
Abstract
Evidence demonstrates an association between symptoms of attention-deficit/hyperactivity disorder (ADHD) and alcohol outcomes, though mechanisms underlying relations are unclear. Given that drinking motives (coping-anxiety, coping-depression, enhancement, social, and conformity) appear to serve as a mediator through which other factors influence drinking behavior, the current multi-site study examined the relation between ADHD symptoms and alcohol outcomes through motives. Past-month drinkers completed online measures assessing ADHD symptoms, alcohol use and problems, and drinking motives. A multiple-mediator model found inattention symptoms were: 1) positively associated with coping-depression, which positively related to alcohol use, which positively related to alcohol problems; 2) positively associated with enhancement motives, which positively related to use, which positively related to problems; and 3) positively associated with coping-anxiety, which negatively related to use, which positively related to problems. No indirect relations via motives were found for hyperactive-impulsive symptoms. Findings highlight unique associations depending on ADHD symptoms and specific drinking motives.
Keywords
Introduction
Prevalence rates for alcohol use are highest among young adults (Schulenberg, 2021), with college students reporting higher rates of annual and past-30-day use compared to their non-college peers, identifying this population as a significantly at-risk group for problematic alcohol use. Attention-deficit/hyperactivity disorder (ADHD) is a neurodevelopmental disorder characterized by a persistent pattern of inattentive (e.g., difficulty sustaining focus) and/or hyperactive-impulsive (e.g., excessive fidgeting or talking, interrupting others) symptoms (American Psychiatric Association [APA], 2013). Attention-deficit/hyperactivity disorder symptoms and related impairment often persist into adolescence and adulthood (Barkley et al., 2010), and 2–8% of college students report ADHD symptoms (DuPaul et al., 2009). College students with ADHD symptoms appear to be at a higher risk for problematic drinking compared to their peers without these symptoms, given positive associations between ADHD symptoms and both alcohol use (Blase et al., 2009) and alcohol-related problems (Baker et al., 2012; Rooney et al., 2015). Further research to understand these relations is needed, including whether ADHD symptoms may be particularly associated with certain drinking motives (i.e., reasons for alcohol use), and consequently associated with greater levels of use and related problems.
Motivational models of alcohol use suggest that an individual’s reasons for drinking are among the most proximal predictors of drinking patterns and are thought to serve as a mediating mechanism by which other variables, including potentially ADHD symptoms, operate to influence alcohol use (Cox & Klinger, 1988). These motives are thought to vary along two dimensions: type of reinforcement (positive or negative reinforcement) and source of motivation (internal or external). The combination of these two dimensions results in four distinct drinking motives: coping (internal, negative, i.e., drinking to reduce or avoid negative mood), enhancement (internal, positive, i.e., drinking to enhance positive mood), social (external, positive, i.e., drinking to obtain social rewards), and conformity (external, negative, i.e., drinking to avoid negative social consequences). Different drinking motives predict unique aspects of drinking behavior, whereby negatively reinforcing motives (coping and conformity) are found to be most associated with alcohol-related problems, and internal motives (enhancement and coping) are most related to frequency of use (Kuntsche et al., 2005). However, some research investigating coping motives among older adolescents and undergraduates has yielded discrepant findings, whereby coping motives were not found to predict higher alcohol consumption and related problems (Bradizza et al., 1999; Perkins, 1999; Read et al., 2003). To account for these inconsistent findings and combined with evidence that depression and anxiety may be differentially associated with certain patterns of alcohol use (Graham et al., 2007; Morris et al., 2005), a five-factor motives model has been proposed differentiating between drinking to cope with anxiety and drinking to cope with depression. Using this modified model, Grant et al. (2007) found that coping-depression motives were associated with drinking quantity, while coping-anxiety motives were directly related to alcohol-related problems among undergraduates.
Drinking motives are also differentially associated with several personality and behavioral constructs such as impulsivity, emotion dysregulation, and disinhibition (Jones et al., 2014; Retz et al., 2012; Rooney et al., 2015; Simons et al., 2017). For example, among college students, the urgency (i.e., tendency to act rashly when faced with intense emotional contexts) facet of impulsivity is associated with coping motives, whereas the lack of premeditation (i.e., tendency to make decisions without considering their consequences) facet is associated with enhancement motives (Jones et al., 2014). Additionally, both coping and enhancement drinking motives have been found to mediate the link between emotion regulation and problematic drinking (Aurora & Klanecky, 2016). Given that individuals with high levels of ADHD symptoms tend to also be high in impulsivity and experience elevated emotion dysregulation (Hirsch et al., 2019), and that ADHD symptoms are also positively associated with perceived stress (Combs et al., 2015), it is possible that ADHD symptoms may be uniquely related to certain drinking motives (e.g., drinking to cope), which in turn are related to alcohol use and problems.
Though limited, existing research that has investigated drinking motives among college students with ADHD symptoms found that enhancement and/or coping motives may convey greatest risk for engaging in problematic alcohol use (Grazioli et al., 2019; Howard & Pritchard, 2017). Yet, the scope of this research has been limited to examination of only these two specific motives and has not differentiated between coping with anxiety and coping with depression as recommended by Grant et al. (2007). Therefore, to our knowledge, a comprehensive test of the five-factor motives model has not been conducted among college students with ADHD symptoms. Given existing research demonstrating that ADHD commonly co-occurs with both anxiety and depression (D’Agati et al., 2019; Sobanski et al., 2007), the five-factor model may provide invaluable insight for understanding pathways underlying the association between ADHD symptoms and alcohol use and may aid in treatment recommendations. This may be of particular importance as more recent research has highlighted the substantial burden that both anxiety and depression have on individuals with ADHD (Babinski et al., 2020; Quenneville et al., 2022). It has been posited that emotion dysregulation may be responsible for the functional impairment associated with ADHD symptoms as well as comorbid symptoms such as anxiety and depressive symptoms, which may ultimately leave limited resources for one’s ability to effectively cope (Howard et al., 2019). Thus, it may be possible that students high in ADHD symptomatology are particularly likely to drink to cope with either or both types of associated affective symptoms. It is particularly important to examine whether there are differential associations with each type of coping, which may more precisely inform future research on mechanistic pathways and targeted interventions for problematic alcohol use among students with ADHD.
Despite the evident link between ADHD and alcohol use among college students, the mechanisms explaining this relation remain unclear. A comprehensive examination of the indirect effects of drinking motives on the relation between ADHD symptoms and alcohol-related outcomes is necessary and may aid in understanding the increased risk of problematic drinking associated with ADHD symptoms. Additionally, research investigating ADHD symptoms and substance use more generally suggests that ADHD symptom clusters (i.e., inattention and hyperactive-impulsive) may differentially relate to aspects of substance use behavior (Chang et al., 2012; Elkins et al., 2007). Therefore, relations between alcohol use and ADHD symptoms, including the role of drinking motives, may be better understood when examined by symptom cluster. As such, we tested a path model examining relations between ADHD symptom clusters and alcohol-related problems via drinking motives and frequency of alcohol use. Based on past research demonstrating associations between both inattention and hyperactivity/impulsivity symptom clusters with alcohol use (Roberts et al., 2014), we expected to find direct effects from both symptom clusters to alcohol use and associated problems. Yet, consistent with work by Grazioli et al. (2019), we expected to find differences in indirect effects by ADHD symptom cluster, such that only inattentive ADHD symptoms would be associated with stronger enhancement and coping motives, which in turn would be associated with greater alcohol use, and subsequently more alcohol-related problems. Given the lack of research on other drinking motives as related to ADHD symptom clusters, we did not advance any specific hypotheses for those pathways.
Method
Participants and Procedures
The current study used data collected during the 2018–2019 wave of the Undergraduate Learning, Emotion, and Attention Research Network (U-LEARN) study. Data were collected at three sites (Appalachian State University, University of Northern Iowa, University of Wyoming) across the United States. College students (N = 1513) completed an online survey as part of a course assignment and/or for extra credit via psychology department participant pools. Upon providing informed consent, participants completed measures of demographics, ADHD symptoms, substance use, and other related constructs. Only measures relevant to the current study are described herein. This study was approved by each collaborating university’s Institutional Review Board.
The analytic sample (N = 872) was restricted to past-month alcohol users aged 18–25 who reported on their biological sex, past-six-month ADHD symptoms, and past-month alcohol use, drinking motives, and alcohol-related problems. Participants were predominantly female (68.5%) with a mean age of 19.36 years (SD = 1.44). Participants identified as White (87.0%), Hispanic/Latino (4.6%), mixed race (2.5%), African American (2.2%), Asian/Asian-American (1.9%), American Indian (0.7%), and Pacific Islander (0.5%), with 0.6% not responding.
Measures
Demographics
A demographics questionnaire included items assessing age, race, and biological sex.
Daily Drinking Questionnaire
Past-month alcohol use was assessed using a modified version of the Daily Drinking Questionnaire (DDQ; Collins et al., 1985). Using a 7-day calendar, participants indicated the number of standard drinks they typically consumed for each day of the week during the past month. Number of standard drinks consumed were summed to calculate a past-month weekly drinks score.
Drinking Motives Questionnaire
Drinking motives over the past month were examined via the 28-item Drinking Motives Questionnaire – Revised (DMQ-R; Grant et al., 2007), assessing for five unique drinking motivations: coping-anxiety (e.g., “because it helps me when I am feeling nervous; ” α = 0.73), coping-depression (e.g., “because it helps me when I am feeling depressed; ” α = 0.95), enhancement (e.g., “because I like the feeling; ” α = 0.83), social (e.g., “to be sociable; ” α = 0.73), and conformity (e.g., “so I won’t feel left out; ” α = 0.86). Each item was measured on a 5-point scale (1 = never/almost never; 5 = almost always/always). Items on each motive factor were summed and averaged.
Alcohol-Related Problems
Past-month alcohol-related problems were examined via a modified version of the Rutgers Alcohol Problem Index (RAPI; White & Labouvie, 1989). The RAPI is comprised of 23 items assessing the frequency with which participants have experienced various alcohol-related consequences. The current study utilized a modified 25-item version that included two additional items, “drove shortly after having more than two drinks” and “drove shortly after having more than four drinks” (Neighbors et al., 2006). Frequency with which each consequence was experienced was assessed via a 4-point scale (0 = none; 3 = more than 5 times); scores were summed for an overall problems score (α = 0.92).
ADHD Symptoms
Past-six-month ADHD symptoms were assessed via the 18-item DSM-5 ADHD Symptoms Checklist, in which participants were asked to report how frequently they experienced each symptom via a 4-point scale (0 = never; 3 = very often) when not taking ADHD medication. Items assessed both inattention (9 items; α = 0.93) and hyperactivity/impulsivity (9 items; α = 0.88) symptom clusters based on ADHD symptoms listed in the Diagnostic and Statistical Manual of Mental Disorders (5 th ed.; APA, 2013). Frequency scores for items on each symptom cluster were summed.
Data Analysis Plan
A saturated path model was conducted using Mplus 8.6 (Muthén & Muthén, 1998 – 2017). Specifically, the five drinking motives were tested as parallel mediators in a multiple mediator model: ADHD symptom clusters → drinking motives → past-month alcohol use → past-month alcohol-related problems. Every variable was standardized (i.e., z-scores) to produce standardized regression coefficients. We examined the total, direct, and indirect effects using bias-corrected bootstrapped estimates (Efron & Tibshirani, 1993), which is robust to small departures from normality (Erceg-Hurn & Mirosevich, 2008). Statistical significance was determined by 95% bias-corrected bootstrapped confidence intervals (based on 10,000 bootstrapped samples) that did not contain zero. Though we employed a mediational path model, causal relationships between variables could not be examined given the cross-sectional nature of the study. A power analysis was not conducted, as this was as a secondary analysis from a large, multi-site data set. However, following a recommendation outlined by Kline (1998) that an adequate sample size for path analysis is equal to 10 times the number of parameters in the study, the current study would require a sample size of 720 when accounting for all direct and indirect effects. Thus, it was concluded that the analytic sample of 872 was sufficient for the planned analysis.
Results
Bivariate Correlations and Descriptive Statistics Among All Study Variables.
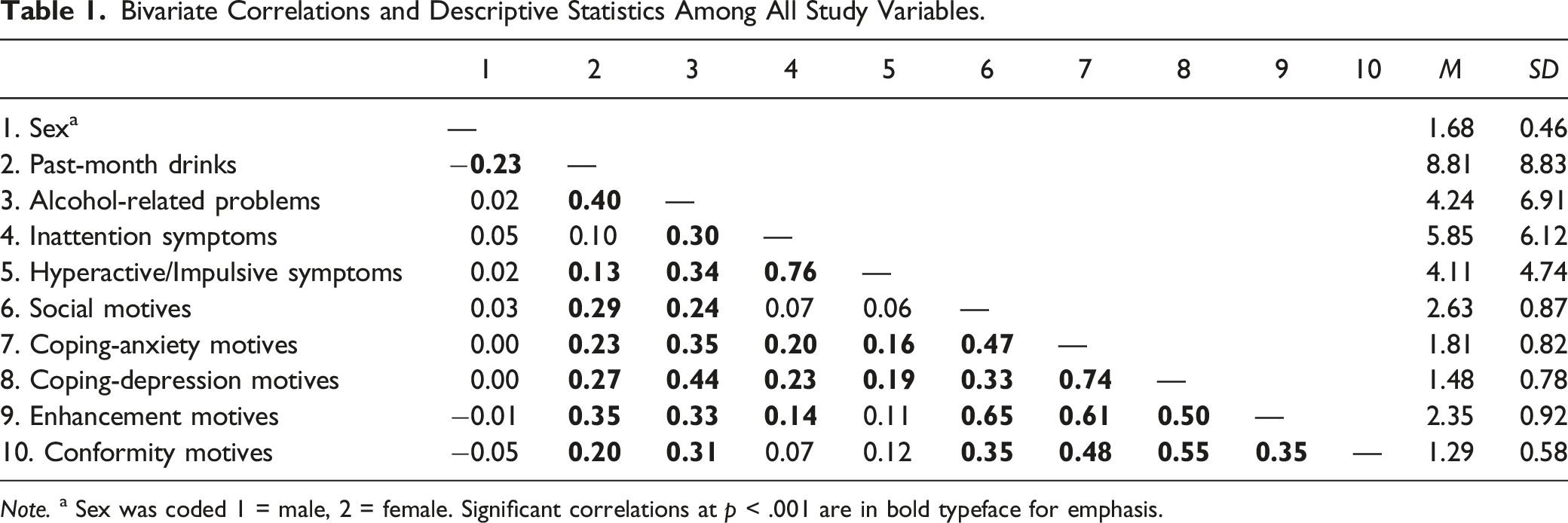
Note. a Sex was coded 1 = male, 2 = female. Significant correlations at p < .001 are in bold typeface for emphasis.
Summary of Total, Indirect, and Direct Effects of ADHD Symptoms on Alcohol-related Problems via Drinking Motives and Alcohol Consumption.
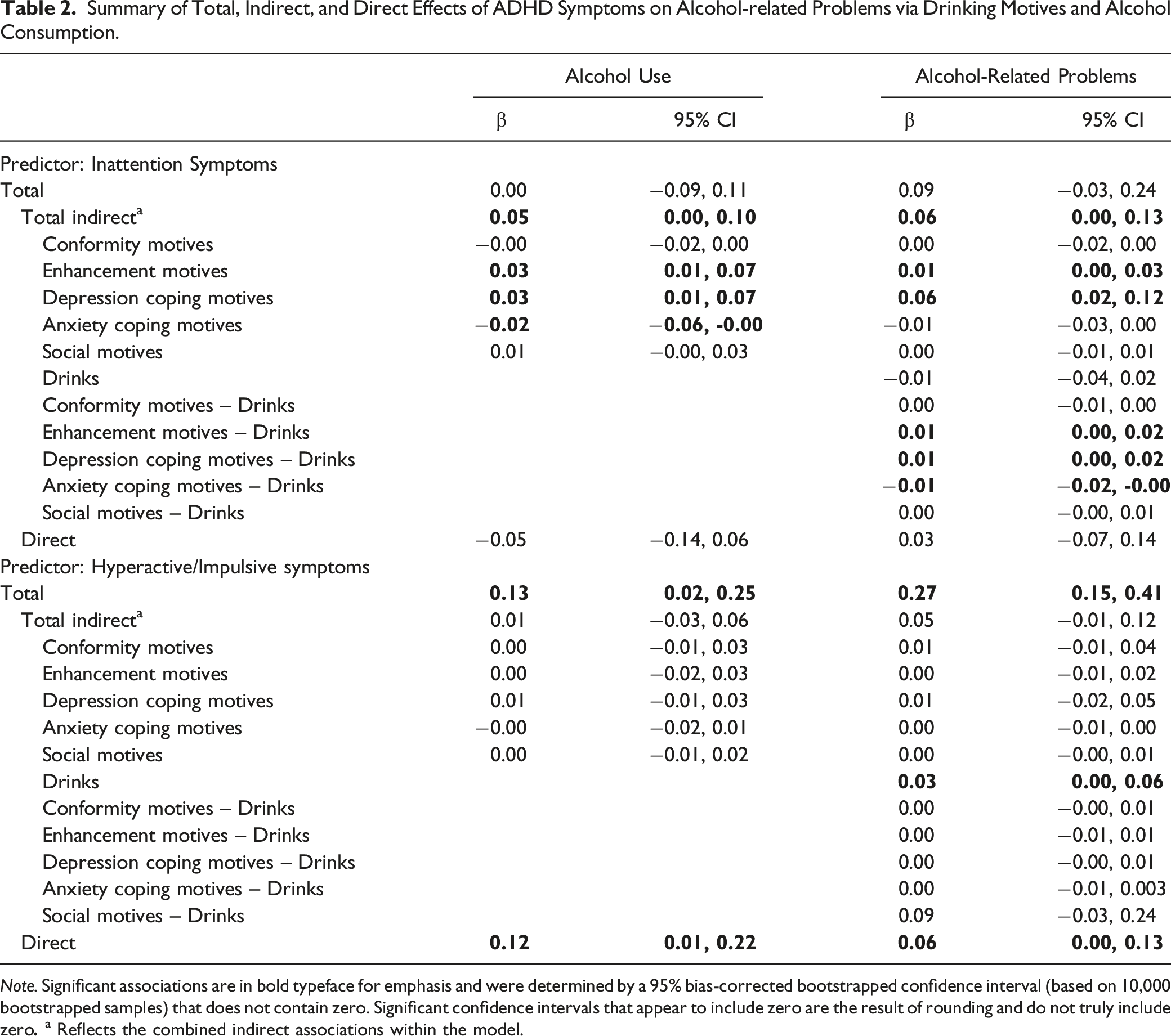
Note. Significant associations are in bold typeface for emphasis and were determined by a 95% bias-corrected bootstrapped confidence interval (based on 10,000 bootstrapped samples) that does not contain zero. Significant confidence intervals that appear to include zero are the result of rounding and do not truly include zero
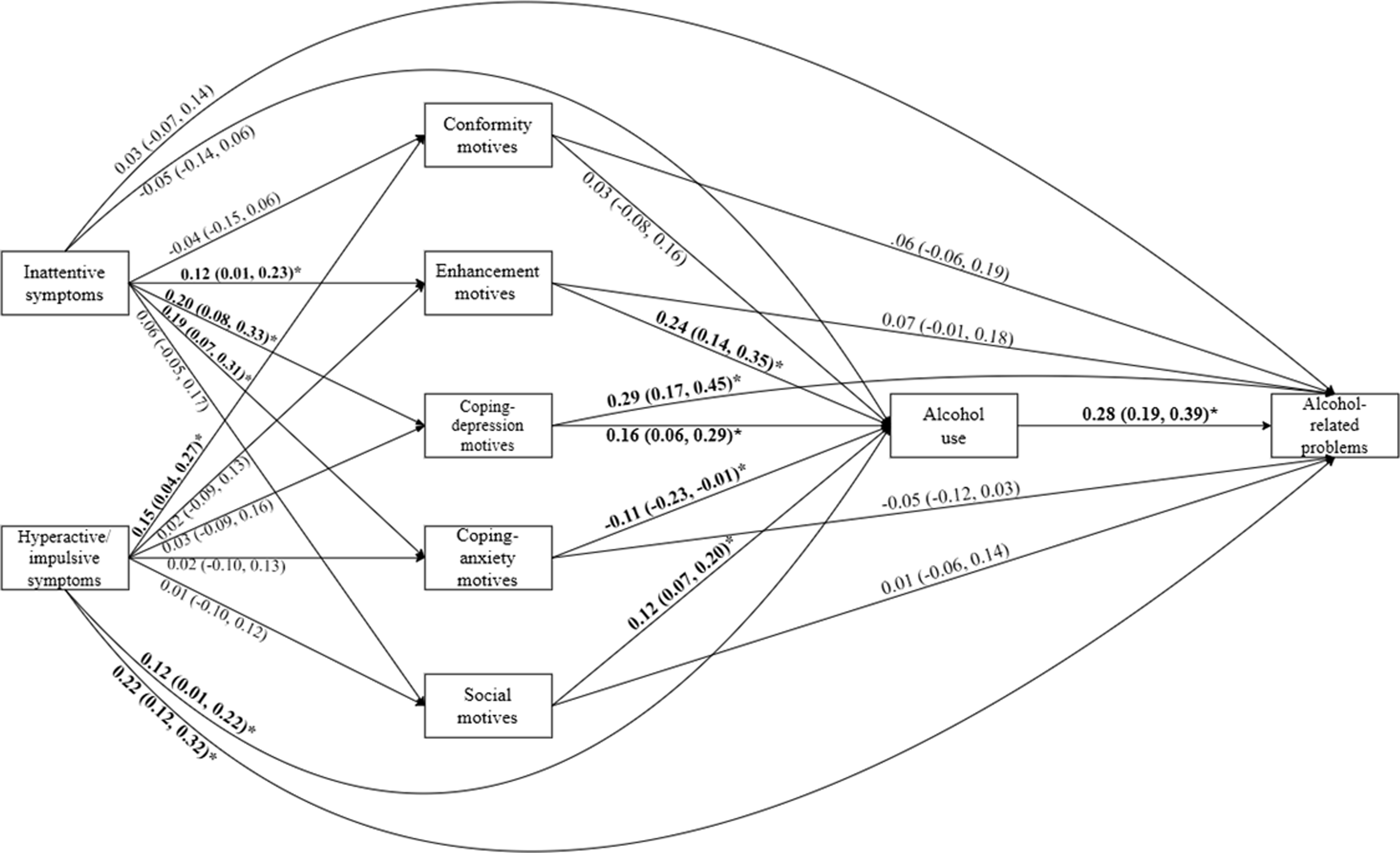
Path model depicting the direct effects of ADHD symptoms on alcohol-related problems via drinking motives and alcohol consumption. Note. Depicts the standardized effects of the path model predicting alcohol-related problems. Significant associations are in bold typeface for emphasis and were determined by a 95% bias-corrected bootstrapped confidence interval (based on 10,000 samples) that does not contain zero.
Inattention Symptoms as Predictor
There was not a significant direct effect of inattention symptoms on alcohol-related problems, nor a significant direct effect of inattention symptoms on past-month alcohol use. Given that a significant zero-order (or direct) effect is not needed to establish indirect effects (Hayes, 2017; Zhao et al., 2010), we proceeded to examine and interpret indirect effects despite lack of direct effects in our model. Significant indirect effects of inattention symptoms through drinking motives were found on both past-month alcohol use and problems. Regarding alcohol use, there were positive indirect effects from inattention symptoms through both enhancement and coping-depression motives. On the other hand, there was a negative indirect effect of coping-anxiety motives, such that greater inattention symptoms were associated with higher coping-anxiety motives, which in turn was associated with lower levels of alcohol use.
Regarding alcohol-related problems, there were again positive indirect effects from inattention symptoms through both enhancement and coping-depression motives. Further, there were three serial indirect effects: (a) inattention symptoms were positively associated with coping-depression motives, which in turn were associated with higher alcohol consumption, which was associated with greater alcohol-related problems; (b) inattention symptoms were positively associated with enhancement motives, which in turn were associated with higher alcohol consumption, which was associated with greater alcohol-related problems; and (c) inattention symptoms were positively associated with coping-anxiety motives, which were associated with lower alcohol consumption, which in turn was associated with fewer alcohol-related problems.
Hyperactive-Impulsive Symptoms as Predictor
In contrast to inattention symptoms, there was a significant positive direct effect of hyperactive-impulsive symptoms on both past-month alcohol use and problems. There was also a significant positive indirect effect of hyperactive-impulsive symptoms on alcohol-related problems through alcohol use. However, there were no significant indirect effects of hyperactive-impulsive symptoms on either alcohol use or related problems through drinking motives.
Exploratory Sex Invariance Testing
Given prior research demonstrating sex or gender differences on all variables in the model (Foster et al., 2014; Nolen-Hoeksema, 2004), we conducted an exploratory multi-group analysis to determine whether associations in the model were invariant by biological sex. We used χ2 difference tests to evaluate whether a freely estimated multi-group model differed from a constrained multi-group model. Given that the χ2 test statistic is sensitive to sample size (Brown, 2015), invariance was determined at p > .01. Results for the fully constrained model suggested that this model was not invariant across biological sex (p < .001). To identify an invariant model, we identified the path with the greatest contribution to reducing model fit within the fully constrained model. Once we identified this path and allowed it to be freely estimated, we identified and freely estimated the next path with the greatest contribution at reducing model fit, repeating this procedure until we achieved acceptable model fit.
In the final multi-group model (χ2 (34) = 45.78, p = .09; CFI = 1.0, TLI = 0.99), all associations were constrained between sex except for two paths: (a) the path between conformity motives and past-month alcohol-related problems, and (b) the path between social motives and past-month alcohol use. The relation between conformity motives and alcohol-related problems was positive and significant for female students (β = 0.16, 95% CI [0.00, 0.34]), yet negative and non-significant for male students (β = −0.06, 95% CI [−0.18, 0.07]). The relation between social motives and alcohol use was positive and significant for both male (β = 0.34, 95% CI [0.20, 0.48]) and female (β = 0.07, 95% CI [0.00, 0.14]) students, but the effect was much larger for male students. Examination of indirect effects involving these pathways in the multigroup model indicated a significant indirect effect whereby higher levels of hyperactive-impulsive symptoms were related to stronger conformity motives, which were related to more alcohol-related problems for female students (β = 0.03, 95% CI [0.00, 0.07]) but not male students (β = −0.01, 95% CI [−0.04, 0.01]). There were no other significant indirect effects in the multi-group model for either male or female students that involved other non-invariant paths. Importantly, all significant indirect effects identified in the overall model were found to be invariant across biological sex.
Discussion
The current study examined the relations among ADHD symptom clusters (i.e., inattention, hyperactivity/impulsivity), drinking motives, and alcohol outcomes to gain a better understanding of the mechanisms underlying the increased risk of problematic drinking among college students with ADHD symptoms. To explore these relations, we tested a path model through which we examined associations between ADHD symptom clusters and alcohol-related problems via drinking motives and frequency of alcohol use. This study expands upon previous work examining the relation between ADHD symptoms and alcohol use by including a comprehensive examination of five factors of drinking motives, differentiating between drinking to cope with depression and drinking to cope with anxiety motives, and by examining ADHD symptoms separately by cluster. Findings revealed unique indirect paths depending on ADHD symptom cluster and type of drinking motive endorsed, underscoring the importance of distinguishing between ADHD symptom type and specific motive for drinking in examining the relation between ADHD and problematic alcohol use.
There were significant positive indirect effects of coping and enhancement motives on the association between ADHD symptoms and alcohol outcomes; as predicted, this was only true for inattention symptoms. While prior findings link facets of impulsivity (i.e., urgency, lack of premeditation) with coping and enhancement motives (Jones et al., 2014), our results are consistent with and extend those by Grazioli et al. (2019) who similarly found indirect effects of these motives for inattention but not hyperactive/impulsive symptoms on heavy episodic drinking and alcohol use disorder symptoms among young men. The authors suggested that men high in inattention symptoms may be uniquely at-risk for problematic alcohol use due to attempts to cope with their symptoms. Yet, the present study, which differentiated between types of coping, revealed an important nuance: inattentive ADHD symptoms were associated with greater alcohol use and problems through higher coping with depression motives, but less alcohol use and related problems through higher coping with anxiety motives, and this was invariant across biological sex. Thus, it appears that depression symptoms, specifically, may convey increased risk for problematic alcohol use among students with inattention symptoms.
The emotional cascade model of dysregulated behavior, which attempts to explain the link between emotional dysregulation and behavioral dysregulation (Selby et al., 2008), may offer one explanation for the current findings. This model suggests that a negative emotion-eliciting event triggers excessive rumination, which increases the emotion’s intensity. This prompts further rumination, creating a positive feedback loop and a highly aversive emotional state. Consequently, engagement in maladaptive behavior as an attempt to distract from the emotion is likely to occur. This model has been used to explain the role of rumination in the relation between emotional disorders (e.g., depressive and anxiety disorders) and alcohol use disorder (Wolitzky-Taylor et al., 2021), and may be extended to include inattention symptoms, as dysfunctions in attention may precipitate, or even be, a negative emotion-eliciting event. Given that individuals with higher levels of ADHD symptomatology are likely to experience deficits in emotion regulation (Hirsch et al., 2019), they may have significant difficulty employing adaptive emotion regulation skills in the face of these negative emotion-eliciting events, resulting in the use of maladaptive strategies, such as rumination, and then subsequent behavioral dysregulation in the form of alcohol use.
There is also evidence that a sluggish cognitive tempo (SCT), characterized by drowsiness, lethargy, and forgetfulness, presents as a prominent feature among those with the predominantly inattentive subtype of ADHD, as well as those experiencing depressive symptoms (Derefinko et al., 2008; Meinzer et al., 2012). Thus, the indirect effects of motives on the relation between inattentive symptoms and alcohol-related problems may in part be explained via the propensity to experience this cognitively impairing SCT symptomatology which individuals then attempt to cope with via drinking. However, this explanation may be specific to depression symptoms only. College students who are high in inattention symptoms report using alcohol to cope with anxiety; however, they report drinking less and experience fewer alcohol-related problems. This may be explained by research suggesting that anxiety (specifically social anxiety) may cause individuals to avoid social situations, thereby reducing the number of opportunities to engage in alcohol use. Using alcohol to cope with anxiety may occur only when social situations cannot be avoided (Norberg et al., 2009; Stewart et al., 2006). Enhancement motives were also a significant mediator of the relation between inattention ADHD symptoms and alcohol outcomes. Specifically, inattention symptoms were positively associated with enhancement motives, which in turn was associated with higher alcohol consumption, which in turn was associated with greater alcohol-related problems. As ADHD is associated with difficulty delaying gratification, tendency to become bored easily, and a proclivity for seeking out thrilling activities (APA, 2013; Hurst et al., 2011), students with elevated inattention symptoms may be motivated to seek ways to enhance their mood (e.g., through alcohol use) when aspects of their environment do not otherwise provide sufficient gratification.
Though several indirect effects were found for inattention symptoms, there were surprisingly no significant direct effects to alcohol use or problems, indicating that motives for alcohol use are necessary to consider in understanding risk for problematic use among students experiencing problems with inattention. In contrast, hyperactive-impulsive symptoms were directly related to both alcohol use and problems, though there were no indirect effects related to this symptom cluster. Other research also finds direct associations between impulsivity and alcohol use (e.g., Magid et al., 2007), complementing these findings. Additionally, perhaps drinking motives do not have a significant impact on the relation between hyperactive-impulsive symptoms and alcohol use because the behavior is more impulsively driven, therefore the individual lacks adequate time to consider the motives for which they are drinking.
The current study extends previous research related to ADHD and alcohol use, indicating that enhancement and coping motives should be considered in understanding the relation between inattention symptoms and alcohol use, and highlighting the need to assess coping with depression and anxiety separately. Importantly, the indirect paths from ADHD symptoms to alcohol use and problems through motives were largely sex invariant, suggesting that these factors function similarly for biological male and female students. However, since our analyses examining invariance by sex were post-hoc and exploratory, studies are needed that are specifically designed to examine how indirect pathways between ADHD symptoms and alcohol use differ by sex, gender, and other diversity factors. Additionally, clarification on why there were not indirect effects on alcohol use and problems through social and conformity motives is needed. Notably, coping and enhancement motives are internal motives, while social and conformity motives are external. As mentioned, elevated ADHD symptoms are often associated with emotion dysregulation (Hirsch et al., 2019), perceived stress (Combs et al., 2015), and other negative internal experiences, which may explain why internal motives are relevant for alcohol-related outcomes associated with ADHD symptoms. Further, adults with elevated ADHD symptoms often also experience social and interpersonal difficulties and unstable relationships (Biederman et al., 1993), which may limit their social opportunities, thereby reducing the relevance of external motivations for alcohol-related outcomes in this population.
Although our study yielded novel and important findings, there were several limitations that should be addressed in future research. First is the cross-sectional nature of our data, which limited the ability to make causal inferences. Future research should attempt to replicate these findings using longitudinal or momentary research. Next, our sample was not restricted to individuals with clinically significant ADHD symptoms or a validated diagnosis. Instead, we assessed ADHD symptoms continuously and through self-report only. This has the benefit of including students with sub-threshold symptoms of ADHD who often still experience impairment due to their symptoms, but future research should also examine these pathways in clinical samples to fully understand the link between ADHD diagnosis and alcohol use outcomes. Additionally, given that inattention can be a symptom of depression and anxiety, and that co-occurrence of ADHD and depressive and anxiety disorders is relatively common (D’Agati et al., 2019; Sobanski et al., 2007), some instances of self-reported inattention may be reflective of individuals with symptoms of other psychopathologies rather than ADHD. We unfortunately did not collect data on depression or anxiety, and thus are unable to account for this possibility statistically. Future research should examine whether the present findings of indirect pathways from inattention symptoms to alcohol use and related consequences through drinking motives are replicated when symptoms of depression and anxiety are included in the model. Finally, one must use caution when generalizing these findings to non-college students or racially diverse samples, as the current sample was largely comprised of White college students.
Despite these limitations, this study extends previous literature on ADHD symptoms and alcohol use and related problems, bolstering the limited work examining the role of drinking motives in this association. Particularly, results indicate that students with higher levels of inattentive ADHD symptoms may be uniquely at-risk for problematic alcohol use when drinking to cope with depression and for enhancement purposes. Thus, the development of targeted interventions aimed at supporting those with inattentive ADHD symptoms who drink to cope with depression or for enhancement reasons may be particularly important. Recent research supports the use of mindfulness-based interventions (MBI) in adults with ADHD, citing improvements to ADHD symptoms and negative affect (Poissant et al., 2020). College students experiencing symptoms of inattention and depression, who may be motivated to use alcohol to cope with their symptoms, may particularly benefit from MBI. Further, the implementation of alcohol-related harm reduction interventions may be useful for this population, particularly for students high in inattention who are motivated to drink for enhancement purposes. For example, use of protective behavioral strategies (PBS), which conveys protection against higher levels of alcohol-related consequences among students high in ADHD symptoms (Looby et al., 2021), may provide a means by which students can obtain some enhancement benefit from alcohol use, while minimizing the likelihood of negative consequences. These hypotheses should be tested in future research studies.
Supplemental Material
Supplemental Material - Drinking Motives Mediate the Relation between Attention-Deficit/Hyperactivity Disorder Symptoms and Alcohol-Related Problems among College Students
Supplemental Material for Drinking Motives Mediate the Relation between Attention-Deficit/Hyperactivity Disorder Symptoms and Alcohol-Related Problems among College Students by Caitlin A. Falco, Lauren Zimmerman, John M. Vasko, Michael C. Meinzer, Cynthia M. Hartung, Kate Flory and Alison Looby in Emerging Adulthood
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Transparency and Openness Statement
Analysis code and materials used in this manuscript/study are not openly available but can be requested from the corresponding author. The raw data contained in this manuscript are not openly available due to privacy restrictions set forth by institutional review boards but can be requested by contacting the corresponding author No aspects of the study were pre-registered.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.