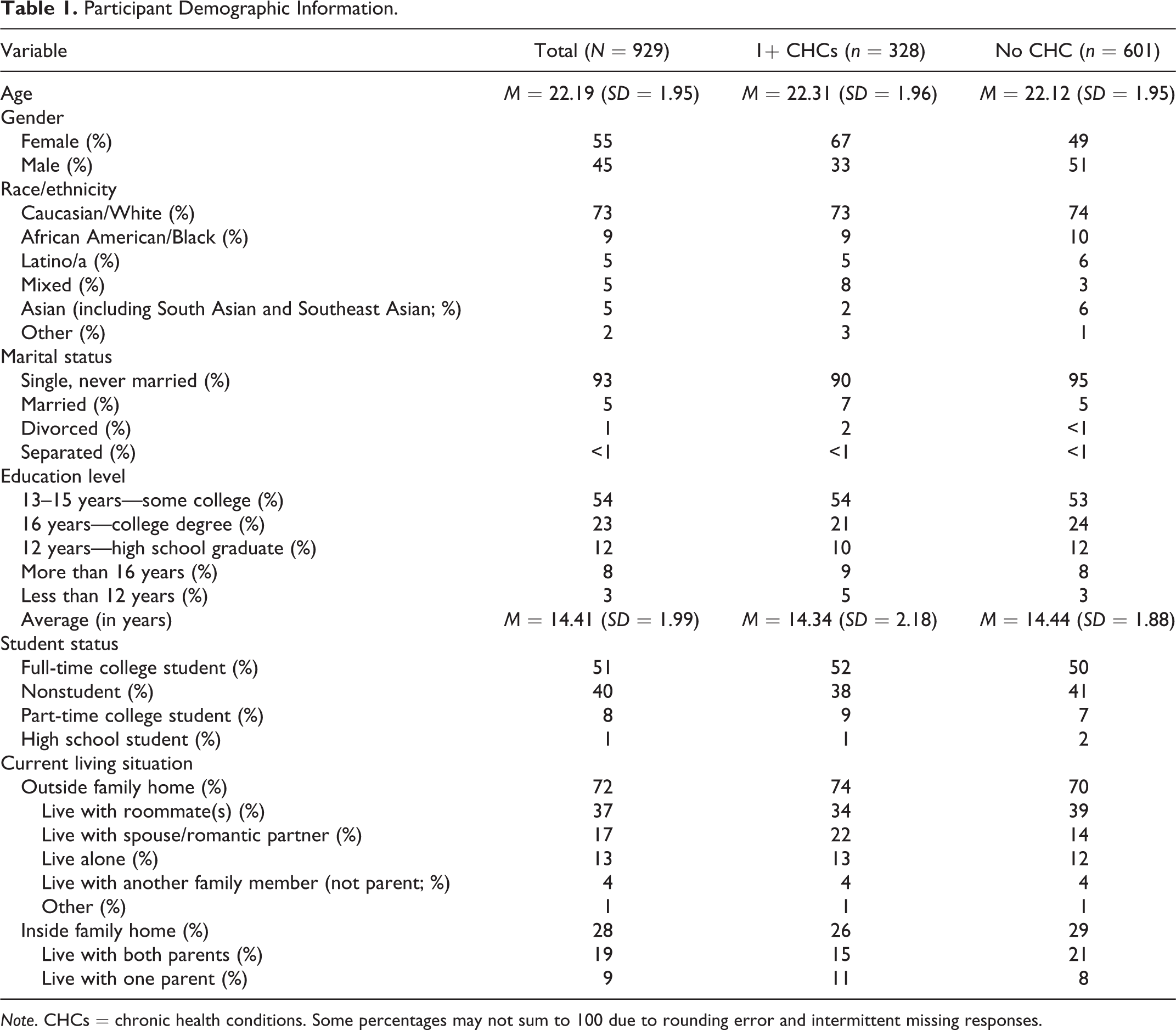
Note. CHCs = chronic health conditions. Some percentages may not sum to 100 due to rounding error and intermittent missing responses.
Three hundred twenty-eight emerging adults (35%) reported having one or more CHCs. Of the emerging adults with a CHC, 35% reported having two or more conditions. Sixty-one percent had only physical health conditions, 27% had only mental health conditions, and 12% had both physical and mental health conditions. Prevalence of specific CHCs represented in the sample is presented in Table 2. There was a significant difference in the percentage of females with one or more CHCs (67%) versus no CHC (49%), χ2 = 27.79, p < .001. There were no significant differences in age, race/ethnicity, marital status, education level, student status, or living situation between these two subgroups of participants (all p > .05).
Prevalence of Specific CHCs in the Community Emerging Adult Sample.
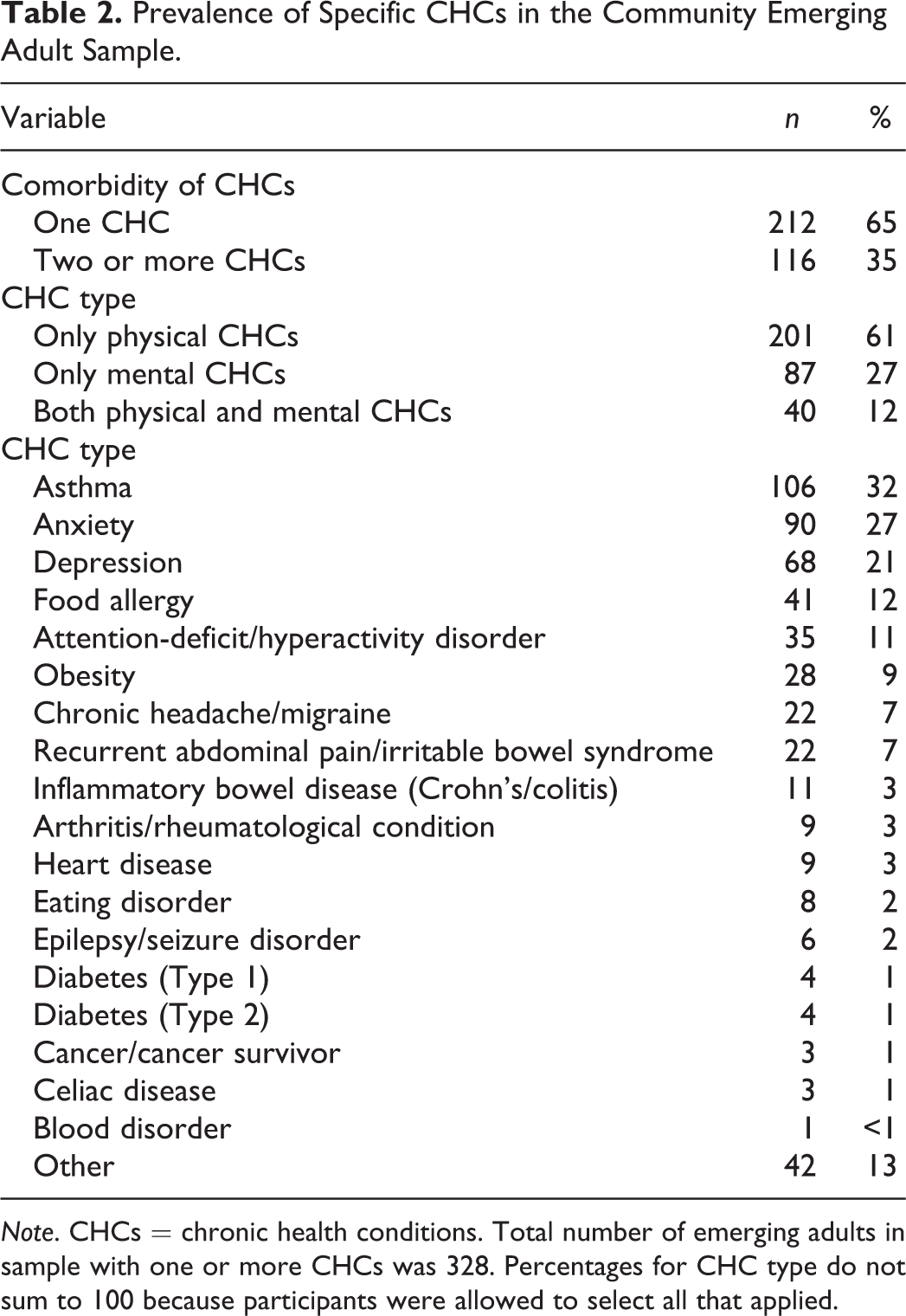
Note. CHCs = chronic health conditions. Total number of emerging adults in sample with one or more CHCs was 328. Percentages for CHC type do not sum to 100 because participants were allowed to select all that applied.
Procedure
Graduate and undergraduate students in an upper-level psychology laboratory course were trained in the ethical conduct of research prior to recruiting a community sample of emerging adults to participate in the larger online survey. If students were unable to recruit a sufficient number of participants, they were allowed to complete an alternative assignment in order to minimize incentive to coerce participation. Students provided potential participants with a one-page informed consent sheet, which explained the purpose of the larger study, assured confidentiality, reminded individuals that their participation was completely voluntary, and included the link to the larger online survey. Before completing the survey, participants were required to indicate that they were at least 18 years, were participating voluntarily, and understood that the student who recruited them would not be penalized if they decided not to participate. Data collection was accomplished via SurveyMonkey and QualtricsXM.
Measures
Demographic information
Participants provided demographic information, including age, gender, race/ethnicity, marital status, education level, student status, and current living situation.
CHC status
Participants were asked to indicate on a list of 18 CHCs all that applied to them. If participants had a CHC that was not included in the checklist of 18 conditions, they could select “other (please specify).” Responses to “other (please specify)” were analyzed using the Delphi coding method (Holey et al., 2007; Jones & Hunter, 1995). For primary data analyses, participants were grouped based upon presence of one or more CHCs or absence of a CHC. For exploratory analyses, participants were grouped based upon presence of a single CHC or presence of two or more CHCs and based upon type of CHCs (i.e., only mental health conditions, only physical health conditions, or both mental and physical health conditions).
CHC status follow-up
Participants who reported having one or more CHCs were asked two follow-up questions regarding their conditions. Participants were asked to indicate their perception of how well controlled the symptoms of their conditions were on a scale from 1 being very poorly controlled to 5 being very well controlled. Participants were also asked if they were currently seeing a physician or other provider for their conditions and allowed to select one of the following three response options: “Have a chronic condition, but not under the care of a provider,” “Under the care of the provider I saw as an adolescent,” or “Under the care of a new provider since I became an adult.”
Perceived Health Competence Scale (PHCS)
The PHCS (Smith et al., 1995) was used as the measure of PHC. This 8-item scale measures the degree to which an individual feels capable of effectively managing their health outcomes. All items were answered on a 5-point Likert-type scale from 1 being strongly disagree to 5 being strongly agree. A total PHC score was calculated by summing the responses to all 8 items, after 4 items were reverse-scored. PHC scores ranged from 8 to 40, with higher scores indicating a stronger perception of health competence.
Measure of QoL
A single item from the Patient-Reported Outcomes Measurement Information System (PROMIS) Scale Version 1.2—Global Health (Hays et al., 2009) was used as the measure of QoL for the current study. Emerging evidence supports the reliability and validity of a single-item measure of QoL in the adult CHC literature (e.g., Siebens et al., 2015; Yohannes et al., 2011). PROMIS is a set of person-centered measures that evaluates one’s physical, mental, and social health (Cella et al., 2010). The PROMIS test items have been shown to be valid with the general population and with individuals with CHCs (Cella et al., 2010). The PROMIS—Global Health is a measure of health status, which incorporates physical and mental health (Hays et al., 2009). As QoL was the variable of interest, a single-item assessing QoL was used for this study. Participants were asked to respond on a 5-point Likert-type scale, from 1 being poor to 5 being excellent, to the following prompt: “In general, would you say your QoL is….” Higher scores on this item were indicative of higher QoL.
Data Analyses
Primary data analyses for full emerging adult sample
The sample was characterized using descriptive statistics. A p value of <.05 was used to determine the significance of results. A hierarchical multiple regression analysis was conducted to assess the ability of PHC and CHC status to predict QoL. Preliminary analyses found that there were no violations of the homoscedasticity, linearity, and multicollinearity assumptions for multiple regression analysis. Since there was a significant difference in the proportion of females based on CHC status, the primary analysis controlled for gender in Step 1. PHC (M = 29.25, SD = 5.52) was mean centered and CHC status was dummy coded (0 = absence of CHCs, 1 = presence of one or more CHCs) prior to being entered into the hierarchical regression. PHC and CHC status were entered in Step 2. Finally, the two-way interaction between PHC and CHC status was entered in Step 3. Statistically significant interactions were followed up with post hoc regression analyses to further characterize the relationship between PHC, CHC status, and QoL. Effect sizes of unique contributions of each independent variable are reported in terms of squared semipartial correlation (sr2), with .01–.08 being a small effect size, .09–.24. being a medium effect size, and ≥.25 being a large effect size. A post hoc power analysis, performed using G*Power Version 3.1 (Faul et al., 2009), indicated that the observed power to detect significant relationships for the primary analyses was >.99.
Exploratory data analyses for comorbidity of condition
For exploratory analyses, the effect of comorbidity of CHCs on the relationship between PHC and QoL was investigated using a hierarchical regression analysis. Comorbidity of CHCs was dummy coded (0 = one CHC, 1 = two or more CHCs) before being entered in Step 1 with PHC (mean-centered based on full sample). The two-way interaction between comorbidity and PHC was entered in Step 2. Additionally, the effect of type of CHC on the relationship between PHC and QoL was investigated. Type of condition was dummy coded (reference group = only physical health conditions) before being entered into Step 1 with PHC (mean-centered based on full sample). The two-way interactions between type of CHC and PHC were entered in Step 2.
Results
Descriptive Statistics
The following descriptive statistics are reported regarding the 328 emerging adult participants who reported having one or more CHCs. A majority of participants reported that the symptoms of their conditions were well or very well controlled (53%), and only 2% of emerging adults reported that the symptoms of their conditions were very poorly controlled. Additionally, 71% of emerging adults with one or more CHCs reported that they were currently under the care of a provider; however, over one fourth (29%) of participants reported that they had a CHC but were not currently under the care of a provider.
Primary Hierarchical Multiple Regression Analyses
Gender, which was controlled for in these analyses, was not significantly associated with QoL and accounted for less than 1% of the variance in QoL for the primary and post hoc regression analyses (all sr2 < .005). Step 2 of the primary regression analysis revealed a statistically significant association between the two independent variables (PHC and CHC status), as a set, and QoL (see Table 3). Combined, PHC and CHC status accounted for 23% of the variance in QoL in this model. PHC uniquely explained 10% of the variance in QoL and demonstrated a positive association with QoL of medium effect size (sr2 = .105). Higher PHC was associated with higher QoL. CHC status uniquely explained minimal additional variance in QoL (sr2 = .002) and was negatively associated with QoL. Emerging adults with a CHC demonstrated lower QoL than those without a CHC.
Hierarchical Multiple Regression Analysis Assessing the Ability of CHC Status and PHC to Predict Quality of Life.
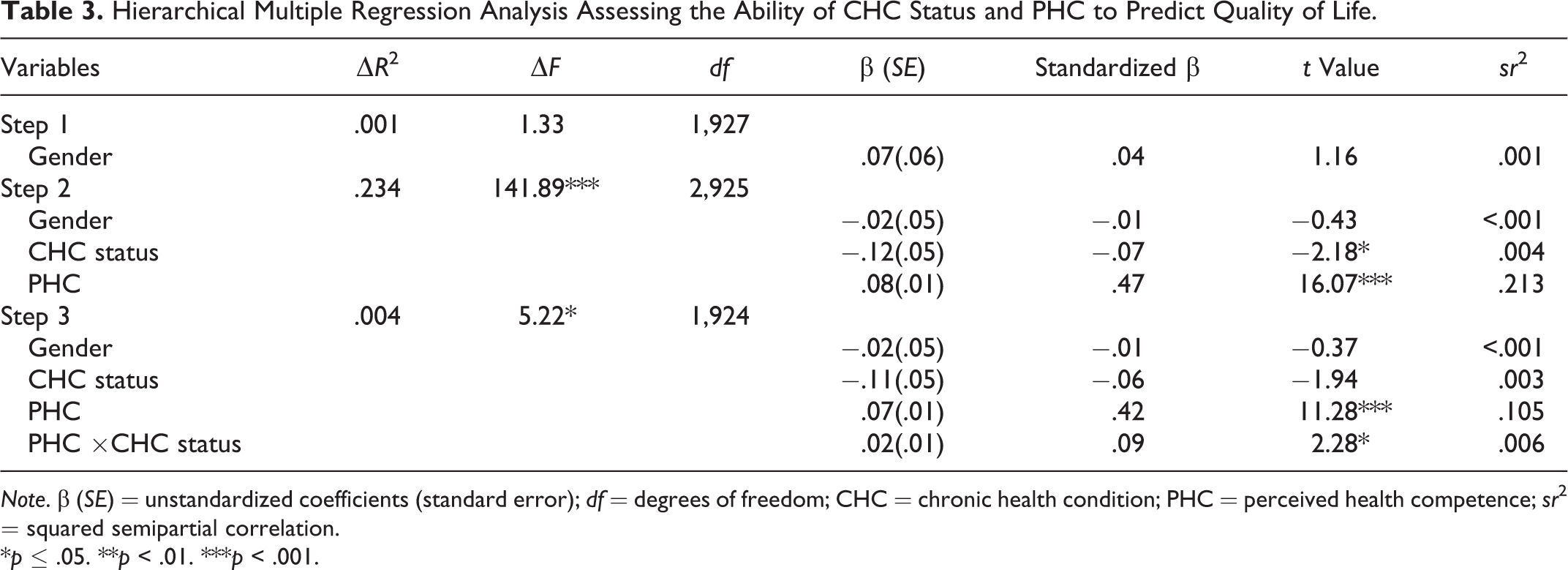
Note. β (SE) = unstandardized coefficients (standard error); df = degrees of freedom; CHC = chronic health condition; PHC = perceived health competence; sr2 = squared semipartial correlation.
*p ≤ .05. **p < .01. ***p < .001.
Results of Step 3 of the primary regression analysis showed that the two-way interaction between PHC and CHC status was significantly positively associated with QoL (see Figure 1). This significant two-way interaction was followed up with post hoc analyses that examined the impact of PHC on QoL within the subgroup of emerging adults without a CHC and within the subgroup of emerging adults with a CHC (see Table 4). Results from these post hoc analyses showed that PHC was positively associated with QoL for emerging adults without a CHC and for emerging adults with one or more conditions. Higher PHC was associated with higher QoL for both subgroups of emerging adults. For emerging adults without a CHC, PHC uniquely explained 18% of the variance in QoL and demonstrated a positive association with QoL of medium effect size (sr2 = .183). For emerging adults with one or more CHCs, PHC uniquely explained 28% of the variance in QoL and demonstrated a positive association with QoL of large effect size (sr2 = .276).
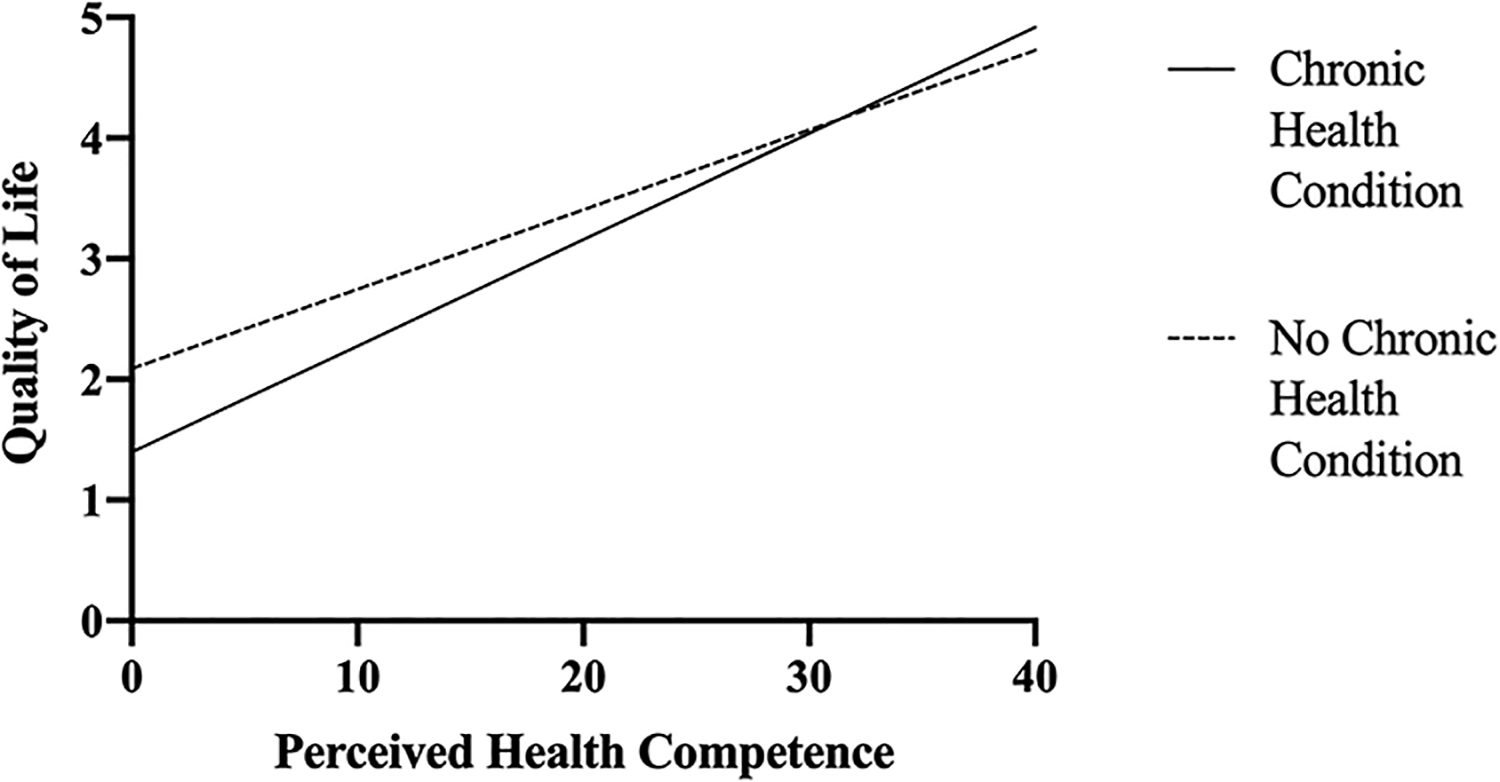
Significant positive association of the two-way interaction between chronic health condition status and perceived health competence and quality of life.
Post Hoc Analyses Assessing the Ability of PHC to Predict Quality of Life for Two Subgroups of Emerging Adults Based on CHC Status.
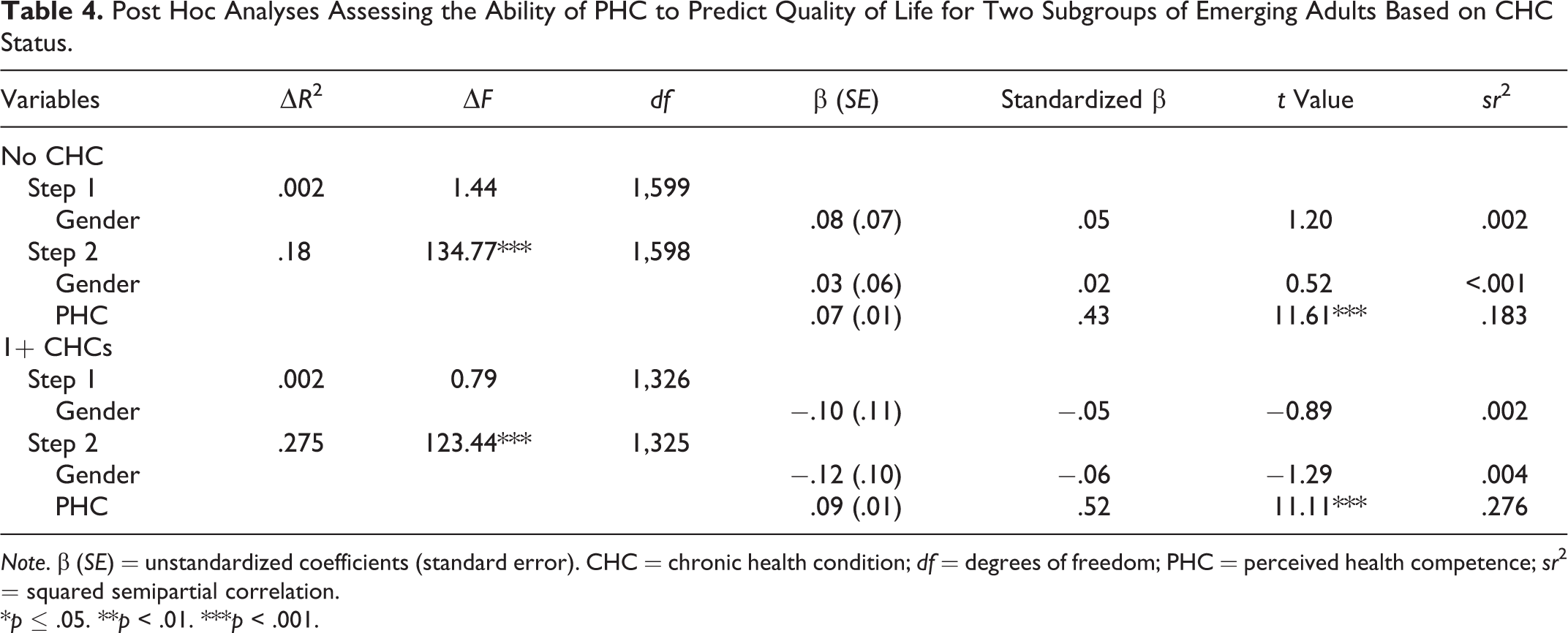
Note. β (SE) = unstandardized coefficients (standard error). CHC = chronic health condition; df = degrees of freedom; PHC = perceived health competence; sr2 = squared semipartial correlation.
*p ≤ .05. **p < .01. ***p < .001.
Post Hoc Analyses for Emerging Adults With One or More CHCs
Comorbidity of CHCs
A post hoc regression analysis was conducted to examine the impact of comorbidity of CHCs on the relationship between PHC and QoL. Results from Step 1 showed that PHC and comorbidity of CHCs, as a set, were positively associated with QoL, ▵R2 = .275, F(2, 325) = 61.66, p < .001. Higher PHC was associated with higher QoL, t(325) = 11.08, p < .001, β (SE) = .09 (.01), standardized β = .53. PHC uniquely explained 16% of the variance in QoL and demonstrated a positive association with QoL of medium effect size (sr2 = .156). However, comorbidity of conditions was not significantly associated with QoL, t(325) = 0.89, p = n.s., β (SE) = .09 (.10), standardized β = .04. Emerging adults with one CHC had QoL scores similar to emerging adults with two or more conditions. Additionally, the two-way interaction between PHC and comorbidity in Step 2 did not significantly account for any additional variance in QoL beyond that accounted for in Step 1, ▵R2 = .003, F(1, 324) = 1.51, p = n.s. These analyses demonstrate that comorbidity of conditions, at least for the specific combinations of conditions reflected in this sample, did not differentially affect the positive relationship between PHC and QoL.
Type of CHC
A second post hoc regression analysis was conducted to examine the impact of type of CHC on the relationship between PHC and QoL. Results from Step 1 showed that PHC and type of CHC, as a set, were positively associated with QoL, ▵R2 = .274, F(3, 324) = 40.83, p < .001. Higher PHC was associated with higher QoL, t(324) = 11.02, p < .001, β (SE) = .09 (.01), standardized β = .52. PHC uniquely explained 27% of the variance in QoL and demonstrated a positive association with QoL of large effect size (sr2 = .276). However, there was no significant difference between mean QoL scores for emerging adults with only mental CHCs (M = 3.70, SD = 1.03), t(324) = 0.65, p > .05, β (SE) = .07 (.10), standardized β = .03, and emerging adults with both mental and physical CHCs (M = 3.55, SD = 1.06), t(324) = 0.38, p > .05, β (SE) = .05 (.14), standardized β = .02, compared to emerging adults with only physical CHCs (i.e., the reference group; M = 3.62, SD = 0.89). Emerging adults had similar QoL scores regardless of what type of CHCs they had. Step 2 that included all two-way interactions between type of CHC and PHC predicted significant additional variance in QoL, F(2, 322) = 3.08, p < .05. In Step 2, PHC again positively predicted QoL, t(322) = 7.43, p < .001, β (SE) = .07 (.01), standardized β = .44, and demonstrated a positive association with QoL of medium effect size (sr2 = .122). Additionally, the two-way interaction between mental CHCs and PHC was statistically significant, t(322) = 2.41, p < .05, β (SE) = .05 (.02), standardized β = .13; however, this two-way interaction only accounted for minimal additional variance in QoL and demonstrated a positive association with QoL of small effect size (sr2 = .013). These analyses demonstrate that type of CHC in the current sample did not have a significant effect on the relationship between PHC and QoL, above and beyond that already accounted for by PHC alone.
Discussion
Consistent with previous literature (e.g., Bai et al., 2017; CDC, 2009; Megari, 2013; Rothrock et al., 2010), emerging adults with one or more CHCs reported lower QoL in comparison to their healthy peers. Previous research suggests that the more diagnosed CHCs an individual is receiving treatment for, the lower their QoL (Rothrock et al., 2010); however, potentially because data were analyzed dichotomously (one condition vs. two or more conditions), rather than continuously, this was not supported by the findings of the current study. Further, type of CHC did not have a differential impact on QoL in the current sample, thus supporting the noncategorical approach to CHCs utilized (Stein & Jessop, 1982, 1989). Results also showed that PHC was a robust predictor of QoL. Emerging adults with higher PHC demonstrated higher QoL. This finding adds to the emerging evidence in the literature regarding the positive association between PHC and QoL (Bachmann et al., 2016; Cramm et al., 2013; van Empelen et al., 2005). Across primary and exploratory analyses, PHC uniquely explained at least 10% of the variance in QoL. The hypothesized two-way interaction between CHC status and PHC was also supported by the results of the current study, such that the relationship between PHC and QoL varied depending on CHC status; however, the two-way interaction only accounted for minimal additional variance in QoL (<1%) beyond what was already accounted for by CHC status and PHC.
The current study found a positive association between health competence and QoL for all community emerging adults; however, health competence was shown to be more strongly associated with QoL for emerging adults with CHCs. In children, adolescents, and emerging adults with CHCs, there is a well-established relationship between higher QoL and healthier coping skills, better prognosis of one’s condition, and more satisfaction with life (e.g., CDC, 2009; Megari, 2013), which highlights the importance of interventions focused on promoting the QoL of individuals with CHCs. Although the cross-sectional nature of the current study does not allow for causal conclusions to be made, the findings suggest that interventions aimed to improve emerging adults’ level of health competence may promote higher QoL, regardless of CHC status. To the authors’ knowledge, no current program exists that is specifically focused on promoting individuals’ health competence, but there is no reason to think that this would not be an appropriate target for intervention. There are existing interventions and recommendations that focus on improving general self-efficacy as it relates to one’s health care (e.g., Coleman & Newton, 2005; Delfs, 2011; Hoffman, 2014; Huang et al., 2014) that may be applied to health competence. Additionally, cognitive behavioral therapy, a commonly used therapeutic intervention, could be beneficial in promoting health competence as it focuses on factors that influence, and are affected by, self-efficacy as a way to change thoughts and behaviors (Beck, 2011).
The primary recommendation across health-related self-efficacy interventions is to engage the child in the process of self-management as soon as appropriate. Parents can begin to promote their child’s health competence early by acting as a partner to their child and sharing health care management responsibilities with their child (Keickhefer et al., 2009). The goal of a gradual transition to individual self-management is to develop a state of interdependence that promotes the child’s competency regarding their own health care (Kieckhefer et al., 2009). In order to be effective facilitators in this process, parents may need to adjust their behaviors, responsibilities, and roles, as they purposefully incorporate health-related behaviors into the daily routines of the child (Heath et al., 2017; Ryan & Sawin, 2009). Additionally, health care provider support of patient self-management is a key component of effective care for CHCs and improved patient outcomes (Coleman & Newton, 2005; Delfs, 2011; Hoffman, 2014). Self-management support by health care providers should focus on developing patient problem-solving skills, promoting overall self-efficacy, and supporting the application of these skills to real-life situations (Coleman & Newton, 2005). Pediatric psychologists may play an important role in helping parents and physicians to navigate what level of independent self-management is appropriate for their child given their developmental age and abilities, as pediatric psychologists are uniquely positioned to partner with children, families, and other health care providers (Gray et al., 2015) and support a more successful transition to adulthood. It is important for both parents and health care providers to view self-management as an ongoing process of collaboration with the child to best manage the child’s condition, health, and overall well-being (Ryan & Sawin, 2009). Unfortunately, over one fourth of the emerging adults with one or more CHCs in the current study reported that they were not currently under the care of a health care provider. Another important area for future interventions should focus on increasing emerging adults’ usage of health care providers in the management of their condition, with the goal of promoting health competence and QoL.
Transitional services for children, adolescents, and emerging adults with CHCs typically focus on developing the necessary skills to advocate for themselves and deal effectively with difficult or unexpected events related to their condition (Coleman & Newton, 2005; Cramm et al., 2013; Delfs, 2011; Hoffman, 2014; Huang et al., 2014). Some conditions, such as diabetes (Peters et al., 2011) and spina bifida (Kelly et al., 2017), already have well-established recommendations for transitional services; however, the majority of CHCs do not have explicit recommendations for transitional services. Researchers have begun to investigate a noncategorical approach to transitional interventions for emerging adults and, thus far, have suggested that promoting individual self-management, health-related self-efficacy, and patient-initiated communications can support a more successful transition to adulthood (Huang et al., 2014; Zhou et al., 2016). Research has shown that unsuccessful transitions to adulthood for emerging adults with CHCs are common and associated with negative emotional, mental, and physical consequences (e.g., Stam et al., 2006), which highlights the importance of continued research in this area. Through tailored interventions that involve early engagement in self-management and health competence promotion, parents and health care providers may be able to better support children, adolescents, and emerging adults as they prepare for a successful transition into adulthood.
Limitations
The majority of participants were Caucasian/White and well-educated (average of 14 years of education), which is not necessarily representative of the greater population of emerging adults (Vespa, 2017). The lack of diversity in the participant demographics limits the ability to generalize findings to a more diverse population, and the results should be interpreted with caution. Another limitation of the current study was the nature of the online cross-sectional survey. In an online survey, as with any survey, it is possible for participants to respond in a socially desirable way or provide false information, which cannot be verified. However, to decrease the likelihood of a social desirability response bias and encourage participants to provide accurate information, they were ensured the confidentiality of their responses prior to beginning the online survey. The cross-sectional nature of the current study allows for conclusions to be made about relationships among health competence and QoL for emerging adults in their current state; however, it limits the conclusions that can be made. Longitudinal data are necessary to clarify the causality and directionality of the relationship between health competence and QoL as well as potential changes over time. Finally, the current study used a single-item measure of QoL, which may be considered a limitation; however, there is emerging literature to support the reliability and validity of a single-item measure of QoL in adult CHC populations (e.g., Siebens et al., 2015; Yohannes et al., 2011).
Future Directions
The findings of the current study suggest that future research is necessary to better understand the unique challenges and opportunities faced by emerging adults with CHCs. In order to better understand the impact of PHC on QoL, future research should utilize more diverse samples and a longitudinal design, which would allow for greater generalizability of findings and clarity regarding causal relationships. Additionally, future research should investigate the potential impact of other auxiliary factors, such as health literacy, severity of condition, and complexity of medical regimen, that may impact health competence and QoL. Finally, although this study points to a potential area for intervention, it does not investigate whether interventions aimed to enhance PHC will result in higher QoL. Future research should focus on the development of interventions aimed to promote health competence through a noncategorical approach to determine the effectiveness of these interventions in improving QoL and promoting a successful transition to adulthood for emerging adults with and without CHCs.
Footnotes
Author Contributions
Lang, A. contributed to conception and design, acquisition, analysis, and interpretation; drafted manuscript, critically revised manuscript, gave final approval; and agrees to be accountable for all aspects of work ensuring integrity and accuracy. Greenley, R contributed to design and interpretation, critically revised manuscript, gave final approval, and agrees to be accountable for all aspects of work ensuring integrity and accuracy. Davies, W. H. contributed to design, acquisition, and interpretation; critically revised manuscript, gave final approval, and agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Open Practices
Data and materials for this study have not been made publicly available. The design and analysis plans were not preregistered.