
Abstract
Exposure to parental problem drinking (PPD)—symptoms of alcohol use disorder, heavy and hazardous drinking—is associated with mental health problems in emerging adults, but mechanisms of risk are not fully explicated. The current study explores the role of parental emotion socialization, a key factor in the development of emotion regulation, in the context of PPD. A sample of 377 U.S. college students reported retrospectively on PPD, parent reactions to participant negative emotions, and participants’ own current depressive and anger rumination. Both mother and father PPD were related to greater same-parent minimization, distress and punitive reactions, and less problem-focused, emotion-focused, and encouragement of expression of negative emotions. Supportive and nonsupportive parental reactions to negative emotions intervened in associations between PPD and emerging adult depressive and anger rumination. Findings suggest that emotion dysregulation may be a key mechanism of risk for mental health problems among emerging adults exposed to PPD.
Approximately one in 10 U.S. children live with a parent who has an alcohol use disorder (Lipari & Van Horn, 2017). Parental problem drinking (PPD) is even more common, as it encompasses the spectrum of symptoms of alcohol use disorder, heavy or hazardous drinking, and related problems (e.g., parental hangovers, alcohol-related injuries, employment loss). PPD is associated with several problems in offspring, including substance use issues (Marino et al., 2018), making it a serious public health concern. College students are at special risk for substance use issues, especially alcohol problems, in comparison to other developmental periods and non-college students (Merrill & Carey, 2016). Further, college students who have been exposed to PPD exhibit greater alcohol problems than their peers (Powers et al., 2017). However, the mechanisms of risk associated with PPD have not been fully explicated. One potential mechanism of risk is poor parental socialization of emotion, which may hinder the development of emotion regulation (Rothenberg et al., 2019), ultimately leading to alcohol use as a way of managing emotions or other mental health problems. However, there are few studies of problem drinking parents’ approach to socializing emotion in their children. The purpose of the current study is to address this research gap by examining how PPD is associated with college students’ retrospective reports of parent reactions to child negative emotions, and whether those reactions are related to emotion regulation in emerging adulthood.
The ability to regulate emotions develops in part via parent emotion socialization. According to the model of emotion socialization developed by Eisenberg and colleagues (1998), emotion socialization of a child refers to teaching a child about emotion via parent emotion expressions, discussions with the child about emotion, and parental reactions to the emotions of the child and others. Parent reactions to the negative emotions of their children have emerged as an especially important part of emotion socialization. Fabes and colleagues (Fabes et al., 1990, 2001) have demonstrated six primary types of parental reactions to child negative emotions. Three of these are unsupportive reactions: (1) distress reactions involve parents experiencing distress in response to their children’s negative emotions; (2) punitive reactions are those in which parents punish children for expressing negative emotions; and (3) minimization reactions invalidate children’s feelings and minimize the seriousness of the situation. These reactions teach children that negative emotions are to be avoided, their expression is a form of misbehavior, and provide no instruction on how to regulate emotions (Cui et al., 2020). The other three reactions are supportive of children. They include (4) parent encouragement of emotion expression, which validates children’s feelings; (5) attempts to reduce children’s negative emotions using emotion-focused strategies that involve comforting, distraction, and other approaches; and (6) attempts to reduce children’s negative emotions through problem-focused strategies that solve the issue that caused the negative emotions to arise. These reactions teach children that negative emotions are normal and scaffold emotion regulation strategies (Breaux et al., 2018). Both mothers and fathers engage in emotion socialization, although fathers may show greater responsiveness to boys’ emotions (Lunkenheimer et al., 2020) and father emotion socialization may be more sensitive to their psychological health than mother emotion socialization (McKee et al., 2018). It is therefore important to consider mother and father emotion socialization separately.
Given the importance of parent emotion socialization for the development of child emotion regulation, it is important for research to establish how factors such as problem drinking may influence whether parents engage in supportive or unsupportive reactions to child negative emotions. We were able to identify only one study of PPD and parent reactions to child negative emotions: Godleski and colleagues (2020) found that unsupportive reactions mediated associations between interparental conflict and adolescent delinquency only in the context of father alcohol problems. Despite the limited prior research on the topic, there are three key reasons why PPD may be associated with unsupportive emotion socialization. First, PPD is associated with other forms of poor parenting. For example, PPD is related to lower positive parenting as reported by adolescents (Sternberg et al., 2018), parents taking less pleasure in parenting and adolescents and young adult perceptions of colder and more distant relationships with their parents (Iacopetti et al., 2021). These characteristics of the parent-child relationship suggest that PPD would also be associated with unsupportive emotion socialization.
Second, parents with drinking problems may themselves suffer from emotion regulation difficulties that prevent them from engaging in supportive emotion socialization. Poor emotion regulation is believed to underlie alcohol use disorder, as patients develop pathological reliance on alcohol to avoid or reduce negative emotions and increase positive emotions (Bradizza et al., 2018; Suzuki et al., 2020). Negative emotionality and problems identifying emotions are also related to other aspects of problem drinking, such as binge drinking (Lannoy et al., 2021). These difficulties with emotion regulation in problem drinking parents may prevent them from engaging in supportive emotion socialization because healthy emotion regulation is needed to practice emotion socialization (Hajal & Paley, 2020).
Third, the frequent intoxication that is associated with alcohol use disorders is likely to undermine the limited emotion regulation skills parents do have, further diminishing their ability to engage in supportive emotion socialization. Multiple areas of the prefrontal cortex and the amygdala are involved in emotion regulation (Berboth & Morawetz, 2021). However, alcohol disrupts neural synchrony in the prefrontal cortex, leading to deficits in goal directed behavior and impulse control (Marinkovic et al., 2019), and this effect is especially strong among problem drinkers (Shokri-Kojori et al., 2017). The implication is that PPD will interfere with their ability to react supportively to child negative emotions.
As a consequence of poor emotion socialization from parents, children exposed to PPD may have difficulties developing emotion regulation abilities. Unfortunately, there have been relatively few studies of emotion regulation in persons exposed to PPD. This gap in research is critical due to the important public health implications of poor emotion regulation, many of which become apparent in emerging adulthood. Emotion regulation is increasingly understood as a mediator of the effects of adverse childhood experiences on mental and physical illness in adulthood (Cloitre et al., 2019). Emotion regulation also plays a key role in emerging adults’ ability to form healthy romantic relationships (Davila et al., 2017). College students may be especially vulnerable to the consequences of poor emotion regulation because they face additional stressors such as academics and paying for college that their non-college peers do not (Karatekin, 2018). This may account for why college students experience high levels of anxiety, depression, and substance abuse (Kenney et al., 2018).
The current study focuses on rumination as a maladaptive strategy for regulating depression and anger. Rumination is the process of repetitively thinking the same thoughts or focusing on the same ideas for an extended period of time, and has the consequence of increasing these negative feelings (Watkins & Roberts, 2020). Rumination is a form of maladaptive emotion regulation that has been causally linked to poor mental health (Topper et al., 2017). Furthermore, rumination has been reported by college students in response to many types of stressors, including interpersonal conflict (Cimsir, 2019), academic stressors (Krys et al., 2020), and the COVID-19 epidemic (Ye et al., 2020), contributing to college students’ depression, substance abuse, and sleep problems (Bravo et al., 2018; Li et al., 2019).
The current study therefore addresses important gaps in the understanding of how PPD contributes to difficulties in the transition to adulthood. It is hypothesized that PPD will be linked to college students’ recall of parents’ greater nonsupportive reactions (minimization, distress, and punitive reactions), and less supportive reactions (problem-focused, emotion-focused, and encouragement of expression) to negative emotions. It is further hypothesized that recall of greater unsupportive and less supportive parental reactions to child negative emotions will serve as intervening variables in the relations between greater PPD and college students’ greater depressive and anger rumination. These associations are examined while controlling for several potential confounds relevant to this population. We control for participant sex because of the potential differences in parental socialization of emotion and reactions to parent emotion socialization between boys and girls (Perry et al., 2017). We also control for family socioeconomic status (SES) because PPD can reduce family SES and low SES can increase parental stress and interfere with parenting (Kendler et al., 2017; Sobowale & Ross, 2018). Finally, we control for whether the parents are biologically related to the participant because it is possible that step-parents may interact with their children differently from biological parents (Lardier et al., 2017). Given the low level of variability in participant age, this variable was not included as a covariate.
Method and Materials
Participants and Procedures
This study was approved by the college’s internal review board and informed consent was obtained. Participants were U.S. college students enrolled in psychology courses requiring participation in research studies for credit. To ensure a sufficient number of participants exposed to PPD, invitations were sent to students answering “yes” to three or more questions on the short form of the Children of Alcoholics Screening Test (Hodgins et al., 1993). These items were part of a screening survey sent to all subject pool students at the beginning of the semester and 170 participants received this invitation. Students who did not receive an invitation were also eligible to participate by viewing the study description in the online research participant system and signing up for the study. 207 participants self-selected into the study in this way (total N = 377).
Participants attended a single laboratory session, during which they completed several questionnaires concerning their childhood experiences, as described below. The use of retrospective reports of PPD is very common in research (e.g., Klostermann et al., 2011; Lyvers et al., 2019). Retrospective reports of adverse childhood experiences have been found to be reliable (Hardt & Rutter, 2004). Further, retrospective reports provide researchers with an assessment of adverse family experiences they may not otherwise be able to obtain and may be more relevant to adult development (Bell & Bell, 2018).
Measures
Parental problem drinking
Participants completed the full version of the Children of Alcoholics Screening Test (CAST; Jones, 1983) with respect to their mother and father figures (if they had each). The CAST includes 29 items describing experiences common to having a parent with a drinking problem (e.g., “did you ever threaten to run away from home because of your parent’s drinking?”). The 30th item was removed because it asked about the opposite sex parent. Items are answered “yes” or “no” and scores are created by summing the “yes” responses. Internal reliability was excellent for reports of mother figures (Cronbach’s α = .97), and father figures (Cronbach’s α = .96).
Parental reactions to child negative emotions
Participants completed a modified version of the Coping with Children’s Negative Emotions Scale (Fabes et al., 1990). The original version presents 12 vignettes in which children experience negative emotions (e.g., child falls off of a bike and breaks it, then becomes upset and cries) and asks parents to rate the likelihood that they would react in six different ways. The modified version asks participants to imagine if they were in each of the situations as a child and rate how likely their parents would have reacted in the same ways: (1) minimizing their distress (e.g., “told me that I was over-reacting”), (2) with their own distress (e.g., “remained calm and not let him/herself get anxious”—reverse scored), (3) punitively (e.g., “told me to stop crying or I wouldn’t be allowed to ride my bike any time soon”), (4) with emotion focused solutions (e.g., “comforted me and tried to get me to forget about the accident”), (5) with problem focused solutions (e.g., “helped me figure out how to get the bike fixed”), and (6) with encouragement of emotional expression (e.g., “told me it’s ok to cry”). Cronbach’s α ranged from .79 to .96 for the six subscales. The measure was completed once with respect to father emotion socialization and once with respect to mother emotion socialization.
Emotion regulation
Two measures were used to assess participant emotion regulation: the Anger Rumination Scale (ARS; Sukhodolsky et al., 2001) and the Rumination Responses Scale (RRS; Treynor et al., 2003). The ARS includes 20 items assessing the degree to which participants ruminate over events that make them feel angry (e.g., “I analyze events that make me angry”) on a scale from 0 (“almost never”) to 3 (“almost always”). The RRS includes 22 items assessing the degree to which participants ruminate over depressive events (e.g., “think about a recent situation wishing it had gone better”) on a scale from 0 (“never”) to 3 (“always”). Scores for both measures are created by summing the responses. Cronbach’s α for both was .94.
Data Analysis
Data were analyzed using structural equation modeling in Mplus version 6.12. In initial models, mother or father problem drinking were examined as a predictor of the six dimensions of coping with children’s negative emotions, controlling for participant sex (1 = female, 0 = male), whether the parent is biologically related to the participant (1 = biologically related, 0 = not biologically related), and socioeconomic status (SES). In subsequent models, supportive (encouragement of expression, emotion-focused coping, and problem-focused coping) and nonsupportive (distress, minimization, and punitive) forms of coping with children’s negative emotions were specified as latent variables and considered as intervening variables of relations between PPD and participant emotion regulation (depressive and anger rumination) controlling for participant sex, parent relationship type, and SES. Separate models were fit for mother and father problem drinking, and for supportive and nonsupportive reactions to children’s negative emotions. Models were estimated using maximum likelihood with robust standard errors (MLR). Bootstrapping of indirect effects is not possible with MLR estimation. Therefore, indirect effects were tested using Sobel (1982) tests. Also, because MLR was employed, missing data were imputed with the expectation-maximization (EM) algorithm. Unstandardized coefficients are reported due to concerns about the reliability of standardized coefficients in SEM (Kline, 2013).
Results
Participant Demographics
Mean participant age was 19.09 (SD = 1.42) and ranged from 18 to 28. However, 96.4% of the sample was between the ages of 18 and 22. Other participant demographics are reported in Table 1. In terms of perceived socioeconomic status (SES), 18.6% of the sample indicated they were below the middle class, and 37.7% of the sample indicated they were upper middle class or higher. Most participants reported on their biological mothers (86.5%) and fathers (82.1%). All participants had at least one parental figure and were included in the analysis sample, but 6.3% did not have a father figure and 8% did not have a mother figure.
Participant Descriptives.
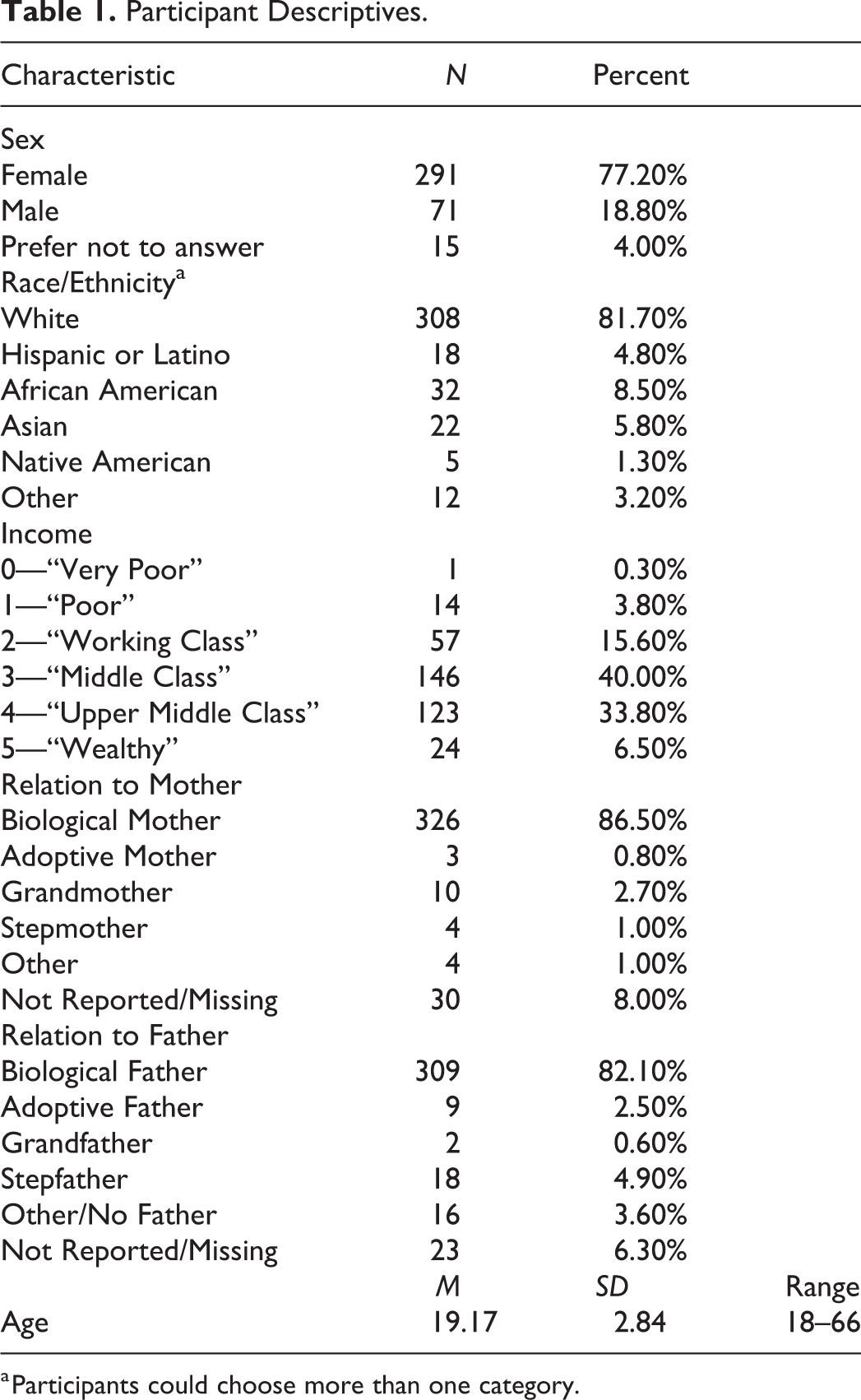
a Participants could choose more than one category.
Preliminary Analyses
Means, standard deviations, and correlations among all study variables are included in Table 2. Preliminary analyses identified 15 possible outliers. Further examination of these variables, as well as other dependent variables in the data set, indicated these resulted from issues with skewed variable distributions. All potential outliers were in the long tail of the skewed distributions. Therefore, analyses made use of an estimation procedure (maximum likelihood with robust standard errors; MLR) designed to address skewed distributions in dependent variables.
Means, Standard Deviations, and Correlations Among Study Variables.
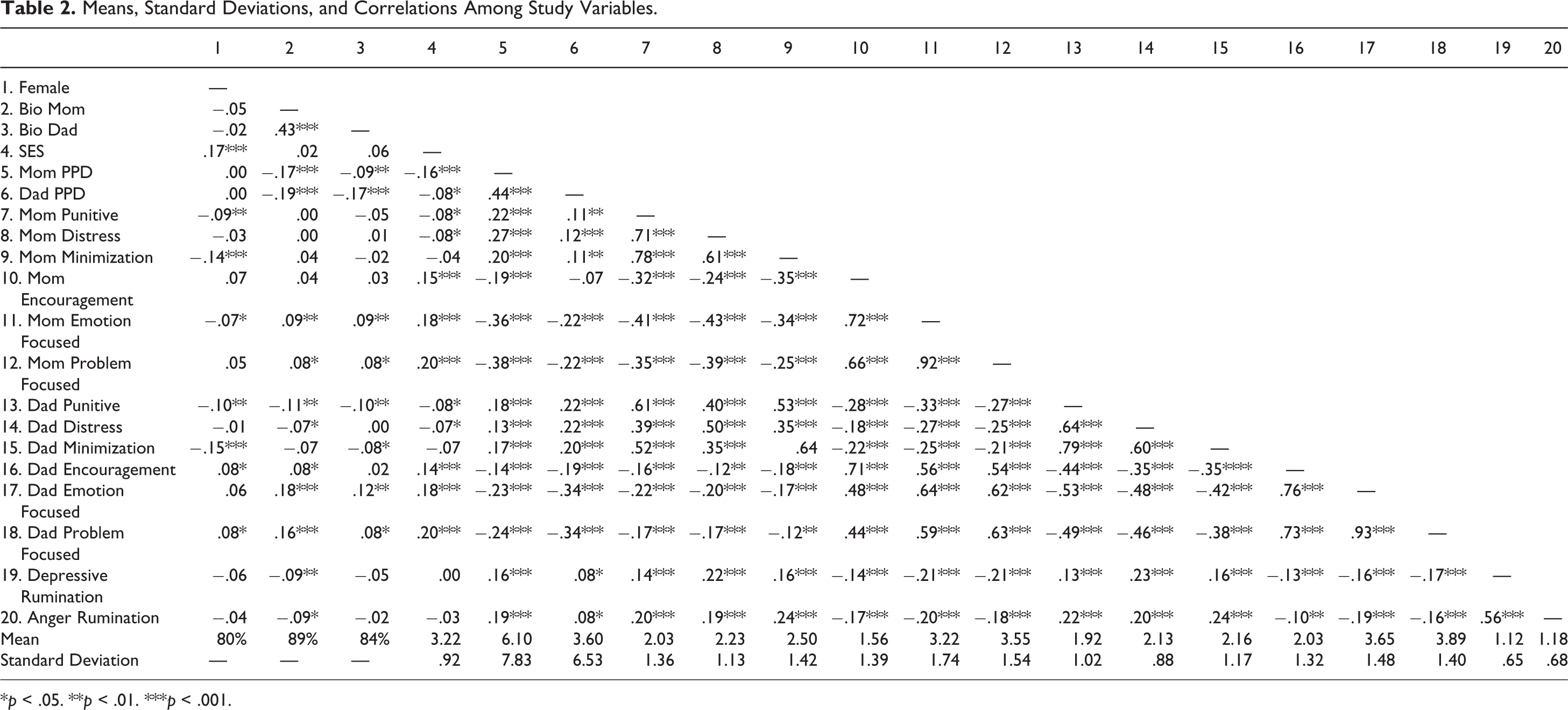
*p < .05. **p < .01. ***p < .001.
Mother Problem Drinking and Emotion Socialization
The initial model in which mother problem drinking was included as a predictor of each individual mother reaction to child negative emotions was fully saturated and therefore fit indices are not interpreted (see Figure 1). Mother problem drinking was significantly associated with greater mother punitive reactions, B = 0.04, p < .01, greater mother minimization, B = 0.04, p < .001, and greater mother distress reactions, B = 0.04, p < .001, and lower mother encouragement of expression, B = −0.03, p < .001, lower mother emotion focused coping, B = −0.07, p < .001, and lower problem focused coping, B = −0.07, p < .001. In addition, higher SES was related to greater mother encouragement of expression, B = 0.17, p < .05, greater mother emotion focused coping, B = 0.21, p < .05, and greater mother problem focused coping, B = 0.22, p < .05. Finally, mothers were more minimizing of boys’ negative emotions than girls’ negative emotions, B = −0.42, p < .01.
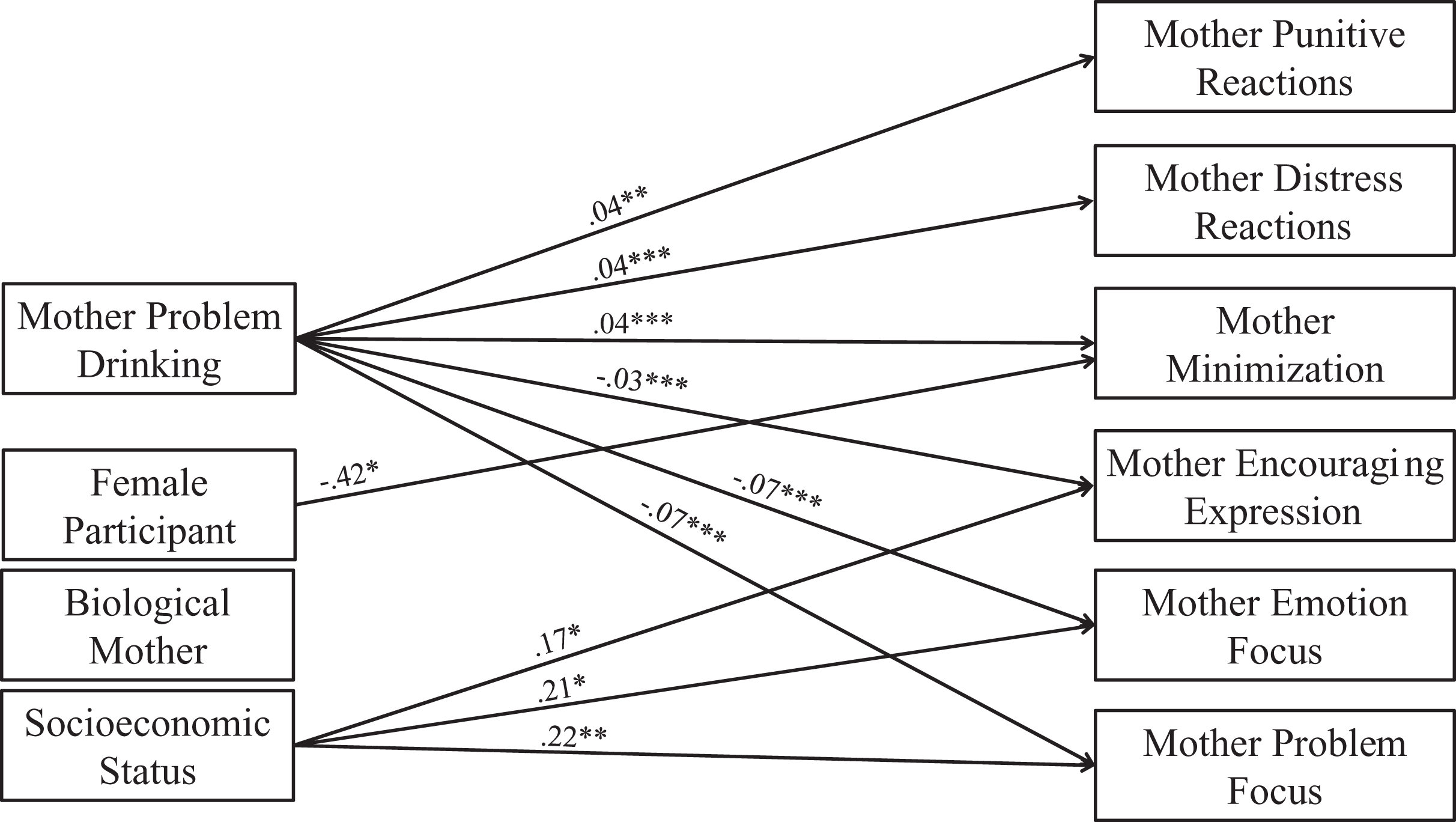
Associations between mother problem drinking and different forms of mother emotion socialization. Note. *p < .05. ** p < .01. *** p < .001. Model is fully saturated. Only significant associations are shown to make the figure easier to read. Coefficients are unstandardized.
The model including mother nonsupportive emotion socialization as an intervening variable of relations between mother problem drinking and offspring emotion regulation was an acceptable fit to the data (see Figure 2), χ2(12) = 21.61, p = .04, RMSEA = .047, CFI = .984, SRMR = .020. Mother problem drinking was significantly related to greater mother nonsupportive emotion socialization, B = 0.04, p < .001. In turn, mother nonsupportive emotion socialization was related to greater depressive rumination, B = 0.08, p < .05, and greater anger rumination, B = 0.01, p < .05. The indirect effect of mother problem drinking on depressive rumination through nonsupportive emotion socialization was significant, ZSOBEL = 2.13, p < .05. Similarly, the indirect effect of mother problem drinking on anger rumination through nonsupportive emotion socialization was significant, ZSOBEL = 2.42, p < .05. In addition to the indirect associations, mother problem drinking was also directly associated with greater depressive rumination and greater anger rumination, B = 0.01, p < .05.
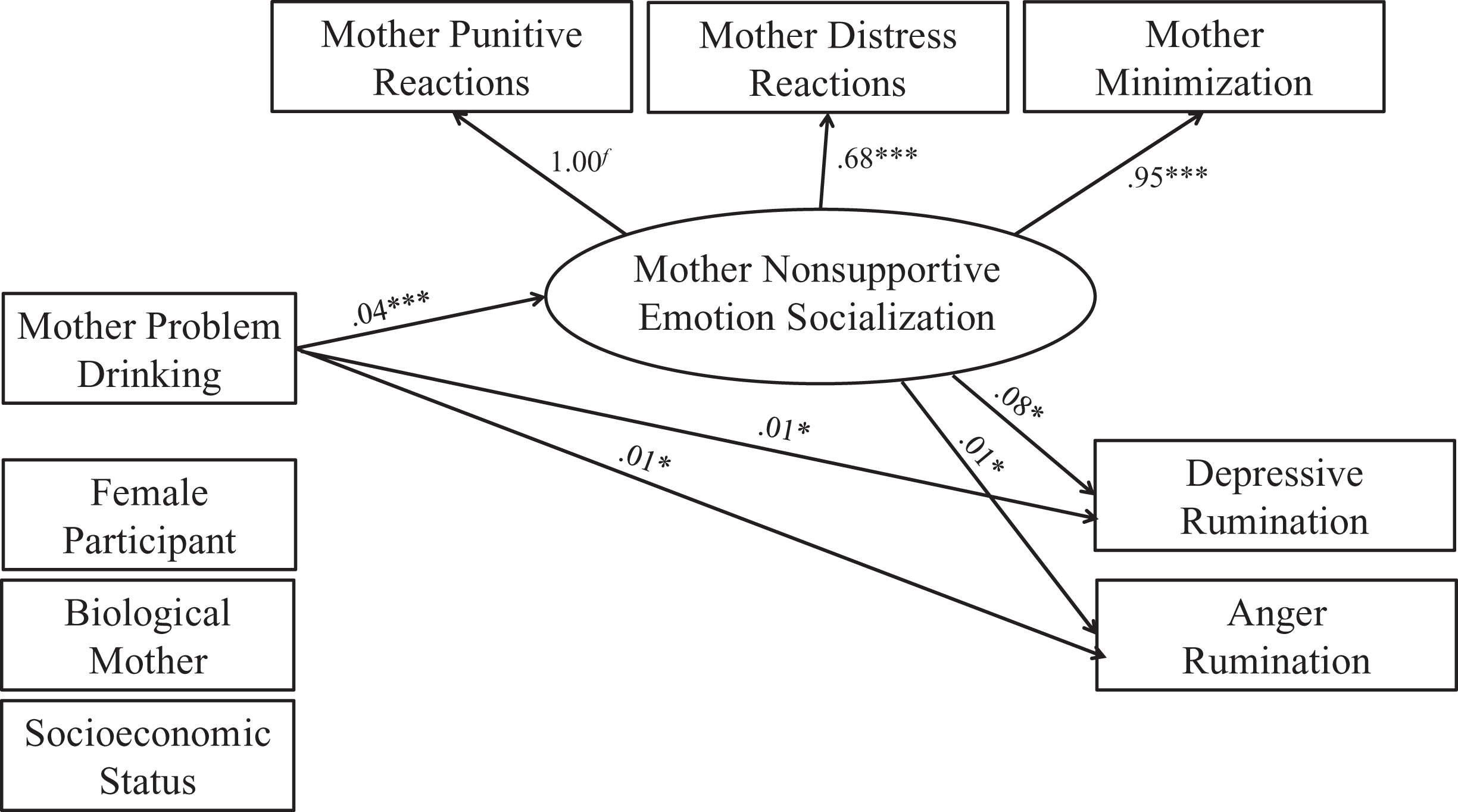
Mother nonsupportive emotion socialization as an intervening variable of relations between mother problem drinking and offspring emotion regulation. Note. *p < .05. **p < .01. ***p < .001. χ2(12) = 21.61; p = .04; RMSEA = .047 (90% CI: .009, .078); CFI = .984; SRMR = .020. Only significant associations are shown to make the figure easier to read. Coefficients are unstandardized.
The model including mother supportive emotion socialization as an intervening variable of relations between mother problem drinking and offspring emotion regulation was a good fit to the data (see Figure 3), χ2(12) = 19.07, p = .09, RMSEA = .040, CFI = .993, SRMR = .013. Mother problem drinking was significantly related to lower mother supportive emotion socialization, B = −0.04, p < .001. In turn, mother supportive emotion socialization was related to lower depressive rumination, B = −0.12, p < .01, and lower anger rumination, B = −0.10, p < .05. The indirect effect of mother problem drinking on depressive rumination through supportive emotion socialization was significant, ZSOBEL = 2.84, p < .01. Similarly, the indirect effect of mother problem drinking on anger rumination through supportive emotion socialization was significant, ZSOBEL = 2.31, p < .05. In addition to the indirect associations, there was a marginal direct association between mother problem drinking and greater depressive rumination, B = 0.01, p < .10, and a significant direct association between mother problem drinking and greater anger rumination, B = 0.01, p < .05.
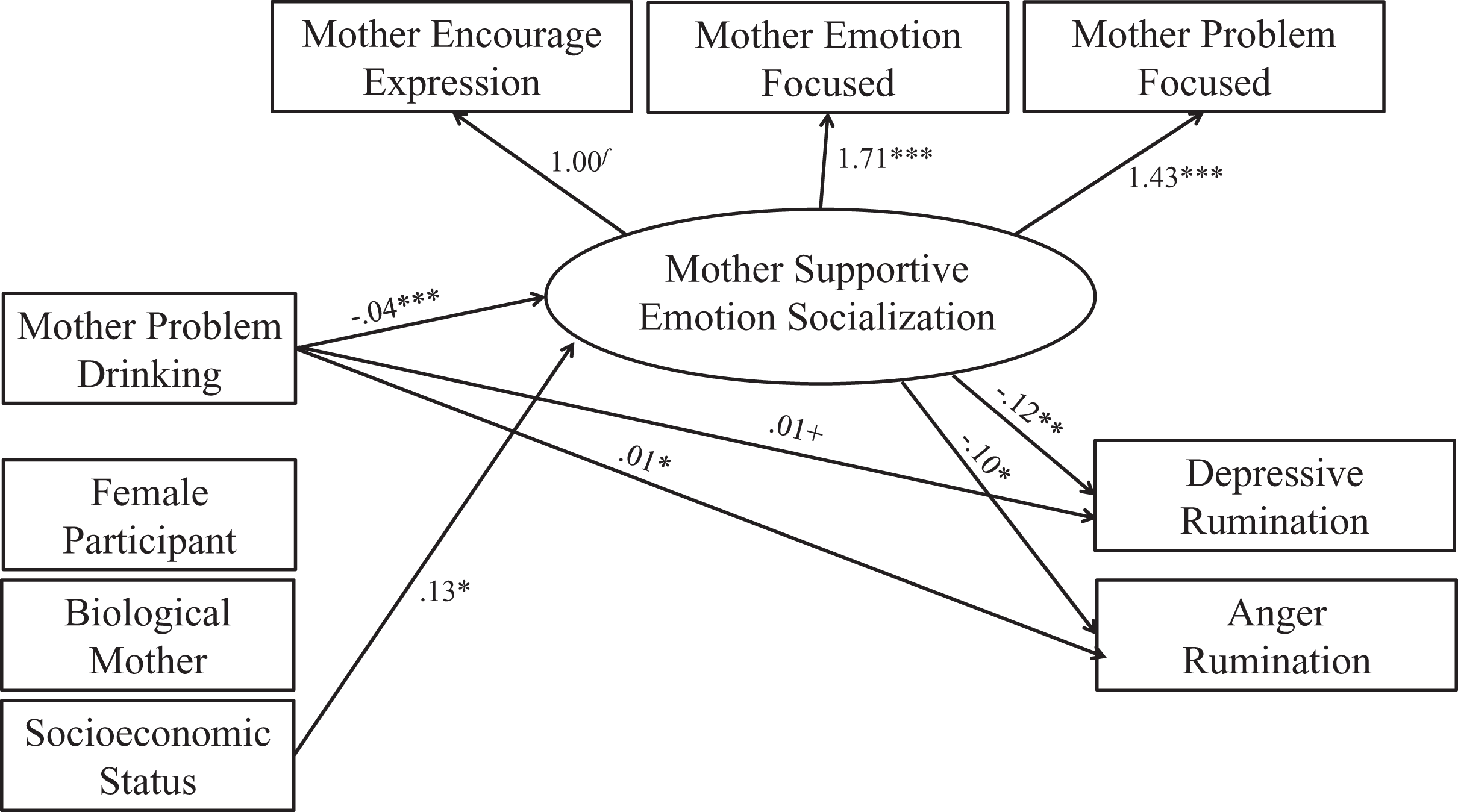
Mother supportive emotion socialization as an intervening variable of relations between mother problem drinking and offspring emotion regulation. Note. *p < .05. **p < .01. ***p < .001. +p < .10. χ2(12) = 19.07; p = .09; RMSEA = .040 (90% CI: .000, .073); CFI = .993; SRMR = .013. Only significant associations are shown to make the figure easier to read. Coefficients are unstandardized.
Father Problem Drinking and Emotion Socialization
The initial model in which father problem drinking was included as a predictor of each individual father reaction to child negative emotions was fully saturated and therefore fit indices are not interpreted (see Figure 4). Father problem drinking was significantly associated with greater father punitive reactions, B = 0.03, p < .001, greater father minimization, B = 0.04, p < .001, and greater father distress reactions, B = 0.03, p < .001, and lower father encouragement of expression, B = −0.04, p < .001, lower father emotion focused coping, B = −0.07, p < .001, and lower father problem focused coping, B = −0.07, p < .001. In addition, higher SES was related to greater father encouragement of expression, B = 0.16, p < .05, greater father emotion focused coping, B = 0.22, p < .01, and greater father problem focused coping, B = 0.24, p < .01. Finally, fathers were more minimizing of boys’ negative emotions than girls’ negative emotions, B = −0.39, p < .001.
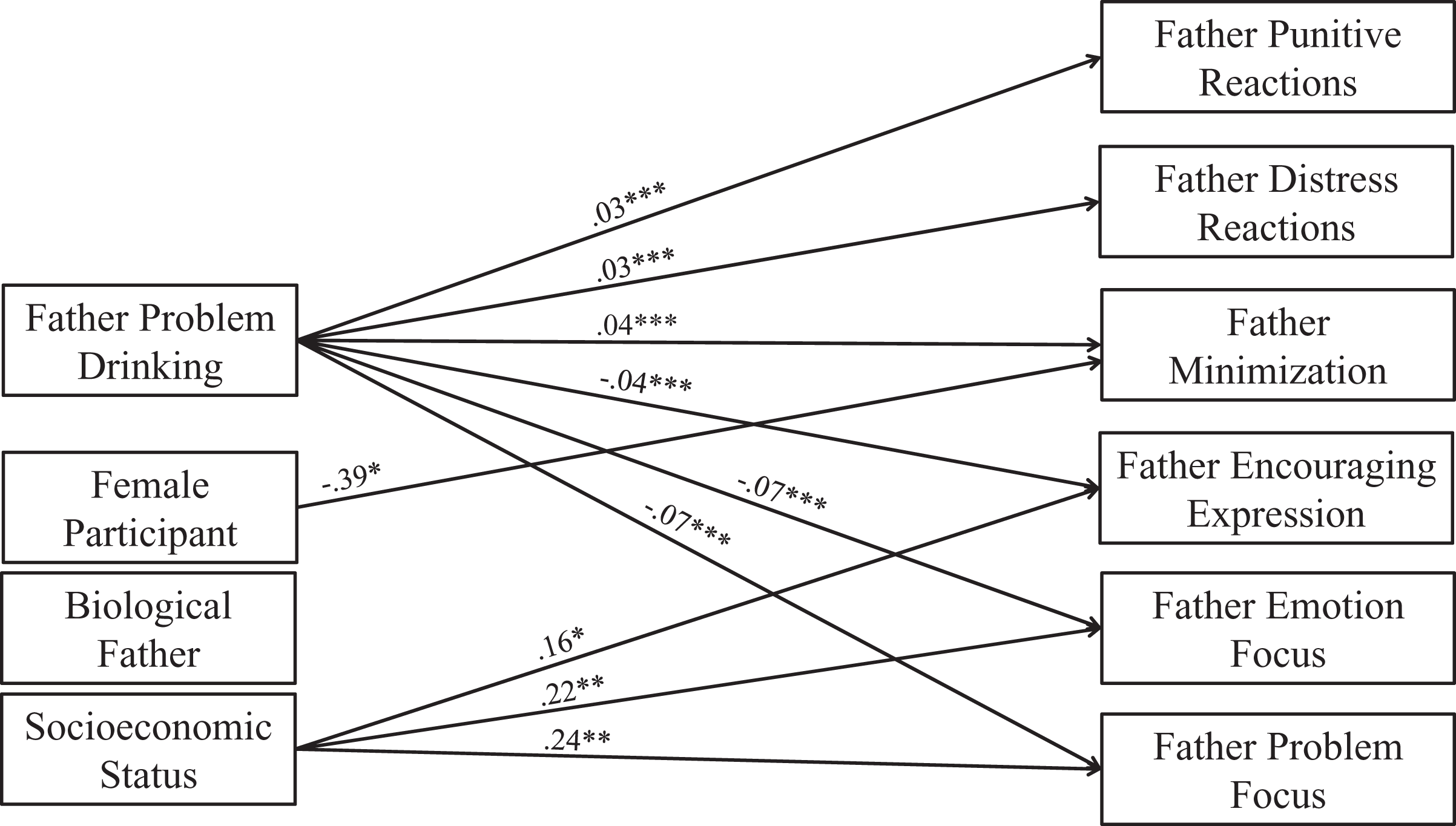
Associations between father problem drinking and different forms of father emotion socialization. Note. *p < .05. ** p < .01. *** p < .001. Model is fully saturated. Only significant associations are shown to make the figure easier to read. Coefficients are unstandardized.
The model including father nonsupportive emotion socialization as an intervening variable of relations between father problem drinking and offspring emotion regulation was an acceptable fit to the data (see Figure 5), χ2(12) = 24.50, p = .02, RMSEA = .053, CFI = .981, SRMR = .022. Father problem drinking was significantly related to greater father nonsupportive emotion socialization, B = 0.03, p < .001. In turn, father nonsupportive emotion socialization was related to greater depressive rumination, B = 0.11, p < .01, and greater anger rumination, B = 0.18, p < .001. The indirect effect of father problem drinking on depressive rumination through nonsupportive emotion socialization was significant, ZSOBEL = 2.19, p < .05. Similarly, the indirect effect of father problem drinking on anger rumination through nonsupportive emotion socialization was significant, ZSOBEL = 2.66, p < .01. There were no significant direct associations between father problem drinking and offspring emotion regulation.
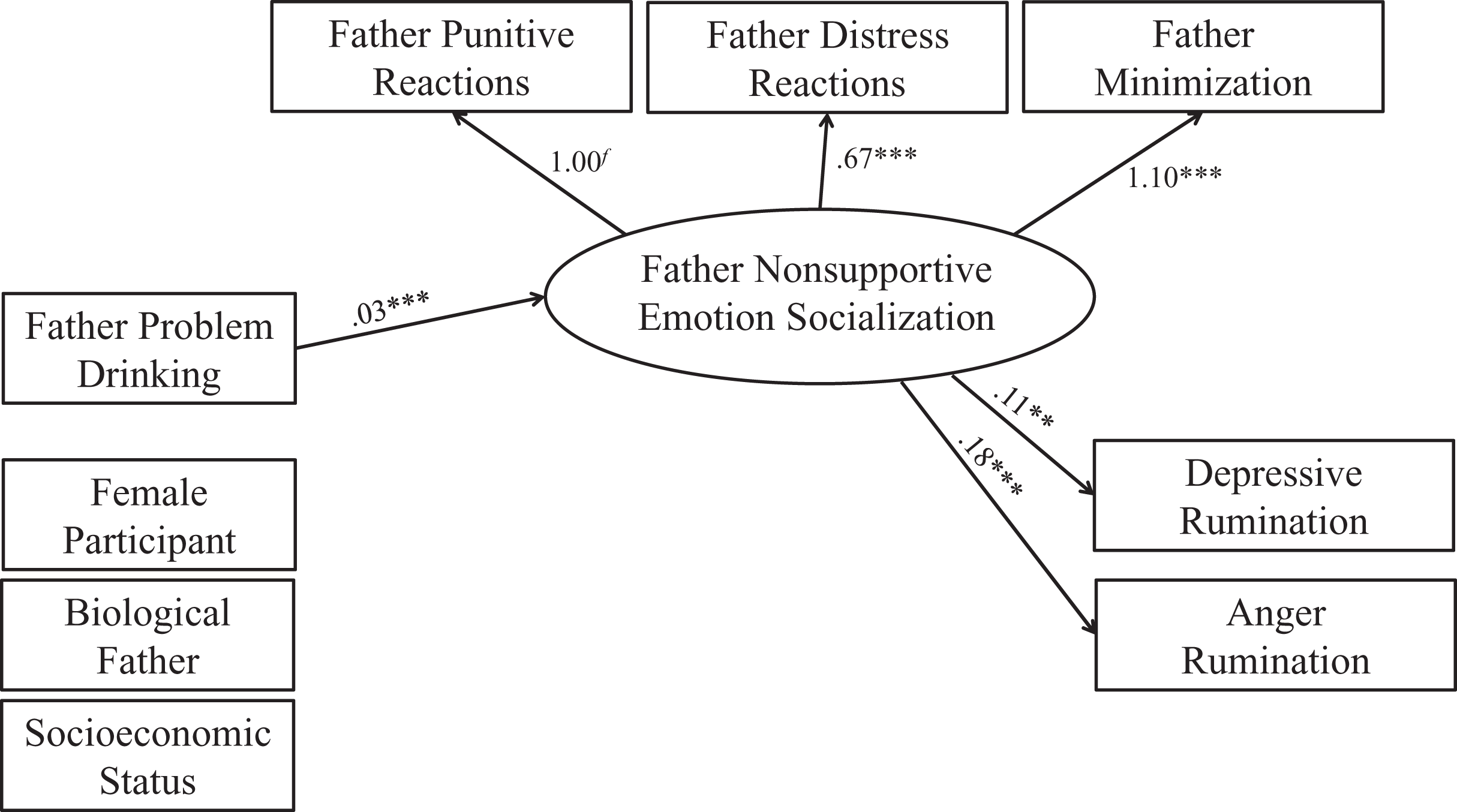
Father nonsupportive emotion socialization as an intervening variable of relations between father problem drinking and offspring emotion regulation. Note. *p < .05. **p < .01. ***p < .001. χ2(12) = 24.50; p = .02; RMSEA = .053 (90% CI: .022, .084); CFI = .981; SRMR = .022. Only significant associations are shown to make the figure easier to read. Coefficients are unstandardized.
The model including father supportive emotion socialization as an intervening variable of relations between father problem drinking and offspring emotion regulation was an acceptable fit to the data (see Figure 6), χ2(12) = 25.20, p = .01, RMSEA = .055, CFI = .988, SRMR = .017. Father problem drinking was significantly related to lower father supportive emotion socialization, B = −0.05, p < .001. In turn, father supportive emotion socialization was related to lower depressive rumination, B = −0.10, p < .01, and lower anger rumination, B = −0.12, p < .01. The indirect effect of father problem drinking on depressive rumination through supportive emotion socialization was significant, ZSOBEL = 2.41, p < .05. The indirect effect of father problem drinking on anger rumination through supportive emotion socialization was also significant, ZSOBEL = 2.73, p < .01. There were no direct associations between father problem drinking and offspring emotion regulation.
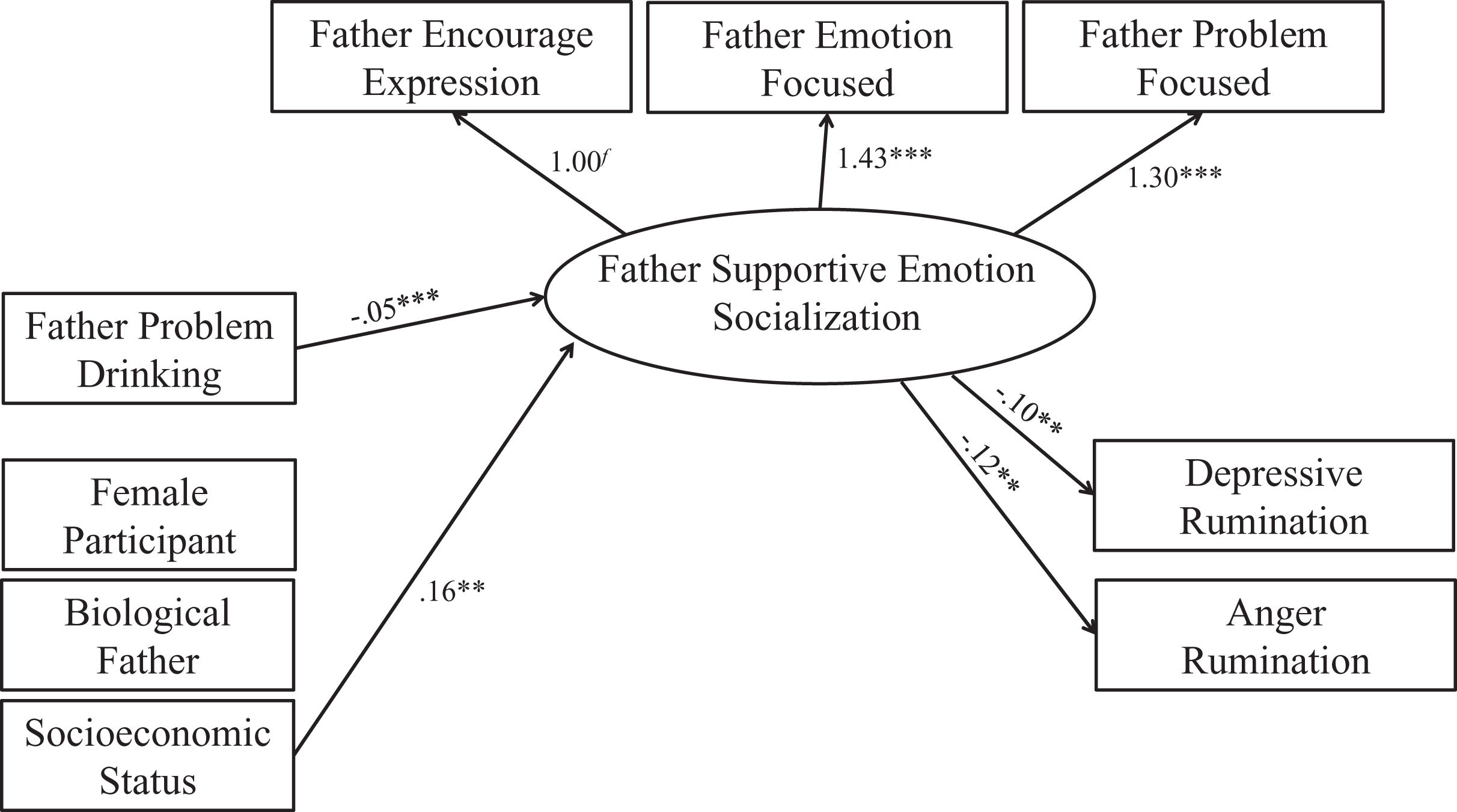
Father supportive emotion socialization as an intervening variable of relations between father problem drinking and offspring emotion regulation. Note. *p < .05. **p < .01. ***p < .001. χ2(12) = 25.20; p = .01; RMSEA = .055 (90% CI: .024, .085); CFI = .988; SRMR = .017. Only significant associations are shown to make the figure easier to read. Coefficients are unstandardized.
Discussion
This study examined associations between retrospective reports of PPD and supportive and nonsupportive emotion socialization by parents, as well as the role of parental emotion socialization in relations between PPD and college student emotion regulation. PPD was linked to college students’ perceptions of mother and father greater minimization, distress, and punitive reactions, and less problem focused reactions, emotion focused reactions, and encouragement of expression in response to the negative emotions of their children. Results also indicated that these perceptions of mother and father emotion socialization (supportive and nonsupportive) intervened in relations between PPD and emerging adult depressive and anger rumination. PPD was associated with recollections of less supportive and more nonsupportive parental emotion socialization, which in turn was related to greater college student anger and depressive rumination. These associations were observed even after controlling for participant sex, SES, and parent relationship type.
This is the first study, to our knowledge, to examine associations between PPD and parental emotion socialization. However, findings are consistent with studies of PPD and other forms of parenting. For example, PPD has been linked to cold and distant parenting (Iacopetti et al., 2021) and less positive parenting (Sternberg et al., 2018), suggesting that parents with drinking problems are unsupportive in other ways. Parents who suffer from drinking problems may be unable to properly socialize their children’s emotions because they have difficulties regulating their own emotions (Suzuki et al., 2020), and because frequent intoxication impairs the types of advanced cognitive functions required to socialize emotions (Shokri-Kojori et al., 2017). According to emerging adult perspectives, there were no specific forms of emotion socialization that were more closely tied to PPD than others. All coefficients were significant and similar in magnitude (although positive for nonsupportive socialization and negative for supportive socialization). This is consistent with an underlying factor structure for the specific behavioral reactions to child negative emotions; parents engage in a pattern of supportive versus nonsupportive (or vice versa) behavior rather than having a preference for one specific behavior (Fabes et al., 1990, 2001). Data are further supportive of such an underlying factor structure as intercorrelations among the different parent reactions were high and significant, and factor loadings on the latent variables were significant.
There were no meaningful differences between mother and father problem drinking associations with recalled parental emotion socialization. All coefficients were significant for both parents and similar in magnitude. Tests of associations controlling for the other parent in the same model were not conducted primarily because there was little rationale for mother problem drinking as a predictor of father emotion socialization or for father problem drinking as a predictor of mother emotion socialization. However, some reflection on the similarities in the coefficients is warranted. One possibility is that, as an artifact of the retrospective research design, participants did not distinguish between mother and father behavior. Examination of the correlation between mother and father problem drinking shows that it is under .5, indicating that participants were able to make a distinction between mother and father problem drinking. Correlations between the same mother and father emotion socialization behaviors ranged from .50 to .71, with most between .61 and .64. These are large correlations but again indicate that participants were evaluating mothers and fathers differently, as over half of the variance was independent between the two reports. Thus, rather than the similarity in coefficients reflecting a methodological artifact, there may in fact be similar psychological dynamics operating for mothers and fathers. This is consistent with research on associations between PPD and other forms of parenting. For example, college students report that both mothers and fathers exhibited significantly less acceptance growing up if they were alcoholics than if they were non-alcoholics (Kelley et al., 2005).
Results also indicated that recalled parent emotion socialization intervened in relations between PPD and emerging adult anger and depressive rumination. Less supportive emotion socialization and greater nonsupportive emotion socialization was linked to greater anger and depressive rumination. These findings are consistent with research on the importance of parent emotion socialization (Hajal & Paley, 2020). For example, mother daily supportive emotion socialization is related to more positive daily affect in adolescent girls, predicting improved emotion regulation and lower internalizing symptoms over time (Cui et al., 2020). The current study advances prior research by considering how emotion socialization processes may operate in the context of PPD. Persons exposed to PPD are known to have mental and physical health problems that are tied to poor emotion regulation skills. Unfortunately, little research on emotion regulation in this population has been conducted, and there has also been little research on PPD and parent emotion socialization. Findings suggest that parent emotion socialization may be an important pathway of risk for persons exposed to PPD, contributing to forms of emotion regulation that underlie depression and aggression in adulthood, and potentially the development of substance use problems. The public health implications of findings are therefore significant: targeting emotion socialization in problem drinking parents and emotion regulation in the offspring of problem drinkers may reduce negative health outcomes for the millions of Americans affected.
Although this study breaks important new ground in examining links between PPD and emotion regulation of emerging adults, study limitations should be taken into account. First, the study utilizes a retrospective design in which college students reported on the problem drinking and emotion socialization behaviors of their parents when they were children. Childhood memories may not be perfectly accurate. However, retrospective reports are a common research design in the study of persons exposed to PPD (Kelley et al., 2005), and there is evidence of the validity of retrospective reports (Hardt & Rutter, 2004). In addition, college students may not represent all emerging adults. Four-year college students are less diverse socioeconomically and racially, and are more likely to be female than the general population (https://nces.ed.gov/). Further, compared to emerging adults who are not attending college, college students are less likely to have children (Gault et al., 2016). These differences should be taken into account when generalizing findings. Second, emotion regulation is a complex skill. Examples of different forms of cognitive emotion regulation include catastrophizing, self-blame, and reappraisal (Dryman & Heimberg, 2018). Additional research is therefore needed to examine different aspects of emotion regulation in emerging adults exposed to PPD. Third, other forms of parental psychopathology related to PPD may be associated with emotion socialization difficulties. Breaux and colleagues (2016) also identified maternal anxiety, cluster A personality symptoms (odd and eccentric thinking and behavior; includes paranoid, schizoid, and schizotypal personalities), and cluster C personality symptoms (anxious and fearful thinking and behavior; includes avoidant, dependent, and obsessive-compulsive personalities) as correlates of non-supportive reactions to young child negative emotions (each examined in separate models). College students may have greater difficulty reporting on the depressive or anxiety symptoms of parents (there is no “Children of Depressed Parents Screening Test” as there is for PPD, for example), and thus we did not include these parental characteristics in the study.
Despite these limitations, findings support a model in which PPD is associated with poor parental emotion socialization of offspring, which contributes to difficulties in emotion regulation for those offspring during the transition from adolescence to adulthood. Both mother and father problem drinking were indirectly related to emerging adult rumination, but mother problem drinking was also directly related to emerging adult rumination. There are important public health implications of these findings, given the large number of persons exposed to PPD (Lipari & Van Horn, 2017), and the importance of emotion regulation for physical and mental health. Poor emotion regulation can contribute to over-eating, reduced exercise, increased substance use, depression, anxiety, and other mental disorders (Cludius et al., 2020). An important next step for research is to evaluate the role of emotion regulation difficulties in the development of such physical and mental health issues among persons exposed to PPD.
Footnotes
Author Contributions
Peggy S. Keller was responsible for pioneering the study, overseeing the collection of data, conducting the analyses, and oversaw the preparation of the manuscript. Haley Michlitsch was responsible for writing the manuscript and performing the literature review. Kyle P. Rawn was responsible for editing the document, preparing and formatting the document for submission, and for helping with the publishing process.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Open Practices
The raw data contained in this manuscript are not openly available due to privacy restrictions set forth by the institutional ethics board. However, the correlation matrix, means, and standard deviations presented in ![]() can be supplied as input into statistical software for analysis. No aspects of the study were pre-registered.
can be supplied as input into statistical software for analysis. No aspects of the study were pre-registered.