
Abstract
Suicidal thoughts and behaviors are complex phenomenon and their relationship to trait impulsivity remains unclear. Although suicidal thoughts and behaviors are common among emerging adults, the availability and quality of data is scarce in countries like Kenya, due to stigmatization and illegality of suicidal behaviors. This research sought to determine the prevalence of suicidal ideation and suicide attempt in emerging adults in Kenya and examine the role of trait impulsivity. Data from 297 undergraduate students were collected using a sociodemographic questionnaire and the Barratt’s Impulsiveness Scale (BIS-11). Results showed that 15.8% (n = 47) of students reported suicidal ideation only while 8.4% (n = 25) reported suicide attempt. Significant gender differences were observed with females more likely than males to report suicidal ideation and suicide attempts. Higher attentional impulsivity was observed in those with suicidal ideation and attempted suicide than those with no suicidality. These findings help highlight the magnitude of suicidality in Kenya.
Keywords
Introduction
Emerging adulthood is a unique developmental age, between 18 and 25 years, that is characterized by identity exploration before committing to lifelong careers and relationships (Arnett, 2013) as the continually developing brain strengthens its cognitive and emotional functions in order to achieve, among other things, better impulse control (Hochberg & Konner, 2020). Evidence shows that most people adapt successfully to the challenges of emerging adulthood (Arnett, 2007) but some individuals experience serious mental health problems including suicidal thoughts and related behaviors (Beadnell et al., 2016; Crispim et al., 2021; Lisznyai et al., 2014). Initial studies from Western countries had indicated that emerging adulthood was only present in highly industrialized countries with expectations that emerging adulthood would become more obvious worldwide due to increased globalization of the world economy (Arnett, 2000). There has since been calls for studies that evaluate mental health declines and factors contributing to the escalation in risky behaviors, among emerging adults from different cultures and ethnicities, in order to guide prevention (Schwartz & Petrova, 2019).
Suicidal ideations and suicide attempts are prevalent in emerging adulthood (Crispim et al., 2021; Demenech et al., 2021; Sheldon et al., 2021; WHO 2021a). Suicidal ideation is defined as thoughts about wanting to die or killing oneself that is not accompanied by preparatory behavior (O’Connor et al., 2013). Suicide attempt on the other hand is a nonfatal, self-directed, potentially injurious behavior with an intent to die as a result of the behavior (O’Connor et al., 2013). A previous suicide attempt is a significant risk-factor for suicide mortality with the ratio of suicide attempts to death by suicide among people under 25 years being as high as 100 – 200:1 (WHO 2002; 2021b).
Around the world, individual and comparative studies focused on emerging adults at the university have reported prevalence rates for suicidal ideation at between 9 and 32% (Asfaw et al., 2020; Lew et al., 2020; Pereira & Cardoso, 2015; Mamun et al., 2020) while the prevalence rates for attempted suicide have been reported at between 4% and 10% (Donath et al., 2019; Mortier et al., 2018; dos Santos et al., 2017; Owusu-Ansah, 2020). Data on suicidality among emerging adults in Kenyan universities tends to focus on risk factors for suicidal thoughts and behaviors (Ndegwa et al., 2017; Wanyoike, 2015) without evaluation for the prevalence of suicidal thoughts and behaviors necessitating the need for additional research.
Among university student samples, suicidal thoughts and behaviors differ by age and gender. Suicidal ideation is more common in younger students with first year students being more likely to report suicidal ideation compared to students in later years (Dendup et al., 2020). Furthermore, women are noted to report suicidal ideation more often than men (Abdu et al., 2020; Dendup et al., 2020; Lew et al., 2020) although men are more likely to die from suicide attempts compared to women (Nock et al., 2008; WHO 2002). Several socio-behavioral factors appear to predispose emerging adults at the university to suicidal thoughts and behaviors. These include being single, struggling with financial hardships, academic demands and relationship challenges (Sivertsen et al., 2019; Kabugi, 2019; Muertigue & Naiker, 2018). Suicidal thinking and behaviors are also higher among individuals without structured religious practices, those with history of suicide attempts in the family or among friends and among those with alcohol or drug misuse (Desalegn et al., 2020; Kabugi, 2019; dos Santos et al., 2017). Finally, while some studies show that being in the university environment is protective against suicide mortality (Schwartz, 2011), others have shown that students currently enrolled in the university have higher risk for suicide mortality compared to students who have graduated (Lageborn et al., 2017). This may be partially explained by reduced likelihood by enrolled students to seek for help from their own university’s mental health services for fear of stigmatization (Kearn et al., 2015).
Many factors affect suicidal thoughts and behaviors, including trait impulsivity, which is defined as a predisposition towards rapid, unplanned reactions to internal and external stimuli with diminished regard to negative consequences (Chamberlain & Sahakian, 2007). Trait impulsivity indicates a person’s characteristic way of planning or not planning for activities and is assessed using self-reported scales (Glicksohn et al., 2016). Impulsiveness however is multi-faceted and the 11th edition of the Barratt’s Impulsiveness Scale (BIS-11) reflects three dimensions of trait impulsivity; attentional impulsivity which is lack of concentration necessary to complete mental tasks, motor impulsivity which describes one’s propensity to act in the spur of the moment and non-planning impulsivity which is a lack of consideration for future consequences (Patton et al., 1995).
The BIS-11 has been used in numerous studies to examine the relationship between impulsivity and suicide thoughts and behaviors with findings of a positive association between impulsivity and suicidal ideation (Huang et al., 2017). However, there are inconsistencies across studies with regard to which facets of impulsivity are most relevant to suicide risk. Many studies associate suicidal ideation among college students with higher motor and non-planning impulsiveness (Loftis et al., 2019; Wang et al., 2014) while a recent study reported an association with attentional impulsivity only (Daneshmend et al., 2022). For suicide attempts, some studies have shown that people who attempt suicide have higher levels of trait impulsivity (Hameed et al., 2017) while others differ. For example, a review of hospitalized 15 – 25 year-olds noted that suicide attempts were associated with lower scores on the motor and non-planning impulsivity scores (Gade et al., 2018). Meta-analytic studies on the other hand suggest that the relationship between trait impulsivity and suicidal thoughts and behaviors is small and may be clinically insignificant (Franklin et al., 2016; Anestis et al., 2014). Around the world however, the availability and quality of data on suicidal thoughts and behaviors as well as corresponding factors such as impulsivity remains poor due to stigmatization and the fact that suicidal behaviors remains illegal in some countries (WHO 2021a).
Kenya is one of the 20 countries in the world where suicidal behaviors are still considered a crime and attempted suicide is punishable by incarceration or a fine or both (Lew et al., 2022). Regardless, suicide mortality rates have been on an upward trajectory in Kenya from 2016 and by 2019 the national suicide prevalence rate was 6.1 per 100,000 including a three times higher prevalence among males than females at 9.1 per 100,000 (World Bank Group, 2020). In spite of this, mental health professionals tend to focus on prevalence data only for suicide mortality and this is extrapolated posthumously (Ongeri et al., 2022). Data is also sourced from law enforcement officers who revealed that in 2021, approximately 500 deaths by suicide were reported nationwide over a 3-month period and this figure superseded the number of reported suicides in the whole of 2020 (The Guardian, 2021). There is concerted effort to mitigate this rise in suicide cases by the Kenyan government (Ministry of Health, 2022) however the focus has remained on suicide mortality and therefore may not be reflective of the magnitude of suicidal thoughts and behaviors in Kenya. This study thus sought to answer the following research questions. 1. What is the prevalence of suicidal thoughts and behaviors among emerging adults at a Kenyan university? 2. What are the levels of trait impulsivity in emerging adults at the university? 3. Is there an association between total and subscales of trait impulsivity and suicidal thoughts and behaviors?
Material and Methods
Participants
This cross-sectional study was conducted in a small private university in Kenya with 3,951 registered undergraduate students at the time of the study with the majority of students being female (n = 2,431). The main characteristics targeted were male and female undergraduate students aged between 18 and 25 years. Yamane formula was used to calculate the sample size, as the sampling frame was available, as follows
n = Sample size
N = Population Size
e = Level of precision (95% confidence interval)
N = 3951 (number of registered undergraduate students in the semester).
Subsequently, 400 questionnaires were distributed with 329 questionnaires returned representing an 82.25% response rate. Of these, 32 questionnaires were not analyzed as eight lacked most of the sociodemographic and risk-taking data required, 22 did not respond to the BIS-11 while two more participants were excluded due to atypical response patterns on the BIS-11.
Assessments
Barratt’s Impulsiveness Scale (BIS-11)
The BIS-11 is a widely used, well-validated, self-report questionnaire that is considered to be a reliable indicator of impulsiveness in research and clinical settings for individuals between 17 – 45 years (Stanford et al., 2009). It consists of 30-items reflecting the frequency of common impulsive (e.g. “I do things without thinking”) or non-impulsive (“I am self-controlled”) behavioral traits which are rated on a scale from 1 = Rare/Never to 4 = Almost Always/Always (Mathias et al., 2018). Responses from all the 30 items are summed and total scores can range from 30 to 120 points. BIS-11 total scores of 52–71 are considered to be within normal limits for impulsiveness thus participants with scores of 72 and above are considered highly impulsive (Stanford et al., 2009) while those with scores lower than 52 are considered extremely controlled or not honest in the completion of the questionnaire (Helfritz et al., 2006). The BIS-11 has demonstrated acceptable validity and reliability among college students (Patton et al., 1995). While originally developed and normed in English, the BIS-11 has since been translated into 11 other languages with Cronbach α scores of 0.71–0.83 indicating its reliability for use in diverse cultures (Stanford et al., 2009) and specifically among non-Western college students (Tsatali et al., 2021; Ziada et al., 2020). The Cronbach alpha level for the current study was 0.73 for the BIS-Total while the subscales of attentional, motor and non-planning impulsivity had alpha scores of 0.59, 0.52 and 0.61 respectively. Given the low reliability of these subscales, analyses that include them are considered exploratory for the purposes of trying to provide some initial data about trait impulsivity and suicidal thoughts and behaviors in Kenya.
Socio-demographic Questionnaire
A newly constructed questionnaire was used to collect socio-demographic data including age, gender and year of study. Suicidal thoughts and behaviors within the preceding year were specifically assessed using the following questions; (1). In the past 1 year, have you ever had any suicidal thoughts? (Yes/No) (2). In the past 1 year, have you ever attempted suicide? (Yes/No)
Procedure
The study was approved by an accredited Ethics and Research Committee and the national research regulatory authority. Permission to collect data was also sought from the relevant university administration. A day of the week was picked randomly, and permission gained from respective lecturers as needed to distribute the study questionnaires within lecture rooms. A written consent form was attached to the questionnaires and the researcher followed this up with a verbal explanation of the same. Students were advised that participation was voluntary and asked not to put any names or identifying information on the questionnaires which were collected as soon as they were completed.
Statistical Analyses
Descriptive and analytical statistics of the data were conducted in IBM SPSS (version 28.0). Missing data on the BIS-11 for 18 students was imputed using group-level means. The number of entries imputed for missing data for BIS-11 variables ranged between 1 (0.4%) and 14 (4.7%). The Cronbach alpha scores before and after data imputation using means for total and subscales of impulsivity were not significantly altered. For example, the alpha value for BIS-Total was 0.733 before imputation of missing data (279 students) and 0.731 after imputation of missing data (297 students). To examine the relationship between sociodemographic characteristics (gender, age, level of education, marital status, residence) and suicidal thoughts and behaviors, Chi-square tests of independence were utilized. Multivariate analysis of variance was then conducted to evaluate for differences between suicide groups (dependent variable) and the total as well as subscales trait impulsivity scores (independent variable) while adjusting for the effect of significant sociodemographic characteristics (covariate). Finally, post hoc analyses were conducted using Tukey honestly significant difference (HSD) for the independent variable that showed significant association with the suicidality groups (no suicidality, suicidal ideation and suicide attempt) during the multivariate analysis.
Results
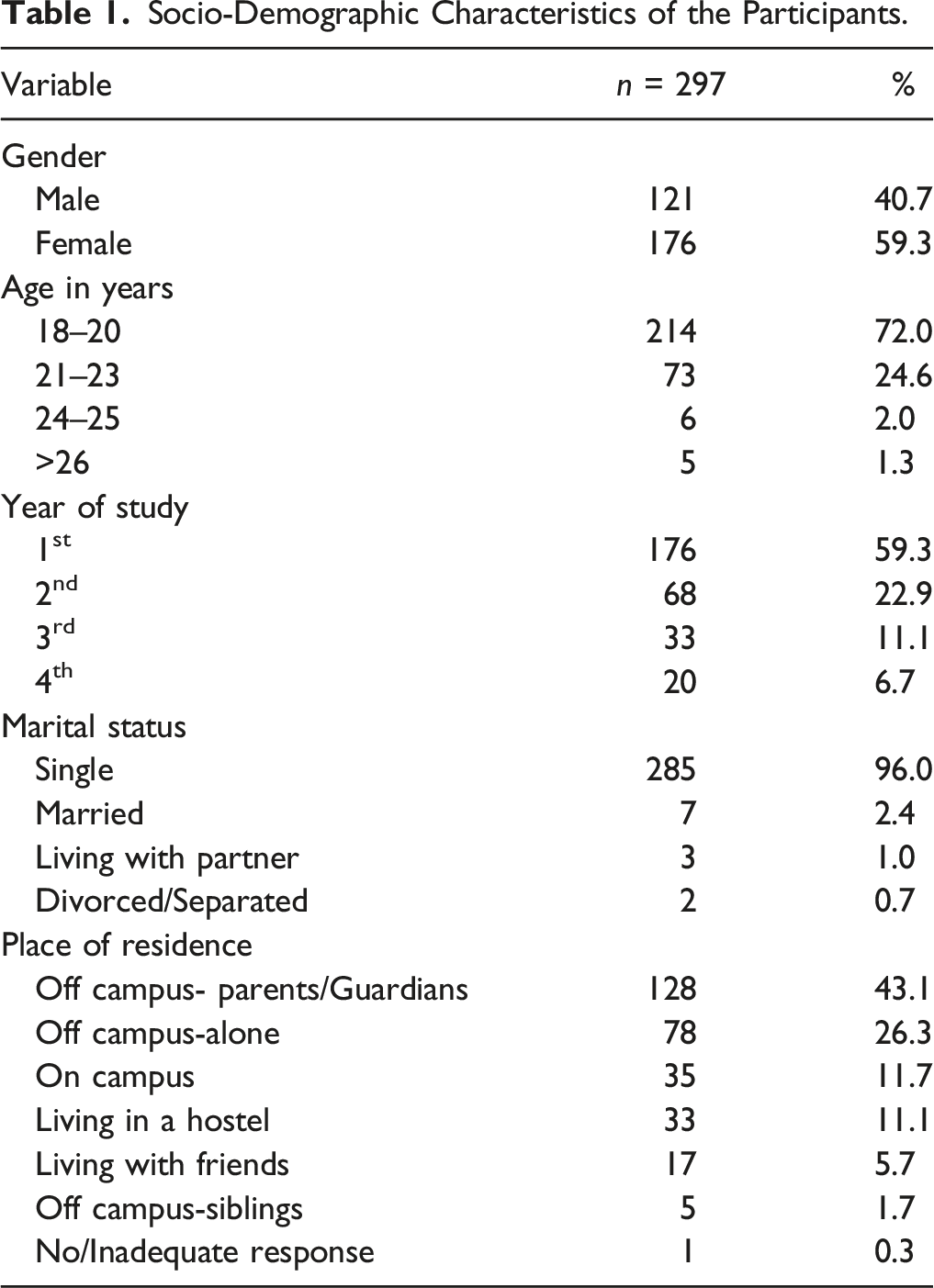
Socio-Demographic Characteristics of the Participants.
Prevalence of Suicidal Thoughts and Behaviors of Study Participants.
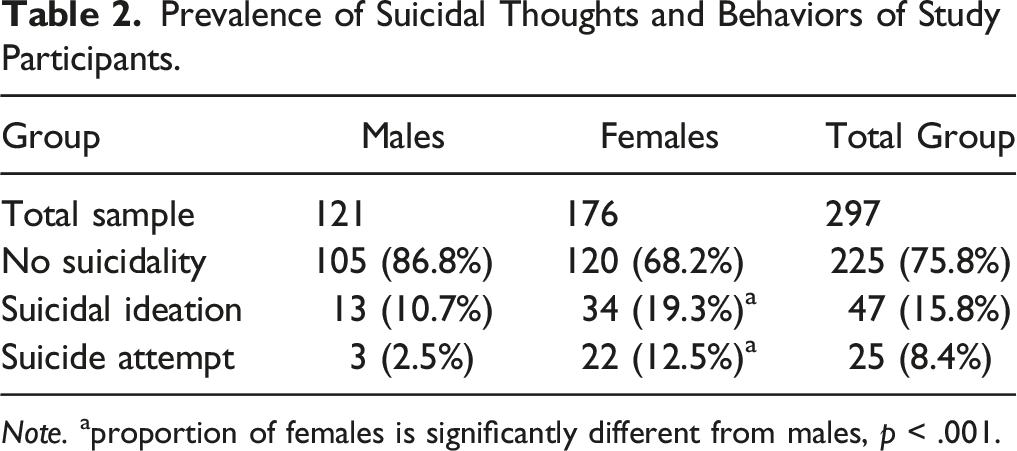
Note. aproportion of females is significantly different from males, p < .001.
Trait Impulsivity Levels among Participants.

Note. Impulsivity scores using the BIS-11; Low impulsivity = 51 and below, Normal impulsivity = 52 – 71, High impulsivity = 72 and above.
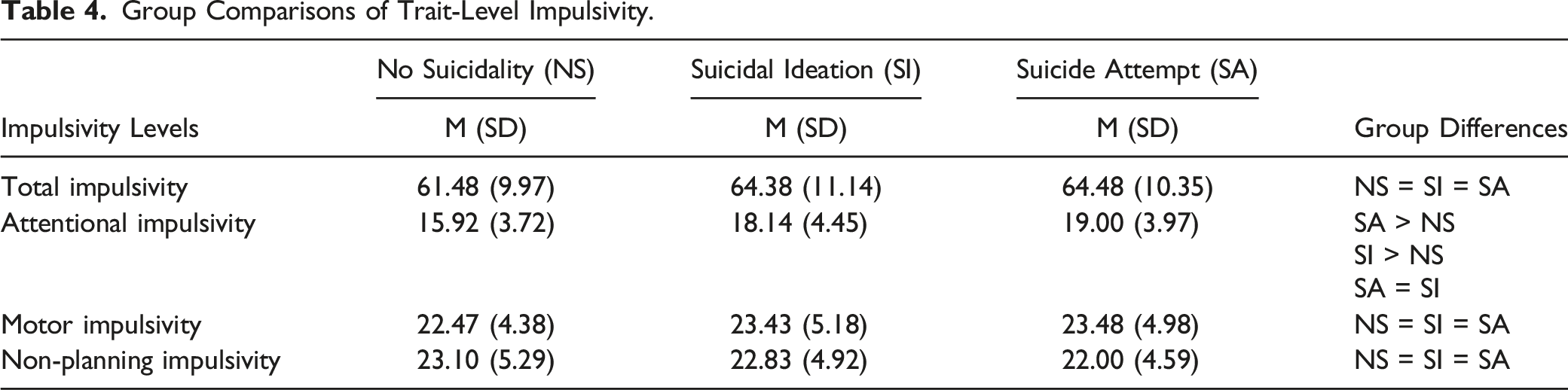
Group Comparisons of Trait-Level Impulsivity.
Discussion
The findings of the current study are some of the first investigating prevalence of suicidal thoughts and behaviors among emerging adults in Kenya and show a prevalence of suicidal ideation of 15.8% and a prevalence of suicide attempt of 8.4% with females being more likely than males to report both suicidal thoughts and behaviors. For impulsivity, only the attentional impulsivity subscale was significantly related to suicidal thoughts and behaviors with higher levels in those with suicide attempt than those with suicidal ideation only or no suicidality.
The prevalence of suicidal ideation and attempt as noted in this study are reflective of global findings (Lew et al., 2020; Mortier et al., 2018) especially higher rates found among females than males (Abdu et al., 2020; Dendup et al., 2020; Pereira & Cardoso, 2015). The similarity between data from a variety of different countries suggests that the gender differences in suicidal thoughts and behaviors among emerging adults in the university is not culturally dependent. Female suicidality has been commonly associated with negative life experiences or daily life stressors that result in lower satisfaction with life (Lu et al., 2020; Vijayakumar, 2015). In both Western and non-Western colleges, female students have reported higher levels of stress which they mitigate using emotion-focused coping skills like venting however these provide temporary relief but do not lead to a resolution of stressors (Graves et al., 2021; Misigo, 2015; Oketch-Oboth & Okunya, 2018). This may eventually result in some female students considering suicide a means to permanently resolve problems (Wu et al., 2021).
Although suicidal ideation and attempt among emerging adults in colleges are more prevalent in females than males, serious suicide attempts (SSA) which are defined as suicidal behaviors with clear intent to die irrespective of the method employed, are more common in males (Freeman et al., 2017). Male college students are less likely to report a previous suicidal attempt or tell someone about their suicidal ideations (Becker et al., 2018) potentially making them more likely to die in the first suicide attempt. This lower likelihood by male college students to disclose suicidal thoughts and behaviors may partially explain the findings of this current study where more females (n = 56) reported suicidal ideation and suicide attempt than males (n = 16). Additionally, reluctance to disclose suicidal thoughts and behaviors by males may be driven by cultural factors such as internalization of masculinity norms which also makes African men more susceptible to mental health problems (Ezeugwu & Ojedokun, 2020). With higher national prevalence of suicide mortality among men than women in Kenya (a ratio of 3:1), there is need for avenues that encourage male students to disclose suicidal ideations.
In the current study, total, motor and non-planning impulsivity were not associated with suicidal ideation or suicide attempt. This differs from earlier studies that report higher total, motor and non-planning impulsivity among college students with suicidal thoughts and behaviors (Hameed et al., 2017; Loftis et al., 2019; Wang et al., 2014) but appears to agree with meta-analytic studies that suggest that trait impulsivity is not a critical risk factor for suicide mortality (Anestis et al., 2014; Franklin et al., 2016). However, attentional impulsivity was related to suicidal ideation and suicide attempt which mirrors similar findings in a Canadian study (Daneshmend et al., 2022), suggesting that our finding may not be culturally specific.
It is possible that attentional impulsivity may be more related to depression than suicide risk and as noted by Thompson & Ong (2018), dysfunction in executive cognitive processes like attention in populations at high risk for suicide may be due to depression and not trait impulsivity per se. Depressed patients who are not on treatment have been shown to perform poorer than healthy individuals in activities requiring selective attention which is the ability to concentrate on a specific task while ignoring other irrelevant distractions (Keller et al., 2019). Bearing this in mind, our study finding may suggest that evaluations for trait impulsivity and suicidality, in research and clinical settings, should go hand in hand with assessment for depression. On the other hand, it is also possible that persons who die by suicide, rather than those with suicidal thoughts or suicide attempts, have greater impulsivity levels. This may point to a need for longitudinal studies in Kenya focused on trait impulsivity as a risk factor for suicide mortality.
Our current results are both compatible (e.g. Daneshmend et al., 2022) and incompatible (e.g. Huang et al., 2017; Loftis et al., 2019) with the broader literature regarding trait impulsivity and suicidal thoughts and behaviors. The lack of significant relationship observed between suicidal ideation and suicide attempt, and total as well as motor and non-planning subscales of impulsivity may reflect a true non-significant relationship (Franklin et al., 2016) or it could be due to low reliability of the items, which may reflect poor cultural relevance. Other non-Western studies have also observed acceptable Cronbach alpha scores for BIS-Total but have been unable to validate the original factor structure of the BIS-11 with this being attributed to challenges in cultural and linguistic interpretations of items (Lau et al., 2022; Malloy-Diniz et al., 2015). The poor reliability across BIS-11 subscales in the current sample, along with other non-Western samples, reiterates a need for the establishment of cross-cultural normative data for the BIS-11 in specific ages, genders and populations.
Recommendations
The findings of this study are significant to policy makers at the university, community and national level as they highlight a need for the evaluation of prevalence rates of suicidal ideation and suicide attempts across different populations. It also calls attention to a need for reduced singular focus on suicide mortality in order to understand the magnitude of suicidal thoughts and behaviors in Kenya and offer timely and effective suicide prevention strategies. The findings are also important to practitioners working with emerging adults to encourage more forthright inquiries about suicidal ideations, especially among male students who are less likely to volunteer information related to suicidality. In addition, universities may want to be more intentional and proactive in publicizing and enhancing mental health programs. They may consider the use of self-administered, normed, short screens for mental health assessment within classrooms where students will also be taught how to evaluate their scores and resources will be offered to ask for help within or outside the campus (Lee et al., 2021).
Future studies can be geared towards identifying life stressors that contribute to suicidal thoughts and behaviors in male and female emerging adults in Kenyan universities so as to offer more timely interventions. It may also be important to assess for state impulsivity in order to establish if risk-taking behaviors like suicide attempt are a function of cognitive processes where individuals, with low or normal impulsivity, select immediate versus delayed solutions to problems when they find themselves in highly stressful conditions.
Limitations
Due to COVID-19 restrictions at the time of the study, there was limited access to some students. Although the intention was to get equal representation of the four academic levels in the sample, only first year students had in-person classes while all other levels had in-person classes only for selected courses. A second limitation was that this study utilized two specific questions targeting suicidal thoughts and behaviors rather than established questionnaires. This was done to control the time for the completion of the questionnaires to enhance maximum participation. Despite this precaution, some students did not complete the BIS-11 therefore in the future, researchers may consider using the brief version of the BIS. A third limitation was that we did not assess for other risk-factors that could predispose emerging adults to suicidality and these may have included among other things presence of depression and/or history of childhood trauma which may have explained the observed relationship between attentional impulsivity and suicidal thoughts and behaviors in this sample. Finally, this study is limited as it only focused on trait impulsivity without assessing for state impulsivity which may be more relevant to understanding at-risk coping during moments of distress. The Theory of Reasoned Action postulates that a person’s behavior is determined by their attitude towards that behavior and their intentions for the behavior (Al-Suqri & Al-Kharusi, 2015) thus future studies could seek to evaluate the attitudes and beliefs that emerging adults in Kenya hold towards suicidal thoughts and behaviors and how those relate to the prevalence of, and willingness to disclose suicidality.
Conclusion
The findings of this study highlight that suicidal ideation and suicide attempts are prevalent among emerging adults in the university in Kenya especially among female students compared to males. While attentional impulsivity was related to both suicidal ideation and suicide attempt, further studies are needed to gain confidence that this was a meaningful and generalizable effect. Collectively, this provides evidence that there is a need for institutional, community and national mental health policies and programs geared towards gender-specific, suicide prevention programs.
Supplemental Material
Supplemental Material - The Role of Trait Impulsivity on Suicidality in the Emerging Adult in Kenya
Supplemental Material for The Role of Trait Impulsivity on Suicidality in the Emerging Adult in Kenya by Caroline Mwendwa-Karinge, Douglas Matthews, Wilfridah Mucherah and Jennifer MuehlenKamp in Emerging Adulthood
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the The Mayo Healthcare – Eau Claire Research Innovation Council Grants (DBM; JJM).
Transparency and Openess Statement
The raw data, analysis code and materials used in this study are not openly available but are available upon request to the corresponding author. The data collection and analysis plans were preregistered with my university as part of my PhD dissertation and all deviations from the preregistered plans are clearly indicated in the manuscript with justification for the same.
Supplementary Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.