
Abstract
Attachment representations are increasingly operationalized as secure base script knowledge—one’s level of awareness of the temporal-causal schema that summarizes basic features of seeking and receiving effective support from caregivers when in distress. A method was recently developed to assess secure base script knowledge during the Adult Attachment Interview (AAIsbs), though its predictive validity for mental health outcomes is largely unknown. A series of pre-registered analyses, leveraging two large, longitudinal cohorts to assess the associations between AAIsbs and depression in emerging adults revealed that higher AAIsbs at age 18 years in the normative-risk sample, but not in a higher-risk cohort, predicted fewer depressive symptoms at age 30 years. In general, these associations were robust to concurrent depressive symptoms, sociodemographic and cognitive functioning covariates, and other traditional attachment representation measures. Findings support the importance of considering schematic attachment representations in developing interventions to improve young adults’ well-being.
Introduction
A core premise of attachment theory is that the quality of early care shapes the development and consolidation of subsequently constructed mental representations of attachment, which, in turn, influence mental health (Bowlby, 1973; Sroufe et al., 2005). Based on this premise, this set of pre-registered analyses aims to build on a programmatic line of research (Dagan, Buisman, et al., 2021; Dagan et al., 2018) to investigate the predictive significance of attachment representations in general, and scripted attachment representations (i.e., secure base script knowledge; Waters & Waters, 2006) more specifically, for depressive symptoms in adulthood.
According to attachment theory, through repeated interactions with their parents or other primary caregivers, children form attachment relationships (Bowlby, 1969). When parents are available and responsive in times of need, children are thought to experience an ongoing sense of safety from physical or perceived proximity to caregivers when facing distress, and thus likely to develop secure attachment relationships (Ainsworth et al., 1978; Marvin & Britner, 2008). Alternatively, when parents respond insensitively to children’s distress, children are likely to develop insecure attachment relationships. Bowlby (1973, 1980) hypothesized that such early insecure attachment relationships may increase individuals’ vulnerability to depression across the lifespan (for meta-analytic findings on the association between attachment relationships and depression symptoms in childhood, adolescence, and adulthood, see Dagan et al., 2018; Spruit et al., 2020). Specifically, he proposed that increased vulnerability to depression may be a result of a set of expectations that one’s efforts to seek help or support from close others are futile. By and large, this set of expectations in adulthood has been assessed by developmental psychologists via the Adult Attachment Interview (AAI; George et al., 1985).
The AAI is a 20-question, semi-structured interview that asks individuals about their early life experiences with their caregivers and how these might have influenced who they are today. Traditionally, attachment classifications coded via the AAI have heavily relied on coding adults’ coherence of discourse (AAIcoh). That is, coders evaluate the speaker’s manner of speech, rather than its content, to assess the quality and consistency of their autobiographical memories regarding their childhood experiences. Higher AAIcoh is observed in interviews in which speakers convey their childhood experiences with caregivers in an internally consistent but not emotionally overwrought manner (e.g., Roisman, 2009), and which are classified as secure/autonomous (Main & Goldwyn, 1998). In contrast, lower AAIcoh scores are coded in interviews classified as one of two insecure attachment patterns. Repeated indices of caregivers’ idealization and/or insistence on a lack of memory of childhood events are classified as insecure-dismissing attachment. An interview is classified as insecure-preoccupied, in contrast, when the discourse is rich with expressions of anger regarding negative experiences with one or multiple caregivers, and/or difficulty in focusing on such experiences (i.e., passivity).
AAIs are known to be used by attachment-informed mental health professionals since they entail clinical applications (Steele & Steele, 2008). Indeed, empirical evidence supports the association between attachment representations coded via the AAI and depression. Specifically, a meta-analysis of over 4000 adolescents and adults reported that individuals who are classified as securely attached via the AAI were likely to report fewer depression symptoms compared to their insecure counterparts (Dagan et al., 2018). In addition, insecurely attached individuals are overrepresented in samples of depressed individuals compared to normative-risk samples (Bakermans-Kranenburg & van IJzendoorn, 2009). Indeed, However, a detailed cognitive schema or script that biases insecurely attached individuals to experience more depression symptoms compared to their securely attached counterparts has been notably missing. A cognitive model is thus needed to delineate why insecure attachment representations are predictive of individual differences in depression, and which lays itself better to testable observations than traditional attachment representation measures.
The Potential Contribution of Scripted Attachment Representations to Understanding Vulnerability to Depression
Since the emergence of the cognitive framework to explain depression (Beck, 1967), cognitive schemas—or (negative) representations of the self, the world, and the future—have been understood as underlying depression. Individuals with negative cognitive schemas, such as “I am worthless”, “the world is a scary place”, and “the future will never get better,” tend to process information in congruency with these schemas, which gives rise to, and perpetuate their depression symptoms. Indeed, interventions aimed at modifying such “maladaptive” cognitive schemas have been successfully utilized across the lifespan (e.g., Cognitive Behavioral Therapy; Cuijpers et al., 2023), suggesting the causal role of these schemes in the development and maintenance of depression.
Attachment theory, too, has emphasized the centrality of cognitive biases in individual differences regarding information processing (Dykas & Cassidy, 2011). These cognitive biases (often referred to as “internal working models”; Bretherton & Munholland, 2008) are formed and consolidated through repeated interactions with one’s caregivers, leading to representations of them that, with time, become generalized to other close relationships across the lifespan. In this context, insecure attachment representations can be viewed as “maladaptive cognitive schemas.” That is, insecurely attached individuals tend to view themselves as more vulnerable to rejection and, in expecting such rejection in the future from close others, they are more likely to defend themselves via excessively seeking or rejecting closeness with others, leading to psychopathology (Bosmans et al., 2010; Shaver & Mikulincer, 2007). Despite the clear overlap between the cognitive framework of depression and attachment theory, relatively little effort has been devoted to articulating a detailed cognitive schema that evolved from early attachment experiences and that increases vulnerability to depression (but see Bosmans, 2016; Morley & Moarn, 2011).
Recent development and validation of cognitive assessments of attachment representations allow for a more direct approach to testing the link between attachment-relevant cognitive structures and later depression. To increase the coherence and specificity of the cognitive “building blocks” of attachment representations, Waters and Waters (2006) proposed that individuals develop and consolidate schemas, or script-like attachment representations, which they refer to as secure base script knowledge. Secure base script knowledge reflects a cognitive schema entailing the typical sequence of events in which a caregiver provides support and resolves distress (Waters & Roisman, 2019; Waters & Waters, 2006). These typical events include seeking comfort from a caregiver at times of distress, being effectively soothed by the caregiver, and returning to exploration. A scripted attachment representation that lacks the expectation that caregivers’ emotional support is available at times of need decreases the likelihood of constructing adequate access to, and elaborated knowledge of the secure base script.
Limited access to, and knowledge of the secure base script reflects a set of expectations that soliciting efforts from close others in times of need would be futile or ineffective. As such, limited access to, and knowledge of the secure base script may lead to a reappraisal of stressful events as disproportional to one’s ability to cope with them (Rueger et al., 2016; Stice et al., 2004). Given that adolescence is a period in which vulnerability to depression increases dramatically (Auerbach et al., 2014; Merikangas et al., 2010), and that depression in adolescence persists into emerging adulthood (Copeland et al., 2009; Costello et al., 2008; Waszczuk et al., 2016), secure base script knowledge assessed in adolescence may be a significant predictor of depression symptoms in adulthood.
Individual differences in secure base script knowledge have been assessed using two methods: the Attachment Script Assessment (ASA; Dykas et al., 2006; Waters & Waters, 2006) and a secure base script coding scheme developed for use with the Adult Attachment Interview (AAIsbs; Waters & Facompré, 2021; Waters et al., 2013; Waters et al., 2017). Only the ASA has thus far been assessed regarding its predictive significance for depressive symptoms in adulthood, in a sub-sample (n = 584) of the NICHD Study of Early Child Care and Youth Development (SECCYD; NICHD Early Child Care Research Network, 2005). In that study (Dagan, Buisman, et al., 2021), ASAs at age 18 and depressive symptoms at age 26 were negatively correlated, though the effect size was small in magnitude (r = −0.13, p < .01). Relatedly, a meta-analysis (Dagan et al., 2018) reported that individuals classified as securely attached via the AAI, which relies heavily on the coherence of discourse during the interview, reported more depressive symptoms than did individuals classified as insecure, albeit also with a small effect size (r = −0.10). These results further support the notion that the schemas individuals have developed regarding their past relationships with their primary caregivers are statistically associated with their depression symptoms in adulthood.
To date, the power of AAIsbs in predicting depression in adulthood has yet to be examined. Empirically, AAIsbs was shown to predict romantic relationship quality during adulthood, including caregiving and care-seeking behaviors with romantic partners under interpersonal distress (Dagan et al., 2024; Waters et al., 2013, 2018). Given that the quality of romantic relationships reflects a variation in chronic experiences of interpersonal stress, itself a strong predictor of depressive symptoms in adulthood (Hames et al., 2013; Sheets & Craighead, 2014), AAIsbs is well suited to predict vulnerability to depressive symptoms in adulthood.
The Present Study
The pre-registered analyses presented here are part of a programmatic line of research designed to investigate the antecedents and sequelae of AAIsbs in the SECCYD (see Dagan et al., 2024; Nivison et al., 2023). The current pre-registered study has three main aims. The first aim (Aim 1) was to examine the strength (Aim 1a) of the longitudinal associations between AAIsbs in late adolescence and depressive symptoms in adulthood in both a normative- and a higher-risk sample, above and beyond concurrent depressive symptoms (Aim 1b). Given prior evidence, we predicted that higher AAIsbs at age 18 (in the SECCYD), and ages 19 and 26 (in the higher-risk Minnesota Longitudinal Study of Risk and Adaptation [MLSRA] sample) would be associated with less depressive symptoms in adulthood, and that these associations would be robust to concurrent depressive symptoms (Aim 1b). The second aim (Aim 2) was to compare the associations between AAIsbs and depressive symptoms in adulthood relative to the associations between the ASA and the traditional coding scales of the AAI and depressive symptoms in adulthood. Specifically, in exploratory analyses, we examined whether AAIsbs predicted depressive symptoms more strongly (Aim 2a) and incrementally (Aim 2b) compared to the traditional attachment representation measures. Consistent with current programmatic research assessing the antecedents and sequalae of AAIsbs (Dagan et al., 2024; Nivison et al., 2023), the third aim (Aim 3) of this study was to assess the sociocultural generalizability of the associations between attachment representations in late adolescence and depressive symptoms in adulthood. Given prior evidence (i.e., Nivison et al., 2023), we hypothesized that sociodemographic variables (i.e., biological sex, ethnicity, and socioeconomic status) would not moderate the expected associations between attachment representations in late adolescence and depressive symptoms in adulthood.
We added two sets of non-pre-registered analyses based on input during the review process. First, we assessed Aims 2 and 3 with respect to the AAI unresolved classification (AAIu). Specifically, we compared the predictive power of AAIsbs on depression with that of the AAIu, and assessed the sociocultural generalizability of the associations between AAIu and depression in both the SECCYD and the MLSRA. Second, we extended Aim 1 to assess the predictive power of AAIsbs for clinically significant self-reported depression (i.e., a T-score of 65 or above) over and above traditional AAI measures and the ASA in the SECCYD and the MLSRA. We also extended Aim 2 to examine whether AAIsbs predicted clinical-level self-reported depression in adulthood more strongly and incrementally compared to the traditional attachment representation measures.
Method
Participants
Bivariate Associations Among all Study Variables Within the Normative-Risk NICHD SECCYD Sample.
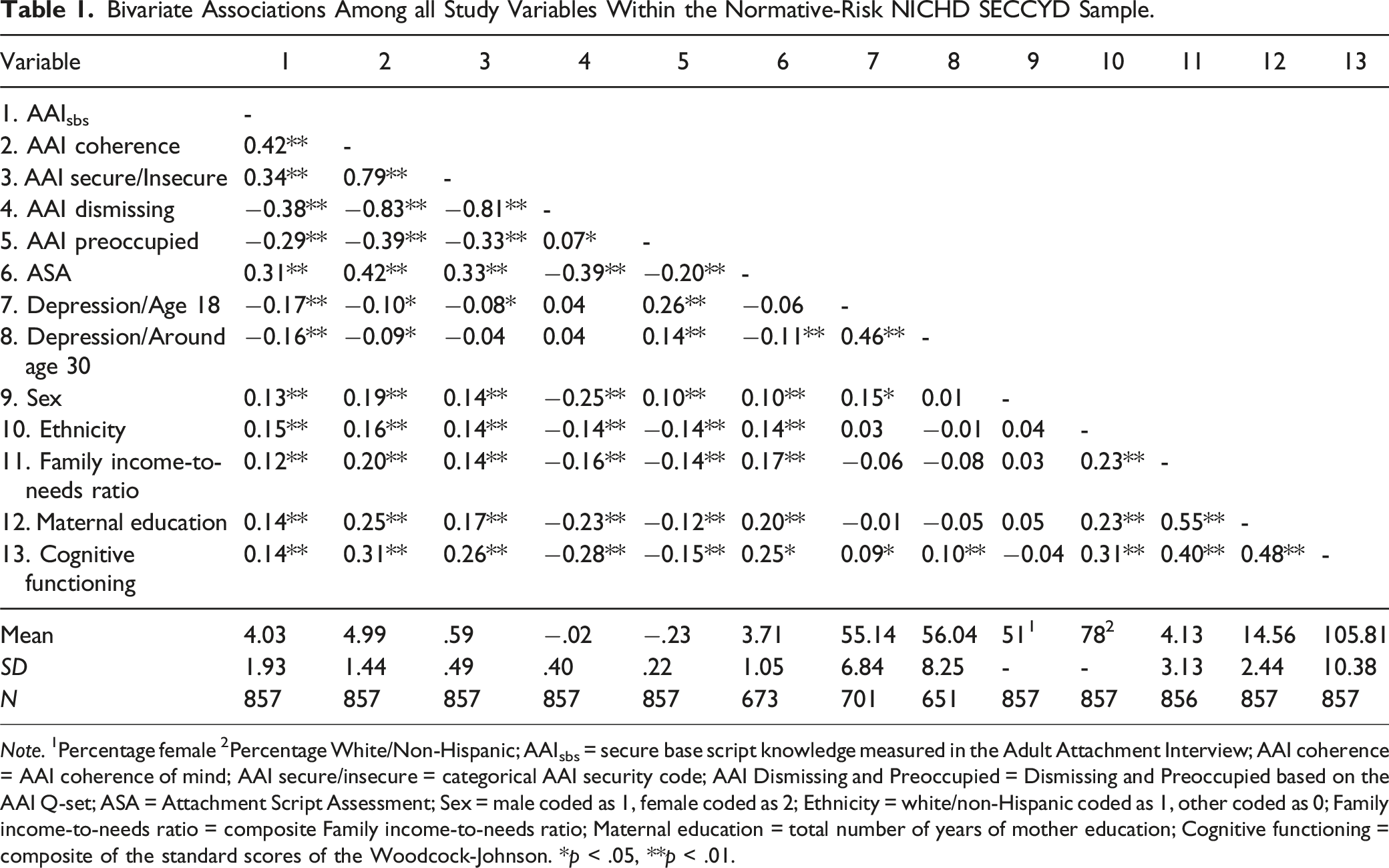
Note. 1Percentage female 2Percentage White/Non-Hispanic; AAIsbs = secure base script knowledge measured in the Adult Attachment Interview; AAI coherence = AAI coherence of mind; AAI secure/insecure = categorical AAI security code; AAI Dismissing and Preoccupied = Dismissing and Preoccupied based on the AAI Q-set; ASA = Attachment Script Assessment; Sex = male coded as 1, female coded as 2; Ethnicity = white/non-Hispanic coded as 1, other coded as 0; Family income-to-needs ratio = composite Family income-to-needs ratio; Maternal education = total number of years of mother education; Cognitive functioning = composite of the standard scores of the Woodcock-Johnson. *p < .05, **p < .01.
Bivariate Associations Among all Study Variables Within the High-Risk MLSRA Sample.
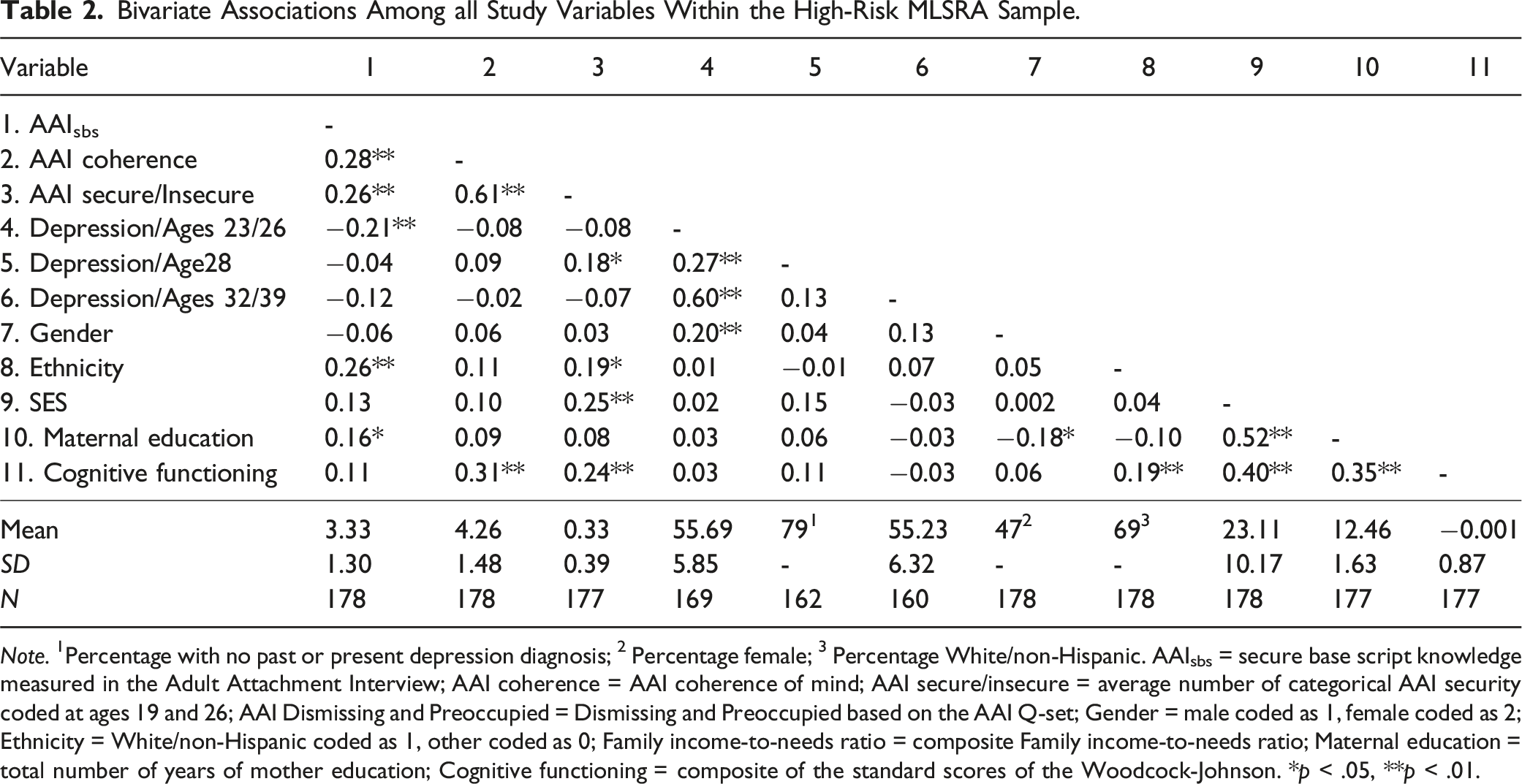
Note. 1Percentage with no past or present depression diagnosis; 2 Percentage female; 3 Percentage White/non-Hispanic. AAIsbs = secure base script knowledge measured in the Adult Attachment Interview; AAI coherence = AAI coherence of mind; AAI secure/insecure = average number of categorical AAI security coded at ages 19 and 26; AAI Dismissing and Preoccupied = Dismissing and Preoccupied based on the AAI Q-set; Gender = male coded as 1, female coded as 2; Ethnicity = White/non-Hispanic coded as 1, other coded as 0; Family income-to-needs ratio = composite Family income-to-needs ratio; Maternal education = total number of years of mother education; Cognitive functioning = composite of the standard scores of the Woodcock-Johnson. *p < .05, **p < .01.
Measures
Attachment Representations Measures
Secure Base Script Knowledge Coded in the Adult Attachment Interview (AAIsbs)
The Adult Attachment Interview (AAI; George et al., 1985) was administered at age 18 years in the SECCYD, and ages 19 and 26 in the MLSRA. The AAI is a semi-structured, 20-question protocol that requires participants to describe their early relationships with their parents and evaluate how they have influenced who they are today. AAIs were coded using a recently developed system based on the extent to which an individual’s narrative provides evidence of access to, and elaborated knowledge of, the secure base script (AAIsbs; Waters & Facompré, 2021; Waters et al., 2017). The AAIsbs coding system is rated on a 9-point scale for the extent to which the narratives produced in the interview follow, or imply, the secure base script.
SECCYD AAI transcripts were coded for this analysis by a team of two coders with one master coder coding a subset of reliability cases. Overall, the full sample (n = 857) was coded by Coders 1 [OD] and 2 [MDN] with ∼40% cases (n = 339) overlapping for reliability (ICC = 0.86). Coders 1 and 2 demonstrated high reliability with the Expert Coder (ICC = 0.93, 0.91, respectively, n = 236). For the MLSRA, all AAIs were coded for AAIsbs by two trained and reliable coders. ICCs for the 19-year and 26-year AAIs were 0.80 at both assessments, and scores were averaged across the two assessments (r = 0.55, p < .001, Cronbach’s α = 0.69).
AAI Traditional Coding
AAI transcripts were previously coded using Main and Goldwyn’s (1998) standard classification-based coding system, though none of these coders were involved in the AAIsbs coding. Specifically, AAI transcripts were categorized into one of three primary attachment classifications (secure/autonomous, dismissing, or preoccupied). In addition, a fourth category-unresolved/disorganized with respect to trauma or loss - was assigned in conjunction with one of the three other classifications. In the SECCYD, we coded the secure and unresolved classifications in a binary manner (i.e., insecure [“0”] vs. secure [“1”], and unresolved [“0”] vs. resolved [“1”]), respectively). In the MLSRA we coded the secure and unresolved classifications semi-continuously, averaging the number of times an individual was classified as secure or unresolved, respectively, across AAI assessments at ages 19 and 26). In light of factor-analytic and taxometric evidence indicating that AAI narratives vary along two primary dimensions (i.e., dismissing and preoccupied; e.g., Raby et al., 2022), we also used the AAI Q-set (Kobak, 1993) to scale participants on dismissing and preoccupied states of mind in the SECCYD (but not in the MLSRA). The AAI Q-set consists of 100 cards that describe attachment-related states of mind and inferred parental experiences. Prototypically insecure-dismissing cards include “subject persistently does not remember” and “provides only minimal responses.” Prototypically insecure-preoccupied cards include “subject is confused or overwhelmed with information about parents” and “subject is caught up with analyzing parental shortcomings”. Coders sort cards into a forced normal distribution from least to most characteristic of each individual’s AAI narrative. Sorts are then correlated with prototypic sorts that reflect theoretically relevant attachment state of mind dimensions, with each participant given two continuous scores ranging from −1 to 1 (i.e., one for prototypic dismissing and one for preoccupied). For details regarding reliability of the Main and Goldwyn’s (1998) AAI coding in the SECCYD and MLSRA, see Steele et al. (2014) and Waters et al. (2017), respectively. For details regarding reliability of AAI Q-set (Kobak, 1993) coding in the SECCYD, see Steele et al. (2014).
Attachment Script Assessment (ASA)
At the SECCYD age 18 assessment, the adolescent version of the Attachment Script Assessment (ASA; Dykas et al., 2006; Waters & Waters, 2006) was administered. The ASA is a narrative-based measure of attachment for which individuals are asked to tell the best story that they can based on a list of 12 words that serve as an outline for a story about a distressing event (e.g., difficulty studying for an exam) that triggers the adolescent to seek out an attachment figure. Each ASA story was coded on a 7-point secure base script knowledge scale (1 = No secure base script content is apparent to 7 = extensive secure base script organization with substantial elaboration) developed by H. Waters and Rodrigues-Doolabh (2001). Based on prior studies using the ASA (e.g., Steele et al., 2014; Waters, Fraley, et al., 2015), analyses in the current report focused on a single composite score derived by averaging the secure base script knowledge scores across all four stories. ASAs were assessed by two coders in two different locations (n = 424 and n = 420; ICC values of 0.95 between the two coders in each site), and a subset of cases that were evaluated by both sites (n = 170; ICC of 0.93). Additionally, a master coder evaluated a subset of ASAs included in the reliability analysis (n = 70; ICC of 0.93 between the coders in each coding site and the master coder). For further details regarding reliability of the ASA in the SECCYD, see Steele et al. (2014). ASAs were not administered to participants concurrently with the AAIs in the MLSRA.
Depression and Covariate Variables
Depressive Symptoms
At a single time point between ages 26 and 31, all SECCYD individuals were administered the Adult Self-Report (ASR; Achenbach & Rescorla, 2003), and age-appropriate T scores from the ASR’s DSM-oriented Depressive Problems scale were used for the purpose of this study. We used T scores from the Youth Self-Report (YSR; Achenbach & Rescorla, 2001) administered at the time of the AAI at around age 18 were as concurrent depression scores in this sample. In the MLSRA, depressive symptoms were measured both continuously and categorically. Continuous depressive symptomatology variables were derived from the Young Adult Self-Report (YASR; Achenbach, 1997) at ages 23 and 26 years, and from the ASR (Achenbach & Rescorla, 2003) at ages 32 and 39. To obtain a reliable concurrent depressive symptoms composite score we averaged the DSM-oriented Depressive Problems scale items at ages 23 and 26 and then converted that average into age- and sex-appropriate T scores. We followed the same procedure with data from ages 32 and 39 to obtain an adult depressive symptoms composite score. In addition, the Structured Clinical Interview for DSM Disorders (SCID) was used to categorically diagnose depression at age 28, based on reported symptoms from the past 10 years (i.e., starting at age 18), using criteria from the fourth edition of the DSM (DSM-IV; First et al., 1997; Ventura et al., 1998). We created a dichotomous age-28 depression diagnosis (i.e., 0 = never having a major depressive episode in the past 10 years; 1 = having at least one major depressive episode in the past 10 years). We also assessed the predictive validity of AAIsbs on clinically significant self-reported depression over and above traditional AAI derived measures and concurrent depression symptoms. To this end, we dichotomized the depression outcomes T-scores into “non-clinical” and “clinical” depression, using the recommended ASR’s DSM-oriented Depressive Problems clinical cut-off score of 65. In the SECCYD, participants were coded as “0” if their T-scores were below 65, and “1” if their T-scores equaled or exceeded 65. In the MLSRA, participants were coded as “0” if their average T-scores at ages 32 and 39 were below 65, and “1” if their average T-scores in those time points equaled or exceeded 65.
Covariates
Covariates in both the SECCYD and the MLSRA included child ethnicity (White/non-Hispanic vs. other), child sex, maternal years of education, SES, and antecedent measures of cognitive functioning. In the SECCYD, SES was operationalized as a composite score of family income-to-needs assessed at 1, 6, 15, 24, 36, and 54 months; Grades 1, 3, 4, 5, and 6; and age 15 years. Cognitive functioning was measured via the Woodcock-Johnson Psycho-Educational Battery-Revised (WJ-R; Woodcock & Johnson, 1989; Woodcock, 1990; scores available at 54 months, Grades 1, 3, and 5, and age 15). We averaged the standard scores for all available sub-scales at each time point and created a reliable composite from 54 months through age 15 years. In the MLSRA, maternal education was measured as a composite score from seven time points throughout the MLSRA: 3 months before the child’s birth, 42 months, Grades 1–3, Grade 6, and age 16 years. We assessed SES with Duncan’s Socioeconomic Index (Stevens & Featherman, 1981), with composite scores based on the average of caregiver’s occupational prestige at the following child’s age timepoints: 42 months, 54 months, Grades 1–3, Grade 6, and age 16. We measured cognitive functioning with a composite score that included academic achievement assessment during Grades 1, 2, 3, and 6 (via the Peabody Individual Achievement Test; Dunn & Markwardt, 1970) and age 16 years (via the WJ-R).
Analytic Strategy
The protocol for the analyses we conducted in the current study was preregistered with the Center for Open Science, and is accessible via the following link: https://osf.io/c3ax7/?view_only=200065085c4345eb95445db7f045d226. First, we computed zero-order correlations to examine associations between AAIsbs in late adolescence and depressive symptoms in adulthood (Aim 1a). To examine the unique associations between AAIsbs and depressive symptoms above and beyond concurrent depressive symptomatology, we conducted a series of linear and logistic regression analyses, simultaneously entering both AAIsbs and concurrent depressive symptoms scores as model predictors (Aim 1b). Second, to examine whether AAIsbs is more strongly associated with depressive symptoms compared to the ASA (in the SECCYD) and traditional coding scales of the AAI (in both samples), we conducted partial correlations (controlling for concurrent depressive symptoms) between each measure of adult attachment representations and depressive symptoms, which were then compared using Steiger’s Z comparison test (Steiger, 1980) (Aim 2a). To address whether AAIsbs in late adolescence incrementally predicted depressive symptoms in young adulthood relative to the ASA and the traditional coding scales of the AAI, we conducted a series of hierarchal linear and binary logistic regression analyses, with traditional coding scales of the AAI or ASA entered in the first step, and AAIsbs entered in the second step (Aim 2b). Third, we assessed whether and to what extent biological sex, ethnicity (both White/non-Hispanic participants compared to others, and White/non-Hispanic compared to Black participants), and SES moderated any of the attachment representation measures in late adolescence and depressive symptoms in adulthood (Aim 3). Fourth, we conducted all analyses controlling for demographic covariates (i.e., sex, ethnicity, SES, and maternal education) and cognitive functioning. We performed all linear regression analyses for this sample using the ‘lavaan’ package (Rosseel, 2012) in R (R Core Team, 2023) to allow for handling outcome missingness with full information maximum likelihood (FIML). Given that FIML cannot be used to treat missingness when the outcome is binary, when predicting the binary depression diagnosis outcome in the MLSRA subsample we conducted a set of binary logistic regression analyses using SPSS, version 29, using the PROCESS macro, version 4.1 (Hayes, 2017; available at https://processmacro.org/index.html) and cases with missing outcomes were excluded listwise.
Results
For simplicity, we report all analyses with models that included sociodemographic (sex, ethnicity, and SES) and cognitive functioning covariates, which did not differ from the ones without these covariates. We refer the reader to the relevant appendices for results without these covariates.
Aim 1a: How Strong are the Longitudinal Associations Between AAIsbs in Late Adolescence and Depressive Symptoms in Adulthood?
Controlling for demographic covariates and cognitive functioning, a partial correlation between AAIsbs at age 18 and depressive symptoms at around age 30 years was significant in the SECCYD subsample (r = −0.18, p < .001). However, partial correlations between AAIsbs at age 19 and 26 and depressive symptoms in the MLSRA—measured both continuously at ages 32 and 39 and dichotomously at age 28—were non-significant (r = −0.08, p = .31 and r = −0.05, p = .52, respectively).
Aim 1b: Are the Associations Between AAIsbs in Adolescence and Depressive Symptoms in Adulthood Robust to Concurrent Depressive Symptomatology?
In a hierarchal linear regression analysis, AAIsbs in late adolescence was uniquely associated with depressive symptoms at around age 30, above and beyond concurrent (i.e., age 18) depressive symptoms in the SECCYD (B = −0.31, p = .04; Appendix S1, eTable 31). In the MLSRA, AAIsbs was not uniquely associated with depressive symptoms in adulthood above and beyond concurrent depressive symptoms, both when measured continuously at ages 32 and 39 and categorically at age 28 (Appendix S2; B = 0.23, p = .56, eTable 15; and B = 0.04, p = .83, eTable 41, respectively).
Aim 2a: To What Degree Do AAIsbs in Late Adolescence More Strongly Predict Depressive Symptoms in Adulthood Compared to the ASA and the Traditional Coding Scales of the AAI?
A series of Steiger’s Z comparison tests revealed that AAIsbs in late adolescence did not predict depressive symptoms in adulthood significantly more strongly than the ASA (in the SECCYD) or any of the traditional coding scales of the AAI (in both the SECCYD and the MLSRA) (Appendix S1, eTable 32; and Appendix S2, eTable 16, respectively). The same pattern held when comparing the associations between AAIsbs and traditional coding scales of the AAI in predicting categorical depression diagnosis in the MLSRA (eTable 42).
Aim 2b: To What Degree Does AAIsbs in Late Adolescence Incrementally Predict Depressive Symptoms in Adulthood Compared to the ASA and the Traditional Coding Scales of the AAI?
Hierarchical Linear Regression of AAIsec, AAIcoh, Prototypic Dismissing, Prototypic Preoccupied, and ASA Predicts Depression at Around Age 30, Controlling for AAIsbs, Demographic Covariates, and Cognitive Functioning in the Normative-Risk NICHD Study of Early Child Care and Youth Development.
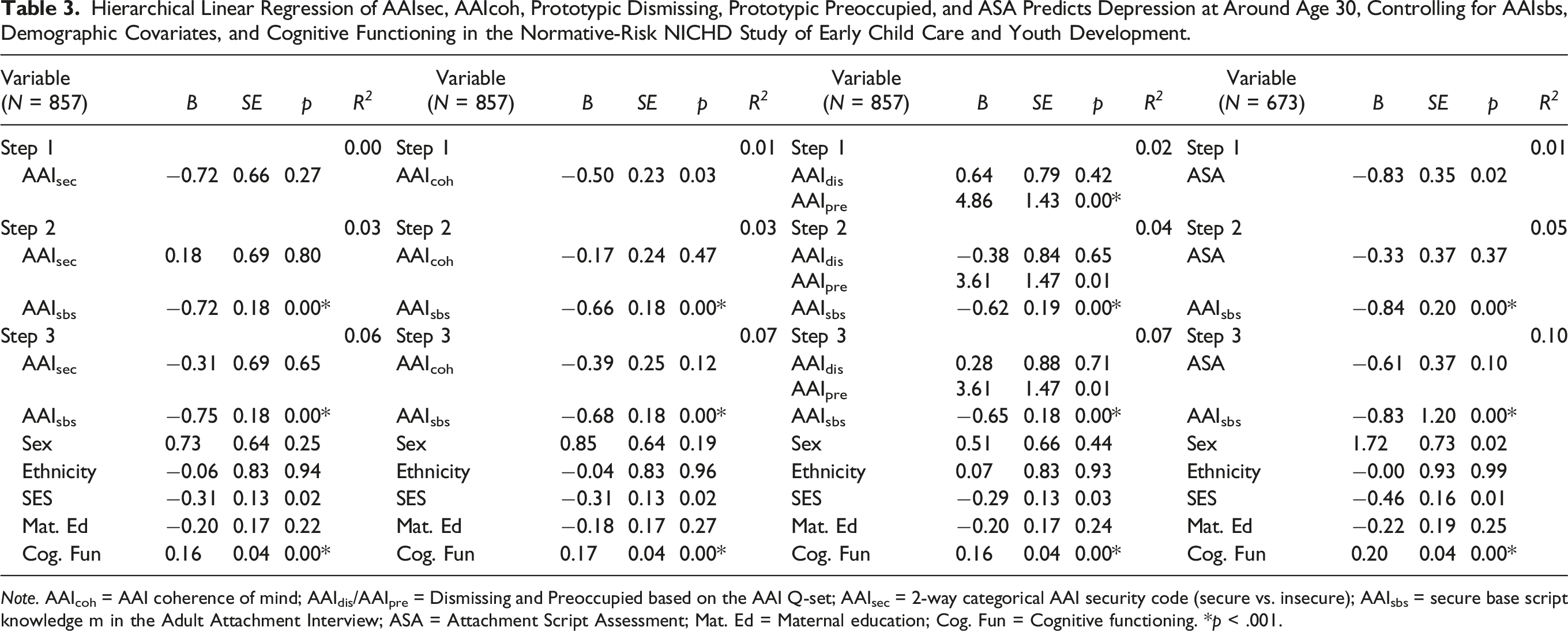
Note. AAIcoh = AAI coherence of mind; AAIdis/AAIpre = Dismissing and Preoccupied based on the AAI Q-set; AAIsec = 2-way categorical AAI security code (secure vs. insecure); AAIsbs = secure base script knowledge m in the Adult Attachment Interview; ASA = Attachment Script Assessment; Mat. Ed = Maternal education; Cog. Fun = Cognitive functioning. *p < .001.
Hierarchical Linear Regression of AAIsec and AAIcoh Predicts Depression Symptoms (at Ages 32 and 39) and Diagnosis (at Age 28), Controlling for AAIsbs, Demographic Covariates, and Cognitive Functioning in the Higher-Risk Minnesota Longitudinal Study of Risk and Adaptation.
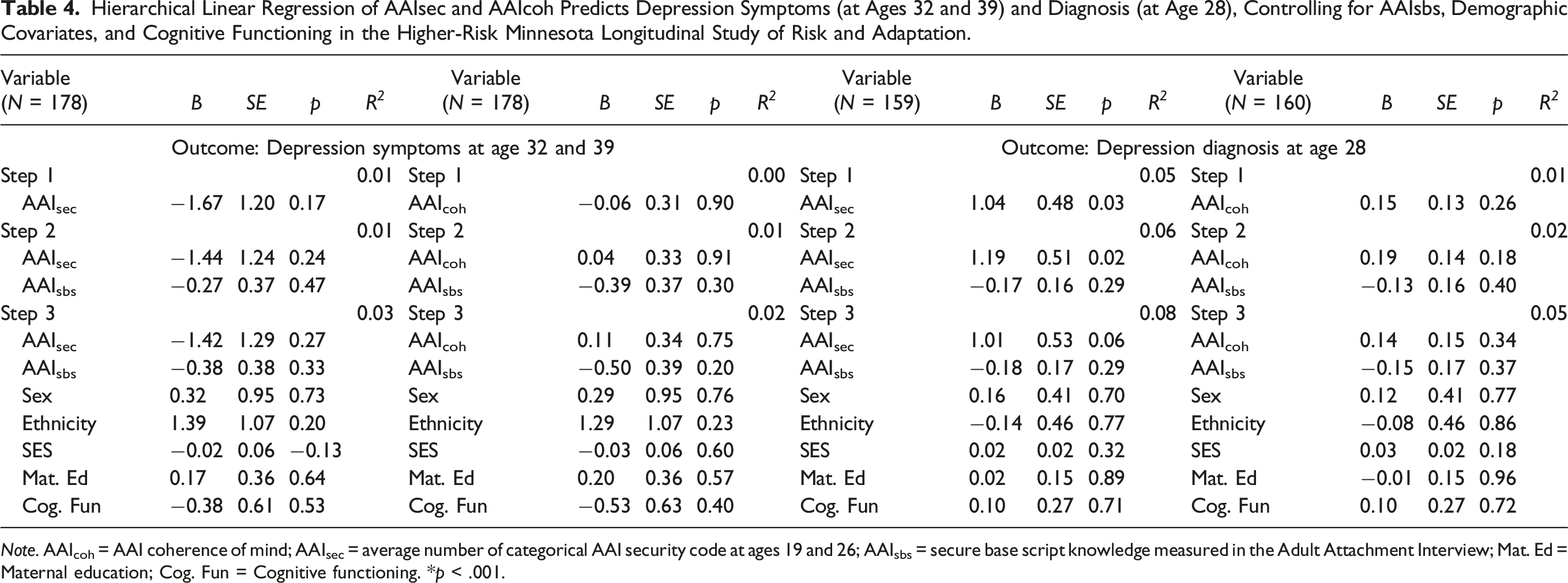
Note. AAIcoh = AAI coherence of mind; AAIsec = average number of categorical AAI security code at ages 19 and 26; AAIsbs = secure base script knowledge measured in the Adult Attachment Interview; Mat. Ed = Maternal education; Cog. Fun = Cognitive functioning. *p < .001.
Aim 3: To What Extent Do Participants’ Sociodemographic Characteristics Moderate the Associations Between Attachment Representations in Late Adolescence and Depressive Symptoms in Adulthood?
In the SECCYD, ethnicity (White/non-Hispanic vs. Black) moderated the association between AAIsbs in late adolescence and depressive symptoms in adulthood (B = -1.53, p = .01; Appendix S2, eTable 45), such that the AAIsbs significantly predicted lower depressive symptoms in adulthood above and beyond concurrent depression symptoms among White/non-Hispanic participants (n = 670; B = −0.39, p = .02), but higher depressive symptoms for Black participants (n = 90; B = 1.22, p = .03). In this sample, ethnicity (White/non-Hispanic vs. Black) also moderated the association between AAIsec and AAIdis in late adolescence and depressive symptoms in adulthood (B = -4.33, p = .03; Appendix S2, eTable 46), such that the AAIsec did not significantly predict depressive symptoms in adulthood above and beyond concurrent depression symptoms for White/non-Hispanic participants (B = −0.49, p = .47), but significantly predicted higher depressive symptoms over and above concurrent depression symptoms for Black participants (B = 4.31, p = .02). Lastly, ethnicity moderated the association between AAIdis in late adolescence and depressive symptoms in adulthood (B = 4.81, p = .04, respectively; Appendix S2, eTable 48), but the association between AAIdis and depression symptoms in adulthood was not significant above and beyond concurrent depression symptoms for neither White/non-Hispanic participants (B = 1.26, p = .12) nor Black participants (B = -4.11, p = .06). No other sociocultural variables in either the SECCYD or the MLSRA moderated the associations between adult attachment representations assessed in late adolescence and young adulthood and depressive symptoms (Appendix S1, eTables 33–56 for the SECCYD; Appendix S2, eTables 19–27 and 45–53 for the MLSRA).
Non-Pre-Registered Analyses
Non-pre-registered analyses revealed a similar pattern of results to those we pre-registered. Controlling for demographic covariates and cognitive functioning, a partial correlation between AAIu at age 18 and depressive symptoms at around age 30 was not significant in the SECCYD subsample (r = 0.01, p = .88). In the MLSRA, AAIu at ages 19 and 26 was not significantly associated with depression, both as assessed continuously at ages 32 and 39 and dichotomously at age 28 (r = 0.05, p = .51 and r = 0.14, p = .09, respectively). AAIu was not correlated with Steiger’s Z comparison tests revealed that AAIsbs in late adolescence did not predict depressive symptoms in adulthood significantly more strongly than AAIu in both the SECCYD (Appendix S3, eTable 7) and the MLSRA (Appendix S4, eTable 6 [predicting continuous depression symptoms at ages 32 and 39] and eTable 16 [predicting categorical depression diagnosis at age 28]). Second, in the SECCYD subsample, AAIsbs was a significant predictor of depressive symptoms at around age 30 above and beyond AAIu (B = −0.78, p < .001; Appendix S3, eTable 8). However, in the MLSRA, AAIsbs did not incrementally predict depressive symptoms (Appendix S4, eTable 7 [predicting continuous depression symptoms at ages 32 and 39] and eTable 17 [predicting categorical depression diagnosis at age 28]). Third, no sociocultural variables in either the SECCYD or the MLSRA moderated the associations between adult attachment representations assessed in late adolescence and young adulthood and depressive symptoms (Appendix S3, eTables 9–12 for the SECCYD; Appendix S4, eTables 8–10 and 18–20 for the MLSRA).
With respect to the set of analyses pertaining to clinical-level self-reported depression outcomes (i.e., ASR T-score of below 65 vs. equal to or exceeding 65), a partial correlation between AAIsbs at age 18 and depression at around age 30 was significant in the SECCYD subsample (r = −0.15, p < .01), but not in the MLSRA subsample (r = −0.09, p = .24). In addition, AAIsbs was not a significant predictor of clinical-level self-reported depression over and above concurrent depression symptoms, sociodemographic covariates, and cognitive functioning in both the SECCYD (Appendix S5, eTable 7) and the MLSRA (Appendix S6, eTable 5). AAIsbs in late adolescence also did not significantly predict clinical-level self-reported depression in adulthood more strongly than the ASA (in the SECCYD) or any of the traditional coding scales of the AAI in both the SECCYD and the MLSRA (Appendix S5, eTable 8; and Appendix S6, eTable 6, respectively). In the SECCYD subsample, AAIsbs was a significant predictor of clinical-level self-reported depression at around age 30 above and beyond any traditional measures of adult attachment and secure base script knowledge (B = −0.23, p < .001 when compared to AAIsec; B = −0.20, p = .004 when compared to AAIcoh; B = −0.18, p = .01 when compared to AAIdis and AAIpre; and B = −0.29, p < .001 when compared to the ASA; Appendix S5, eTable 9). However, in the MLSRA, AAIsbs did not incrementally predict clinical-level self-reported depression at ages 32 and 39 above and beyond any traditional measures of adult attachment (Appendix S6, eTable 7).
Discussion
The aims of the current report were to examine the predictive significance of secure base script knowledge assessed from the AAI (AAIsbs) for depression, compare such associations to other attachment representation measures and their respective associations with depression in adulthood, and assess their sociocultural generalizability. Consistent with our hypothesis, AAIsbs in late adolescence was a significant predictor of depressive symptoms in adulthood above and beyond concurrent depressive symptoms, sociodemographic and cognitive functioning covariates, and did so incrementally compared to the traditional AAI derived measures and the ASA in the normative-risk sample of the SECCYD. However, in contrast to our prediction, this pattern of results did not hold when examined in the higher-risk sample of the MLSRA.
Exploratory analyses revealed that by and large, across both a normative- and high-risk sample, (a) AAIsbs did not significantly differ from AAI derived measures and the ASA in the strength of their respective associations with depression in adulthood, and (b) demographics and cognitive functioning did not moderate the associations reported here between AAIsbs and depression. In one exception, higher levels of AAIsbs were associated with decreased depressive symptoms in the SECCYD in White/non-Hispanic individuals, but was associated with increased depressive symptoms in Black individuals. Taken together, findings from this study extend emerging literature suggesting that secure base script knowledge, which is correlated with early experiences with primary caregivers (e.g., Nivison et al., 2023; Waters et al., 2017), predicts mental health symptoms across the lifespan (e.g., during childhood: Ruiz et al., 2019; Van Aswegen et al., 2023; Waters, Bosmans, et al., 2015; and in young adulthood: Dagan, Groh, et al., 2021).
We did not find significant associations between any of the attachment measures and depression in adulthood in the higher-risk MLSRA sample. As such, findings from this study raise the question regarding the validity of the attachment representation measures in predicting depression in individuals who experience more environmental social stressors (e.g., poverty, low stability of living situations, and low social support), such as those who were initially recruited for the MLSRA (Sroufe et al., 2005). Heightened intensity and quantity of everyday stressors might compromise individuals’ ability to provide effective soothing and interfere with their opportunities to seek out support at times of need, which in turn may increase their depressive symptoms independent of their secure base script knowledge. Methodologically, one should also consider that the MLSRA sample is considerably smaller than that of the SECCYD and, as such, has lower power to detect small effects such as those we observed in the links between AAIsbs and depressive symptoms in the normative-risk SECCYD sample.
Findings from this report suggest that adolescents’ secure base script knowledge— that is, increasing their confidence in the ability to solicit and receive effective support from close others—may function as a modifiable target to reduce their vulnerability to depression symptoms later in life. From a relational perspective—a clinical stance that emphasizes the patient’s relationship to and experience with the therapist (for a collection of seminal papers describing this perspective, see Mitchell & Aron, 1999)—low secure base script knowledge may interfere with the therapeutic relationships clients develop with their mental health practitioners. This is so since suboptimal support soliciting efforts (e.g., being emotionally closed off when in session with the therapist) and difficulties in effectively receiving therapeutic support (e.g., canceling therapy sessions or dropping out from therapy altogether) reduce the therapeutic relationship quality, and thus its ability to function as a secure base from which therapeutic growth (e.g., effective learning of skills or corrective emotional experiences) can occur. Clinicians and mental health practitioners may thus benefit from explicitly teasing out clients’ secure base scripts and communicating with them about how they may play out in the therapeutic relationship, such that adjustments can be made to increase access to secure base scrip knowledge in a way that may be generalized and utilized in other close relationships in the clients’ lives.
Study Limitations and Future Research
Whereas this study leveraged two relatively large, prospective longitudinal studies with participants from diverse sociodemographic backgrounds, two limitations should be noted. First, the current study is correlational in nature. Given preliminary evidence indicating a potential increase in secure base script knowledge following an attachment-based intervention (Raby et al., 2021), future research will benefit from following and experimentally testing both the degree to which AAIsbs scores may be improved post-intervention and whether such change is causally associated with a decrease in depressive symptoms in long-term follow-up assessments. Second, we were unable to assess stability and change in AAIsbs scores during early adulthood in the SECCYD sample, given that AAIs were administered at a single time point. Future research will benefit from multiple assessments of attachment representations over time and a multi-method (and informant) approach to evaluate the development and maintenance of depression levels in adolescence and into adulthood. Lastly, the depression measure we utilized in the SECCYD subsample, in which AAIsbs was found to be significant predictors of depression, was self-reported (i.e., the ASR). It is possible that depression outcomes assessed via a third-party observer (e.g., a clinical interview, as in the case of depression assessment via the SCID in the MLSRA) may lead to different results. Thus, future studies with large samples like that of the SECCYD should incorporate objective clinical assessments of depression to ensure generalizability of the results we obtained in this study across depression assessments.
Conclusion
Attachment theory has long emphasized the crucial role that individuals’ expectations regarding seeking and receiving effective support from close others play in shaping one’s vulnerability to depression (Bowlby, 1973). This study is the first to demonstrate that such expectations extracted from autobiographical narratives during the AAI in late adolescence significantly predict depressive symptoms 12 years later, albeit only in a normative-risk (but not higher-risk) sample. Practitioners are therefore encouraged to assess not only individuals’ life difficulties, but also their tendencies to effectively use others to support them in dealing with these difficulties. Future experimental research is needed to assess whether attachment-based interventions improve AAIsbs and whether such changes are causally associated with a decrease in depressive symptomatology.
Supplemental Material
Supplemental Material - Longitudinal Associations Between Scripted Attachment Representations in Late Adolescence and Depression in Adulthood in a Normative and a Higher-Risk Cohort
Supplemental Material for Longitudinal Associations Between Scripted Attachment Representations in Late Adolescence and Depression in Adulthood in a Normative and a Higher-Risk Cohort by Or Dagan, Marissa D. Nivison, Cathryn Booth-LaForce, Maria E. Bleil, Glenn I. Roisman, and Theodore E. A. Waters in Emerging Adulthood.
Supplemental Material
Supplemental Material - Longitudinal Associations Between Scripted Attachment Representations in Late Adolescence and Depression in Adulthood in a Normative and a Higher-Risk Cohort
Supplemental Material for Longitudinal Associations Between Scripted Attachment Representations in Late Adolescence and Depression in Adulthood in a Normative and a Higher-Risk Cohort by Or Dagan, Marissa D. Nivison, Cathryn Booth-LaForce, Maria E. Bleil, Glenn I. Roisman, and Theodore E. A. Waters in Emerging Adulthood.
Supplemental Material
Supplemental Material - Longitudinal Associations Between Scripted Attachment Representations in Late Adolescence and Depression in Adulthood in a Normative and a Higher-Risk Cohort
Supplemental Material for Longitudinal Associations Between Scripted Attachment Representations in Late Adolescence and Depression in Adulthood in a Normative and a Higher-Risk Cohort by Or Dagan, Marissa D. Nivison, Cathryn Booth-LaForce, Maria E. Bleil, Glenn I. Roisman, and Theodore E. A. Waters in Emerging Adulthood.
Supplemental Material
Supplemental Material - Longitudinal Associations Between Scripted Attachment Representations in Late Adolescence and Depression in Adulthood in a Normative and a Higher-Risk Cohort
Supplemental Material for Longitudinal Associations Between Scripted Attachment Representations in Late Adolescence and Depression in Adulthood in a Normative and a Higher-Risk Cohort by Or Dagan, Marissa D. Nivison, Cathryn Booth-LaForce, Maria E. Bleil, Glenn I. Roisman, and Theodore E. A. Waters in Emerging Adulthood.
Supplemental Material
Supplemental Material - Longitudinal Associations Between Scripted Attachment Representations in Late Adolescence and Depression in Adulthood in a Normative and a Higher-Risk Cohort
Supplemental Material for Longitudinal Associations Between Scripted Attachment Representations in Late Adolescence and Depression in Adulthood in a Normative and a Higher-Risk Cohort by Or Dagan, Marissa D. Nivison, Cathryn Booth-LaForce, Maria E. Bleil, Glenn I. Roisman, and Theodore E. A. Waters in Emerging Adulthood.
Supplemental Material
Supplemental Material - Longitudinal Associations Between Scripted Attachment Representations in Late Adolescence and Depression in Adulthood in a Normative and a Higher-Risk Cohort
Supplemental Material for Longitudinal Associations Between Scripted Attachment Representations in Late Adolescence and Depression in Adulthood in a Normative and a Higher-Risk Cohort by Or Dagan, Marissa D. Nivison, Cathryn Booth-LaForce, Maria E. Bleil, Glenn I. Roisman, and Theodore E. A. Waters in Emerging Adulthood.
Supplemental Material
Supplemental Material - Longitudinal Associations Between Scripted Attachment Representations in Late Adolescence and Depression in Adulthood in a Normative and a Higher-Risk Cohort
Supplemental Material for Longitudinal Associations Between Scripted Attachment Representations in Late Adolescence and Depression in Adulthood in a Normative and a Higher-Risk Cohort by Or Dagan, Marissa D. Nivison, Cathryn Booth-LaForce, Maria E. Bleil, Glenn I. Roisman, and Theodore E. A. Waters in Emerging Adulthood.
Footnotes
Acknowledgements
A cooperative agreement (5 U10 HD027040) between the study investigators that included Cathryn Booth-LaForce and Glenn I. Roisman and the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD) supported the design and data collection of the NICHD Study of Early Child Care and Youth Development (SECCYD) from birth through age 15 years. The age 18-year follow-up data collection was supported by the NICHD under Award Number R01 HD054822 to Cathryn Booth-LaForce and a grant from the NICHD under Award Number R01 HD069442 to Glenn I. Roisman supported the coding of the Attachment Script Assessments. The most recent assessments of the SECCYD with a focus on adult health were supported by the National Heart, Lung, and Blood Institute under Award Number R01 HL130103 to Maria Bleil and by the NICHD under Award Number R01 HD091132 to Maria Bleil and Glenn I. Roisman. Research reported in this publication was also facilitated by the National Institute of Mental Health of the National Institutes of Health via a training grant (T32 MH015755) supporting pre-doctoral research by Marissa D. Nivison at the University of Minnesota. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. The authors have declared that they have no competing or potential conflicts of interest.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute of Mental Health (T32 MH015755), Eunice Kennedy Shriver National Institute of Child Health and Human Development (5 U10 HD027040, R01 HD054822, R01 HD069442, R01 HD091132), and National Heart, Lung, and Blood Institute (R01 HL130103).
Transparency and Openness Statement
The protocol we followed to produce this research paper, including the analytic plan and hypotheses, was pre-registered with the Center for Open Science and is accessible via the following link: ![]() . The data necessary to reproduce the analyses presented here are not publicly accessible. The analytic code used in the analyses presented in this paper is available from the first author.
. The data necessary to reproduce the analyses presented here are not publicly accessible. The analytic code used in the analyses presented in this paper is available from the first author.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.