
Abstract
In this study, we investigated the prospective relationship between maternal behaviors observed during mother-adolescent interactions and the onset of major depressive disorder (MDD) between early and late adolescence (ages 12–18). Maternal expressions of emotion and maternal responses to their child’s expressions of emotion were both examined. Results demonstrated that higher rates of maternal aggressive behavior and lower rates of maternal positive behavior prospectively predicted MDD onset across adolescence. In addition, negative (i.e., aggressive and dysphoric) maternal responses to adolescents’ aggressive and positive behaviors predicted MDD onset. Maternal dysphoric behavior and the way mothers respond to adolescents’ dysphoria were not related to MDD onset. These results extend previous findings on the relationship between parenting behaviors and depression onset in early to midadolescence and suggest that maternal emotion socialization behaviors in early adolescence prospectively predict MDD onset across the entire course of adolescence.
Depression in adolescence is common, with 12% to 28% of young people experiencing an onset of major depressive disorder (MDD) by age 18 or 19 (Lewinsohn, Rohde, & Seeley, 1998; Merikangas et al., 2010). Myriad family factors have been investigated in relation to adolescent depression (Restifo & Bögels, 2009; Sheeber, Hops, & Davis, 2001; Weich, Patterson, Shaw, & Stewart-Brown, 2009), including parental socialization of emotion (PSE), which has been identified as an important and potentially modifiable component of risk (Eisenberg, Cumberland, & Spinrad, 1998; Morris, Silk, Steinberg, Myers, & Robinson, 2007). PSE is defined as parental behaviors that shape the development of children’s understanding, experience, expression, and regulation of emotion (Denham, Bassett, & Wyatt, 2007; Eisenberg et al., 1998; Morris et al., 2007). Two specific PSE behaviors are considered here: (a) maternal expression of emotion, which is thought to shape the emotional climate of the family and influence the emotional development of children through processes such as modeling and social referencing (Halberstadt, Crisp, & Eaton, 1999; Morris et al., 2007); and (b) maternal response to their child’s expression of emotion, which is a more explicit and active process by which mothers shape their child’s emotional development (Denham et al., 2007; Sheeber, Hops, Andrews, Alpert, & Davis, 1998).
Observational research into parental expressions of emotion has revealed that high rates of negative emotion expression (i.e., aggression, dysphoria) and low rates of positive emotion expression are associated with adolescent depressive symptoms, both cross-sectionally and longitudinally (Burge & Hammen, 1991; Messer & Gross, 1995; Schwartz et al., 2012; Sheeber, Davis, Leve, Hops, & Tildesley, 2007; Sheeber & Sorensen, 1998). Observational research into parental responses to youth emotional behaviors has generally been conducted by comparing the family interactions of young people diagnosed with depression or elevated depressive symptoms with the family interactions of nondepressed control participants. Such studies have shown that parental reinforcement of youth sadness or dysphoria (Dadds, Sanders, Morrison, & Rebgetz, 1992; Schwartz et al., 2011; Sheeber, Allen, Davis, & Sorensen, 2000; Sheeber et al., 1998), parental reciprocity of anger (Cook, Asarnow, Goldstein, Marshall, & Weber, 1990; Schwartz et al., 2011), and a lack of parental reinforcement of positive behavior (Cole & Rehm, 1986; Messer & Gross, 1995; Yap, Allen, & Ladouceur, 2008) have all been associated with youth depression. To the best of our knowledge, however, the only published longitudinal research examining family behaviors as predictors of case-level MDD onset is that reported in a previous analysis of the current cohort. Schwartz et al. (2011) reported that the onset of MDD up to midadolescence (i.e., approximately age 15) was prospectively predicted by maternal aggression and dysphoria in response to adolescent aggression, as well as by the suppression of maternal aggression and dysphoria in response to adolescent dysphoria.
The current study fills four important gaps in the existing knowledge base. First, no published research exists on the prospective relationship between maternal expression of emotion and the onset of case-level depressive disorder (as opposed to elevated symptoms) during adolescence. Thus, we do not know whether higher rates of negative maternal behavior and lower rates of positive behavior are present prior to the onset of disorder or whether these behaviors emerge as concomitant or consequent features of adolescent depression. Second, in our previous work, we identified parental response behaviors that prospectively predict depression onset up to age 15 (Schwartz et al., 2011). This work is fundamentally limited by its inability to account for depression onset in the late adolescent years from age 15 to 19, which are the peak years for adolescent-onset depression (Hankin et al., 1998; Kessler, McGonagle, Swartz, Blazer, & Nelson, 1993; Seeley & Lewinsohn, 2009). In the current study, we considered depression onset across the entire course of adolescence, from age 12 to age 18 or 19, thereby providing a comprehensive assessment of the prospective relationship between affective parenting behaviors and adolescent-onset depression. Third, in the current study, we significantly extend previous work by examining both maternal expressions of emotion and maternal responses to their child’s emotions within one study, thereby providing the most thorough examination to date of both individual and interactional maternal socialization behaviors and their prospective relationship with adolescent-onset depression. Fourth, in most observational studies, researchers have collected parenting behavior data only in a single context (usually a family problem-solving discussion designed to elicit conflict) and, thus, cannot address the question whether it is the overall rates of behaviors across contexts or the rates of behaviors within specific types of interactions that are most strongly predictive. In this study, we used observational assessments during interaction tasks designed to differentially elicit positive and negative affect, thereby enabling an explicit examination of the effect of the interactional context, a factor that has been increasingly emphasized as important to the study of affective processes (Aldao, 2013). Our previous work using positive and negative interaction tasks suggests that negative parental behaviors exhibited during a positive task are particularly salient in regard to the prediction of adolescent depression, possibly because they are not elicited by task demands (Schwartz et al., 2011). Although we have not found positive parental behaviors during a negative task to be similarly predictive (Schwartz et al., 2012), there is evidence from the marital literature that the use of positive affect during conflictual discussions is a predictor of both marital stability and marital satisfaction 6 years after the wedding (Gottman, Coan, Swanson, & Carrere, 1998), which suggests that a similar interpersonal process may also corrode parent-child relationships and increase risk for adolescent depression.
In addition to addressing these gaps, this study extends the existing literature by controlling for maternal depressive symptoms in examining the relations between parenting behavior and onset of adolescent MDD. Given that maternal depression has been identified as a risk factor for emergence of depressive disorder and has been shown to affect parenting behaviors (Goodman & Gotlib, 1999; Lovejoy, Graczyk, O’Hare, & Neuman, 2000), we controlled for maternal depressive symptoms and thereby enabled a clearer delineation of the associations between parenting behavior and outcome by removing the variance in maternal parenting behaviors attributable to maternal depressive symptoms per se.
The aim of the current study was to identify maternal socialization behaviors that prospectively predict the onset of case-level MDD across the entire course of adolescence. On the basis of previous findings, we hypothesized that MDD onset would be predicted by higher rates of maternal aggression, lower rates of maternal positivity, negative maternal responses to adolescent aggression and positivity, and the suppression of maternal negativity in response to adolescent dysphoria. In addition, we hypothesized that both negative maternal behaviors during the positive interaction task and positive maternal behaviors during the negative interaction task would predict adolescent depression.
Method
The Orygen Adolescent Development Study (ADS) is a large longitudinal study conducted in Melbourne, Australia. 1 The first wave of intensive data collection (T1) included mother-adolescent interactions, a diagnostic interview to exclude adolescent participants with a history of MDD, and adolescent- and parent-rated questionnaires. Waves 2, 3, and 4 (T2–T4) were conducted approximately 2.5, 4, and 6 years after T1, respectively, and included a diagnostic interview and adolescent- and parent-rated questionnaires.
Recruitment and screening of participants
The recruitment and screening of participants has been reported in detail previously (e.g., Yap, Allen, & Ladouceur, 2008). Screening was conducted to identify a community sample of 10- to 12-year-old primary school students representing the full spectrum of risk for psychopathology as a function of temperament, as measured by the Early Adolescent Temperament Questionnaire–Revised (Ellis & Rothbart, 2001). To ensure equal representation of adolescents at high, medium, and low risk, we selected equal numbers of students with scores on the Negative Affectivity and Effortful Control dimensions of temperament that were 0 to 1, 1 to 2, 2 to 2.5, and more than 2.5 standard deviations above and below the mean. These dimensions were chosen because they have been associated with depressed mood in adolescents (Ellis & Rothbart, 2001). A total of 2,453 students (53.5% of the total sampling population; 52% female, 48% male; mean age = 11.62 years) participated in the screening, from which a sample comprising 415 students was selected on the basis of temperament scores. Of these selected students, 245 participated in the T1 intensive data collection.
Family-interaction data were available for 197 participants. Two adolescents were diagnosed with MDD at T1 and were excluded to enable the study to be prospective in relation to MDD onset, leaving a sample of 195 participants (95 females and 100 males). Of the 195 families, 160 were mother-adolescent dyads and 35 were father-adolescent dyads. Given the low number of participating fathers, only the mother-adolescent dyads were included in the current analyses, leaving a final sample comprising 160 participants. There were no differences between these 160 participants and the remaining 255 of the selected 415 participants with regard to gender, χ2(1, N = 415) = 0.15, n.s., d = 0.04, age, t(413) = 0.19, n.s., d = 0.02, socioeconomic status, t(413) = 0.41, n.s., d = 0.04, or temperament scores on Negative Affectivity, t(413) = 0.16, n.s., d = 0.02, and Effortful Control, t(413) = 0.001, n.s., d < 0.01.
Procedure
Psychosocial assessments at T1 to T4
At each of the four waves of the ADS, adolescents completed a semistructured diagnostic interview and were reimbursed for their time. The T1 interview assessed for current and lifetime episodes of MDD, and the T2 through T4 diagnostic interviews assessed for current MDD and any new episodes of MDD since the date of the last assessment. The rate of participation in each wave is outlined in Figure 1. Diagnostic interview data from all of the time points were integrated by two reviewers (O. S. Schwartz and M. L. Byrne) who made independent ratings and then constructed a consensus variable that indicated whether participants had experienced an onset of MDD at any time between the T1 and T4 time points. This variable was calculated for the 120 participants for whom diagnostic data were available at each time point. Between-group analyses indicated that there were no differences between these 120 participants and the 40 participants with missing data (for whom these data were imputed; see our discussion later) with regard to gender, χ2(1, N = 160) = 0.00, n.s., d < 0.01, socioeconomic status, t(156) = 1.16, n.s., d = 0.22, and T1 scores on Negative Affectivity, t(157) = −0.58, n.s., d = 0.11, Effortful Control, t(158) = 0.58, n.s., d = 0.11, and depression symptoms (as measured by the Centre for Epidemiological Symptoms−Depression scale, CES-D; Radloff, 1977), t(130) = 1.11, n.s., d = 0.22. Participants with missing T1 through T4 MDD-onset data were found to be younger than participants with data, t(158) = 2.40, p = .02, d = 0.44; however, because the average difference in age was approximately 2 months, this difference was not considered developmentally meaningful.

Flowchart of participation across Waves 1 through 4 (T1–T4, respectively).
Family-interaction assessment at T1
Adolescents and mothers completed the lab-based interaction assessment approximately 2 months (range = 0.03–8.04 months) after the psychosocial assessment at T1. Mother-adolescent dyads completed two 20-min interaction tasks that were video recorded for subsequent coding. An event-planning interaction (EPI) was completed first, followed by a problem-solving interaction (PSI). The EPI and PSI tasks were intended to differentially elicit positive and negative behavior, respectively. The ordering of tasks was fixed because of concern that negative affective states elicited by the PSI had the potential to persist into the positive EPI if conducted second (Gilboa & Revelle, 1994).
For the EPI, mothers and adolescents were instructed to plan one or more pleasant activities to do together, with up to five activities chosen on the basis of items that both the mother and adolescent rated as being “very pleasant” on the Pleasant Events Schedule (MacPhillamy & Lewinsohn, 1976). For the PSI, mother-adolescent dyads were instructed to try to resolve one or more issues of disagreement, with up to five issues selected that the mother and adolescent endorsed as occurring the most frequently and generating the highest intensity of anger on the Issues Checklist (Prinz, Foster, Kent, & O’Leary, 1979). One family did not complete the PSI. Mothers and adolescents were reimbursed for their time and travel expenses.
Measures
Living in Family Environments (LIFE) coding system
The LIFE (Hops, Biglan, Tolman, Arthur, & Longoria, 1995) is an observational, microsocial coding system that allows for a detailed analysis of individual family members’ behaviors and interactive family behaviors. The LIFE system consists of 10 nonverbal affect codes (e.g., anger, dysphoria, happy) and 27 verbal content codes (e.g., validation, complaint, provoke). To code the video-recorded interactions, we used an event-based protocol in which new codes were entered each time the affect or content of one of the interactants changed. The affect and content codes were used to develop composite behavior constructs. In this study, the constructs were aggressive, dysphoric, and positive behaviors. The aggressive construct included all behaviors with contemptuous, angry, or belligerent affect, as well as cruel, provocative, annoying/disruptive, or argumentative verbal statements made with neutral affect. The dysphoric construct consisted of all behaviors with dysphoric, anxious, or whining affect, as well as complaints and self-derogatory verbal comments made with neutral affect. The positive construct included all behaviors with happy or caring affect as well as approving, validating, affectionate, or humorous comments made with neutral affect.
We used the LIFE data to construct two variables representing maternal socialization behaviors. First, the rate-per-minute variables were used to measure maternal expression of emotion. These variables indicate the average number of times a mother expressed each behavior type (i.e., aggressive, dysphoric, and positive) per minute and were calculated separately for the EPI and PSI. Second, the conditional probabilities of negative maternal behaviors occuring in response to adolescent behaviors were measured using behavior sequences in which adolescents’ aggressive, dysphoric, and positive behaviors were followed by maternal aggressive and dysphoric behaviors. These behavior sequences were selected for analysis on the basis of previous research (Schwartz et al., 2011, 2012; Yap, Allen, & Ladouceur, 2008). The conditional probability of a particular maternal behavior occurring immediately after a particular adolescent behavior was calculated by dividing the number of times the particular adolescent behavior was followed by the particular maternal behavior by the base rate (i.e., total frequency) of the particular adolescent behavior (Gottman & Roy, 1990). We then used these conditional probabilities to calculate Allison-Liker z scores (Allison & Liker, 1982), using a binomial test that also takes into account the base rate of the maternal behaviors. The z scores thus reflect the extent to which a specified sequence of behavior occurred more or less frequently than would be expected as a function of the base rate of each behavior based on a normal distribution.
Coders were extensively trained and blind to the clinical and demographic characteristics of the participants. Approximately 20% of the interactions were coded by a second observer to provide an estimate of observer agreement. Random pairs of observers were assigned to the interactions to minimize “drift” between any two observers. Interobserver agreement was assessed using kappa, a conservative index that controls for chance agreement (Fleiss, 1981). Kappa coefficients for the aggressive, dysphoric, and positive behavior constructs were .70, .60, and .86, respectively, across interactants. The validity of the LIFE system as a measure of family processes has been established in numerous studies (e.g., Katz & Hunter, 2007; Sheeber et al., 2007).
Schedule for Affective Disorders and Schizophrenia for School-Age Children, Present and Lifetime version (K-SADS-PL)
The K-SADS-PL (Kaufman et al., 1997) is a semistructured diagnostic interview assessing current and lifetime symptoms and diagnoses of Axis I disorders in youths aged 6 to 18 years. The K-SADS-PL has demonstrated good interrater agreement, test-retest reliability, and diagnostic validity (Kaufman et al., 1997). Recordings of 20% to 25% of all K-SADS-PL interviews at each of the four ADS waves of data collection were rerated by a second coder. The kappa coefficient for symptom-level agreement was 0.80 at T1, 0.78 at T2, 0.86 at T3, and 0.81 at T4, which suggests excellent interrater reliability across diagnoses at all time points (Kaufman et al., 1997).
CES-D
The CES-D (Radloff, 1977) is a 20-item self-report questionnaire designed to measure depression symptoms in the general population. Higher scores indicate greater frequency and number of depression symptoms. The CES-D was used to quantify levels of depressive symptoms among mothers who took part in the study.
Results
Descriptive analyses
Table 1 shows the rate of first-onset MDD at each of the three follow-up time points and the total number of participants who experienced first-onset MDD following the T1 assessment. Overall, significantly more females than males experienced MDD onset during the follow-up period, χ2(1, N = 120) = 6.14, p = .013.
Rates of Major Depressive Disorder Onset Between Time 2 and Time 4
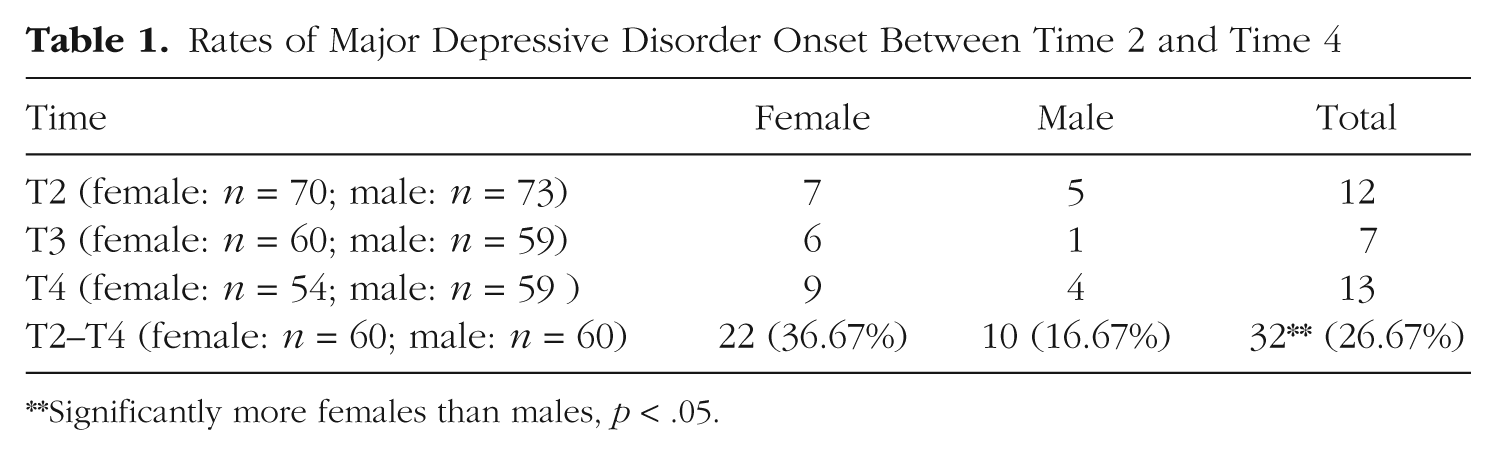
Significantly more females than males, p < .05.
Design of path analyses
Four path analyses were used to test whether maternal PSE behaviors prospectively predicted MDD onset across adolescence. Two models assessed the association between the rate per minute of the three maternal behavior constructs and MDD onset, with separate models specified using data from the EPI and PSI, and two models assessed the association between negative maternal responses (i.e., aggressive and dysphoric) to adolescent aggressive, dysphoric, and positive behavior and MDD onset, with separate models specified for data taken from the two tasks. In all models, we controlled for maternal depression in the prediction of the observed maternal behavior variables and for the duration of time between the T1 psychosocial and family-interaction assessments on the MDD-onset outcome variable (see Figs. 2–5; for ease of presentation, the figures do not show the paths representing the regression of MDD onset on the duration of time between the T1 assessments or the covariances between the observed parenting variables). Path analyses were run using Mplus software (version 7.11) and weighted least squares mean- and variance-adjusted estimation. Missing data were estimated using full-information maximum likelihood in Mplus. Full-information maximum likelihood yields comparatively good standard errors and is efficient in evaluating parameter significance with missing categorical data (Graham, 2009; Wothke, 2000).
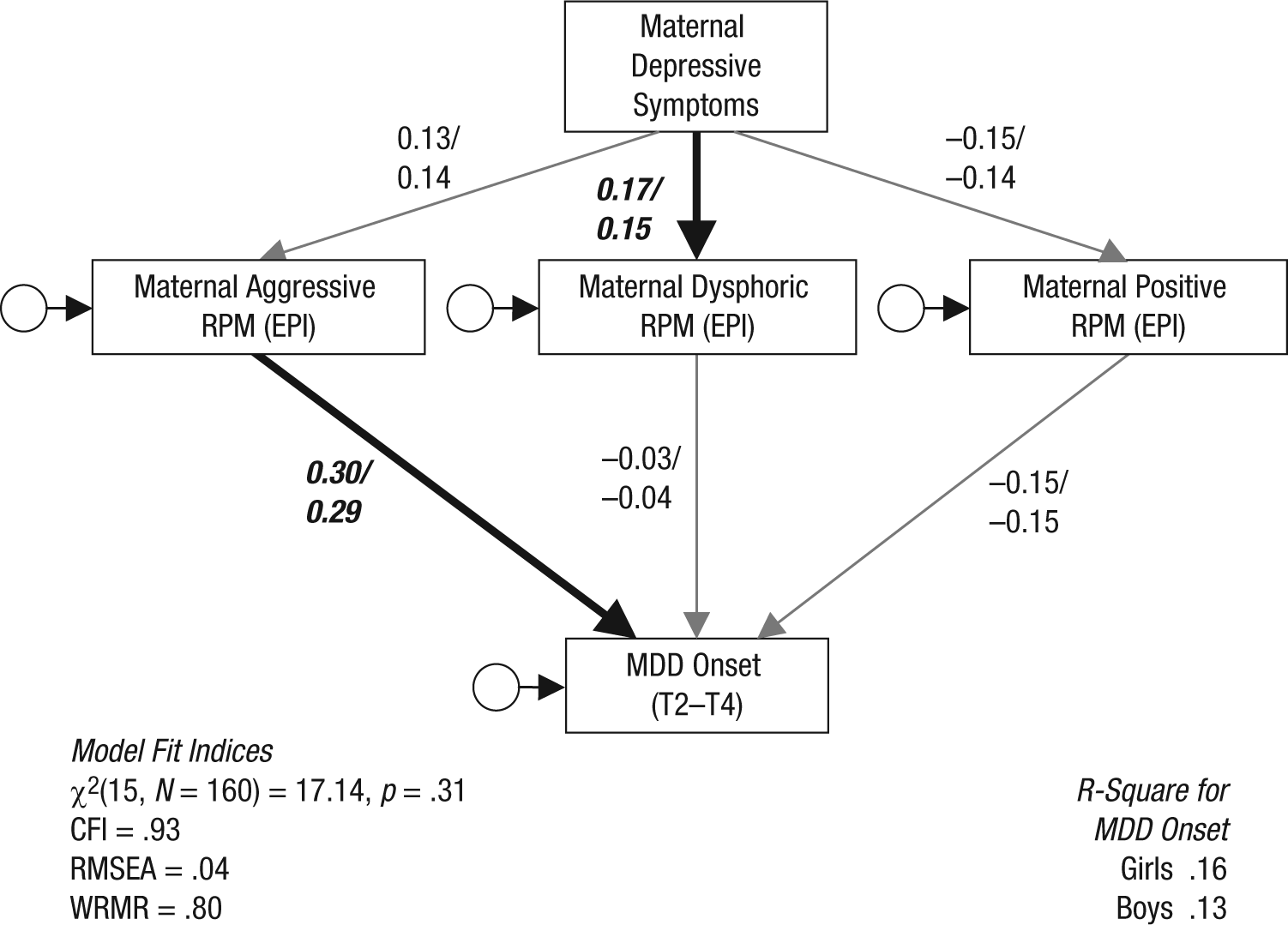
The influence of rates of maternal behaviors during the EPI on MDD onset across adolescence. Thick black arrows represent significant regression paths for girls and boys. Thin grey arrows represent nonsignificant regression paths for girls and boys. Data for girls are provided on the left side of the forward slash. RPM = rate per minute; EPI = event-planning interaction; MDD = major depressive disorder; CFI = comparative fit index; RMSEA = root-mean-square error of approximation; WRMR = weighted root-mean-square residual; T2–T4 = Waves 2–4.
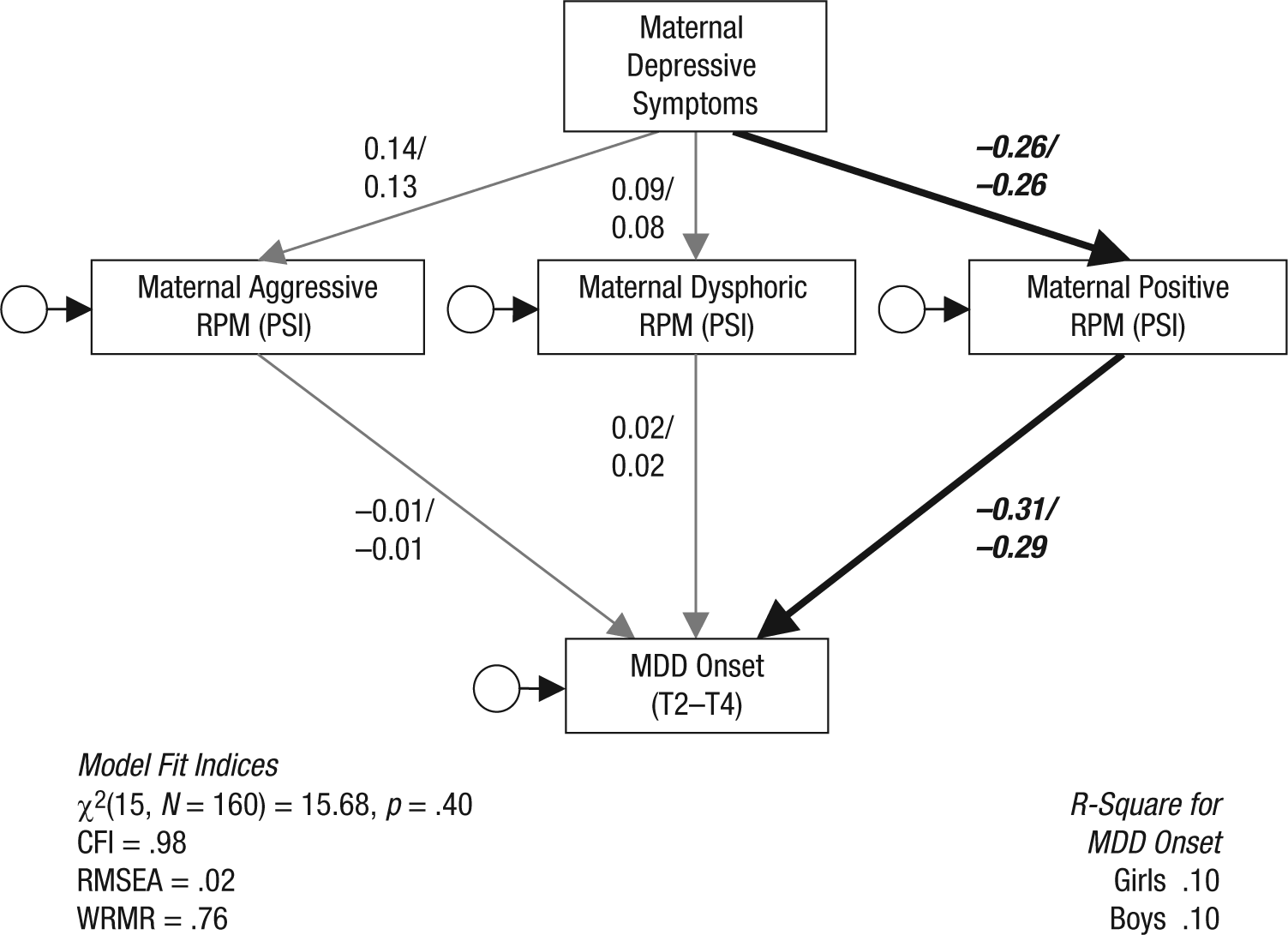
The influence of rates of maternal behaviors during the PSI on MDD onset across adolescence. Thick black arrows represent significant regression paths for girls and boys. Thin grey arrows represent nonsignificant regression paths for girls and boys. Data for girls are provided on the left side of the forward slash. RPM = rate per minute; PSI = problem-solving interaction; MDD = major depressive disorder; CFI = comparative fit index; RMSEA = root-mean-square error of approximation; WRMR = weighted root-mean-square residual; T2–T4 = Waves 2–4.
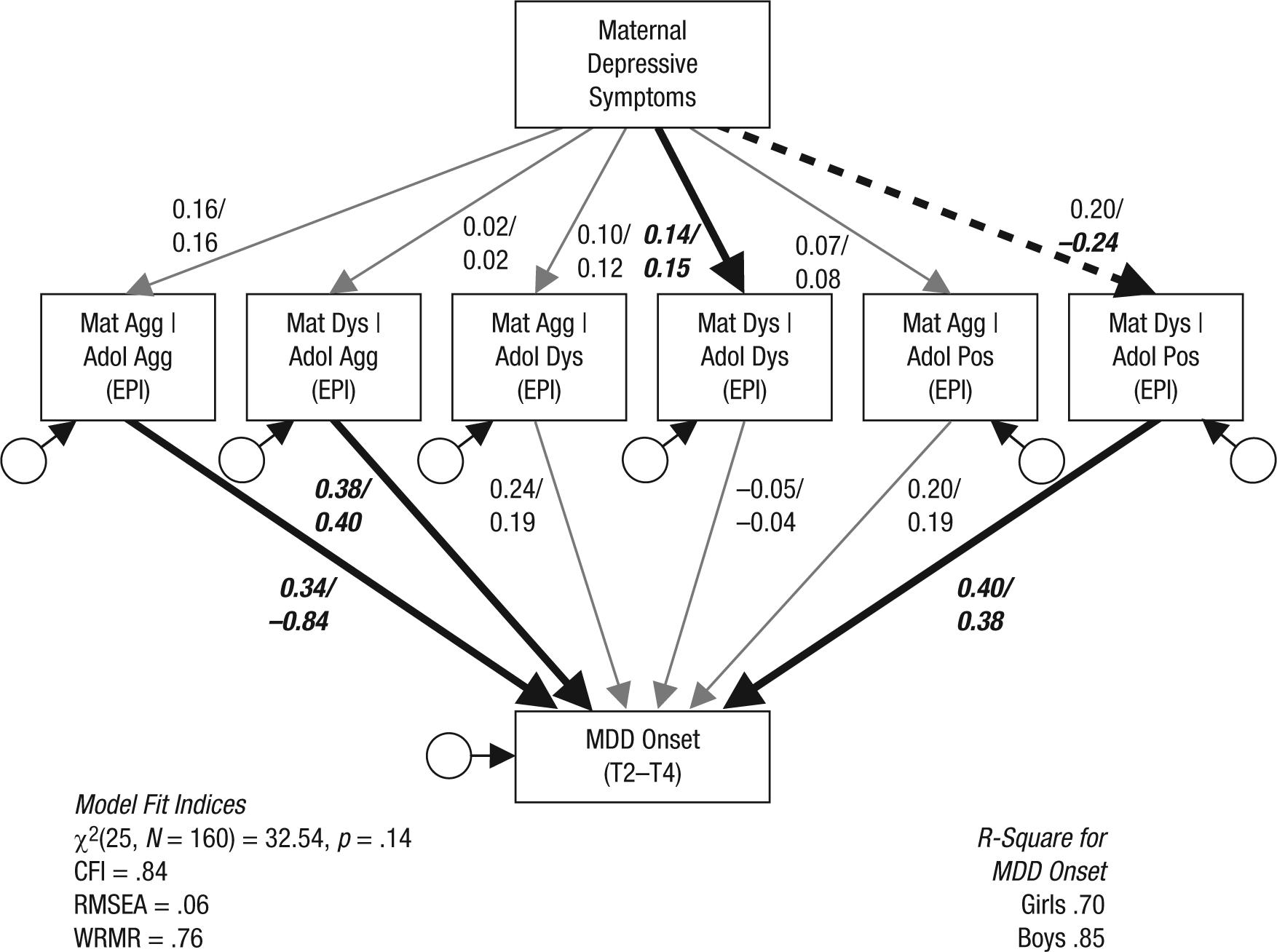
The influence of maternal response behaviors during the EPI on MDD onset across adolescence. Thick black arrows represent significant regression paths for girls and boys. Thick dashed arrows represent regression paths that are significant for boys but not girls. Thin grey arrows represent nonsignificant regression paths for girls and boys. Data for girls are provided on the left side of the forward slash. Mat = maternal; Agg = aggressive; Dys = dysphoric; Pos = positive; | = given; Adol = adolescent; EPI = event-planning interaction; MDD = major depressive disorder; CFI = comparative fit index; RMSEA = root-mean-square error of approximation; WRMR = weighted root-mean-square residual; T2–T4 = Waves 2–4.
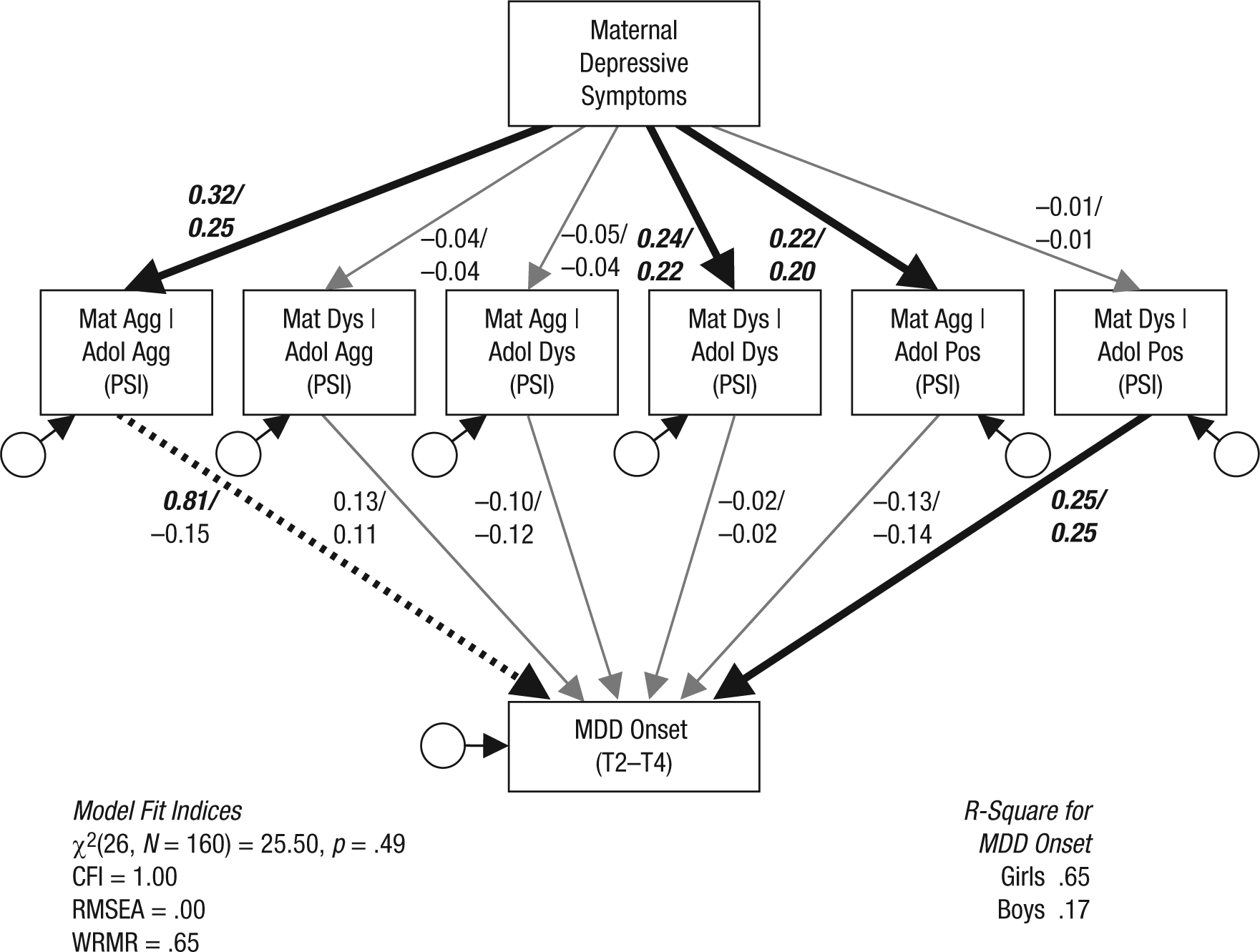
The influence of maternal response behaviors during the PSI on MDD onset across adolescence. Thick black arrows represent significant regression paths for girls and boys. Thick dotted arrows represent regression paths that are significant for girls but not boys. Thin grey arrows represent nonsignificant regression paths for girls and boys. Data for girls are provided on the left side of the forward slash. Mat = maternal; Agg = aggressive; Dys = dysphoric; Pos = positive; | = given; Adol = adolescent; PSI = problem-solving interaction; MDD = major depressive disorder; CFI = comparative fit index; RMSEA = root-mean-square error of approximation; WRMR = weighted root-mean-square residual; T2–T4 = Waves 2–4.
Analysis of adolescent gender
A multiple-group analysis was employed in all models to test the invariance of regression parameters across adolescent gender (Muthén & Muthén, 1998–2012). All parameter estimates corresponding to regression coefficients initially were constrained to be equal across groups. Following the procedure recommended by Muthén and Muthén (1998–2012), we sequentially released constrained parameters with a modification index of approximately 2 or more in both groups and reran the model. A chi-square difference test determined whether releasing the identified parameter resulted in a significant improvement in model fit. No modifications were made to the two models analyzing the rate-per-minute variables, which suggested no significant gender moderation in these models. In both models analyzing the conditional probability variables, the gender equality constraint was released for the regression of MDD onset on the conditional probability of maternal aggressive behavior given adolescent aggressive behavior—EPI: χ2diff(1, N = 160) = 13.27, p < .001; PSI: χ2diff(1, N = 160) = 9.62, p = .002. And in the EPI, the regression of the conditional probability of maternal dysphoria given adolescent positivity on maternal depressive symptoms was also released, χ2diff(1, N = 160) = 6.69, p = .01, which indicated gender moderation of these paths.
Path analysis results
Model fit indices showed that the final version of all models provided an acceptable fit to the data (see Figs. 2–5).
Maternal depressive symptoms
Results showed that higher levels of maternal depressive symptoms predicted higher rates of maternal dysphoric behavior in the EPI—Girls: β = 0.17, 95% confidence interval (CI) = [0.04, 0.29]; Boys: β = 0.15, 95% CI = [0.03, 0.26]. Higher levels of maternal depressive symptoms also predicted lower rates of maternal positivity in the PSI—Girls: β = −0.26, 95% CI = [–0.42, –0.10]; Boys: β = −0.26, 95% CI = [–0.42, –0.11] (see Tables 2 and 3 for regression parameter estimates). In both interactions, maternal depressive symptoms were also associated with an increased likelihood of mothers’ reciprocating their adolescent’s dysphoric behavior—EPI Girls: β = 0.14, 95% CI = [0.01, 0.26]; EPI Boys: β = 0.15, 95% CI = [0.01, 0.29]; PSI Girls: β = 0.24, 95% CI = [0.09, 0.40]; PSI Boys: β = 0.22, 95% CI = [0.07, 0.36]. In the EPI, maternal depressive symptoms were associated with a lower likelihood of responding with dysphoria to boys’ positivity, β = −0.24, 95% CI = [–0.44, –0.04]. In the PSI, maternal depressive symptoms were associated with an increased likelihood of mothers’ both reciprocating aggression, Girls: β = 0.32, 95% CI = [0.12, 0.51]; Boys: β = 0.25, 95% CI = [0.11, 0.39], and responding with aggression to adolescent’s positivity—Girls: β = 0.22, 95% CI = [0.10, 0.33]; Boys: β = 0.20, 95% CI = [0.08, 0.31].
Regression Parameter Estimates for Rate-Per-Minute Data
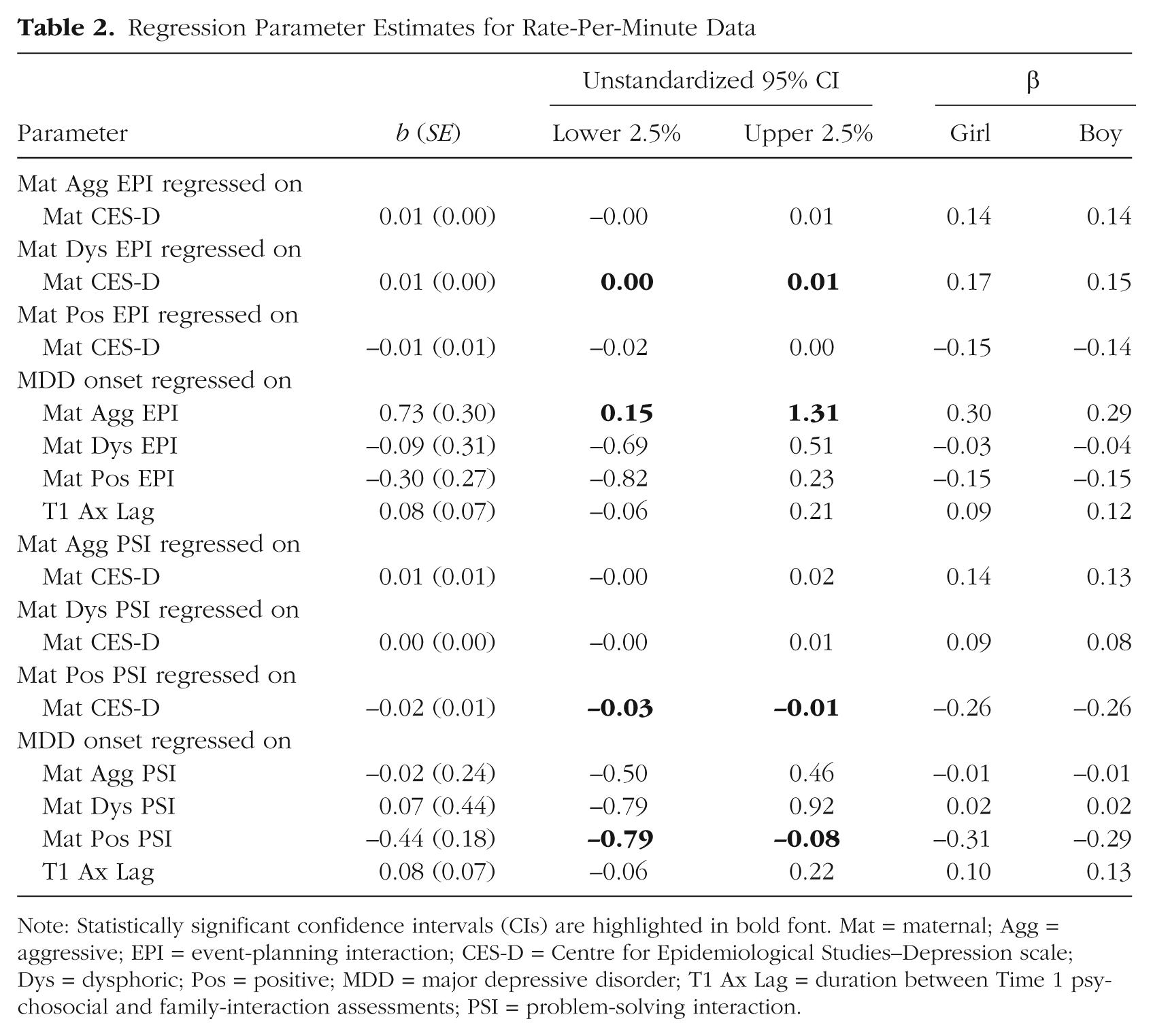
Note: Statistically significant confidence intervals (CIs) are highlighted in bold font. Mat = maternal; Agg = aggressive; EPI = event-planning interaction; CES-D = Centre for Epidemiological Studies–Depression scale; Dys = dysphoric; Pos = positive; MDD = major depressive disorder; T1 Ax Lag = duration between Time 1 psychosocial and family-interaction assessments; PSI = problem-solving interaction.
Regression Parameter Estimates for Conditional Probability Variables
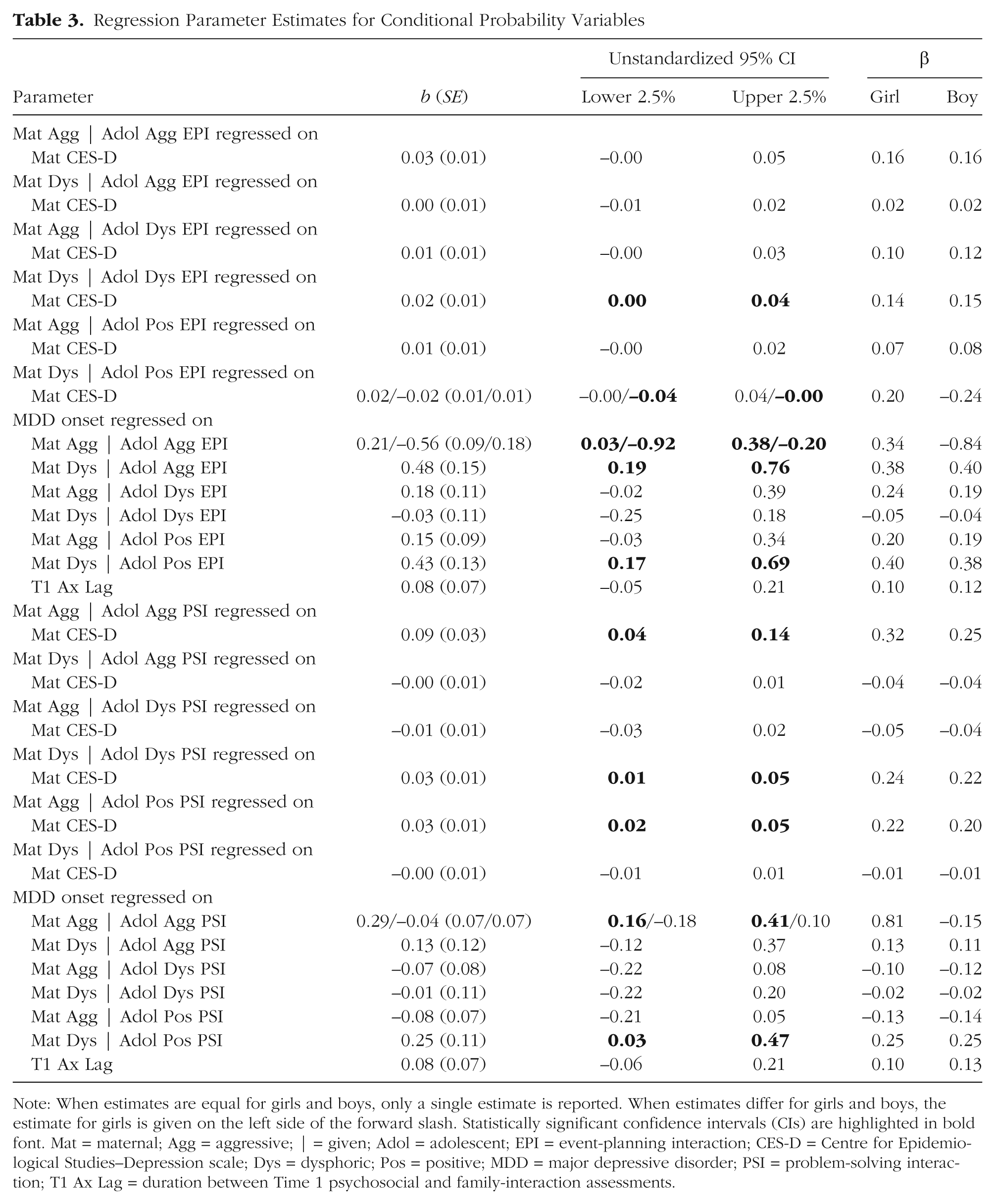
Note: When estimates are equal for girls and boys, only a single estimate is reported. When estimates differ for girls and boys, the estimate for girls is given on the left side of the forward slash. Statistically significant confidence intervals (CIs) are highlighted in bold font. Mat = maternal; Agg = aggressive; | = given; Adol = adolescent; EPI = event-planning interaction; CES-D = Centre for Epidemiological Studies–Depression scale; Dys = dysphoric; Pos = positive; MDD = major depressive disorder; PSI = problem-solving interaction; T1 Ax Lag = duration between Time 1 psychosocial and family-interaction assessments.
Maternal socialization behaviors and MDD onset
After accounting for the influence of maternal depressive symptoms on the maternal socialization behaviors, we found that a number of these behaviors prospectively predicted MDD onset in adolescents. Table 2 shows that for both girls and boys, MDD onset during adolescence was prospectively predicted by higher rates of maternal aggressive behavior during the EPI, Girls: β = 0.30, 95% CI = [0.06, 0.55]; Boys: β = 0.29, 95% CI = [0.06, 0.51], and by lower rates of maternal positive behavior during the PSI—Girls: β = −0.31, 95% CI = [–0.56, –0.05]; Boys: β = −0.29, 95% CI = [–0.52, –0.05]. Rates of maternal dysphoric behavior did not predict MDD onset in either model.
Table 3 shows that maternal responses to both adolescent aggression and positivity prospectively predicted MDD onset in adolescence. Specifically, adolescent girls were at increased risk for MDD onset when their mothers were more likely to reciprocate their expressions of aggression in both the EPI, β = 0.34, 95% CI = [0.05, 0.62], and the PSI, β = 0.81, 95% CI = [0.53, 1.08]. In contrast, adolescent boys were at increased risk for MDD onset when their expression of aggression suppressed their mothers’ aggression during the EPI, β = −0.84, 95% CI = [–1.36, –0.32], but this behavior sequence during the PSI was not associated with MDD onset in boys, β = −0.15, 95% CI = [–0.62, 0.32]. Both girls and boys were at increased risk of MDD onset when their mothers responded with dysphoric behavior to the adolescents’ expression of aggression during the EPI but not during the PSI—EPI Girls: β = 0.38, 95% CI = [0.14, 0.62]; EPI Boys: β = 0.40, 95% CI = [0.15, 0.64]; PSI Girls: β = 0.13, 95% CI = [–0.12, 0.37]; PSI Boys: β = 0.11, 95% CI = [–0.10, 0.32]. Finally, adolescents whose mothers were more likely to respond with dysphoric behavior to the adolescents’ expression of positivity in both interaction tasks were at increased risk of MDD onset—EPI Girls: β = 0.40, 95% CI = [0.16, 0.65]; EPI Boys: β = 0.38, 95% CI = [0.14, 0.62]; PSI Girls: β = 0.25, 95% CI = [0.03, 0.47]; PSI Boys: β = 0.25, 95% CI = [0.02, 0.48]. Maternal responses to adolescent dysphoric behavior and maternal aggressive responses to adolescent positivity were not prospectively associated with MDD onset.
Discussion
The results showed that higher rates of maternal aggressive behavior and lower rates of maternal positive behavior prospectively predicted the onset of MDD across adolescence. Consistent with previous findings, our findings showed that there was no evidence that maternal expressions of dysphoria were associated with MDD onset. In addition, we found that maternal aggressive responses to adolescent aggression predicted adolescent-onset MDD in girls, whereas the suppression of maternal aggression in response to adolescent aggression was associated with risk for MDD onset for boys. In both boys and girls, maternal dysphoric responses to adolescent aggression and positivity prospectively predicted MDD onset across adolescence. However, there was no evidence that maternal responses to adolescent dysphoria were associated with MDD onset. Overall, these results indicate that maternal expression of emotion and the way mothers respond to their child’s expression of emotion during early adolescence are prospectively associated with MDD onset across the entire course of adolescence. It is important to note that we controlled for the influence of maternal depressive symptoms on maternal behaviors and, thus, discounted the possibility that the observed relationships were purely attributable to the effects of maternal depression on parenting (which were again demonstrated in this study).
The finding that MDD onset across adolescence was prospectively predicted by both aggressive and positive maternal behaviors is consistent with findings from previous research that have respectively associated negative and positive parental behaviors with higher and lower levels of depressive symptoms over time (Burge & Hammen, 1991; Schwartz et al., 2012; Sheeber, Hops, Alpert, Davis, & Andrews, 1997). The current findings demonstrate that such parenting behaviors also prospectively predict the onset of case-level depressive disorder across adolescence.
As predicted, the affective context of family interactions appeared to play an important role in determining the predictive salience of some maternal socialization behaviors. Specifically, rates of maternal aggressive behavior during the positive EPI task significantly predicted MDD onset (even though rates of maternal aggression were higher during the PSI), whereas rates of maternal positive behavior during the negative PSI task were associated with risk for MDD onset. Thus, the predictive maternal behaviors occurred during tasks that were not designed to elicit these behaviors. It is possible that the predictive importance of maternal behaviors is contextually determined and not based simply on the rates of these behaviors. Specifically, adolescents whose mothers behave aggressively when asked to discuss something pleasant with their child, or who display low levels of positivity when attempting to resolve a conflictual topic, may be at particular risk for depression onset across the course of their adolescence.
However, the interactional context was less differentiating in relation to the results based on mothers’ responses to adolescent emotional behavior. Rather, the results across both tasks were similar in suggesting that maternal responses to adolescent aggression and positivity are particularly relevant in relation to MDD onset, whereas maternal responses to dysphoria are not.
Links between aggressive or angry behavior and depression have been well documented (e.g., Painuly, Sharan, & Mattoo, 2005; Safer, 2009). We speculate that our findings might suggest that the way young people are socialized in relation to their anger and, thus, how they learn to regulate their anger may be particularly important for the development of depression across adolescence (Jackson, Kuppens, Sheeber, & Allen, 2011). Our findings regarding the reciprocation of aggressive behavior were different for girls and boys, which suggests that different family-interaction processes may be operating (Cassano, Perry-Parrish, & Zeman, 2007; Eisenberg et al., 1998). For girls, it may be that maternal reciprocity of aggression is particularly stressful, or this finding might reflect a more conflictual mother-daughter relationship for girls who go on to develop depression. For boys, the reverse may be true, in that maternal suppression of aggression in response to their sons’ aggression may function as a negative reinforcement of this behavior and could possibly increase vulnerability to depression through an externalizing pathway (Kendler, Gardner, & Prescott, 2006).
Consistent with the findings in our earlier work with this sample, in which we investigated predictors of MDD onset in midadolescence, our current results showed that maternal dysphoric responses to adolescent aggression prospectively predicted MDD onset into late adolescence, which speculatively could indicate a maladaptive form of conflict resolution that prevents adolescents from learning optimal aggression-regulation strategies. Overall, our findings suggest that the way mothers respond to adolescent aggressive behavior, or the way that conflict is managed within the family, may be particularly important predictors of future depression.
Our findings also highlight that maternal dysphoric responses to adolescent positivity are prospectively associated with MDD. A study based on the first wave of the ADS data demonstrated a cross-sectional association between this behavior sequence (referred to as “dampening”) and depressive symptoms in early adolescence (Yap, Allen, & Ladouceur, 2008), and the current findings are the first to suggest that such behaviors are also prospectively associated with case-level MDD onset across adolescence. In particular, maternal dampening of adolescent positivity, or the failure to appropriately reinforce positivity, may be associated with difficulty upregulating positive emotion, which may create vulnerability to depression, particularly in relation to the anhedonic features of this disorder (Feng et al., 2009; Silk, Shaw, Forbes, Lane, & Kovacs, 2006).
We previously found that the suppression of maternal aggression in response to adolescent dysphoria predicted MDD onset in early to midadolescence (Schwartz et al., 2011); however, this finding did not replicate in the current analyses, in which depression onset was examined into late adolescence, and thereby suggests that this association may be more proximal and may wash out over longer time frames.
The absence of significant findings relating to rates of maternal dysphoria and maternal responses to adolescent dysphoria is puzzling given the critical role of dysphoric affect in MDD. A possible explanation is that although parental socialization processes are important in the development of aggressive and positive emotion regulation abilities across the entire duration of adolescence, these family processes do not significantly shape the development of the regulation of dysphoric emotions during this time.
The primary strength of the current study is its prospective, longitudinal design, which enabled the examination of potential risk factors for MDD onset across the entire course of adolescence. In addition, the observational measurement of maternal socialization behaviors allowed for a relatively objective assessment of maternal behavior, and the observation of behavior across two affective contexts permitted the identification of context-specific family processes that predict MDD onset. Finally, our use of the LIFE coding system enabled the differentiation of aggressive and dysphoric behaviors, which are often combined and considered together as negative behaviors. Our work suggests important differences in relation to these affective behaviors and highlights the importance of considering them independently.
A limitation of this study is the inability to validly examine fathers’ behavior because of the low number of participating fathers. Fathers play a significant role in the socialization of emotion in their children, and the findings relating to mothers’ socialization behaviors may not generalize to fathers (Cassano, Adrian, Veits, & Zeman, 2006; Jacob & Johnson, 2001; Sheeber et al., 2007). Furthermore, maternal and paternal socialization behaviors may interact in important ways such that they may be additive or may buffer the effects of the other parent on child outcomes.
In addition, as a result of the low power associated with examining the onset of other disorders with lower incidence rates, only MDD outcomes have been considered in the current analyses. Hence, it is unknown whether the maternal socialization behaviors identified as prospective predictors are specific to risk for depression or whether they represent a more general vulnerability to psychopathology across adolescence.
Finally, although these findings are prospective and longitudinal, they are correlational. Prospective longitudinal designs are considered more powerful than are cross-sectional designs because they can explicitly test the directionality of effects and discount the possibility that observed relationships are solely due to state-dependent factors (Cowan & Cowan, 2002; Sheeber et al., 2001). However, the current findings could be attributed to one of three possible scenarios: (a) Parenting behaviors may influence the onset of adolescent depression, (b) adolescent characteristics at baseline may elicit parenting behaviors, or (c) an unmeasured factor may account for both parenting behaviors and the development of depression (Garber, Robinson, & Valentiner, 1997). Researchers have argued that intervention studies showing that an improvement in parenting is related to an improvement in symptoms, or the prevention of depression onset (e.g., Compas et al., 2009; Compas et al., 2010; Compas et al., 2011), offer the most convincing evidence about the directionality of influence (Cowan & Cowan, 2002). However, prospective studies are required to identify mechanisms to target in intervention studies. Future research could help to elucidate the question of causality by applying the findings of the current study to a clinical prevention trial.
In addition, the question of directionality of effects could be more comprehensively investigated by conducting multiple family-interaction assessments over time. Such assessments would also help to determine whether parenting during early adolescence continues to be associated with depression onset in late adolescence after controlling for more proximal assessments of parenting.
The importance of considering context when observing parenting behaviors has been highlighted in the current study, and in future studies, researchers should consider including an interaction task explicitly designed to elicit depressive affect. The inclusion of such a task may be particularly important in light of the current study’s failure to identify significant predictors in relation to dysphoric behavior.
Finally, the findings of this study also clearly indicate the need for more research into the potentially protective behaviors mothers could use when responding to their child’s aggression, dysphoria, and positivity because the current study has primarily identified potential risk rather than protective factors. For example, the exploration of emotion-coaching techniques may provide an adaptive alternative response that could be offered to parents in intervention research (Gottman, Katz, & Hooven, 1997; Shortt, Sheeber, Low, & Katz, 2010; Stocker, Richmond, Rhoades, & Kiang, 2007).
Footnotes
Declaration of Conflicting Interests
The authors declared that they had no conflicts of interest with respect to their authorship or the publication of this article.
Funding
This research was supported by grants from the Colonial Foundation, the National Health and Medical Research Council Australia (Program Grant 350241), and the Australian Research Council (Discovery Grant DP0878136).