
Abstract
Several previous systematic literature reviews on psychological growth following trauma are available but fail to target emerging adult complex trauma survivors. The aim of the study was to conduct a systematic review and meta-analyses concerning growth-related psychological constructs among emerging adult survivors of complex trauma. Eight major databases were searched. We obtained 18 selectable articles (89% conducted in the US). The results concluded that growth is possible. Generally, it is stimulated by more complex trauma and can be distinguished according to trauma types. The growth is also generally stimulated by the challenges of new roles and mainly involves intrapersonal dynamics. Furthermore, interpersonal processes have not always supported the growth; there are even times when they hindered. Not a few survivors have grown with psychological distress or disorder, problems or conflicts. They have been flexible in using coping strategies. We generated a weighted mean of complex trauma of 2.83, posttraumatic growth above the hypothetical mean score, and a low positive weighted correlation between the two (14.1%). Implications and cautions for future studies and practices are discussed.
Introduction
Complex trauma has massive and profound impacts, including for emerging adult survivors (18–29 years old; Arnett et al., 2014). The emerging adulthood according to Arnett (2024) supposedly experience five main features, namely identity explorations, instability, self-focus, feeling in-between, and possibilities/optimism. It cannot be ignored that emerging adults have their own vulnerabilities naturally present while living through these times (Newcomb-Anjo et al., 2016). However, Arnett (2024) asserted that with the natural features, eventually, virtually all emerging adults will enter new, long-term obligations in love and work, and once they do, their new obligations will assign them on paths that resist change and that may continue for the rest of their lifes.
On the other hand, Borgese (2019) emphasized that apart from the vulnerabilities as natural consequences of the developmental period, adjustments of emerging adults who have complex trauma histories will still be exacerbated. Complex trauma causes emerging adults to suffer psychologically and socially, even physiologically (Cook et al., 2005; Kliethermes et al., 2014, Shonkoff & Garner, 2012). These complaints cannot be avoided since complex trauma is repetitive/cumulative, chronic, and prolonged, often interpersonal in nature, involving the primary system of upbringing, and often occurring during childhood or adolescence (Cook et al., 2005; Courtois, 2008). The experience of traumatic events occurs over long periods of time during sensitive brain development, impairs the development of a child’s personality and basic trust in relationships (Ford & Courtois, 2009). Emerging adults are most likely to experience complex posttraumatic stress disorder (CPTSD), which is most commonly observed as a result of the complex traumatic experience (e.g., Eidhof et al., 2019; Maercker et al., 2018).
CPTSD is specifically characterized by affective dysregulation, profound negative self-concept, and disturbances in relationships—in addition to the trauma symptoms experienced by trauma survivors generally (World Health Organization [WHO], 2019). In fact, the situation requires emerging adults to have great belief in hope, new opportunities and exploring identities which are mostly focused in the areas of work and love (Arnett, 2024). Arnett (2024) once added that the possibilities/optimism feature is actually important for young people who have grown up in difficult conditions. But in cases where they are survivors of complex trauma, we may be pessimistic that instability, and the experiences of failure or disappointment as the consequences, can finally be illuminating for self-understanding. This experience may make them fall further instead of leading to a more stable identity. In addition to CPTSD, literatures have also described a high tendency for the emergence of other psychological symptoms or disorders. Newbury et al. (2018) pointed out the prevalence of psychiatric problems in emerging adult complex trauma survivors from the highest, i.e., depression (20.1%), substance dependence (alcohol/marijuana; 15.9%), behavioral disorders (15.0%), self-harm (14.2%), and anxiety (7.3%).
Regardless of the severity, psychological growth that indicates positive life change and broadly refers to posttraumatic growth (PTG) can be considered natural after traumatic experiences (Tedeschi & Calhoun, 1996). Significant trauma exposure, including complex trauma, is observed to have a positive correlation with PTG dimensions (Copley, 2015). Jirek and Saunders (2018) further confirmed that the positive relationship between cumulative adversity and PTG is linear. Specifically, those who experienced more types of trauma and more chronic stressors experienced more PTG (Jirek & Saunders, 2018). Furthermore, the hypothesis of a curvilinear relationship—such that individuals with moderate levels of cumulative adversity will experience the most growth—is not supported (Jirek & Saunders, 2018). The latter result disproves the hypothesis made based on several other previous studies (e.g., Kleim & Ehlers, 2009; Kunst, 2010; Lechner et al., 2003).
Previous systematic reviews—with/without meta-analysis—have also been conducted to examine this topic. Meta-analyses conducted by Liu et al. (2017), Schubert et al. (2015), Shakespeare-Finch and Lurie-Beck (2014) resulted in positive weighted correlations between posttraumatic stress disorder (PTSD) and PTG, apart from the various types of trauma experienced, not limited to complex trauma. Besides that, these meta-analyses still focus on psychological growth in relation to complex trauma as disorders—another definition of complex trauma—rather than as trauma events. Other systematic reviews have also been conducted to observe PTG among children and adolescents (Meyerson et al., 2011) and its promotion (Henson et al., 2021). However, those systematic reviews highlighted a wide range of participants’ ages (or else, not emerging adulthood) and diverse types of trauma experiences. In other words, they did not specifically focus on survivors within emerging adulthood and with complex trauma types.
Thus, the psychological growth among emerging adult complex trauma survivors needs to be understood, and previous studies can be referred to. The aim of this systematic literature review was to understand whether complex trauma among emerging adult survivors is associated with growth-related psychological constructs and how it is associated. As the results that will be reported, this systematic literature review extracted and synthesized results based on a comprehensive approach and a rigorous methodological framework. The results will be expected to fill the gap surrounding the exploration of growth following complex trauma as well as use it as a framework for practical implications and further research on underrepresented populations.
Methods
The protocol of this systematic literature review has been registered at PROSPERO with registration number CRD42022368951. Besides the main purposes, this review answers specific purposes, i.e., the locations of studies, the methods, the sample characteristics (including types of complex trauma), the instruments, the growth-related psychological constructs measured, and other variables involved. Critical evaluations of previous studies were carried out using narrative synthesis and meta-analysis.
Inclusion and Exclusion Criteria
The inclusion criteria set were (1) complex trauma referring to the event/complex psychological traumatic experiences as reported and/or measured using self-report (or informant-report) questionnaires or surveys, (2) investigating growth-related psychological constructs, (3) considering other psychological constructs which may appear, (4) published in a peer-reviewed journal (incorporating dissertations and theses as indexed in ProQuest), (5) an original research with cross-sectional/longitudinal, prospective/retrospective, quantitative/qualitative study design, (6) written in English, published since 1990 up to early 2022 (the 1990s were the years in which growth began to be widely studied), and (7) focusing on the targeted population who experienced complex trauma particularly—but not limited to—before emerging adulthood (18–29 years old) as long as complex/chronic/cumulative/multiple, and involved in the study during emerging adulthood. While the exclusion criteria set were (1) complex trauma refers to the symptoms experienced/complex non-psychological traumatic experiences, (2) focusing only on physical-related outcomes, (3) a single-case or an experimental study design (exposure is defined as complex trauma experienced), and (4) focusing on other traumatic events, single or acute traumatic events. Qualitative studies defined participants’ specific criteria, in addition to research results, as indicators of growth, in line with Tedeschi et al. (2018) that PTG could occur even in one domain out of five (i.e., relating to others, new possibilities, personal strengths, spiritual and existential changes, and appreciation of life) but was significant for individuals.
Search Strategy
Following PRISMA-P (the preferred reporting items for systematic review and meta-analysis protocols; Moher et al., 2015), pertinent studies were identified through eight major database searches: Scopus, EBSCOhost, PubMed, ProQuest (scholarly journal; dissertations and theses), PsycArticles, Emerald Insight. The selected databases could accommodate Boolean/keyword phrases that had been defined as follows “complex trauma*” (OR “multi* trauma*” OR “mix* trauma*” OR “repeat* trauma*” OR “chronic trauma*” OR “advers* child*” OR “child* advers*” OR “early advers*” OR “early child* advers*” OR “child* trauma*” OR “relation* trauma*” OR “development* trauma*” OR “polyvictimiz*” OR “multi* victimize*” OR “early victimiz*” OR “child* victimiz*” OR “child* interpersonal victimiz*” OR “cumulative trauma*” OR “cumulative child* trauma” OR “lifetime victimiz*” OR “lifetime revictimiz*” OR “child* maltreatment” OR “early child* trauma” OR “complex psychological trauma” OR “parental maltreatment”) in conjunction with grow* (OR “psychological growth” OR “personal growth” OR “post-traumatic growth” OR “posttraumatic growth” OR ptg OR “positive change” OR “positive outcome”), and “emerging adult*” (OR “young adult*” OR youth OR youngster OR “young people” OR “college student*” OR “undergraduate student*” OR “undergraduate*” OR “university student*” OR “transition to adult*” OR “adult* transition” OR “higher education” OR “bachelor student*”).
Data Extraction and Risk of Bias or Quality Assessment
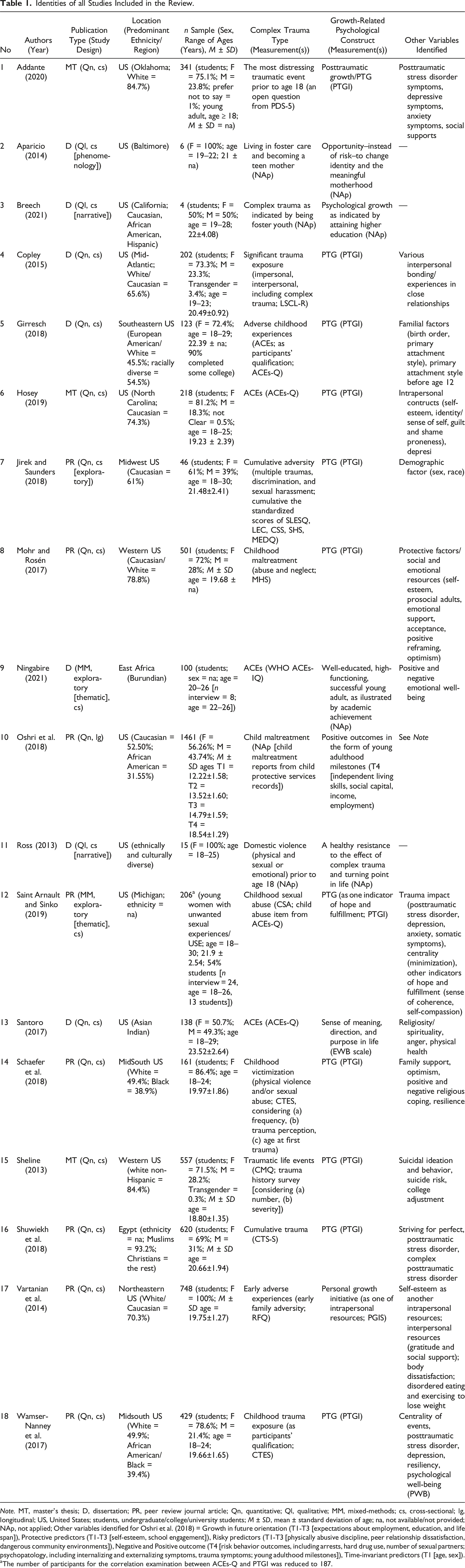
The articles’ selection was conducted in two phases (see Figure 1). The first phase was based on the title and abstract, and the second phase was based on full text to verify whether the article examined the conceptual variables of interest. The final inclusion and exclusion criteria were defined based on a checklist of selection criteria. The organization of all articles was conducted using Rayyan Software and Microsoft Excel. The quality and risk of bias across all the identified studies (see Table 1) were assessed by two reviewers who implemented the checklists created by the Joanna Briggs Institute (JBI). The JBI’s checklists are available for assessing the many aspects of a study’s quality presented in a full-text paper, both quantitative and qualitative evidence. This can decrease the possibility of including biased or misleading results for quantitative evidence, as well as the rigor of the research and the level of transferability for qualitative evidence. If there were discrepancies in the decision to include or exclude any studies, a third reviewer would be consulted. Flow diagram summarizing steps of the systematic literature search according to the PRISMA guideline. Identities of all Studies Included in the Review. Note. MT, master’s thesis; D, dissertation; PR, peer review journal article; Qn, quantitative; Ql, qualitative; MM, mixed-methods; cs, cross-sectional; lg, longitudinal; US, United States; students, undergraduate/college/university students; M ± SD, mean ± standard deviation of age; na, not available/not provided; NAp, not applied; Other variables identified for Oshri et al. (2018) = Growth in future orientation (T1-T3 [expectations about employment, education, and life span]), Protective predictors (T1-T3 [self-esteem, school engagement]), Risky predictors (T1-T3 [physically abusive discipline, peer relationship dissatisfaction, dangerous community environments]), Negative and Positive outcome (T4 [risk behavior outcomes, including arrests, hard drug use, number of sexual partners; psychopatology, including internalizing and externalizing symptoms, trauma symptoms; young adulthood milestones]), Time-invariant predictors (T1 [age, sex]). aThe number of participants for the correlation examination between ACEs-Q and PTGI was reduced to 187.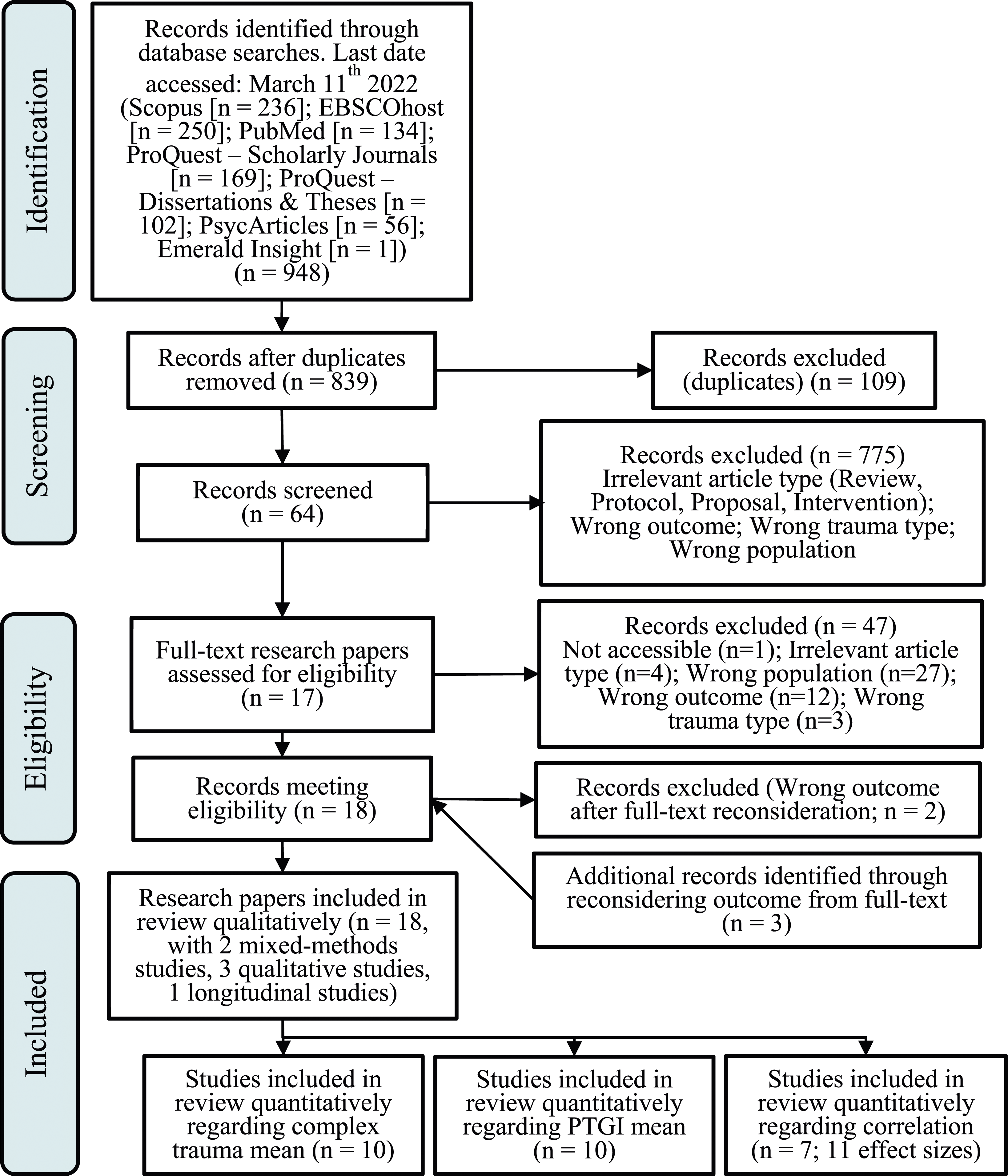
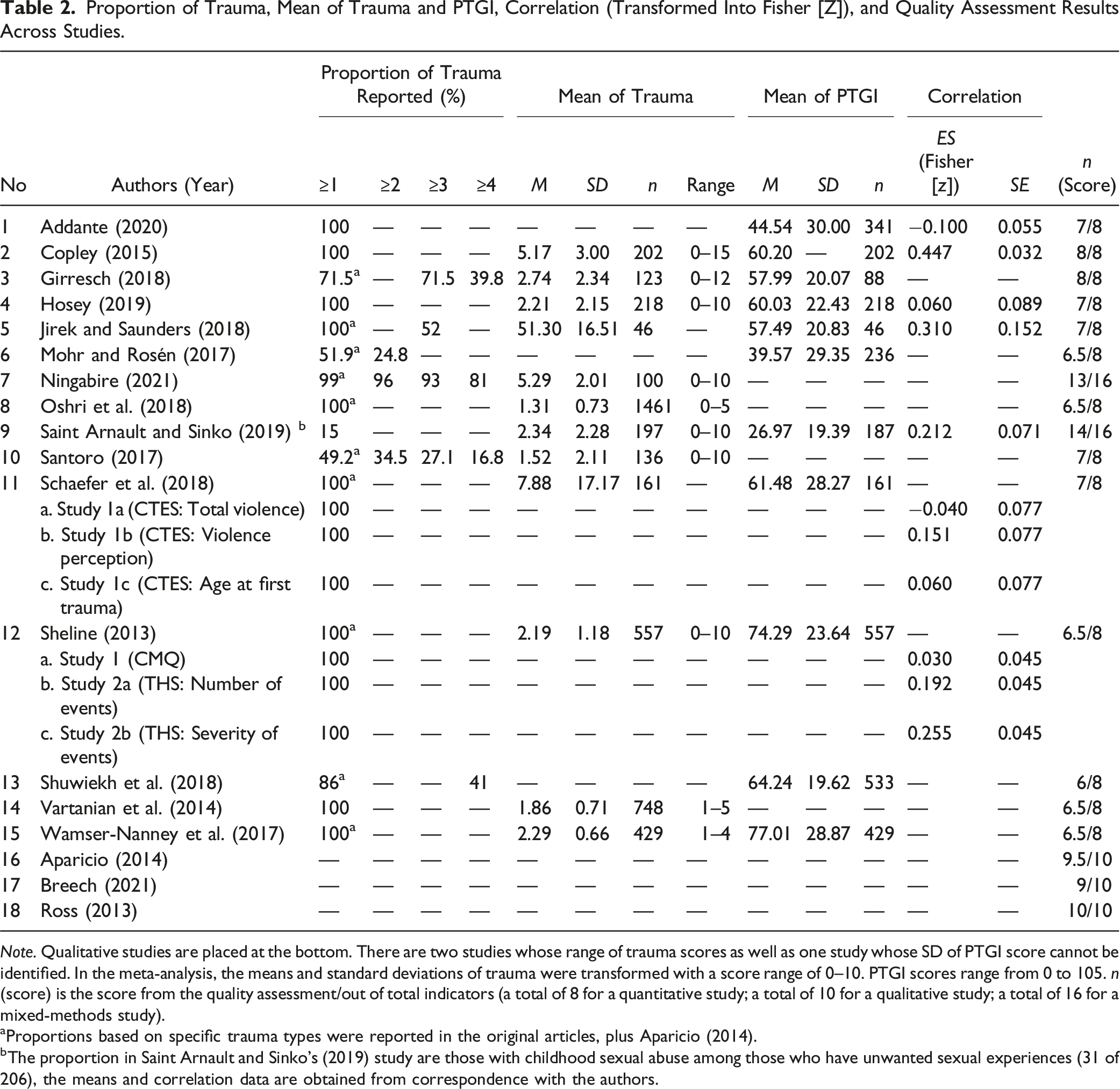
Quantitative papers were assessed with 8 indicators, while qualitative papers were assessed with 10 indicators (see Figure 2). Two of the indicators were applied to both quantitative and qualitative papers. Mixed-methods papers were assessed using combined indicators of qualitative and quantitative papers, consequently 16 indicators were used. Fulfilled indicator was scored 1, and a score of 0 otherwise. Any presence but incomplete information would be scored .5. The score for each paper can be seen in Table 2, while the percentage of papers that meet each indicator can be seen in Figure 2. Percentage of articles that meet each indicator of risk of bias or quality assessment. Proportion of Trauma, Mean of Trauma and PTGI, Correlation (Transformed Into Fisher [Z]), and Quality Assessment Results Across Studies. Note. Qualitative studies are placed at the bottom. There are two studies whose range of trauma scores as well as one study whose SD of PTGI score cannot be identified. In the meta-analysis, the means and standard deviations of trauma were transformed with a score range of 0–10. PTGI scores range from 0 to 105. n (score) is the score from the quality assessment/out of total indicators (a total of 8 for a quantitative study; a total of 10 for a qualitative study; a total of 16 for a mixed-methods study). aProportions based on specific trauma types were reported in the original articles, plus Aparicio (2014). bThe proportion in Saint Arnault and Sinko’s (2019) study are those with childhood sexual abuse among those who have unwanted sexual experiences (31 of 206), the means and correlation data are obtained from correspondence with the authors.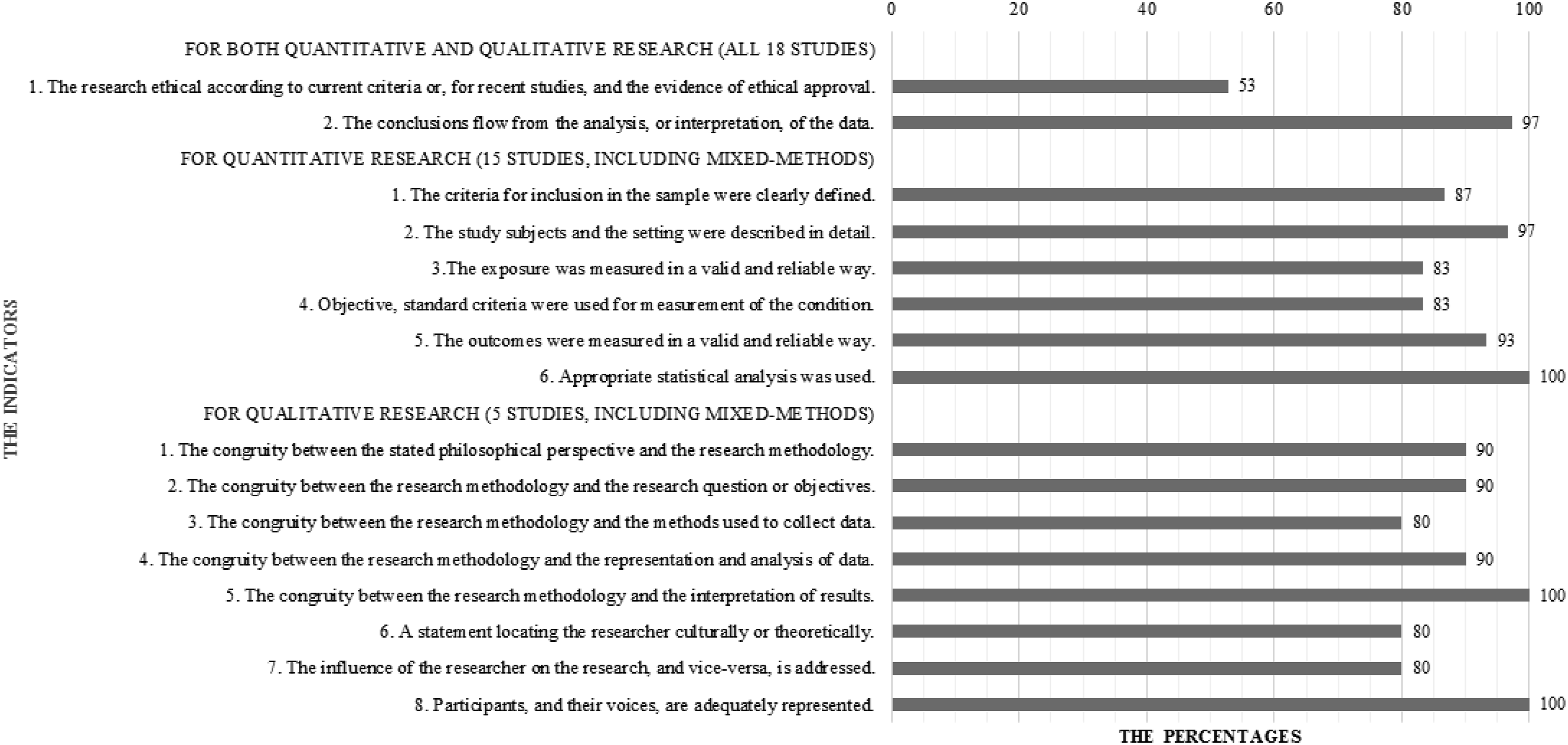
Data Synthesis
To conduct the analysis, growth-related psychological constructs were classified as criterion variables (also could be mediators or moderators) and complex trauma was classified as the predictor variable (also could be a participant qualification). First, the characteristics of each study were summarized (see Table 1). Next, similar studies were grouped within each comparison, then the data that were available for synthesis would be determined. Specifically, we carried out a thematic analysis (Braun & Clarke, 2006), namely in three stages (1) preliminary coding of study abstracts, (2) initial coding and extraction of findings, and (3) focused coding of extracted findings. Preliminary coding was carried out by first familiarizing the study abstracts, making a list of themes, ideas, concepts, and findings. We organized these initial ideas and systematically created initial codes from interesting features of the data. Initial coding was continued by extracting study findings, collating them into potential themes and collecting all relevant data to be assigned to these potential themes. The third stage, namely focused coding reviewed potential themes and produced a thematic “map” of the analysis. Ongoing analysis was carried out for refinement before finally producing clear definitions, naming each theme, and reporting the results of the analysis. A revised model of PTG (Tedeschi et al., 2018) was used as the theoretical framework to guide the review and synthesis.
Comprehensive Meta Analysis (CMA) Version 4 was used to calculate the weighted mean effect size of (1) complex trauma scores, (2) PTG scores using the Posttraumatic Growth Inventory (PTGI), and (3) correlations between complex trauma and PTGI in emerging adults. The meta-analyses that were performed in this review might increase power and precision (or not if relevant), allow investigation of the consistency of effects as well as reasons for differences in effect estimates, and even settle controversies from conflicting studies (Higgins & Thompson, 2011). The weighted mean effect sizes of the three meta-analyses should be analyzed and interpreted by considering the data heterogeneity and potential publication bias. The random effect model was used if the data heterogeneity was significant at Cochrane’s Q (p < .05) or high at I2 (>50%) (Higgins & Thompson, 2011). High heterogeneity also indicated the presence of a moderator(s). Therefore, subgroup analysis which mean separating all participant data into subgroups based on moderator variables could be performed whenever possible. The meta-analysis of mean scores of complex trauma considered the transformation of the score range variation to 0 to 10, while the meta-analysis of PTGI mean scores was based on the same score range. The meta-analysis of correlations transformed each r into Fisher’s z value, then weighted with 95% Confidence Interval (CI). Potential publication bias, that is, the tendency to publish statistically significant rather than nonsignificant results, was evaluated using visual assessment of funnel plot asymmetry (Kendall’s τ, p < .05), significant Egger’s test (z, p < .05), and Fail-safe N with a value of less than 5k + 10 (Egger et al., 1997; Rosenthal, 1991). A large number of studies from Fail-safe N nullify the effect so as not to indicate publication bias.
Results
Characteristics of the Included Studies
Eighteen of the 839 studies were obtained through selection based on inclusion and exclusion criteria (see Figure 1). The characteristics of each study are shown in Table 1. Years of publication ranged from 2013 to 2021, with the majority of studies were conducted in the US (n = 16; culturally diverse, mostly Caucasian/White), while the rest were in East Africa (Burundian) and Egypt (mostly Muslims). The distribution of study areas conducted in the US itself was Northeast (n = 2), Midwest (n = 2), South (n = 6), West (n = 3), and the rest did not mention any specific region (n = 3). One of the studies in the US that did not refer to a specific region specifically involved participants from a collectivistic culture, namely Asian Indians. Eight studies were peer reviewed journal articles, seven studies were dissertations, and three studies were master’s theses. The majority of studies (n = 13) used a quantitative approach, followed by a qualitative approach (n = 3) and mixed-methods approach (exploratory and nested design; n = 2). One of the quantative studies was a longitudinal study, while the rest were entirely cross-sectional. The number of participants involved in the studies ranged from four to 1461 with a total of 5876 participants (the age ranged from 18 to 30 years; the majority of the average age is under 25 years; 32 were nested subsamples), divided into 3927 from twelve studies (n of male = 791; n of female = 3022; n of transgender/not clear = 114) specifically identified as students (8 were nested subsamples) and 1949 from six studies (n of male = 741; n of female = 1208) identified as emerging adults in general with combined status as students and non-students (24 were nested subsamples).
Assessment of Complex Trauma
Complex trauma was positioned as a predictor, observed its presence, or defined as the main characteristic of participants (see Table 1). The terms used ranged from general (adverse childhood experiences [ACEs; n = 4], childhood trauma [exposure; n = 2], significant trauma exposure [n = 1], cumulative adversity/trauma [n = 2], traumatic life events [n = 1], childhood maltreatment [n = 2], early adverse experiences in family [n = 1], childhood victimization with particular types [physical violence and/or sexual abuse; n = 1]) to specific ones (being foster youth [n = 1], domestic violence exposure [physical and sexual or emotional] during childhood or adolescence [n = 1], childhood sexual abuse among those with unwanted sexual experiences [n = 1], becoming a teen mother while living in foster care [n = 1]). Specific traumas, namely sexual harassment and discrimination, were also identified after the measurements for multiple traumas (Jirek & Saunders, 2018).
Complex trauma was measured using a questionnaire (n = 11), multiple questionnaires (two to five; n = 2) or based on a government database (n = 1), an open-ended question from The Posttraumatic Diagnostic Scale for DSM-5 (PDS-5; n = 1) or a participant-specific main criterion especially in qualitative studies (n = 3). The two most used instruments were the Adverse Childhood Experiences Questionnaire (ACEs-Q; n = 4) and the Childhood Traumatic Events Scale (CTES; n = 2); while the rest were used once each, i.e. the WHO Adverse Childhood Experiences International Questionnaire (WHO ACEs-IQ), Trauma History Survey, Cumulative Trauma Scale–Short Form (CTS-S), Maltreatment History Survey (MHS), Childhood Maltreatment Questionnaire (CMQ), Risky Families Questionnaire (RFQ), Life Stressor Checklist-Revised (LSCL-R). One study measured cumulative adversity by calculating the cumulative standardized scores of The Stressful Life Events Screening Questionnaire (SLESQ), The Life Events Checklist (LEC), The Chronic Stress Survey (CSS), The Sexual Harassment Survey (SHS), and The Major and Everyday Discrimination Questionnaire (MEDQ).
Table 2 shows that the majority of studies (n = 12) had 100% participants with at least one type of childhood adversities as a prerequisite for qualifiying participants and/or responding to PTGI. There were five studies that provided proportions of participants with at least one type of adversities less than 100%, ranged from 49.2% to 99%, excluding Saint Arnault and Sinko (2019) that only identified a history of childhood sexual abuse (15%) of those with unwanted sexual experiences. Furthermore, there were three studies that presented at least two types (24.8%–96%) and three types (27.1%–93%) of proportions of adversity experiences, as well as four studies with proportions at least four types of adversity experiences (16.8%–81%). Varying proportions based on specific trauma types were reported by 11 studies.
Assessment of Growth-Related Psychological Constructs
Posttraumatic growth (PTG) as measured using The Posttraumatic Growth Inventory (PTGI; see Table 1) was the most widely used construct (n = 11; two were tested for latent profiles). Other growth-related constucts measured were personal growth initiative (measured using the Personal Growth Initiative Scale [PGIS]), sense of meaning, direction, and purpose in life (measured using the Existential Well-Being [EWB] scale), as well as young adulthood milestones as forms of positive outcomes (independent living skills, social capital, income, employment). In one mixed-methods study and qualitative studies (n = 4), growth was indicated from participants’ specific criteria, i.e., a highly functioning and higher education attainment (n = 2), an opportunity (instead of risk) to change identity and experience the meaningful motherhood (n = 1), and a healthy resistance to the effects of domestic violence exposures and turning point in life (n = 1). Qualitative approaches explained the growth experiences more deeply compare to other approaches.
Other Variables Involved in the Studies
The involvement of other diverse pre-determined variables was observed in quantitative single-method (n = 13) and mixed-methods studies (n = 2). Other variables (see Table 1) can be interpreted as intrapersonal or interpersonal, covert or overt, trait or state. They were positioned as predictor/independent variables, as criterion/dependent variables, as mediators, as moderators, as positive/protective factors or positive outcomes, as negative/risk factors, or psychological distress/disorders/negative impacts, to as health-related behaviors and outcomes. Two studies used demographic factors (i.e., sex and race; Jirek & Saunders, 2018) and familial factors (i.e., birth order and primary attachment style; Girresch, 2018) as other variables to explore trauma and growth. One quantitative study used a longitudinal design involving periodic measurements of growth in future orientation, protective predictos, and risky predictors during adolescence (Oshri et al., 2018).
Narrative Synthesis
The narrative synthesis was conducted in two stages to obtain a growth profile among emerging adults exposed to complex trauma. Stage one was preliminary syntheses that produced eight themes. Stage two was re-analysing the relationships between and within studies and obtaining superordinate categories that produced four major themes with two sub-themes each. In this article, the authors use the abbreviation PTG specifically for posttraumatic growth produced using PTGI. The four major themes with their respective sub-themes are (1) the role of traumatic experiences, including the themes of the role of ‘complexity of the trauma(s)’ and ‘trauma types’; (2) the role of resources, including the role of ‘intrapersonal’ and ‘interpersonal’ matters; (3) the role of negative issues, including the role of ‘psychological distress or disorder’ and ‘problems/conflicts’; (4) the role of challenging adjustments, including the role of ‘a new role(s)’ and ‘flexible coping strategies’. The explanations are as follows.
The Role of Traumatic Experiences
The Role of Complexity of the Trauma(s)
Psychological growth is explained with regard to the history of complex trauma itself, i.e., the complexity of trauma through the presence or absence of correlations, in addition to the presence of growth amidst the complexity of childhood trauma; either through quantitative (Copley, 2015; Girresch, 2018; Hosey, 2019; Jirek & Saunders, 2018; Oshri et al., 2018; Santoro, 2017; Schaefer et al., 2018; Sheline, 2013; Shuwiekh et al., 2018; Vartanian et al., 2014), qualitative (Aparicio, 2014; Breech, 2021; Ross, 2013), and mixed-methods studies (Ningabire, 2021; Saint Arnault & Sinko, 2019).
First of all, the role of complexity can be identified through whether there is a positive correlation between variables indicating complex trauma and PTG. Although unable to prove the curvilinear relationship hypothesis, PTG is positively associated whether with cumulative adversity, the number of trauma types or the number of chronic stressors (Jirek & Saunders, 2018). Meanwhile, Copley (2015) looked specifically at the domains of PTG, gaining significant positive correlations between repeated trauma experiences and the domains of relating to others, personal strengths, and spiritual changes—indicating that the domains may be stimulated differently by the complexity of trauma. Positive correlations are also observed between perceptions of event severity and PTG—significant in one study (Sheline, 2013) but not in another (Schaefer et al., 2018). Similar to the study by Schaefer et al. (2018), the absence of significant positive correlations either between ACEs or number of life events and PTG was observed by Hosey (2019), Jirek and Saunders (2018).
The complexity of trauma also determines PTG through a correlation with independent variables indicating age and duration of complex trauma experiences, that the younger the trauma is experienced, the more complex the trauma, considering inadequate coping capacity. A negative correlation between the age at first trauma and PTG observed by Jirek and Saunders (2018) confirms that the more complex the trauma, the higher the PTG. However, this result was disproved by another study suggesting that there is a positive correlation between the age of experience and PTG—which is also specifically and partially in the domains of the appreciation of life and new possibilities (Shuwiekh et al., 2018). The result by Shuwiekh et al. (2018) is actually similar to what Copley (2015) observed, that the development of the two domains is not supported by the complexity of trauma. Instead, Shuwiekh et al. (2018) explained the negative role of complexity, specifically in terms of age and duration, towards both domains. Meanwhile, Jirek and Saunders (2018) did not confirm a correlation between the calculated amount of time since trauma and PTG, where the trauma can be various, including complex ones. It is true that the correlation’s direction is positive—logically correct, considering that it should be the opposite of the correlation between age of trauma experienced and PTG. However, the positive correlation is not significant.
Other studies indicate a positive association of complexity in various ways, including having experienced multiple or repeated adversities during childhood and adolescence but achieving growth beyond expectations in emerging adulthood. For instance, the participants with unwanted sexual experiences (USE) have significantly higher PTG precisely if they are childhood sexual abuse (CSA) survivors (Saint Arnault & Sinko, 2019). In academics, relatively higher education, which seems to be the reason for high PTG scores, is more likely to be achieved by emerging adults with exposure to 4+ ACEs (Girresch, 2018). Meanwhile, other studies with qualitative approaches set exposures of some complex trauma types in childhood and youth as a qualification, such as experiences of exposure to domestic violence accompanied by some other adversities (including homelessness, poverty, parental substance abuse, child maltreatment and actual abandonment; Ross, 2013), becoming teen mothers besides living in foster care (Aparicio, 2014), or ‘simply’ becoming former foster youths who also have heavy experiences (Breech, 2021).
Some studies with other growth-related psychological constructs explain the opposite result—the increasing complexity of adversity histories may hinder. Oshri et al. (2018) observed that optimal emerging adult developmental milestones were obtained when the protective factor index was higher, conversely the risk factor index was lower during adolescence. It was also observed that the greater number of early adverse experiences, the lower personal growth initiative (Vartanian et al., 2014), sense of hope for the future (Ningabire, 2021), existential well-being, sense of meaning, life purpose, and direction (significantly lower for those with at least one ACE compared to zero ACE; Santoro, 2017). The results indicate that none of the correlational studies with other growth-related psychological constructs in this review correspond to the nature of PTG that presents due to adversity experiences.
The positive role of trauma complexity on PTG may be supported by some studies, but the potential positive correlation in some other studies was not observed to be significant. When it comes specifically to PTG domains, the results of studies with further examinations are more likely to differ between domains—which from this limited study review, the domains of the appreciation of life and new possibilities seem less supported.
The Role of Trauma Types
The role of trauma types is revealed by limited cross-sectional quantitative studies. One result suggests that trauma types, which may also explain higher severity levels, hinder PTG. This was observed by Shuwiekh et al. (2018) that single and secondary trauma were more likely to stimulate PTG, conversely chronic trauma prevented PTG. Such a result is actually the opposite of what was expected from the previous sub-theme, where complexity supports growth. The existence of a curvilinear relationship might explain the result, but this presumption has been refuted by the Jirek and Saunders’s study (2018). Nevertheless, in contrast to the study from Shuwiekh et al. (2018) who compared complex and non-complex trauma, the previous sub-theme emphasizes severity based on the accumulation of complex trauma.
Other results shed light on the role of the interpersonal type of complex trauma, which has only been observed specifically—not cumulatively—by subtype, with mixed results. A study by Addante (2020) did not confirm that cumulative interpersonal trauma distinguishes latent classes of PTG and psychological distress. Meanwhile other studies considering subtypes of interpersonal early childhood trauma have mixed effects. PTG is significantly negatively correlated with the type of attachment trauma, but not with either physical abuse (Shuwiekh et al., 2018), sexual abuse/harassment (Jirek & Saunders, 2018; Shuwiekh et al., 2018), or discrimination stressors (Jirek & Saunders, 2018). However, despite the insignificant correlations, Jirek and Saunders (2018) reported unique contributions of sexual harassment and discrimination to PTG variance of 12% and 6% respectively.
Finally, when specific types of trauma (either sexual victimization, serious illness/injury, or violence exposure) are tested for their moderating role in the positive relationship between event centrality and PTG (with death of a loved one as a reference), they are not proven (Wamser-Nanney et al., 2017). However, sexual trauma as the index event will make stronger ties than for death of a loved one, namely between event centrality and most outcomes—negatively and positively (except PTG and resiliency), including four of the five domains of psychological well-being (PWB, except positive relations).
The Role of Resources
The Role of Intrapersonal Matters
Psychological growth as intrapersonal matters is synthesized from the majority of studies both quantitative (except Sheline, 2013), qualitative (Aparicio, 2014; Breech, 2021; Ross, 2013), as well as mixed-methods (Ningabire, 2021; Saint Arnault & Sinko, 2019). Among them, two specifically explore PTG by domains (Copley, 2015; Shuwiekh et al., 2018), two describe differences between PTG and resilience (Schaefer et al., 2018; Wamser-Nanney et al., 2017), and one describes the difference between PTG and PWB (Wamser-Nanney et al., 2017).
The first is the concern for the influence of demographic or given characteristics on growth, such as sex, age, race/ethnicity, and culture. Neither sex nor age in this review plays a role in their association with PTG. However, contrasting characteristics due to minority status (especially in terms of race/ethnicity) and culture likely play a role. Sex does not distinguish or correlate with PTG (Girresch, 2018; Jirek & Saunders, 2018; Wamser-Nanney et al., 2017), and does not distinguish between the four latent classes of psychological distress and PTG (Addante, 2020). Current age (Jirek & Saunders, 2018; Wamser-Nanney et al., 2017) is not correlated with PTG. Nevertheless, trauma complexity which is inferred based on age and time since the event has its own dynamic (see the first theme). Race/ethnicity or minority status is not correlated with PTG (Jirek & Saunders, 2018; Wamser-Nanney et al., 2017), except for Girresch (2018) that proved a significant difference in the highest scores of black ethnic minority (African American) compared to the lower scores of other racial/ethnic minorities and the lowest scores of white ethnicity (European American). Finally, Santoro (2017) stated that collectivistic (Eastern) culture—where the concept of Dukkha, or suffering inherent to the human condition, is applied—needed to be considered to explain his research results.
The second is the concern for intrapersonal variables related to growth processes. PTG is positively correlated with intrapersonal characteristics which are frequently attributed to the favorability of individuals’ outcome expectancy in the context of adversity. These characteristics include optimism, positive religious coping (i.e., looking to God for support and guidance; forgiveness; Schaefer et al., 2018), acceptance, positive reframing (Mohr & Rosén, 2017), event centrality (Wamser-Nanney et al., 2017), resilience (Schaefer et al., 2018; Wamser-Nanney et al., 2017), and striving for ‘standards’ and ‘order’ (Shuwiekh et al., 2018). A study involving other growth-related psychological constructs indicates that positive outcomes in young adulthood are positively correlated with future orientation at younger ages (Oshri et al., 2018). Even evaluation of individuals’ sense of self and worth i.e., self-esteem, to the point that they perceive themselves as a bad person and feel shame, in this case shame that caused negative self-evaluation, are also positively correlated with PTG (Hosey, 2019). Self-esteem was also observed by Vartanian et al. (2014) to be positively correlated with personal growth. Similarly, Oshri et al. (2018) observed that self-esteem was positively related to future orientation, consistently in periodic measurements during adolescence, which then contributed to positive outcomes in young adulthood.
However, according to another study, disturbance and chaos of individuals’ value processing system due to initial or ongoing self-discrepancy may limit the potential for PTG (Shuwiekh et al., 2018). On the other hand, when the sense of coherence—which also indicates the absence of discrepancy—was examined separately by Saint Arnault and Sinko (2019), it was not proven to be correlated with PTG. Some other constructs that have not been shown to be correlated are negative religious coping (i.e., feeling abandoned by God; anger towards God; Schaefer et al., 2018), shame particularly that caused withdrawn (Hosey, 2019), and self-compassion (Saint Arnault & Sinko, 2019). These last three variables appear to be more diverse in relation to PTG, interestingly self-compassion which is widely attributed to better adaptation. However, this is not surprising as Saint Arnault and Sinko (2019) observed that in contrast to PTG, self-compassion (as well as sense of coherence) was likely to be higher in non-complex trauma than in complex trauma. Ningabire (2021), described in the latter sub-theme, also implied that high levels of self-compassion and a sense of coherence can actually weaken growth. In addition, Mohr and Rosén (2017) suggested no effect of optimism and self-esteem—different form the results of other previously mentioned studies. They argued that the absence of effects is likely to be explained by the failure to consider that individuals are in their healing process. Despite these contrasting results, Schaefer et al. (2018) and Hosey (2019) suggested employing optimism (including practicing gratitude) as well as self-esteem enhancing strategies among individuals following childhood adversity.
Some mechanisms of intrapersonal processes are observed based on qualitative studies where individuals then develop hopefulness and confidence about the future. Self-reliance is strengthened (Breech, 2021; Saint Arnault & Sinko, 2019). The mechanisms include the awakening hope and feeling capable (along with ‘letting-go’, acceptance, strength, and being involved in interpersonal matters; Saint Arnault & Sinko, 2019), the development of compensatory characters (i.e. being creative, curious, resilient, reading avidly; Breech, 2021), the implementation of coping strategies that encourage optimal functioning (i.e., solution-focused, minimization, normalization of the issues, prayer and faith; Ningabire, 2021), and overall acceptance (i.e., having faith in one’s decision making and taking ownership of their experiences or having an internal locus of control, and including acceptance of family imperfections which is included in the interpersonal sub-theme; Ross, 2013). In addition, quantitative studies also find mechanisms for the moderation of emotional, but combined with social resources as individuals may be in their healing process (Mohr & Rosén, 2017). Meanwhile, Santoro (2017) observed that religious/spiritual struggle and unhealthy ways of anger expression were higher as ACEs increased, thus lowered existential well-being—indicating that interventions that specifically address these two mediating variables may increase one’s sense of life meaning and purpose. Despite what Santoro (2017) observed, Schaefer et al. (2018) highlighted the importance of understanding cognitions related to religious coping and optimizing the positive ones, rather than simply encouraging broadband religiosity. This is because adaptive outcomes were only found to be associated with positive, but not negative religious coping (including anger).
Furthermore, two studies observe differences in the mechanisms of PTG attainment compared to PWB and resilience. Paying close attention to these three variables is important because of their joint indication of adaptive and mental health outcomes (Schaefer et al., 2018; Wamser-Nanney et al., 2017). In contrast to PTG which is positively associated with event centrality, almost all PWB subscales are negatively associated (i.e., autonomy, environmental mastery, positive relations with others, purpose in life, and self-acceptance)—interestingly except for the personal growth subscale which is not significant (Wamser-Nanney et al., 2017). It is also observed that contrary to resilience, PTG benefits from event centrality (Wamser-Nanney et al., 2017) but less from family support (Schaefer et al., 2018). When the type of trauma was tested for moderation in the relationship between event centrality and PTG or resilience, both moderations were not significant (Wamser-Nanney et al., 2017). These were in contrast to the negative relationship between event centrality and PWB domains (except positive relations), which were specifically moderated by sexual trauma (Wamser-Nanney et al., 2017). The use of these three variables as adaptive or mental health outcomes requires noticing the clear conceptual differences that have been demonstrated.
The third is the concern for intrapersonal qualities as growth outcomes, such as specifically academic pursuit or broadly the achievement of a decent identity. The academic pursuit as an indication of growth includes successful and high-functioning higher education attainment (Breech, 2021; Ningabire, 2021). The achievement of a decent identity includes the acquisition of young adulthood milestones, such as independent living skills, employment, higher weekly income (Oshri et al., 2018), identity transformation for the better than how they were (Aparicio et al., 2014), and turning point in life (Ross, 2013). These outcomes can be the embodiment of the new role(s) assigned to individuals, as presented in the latter theme. Finally, two other studies simply clarify the outcomes of PTG by domains, i.e., personal strengths and spiritual changes (Copley, 2015) and appreciation of life and new possibilities (Shuwiekh et al., 2018). Referring to the PTG domains, the outcomes do not yet include the interpersonal functions as explained below (see the last sentence of the sub-theme regarding interpersonal matters).
The Role of Interpersonal Matters
Studies that involve interpersonal matters in their design either as predetermined variables or as outcomes, are quantitative (Addante, 2020; Copley, 2015; Girresch, 2018; Hosey, 2019; Mohr & Rosén, 2017; Oshri et al., 2018; Santoro, 2017; Schaefer et al., 2018; Vartanian et al., 2014), qualitative (Aparicio, 2014; Breech, 2021; Ross, 2013), and mixed-methods studies (Ningabire, 2021; Saint Arnault & Sinko, 2019). The terms used to represent the role of interpersonal matters can refer to factual experiences with passive tendencies, psychological internal experiences related to social experiences, outcomes with active tendencies, or simply general terms. The terms that refer to factual experiences with passive tendencies, meaning that individuals receive and perceive their history or current state of social interactions, i.e., early social relations (Oshri et al., 2018), history of primary attachment (Girresch, 2018), social support (Addante, 2020), family support (Schaefer et al., 2018), emotional support, prosocial adult presence (Mohr & Rosén, 2017), attachment with an adult (Breech, 2021), enduring family (Aparicio, 2014), and relationship types (Copley, 2015). The other terms that refer to psychological internal experiences related to social experiences which may be attributed as inhibiting and/or supporting experiences, i.e., lingering feelings regarding family breakdown (Aparicio, 2014), pervasive insecurity in social attachment (Ningabire, 2021), acceptance of parental limitations (Ross, 2013), anger expression (Santoro, 2017), self-esteem and shame (considering how others’ views also impact these variables; Hosey, 2019), trust (Breech, 2021; Saint Arnault & Sinko, 2019), and school engagement (Oshri et al., 2018). The other terms that refer to outcomes with active tendencies specifically refer to being sociable and socially skilled, i.e. being in community (Breech, 2021), having better interpersonal skills (Ross, 2013), relating to others (Copley, 2015), social engagement (Saint Arnault & Sinko, 2019). Meanwhile, the more general terms which allow for both passive and active tendencies, i.e. interpersonal resources (Vartanian et al., 2014; an aggregate of gratitude and social support) and social capital (Oshri et al., 2018).
There are several ways to describe the overall results of studies. First, highlighting the negative role of interpersonal matters. Risky social relationships (from family, i.e., harsh or physical abusive discipline; peers, i.e., peer alienation or peer relationship dissatisfaction) are negatively related to positive outcomes (Oshri et al., 2018). These negative correlations are possible as Aparicio (2014) and Ningabire (2021) stated that memories and current relationships within and outside the family were felt to be unsupportive or even disruptive so that they relied more on themselves. As a consequence, anger, fear, or even dissociation, may be experienced and tends to be expressed or experienced higher among those with more interpersonal complex trauma, thereby can finally lower existential well-being (Santoro, 2017) or mess with identity and overall sense of self (Breech, 2021). Second, highlighting the absence of the role of interpersonal matters, where individuals find it difficult or unable to value social relationships as supporting given the history or current state of social pressures (as indicated just now), while strengthening self-reliance over time. A history of primary attachment trauma (Girresch, 2018) and family support (together with other variables; Schaefer et al., 2018) are unable to predict PTG—in contrast to family support’s predictability for higher resilience (Schaefer et al., 2018). Addante (2020) also observed that social support did not distinguish latent classes of psychological distress and PTG. Meanwhile, in contrast to the role of risky social relationships from family and peers, positive outcomes are barely observed to be negatively correlated with dangerous communities or unsafe neighborhoods (i.e., the presence of assaults and muggings, delinquent or drug-involved gangs, and open drugs use or dealing; Oshri et al., 2018). However, Oshri et al. (2018) observed that those who experienced the highest community disorganization in their early teens, had low future orientation but then increased gradually, and reached young adulthood milestones better than those who had a high start/decreasing future orientation growth pattern.
Third, highlighting the supporting role of positively-atributted interpersonal matters. This indicates hope beyond what was observed in the second highlight where emotional support is positively related to PTG, as well as prosocial adult presence moderates the relationship between childhood maltreatment and PTG (Mohr & Rosén, 2017). There were also observed in qualitative studies, namely the important role of attachment with an adult (i.e., special adults as proxy parents who provide emotional support and encourage goal setting for college; Breech, 2021) and enduring family (i.e., extended family members as guardians who take over the role of caregivers from the nuclear family; Aparicio, 2014). Psychological constructs as consequences of being socially engaged, such as self-esteem and shame are also associated with negative self-evaluation which actually encourage PTG (Hosey, 2019), interpersonal resources including gratitude is positively correlated with personal growth (Vartanian et al., 2014), while school engagement is positively correlated with positive outcomes, especially and persistently with employment (Oshri et al., 2018). Here, the individuals have confidence to sinergize the socially supporting or even suppressing matters as part of efforts to achieve positive outcomes. For instance, as Ross (2013) observed, individuals can move on to having better interpersonal skills due to acceptance of parental limitations. Saint Arnault and Sinko (2019) also observed that finding voice is realized by engaging in feminist work as a means of defending oneself and fighting social injustice. They added that social engagement can then be obtained through helping others, feelings of belonging, seeking universality, and building trust.
Fourth, highlighting combined roles and more elaborated dynamics. Early adverse experiences are negatively related to both interpersonal and intrapersonal resources—including personal growth initiative (Vartanian et al., 2014). However, the more complex results from structural equation model regarding interpersonal and intrapersonal resources on psychological symptoms are represented in the final sub-theme (Vartanian et al., 2014). It has also been reported, not partially but in combination, that social and emotional resources jointly moderate the relationship between childhood maltreatment and PTG (Mohr & Rosén, 2017). Fifth, more elaborated dynamics can also be observed through mixed findings. Copley (2015) explained that attachments were actually related to PTG based on relationship types, from uncorrelated (romantic partner), positively correlated (with mother), partially positive (with father), to negative (close platonic relationship/close friend). While consistent with that, Schaefer (2018) explained that social support specifically obtained from family instead of friends had a positive bivariate correlation with PTG. This important role of the family is actually in accordance with Ningabire (2021) and Ross (2013) who discussed the dynamics of interpersonal pursuit with contrasting cases as presented in the latter sub-theme, namely that individuals will distance themselves from their dysfunctional families and choose to build strong relationships outside their own families. The dynamics of the cases from Ningabire (2021) and Ross (2013) which highlight the important role of dysfunctional families are explained in other themes. Sixth, simply indicating growth outcomes, i.e., social capital, including the number of people who can be relied on in meeting needs and solving problems (Oshri et al., 2018), and social skills (Breech, 2021; Copley, 2015; Ross, 2013; Saint Arnault & Sinko, 2019).
The Role of Negative Issues
The Role of Psychological Distress or Disorder
The presence of psychological distress or disorder despite indications of growth may be identified through quantitative studies using self-report questionnaires particularly using cross-sectional designs (Addante, 2020; Hosey, 2019; Oshri et al., 2018; Saint Arnault & Sinko, 2019; Sheline, 2013; Shuwiekh et al., 2018; Vartanian et al., 2014; Wamser-Nanney et al., 2017), as well as a qualitative study through experiences of access to mental health services (Ross, 2013). Psychological distress and disorders are mostly internalizing, i.e., trauma symptoms (Oshri et al., 2018), posttraumatic stress disorder (Addante, 2020; Saint Arnault & Sinko, 2019; Shuwiekh et al., 2018; Wamser-Nanney et al., 2017), complex posttraumatic stress disorder (Shuwiekh et al., 2018), depressive symptoms (Addante, 2020; Hosey, 2019; Ross, 2013; Saint Arnault & Sinko, 2019; Wamser-Nanney et al., 2017), anxiety symptoms (Addante, 2020; Saint Arnault & Sinko, 2019), somatic symptoms (Saint Arnault & Sinko, 2019), and disordered eating behavior (Vartanian et al., 2014). Meanwhile, Oshri et al. (2018) also used phrases with a broader scope, i.e., psychopathology, internalizing and externalizing symptoms, using different measurements. In addition, sucide risk as an indicator is also examined (Sheline, 2013).
First, there are positive correlations between PTG or growth-related constructs and psychological distress or disorder—indicating possible coexistence. PTG is positively correlated with posttraumatic stress disorder (Saint Arnault & Sinko, 2019; Wamser-Nanney et al., 2017), depression, anxiety, and somatic symptoms (Saint Arnault & Sinko, 2019). Meanwhile, among all the positive outcomes measured by Oshri et al. (2018), only independent living skills are positively correlated with trauma symptoms. In addition to positive correlations, the coexistence is also recognized through the experiences of access to mental health services, such as efforts to treat depression that may still be experienced by some survivors, but hope prevails to create new worlds for themselves (Ross, 2013). The Ross’s study (2013) also demonstrates that access to mental health care can be done if needed. This is described further in the next theme.
Second, on the contrary, negative correlations indicate that coexistence is impossible. Wamser-Nanney et al. (2017) observed that PTG was negatively correlated with depression, contrary to Saint Arnault and Sinko (2019). Likewise, observations by Oshri et al. (2018) also contradicted that all positive outcomes were negatively correlated with internalizing symptoms, whereas employment was the only positive outcome that was negatively correlated with all psychopathology (i.e., internalizing, externalizing, and trauma symptoms) despite the very small effect sizes. The impossible coexistence is also observed through mediation tests where low levels of PTG or other growth-related constructs as a result of high levels of complex trauma actually correlate with high levels of psychological distress or disorder, i.e., the increase in mental health syndromes (posttraumatic stress disorder, complex posttraumatic stress disorder) through a decrease in PTG (Shuwiekh et al., 2018), and the emergence of disordered eating behavior (binged, purged and restricted eating) through a decrease in personal growth initiative (combined with self-esteem as intrapersonal resources; Vartanian et al., 2014). Finally similar to the mediation studies, a moderation study also shows impossible coexistence, i.e., PTG moderates the relationship between the severity of traumatic events and suicide risk (Sheline, 2013). The results also suggest potentially higher levels of PTG among those who have experienced the most severe traumatic life events, and thus are less at risk for suicide.
While distinct results have been described between studies, the third description points more varied results in each of some studies. A study by Hosey (2019) implied that those with ACEs and depressive symptomatology would show variations in PTG—certain characteristics (e.g., self-esteem and sense of self) might influence. In addition, variations in latent classes were also observed by Addante (2020) according to the degree of PTG and psychological distress, and by Oshri et al. (2018) according to growth patterns of future orientation—positive outcomes and psychopathology are then compared between classes. Oshri et al. (2018) also observed mixed results from bivariate correlations—which have been mentioned separately above as positively and negatively correlated, or uncorrelated. Other results are also reported that only externalizing symptoms (of all the psychopathology measured) barely correlate with any positive outcomes.
All the descriptions indicate that psychological distress or disorder—which internalizing types tend to be widely researched—may exist even as survivors grow and achieve milestones. Externalizing symptoms along with growth have been little investigated in this context, as just mentioned in the study by Oshri et al. (2018) with almost no correlation between externalizing symptoms and positive outcomes. Only Vartanian et al. (2014) offer a specific behavioral disorder (although still considered an internalizing symptom, i.e., disordered eating behavior), in which coexistence is impossible. A result may also only validate certain indications of growth in association with certain types of psychological distress or disorder (e.g., Oshri et al., 2018). Conversely, individuals may not thrive and only experience distress or disorder. Besides other possible explanations for the varying results, the use of different concepts and instruments is clearly also a consideration. For example, measuring depression using the Patient Health Questionnaire-8 (PHQ-8; by Saint Arnault & Sinko, 2019) versus the Center for Epidemiological Studies Depression Scale (CES-D; by Wamser-Nanney et al., 2017).
The Role of Problems/Conflicts
Some studies identify problems/conflicts—but not necessarily related to psychological distress or disorder—that are experienced despite growing. Those studies show the depth of methods for understanding experiences i.e., through longitudinal, qualitative, and mixed-methods studies (Aparicio, 2014; Breech, 2021; Ningabire, 2021; Oshri et al., 2018; Ross, 2013; Saint Arnault & Sinko, 2019). Other studies use cross-sectional quantitative methods and explicitly mention the problems/conflicts encountered as positively correlated and potentially coexistent (Copley, 2015; Hosey, 2019; Jirek & Saunders, 2018), or negatively correlated (Santoro, 2017; Vartanian et al., 2014) with growth-related constructs. In addition, a quantitative study clarifies the moderating role of PTG in mitigating potential conflict (Sheline, 2013).
Problems/conflicts can be described in general, including impacts (Copley, 2015) or negative impacts (both interpersonal [e.g., mistrust, peer comparison, difficulty setting boundaries] and intrapersonal [e.g., rumination, hopelessness]; Saint Arnault & Sinko, 2019), and current life events or chronic stressors (Jirek & Saunders, 2018). Problems/conflicts can be interpersonal with regard to relational tensions/capacity in relationships (Ningabire, 2021; i.e., the emotional fallout in the family and recent intimate relationship problems [Ross, 2013]). In contrast, those problems can also be intrapersonal with regard to mental functioning processes both cognitively (i.e., shame-negative self-evaluation [Hosey, 2019]) and emotionally (i.e., disturbing strong emotion [Ross, 2013]; darkness and despair [Aparicio, 2014]). Behaviors can also be their forms, i.e., sexual and drug or addictive substance use (Ningabire, 2021; Oshri et al., 2018), including those that explicitly connect the risks to physical health problems (Santoro, 2017; Vartanian et al., 2014). As a consequence, involvement with public service institutions is also possible, whether in the area of education/college (Sheline, 2013), physical health (Santoro, 2017), mental health (Ningabire, 2021), law (Oshri et al., 2018), or social welfare (Aparicio, 2014; Breech, 2021). Eventually, relatively chronic socioeconomic status as evidenced by poverty, homelessness, multiple placements, and living in a foster care—which also represent complex trauma experiences—are also part of the problems (Aparicio, 2014; Breech, 2021).
Problems/conflicts are actually more common when the presence of psychological distress or disorder cannot yet be decided, as observed by Saint Arnault and Sinko (2019), the syndromes were evaluated in the study. However, these can gradually increase in severity to the point that access to mental or physical health or welfare services is required (Aparicio, 2014; Breech, 2021; Ningabire, 2021; Santoro, 2017) or an arrest is made (Oshri et al., 2018). The problems/conflicts may coexist with indications of growth along with access to these public service institutions. For example, those with USE without or with CSA utilizing the services of the university health care system (sexual assault center) also have higher PTG, especially those with CSA (Saint Arnault & Sinko, 2019), as well as those with higher levels of independent living skills (as a positive outcome) tend to have either more intense or frequent sexual behavior, drug use, or arrests (Oshri et al., 2018). The dynamics may result in discouragement (for example with the failure of child welfare services [Breech, 2021]), avoidance or discontinuation of services (i.e., counseling and psychotherapy [Ross, 2013]), or repeated/multiple institutionalization (i.e., arrests [Oshri et al., 2018]; placements [Aparicio, 2014; Breech, 2021]).
The studies that suggest the negative relationship between growth-related psychological constructs—besides PTG—and health-related behavioral problems through mediation are conducted by Santoro (2017) and Vartanian et al. (2014). Santoro (2017) observed that the decrease in existential well-being and the increase in health disparities were associated with the increasing severity of childhood adversity through the mediation of religious/spiritual struggles and unhealthy ways of expressing anger. Similarly, Vartanian et al. (2014) also observed that body dissatisfaction and poor exercise increased with the increasing severity of early adverse experiences through the mediation of low personal growth initiative and impaired self-esteem. The dynamics become complicated when the mechanism of suppression effects was proposed by Vartanian et al. (2014)—explained in the latter sub-theme. Nevertheless, despite all the problems/conflicts that survivors may face, the adjustment of those who study at college and have experienced PTG following their trauma, will be easier (Sheline, 2013).
The Role of Challenging Adjustments
The Role of a New Role(s)
Some studies clearly show the existence of new role inducements (Aparicio, 2014; Breech, 2021; Hosey, 2019; Ningabire, 2021; Oshri et al., 2018; Ross, 2013; or implicitly, for example by Vartanian et al., 2014) which can be divided into three categories. First, normative new role inducement which is simply challenged by identity development, namely generally regarding young adult developmental milestones, and specifically regarding sense of self, self-esteem and body esteem. Passing through adolescence, individuals should ideally be able to see the future as having many different possible directions for identity development, achieving milestones healthily. Oshri et al. (2018) indicated the milestones in young adulthood as positive outcomes, namely independent living skills, social support and capital, income, and employment. How maltreated youth become in young adulthood is observed by considering the growth pattern of future orientation, protective and risk factor indices during their youth (Oshri et al., 2018). Meeting milestones, even based on normal young adult standards, can be highly difficult for survivors of complex trauma, for example those living in foster care (Aparicio, 2014; Breech, 2021). Consequently, they will not have a sense of self and feel unable to see the available options, experiencing identity instability due to ACEs (Hosey, 2019). Identity instability is very likely to occur and greatly lowers self-esteem (Hosey, 2019). In a negative case among emerging adult survivors, interpersonal resources that should have positive effects on health and mood, preventing body dissatisfaction (indicating low levels of body esteem) can actually become risk factors (Vartanian et al., 2014). Therefore, psychological disorders may be experienced (Vartanian et al., 2014). The mechanism is explained in the following sub-theme.
Second, new role inducement may be normative depending on psychosocial backgrounds. In this case, the new role is controllable as long as it is supported by the individual’s psychosocial background and indicates the ability to choose independently to complete it as the individual grows. Individuals may be confronted with the challenges that are very likely due to their adversity experiences. Education, for instance, is normative for the population at large. But this may be a privilege for some underrepresented populations, unless they then have the resources, and therefore have the control to choose and complete it well. Those who live in foster care, for example, may be discouraged because caseworkers dismiss the idea of going to college (Breech, 2021). Full functioning in the academic field among those populations becomes possible, such as a successful attainment of a post-secondary education in a population of former foster youth after having aged-out of the child welfare system (Breech, 2021), well-educated and high-functioning of college students who had witnessed community violence and suffered emotional abuse, physical abuse, and neglect (Ningabire, 2021). The moderating role of PTG in the relationship between severity of traumatic life events and college adjustment (Sheline, 2013), has been described in the previous sub-theme.
Third, new role inducement which is non-normative and uncontrollable. People at certain developmental periods will experience normative life events, accept and perform similar tasks and social expectations. Those who struggle with childhood adversities and consume adult responsibilities at early ages (experience stolen childhood and role reversal) are the exception, such as caring for siblings or earning income to support their families during childhood and adolescence while living in a chronically chaotic family (Ross, 2013), caring for and replacing the role of the sick parent, protecting parent from the abusive one and then being abandoned for criminal offenses (Breech, 2021), as well as getting pregnant and being a teen mother in foster care, and haunted by past diverse adversities (Aparicio, 2014). The individuals are able to take control as they undergo the healing process and grow. Similar to the previous one, this description also demonstrates that the complex trauma itself may inflict non-normative new roles, thus requiring challenging adjustments.
The Role of Flexible Coping Strategies
Some studies may explicitly concern with certain coping strategies separately or together—as presented in the second theme regarding the role of resources—without really considering the possible flexibility. In fact, there is bargaining over coping strategies in the healing process and growth in the context of adversity. Strategies for dealing with these problems, perhaps initially or continuously—as individuals are still in the healing process—involve exhausting strategies. The coexistence described in the third theme confirms the importance of coping flexibility. Saint Arnault and Sinko (2019) explained the importance of sharing greater negative impacts, i.e., less denial and conversely higher event centrality, thus allowing for more intense conflicts. Those in such conditions are observed to have a lower sense of coherence and self-compassion but higher PTG (Saint Arnault & Sinko, 2019). Saint Arnault and Sinko (2019) added that finding escape but staying active to engage the body or mind is also a strategy, before dealing with the symptoms and bravely going through the discomfort. Another mechanism, Hosey (2019) explained that increased complexity was followed by increased identity instability which was further associated with lower self-esteem and higher shame. Those who show shame-negative self-evaluation actually have higher PTG (Hosey, 2019).
On the other hand, a negative case related to low levels of body esteem indicated by body dissatisfaction has previously been mentioned (Vartanian et al., 2014). This case is the opposite of what is expected in this sub-theme, where ‘inflexibility’ occurs apparently due to preoccupation and is detrimental. Expectedly, body dissatisfaction is negatively predicted by either intrapersonal resources (i.e., personal growth, self-esteem) or interpersonal resources (i.e., gratitude, social support). Unexpectedly, joint examination of both resources results in interpersonal resources having a positive effect on body dissatisfaction, while intrapersonal resources still have a negative effect (Vartanian et al., 2014). Vartanian et al. (2014) argued that the mechanism of suppression effects of intrapersonal resources on interpersonal resources afterwards have negative impacts, where the individuals’ remaining concern is how others view them hence worrying about their body appearance. This is what is then able to predict disordered eating behavior while still having low intrapersonal resources, or coexistence is impossible.
Flexible and adequate coping is indicated by the individuals’ functioning, intrapersonally and interpersonally, but at a cost. The impact of complex trauma as in one’s family is massive and may still be faced or repeated. However, they choose a better life. Ross (2013) observed that besides intrapersonal, interpersonal pursuits might have been achieved but not with their immediate family, since they still retained intrusive memories of abuse. Instead, Ningabire (2021) explained the importance of overcoming interpersonal conflicts and tense relationships by self-distancing from strong disturbing emotions, even avoiding emotional attunement, self-compassion, and self-soothing because of the need to be strong so problems did not affect the individual. After all, Ross (2013) demonstrated that those with childhood adversities were able to develop a healthy resistance to the impacts of past experiences and turning point in life, through academic success, extracurricular activities, writing and creative pursuits. Their interpersonal pursuits were also powerfully connected, emotionally sustaining and adaptive. Similarly, Ningabire (2021) suggested that apart from trust issues and discomfort with emotional vulnerability, survivors experienced success in academics, felt pride regarding their accomplishment, but also engaged religiously, had faith and prayed. Although religious strategies are acknowledged to be able to foster hope, Ningabire (2021) observed that hope was still higher among those with less adversity experiences.
Social support (and/or system support) can be influential as relatively consistent experiences rebuild trust, accompanying the struggle to grow. However, disappointment due to unfulfilled expectations of the social world encourages the use of alternative strategies and develops self-reliance before being part of the community. For instance, the ever-increasing hopes and dreams of teen mothers for their motherhood are greatly fostered by widening the circle of support (including extended families), thereby fighting for education but using alternative ways to finish school (including night school, online courses, summer school) to add time with their young children at home (Aparicio, 2014). Meanwhile, Breech (2021) concluded that transcending poverty, including self-redemption and gaining an image of success, can be confronted with system failures at various levels from families, schools, communities, to child welfare services. However, despite the possible mental health problems, survivors channel their creativity in various outlets to feel joy and freedom, learn about life from reading, imitate the good things they have observed. The greater the fear, the greater the reliance on self. Compared to the perceived failures of the systems, there may be a slight emotional support from the presence of special adults as proxy parents. Once they are set, they rebuilt their communities.
Meta-Analysis
Mean Score of Complex Trauma
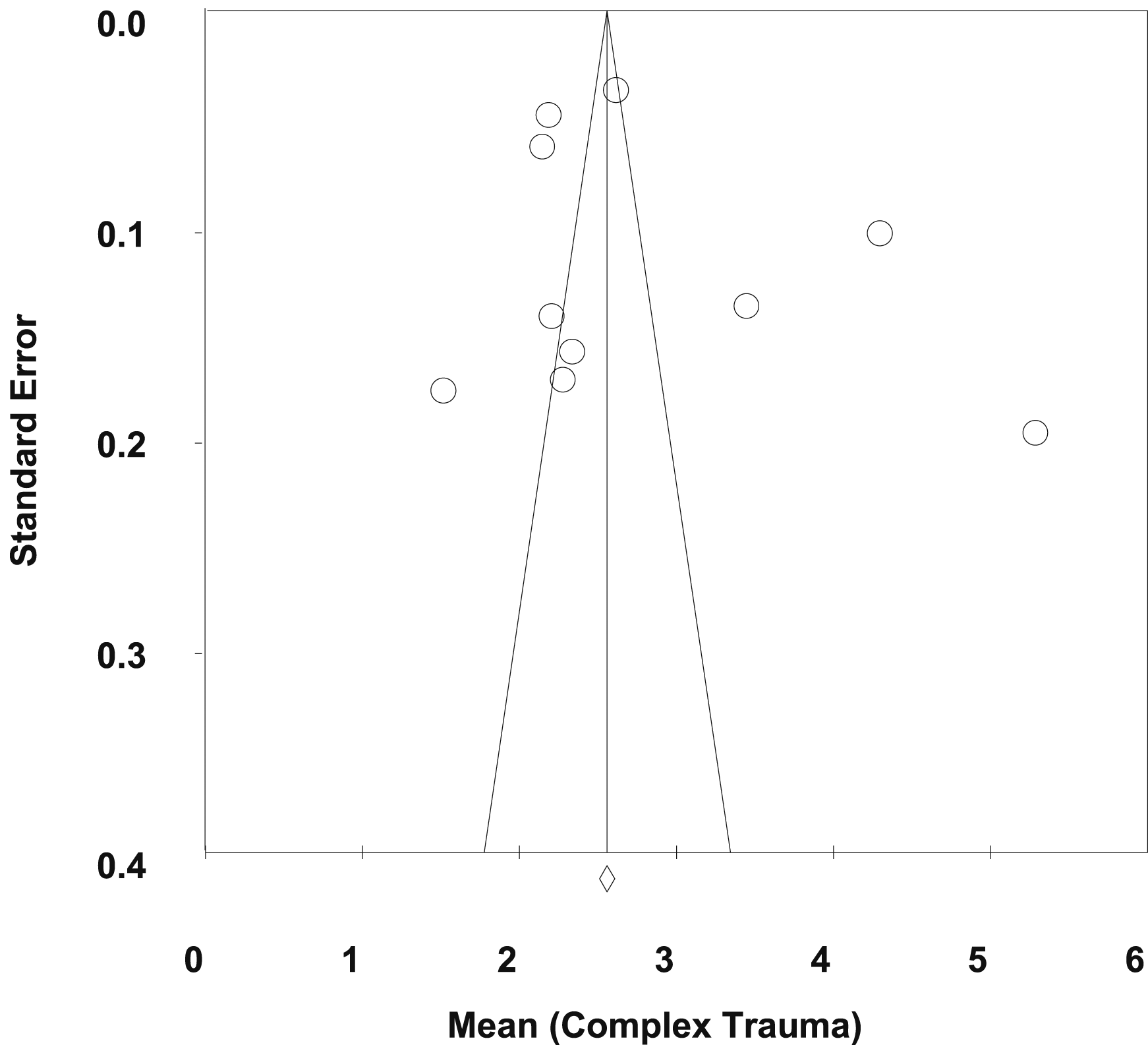
Meta-analysis on complex trauma data (see Table 2) yielded high heterogeneity (Q = 632.930; df = 9; p < .001; I
2
= 99%) hence the random effect model was used. Figure 3 shows that the mean effect size was 2.83 (z = 12.203; p < .001; 95% CI; 2.37–3.28), which means that the majority of study participants in this meta-analysis had at least two types of ten complex traumas. Publication bias was not identified due to obtained symmetry funnel plots (see Figure 4, Kendall’s τ = .111, p = .655) and insignificant Egger’s test (t = 0.909, p = .390), with a large number of studies in Fail-safe N (of 1537). The forest plot of meta-analysis of the complex trauma mean. The funnel plot of standard error with 95% CIs by complex trauma mean.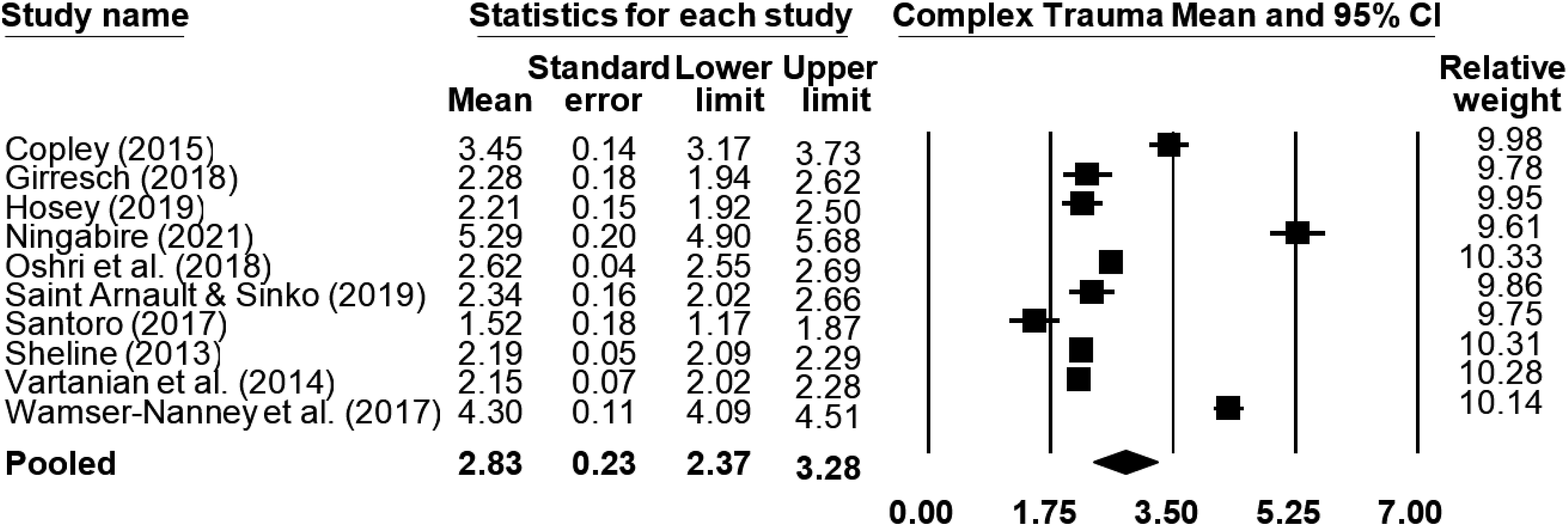
Mean Score of PTGI
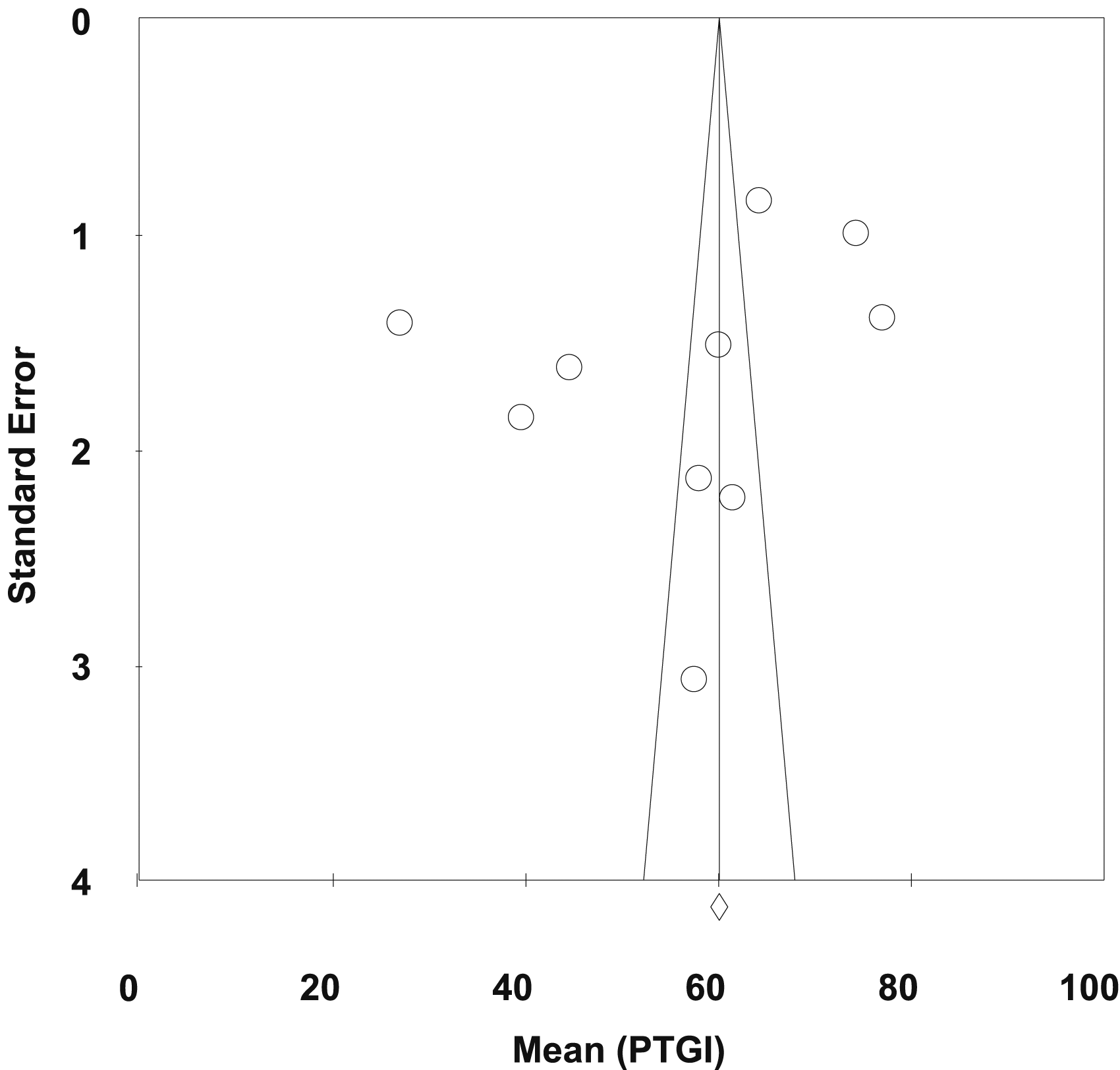
Meta-analysis on PTGI data (see Table 2) yielded high heterogeneity (Q = 1133.646; df = 9; p < .001; I
2
= 99%) hence the random effect model was used. Figure 5 shows that the mean effect size was 56.37 (z = 10.876; p < .001; 95% CI; 46.21–66.53), which means that the majority of study participants in this meta-analysis had PTG above the hypothetical mean score, namely 52.5. Publication bias was not detected due to obtained symmetry funnel plots (see Figure 6, Kendall’s τ = The forest plot of meta-analysis of the PTGI mean. The funnel plot of standard error with 95% CIs by PTGI mean.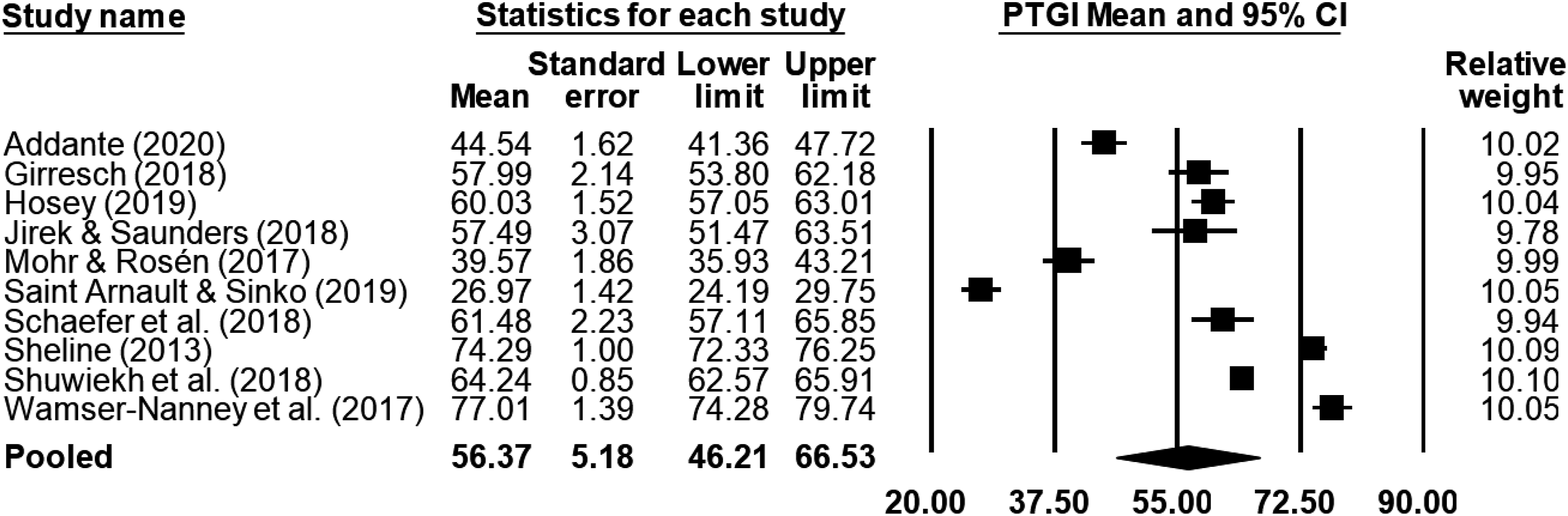
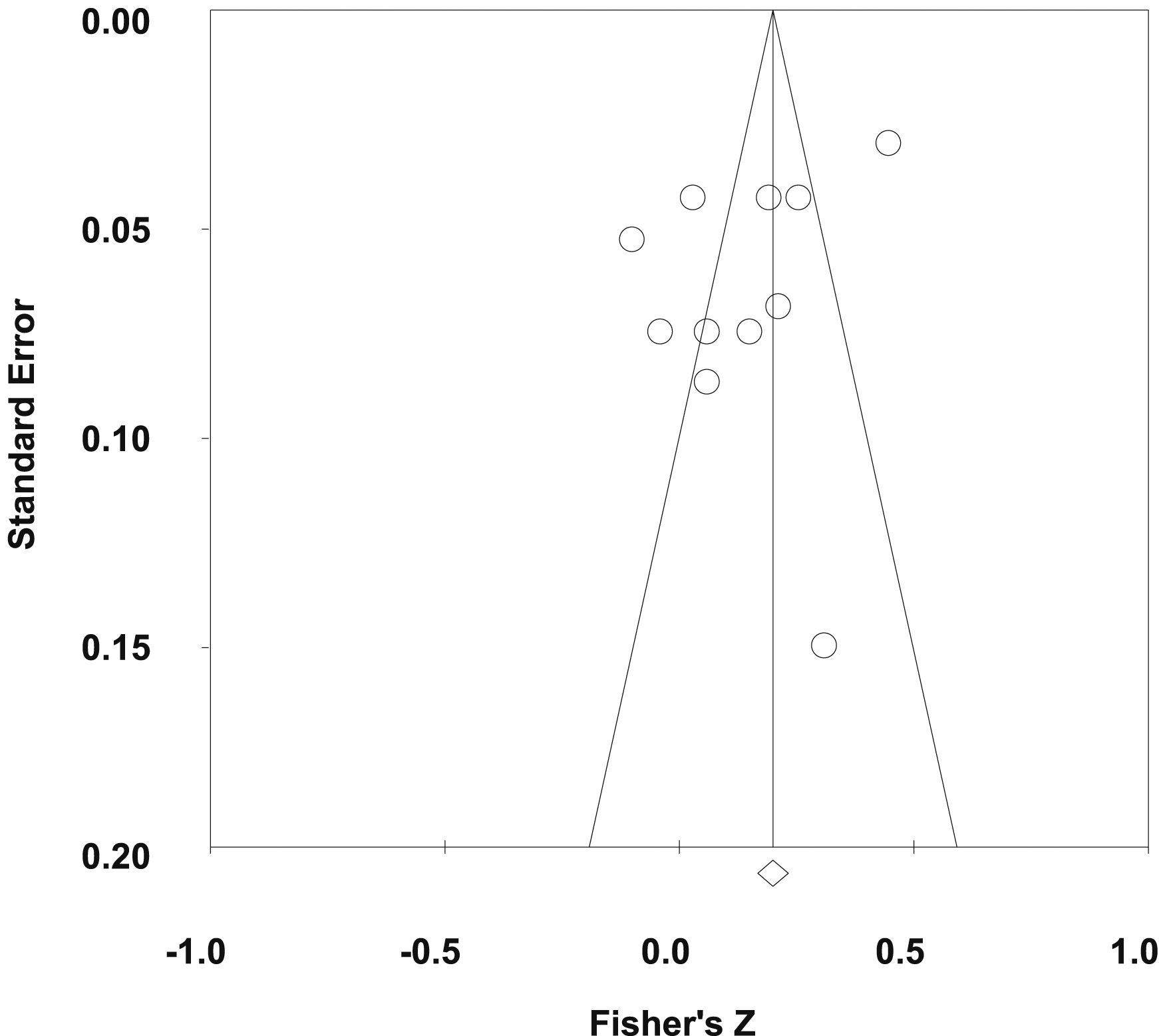
Correlation Between Complex Trauma and PTGI in Emerging Adults
Table 2 shows seven of the eleven articles using PTGI and provides eleven effect sizes of correlations between complex trauma and PTG. Each of two studies (Schaefer et al., 2018; Sheline, 2013) contributed three effect sizes. The random effect model was used given the high heterogeneity (Q = 121.580; df = 10; p < .001; I
2
= 92%). Figure 7 shows that meta-analysis yielded a positive and significant weighted mean effect size of .14 (z = 2.331; p = .020; 95% CI; 0.02–0.26), which means that an increased number in history and severity of complex trauma is followed by an increased PTG in emerging adults with a low pooled effect of 14% (Cohen, 1992). Publication bias was not detected due to obtained symmetry funnel plots (see Figure 8, Kendall’s τ = The forest plot of meta-analysis of the correlation between complex trauma and ptg. The funnel plot of effect sizes and standard error with 95% CIs by Fisher’s z of the correlation between complex trauma and PTG.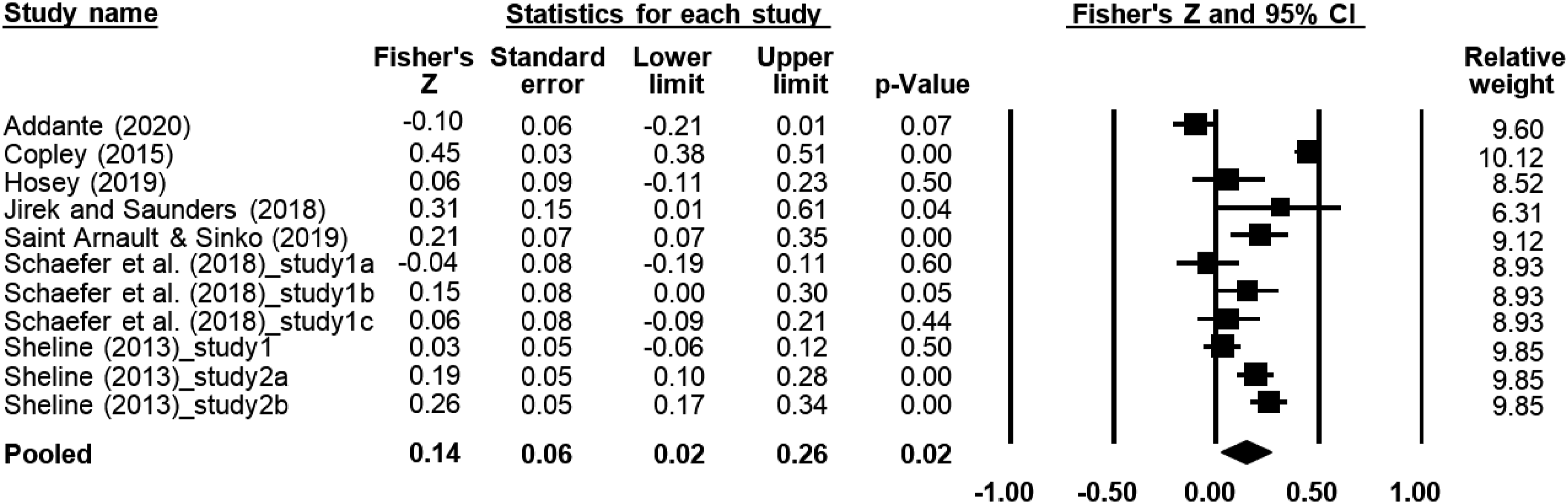
We highlight the need for caution in interpreting the results of meta-analyses. Despite the high heterogeneity in the meta-analyses of this current systematic review, subgroup analyses could not be performed either for subsets of participants (e.g., males and females), or for subsets of studies (e.g., different geographical locations) (Higgins & Thompson, 2011). The moderator checking both within-study and between-study concluded the diversity of data but it was difficult to correspond between studies while raw data was also not available (Cooper, 2017). Taking into account the high heterogeneity, on the other hand it is not yet possible to carry out subgroup analyses, the results of the meta-analyses will be unreliable and should be interpreted with caution (Melsen et al., 2014). Despite the conditions, these results shed light that researchers still have a lot of work to do and therefore further studies need to be carried out in terms of psychological growth among emerging adults, especially those who survive complex trauma as underrepresented populations.
Discussion
The aim of this study was to understand the association beween complex trauma and growth-related psychological constructs among emerging adult survivors. To be able to achieve it, a narrative synthesis of 18 studies and meta-analyses of 10–11 effect sizes were conducted. The narrative synthesis produced four major themes, namely, the role of traumatic experiences, the role of resources, the role of negative issues, and the role of challenging adjustments. The meta-analyses resulted in 2.83 out of 10 of a weighted mean of complex trauma and 56.37 of a weighted mean of PTGI (above the hypothetical mean score), as well as 14% of a low pooled effect between the two variables. However, the studies included in the review were varied. Therefore, attention to their each peculiarity needs to be done to gain a comprehensive but contextual understanding of emerging adults and complex trauma experiences. Thus, the variations of the studies so far, even contradictions, become acceptable. As the result of low weighted correlation with high heterogeneity, the presence of other diverse moderating factors needs to be considered.
This review considers growth outcomes after experiencing complex trauma in the second theme, whether attributed to intrapersonal or interpersonal qualities. Since the PTG concept was developed by Tedeschi and Calhoun (1996), it has been defined through its domains which include relating to others, new possibilities, personal strengths, appreciation of life, and spiritual changes (the latter was later refined to spiritual and existential changes; Tedeschi et al., 2017). These PTG domains were used as references to be examined separately, rather than in aggregate, in a small number of studies (Copley, 2015; Shuwiekh et al., 2018). Apart from the domains conceptualized as PTG, the systematic search obtained some studies that specified manifestations of growth or positive changes as participant criteria such as the achievement of a decent identity (Aparicio et al., 2014; Ross, 2013) and specifically education (Breech, 2021; Ningabire, 2021). The specific achievements, and how these become turning points in life, are in accordance with the assertion of Tedeschi et al. (2018) that PTG can occur even in one domain but is significant for individuals. This argument later becomes a possible reason why the results are dynamic and the healing process among survivors is important to consider.
Those outcomes in this review are explained as manifestations of new role inducements (see theme four), whether they are normative, ‘conditionally’ normative, or non-normative. Whatever the type, they are important to challenge psychological growth, boost mastery of new roles despite the conflict/burden borne (Aparicio, 2014; Breech, 2021; Ningabire, 2021) and contribute to increasing competence (Ross, 2013). The first and second types of new role inducements that are basically normative, such as young adulthood milestones (Oshri et al., 2014) and identity development (Hosey, 2019; Vartanian et al., 2014), are actually in line with the features of emerging adulthood even though the burden of the new role among survivors of complex trauma is sometimes extremely non-normative. Instead, the non-normative one can be ‘normative’ for emerging adult survivors of complex trauma, whose adversity experiences commonly result in them having their childhood stolen and experiencing role reversal (Aparicio, 2014; Breech, 2021; Ross, 2013). These rationales have not been accompanied by reviews of how massive the impacts of complex trauma are. That is why achieving milestones and identity in young adulthood in this context may be equivalent to PTG. As defined by Tedeschi et al. (2018), PTG is the ability to find strength, not only to bounce back from the adversity experiences, but to realize beyond what has previously been taken from individuals.
Ignited by the role of new role inducements, the results of this review confirm that PTG is not as simple as realizing outcomes as described in its domains. This impermissible simplification is still in line with the model of Tedechi et al. (2018). However, before going any further, distinguishing PTG from other growth-related psychological constructs (i.e., personal growth initiative, well-being) is relevant and important since this review suggests that the results of their studies have been less congruent. The outcome-focused concept of PTG is the most likely reason to differentiate it from other growth-related psychological constructs, such as personal growth initiative (Tedeschi et al., 2018). This is supported by Robitschek (1998) who concluded that personal growth initiative (containing four subscales, namely readiness for change, planfulness, using resources, intentional behavior) is the active and deliberate involvement of individuals in the personal growth process, rather than outcome. Roepke (2020) explained that when growth is interpreted as a process, it will actually be in line with meaning-making coping or positive reappraisal coping.
Meanwhile, well-being in this case PWB (comprising six elements, namely self-acceptance, purpose in life, environmental mastery, positive relationships, personal growth, and autonomy; Ryff & Singer, 2008) which is equated with eudemonic well-being, has more conceptual closeness to PTG than hedonic well-being/subjective well-being (Tedeschi et al., 2018). However, PTG and PWB are considered different constructs and cannot be used interchangeably because the PWB measurement is more general rather than specific to adjustment following highly stressful traumatic events (Tedeschi et al., 2018). This is actually in accordance with Ryff (1989) that the measurement construction of PWB is based on the construct-oriented approach to personality assessment. Additionally, Tedeschi et al. (2018) added that instead of emphasizing perceived benefits (as in terms of measuring the concept of existential well-being proposed by Ellison (1983), including life direction and life satisfaction), PTG goes beyond individuals’ previous level of adaptation, psychological functioning, or life awareness.
Equally important is distinguishing PTG from resilience, as this review observed that both variables are used as indications of adaptive and mental health outcomes along with PWB (Schaefer et al., 2018; Wamser-Nanney et al., 2017). However, as will be noted later, resilience is emphasized more than PTG in the emerging adulthood literature (Arnett, 2024). Resilience among emerging adults seems urgent to be observed, allegedly because their identity development is challenged by toxic pressures, as experienced in the family or environment, which happen repeatedly and chronically as is common in complex trauma (Arnett, 2024). Resilience to resist trauma is more likely to be achieved through mitigating emotional distress with beliefs, which is less likely to lead to PTG (Tedeschi et al., 2018). Highly resilient people can adjust quickly and successfully, even under the most stressful circumstances. Meanwhile, PTG in this context needs to be raised because it values the willingness to struggle with challenged assumptions or cognitions due to emotional distress, and to process profound transformational changes (Tedeschi et al., 2018). This review may support the mechanism described by Tedeschi et al. that PTG benefits from event centrality while resilience does not (Wamser-Nanney et al., 2017). The role of event centrality is particularly found in traumatic memories that are so apparent and impactful that they become highly accessible reference points for subsequent experiences, thus potentially turning points in one’s life (Berntsen & Rubin, 2007). This review indeed observed a positive correlation between resilience and PTG in two studies (Schaefer et al., 2018; Wamser-Nammey et al., 2017), but varying correlations may be found in other studies. In some cases, the participants with higher resilience may actually not grow because they maintain their status quo but distance themselves from growth efforts (Levine et al., 2009). After all, appropriate distancing in certain studies also seems to protect one’s self when confrontation is too overwhelming and encourage psychological growth where self-reliance is ultimately accentuated (Ningabire, 2021).
Despite the well-known outcome-based PTG concept, Tedeschi et al. (2018), on the other hand, acknowledged that those outcomes are not static or in ongoing processes. They clearly proposed this in the model of PTG formation starting from highly challenging life events. We are about to comprehend the interconnectedness of all this review’s findings to confirm the process. The ongoing process of PTG (despite the outcomes achieved) in those who have just passed through adolescence seems increasingly reasonable when considering the nature of complex trauma (Cook et al., 2005; Courtois, 2008), its massive consequences (Cook et al., 2005; Kliethermes et al., 2014, Shonkoff & Garner, 2012) and long-term impacts (Borgese, 2019). In response to this, Tedeschi et al. (2018) emphasized that PTG can be both an outcome and a process depending on where individuals are standing in time. The non-normative complex trauma experiences from childhood to adolescence and the normative new role inducements of emerging adulthood as discussed may initiate the growth process.
First, experiencing traumatic events are asserted to be necessary for PTG (Tedeschi et al., 2018). Centrality of traumatic events has been suggested to contribute to PTG more than to resilience (Wamser-Nanney et al., 2017) that the traumatic events are seismic, will be perceived as significant, so challenging individuals’ core beliefs that they are likely to encourage rumination as well as result in stimulating change or PTG (Boals et al., 2010; Tedeschi et al., 2018). This role of the seismic nature of complex trauma among emerging adult survivors is exhibited by Aparicio (2014) and Breech (2021), for examples, that individuals with complex traumatic experiences counteracted the excessive adverse one-sidedness created by complex trauma and perceived better opportunities. Meanwhile, from a developmental perspective, emerging adults are generally characterized by a feature where possibilities are highlighted, including those who have grown up in difficult conditions (Arnett, 2024). However, this review highlights that higher psychological growth among emerging adults is actually associated with increased complexity, namely from multiple types or combinations, frequency or repetition, perceived severity, to an earlier age of trauma experience (e.g., Copley, 2015; Jirek & Saunders, 2018; Sheline, 2013). This seems to confirm the role of event centrality that the increased complexity will increase stimulation. Only one study has examined the possible curvilinear relationship between the complex trauma and PTG (Jirek & Saunders, 2018), but failed to agree with this hypothesis as in several previous studies (e.g., Kleim & Ehlers, 2009; Kunst, 2010; Lechner et al., 2003). Instead of a curvilinear relationship, we note in the third theme a possible coexistence with negative issues as PTG increases. Anyway, some studies have observed that the complexity of adversity histories can hinder opportunities to grow—which are not measured using PTGI (i.e., Ningabire, 2021; Oshri et al., 2018; Santoro, 2017; Vartanian et al., 2014). The adjustment seems challenging, includes flexible coping strategies as presented by the fourth theme. This will enrich the discussion that will be presented later.
Furthermore, the PTG domains appear to be differentially stimulated. It appears that two PTG domains (i.e., appreciation of life and new possibilities) are less supported than the other three (i.e., relating to others, personal strengths, and spiritual changes) as complexity increases (Copley, 2015; Shuwiekh et al., 2018). This is simply explained by Tedeschi et al.’s (2018) assertion that PTG may be manifested only in certain but prominent domains. However, attention based on the developmental period needs to be given. There are at least three pillars for identity development of emerging aduls that can be integrated in this discussion for now, i.e., love, ideology, and work (Erikson as cited by Arnett, 2024). First, along with PTG, meaningful relationships, especially love that ensures marriage and parenthood, may be achieved considering that toxic relationships have been consumed a lot at younger ages. Second, the same thing may happen to the pillar related to ideology which is manifested in better spiritual changes resulting from a worldview challenged by complex trauma. Third, emerging adults may develop strengths as they strive for self-reliance, but life may be underappreciated as well as opportunities may be perceived to be lacking. Whereas, possibilities are important and should characterize emerging adults. This is especially true for work that takes on much greater significance in emerging adulthood for achieving financial independence, becomes a central part of life and is desired for long-term prospects to secure life and the pillar of love. Future studies could deepen the examination of the role of trauma complexity across domains among emerging aduls and compare the possible differences based on developmental period, such as older or even younger (i.e., adolescence).
Not yet finished with the above homework, we face another challenge, namely the possible differences in the direction of the correlations. For instance, complexity as a consequence of the age of traumatic experiences still indicates contradiction in its role for PTG (Jirek & Saunders, 2018; Shuwiekh et al., 2018). Correspondingly according to Shuwiekh et al. (2018), differences in PTG could be determined by the trauma types, where complex trauma is less stimulating than single or secondary ones. Furthermore, challenges also come from the role of complex trauma events experienced. There are various types of complex trauma, but this review suggests that they have not been widely observed in this context, let alone studied with a longitudinal design and with repeated measurements. Intrapersonal complex traumas appear to be a more central topic in studies than non-interpersonal traumas, presumably because they are more common. Cumulatively, the correlation between interpersonal complex trauma and PTG is not significant (Addante, 2020), but specifically, the correlations are various. For example, the correlation is only significant with attachment trauma which is negative (Shuwiekh et al., 2018), but an aggregate score of primary attachment trauma is not able to predict PTG (Girresch, 2018). Copley (2015) might offer a solution that attachments are actually related to PTG based on relationship types. In line with the previous discussion, those contradictions might be determined by cognitive factors such as event centrality (Tedeschi et al., 2018). It can be a double-edged sword depending on how the event(s) becomes the center of the emerging adult survivor’s identity organization. Consequently, it will not have any influence, aggravate, or mitigate and encourage growth (Boals & Schuettler, 2011; Henson et al., 2021; Wamser-Nammey et al., 2017). Such complex mechanisms were also observed in this review. In addition to mixed findings, types of trauma in another study did not moderate the positive relationship between event centrality and PTG (Wamser-Nammey et al., 2017). In fact, the pre-traumatic circumstances play an important role (Tedeschi et al., 2018) but individuals who experience complex trauma at earlier ages may not have had sufficient developmental skills in their pre-trauma state. Instead, the values and beliefs that develop later and are held in emerging adulthood are the product of complex trauma.
Emerging adulthood is generally described by five main features, i.e., identity explorations, instability, self-focus, feeling in-between, possibilities (Arnett, 2024). However, this review of growth following complex trauma experiences among emerging adult survivors suggests that the hope and optimism commonly aligned with the feature of emerging adulthood may be varied and complicated. PTG has been widely researched to answer differences and correlations with many other variables in at least the last two decades. Tedeschi et al. (2018) described that the PTG model/dynamics is complicated, especially when it involves complex trauma. The complexity of the PTG dynamics among emerging adult survivors becomes increasingly apparent since that complex trauma greatly disrupts the organization of core beliefs from an early age to adolescence which is the basis for personality formation (Lawson & Quinn, 2013). They have been exposed to non-normative experiences in the form of chronic and cumulative trauma, conversely, they may also have been exposed to more normative experiences in more ideal models such as from their peers or the media. These experiences happen to varying degrees and can influence how they adopt strengths that lead to experiences of psychological growth.
The remaining themes (or sub-themes) are interrelated with those previously discussed. They need to be understood as a whole. Various characteristics that could not be controlled in this review are simply likely to be the reasons for the wide differences observed. Psychological growth as intrapersonal matters, first, highlights the role of demographic characteristics, which may be mutually confirming (e.g., Girresch (2018) and Jirek & Saunders (2018) in terms of sex not having association with PTG) but also contradictory (e.g., Girresch (2018) vs. Jirek and Saunders (2018) in terms of race/ethnic). Compared to the previously mentioned regarding complexity, two studies (i.e., Jirek & Saunders, 2018; Wamser-Nanney et al., 2017) also indicated that rather than with current age, PTG is more likely to be associated with the age at trauma. Furthermore, contrasting characteristics due to minority status of ethnicity (Girresch, 2018) and culture (Santoro, 2017) seem to have consequences for resources, resulting in increased challenges for PTG stimulation.
The next highlight relates to the growth process, involving some different variables and correlations, but in other studies there can be no correlation (e.g., Schaefer et al. (2018), Hosey (2019), vs. Mohr and Rosén (2017)). However, some notes can be made. Some variables may be clearly attributed to the favorability of individuals’ outcome expectancy in the context of adversity, thereby supporting PTG (including event centrality, resilience, positive coping, and cognitions leading to direct action). In certain circumstances, optimism is not correlated. Likewise, certain challenges that may be stimulating, can pose a threat to the point of having no effect on PTG achievement, such as self-esteem and shame. The researchers argue that the absence of a stimulating effect on the PTG appears to be due to a failure to take the healing process into account (Mohr & Rosén, 2017). Furthermore, Hosey (2019) emphasized that shame provides benefits only if it can initiate self-evaluation, even if it is negative, without actually causing withdrawal. Meanwhile, some other variables that may be attributed negatively are not necessarily likely to have a negative effect on PTG, but rather have no effect (e.g., negative religious coping). Instead, self-compassion and sense of coherence (as the opposite state of self-discrepancy) may not stimulate (Saint Arnault & Sinko, 2019) but rather may weaken growth (Ningabire, 2021). This appears to be due to self-soothing and the absence of mental discomfort. However, it is worth considering that increasing self-discrepancy at a certain point may actually hinder PTG (Shuwiekh et al., 2018). Qualitative studies are able to provide in-depth mechanism explanations (Breech, 2021; Ningabire, 2021; Ross, 2013). In summary of these mechanisms, individuals strengthen self-reliance, develop hopefullness and confidence about the future, through strategies both emotional, cognitive, and behavioral that escalate capacity and enhance feelings of control. Equally important, when interpersonal resources are available and individuals are ready, these resources are integrated to optimize outcomes. The last highlight regarding intrapersonal matters as outcomes has been discussed at the beginning to start the discussion section.
Besides intrapersonal matters, psychological growth as interpersonal matters may be considered supportive or inhibiting, determined by their forms. They can also be past experiences or current states, have passive or active tendencies, correspond to whether they involve internal processes, or are factual experiences (or outcomes that have been discussed earlier). Social support may not play a role (Addante, 2020) let alone risky relationships over time which tend to hinder positive outcomes (Oshri et al., 2018), given that memories and relationships are considered unsupportive or even disruptive (Aparicio, 2014; Girresch, 2018; Ningabire, 2021). Without ignoring the role of community and social presence in general, they seem to be less important than family (and the attachments built within it) in either supporting or undermining growth (Addante, 2020; Copley, 2015; Oshri et al., 2018). We have discussed that the types of complex trauma commonly found are relational, involving significant others in the family on a prolonged and repeated basis. These types of complex trauma actually undermine basic trust in early child development and have long-term impacts (Cook et al., 2005; Courtois, 2008), resulting in current relationship issues both inside and outside the family (Ningabire, 2021; Ross, 2013). The issues can characterize and lead to disorders as explained by WHO (2019) that those with a diagnosis of CPTSD are confirmed to experience symptoms of disturbances in relationships which are mostly a natural consequence of complex trauma. Conceptually, the conditions may indicate disruption of the emerging adulthood feature, namely self-focusing (Arnett, 2024), that the goal of their self-focusing to learn to stand alone as a self-sufficient person is hard to achieve. Arnett (2024) suggested that self-focusing is a necessary step before committing oneself to enduring relationships with others, in love and work.
Except, as explained by McCormack and Issaakidis (2018), interpersonal matters may become positive predictors for the growth of complex trauma survivors because their continuous presence helps recovery. Similarly, prosocial adult presence is important throughout the struggle following childhood trauma (Mohr & Rosén, 2017). Individuals need time to build trust along with the persistence of perceived social supports, while on the other hand strengthening self-reliance amidst expectations of system supports. Mohr and Rosén (2017) observed that emotional support has a tangible impact. This process of rebuilding trust also applies to family resources, whether they are members of the nuclear family or extended families. This is why PTG does not seem to benefit from family support, in contrast to resilience (Schaefer et al., 2018). In fact, an individual’s bond with their parents in particular is more impactful than their romantic partner (Copley, 2015). This becomes especially conflicting when they were part of the complex trauma experiences. Meanwhile, close platonic relationships (that are very likely to be acquired from peers) among emerging adult survivors can be obstacles to PTG (Copley, 2015). Especially among those who are not ready to grow, the negative impact of peers on PTG may be due to the need-fulfillment function of being dependent instead of self-reliance (Johnson et al., 1999). This also means that the interpersonal support will help recovery if it also encourages independence in addition to being present continuously.
The increasing role of social support has been mentioned along with the healing process, acceptance, building trust, readiness to accept help, and then having meaningful relationships and contributing to society as outcomes. On the other hand, when growth happens, individuals will still encourage self-reliance instead of bewailing themselves. The PTG model explains that rumination will provide benefits if it is deliberate, whereas it is detrimental if it is automatic and intrusive (Tedeschi et al., 2018). The process may be complicated as it allows for interactions between intrapersonal (including given characteristics) and interpersonal resources (including social and cultural influences). The worst scenario, for example, is suppression effects that may occur and change ‘the direction of support’. This effect was observed by Vartanian et al. (2014) that when individuals begin to consider self-esteem and personal growth (as intrapersonal resources), then social support and gratitude (as interpersonal resources) actually turn around to increase body dissatisfaction, leading to disordered eating behavior. The mechanism happens by changing the individual’s concern, remaining on how others view the individuals hence worrying about their body appearance.
Psychological distress/disorders and problems/conflicts are two negative issues that happen despite growing that may, but not always, be interconnected. Among emerging adult survivors of complex trauma, the identified psychological distress or disorders may be various, whether internalizing (e.g., Addante, 2020; Saint Arnault & Sinko, 2019; Shuwiekh et al., 2018) or externalizing (Oshri et al., 2018). They do not fully describe the psychological distress/disorders faced by emerging adults in this context, considering that this review’s systematic search focused more on the topic of psychological growth. It can be concluded that studies on psychological growth in this context involve more internalizing than externalizing symptoms. Only one study observed a relationship between externalizing symptoms and other growth-related psychological constructs yielding virtually no correlation with any positive outcomes (Oshri et al., 2018). Meanwhile, Vartanian et al. (2014) who observed an internalizing symptom in the form of a specific behavioral disorder (i.e., disordered eating behavior) actually concluded a negative correlation with personal growth initiative. Despite limited studies, the trend of results suggests that the relationships between externalizing symptoms (and perhaps internalizing symptoms in the form of disordered behavior) and growth, particularly as an outcome (i.e., PTG), may not enrich this topic of interest. It is assumed that individuals with high levels of PTG (with levels of adaptation, psychological functioning, or life awareness beyond those previously had; Tedeschi et al., 2018) may have low levels of externalizing symptoms, or vice versa. On the other hand, internalizing symptoms are more likely to be experienced by individuals while striving for or even achieving growth (Saint Arnault & Sinko, 2019; Wamser-Nanney et al., 2017). However, the absence of coexistence is still possible (e.g., Oshri et al., 2018; Wamser-Nanney et al., 2017).
The description is in line with Tedeschi et al. (2018) that distress or disorder may but not always be a prerequisite, and that growth is a continuous process or not a static outcome as explained previously. Event centrality also plays a role in predicting possible coexistence, through the double-edged phenomenon (Boals & Schuettler, 2011). Tedeschi et al. (2018) asserted that some enduring distress resulting from distinct and impactful traumatic memories could keep the focus on change and growth. Meanwhile, the distress can also become “over-integrated” and result in increased negative emotions, rumination, disruption, and avoidance (Berntsen & Rubin, 2007). The dynamics allow for the presence of PTG as well as symptoms/disorders, such as PTSD (Boals & Schuettler, 2011). These possible coexistences are likely to be accompanied by challenges in adjustments as the last theme, as well as in line with the first theme (particularly the positive relationship between PTG and trauma complexity) and the positive weighted correlation obtained. Contradictory correlations, for example in the relationship between PTG and depression (Saint Arnault & Sinko, 2019; Wamser-Nanney et al., 2017) may suggest the possible curvilinear relationship that the positive correlation between the two will reach a culmination point before PTG declines. On the other hand, a pessimistic view on this matter was explained by Schubert et al. (2015) that PTG needs to be addressed carefully because it may be a positive illusion in favor of avoidance and denial strategies for the traumatic event. Therefore, it may lead to self-destruction, such as non-suicidal self-injury (Swannell et al., 2012). Furthermore, the mixed findings in the relationship between outcomes of psychological growth and certain types of symptoms/disorders (e.g., Oshri et al., 2018) may imply peculiarities that also need attention.
Meanwhile, the identified problems/conflicts, which are actually more widely experienced even when distress/disorders cannot yet be decided, can be impacts or current stressors (e.g., Copley, 2015; Jirek & Saunders, 2018), interpersonal (Ningabire, 2021; Ross, 2013), intrapersonal (including cognitive, emotional; e.g., Aparicio, 2014; Hosey, 2019), or manifested in actual behaviors (Ningabire, 2021; Oshri et al., 2018) including poor health behaviors that may result in health problems (Santoro, 2017; Vartanian et al., 2014). Chronic disadvantaged socioeconomic status (Aparicio, 2014; Breech, 2021) which may result in other complex trauma and prolonged experiences, as well as increasing impacts of problems/conflicts gradually to the point where access to certain public service institutions is required (e.g., Ningabire, 2021; Santoro, 2017), are also part of what must be faced.
On the other hand, this review confirms the importance of support from systems (i.e., public service institutions) that have standardized service procedures and relevant resources needed to meet individual needs (including material, physical, mental and rehabilitation on an ongoing basis). This is highly required because individuals are likely to be under-resourced, due to possible experiences such as separation from familiar surroundings (i.e., family, peers), uncertainty about the future, loss of familiar routines (Kliethermes et al., 2014). However, it has been discussed that merely accepting support even requires readiness since the system(s) may be the ‘perpetrator’ that breaks trust. The struggle to re-build trust is tested through experiences such as discouragement, avoidance/unilateral termination, and repeated institutionalization. Above all the problems, once individuals have a high level of growth, this can alleviate the problems so that they have better self-adjustment despite the most severe complex trauma experiences (Sheline, 2013).
However, the experiences of negative issues also need to be understood from the perspective of emerging adult life as explained by Arnett (2024) that those kinds of problems are more prevalent than in any subsequent adult life stage. The problems are actually caused by complex trauma such as poverty, harsh and punitive parenting, family conflict, poor schools, and disorganized neighborhoods (Arnett, 2024). Furthermore, in line with the coexistence previously introduced, emerging adulthood theory also recognizes the paradox of mental health, namely that overall, self-esteem and life satisfaction can be high parallel with high rates of depression and anxiety (Arnett, 2024). Arnett (2024) asserted that emerging adults in this situation are dealing with their own efforts, facing five main features that have been mentioned to build the structure of adult life. Most young people thrive on the freedom and independence, but many struggle to stay afloat. That may be why, as previously mentioned, resilience is emphasized in the literature on emerging adulthood instead of psychological growth. When resilience is emphasized, the externalizing symptoms that were less prevalent in this review appear to be highlighted among emerging adults in their struggle to reach their milestones and identities along with the internalizing symptoms (Arnett, 2024).
Although the presence of high levels of PTG seems to be challenged by highly traumatic experiences as well, the risk of falling and experiencing psychological symptoms/disorders remains higher as predicted by event centrality (Boals & Schuettler, 2011). The challenges are not so easy for emerging adult survivors of complex trauma that coping may harm themselves, or instead use avoidance or sublimation. It can be explained that they may have observed and learned coping that tended to be maladaptive in previous life stages, used it in later life but at the same time explored new adaptive coping from the possibilities available once they became emerging adults (Arnett, 2024; Tedeschi et al., 2018). Therefore, the challenge may be detrimental so that it requires a higher protective factor index and conversely a lower risk factor index (Oshri et al., 2014). Similar to bargaining in coping strategies, individuals may perform psychological mechanisms that harm themselves to encourage self-perceived personal strength in relation to higher PTG (Hosey, 2019; Saint Arnault & Sinko, 2019). Others choose to distance themselves from disturbing strong emotions (Ningabire, 2021) and find alternatives to avoid subsequent impacts, such as in terms of interpersonal pursuits (Ross, 2013). They gradually adopt coping strategies, especially high engagement types, that lead them to increased favorability for PTG, as high engagement coping encourages PTG while avoiding some other high disengagement copings which actually inhibit PTG (Hasselle et al., 2019). Appraisal of events, their positioning separately from individual identity, as well as deliberate rather than automatic and intrusive rumination, are important (Boals & Schuettler, 2011; Kramer et al., 2020; Tedeschi et al., 2018). In line with that, Kunz et al. (2018), Shigemoto and Robitschek (2021) proved that coping flexibility among emerging adults is ultimately important for psychological growth. Here, the ability to abandon and substitute coping with something more helpful (re-coping) is based on a mature evaluation of the feedback he received (meta-coping) (Kato, 2020). When those individuals have finally experienced growth, they tend to have ameliorated effects of suicide-inducing trauma and better self-adjustment even with the most severe traumatic event history (Sheline, 2013).
This review contains advantages as well as limitations. First, searches were performed on eight major databases including theses and dissertations as indexed in ProQuest to cover wider previous studies. However, authors only involved English-language studies. The majority of the studies were also conducted in the US or were not culturally diverse which might influence the generalizability of the results. Differences based on ethnicity or minority status are also strongly thought to require attention, but little has been considered in this context. This review may not consider other language-relevant studies in other countries but may also initiate further studies on this topic in various other countries as well as considering different cultural contexts, ethnicity or minority status.
Second, with more inclusive keywords and methods, limited studies were obtained but the data were varied and to correspond between studies has become a challenge. This limited the data for reviews including for meta-analyses and reduced the chances for subgroup analyses despite its high heterogeneity. The variation in results among few studies made the conclusions more dynamic and less convincing. These limitations also indicate the need for further studies on similar topics to confirm the previous results. The majority of methods were quantitative cross-sectional thereby limiting causal and in-depth explanations. They were supplemented by one longitudinal study, three qualitative studies, and two mixed-method studies. However, more similar studies are still needed to explore from the depth of growth, growth trajectories, to causal relationships between growth and other variables. Researchers are also necessary to consider how the PTG construct needs to be cautious in using it interchangeably with several other growth-related psychological constructs.
Third, there was wide variability in measurements, especially complex trauma. Its measurements were retrospective using self-reports and mostly binary responses. Severity was indicated by the number of types and combinations, whereas few studies considered perceived severity. Instruments that consider frequency of events, perceived impact, or perceived severity can be used in future studies. The role of trauma types in differentiating growth also deserves more research, besides in-depth explorations based on specific complex trauma. Psychological growth was mostly measured as outcomes rather than processes. There were also few studies that examined PTG by its domains. Future research may look at psychological growth as a process or analyze the role of growth domains as latent factors.
Finally, to the extent of authors’ knowledge, this is the first systematic review of psychological growth in emerging adult complex trauma survivors. The studies described the variety of the methods, variables, and results, therefore whether exploratory or explanatory studies can be carried out in the future. However, examining the psychological growth of emerging adult complex trauma survivors both in understanding, assessing, and intervening, should consider the peculiarities of traumatic experiences, resources, negative issues that accompany, and the challenging roles that are chosen or given as well as their coping tracks. Intrapersonal resources may be more prioritized and relied on, while the role of interpersonal matters for individuals need to be more contextually observed. Positive changes (outcomes) in certain areas may be the indicators, but those should not be considered as final achievements since possible challenges and issues should be addressed. The specificity of emerging adulthood needs to be elaborated, and later, its processes and outcomes can be observed for differences with other developmental phases in cross-sectional and longitudinal studies.
Conclusion
This systematic review has provided the conclusion that there is an association between complex trauma and growth-related psychological constructs among emerging adult survivors. The narrative synthesis resulted in four major themes involving the role of traumatic experiences, resources, negative issues, and challenging adjustments. Meta-analyses resulted in a positive weighted correlation between complex trauma and PTG in the low category, with the weighted complex trauma mean of 2.83 below the hypothetical mean score and the weighted PTGI mean above the hypothetical mean score. Various characteristics and results were obtained from few studies and they were difficult to correspond between studies. Those findings indicate the need for future similar studies across different cultural contexts that concern emerging adults as underrepresented populations, especially those who survive complex trauma, to enrich the body of knowledge (e.g., examining the moderating variables and the role of growth domains), confirm contradictory results (e.g., regarding optimism or self-esteem as an intrapersonal resource, or the role of the presence of others as an interpersonal resource), examine causal relationships, and explore the depth of growth processes and dynamics. For practical purposes, clinicians may use these results both for understanding, assessment, and intervention should consider the individuals’ context and understand the roles of the four themes in them (e.g., performing assessments and understanding its dynamics in an empathetic way on the trauma complexity, the area and the role of each interpersonal resource, whether it has the potential to damage or provide ongoing support and encourage self-reliance, the intrapersonal resources they have, the histories of psychological symptoms/disorders and problems faced, the roles they must play as well as how they cope; and finally encouraging their areas of strength). Meanwhile, policymakers at the university level in particular or at the government level in general may use the results to provide both primary and secondary prevention programs through psychoeducation for students or societies.
Supplemental Material
Supplemental Material - Is Growth Possible in Emerging Adults Exposed to Complex Trauma?: A Systematic Review and Meta-Analyses
Supplemental Material for Is Growth Possible in Emerging Adults Exposed to Complex Trauma?: A Systematic Review and Meta-Analyses by Amalia Rahmandani, Subandi Subandi, and Muhana Sofiati Utami in Emerging Adulthood
Footnotes
Acknowledgments
We would like to thank the authors of the studies included in review for sharing the data or information especially those that were not available in the published articles. We would also like to thank Anindhita P. Amaranggani, S.Psi. as a research assistant, Fika Nadia Tirta Maharani, S.Psi., M.Psi., Psychologist as a colleague proofreader before revision, and Universitas Diponegoro for the scholarship for the first author’s doctoral study based on the Rector’s Decree Number 1276/UN7.P/HK/2021. However, the authors convey that the preparation, the research, and the publication of this manuscript were not under this funding.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Transparency and Openness Statement
Regarding the Raw Data
The authors of this manuscript entitled “Is Growth Possible in Emerging Adults Exposed to Complex Trauma?: A Systematic Review and Meta-Analyses” state that the raw data contained in this manuscript are not openly available for download. However all articles in this review can be accessed online and correspondence with the authors of the articles can be made to obtain data. All data presented in the table is data processed in this review, and obtained from each manuscript.
Regarding Quantitative Analyses
The authors of this manuscript entitled “Is Growth Possible in Emerging Adults Exposed to Complex Trauma?: A Systematic Review and Meta-Analyses” state that the analysis code/syntax used for the analyses is not openly available for download. However it can be obtained from the corresponding author following the completion of a privacy and fair use agreement.
Regarding Qualitative Analyses
The authors of this manuscript entitled “Is Growth Possible in Emerging Adults Exposed to Complex Trauma?: A Systematic Review and Meta-Analyses” state that the list of questions and coding manuals are not openly available for download. However they can be obtained from the corresponding author following the completion of a privacy and fair use agreement.
Regarding Materials Used
The authors of this manuscript entitled “Is Growth Possible in Emerging Adults Exposed to Complex Trauma?: A Systematic Review and Meta-Analyses” state that all materials used in the study are not openly available for download. However all articles in this review can be accessed online and correspondence with the authors of the articles can be made to obtain the materials used.
Regarding a Pre-Registration Plan for Data Collection and/or Analysis
The authors of this manuscript entitled “Is Growth Possible in Emerging Adults Exposed to Complex Trauma?: A Systematic Review and Meta-Analyses” state that this study include a pre-registration plan for data collection and/or analysis, namely at PROSPERO (![]() ). There were no deviations from the pre-registration plan indicated in the study.
). There were no deviations from the pre-registration plan indicated in the study.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.