
Abstract
This study examines associations between screen time, digital sleep-interrupted behaviors, and risk for major depressive episodes among emerging adults, with attention to the roles of personality traits, gender, and race. Data were drawn from 2,781 participants in the Future Families and Child Wellbeing Study. Results indicated that excessive screen time, particularly more than 6 hours per day, and the interaction between nighttime device co-sleeping and sleep-interrupted device checking were associated with higher likelihood of major depressive episodes. Individual differences were salient. Conscientiousness was linked to lower screen use and reduced risk of depression, whereas neuroticism showed the opposite pattern. Gender and racial differences further shaped these associations. The findings suggest that excessive screen engagement and sleep-disruptive device behaviors were related to adverse mental health outcomes in emerging adulthood. Prevention and intervention efforts should emphasize digital literacy, development of balanced media use habits, and culturally responsive strategies to promote psychological well-being.
Keywords
Introduction
The rapid growth of screen time has raised concerns about its impact on mental health, particularly depression (Boers et al., 2019; Ma & Sheng, 2023; Twenge et al., 2018). Research indicates that prolonged exposure and problematic use such as nighttime device co-sleeping and sleep-interrupted device checking are linked to sleep disruption, impaired functioning, and emotional distress (Andersen et al., 2023; Li et al., 2022; Madhav et al., 2017; Shannon et al., 2022). The association between digital engagement and well-being, however, may be non-linear, (Przybylski & Weinstein, 2017). Moderate levels of use may confer benefits, such as enhanced social connectivity and digital literacy, whereas excessive engagement appears to surpass an optimal threshold, producing displacement effects. Under such conditions, excessive screen time may encroach upon essential health behaviors, including sleep and physical activity (Orben & Przybylski, 2019; Przybylski & Weinstein, 2017; Shannon et al., 2022).
Behaviors like using devices in bed or waking to check them worsen sleep and may increase mental health risks (Dibben et al., 2023; Kheirinejad et al., 2023). These effects vary across individual factors, including personality traits, age, race, and gender, suggesting some individuals are more vulnerable (Forte et al., 2023; Kayiş et al., 2016; Lizandra et al., 2019; Pettorruso et al., 2020). For example, females show a stronger link between screen use and depression than males (Forte et al., 2023; Wang et al., 2019). Overall, screen-related behaviors and their associated mental health outcomes are influenced by both behavioral patterns and individual-level differences, reflecting a dual heterogeneity that captures variation both across different types of behaviors and within specific behavioral categories (Grubbs & Boness, 2025; Lizandra et al., 2019).
While existing research has identified associations between screen use, sleep-interrupted behaviors, and depression, relatively few studies have investigated how personality traits may alter this relationship, particularly within diverse populations of emerging adults. This study addresses this gap by examining the associations among screen time, sleep-interrupted behaviors, and risk of major depressive episodes, when taking roles of personality traits, age, gender, and race into account. Screen time refers to the extent of time in non-school or non-work-related digital activities (e.g., gaming, social media, internet browsing), while sleep-interrupted behaviors are assessed through nighttime device co-sleeping and sleep-interrupted device checking. Major depressive episode refers to a period of at least two weeks characterized by persistent depressed mood or loss of interest or pleasure, accompanied by symptoms such as changes in sleep, appetite, energy, concentration, or feelings of worthlessness, that cause significant impairment in daily functioning (American Psychiatric Association, 2022). Emerging adulthood (ages 18–25) is a key developmental stage characterized by increased autonomy, reduced parental monitoring, and significant identity formation and neurodevelopmental changes (Arnett, 2023). During this period, young adults gain greater control over their time and decisions, often resulting in increased media and smartphone use, which has been linked to heightened depressive symptoms (Coyne et al., 2013; Ivie et al., 2020; Wacks & Weinstein, 2021). This period is especially important for studying the mental health effects of screen behaviors, as individuals are navigating critical psychological and neurological transitions that may heighten vulnerability to the negative impacts of digital media use (Stockdale & Coyne, 2020). Building on the media displacement framework and the Goldilocks Hypothesis (Boers et al., 2019; Bryant & Fondren, 2009; Lizandra et al., 2019; Ma & Sheng, 2023; Przybylski & Weinstein, 2017), the current study aims to clarify and reconcile conflicting findings in the literature by examining both quantitative screen time and behavioral use of digital engagement, while accounting for individual factors such as gender, income, and race/ethnicity. This multidimensional approach moves beyond simplistic assumptions to explore how the context and nature of screen use influence the risk of major depressive episodes. By doing so, this study advances theoretical understanding of media effects and provides evidence to inform more targeted, developmentally appropriate, and equity-focused mental health interventions for emerging adults.
Literature Review
Screen Time and Sleep-Interrupted Behaviors
Screen time is defined as the total duration an individual spends engaging with any type of electronic, screen-based device (e.g., computers, smartphones, televisions, tablets) and nighttime device co-sleeping refers to the practice of maintaining a mobile electronic device within the sleep environment or actively using the device while in bed during the typical sleep cycle. Sleep-interrupted behaviors refer to patterns of technology use that intrude upon or disrupt the sleep period, such as nighttime device co-sleeping and sleep-interrupted device checking, in this study. Nighttime device co-sleeping describes the practice of keeping a mobile electronic device within the immediate sleep environment while sleep-interrupted device checking refers to waking during the night to view, respond to, or engage with content on a mobile device, thereby fragmenting sleep continuity. Personality traits, particularly conscientiousness and neuroticism, play a key role in shaping screen time and sleep-interrupted behaviors. Conscientiousness, marked by organization, discipline, and self-control, is linked to healthier media habits and lower risk of excessive internet use (Kayis et al., 2016; Marciano et al., 2022). Those who are low in conscientiousness tend to struggle with self-regulation, making them more prone to sleep-interrupted behaviors, problematic media use, and internet addiction (Gao et al., 2022; Toyama & Hayashi, 2022). In contrast, neuroticism, characterized by emotional instability, anxiety, and a tendency toward negative emotions, is strongly associated with problematic screen behaviors (Barlow et al., 2014; Gao et al., 2022). Individuals high in neuroticism often use the internet as a coping mechanism to manage distress, relying on digital escapism to avoid unpleasant emotions (Cho et al., 2017). This maladaptive coping can lead to greater emotional dependency on screens. Meta-analyses confirm a negative correlation between conscientiousness and internet addiction, while neuroticism shows a consistent positive link with problematic media use (Gao et al., 2022; Kayis et al., 2016; Marciano et al., 2022). Additionally, emotion dysregulation, commonly found in neurotic individuals, has been tied to impulsivity and a higher risk of addictive behaviors (Pettorruso et al., 2020). These findings highlight how personality traits influence screen habits, suggesting that emotional and behavioral regulation are critical in understanding media-related mental health risks.
Research shows age, gender and racial differences in screen time and problematic media use. Screen time typically demonstrates a curvilinear developmental trajectory across adolescence and youth. Throughout adolescence, digital media engagement tends to increase linearly. This escalation is frequently attributed to the developmental imperatives of this stage, specifically the pursuit of greater autonomy, the formation of self-identity, and the intensification of peer relationships, which digital platforms are extensively utilized to facilitate (Coyne et al., 2018; Zhu et al., 2023). Screen time often reaches its peak prevalence around the transition into emerging adulthood, typically near age 20 (Politte-Corn et al., 2023). Following this peak, the association between increasing age and screen time either becomes stable or slightly negative (Coyne et al., 2018; Politte-Corn et al., 2023; Zhu et al., 2023). This stabilization or decrease may reflect the displacement of leisure screen time as young adults assume new responsibilities associated with independence, such as entering the workforce, pursuing higher education, or establishing independent living arrangements. Males are more likely to engage in excessive gaming and entertainment-driven media, while females tend to use social media and communication platforms more frequently (Twenge & Martin, 2020). These differences reflect varying motivations: males often seek competition and escapism, while females prioritize social connection and emotional expression (Orben et al., 2020). Problematic use also varies, with males showing higher rates of gaming disorder and internet addiction, and females more prone to compulsive social media use linked to anxiety and body image concerns (Andreassen et al., 2016; Fardouly et al., 2018). Race and ethnicity play a role in screen time and problematic media use, with research showing that Black and Hispanic youth often have higher screen time than their White peers, largely due to socioeconomic factors like limited access to safe outdoor spaces and extracurricular activities (Hasson, 2018; Tandon et al., 2021). Black adolescents were also more likely to report higher night-time sleep-interrupted behaviors or screen-based media devices use than other adolescents (Mireku et al., 2019; Nagata et al., 2025). This increased exposure may heighten the risk of sleep-interrupted behavior, especially in communities where digital media is a key source of entertainment and connection.
Screen Time, Sleep-Interrupted Behaviors, and Depression
The link between screen time, sleep-interrupted behaviors, and mental health is especially relevant during emerging adulthood, a period marked by greater independence and heightened vulnerability to depression. While screen use can support social connection, excessive or problematic use is consistently associated with negative mental health outcomes. Madhav et al. (2017) found that adults spending over 6 hours daily on screens had significantly higher odds of moderate to severe depression, even after adjusting for individual factors. Zhang et al. (2022) reported that high screen time, particularly on phones and tablets, increased depression risk among Chinese adults. This effect was evident on both weekdays and weekends, suggesting a consistent negative impact of screen exposure on mood. The type and purpose of screen use appear to impact its effect on depression. Santos et al. (2024) found that recreational screen time was linked to depression, while screen use for schoolwork was not, highlighting the importance of context. Stockdale and Coyne (2020) studied social media use from late adolescence to emerging adulthood and found that using platforms to alleviate boredom increased over time and was associated with anxiety and stress. However, they found no direct link between overall social media use and depression. Similarly, Przybylski and Weinstein (2017) found that moderate digital technology use was not inherently detrimental, with the associations varying according to contextual factors such as timing of use (e.g., weekdays versus weekends). Orben and Przybylski (2019) likewise found minimal evidence of substantial negative associations between digital screen engagement and adolescent well-being. Collectively, this body of evidence suggests that mental health outcomes may be shaped less by total screen time, provided it remains within non-excessive thresholds, and more by the motivations, contexts, and patterns of technology use. It is also important to note that emerging post-2020 research suggests that, particularly during the COVID-19 pandemic, digital media use may have functioned as a critical social and emotional lifeline for some young adults by facilitating connection and support during periods of physical isolation (Chase et al., 2022; James et al., 2023; Osborne, 2025).
In addition, research shows mixed effects of screen time on depression, influenced by individual differences and context. Coyne et al. (2020) found that adolescents increasing social media use beyond their average did not show higher depression or anxiety, suggesting within-person changes may not be harmful. Personality traits and usage motives likely moderate these outcomes. Santos et al. (2024) noted that messaging apps reduced loneliness, showing a potential protective effect. However, overall screen use during the pandemic was linked to increased depression, anxiety, and loneliness, reflecting the double-edged impact of digital technology.
Digital sleep-interrupted behaviors such as recurrent nighttime smartphone activity or waking to check a device during intended sleep periods have been identified as salient factors of poorer mental health in adolescents and emerging adults. For example, Andersen et al. (2023) found that frequent self-reported nighttime smartphone use was strongly associated with higher odds of severe depressive symptoms and perceived stress, and that repeated smartphone activity throughout the self-reported sleep period was linked to greater likelihood of severe depressive symptoms in adults across three samples using both self-report and high-resolution tracking data. Converging evidence from longitudinal tracking in the Copenhagen Network Study demonstrated that mobile phone activity recorded during self-reported sleep periods was associated with elevated depressive symptoms and perceived stress at baseline among young adults, though longitudinal associations were smaller or not consistently replicated over time (Dissing et al., 2022). Taken together, these recent studies suggest that not merely total screen time but the timing and fragmentation of sleep due to device use constitute important risk factors for adverse mental health outcomes among adolescents and emerging adults.
Emerging evidence further supports the mediating role of sleep in this relationship. Zou et al. (2019) demonstrated that sleep quality partially mediates the link between problematic mobile phone use and depressive symptoms, highlighting sleep as a modifiable risk factor. Zhang et al. (2022) expanded on this by identifying mobile phone addiction and sleep disturbances as dual mediators between academic stress and depression. Collectively, these findings underscore the need for mental health interventions that account for the indirect effects of digital media use on psychological well-being, particularly through sleep-related mechanisms. In summary, research shows a complex link between screen time, digital sleep-interrupted behaviors, and depression in emerging adults, influenced by activity type, individual differences, and social context. While excessive use often correlates with depressive symptoms, further study is needed to better understand and address these mental health risks.
Theoretical Framework
The media displacement hypothesis provides a foundation for understanding how screen time and nighttime device co-sleeping influence depression (Bryant & Fondren, 2009). This framework posits that digital engagement replaces essential health-promoting behaviors, such as in-person socialization, physical activity, and sleep (Kaya et al., 2021; Twenge et al., 2018). Displacement is particularly critical during emerging adulthood, where disrupted routines and weakened social ties can undermine identity formation and mental health. Nighttime device use exposes individuals to blue-wavelength light and cognitively or emotionally stimulating content, which can impair sleep quality and duration, thereby increasing risk for depressive symptoms. (Cain & Gradisar, 2010; Zou et al., 2019).
However, recent evidence suggests that the impact of technology is not strictly linear. The Goldilocks Hypothesis proposes that moderate digital engagement is not intrinsically harmful and may even be advantageous for social connectivity in a digitally integrated world (Przybylski & Weinstein, 2017). Research indicates a quadratic, U-shaped relationship where low-to-moderate use (typically <1 hour daily) was associated with higher life satisfaction and prosocial behavior, while negative outcomes only emerge once use becomes excessive, exceeding 3 hours daily (Orben & Przybylski, 2019; Przybylski, 2014). Consequently, mental health outcomes may be determined less by total duration and more by specific motivations and contexts of use. Based on this integrated framework, we hypothesize that a higher risk of major depressive episodes is associated with excessive screen time and sleep-interrupted behaviors, while accounting for individual factors such as personality traits, gender, and race.
Method
Data
The data for this study came from Wave 7 of the Future Families and Child Wellbeing Study (FFCWS), a longitudinal project examining parental characteristics and child outcomes. The initial wave (1998–2000) included 4,898 mothers. Follow-up surveys occurred when the child was ages 1, 3, 5, 9, 15, and 22. By Year 22, 2,990 children responded. Prior to conducting the interview, field staff obtained a signed informed consent form from each participant. Interviewers were instructed to provide time for participants to read the form thoroughly and to offer an opportunity for them to ask any questions regarding their involvement in the study. These procedures were overseen by the Institutional Review Board of Princeton University. For this analysis, we included only participants from Wave 7 who had complete data on screen time, sleep-interrupted behaviors, depressive symptoms, personality traits, gender, and race, resulting in a final analytic sample of 2,781 cases. Earlier waves were not included in the analysis due to the absence of consistent measures of non-school/work-related digital activity. Half of the final sample was female, with 46% non-Hispanic Black, 27% Hispanic, 19% non-Hispanic White, and 8% other racial/ethnic groups. The average age was 22.3 years. Most had a high school education, and 22% had a college degree. About 64% were employed.
Measures
Depression was measured using items from the Composite International Diagnostic Interview–Short Form (CIDI-SF; Kessler et al., 1998), assessing major depressive episodes in the past 12 months. Respondents reporting at least two weeks of persistent dysphoria or anhedonia answered seven symptom questions (e.g., fatigue, sleep issues, worthlessness, etc.). A major depression (MD) score was calculated by summing affirmative responses. Participants scoring three or more were classified as probable depression cases (coded as 1), while those scoring below three were considered non-cases (coded as 0). This measure provides a reliable indicator of probable major depression in population-based surveys (Walters et al., 2002).
Screen time was assessed using an open-ended question that asked participants to report the number of hours spent on screen-based activities, as follows: “On an average day, how many hours do you play video or computer games or use a computer for something that is not school or work related? Count time spent on things such as Xbox, PlayStation, an iPad or other tablet, a smartphone, YouTube, Facebook or other social networking tools, and the internet.”
Sleep-interrupted behaviors were measured using two indicators: nighttime device co-sleeping and sleep-interrupted device checking. Nighttime device co-sleeping was assessed with the item, “Do you sleep with a mobile device in your bed?” Responses were dichotomized, with “yes” coded as 1 and “no” coded as 0. Sleep-interrupted device checking was measured with the question, “How often do you wake up to check your mobile device during the night?” Response options included: “Never,” “Rarely (<2 nights per week),” “About once per night,” “Two or more times per night,” and “It depends.”
Personality was measured using a short version of the Big Five Inventory (BFI; John et al., 2008), a reliable scale for adults (Soto & John, 2017). This study focused on conscientiousness and neuroticism, each assessed by four items. Respondents rated their agreement on a 5-point Likert scale (1 = Disagree Strongly to 5 = Agree Strongly). Conscientiousness items included statements like “I get chores done right away” and reverse-scored items such as “I often forget to put things back.” Neuroticism items included “I have frequent mood swings” and reverse-scored items like “I am relaxed most of the time.” In this study, the reliability estimates for the measures indicated marginal internal consistency, with Cronbach’s alpha values of 0.58 for conscientiousness and 0.57 for neuroticism. Consistent with prior research using abbreviated Big Five measures in large-scale surveys, the relatively modest internal consistency likely reflects the limited number of items per subscale rather than poor construct validity, and results involving personality traits should therefore be interpreted cautiously (Soto & John, 2017).
Gender was coded as 1 for female and 0 for male. Race and ethnicity were categorized into four mutually exclusive groups: non-Hispanic White, non-Hispanic Black, Hispanic, and other racial/ethnic groups. Age was measured as a continuous variable. Educational attainment was originally measured using 12 categorical responses and subsequently recoded into three levels for analytical purposes: less than high school, high school diploma, and more than high school. Employment status was based on whether respondents worked for pay in the past week (1 = yes, 0 = no).
Analytic Strategy
Descriptive and bivariate analyses were conducted to examine sample characteristics and relationships among key variables (e.g., personality traits, gender, and race). Multivariate regression analyses were conducted to examine the effects of key independent variables on the likelihood of experiencing a major depressive episode. The analysis was guided by the hypothesis that depression risk is shaped by screen time, sleep-interrupted behaviors, and a range of individual factors, including personality traits, gender, race, age, educational attainment, and employment status. Logit regression was used for depression and problematic use, while OLS regression was applied to screen time analysis. All analyses were performed using STATA version 16.0.
Results
Descriptive and Bivariate Analysis
Characteristics of Key Variables
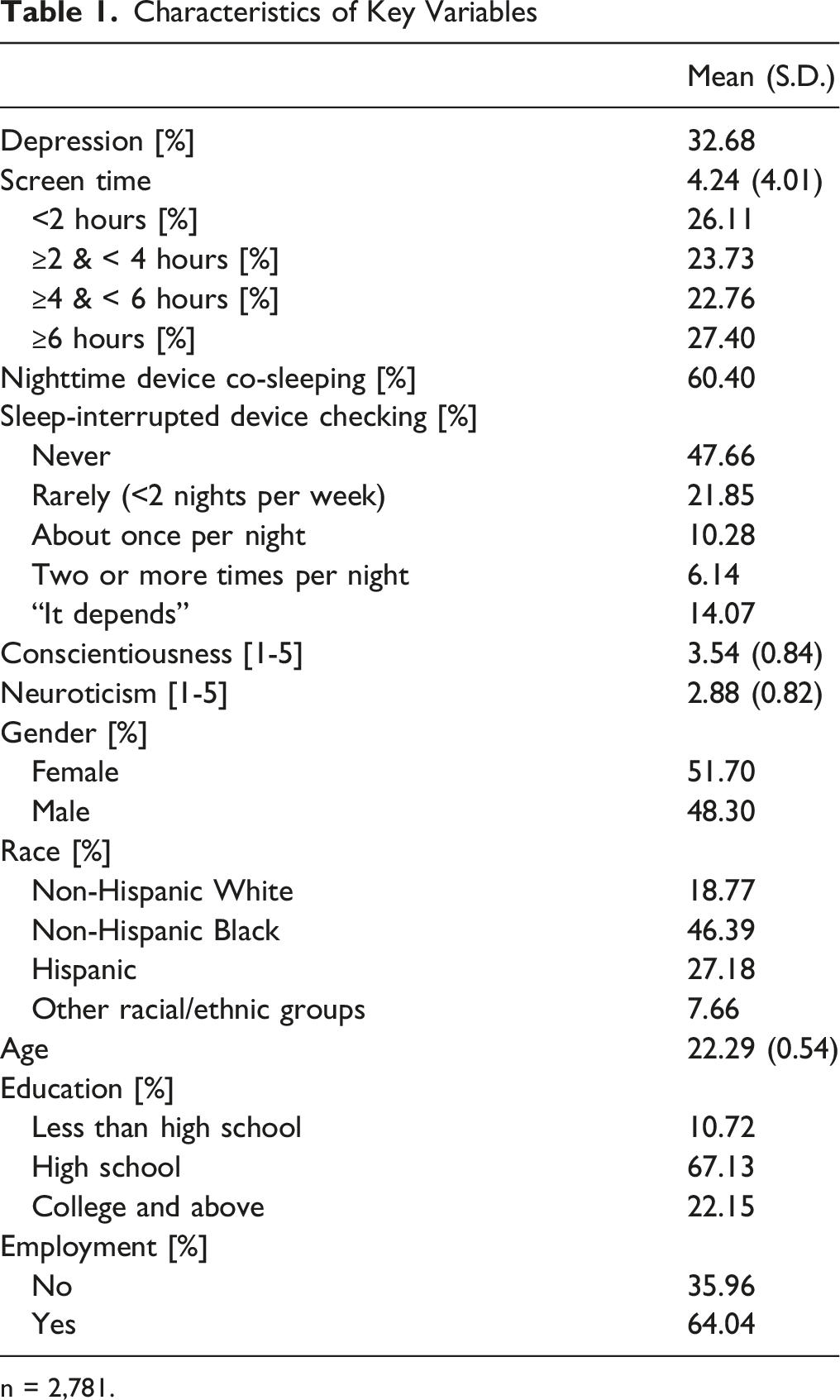
n = 2,781.
Screen Time, Nighttime Device Co-Sleeping, and Depression by Key Variables
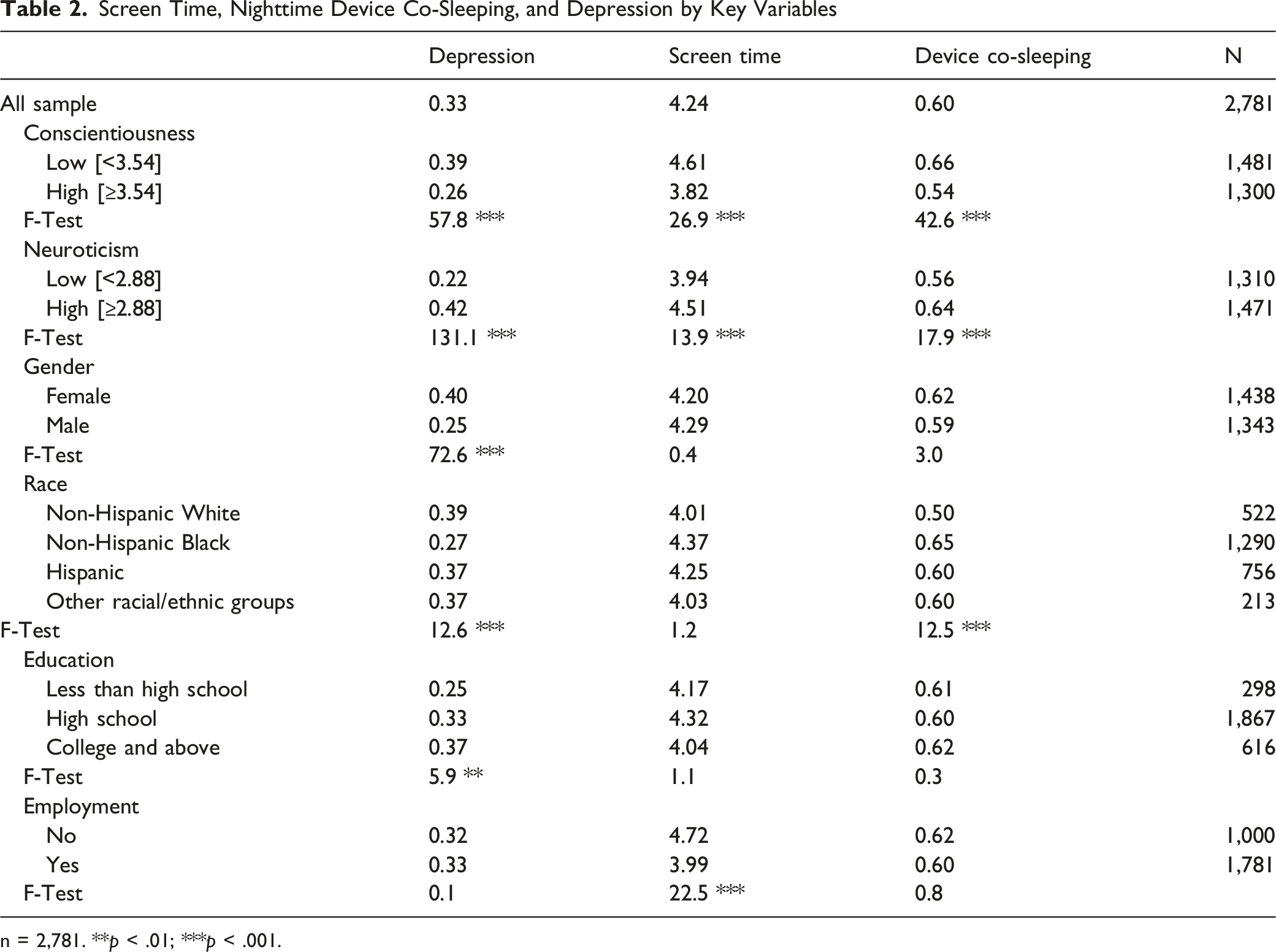
n = 2,781. **p < .01; ***p < .001.
Sleep-Interrupted Device Checking by Key Variables
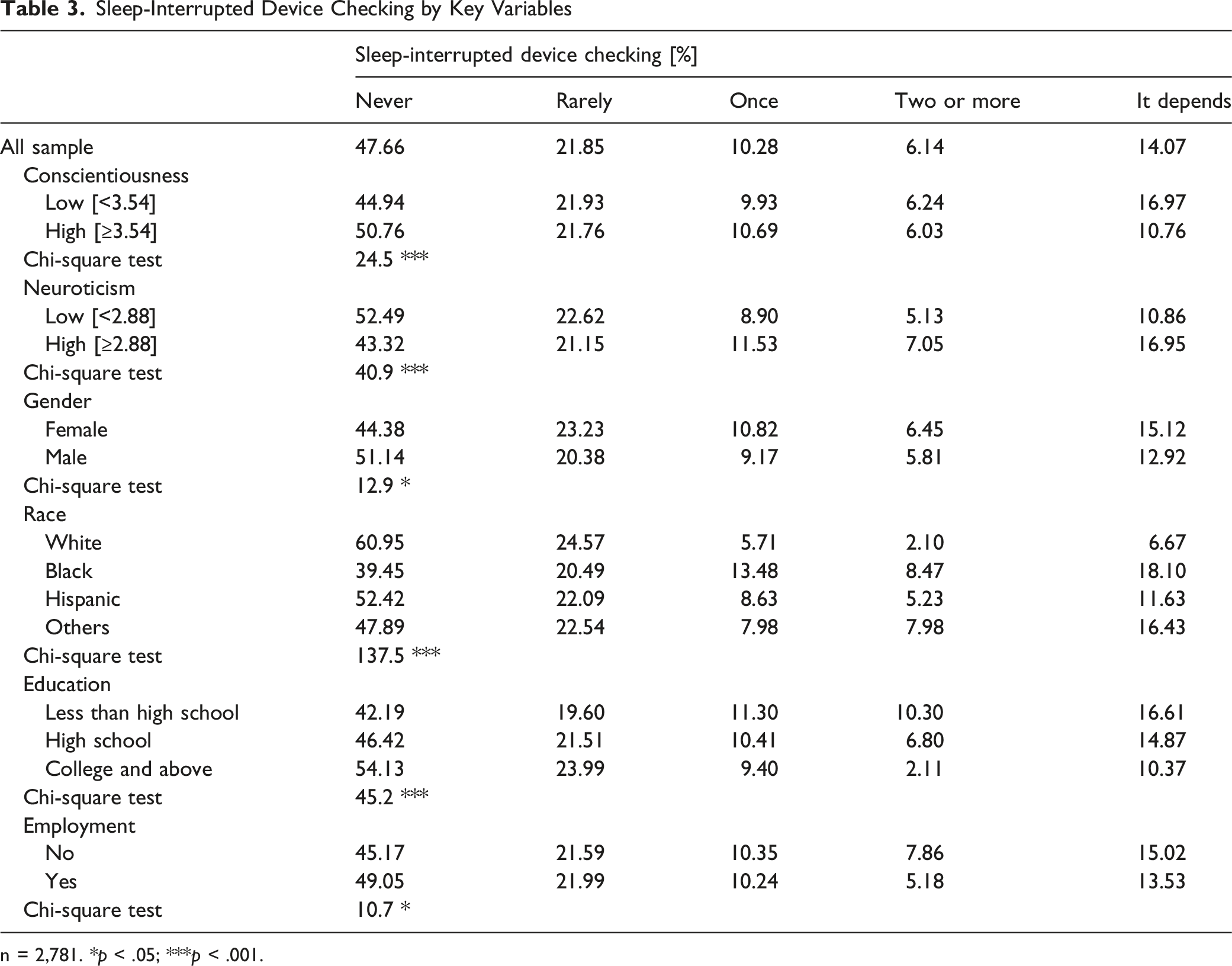
n = 2,781. *p < .05; ***p < .001.
We further examined the interaction between nighttime device co-sleeping and sleep-interrupted device checking, which was statistically significant (p < .001). Adults who engaged in device co-sleeping were more likely to wake up during the night to check their device once (13.4%) or two or more times (8.5%) per night compared with those who did not co-sleep with their device (5.6% and 2.5%, respectively). Notably, 38.8% of adults who reported device co-sleeping indicated that they never woke to check their devices, while this proportion was lower than that observed among adults without device co-sleeping (61.1%), the pattern suggests that, for some individuals, co-sleeping with a device may primarily serve functions such as alarms or emergency access rather than routine nighttime checking.
Regression Results
Regression Analyses of Screen Time
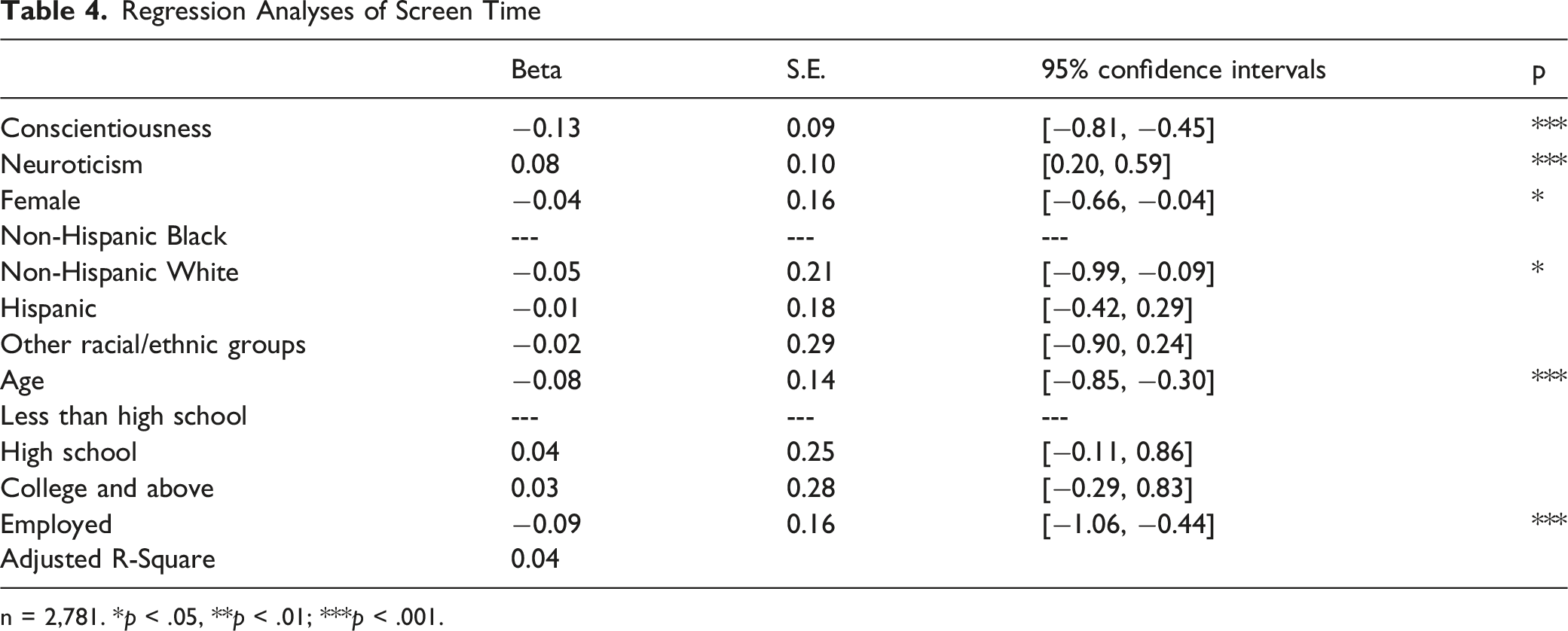
n = 2,781. *p < .05, **p < .01; ***p < .001.
Logit Regression Analyses of Nighttime Device Co-Sleeping
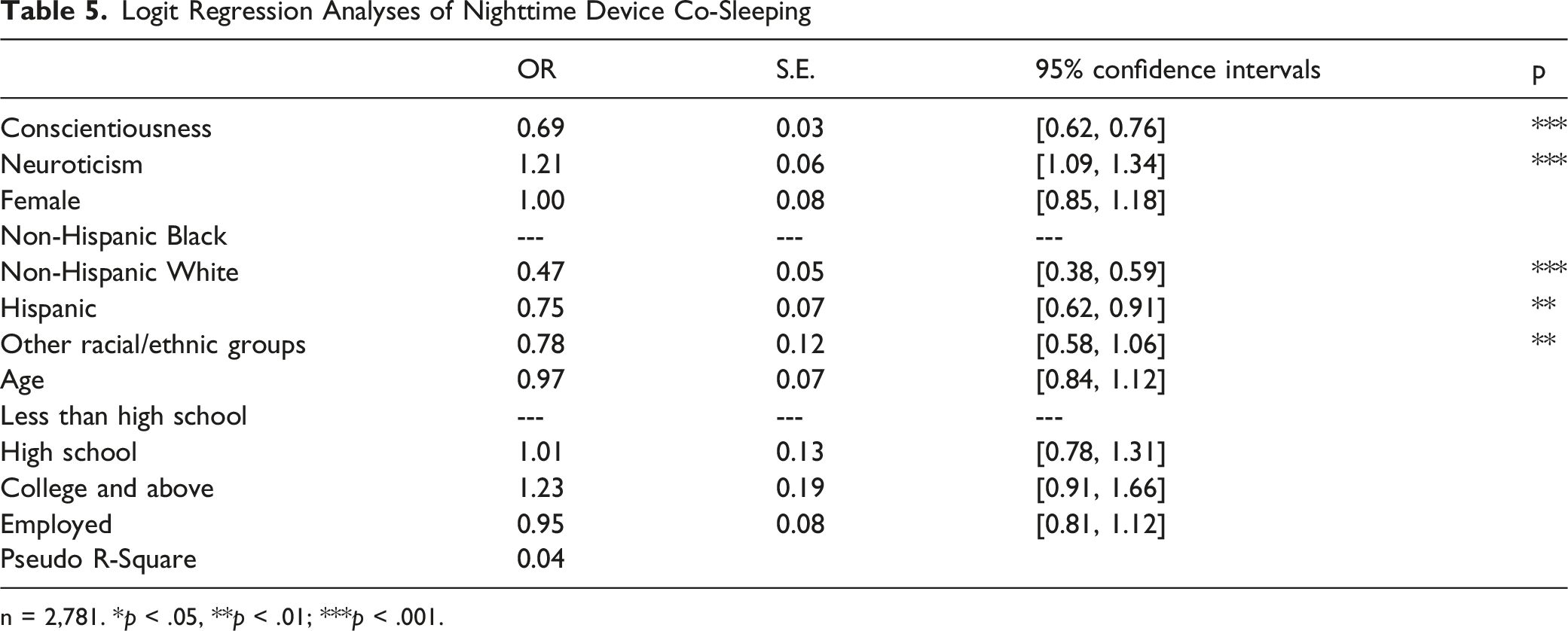
n = 2,781. *p < .05, **p < .01; ***p < .001.
Regression Analyses of Sleep-Interrupted Device Checking
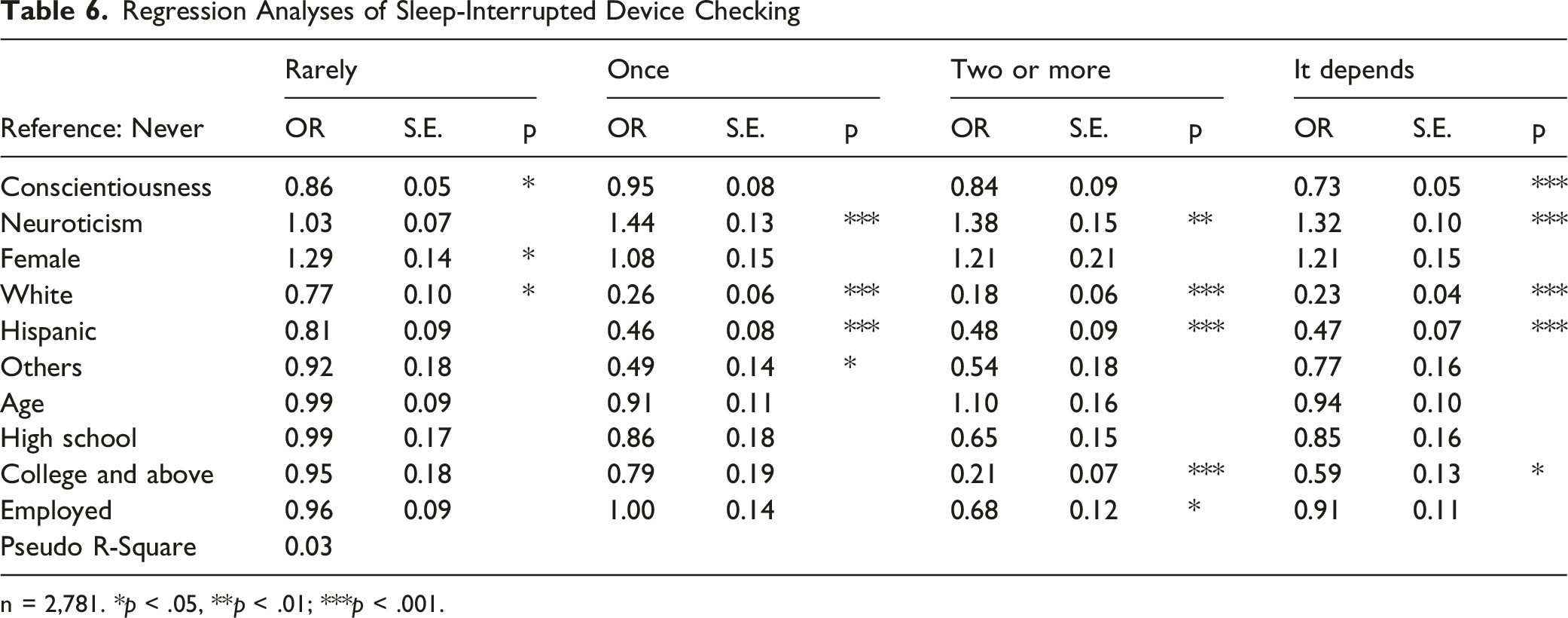
n = 2,781. *p < .05, **p < .01; ***p < .001.
In terms of nighttime device co-sleeping, conscientiousness again showed a protective effect (OR = 0.69, p < .001, dy/dx = −0.09), while neuroticism heightened the odds of device co-sleeping (OR = 1.21, p < .001, dy/dx = 0.05). Additionally, individuals from all other racial/ethnic groups had significantly lower odds of nighttime device co-sleeping compared to Black respondents. Regarding sleep-interrupted device checking, higher neuroticism was associated with increased odds of checking once per night (OR = 1.44, p < .001) and two or more times per night (OR = 1.38, p < .01), relative to never checking. In contrast, higher conscientiousness was associated with lower odds of rarely checking (OR = 0.86, p < .05) and selecting “it depends” (OR = 0.73, p < .001), compared with never checking. Respondents from all other racial and ethnic groups had significantly lower odds of nighttime device checking than Black respondents, indicating disparities in digital behavior patterns across racial groups. Additionally, adults with a college education and those who were employed were less likely to check their devices two or more times per night compared with their respective counterparts.
Logit Regression Analysis of Depression
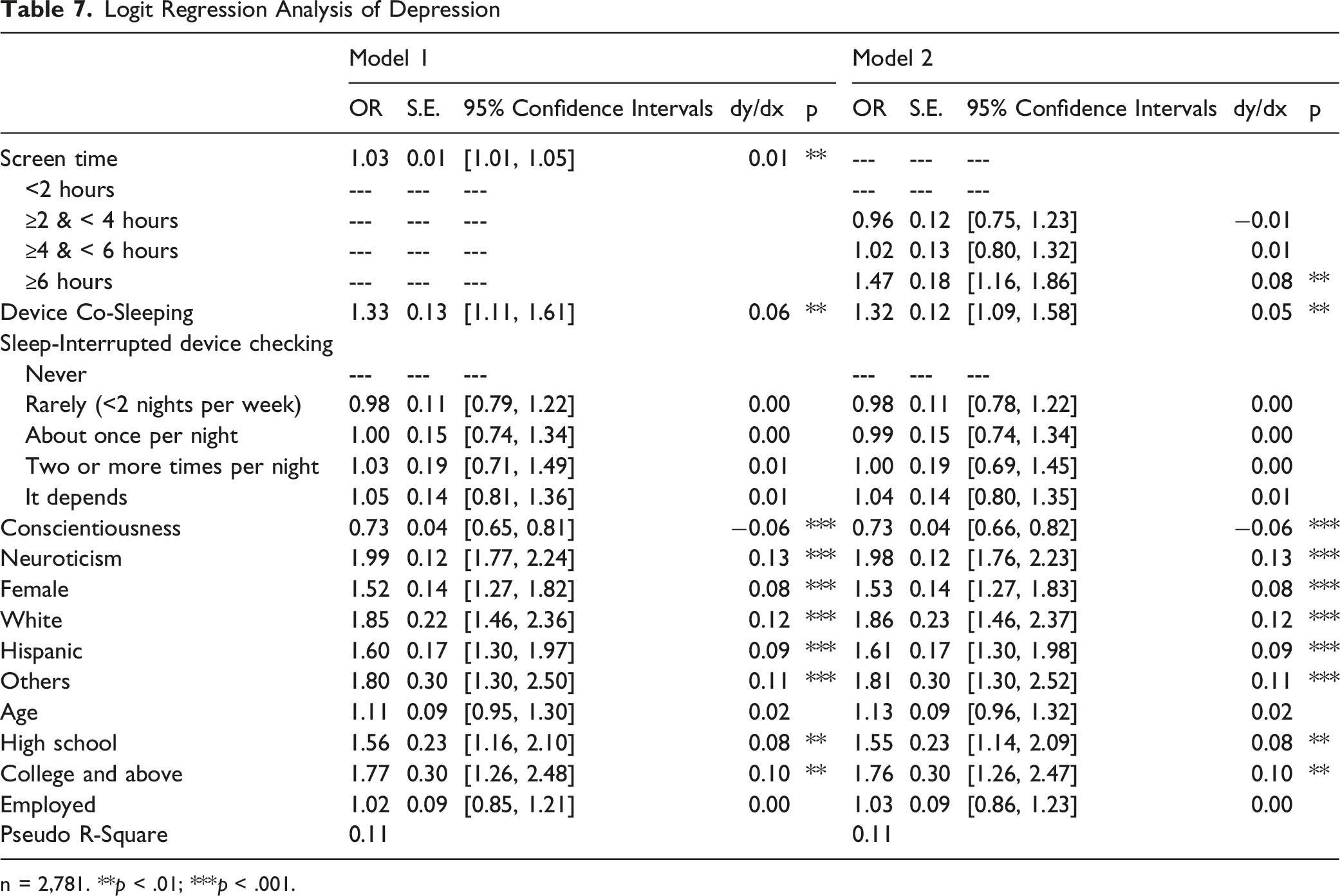
n = 2,781. **p < .01; ***p < .001.
We further examined the interaction effect between nighttime device co-sleeping and sleep-interrupted device checking on the risk of major depressive episodes. This model was identical to Model 1 in Table 6, with the exception that an interaction term was included in the analysis. Figure 1 illustrates this interaction effect. Among adults who engaged in device co-sleeping and checked their devices two or more times per night, the predicted probability of experiencing a major depressive episode was 0.38, which was significantly higher than that observed for other combinations of behaviors (ranging from 0.30 to 0.36). Interaction of device Co-sleeping and sleep-interrupted device checking on depression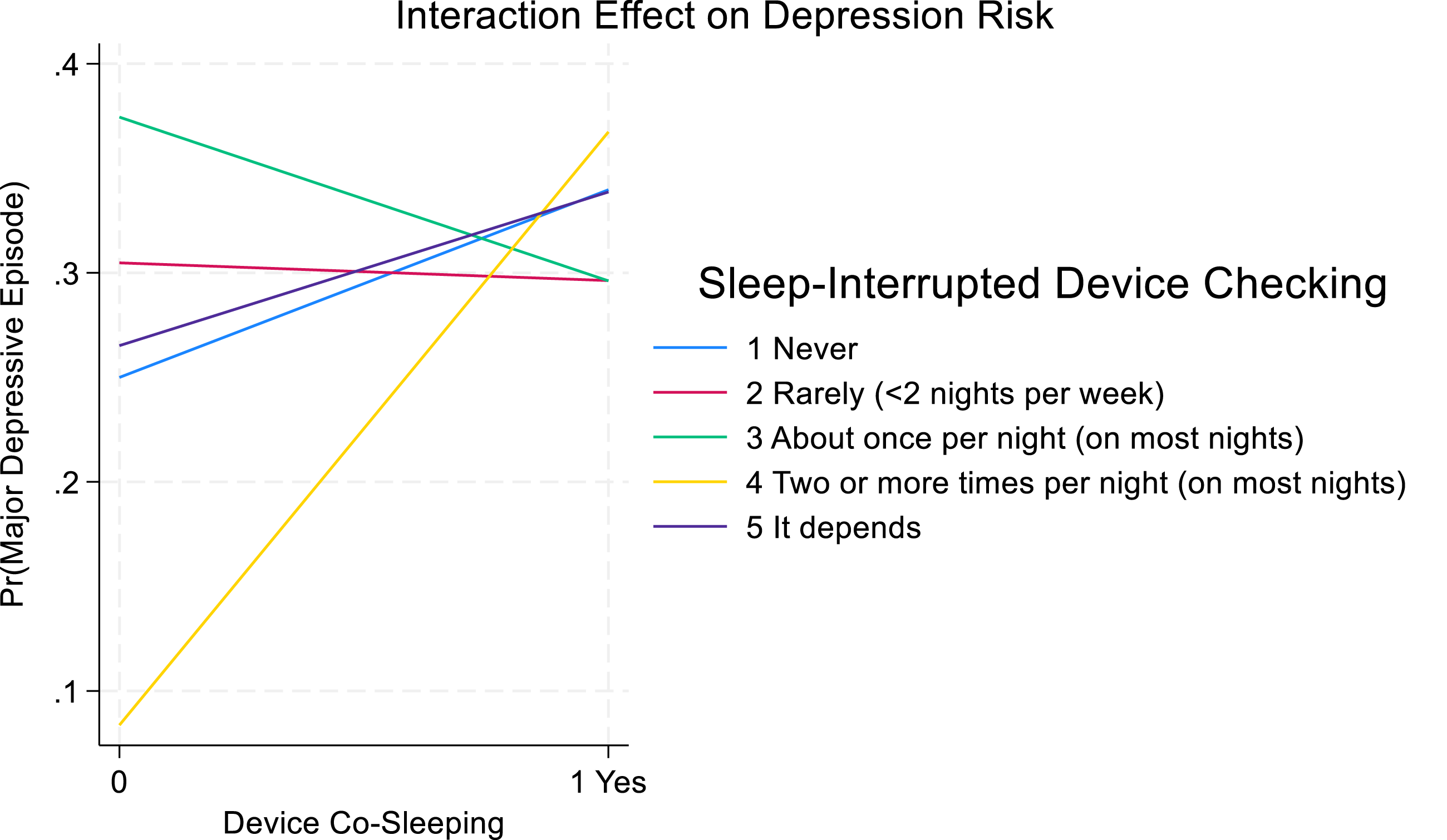
Discussion
This study was designed to examine the media displacement and the Goldilocks hypotheses in the context of emerging adults’ mental health, specifically focusing on the risk posed by screen time and sleep-interrupted behaviors. Our work moves beyond simple linear associations by integrating personality, gender, and racial/ethnic background into the analysis. By assessing how these fundamental individual characteristics condition the link between digital engagement and mental health risk, this study sought to establish a more nuanced and clinically relevant understanding of these two domains.
Overall, the findings support the hypotheses, which posit that excessive screen use displaces activities vital for well-being (like sleep and social interaction), thereby contributing to poorer mental health outcomes (Madhav et al., 2017; Orben & Przybylski, 2019; Przybylski & Weinstein, 2017; Twenge et al., 2018). Our key findings confirmed the mechanisms central to the hypotheses. First, consistent with prior research (Coyne et al., 2013), the average screen time of 4.24 hours per day was observed. The association between increased screen time and risk of major depressive episode was significant, particularly for individuals spending over 6 hours per day, who had significantly higher odds of experiencing an episode. This supports the notion that a substantial threshold of screen exposure is detrimental to psychological well-being (Madhav et al., 2017; Orben & Przybylski, 2019; Przybylski & Weinstein, 2017; Twenge & Campbell, 2018). Secondly, this study identified high-risk behaviors of nighttime device co-sleeping and sleep-interrupted device checking as critical factors. Over 60% of participants reported sleeping with a mobile device, and this behavior was significantly associated with 1.32 times higher odds of experiencing a major depressive episode. More than half of the adults reported waking during the night to check their mobile devices, with 6.1% indicating that they did so two or more times per night. Adults who both slept with a mobile device and checked their device more than twice per night exhibited a substantially elevated risk of experiencing a major depressive episode, with a prevalence rate of 38%. This aligns with prior literature that links sleep disruption and elevated depression risk (Andersen et al., 2023; Dissing et al., 2022; Kaya et al., 2021; Wacks & Weinstein, 2021). Additionally, maladaptive coping mechanisms such as screen-based escapism may exacerbate depressive symptoms by displacing restorative activities like sleep or in-person social interaction (Marciano et al., 2022; Pettorruso et al., 2020). The finding specifically underscores a behavioral mechanism of displacement, where device proximity actively and sleep-interrupted device checking interferes with restorative sleep, reinforcing the hypotheses.
One of central objectives of this study was to assess whether personality, gender, and race/ethnicity served as significant factors of the digital media-mental health link. The results confirmed their importance, demonstrating that the risks associated with digital media use and mental health are highly individualized. Personality traits were robustly associated with digital behavior and mental health outcomes. High level of conscientiousness was linked to lower screen time and reduced odds of nighttime device co-sleeping and sleep-interrupted device checking, reflecting the protective role of self-discipline (Kayış et al., 2016; Marciano et al., 2022). In contrast, neuroticism trait was positively associated with screen time, nighttime device co-sleeping, and sleep-interrupted device checking, suggesting a tendency to use digital media as a coping mechanism for emotional distress (Cho et al., 2017; Pettorruso et al., 2020). Critically, neuroticism was also strongly associated with elevated odds of a major depressive episode, confirming its established role as a vulnerability factor for mood disorders that are likely exacerbated by problematic digital engagement.
The study also identified notable gender and racial differences in media use and risk of major depressive episodes. Female participants reported higher rates of major depressive episodes, a finding supported by previous work (Forte et al., 2023). This disparity may reflect gendered experiences with digital media, including greater exposure to appearance-based content, cyberbullying, or social comparison (Fardouly et al., 2018; Orben et al., 2020). Meanwhile, males exhibited higher levels of gaming-related problematic use (Andreassen et al., 2016; Przybylski, 2014; Twenge & Martin, 2020), highlighting the need for gender-sensitive interventions that reflect distinct patterns of digital behavior and risk.
Racial and ethnic differences emerged in both digital use and mental health outcomes. Black participants reported higher levels of screen time, nighttime device co-sleeping, and sleep-interrupted device checking than their White and Hispanic peers. While the study cannot establish causality, this pattern may reflect broader contextual factors such as disparities in access to structured recreational activities, neighborhood safety, or educational resources (Tandon et al., 2021). Conversely, White respondents exhibited higher reported rates of experiencing major depressive episodes. This may be partially influenced by cultural differences in mental health stigma, expression, or help-seeking behavior, although such interpretations require further investigation. These findings suggest that racial disparities in both digital engagement and mental health are shaped by a complex interplay of social, structural, and cultural factors. Taken together, these results point to the importance of intersectional and context-sensitive approaches in developing interventions. Rather than one-size-fits-all strategies, efforts to reduce the mental health risks associated with problematic digital media use may benefit from tailoring based on personality, gender, and racial or ethnic background.
While our findings offer insights into the digital habits of emerging adults, it is critical to interpret these results within the specific context of the FFCWS sample, which is characterized by a higher prevalence of lower-income, urban, and unmarried-parent households. Consequently, the observed associations may be influenced by unique systemic stressors and limited resources specific to this cohort, suggesting that the displacement of healthy behaviors might be exacerbated by environmental constraints rather than individual choice alone.
The findings of this study have important implications for practice, particularly for developing context-specific and individualized interventions. First, Interventions should be context-sensitive and tailored to individual differences. Given the identified differences in risk profiles in gender, race, and ethnicity (Mireku et al., 2019; Orben et al., 2020; Tandon et al., 2021; Twenge & Martin, 2020), interventions should be tailored to the specific digital activities more salient for each group. For example, focusing on social comparison issues for female youth, while addressing compulsive gaming pressures for male youth (Orben et al., 2020; Twenge & Martin, 2020). For Black and Hispanic youth, addressing systemic barriers to alternative activities is important (Hasson, 2018; Mireku et al., 2019; Tandon et al., 2021). Mental health professionals should utilize individualized intake assessments to determine the specific digital activities, personality traits, or socio-cultural contexts that drive screen time, nighttime device co-sleeping, and sleep-interrupted device checking for each individual, allowing for the selection of the most relevant therapeutic module. Second, interventions should integrate digital literacy and behavioral health strategies. While broad workshops are useful (e.g., group school-based interventions on digital literacy and balanced media use), their delivery should be structured to encourage personal reflection on how specific digital risks apply to the students’ unique engagement patterns. Mental health professionals should incorporate screen time and sleep-interrupted behavior assessments in evaluations. Therapies like Cognitive-Behavioral Therapy (CBT) should be adapted to help individuals develop healthier relationships with digital media by specifically targeting their identified triggers rather than simply advocating for general screen reduction (Hrynyschyn & Dockweiler, 2021; Wilhelm et al., 2020). These efforts can promote better mental health outcomes and encourage healthier digital engagement habits across different populations.
This study provides valuable insights but has several limitations. First, its cross-sectional design limits causal inferences between screen time, sleep-interrupted behaviors, and risk of major depressive episodes. Longitudinal studies are needed to examine these relationships over time. Second, self-reported measures may be biased, so future research should use objective data, like screen tracking software. In addition, screen time measure presents limitations. Screen time, as a quantitative metric, does not account for the context, content, type, or purpose of digital engagement, which can vary widely in their psychological impact (Perlmutter et al., 2024; Roberts & David, 2023). Future research should incorporate more nuanced and multidimensional measures of screen use that distinguish between passive versus active engagement, type of content consumed, and situational context. Third, the focus on emerging adults limits generalizability to other age groups, as patterns may differ for adolescents and older adults. Further research should also explore specific types of screen activities and how personality and environmental factors, such as social support and cultural norms, influence the relationship between digital media use and mental health. Addressing these factors can inform more effective interventions. Finally, the low Cronbach’s alpha values for conscientiousness and neuroticism are concerning, as they suggest marginal internal consistency for these revised short scales (Soto & John, 2017). These low values indicate that the abbreviated scales may not adequately capture the full breadth and complexity of the underlying psychological constructs. Future research should consider utilizing the full, established scales for these concepts to ensure greater reliability and validity in measuring these critical personality factors.
Conclusion
This study highlights the complex relationship between screen time, nighttime device co-sleeping, sleep-interrupted device checking, and risk of major depressive episodes among emerging adults, with variations based on personality traits, gender, and race and ethnicity. Excessive screen time and the interaction of nighttime device co-sleeping and sleep-interrupted device checking were significantly associated with higher likelihood of experiencing a major depressive episode, particularly among those with low conscientiousness and high neuroticism. Females reported higher rates of major depressive episodes, while racial disparities revealed distinct patterns in both screen use and mental health outcomes. The study emphasizes the need for interventions targeting maladaptive media behaviors. Policymakers and practitioners should promote balanced media use and healthy lifestyles. Future research should explore longitudinal effects, individual disparities, and the role of socioeconomic and cultural factors in shaping these behaviors.
Supplemental Material
Supplemental Material - Screen Time, Sleep-Interrupted Behaviors, and Depression in a Diverse Sample of Emerging Adults
Supplemental Material for Screen Time, Sleep-Interrupted Behaviors, and Depression in a Diverse Sample of Emerging Adults by Chien-Chung Huang, Bin Tu, and Julia Vallario in Emerging Adulthood
Footnotes
Ethical Considerations
All participants in the Fragile Families and Child Wellbeing Study have consented to have their data used for social research. These procedures, as well as procedures to make de-identified data available to researchers, have been reviewed and approved by the Institutional Review Board of Princeton University (#5767). The procedures for the Fragile Families Challenge have been reviewed and approved by the Institutional Review Board of Princeton University (#8061).
Consent to Participate
Prior to conducting the interview, field staff obtained a signed informed consent form from each participant. Interviewers were instructed to provide time for participants to read the form thoroughly and to offer an opportunity for them to ask any questions regarding their involvement in the study. These procedures were overseen by the Institutional Review Board of Princeton University.
Author Contribution
CH, BT, and JV: conceptualization. CH and BT: methodology and software. CH: resources. CH and BT: validation. CH, BT, and JV: formal analysis. CH, BT, and JV: writing—original draft preparation.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data will be made available on reasonable request.
Permission to reproduce material from other sources
Yes.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.