
Abstract
African American youth who experience racial discrimination are at heightened risk to use drugs as a coping response to distress. Based on the buffer-stress hypothesis, we proposed that parental support would attenuate this effect. Participants were 1,521 African American youth between 4th and 12th grade. As hypothesized, a mediation pathway was observed among racial discrimination, depression symptoms, and drug use. This effect was observed for both genders, although the pathway was partially mediated for males. In addition, as hypothesized, parental support buffered the negative effect of depression symptomatology on drug use as a consequence of discrimination. Our findings highlight the impact racial discrimination has on health outcomes for African American youth and the importance of managing youths’ emotional responses to discrimination. Moreover, findings illuminate the protective role of supportive parenting within the risk model and should thus be considered as an important component within prevention programming for this population of youth.
Keywords
Despite ongoing prevention efforts, alcohol and marijuana continue to be used at staggering rates among youth in the United States. By the end of high school, approximately two thirds of adolescents report use of alcohol and nearly half report use of marijuana (Johnston, Miech, O’Malley, Bachman, & Schulenberg, 2015). Drug use during this developmental period is also of concern due to the considerable health and social consequences associated with use, including increased risk for violent or delinquent behavior, risky sexual behavior, impairments in critical thinking and memory, stagnation of brain development, negative academic performance, family and interpersonal problems, and drug-related injuries and illness (Bryant & Zimmerman, 2002; Gil, Wagner, & Tubman, 2004; Larm, Hodgins, Larsson, Samuelson, & Tengström, 2008; Volkow, Baler, Compton, & Weiss, 2014). It is striking that many of these consequences are found at disproportionately higher rates among African American youth compared with their peers, even at comparable levels of use (Golub, Johnson, & Dunlap, 2007; Maag & Irvin, 2005; Ramchand, Pacula, & Iguchi, 2006; Welte & Barnes, 1987). Moreover, current risk models aimed at understanding vulnerability to drug use and the experience of subsequent negative outcomes have largely failed to adequately explain variation in risk for African American youth (Bersamin, Paschall, & Flewelling, 2005; J. M. Wallace & Muroff, 2002). Thus, it has been postulated that variables associated with risk in the general population may or may not be salient to African American youth and their experiences, and therefore culturally specific risk models are necessary to better understand vulnerability to drug use among this population of youth (Brown, Miller, & Clayton, 2004; Burlew, Feaster, Brecht, & Hubbard, 2009; Chartier, Hesselbrock, & Hesselbrock, 2009; J. M. Wallace & Muroff, 2002).
Discrimination, Negative Affect, and Drug Use
Within race-specific risk models, the experience of discrimination has been highlighted as an important psychosocial factor for a number of negative behavioral, psychological, and health outcomes among African American populations (e.g., Gibbons, Gerrard, Cleveland, Wills, & Brody, 2004; Pachter & Coll, 2009; Williams & Mohammed, 2009). This platform is based on research documenting that African American youth and adults report greater experiences of discrimination relative to other ethnic/racial groups (Kessler, Mickelson, & Williams, 1999; Phinney & Chavira, 1995; Sellers, Copeland-Linder, Martin, & Lewis, 2006), and associations between racial discrimination experiences and mental health are stronger among African Americans (Kessler et al., 1999). Thus, it has been conceptualized that racial discrimination leads to both negative mental health outcomes (e.g., depression, sadness, anger, frustration) and engagement in drug use and other health risk behaviors as a coping response to such stress (R. Clark, Anderson, Clark, & Williams, 1999).
Findings support this hypothesis with racial discrimination associated with increased risk for drug use (Brody, Kogan, & Chen, 2012; Fuller-Rowell et al., 2012; Gibbons et al., 2004; Guthrie, Young, Williams, Boyd, & Kintner, 2002) and internalizing outcomes (i.e., depression and anxiety) among African American youth (Gibbons et al., 2007; Hurd, Varner, Caldwell, & Zimmerman; 2014). Path models have also documented that drug use and psychological outcomes interact, such that racial discrimination increases vulnerability to negative affect, which in turn increases risk for drug use (T. T. Clark, 2014; Gibbons et al., 2004; Gibbons et al., 2014). For example, Sanders-Phillips and colleagues (2014) conducted a study among 567 African American high school students, finding that the experience of perceived racial discrimination was linked to greater depressive symptomatology, which was subsequently associated with greater alcohol and marijuana use.
Although the literature has provided robust support on the negative impact racial discrimination has on psychological and behavioral health outcomes among African American youth, gender differences have also been observed within this risk model. Specifically, existing literature has documented higher rates in depression symptoms among females (Hasin, Goodwin, Stinson, & Grant, 2005) and higher rates of reported discriminatory encounters (Banks, Kohn-Wood, & Spencer, 2006; Sellers & Shelton, 2003) and drug use among males (Chen & Jacobson, 2012). However, findings are less consistent when examining gender difference within the risk pathway between racial discrimination and drug use. For example, two recent studies by Brodish and colleagues (2011) and Wiehe, Aalsma, Liu, and Fortenberry (2010) found a strong and positive association between the experience of racial discrimination and subsequent drug use for African American males, with a negative or null relationship observed for African American females. Among studies where depression was the outcome variable of interest, a stronger association was found between discrimination and depressive symptomatology for African American females compared with males (English, Lambert, & Ialongo, 2014). Yet, when examining the mediating role of depressive symptomatology, although it has been postulated that this effect may be stronger for females (Nolen-Hoeksema, Larson, & Grayson, 1999), comparable effects have been found across gender (Boynton, O’Hara, Covault, Scott, & Tennen, 2014; Hurd et al., 2014). Thus, although gender differences are found between the direct link between discrimination and depression or drug use, these differences appear to not be present when examining the total mediation pathway.
Protective Effect of Parenting
Developmental models have also identified important protective factors that can attenuate risk for drug use among adolescent populations. Among such studies, supportive parenting has been identified as a critical protective factor within the risk process (Eisman, Stoddard, Heinze, Caldwell, & Zimmerman, 2015; Gibbons et al., 2004; Hazel, Oppenheimer, Technow, Young, & Hankin, 2014; Hemovich, Lac, & Crano, 2011; Ryan, Jorm, & Lubman, 2010; Schmeelk-Cone & Zimmerman, 2003; Wills, Gibbons, Gerrard, & Brody, 2000). It has been postulated that parental support is protective for youth because it fosters a closer bond between the parent and child, which allows for more open communication within the parent–child relationship and a sense of security for the child (Bowlby, 1973). Moreover, this secure bond helps prepare adolescents to safely negotiate autonomy and to adaptively manage stressors that may occur throughout their life (Parker & Benson, 2004). Thus, although parental support has a similar protective effect on health outcomes across racial groups (Wills, Resko, Ainette, & Mendoza, 2004; Parker & Benson, 2004), based on the stress-buffering hypothesis (Cohen & Wills, 1985) this protective role may be particular important for African American adolescents when exposure to discrimination is expected to increase (Douglass, Mirpuri, English, & Yip, 2016; C. B. Fisher, Wallace, & Fenton, 2000).
The parenting styles of African American parents also have cultural aspects that differ from those in other racial groups, which make them particularly beneficial for youth in the presence of exposure to racial discrimination. Specifically, due to experiences of racism and discrimination themselves, African American parents tend to engage in more strict parenting practices. This parenting style developed as a coping mechanism against stressful race-based experiences to keep children safe (Julian, McKenry, & McKelvey, 1994). It is well documented in the literature that African American parenting styles are often more harsh (McWayne, Owsianik, Green, & Fantuzzo, 2008) and less warm overall (Klebanov, Brooks-Gunn, & Duncan, 1994; Pinderhughes, Nix, Foster, Jones, & Conduct Problems Prevention Research Group, 2001) than the parenting styles of other ethnic groups. Even so, many African American parents do, however, balance their strict behavioral expectations with warmth and affection (Brody & Flor, 1998).
Thus, there is accumulative evidence to support the protective effect of parental support against the negative impact stressful life events, more broadly (Ozer & Weinstein, 2004; Zimmerman, Ramirez-Valles, Zapert, & Maton, 2000), and racial discrimination, more specifically, on African American youth health outcomes (Broman, Reckase, & Freedman-Doan, 2006; Cleveland, Gibbons, Gerrard, Pomery, & Brody, 2005). For example, Brody and colleagues (2014) found that perceived racial discrimination predicted increases in allostatic load (i.e., physiologic effects on the body due to chronic stress exposure) among their sample of African American youth and that this effect was not observed for those participants who received high emotional support. A second study by Brody and colleagues (2006) also reported similar protective results, with supportive parenting reducing the negative impact racial discrimination on African American youths’ depressive symptomatology and conduct problems. The protective effect of parental support has also been observed in regard to drug use, with parental support buffering the effect of perceived discrimination on both drug willingness and use among African American youth (Gibbons et al., 2010). Moreover, Gibbons et al. (2010) found a mediation pathway, such that adolescents whose parents offered more support were less likely to report feeling angry and to report subsequent drug and drinking willingness if they had experienced discrimination.
Given evidence of gender differences in risk for racial discrimination, depression symptomatology, and drug use among African American youth, it is important to also note evidence of gender differences in the protective effect of parenting practices based on the adolescent’s gender. Specifically, studies have documented greater levels of support (Richardson et al., 2015; Tamis-LeMonda, Briggs, McClowry, & Snow, 2009) and a stronger buffering effect of parental support on health outcomes (Gaylord-Harden, Elmore, & Montes de Oca, 2013) for African American females than males. However, some researchers have also acknowledged that this effect varies based on whether support is provided by mothers compared with fathers (Cooper, Brown, Metzger, Clinton, & Guthrie, 2013; Pernice-Duca, 2010). Thus further research is needed on the topic, particularly given that among studies examining the protective effect of parental support on the risk pathway between discrimination and drug use, gender differences have generally been controlled for (e.g., Brody et al., 2006; Gibbons et al., 2010) or found to not be present (e.g., Brody et al., 2014). The current study aims to expand on the existing literature by observing potential gender differences in both the discrimination–depression–drug use pathway and the protective role of parental support within the risk model.
Current Study and Hypothesis
Previous findings have documented a robust negative effect of racial discrimination on drug use risk among African American youth and that this risk pathway is mediated through depressive symptomatology (Gibbons et al., 2004; Sanders-Phillips et al., 2014). In addition, based on the stress-buffering framework (Cohen & Wills, 1985), parental support has been shown to protect youth against drug use as a consequence of discrimination, though this protective pathway has yet to be examined in regard to the risk pathway among racial discrimination, depression, and drug use. Moreover, limited work has been conducted to untangle whether gender differences are present within the racial discrimination, depression, drug use pathway or within the protective effect of parental support.
The aim of the current study was to examine the mediating role of depressive symptomatology within the racial discrimination–drug use pathways, and the moderating effect of both parental support and gender among a sample of 1,521 African American youth. First, based on previous literature, we hypothesized that racial discrimination and drug use would be reported at higher rates for males and depressive symptomatology would be reported at higher rates among females. Consistent with previous findings, we hypothesized that racial discrimination would be positively associated with both depressive symptomatology and drug use. In addition, a protective effect would be found for parental support, such that it will be negatively associated with depressive symptomatology and drug use among our sample of youth. For our second set of analyses, we examined mediating and moderating effects on the discrimination–drug use relationship. Specifically, we hypothesized that racial discrimination would be associated with greater drug use and this effect would be mediated through higher depressive symptoms. We did not anticipate gender differences within this risk pathway. Second, based on the stress-buffering model, we hypothesized that parental support would moderate the relationship between racial discrimination and drug use and this moderating effect would also operate through the mediation pathway by impacting depressive symptomatology. Based on the limited literature available in this area, we hypothesized that this effect may be stronger for African American females compared with males.
Method
Participants
The current study involves participants drawn from a larger parent study examining school and health behavior outcomes among students between 4th and 12th grades. Participants were sampled from 127 schools (21 districts) across a large midwestern county. Informed consent forms were sent home to parents of potential participants and were asked to return signed forms back to the school if they wished to provide consent (see J. Barnes, Almerigi, & Hsu, 2009, for further information about the parent study). For the current study, we examined the relationship among racial discrimination, depressive symptomatology, parental support, and drug use among all African American youth, controlling for school enrollment, gender, and age. Of the 2,347 African Americans who participated in the study, only a subset provided complete data on drug use outcomes. Thus, the current study is based on a sample of 1,521 African American youth. A majority of participants were female (56.3%) and were in middle school (27.2% in 6th grade, 22.3% in 7th grade, and 18.9% in 8th grade). Those excluded from the study were less likely to be female (50.7% compared with 56.3% of included participants) and younger (86.9% were in 4th or 5th grade compared with 0.4% of included participants).
Measures
Demographic and background measure
Participants were asked to indicate their gender, grade, birth date, and ethnic/racial background (i.e., African American, American Indian, Asian, Hispanic, Multiracial, White, and Other). Participants were allowed to choose only one ethnic/racial background; those participants who identified as African American were included in the current study.
Drug use
The drug use measure was adapted from items included in various national studies conducted among youth (e.g., Monitoring the Future, Youth Risk Behavior Surveillance System). Participants were asked to indicate how many days in the past 30 days they had engaged in the following six behaviors: “had at least one drink of alcohol,” “smoke cigarettes,” “use smokeless tobacco,” “used marijuana,” “used inhalants,” and “used other drugs.” Response choices were provided on a 7-point Likert-type scale: 1 (0 days), 2 (1 or 2 days), 3 (3–5 days), 4 (6–9 days), 5 (10–19 days), 6 (20–29 days), and 7 (everyday). A composite scale was used for drug use. For the current study, the internal consistency reliability estimate was good (α = .89).
Racial discrimination
A single item was used to assess racial discrimination among youth. This item is similar to other single-item discrimination measures found in the literature (Bennett, Wolin, Robinson, Fowler, & Edwards, 2005; Durkin et al., 2012; S. Fisher et al., 2015; Kressin, Raymond, & Manze, 2008). For the current study, participants were asked the following prompt: “In the past year, how often did a kid at my school tease me about my race/ethnicity or the color of my skin?” Participants responded on a 4-point Likert-type scale: 1 (never), 2 (not much), 3 (sometimes), and 4 (a lot).
Depressive symptomatology
The Center for Epidemiologic Studies Depression Scale (CES-D; Radloff, 1977) was used to assess depressive behaviors and feelings experienced in the past week. The assessment used for the current study was based on 13 items adopted from the original 20-item CES-D. Participants responded to a prompt (“During the past year, how often did the following things happen?”) on a 4-point scale: 1 (not at all), 2 (a little), 3 (some), and 4 (a lot). Higher scores are indicative of greater depressive symptoms. The CES-D has moderately high test–retest reliability between .45 and 70 and high internal consistency (α = .85 for the general population and .90 for the patient sample). Similar internal consistency was found for the current study (α = .86). Furthermore, this measure has been validated for use with African American youth (Fitzpatrick, Piko, Wright, & LaGory, 2005; Nguyen, Kitner-Triolo, Evans, & Zonderman, 2004).
Parental support
The parental emotional support and closeness measure was constructed for the current study. The eight-item measurement asked participants to indicate on a 4-point Likert-type scale their agreement with statements regarding their parent or caregiver level of emotional support and closeness. Items included “Enjoy spending time with you,” “Listen to you,” and “Do fun things with you” (see the appendix for a complete list of items). Response choices ranged from 1 (strongly disagree) to 4 (strongly agree). A composite scale was used for parental support. For the current study, the internal consistency reliability estimate was good (α = .89).
Data analyses
All analyses were performed using SAS 9.4. With students nested within schools, preliminary analyses revealed no significant contribution by school, so analyses were analyzed at the individual level. However, age was included as a covariate in our analysis, as, consistent with previous literature, drug use was found to significantly increase with age (National Institute on Drug Abuse, 2014).
Mediation–moderation analyses were performed using the PROCESS macro (Hayes, 2013) to explore the relationship between the racial discrimination and drug use, with depression as the mediator, and whether this effect varied based on gender (Model 59 specified by Hayes, 2013). This analysis was run controlling for age. In addition, we ran a mediation–double moderation model to explore the mediation relationship among racial discrimination, depression, and drug use was moderated by parental support, and if the moderating effect of parental support varied based on participant’s gender (Model 73 specified by Hayes, 2013), controlling for the effect of age. The PROCESS macro estimates the total and direct effect of the independent variable on the dependent variable and indirect effect of the independent variable through the mediator. The PROCESS macro also estimated the indirect effect of the moderator on both the predictor on the mediator and the outcome variable, as well as the mediator on the outcome variable. It used bootstrapping to generate bias-corrected confidence intervals for the indirect effect and various indices of effect size for the indirect effect (Hayes, 2013). For all mediation analyses in the current study, we used 20,000 bootstrap samples.
Only participants who provided complete data were included in the current study; thus no imputation of missing data was required. It should be noted that participants that were excluded (n = 826) were younger and reported significantly higher scores on the study variables (i.e., parental support, racial discrimination, and depression symptoms) compared with those included in the study analysis.
Results
Preliminary analyses
Contrary to our hypothesis, preliminary analyses indicated no significant differences on racial discrimination based on gender (t test, p = .128) or age (rSpearman = .016, p = .523). In addition, no significant differences were observed between males and females (t test, p = .090) regarding drug use, although older youth did report higher rates of drug use than younger youth (rSpearman = .163, p < .001). Consistent with our hypothesis, significant differences were observed for depressive symptomatology, with females (t test, p < .001) and older youth (rSpearman = .086, p < .001) reporting higher scores on the depression measure (see Table 1 for more details).
Statistics for African American Participants
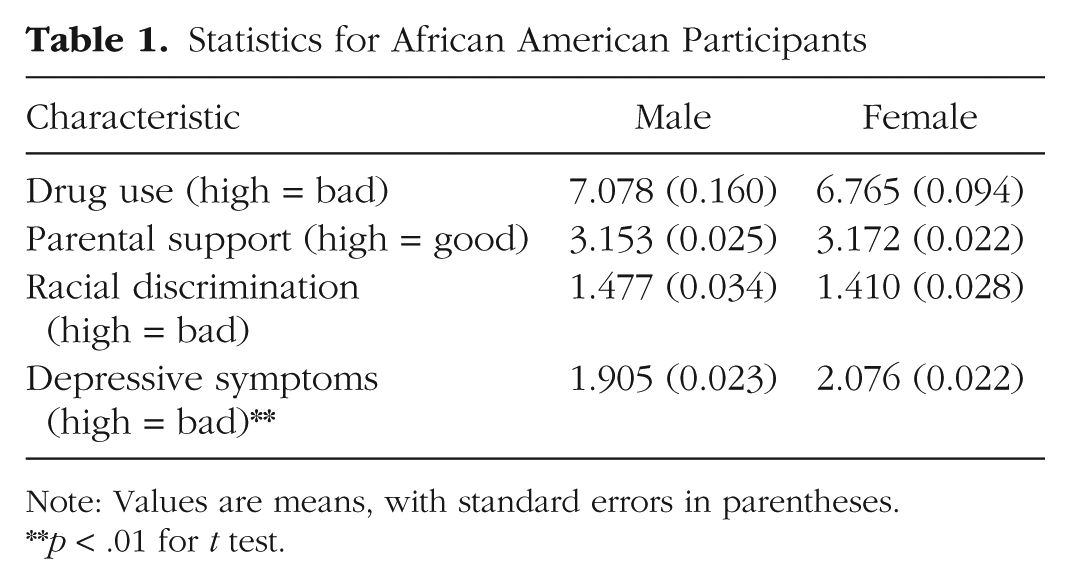
Note: Values are means, with standard errors in parentheses.
p < .01 for t test.
As anticipated, racial discrimination was positively associated with both drug use (rSpearman = .080, p = .002) and depressive symptomatology (rSpearman = .166, p < .001). In addition, as anticipated by our hypothesis, a protective effect was found for parental support, such that it was negatively associated with drug use (rSpearman = −.175, p < .001) and depressive symptomatology (rSpearman = −.254, p < .001) among our sample of youth (see Table 2 for associations).
Rank Correlation Coefficient (Spearman) Matrix
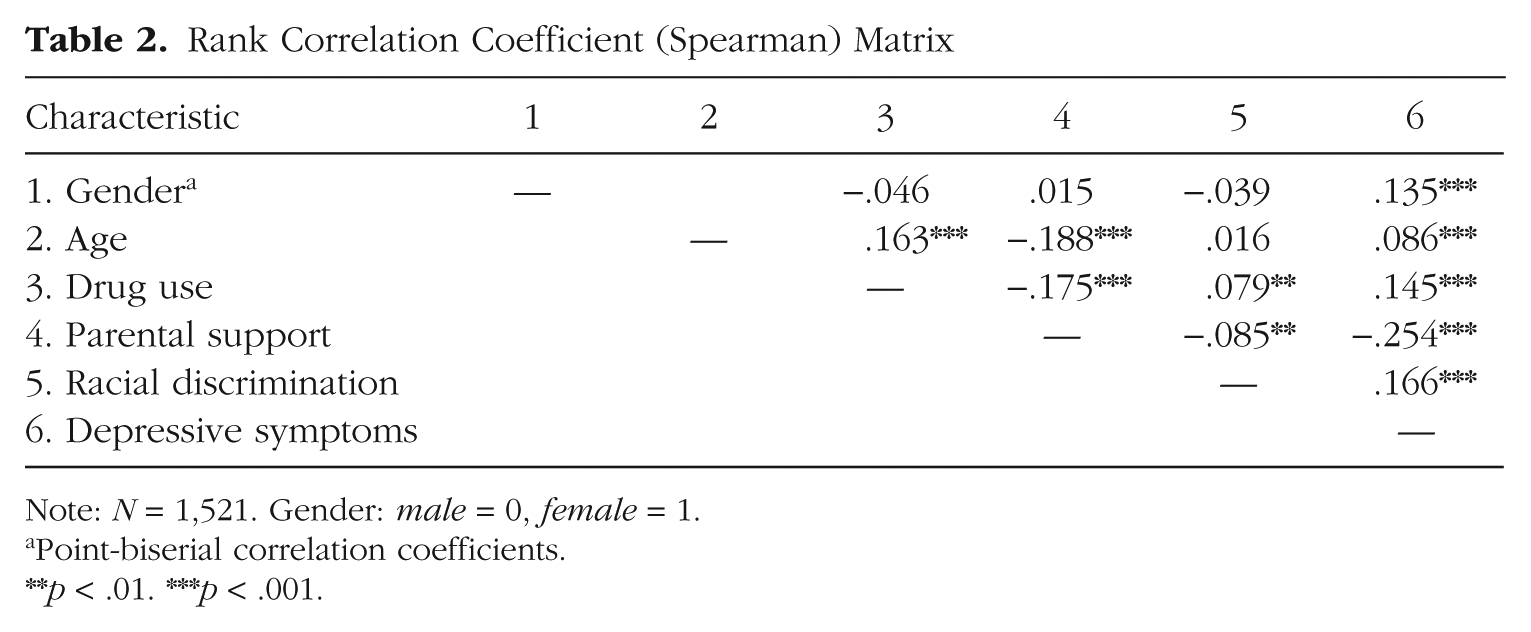
Note: N = 1,521. Gender: male = 0, female = 1.
Point-biserial correlation coefficients.
p < .01. ***p < .001.
Mediation analyses of discrimination, depression, and drug use by gender
In accordance with our second set of hypotheses, and consistent with previous literature, after controlling for age, the relationship between racial discrimination and depressive symptomatology was significant (estimate = 0.245, p < .01), as well as the relationship between depressive symptoms and drug use (estimate = 1.653, p < .01). These results revealed the relationship between racial discrimination and drug use was mediated through depressive symptomatology. This mediation pathway was found for both genders, but contrary to hypothesis, was stronger for males (estimated indirect effect = 0.205, boot 95% confidence interval [CI] = 0.081–0.415) than females (estimated indirect effect = 0.070, boot 95% CI = 0.030–0.137). Moreover, the direct effect of discrimination on drug use was found to remain significant for males (estimated direct effect = 0.697, boot 95% CI = 0.390–1.00), but nonsignificant for females (estimated direct effect = −.048, ns), suggesting that the depression partially explains the relationship between discrimination and drug use for males, but fully explains the risk model for females.
Moderation analyses of parental support within risk model based on gender
For the final hypotheses, we tested a mediation–double moderation model to examine whether parental support moderated the relationship among racial discrimination, depressive symptomatology, and drug use, and whether this protective role of parental support varied by gender. We found support for these hypotheses, after controlling for age, the mediation pathways among racial discrimination, depression symptomatology, and drug use was buffered by parental support. It is interesting that when examining each segment of the mediation pathways, it appears that parental support’s protective effect on drug use was not produced by moderating the impact of racial discrimination on depressive symptomatology (estimate = −0.004, ns), but by moderating the impact of depression on drug use (estimate = −1.799, p = .005).
Gender differences were also examined. Contrary to our hypothesis, the moderating effect of parental support was found for both genders, but was stronger for males. Specifically, at low and moderate levels of parental support, there was a significant mediation pathway such that higher levels of discrimination were associated with more depressive symptoms, which resulted in more drug use among male (low: estimated indirect effect = 0.265, boot 95% CI = 0.032–0.636; moderate: estimated indirect effect = 0.135, boot 95% CI = 0.036–0.289) and female participants (low: estimated indirect effect = 0.077, boot 95% CI = 0.026–0.168; moderate: estimated indirect effect = 0.046, boot 95% CI = 0.017–0.098). However, this effect was nonsignificant at higher levels of support for both genders, suggesting a protective role of parental support on risk for drug use for both male (estimated indirect effect = 0.014, ns) and female participants (estimated indirect effect = 0.019, ns). See Table 3 and Figure 1 for details on all path coefficients.
The Indirect and Direct Effects of Racial Discrimination on Drug Use Through Depressive Symptoms by Gender, Given Fixed Rates of Parental Support
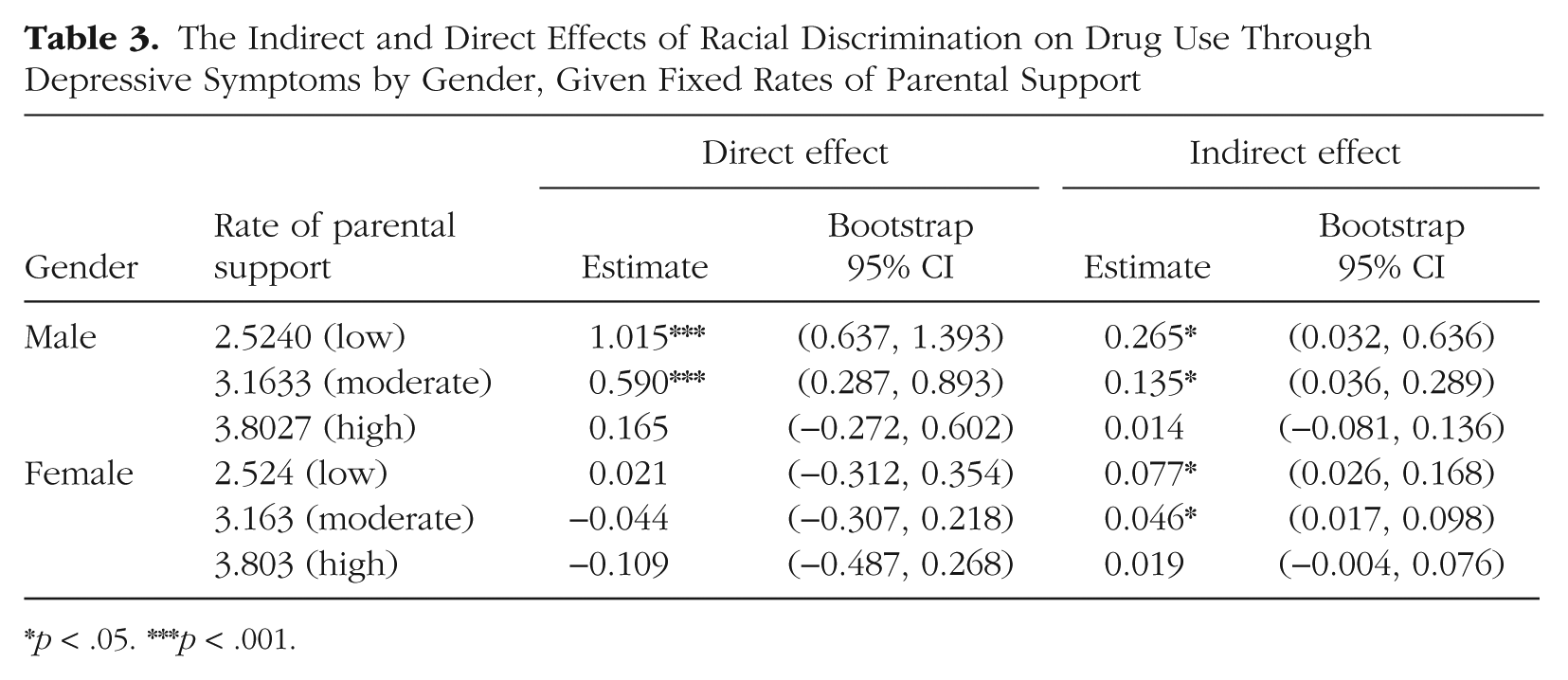
p < .05. ***p < .001.
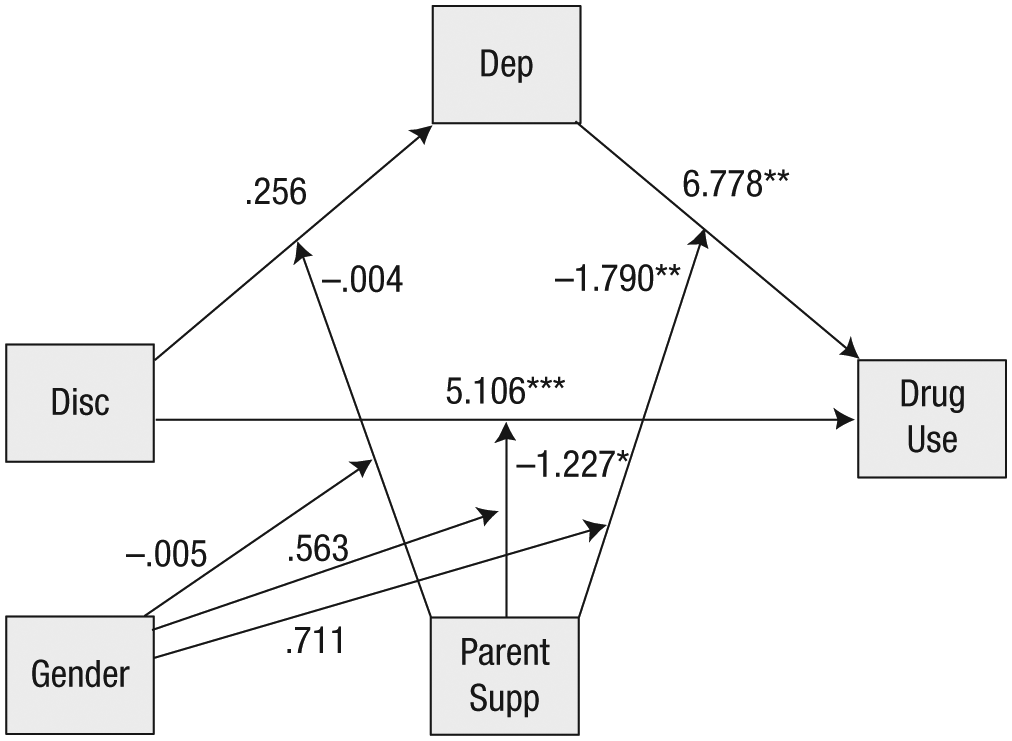
The estimated pathways of the mediation–moderation model in drug use for African American youth. Depiction of structural model representing the pathways to drug use for African American youth based on experiences of racial discrimination (Disc), depression (Dep), and parental support (Parent Supp). Only hypothesized pathways are presented. Not included in the figure, for ease of presentation, are disturbance terms and error terms. *p < .05. **p < .01. ***p < .001.
Discussion
Previous research has documented the negative impact of racial discrimination on drug use and other health behaviors among African American youth (Gibbons et al., 2004; Guthrie et al., 2002). There is also evidence to support that this relationship is mediated through negative affect, such that experiencing racial discrimination increases vulnerability to negative emotionality, which subsequently increases risk for drug use (Sanders-Phillips et al., 2014). Given gender differences in the relationship between discrimination and depression—with a stronger association found for females—and between discrimination and drug use—with a stronger association found for males—it is plausible that gender differences may also be present in the mediation pathway among discrimination, depression symptomatology, and drug use. The current study’s first aim was to examine this relationship.
Consistent with previous literature, we found a positive relationship between racial discrimination and greater drug use, which was mediated through higher depressive symptoms. This mediation pathway was found for both males and females, suggesting that exploring the effect of racial discrimination on mood among African American youth and providing adaptive coping skills to manage distress, particularly depressive symptomatology, can be a useful prevention technique for this population of youth. Our findings also highlighted an interesting gender difference in the mediation pathways, in that depressive symptomatology fully mediated the relationship between discrimination and drug use for females, but only partially meditated the relationship for males. This partial mediation suggests that there are other factors that indirectly effect vulnerability to drug use as a consequence of racial discrimination for African American males that were not assessed in the current study. One possibility is the indirect effect of externalizing responses to discrimination, such as anger or hostility.
There is a growing body of literature to suggest that anger may be an important factor to consider within the discrimination–drug use risk pathway, as it has been shown to be directly related to exposure to racial discrimination (Pittman, 2011) and mediates the relationship between discrimination and drug use (Boynton et al., 2014; Gibbons et al., 2004; Gibbons et al., 2014; Terrell, Miller, Foster, & Watkins, 2006). Moreover, Pittman (2011) observed a link between anger and depression, such that those African Americans who engaged in active anger in response to racial discrimination were also more likely to report psychological distress. Based on these findings and those from the current study, it may be the case that racial discrimination influences drug use risk indirectly through both anger and depression for African American males, but primarily through depression for females. Further research is needed to test these hypotheses.
The second aim of the study was to examine the role of supportive parenting within the discrimination–drug use pathway, as previous literature has highlighted parental support as an important protective factor against youth drug use (Elmore & Gaylord-Harden, 2013; Gibbons et al., 2004; Schmeelk-Cone & Zimmerman, 2003; Wills & Cleary, 1996; Wills et al., 2000; Wills & Yaeger, 2003), particularly among youth who have experienced significant stress (Brody et al., 2014; Raffaelli et al., 2013; Sullivan, Kung, & Farrell, 2004; Tanigawa, Furlong, Felix, & Sharkey, 2011). Yet, no study to date has been conducted examining the protective effect of parental support within the racial discrimination, depression, drug use pathway. Moreover, it was unclear as to whether this protective effect would vary as a function of the youths’ gender.
The results of the present study confirmed our hypotheses with parental support attenuating the negative effect found between racial discrimination and drug use. The protective effect of parental support was also evident within the mediation pathway among discrimination, negative affect, and drug use. These relationships were invariant across gender. Specifically, it was found that although parental support was not protective against the negative impact racial discrimination had on depressive symptoms, it did play a buffering role on reducing the impact depressive symptoms had on subsequent drug use as a consequence of experiencing discrimination. Our findings provide further confirmation in the literature on the importance of supportive parenting on adolescent health outcomes. Moreover, they speak to the need for inclusion of parental components in prevention programming for African American adolescents, such as the strong African American families program (SAAF; see Brody, Chen, et al., 2012; Kogan et al., 2016). Specifically through the SAAF, caregiver practices such as parental warmth and support, parental monitoring, enhancement of racial pride, and the teaching of coping skills are cultivated, which in turn help the adolescent develop self-regulation skills, achievement orientation, and negative attitudes toward drug use and other risky behaviors (Brody, Chen, et al., 2012). Thus, such programs are able to foster family interconnectedness and coping skills, which enable African American youth to better withstand adversity and maintain good health and behavioral outcomes (Washington, Rose, Colombo, Hong, & Coard, 2015).
Given this evidence, in addition to parental support, other parenting practices warrant further empirical investigation within the racial discrimination–drug use risk pathway (Washington et al., 2015). For the example, as eluded to in the SAAF program, racial socialization—defined as the process by which children and young adults learn about their race and ethnicity, raise awareness of prejudice and racism, and prepare to manage cultural diversity—is often found within African American families (Phinney & Chavira, 1995). Racial socialization is associated with several positive outcomes, including positive ethnic identity development (Else-Quest & Morse, 2015; McHale et al., 2006), academic achievement (Chavous et al., 2003; Chavous, Rivas-Drake, Smalls, Griffin, & Cogburn, 2008), and lower prevalence of mood problems, aggression, and drug use (Caughy, Nettles, O’Campo, & Lohrfink, 2006; Davis & Stevenson, 2006; Hughes et al., 2006; S. A. Wallace & Fisher, 2007) among African American youth. Thus, in the presence of racial discrimination, youth who have been socialized to cope with racism are more apt to utilize adaptive coping strategies, and thus may be at reduced risk to use drugs to cope with distress (Wills, McNamara, Vaccaro, & Hirky, 1996).
Alternatively, racial socialization may also operate by reducing the distress youth feel in response to experiencing discrimination. Studies have found a positive relationship between racial socialization and lower levels of perceived stress (Bynum, Burton, & Best, 2007; Neblett et al., 2008; Neblett, Rivas-Drake, & Umaña-Taylor, 2012). However, this protective effect has yet to be examined within the racial discrimination–drug use pathway. Thus, related to our findings, it is plausible that although parental support did not protect youth from the development of depressive symptomatology as a consequence of discrimination, it could be that racial socialization practices would. If this protective effect is supported, racial socialization would also warrant inclusion in prevention programming for African American youth.
Another aspect of the parent–child relationships that has shown to play an important in youth development and health behaviors is parental monitoring. Parental monitoring—defined as parental supervision and knowledge about a child’s activities—has been associated with reduced risk of adolescent problem behaviors, including drug use (G. M. Barnes & Farrell, 1992; G. M. Barnes, Hoffman, Welte, Farrell, & Dintcheff, 2006; Branstetter & Furman, 2013). Ryan et al. (2010) conducted a systematic review of parental factors associated with adolescent alcohol use, finding that parental monitoring was significantly associated with later age of initiating alcohol use and lower levels of alcohol consumption among youth. The protective effect of parental monitoring has also been observed among studies specific to African American youth. Li, Feigelman, and Stanton (2000) found among their sample of low-income African American youth age 9 to 17 that perceived parental monitoring was associated with decreased risk for drug use and several other risk behaviors, including sexual behavior, school truancy, and violent behaviors. In a secondary study the authors also found that perceived parental monitoring served a long-term effect, protecting African American youth from drug use over the course of the 4-year study (Li, Stanton, & Feigelman, 2000). Further research is needed to understand whether these protective effects of parental monitoring on drug use outcomes are also evident among youth in the context of environmental stressors, such as racial discrimination.
Last, though not part of the nuclear family, extended family members can also provide important sources of support for African American youth, and are often identified as central support figures among this sample of youth (Bost, Vaughn, Boston, Kazura, & O’Neal, 2004). McMahon, Felix, and Nagarajan (2011) found among their sample of middle-school-aged African American youth, participants reported receiving emotional, tangible, and informational support from not only mothers but also grandmothers, sisters, friends, fathers, and teachers. In addition, participants noted extended family, such as godmothers and great-grandmothers, as being important sources of support for the youth. These sources of support have also been shown to be protective against risky health outcomes and drug use (Blake, Ledsky, Goodenow, & O’Donnell, 2001). Related to clinical application, these findings suggest that intervention programming should include support from not only the nuclear family but also other sources available to African American youth (e.g., grandparents, friends, neighbors, teachers, godparents, etc.).
Limitations
The current study provided important knowledge to advance our understanding of the influence of parental support on the drug use vulnerability among African American youth; however, there are several limitations that should be noted. First, though data were collected within a specific subgroup of youth that are understudied in the area of drug use prevention, the sample was collected from one area of the United States and is thus not nationally representative of all African Americans. Second, racial discrimination was assessed using a single-item measure. Although the use of a one-item racial discrimination measure is not uncommon (e.g., Bennett et al., 2005; Durkin et al., 2012; S. Fisher et al., 2015; Kressin et al., 2008) and the item used for the current study assessed a specific type of discrimination (i.e., peer-inflicted racial discrimination) that is commonly experienced by adolescents and is associated with significant negative psychological outcomes among youth (Douglass et al., 2016), there is evidence that single-item measures of discrimination are less reliable than multi-item discrimination measurements (Krieger, Smith, Naishadham, Hartman, & Barbeau, 2005). Moreover, given that perceived discrimination encompasses both sensing racist attitudes (e.g., beliefs) and the experience of racists actions (Atkins, 2014), and can be experienced at multiple levels (e.g., personally mediated, institutional racism, or internalized racism; Jones, 2000), the use of multi-item measurements would be a more comprehensive assessment of racial discrimination that could provide important insight as to the differing impact each type of racism has on behavioral outcomes for African American youth.
Third, the findings provided further support for the clinically significant impact racial discrimination has on health outcomes for African American youth, that this process is influenced by the elevation of depressive symptomatology, and that parental support can be an important target for preventing drug use vulnerability for these at-risk youth. However, although consistent with previous literature, with average effects of discrimination on broad health outcomes at r = −.18 (Pascoe & Richman, 2009) and between .11 and .15 specifically for drug use outcomes among African American youth (Gibbons et al., 2004; Gibbons et al., 2010; Gibbons et al., 2012), our effects sizes were not large and accounted for only 11% of the variance in predicting youth drug use. These effect sizes indicate that although the variables presented are important to investigate, there are other variables that should also be considered to provide a more comprehensive assessment of risk for African American youth. Future research should include variables such as those parental factors, social support factors, and anger/hostility response processes presented earlier, as well as other peer factors, such as affiliation with substance-using peers (Brody, Kogan, et al., 2012). In addition, research has long demonstrated a significant relationship between drug-use attitudes and subsequent use (Burlew et al., 2000; Corneille & Belgrave, 2007), thus given that a majority of the youth in the study did not use drugs (78.83%), using other outcomes such as drug-use attitudes among this population of youth may have provided stronger effect sizes due to greater variability in responses. Last, although the proposed mediation–moderation pathways were based on previous literature and theory, cross-sectional data were used to test the study’s hypotheses, thus precluding interpretation of a causal relationship. Future studies utilizing a prospective study design are needed to confirm these findings.
In sum, our study provides promising evidence for the protective effect of parental support on drug use among African American youth as a consequence of the experience of racial discrimination. This effect was found for both genders; however, the pathway was only partially explained for males. This finding suggests that there are other factors, such as anger/hostility, that may be important mediators in drug use vulnerability as a consequence of racial discrimination for African American males. Moreover, our findings point to the importance of managing negative affect in the presence of stressors, such as racial discrimination, for African American youth to mitigate risk for drug use. Our findings also provided insight into the protective role of parenting within the risk model. Parental support was found to have no effect of the negative relationship between racial discrimination and depressive symptomatology, but was able to significantly impact the effect negative mood had on drug use vulnerability. Thus, in additional to teaching youth coping skills to manage their mood, aiding parents in supportive parenting techniques can provide additional buffers for drug use vulnerability by providing additional emotional support networks for the youth and outlets to learn additional coping skills. Further research is still needed to better understand how additional types of emotion support available to African American youth impact their risk for drug use, as well as the indirect effect of externalizing responses, such as anger, have on drug use vulnerability for African American youth. Such work can be used to inform culturally adaptive prevention programming to ultimately reduce health disparities in drug use outcomes.
Footnotes
Appendix
Declaration of Conflicting Interests
The authors declared that they had no conflicts of interest with respect to their authorship or the publication of this article.
Funding
This research was supported by National Institutes of Health Award KL2TR001106 to Anantha Shekhar and Tamika C. B. Zapolski and by National Institutes of Health Award DA05312 to Sycarah Fisher.