
Abstract
Despite being a significant public health concern, the role of opioid prescriptions in potentiating risk of opioid misuse in the context of pediatric pain has been underinvestigated. To address this gap, the present review identifies theory-based hypotheses about these associations, reviews the extant literature on opioid prescriptions that supports these hypotheses, and provides routes for future empirical studies. A multilevel model of mechanisms through which opioid prescriptions may impact pain and other negative outcomes in youth, including risk for opioid misuse and related problems, is proposed with particular attention paid to the role that psychologists can play in informing policies and developing preventative interventions in healthcare settings.
Prevention of chronic pain states is a critical piece of a comprehensive approach to reduce the negative impact of chronic pain in children and adolescents. The benefits of opioid analgesics in youth experiencing noncancer pain must be thus weighed against the potential risks of opioid use. Pediatric medical settings are a point of entry to opioid use for youth, including youth who would otherwise not seek out psychoactive substances. Eighty percent of high school students reporting medical use of opioids prior to misuse indicated sourcing the substance from their own previous prescription (McCabe, West, Teter, & Boyd, 2012), demonstrating that even legitimate receipt of an opioid prescription potentiates risk for problem use. As rates of adult prescription misuse have been connected to persistent and serious negative sequelae, including the transition from opioid prescriptions to heroin use and overdose death (Banerjee et al., 2015; Bartels, Binswanger, & Hopfer, 2016; Martins et al., 2017), an examination of risk factors for youth who receive legitimate opioid prescriptions in the context of pain experiences is warranted.
With limited exceptions, such as the use of amphetamines as treatment for Attention Deficit/Hyperactivity Disorder, youth are not routinely introduced to substances with abuse potential (e.g., cannabis, alcohol) by adults providing medical care. Use of medical cannabis in adolescents is highly contentious (Choo, Feldstein Ewing, & Lovejoy, 2016), and no medical professional would recommend anyone under legal drinking age consume alcohol (Feldstein Ewing, Lovejoy, & Choo, 2017). In fact, where legal, the age of recreational use for alcohol and cannabis is 21 and therefore much closer to the close of neural development (approximately age 25; Giedd & Rapoport, 2010). However, pediatric medical providers in the United States routinely prescribe prescription opioids with addictive properties to children, most frequently to 12- to 17-year-olds (Dowell, Haegerich, & Chou, 2016; Livingstone, Groenewald, Rabbitts, & Palermo, 2017), and often do so in an “off label” manner. Postoperative pain, sickle cell disease, and pain due to cancer are the only pain conditions for which opioids are indicated in pediatrics, yet numerous other pain conditions frequently yield an opioid prescription (Berde & Sethna, 2002; Friedrichsdorf et al., 2016). As a result, almost 20% of high school students have received at least one opioid prescription by their senior year (McCabe et al., 2012). While these prescriptions may be needed for controlling pain in medical settings, the result is a large proportion of youth who have been introduced to this addictive substance, placing them at increased risk for opioid misuse and addiction.
Traditional models of adolescent health risk and addiction do not fit well with this unique route of entry that occurs for prescription opioid misuse. Most adolescent addiction models emphasize the interaction between predisposing factors (e.g., genetic factors, peer factors, environmental context) and the pattern of neuromaturation during this period, which favors enhanced reward sensitivity coupled with less developed control systems (Casey, 2015; Conrod & Nikolaou, 2016; Ernst, 2014; Feldstein Ewing, Tapert, & Molina, 2016; Shulman et al., 2016). Furthermore, because almost all substances are illegal for youth, a defining feature of most adolescent substance use is the adolescent’s willingness to violate a rule or norm in order to obtain the desired substance (Asghari & Nicholas, 2001; Conrod & Nikolaou, 2016; Osilla et al., 2014). In the case of prescription opioids, youth need not effortfully obtain a substance that they should not have, as that step has been circumvented by the medical system treating them. This creates opportunity for experimentation for youth who may otherwise never have sought out a substance of abuse and even opens a door for experimentation among those who highly disapprove of substance use (Miech, Johnston, O‘Malley, Keyes, & Heard, 2015).
Among adults, chronic pain treatment guidelines now recommend against the initiation of long-term opioid therapy for chronic pain, indicating a lack of high-quality evidence of benefit compounded by growing evidence of harms (Dowell et al., 2016; Volkow & Koroshetz, 2017). Yet few have addressed how legitimate opioid prescriptions might contribute to the development and persistence of opioid misuse and pain in pediatric populations. To address this gap, the present review identifies theory-based hypotheses about these associations, reviews the extant literature on opioid prescriptions that supports these hypotheses, and provides routes for future empirical studies. A multilevel model of mechanisms through which opioid prescriptions may impact pain and other negative outcomes in youth, including risk for opioid misuse and related problems, is proposed with particular attention paid to the role that psychologists can play in informing policies and developing preventative interventions in healthcare settings.
Pediatric Opioid Prescribing
Analgesic medication is routinely overprescribed in pediatric patients (Yaster et al., 2015). However, disjointed timelines of data collection foster difficulty in adequately assessing the progression of opioid use trends among youth. According to Center for Behavioral Health Statistics and Quality (CBHSQ, 2016) data from 2015, 22.7% of youth age 12 to 17 used and 3.9% misused pain relievers in the past year. A decline in overall use rates (both medical and nonmedical/misuse) among adolescents has been observed since 2013 (McCabe et al., 2017), and initially prescription rates for adolescents appeared to decline between 1996 and 2012 (Groenewald, Rabbitts, Gebert, & Palermo, 2016). Contrary to expectations, provision of opioid prescriptions to youth with noncancer pain increased between 2005 to 2014 (Pielech, Rivers, Bailey, & Vowles, 2016). Further, subgroups of youth with specific pain conditions are more likely to receive an opioid prescription. For instance, in a study of over 8,000 youth with headache, 46% received at least one opioid prescription in the 1-year period following initial diagnosis (DeVries et al., 2014). This is in the face of prescribing guidelines delineating that opioids are not an indicated treatment for this condition and thus should not be the first-level treatment for headache or other primary pain conditions in children (Berde & Sethna, 2002; Chou et al., 2009; Friedrichsdorf et al., 2016; Tepper, 2012). Despite efforts to improve prescribing guidelines to reduce overprescribing (e.g., Dowell et al., 2016), prescription of opioid analgesics to children and adolescents merits close attention given the cataclysmic outcomes being observed among opioid-addicted adults (Wilkerson, Kim, Windsor, & Mareiniss, 2016) and the increased risk of future misuse among youth who use prescription opioids, even as directed by a medical provider (Miech et al., 2015).
Efficacy of Opioid Treatment for Pain Conditions
Despite also not being indicated for most acute pain conditions, most youth receive opioid prescriptions for acute pain (Berde & Sethna, 2002). Many providers report that most acute pain can be managed easily and well for children and adolescents without opioids (Dowell et al., 2016), but this is a tricky empirical question, as little research has evaluated the comparative efficacy or effectiveness because of a historical reluctance to conduct clinical trials in this young age group (Berde & Sethna, 2002; Coté, Kauffman, Troendle, & Lambert, 1996).
Within the extant literature, opioid analgesics do indeed appear to be effective in assuaging acute moderate to severe postsurgical pain in youth (Committee on Psychosocial Aspects of Child and Family Health, 2001; Tyler, Woodham, Stocks, Leary, & Lloyd-Thomas, 1995). In addition, a number of trials have shown no advantage to opioids over nonsteroidal anti-inflammatory drugs (NSAIDs) in terms of postoperative pain reduction in children and adolescents, such as in tonsillectomy and minor orthopedic surgeries (Best et al., 2017; Kelly et al., 2015; Poonai et al., 2017). There is also evidence from multiple trials for common pain experiences in adults (e.g., acute low back pain, wisdom tooth extraction) that opioids coupled with NSAIDs do not add significant pain relief over NSAIDs alone (Best et al., 2017; Friedman et al., 2015). Thus, acute pain experiences may, in fact, represent a highly preventable route of opioid access in a legitimate context, as opioids are not indicated as a primary treatment for a majority of the acute pain conditions for which they are prescribed.
Similarly, there is a dearth of research regarding the efficacy of opioid therapy as a long-term treatment of chronic noncancer pain in youth. It is also not recommended for primary pain disorders in pediatric populations because of poorer clinical outcomes (Friedrichsdorf et al., 2016). While indicated for youth with sickle cell disease and/or pain due to cancer (Berde & Sethna, 2002), no experimental studies—in any age group—have addressed the effectiveness of long-term opioid therapy (i.e., greater than 1 year) for chronic noncancer pain compared to placebo or to no opioid therapy (Chou et al., 2015; Dowell et al., 2016).
Outcomes for shorter term treatment episodes shed light on the role of opioids in pain management and treatment. This research has been primarily conducted in adults. A meta-analysis by Furlan, Sandoval, Mailis-Gagnon, and Tunks (2006) examined the efficacy of various opioid medications, both strong (e.g., morphine) and weak (e.g., tramadol), in the treatment of chronic noncancer pain (i.e., nociceptive, neuropathic, fibromyalgia, mixed) in adults over 3 to 9 weeks. This team found that while opioids outperform placebo, they are not superior to nonopioid analgesics (e.g., NSAIDs), particularly in functional outcomes and for nonopioid analgesics as compared with weak opioids (Furlan et al., 2006). These data suggest that medications such as NSAIDs could take precedent as a first line of treatment in patients without severe pain, for whom the greatest risk without associated benefit is likely to be derived. Furthermore, the benefits of long-term opioid therapy have been repeatedly called into question with assertions that there is inadequate evidence regarding its efficacy for managing chronic pain in both adults and children, and the current guidelines for opioid treatment include recommendations for using nonpharmacological/behavioral strategies as part of a comprehensive approach to pain management (Chou et al., 2014, 2015; Dowell et al., 2016; Friedrichsdorf et al., 2016; Volkow & Koroshetz, 2017).
Individual Risk Factors for Opioid Misuse in the Context of Pain
Preexisting contextual risk factors
Demographics
A number of sociodemographic factors of both patients and their providers contribute to the receipt and utilization of prescription opioids. Pediatric patient characteristics that predict receipt of an opioid prescription include age, gender, race/ethnicity, insurance type, and quality of health; older, insured, European American children in fair to poor parent-reported health receive the most prescriptions (Groenewald et al., 2016). African American children are significantly less likely to receive a codeine prescription than European American children (Kaiser et al., 2014), despite that African American children frequently report higher pain scores (Sadhasivam et al., 2012). Provider characteristics include geographic region and provider type, with northeast providers and physicians more likely to prescribe than unlicensed medical providers (Kaiser et al., 2014). The most recent Centers for Disease Control and Prevention (CDC, 2017) data also reflect regional and urban/rural differences in prescribing patterns by county.
Socioeconomic status (SES) also factors into receipt of opioid prescriptions for pain. Among adults who presented to the emergency department (ED) for pain, Joynt and colleagues (2013) found that patients from low-SES and high-poverty neighborhoods were less likely to receive opioids for their pain. African American patients were prescribed fewer opioids than European American patients at all SES levels (Joynt et al., 2013), reflecting a comparable pattern of prescriber bias across children and adults (Kaiser et al., 2014). Similarly, adult Hispanic patients less frequently received opioid prescriptions for moderate to severe pain as compared with non-Hispanic patients. Overall, high-SES European American patients presenting to the ED for moderate to severe pain appear to be most likely to receive an opioid prescription (Joynt et al., 2013).
Experience of pain conditions commonly treated with opioids
Long-term opioid use frequently begins with opioid treatment for acute pain (Edlund et al., 2014; Shah, 2017). Approximately 10% of adolescents’ and young adults’ non-injury-related visits and 14.5% of injury-related visits yield an opioid prescription, most commonly in ED settings (Fortuna, Robbins, Caiola, Joynt, & Halterman, 2010). Of all outpatient visits for 15- to 19-year-olds, the highest rates of opioid prescriptions stemmed from treatment for back/musculoskeletal pain (21.5%/11.3%), injury (15.0%), and headache (12.7%; Fortuna et al., 2010). For noncancer pain in outpatient settings, acute musculoskeletal pain or injury (e.g., sprain, fracture, back pain), postsurgical or procedural pain (e.g., dental surgery, tonsillectomy), and pain flares in the context of recurrent pain (e.g., recurrent headache, abdominal pain; Fortuna et al., 2010) are the conditions that most often generate opioid prescriptions for youth. However, notably, opioids are only indicated for pediatric postsurgical pain (Berde & Sethna, 2002). Dental and medical procedures account for 65% of child and adolescent opioid prescriptions (Groenewald et al., 2016). In these cases, relatively brief recovery periods are expected, with natural discontinuation of medication expected within 3 months of prescription. Within the United States, physicians most frequently prescribe opioids with the expectation that children and adolescents will stop taking the medication as soon as their pain resolves (Holman, Stoddard, Horwitz, & Higgins, 2014). However, even short-term (e.g., 5 days) use of opioids for acute pain sharply increases risk for later and continued use, even when used as prescribed by a medical provider (Shah, 2017).
Psychological distress
Psychological distress can confer significant additional risk for opioid misuse, particularly when it co-occurs in the pain context. Among adults, both mental health problems (Boscarino et al., 2010; Edlund et al., 2010; Swendsen et al., 2010) and pain-related factors (Blanco et al., 2016; Liebschutz et al., 2010; Sullivan, Von Korff, Banta-Green, Merrill, & Saunders, 2010) are associated with chronic opioid use, misuse, and use disorder. Specifically, these vulnerabilities can synergistically exacerbate risk for both chronic pain and opioid misuse. Mental health vulnerabilities, most commonly anxiety and depression (Richardson et al., 2012), have been shown to increase risk for opioid misuse in adolescents (Edlund et al., 2015). The avenue through which this may occur is via use of prescribed analgesics to alleviate symptoms of mental health conditions (Geisser, Cano, & Foran, 2006; Lord, Brevard, & Budman, 2011; Wasan et al., 2007), an effect that is compounded when acute pain persists.
About one third of youth presenting for acute pain treatment report clinically significant depressive symptoms, which can, in turn, increase persistence of pain (Lewandowski Holley, Wilson, Cho, & Palermo, 2017). This can subsequently enhance risk of protracted opioid use for relief of both pain and depressive symptoms. Among adolescents admitted to the hospital for acute injury and given an opioid prescription, those who reported depressive symptoms at intake reported significantly more sustained prescription opioid use postrelease (Whiteside et al., 2016). Additionally, youth experiencing comorbid chronic pain and mental health diagnoses show two times the risk for developing long-term opioid use as compared to no use (Richardson et al., 2012).
Childhood trauma can also contribute to increased risk of adverse pain and opioid use outcomes, independent of mental health diagnoses such as anxiety and depression (Tietjen et al., 2010). Physical and emotional abuse in childhood are associated with various pain diagnoses in adulthood, including chronic migraines, arthritis, irritable bowel syndrome, and fibromyalgia (Tietjen et al., 2010). Further, individuals reporting childhood trauma are also more likely to experience comorbid pain conditions in adulthood (Tietjen et al., 2010), and higher subjective pain and multiple pain complaints are associated with higher risk of opioid misuse (Sehgal, Manchikanti, & Smith, 2012). Additionally, childhood trauma is associated with increased incidence of mental health symptoms, particularly anxiety and depression (Hovens et al., 2010), subsequently compounding risk for opioid abuse via potentiating mental health vulnerabilities.
Distress intolerance
Distress intolerance, or the perceived inability to tolerate painful, aversive physical and emotional states, represents a risk factor for prescription opioid misuse among adults with chronic pain (McHugh et al., 2016). Adolescents who experience pain, including relatively greater distress, and have less ability to navigate, mitigate, or tolerate this distress, can experience a positive reduction in physical and psychological pain in the context of opioid use. Prescription opioids not only possess analgesic properties but also induce a euphoric state that can alleviate negative affect (Brady, McCauley, & Back, 2015). Adolescents’ perception of pain severity can be a stronger predictor of long-term use than injury severity itself (Whiteside et al., 2016). Similar findings have demonstrated that fear of pain in children with new-onset pain predicts higher pain-related disability (Lewandowski Holley et al., 2017). Further, anxiety sensitivity predicts pain chronicity (Page, Stinson, Campbell, Isaac, & Katz, 2013). Consequently, youth experiencing high levels of distress intolerance may be at increased risk for both opioid misuse as well as adverse consequences of pain experience. This may turn into a feed-forward loop, as chronic pain and pain-related disability are also associated with long-term opioid use, thereby creating a multidirectional pattern of long-term synergistic risk for opioid consumption compounded by the interaction of psychophysiological and somatic processes (Roeckel, Le Coz, Gavériaux-Ruff, & Simonin, 2016).
Postprescription risk factors
Persistent pain
Given that chronic postoperative pain has been observed in pediatric samples (Fortier, Chou, Maurer, & Kain, 2011) and impacts up to one quarter of children (Page et al., 2013; Rabbitts, Fisher, Rosenbloom, & Palermo, 2017), it is important to account for the compounded risk of opioid misuse in youth whose pain persists and intensifies. Among high school students reporting nonmedical use of prescription opioids, previous medical use was associated with pain relief motives to use (McCabe & Cranford, 2012). This indicates both persistent pain within this population and the risk of postprescription nonmedical use that is facilitated by a legitimate prescription and motivated by ongoing, untreated pain.
Pain catastrophizing
Pain catastrophizing has been associated with increased opioid misuse in adults (Martel, Wasan, Jamison, & Edwards, 2013; Morasco, Turk, Donovan, & Dobscha, 2013). In contrast, low pain catastrophizing and higher pain self-efficacy can be protective (Asghari & Nicholas, 2001; Kalapurakkel, Carpino, Lebel, & Simons, 2015; Ramirez-Maestre, Esteve, Ruiz-Parraga, Gomez-Perez, & Lopez-Martinez, 2017); youth with higher pain self-efficacy are less likely to become disabled in the context of chronic pain (Kalapurakkel et al., 2015) and possibly acute pain (Sandborgh, Johansson, & Soderlund, 2016). Additionally, in adults, prescription opioid use predicts sustained pain and disability as well increased pain sensitivity (Chou et al., 2015; Dobscha et al., 2016; Dowell et al., 2016; Edwards et al., 2016). Thus, seeking to achieve pain relief can perpetuate opioid misuse among adolescents (McCabe & Cranford, 2012; McCabe, West, & Boyd, 2013b; Whiteside et al., 2016).
Positive opioid experience
Receipt of a legitimate opioid prescription can and, unintentionally, does expose previously substance-naïve youth to a pleasurable “high” experience (Brady et al., 2015; McCabe & Cranford, 2012), often under the assumption of safety derived from a prescription from, and presumed oversight by, a medical professional. Youth with little to no drug experience, nonexistent or ambiguous expectations regarding substance use, or negative perceptions of substance use may find these secondary benefits of opioid use to be pleasurable, or at least beneficial in terms of assuaging physical or emotional pain. Thus, non-drug-seeking youth may inadvertently be at elevated risk for opioid misuse simply because they experienced a pain condition and received a legitimate prescription (McCabe & Cranford, 2012; Miech et al., 2015). Among adolescents with minimal exposure to and high disapproval of illicit substances, a legitimate opioid prescription predicted misuse of opioids after high school, potentially because of pain relief and a safe drug experience that contradict negative expectations and high-risk perception (Miech et al., 2015). This is worthy of note, as positive initial drug experience is highly associated with future misuse (Lynskey et al., 2003). In turn, exposure to positive analgesic and stress-reducing aspects of opioids can thus exacerbate both neural and behavioral risk for continued use, even for non-drug-seeking youth, during this highly sensitive period of neurodevelopment.
Peer Group Risk Factors for Opioid Misuse in Youth
Preexisting contextual risk factors
Peer(s) with substance use
As reviewed in recent overviews of the impact of peers on adolescent substance use (Caouette & Feldstein Ewing, 2017), the proportion of substance-using friends continues to be one of the strongest predictors of adolescents’ decision to engage in substance use (Connell, Gilreath, Aklin, & Brex, 2010). Furthermore, adolescents’ perception of peer substance use relates to current and future substance use (D’Amico & McCarthy, 2006; Kilmer et al., 2006). This parallels findings from studies with adolescents and emerging adults (ages 14 to 21), in which peer behavior contributed to much poorer alcohol and cannabis use outcomes as distally as 7 years post-initial examination (Feldstein Ewing, Filbey, Loughran, Chassin, & Piquero, 2015).
Given the high impact of peers on adolescent substance use across the fields of cannabis, alcohol, and tobacco, numerous prevention and treatment teams have increasingly been incorporating peers into their intervention programming in an effort to enhance adolescent treatment response (Colder et al., 2017; Lee et al., 2014), including on electronic/social-media peer platforms (Steers, Moreno, & Neighbors, 2016). Given the strong relationships between peer behavior and risky substance use in other substances of abuse, it is probable that similar effects exist for prescription opioids; however, there is, to date, no research addressing peer influence on prescription opioid use in the context of pediatric pain. Youth with pain are more likely to be bullied and isolated from peers (Forgeron et al., 2010); it therefore stands to reason that, among youth experiencing pain, navigating peers may increase risk of engaging in substance use, including use of opioids, for the purpose of regaining social capital or fitting in. Although there is not yet enough evidence to distinguish youth’s specific motives for opioid use in terms of pain mitigation versus social navigation, this represents a salient risk and potential point of intervention for high-school-aged youth in light of the influential nature of peer relationships on youth engagement in substance use.
Low perceived risk of harm from opioid use
There is an inverse relationship between perception of risk and engagement in substance use (Johnston, O’Malley, Bachman, & Schulenberg, 2012; Lipari, 2013), such that perceived risk of harm is associated with greater likelihood of delayed transition to experimentation and use (Feldstein Ewing et al., 2017; Grevenstein, Nagy, & Kroeninger-Jungaberle, 2015; Piontek, Kraus, Bjarnason, Demetrovics, & Ramstedt, 2013). Opioids are unique by virtue of the fact that they are provided by medical professionals in the context of treatment, potentially resulting in mixed signals with respect to their associated risks; a majority of college students do not perceive great harm from regular use of prescription opioids (Lord et al., 2011). While there is minimal research addressing the trajectory of risk perception surrounding prescription opioids in children and adolescents, low perceived harmfulness is related to misuse of prescription opioids in college students, and high perceived harmfulness is a protective factor (Arria, Caldeira, Vincent, O‘Grady, & Wish, 2008).
Given the evidence that perceived risk of substances is connected to adolescents’ willingness to experiment with substances (Kosterman et al., 2016; Lipari, 2013), teens with low perceived risk of opioids are likely to feel less urgency around limiting their prescription opioid use to the context of pain management. In contrast, they may be more likely to experiment with their peers’ opioid prescriptions and/or transition to misuse of their own opioid prescriptions (Johnston, O’Malley, Bachman, & Schulenberg, 2008; McCabe, Boyd, Cranford, & Teter, 2009; McCabe & Cranford, 2012); this behavior is facilitated by the frequent abundance of leftover medication that remains even after pain remits and easy accessibility of parents’ medications (Friese, Moore, Grube, & Jennings, 2013; Voepel-Lewis, Zikmund-Fisher, Smith, Zyzanski, & Tait, 2015). For example, youth who have low perceived risk of harm from opioids may be at increased risk of using not to manage pain but rather to derive other perceived positive benefits (e.g., mood-enhancing, stress-reducing, and anxiolytic effects). In contrast, adolescents with high perceived risk of harm may be better able to terminate use of prescribed opioids as soon as pain remits. At the same time, a positive first experience within a medically legitimate context can lower perception of risk and increase positive expectancies of pain medication, even among those reporting strong negative feelings about substance use (Miech et al., 2015).
Postprescription risk factors
Available peer opioid prescriptions
Among adolescents, peers are a leading source of prescription opioids that facilitate illicit use (McCabe & Boyd, 2005; McCabe, Cranford, Boyd, & Teter, 2007). Preliminary work shows 12- to 17-year-olds who struggle with opioids obtain them from their peers (Russell, Trudeau, & Leland, 2015); although the proportion of youth who obtain opioids from their peers for pain management versus recreational use remains unknown, these groups are not mutually exclusive (McCabe et al., 2009; McCabe & Cranford, 2012). Among high school seniors who report misuse of prescription opioids, 55% endorsed receiving them for free from a friend or relative, 37.9% endorsed buying them from a friend or relative, and 22.2% endorsed taking them from a friend or relative without asking (McCabe, West, & Boyd, 2013a). It is notable that using prescription opioids received from peers, but not from parents, is associated with riskier routes of administration (e.g., intranasal) and more problematic substance use behavior (McCabe et al., 2007, 2013a). Additionally, adolescents who use opioids nonmedically but were introduced to them in a medical context are more likely to seek out prescription opioids illicitly for pain relief, rather than experimental, reasons as compared to those who initiated opioid use recreationally (McCabe & Cranford, 2012).
Peer norms regarding opioids
Throughout the extensive biopsychosocial changes of adolescence (Windle et al., 2008), peer behavior remains a steadfast predictor of adolescent substance use. Adolescents experience a surge in self-consciousness, becoming keenly attuned to peers’ opinions (Sebastian, Burnett, & Blakemore, 2008) in response to both actual and presumed levels of peer scrutiny (Elkind, 1967). Youth spend less time with parents and peer input takes primacy (Ernst, Pine, & Hardin, 2006; Sebastian et al., 2008), particularly for youth with difficult parent relationships (Windle et al., 2008). Simultaneously, most youth begin to make decisions about whether and when to engage in substance use, situations that most often arise in peer-based contexts (Caouette & Feldstein Ewing, 2017). In light of this, adolescents are particularly susceptible to perceived normative behavior of peers and are more likely to engage in substance use behavior that they believe to be standard in their peer group (Litt & Stock, 2011); roughly 16% of high school seniors report using prescription opioids nonmedically to fit in (McCabe et al., 2009). Many adolescents overestimate the amount of substance use, including prescription opioids, in their peer group (McCabe, 2008; Sanders, Stogner, Seibert, & Miller, 2014), which makes them more susceptible to substance use and related problems (Haug, Ulbricht, Hanke, Meyer, & John, 2011; Perkins, 2012). Youth experiencing pain are vulnerable to bullying from peers (Forgeron et al., 2010), potentially also increasing their vulnerability to peer influence and perceptions of normative peer behavior.
Familial Risk Factors for Opioid Misuse in Youth Experiencing Pain
Preexisting contextual risk factors
Parent(s) with chronic pain
The genetic heritability of chronic pain is well established (Hestbaek, Iachine, Leboeuf-Yde, Kyvik, & Manniche, 2004), and the burden experienced by parents with chronic pain often extends to their children (Stone & Wilson, 2016). A growing body of research reflects increased risk of chronic pain and disability in offspring of adults with chronic pain (Coenders et al., 2014; Hoftun, Romundstad, & Rygg, 2013; Piira & Pullukat, 2006; Stanford, Chambers, Biesanz, & Chen, 2008). While there is a dearth of research specifically on opioid use outcomes in children of parents with chronic pain, parental chronic pain increases the risk for other types of adolescent substance use, including alcohol and tobacco use (Kaasboll, Lydersen, & Indredavik, 2014). Consequently, there is reason to believe that parental chronic pain enhances the risk of adolescent opioid misuse via increased adolescent pain experience, persistence of adolescent pain problems, and, while the mechanisms of effect are unknown, increased risk for overall substance misuse (Stone & Wilson, 2016).
The social and emotional climate in the home can even more substantially impact both pain experience and risk of substance use, particularly among adolescents who live with parents (Hestbaek et al., 2004; Hoftun et al., 2013; Mikkelsson, Kaprio, Salminen, Pulkkinen, & Rose, 2001; Palermo, Valrie, & Karlson, 2014). Parents with chronic pain demonstrate a disruption of parenting and attachment styles that are linked to substance use (Hoffmann & Bahr, 2014; Wilson & Fales, 2015). This effect is compounded in children with two parents experiencing chronic pain (Hoftun et al., 2013; Stone & Wilson, 2016). Children living with at least one parent with chronic pain are at increased risk for chronic pain and psychological problems (Evans, Shipton, & Keenan, 2006; Higgins et al., 2015), factors that themselves exacerbate risk for opioid misuse and addiction (Boscarino et al., 2010; Edlund et al., 2010; Liebschutz et al., 2010; Swendsen et al., 2010). This is concerning in light of findings that mothers with chronic pain exhibit a more permissive parenting style (Evans et al., 2006), also associated with adolescent substance use (Donaldson, Nakawaki, & Crano, 2015; Steinberg, Fletcher, & Darling, 1994). Additionally, these youth are often exposed to chronic stressors, such as poor family functioning, family stress, and low family cohesion, that place them at increased risk for adverse physical and mental syndromes including heart disease, hypertension, depression, and anxiety (Repetti, Taylor, & Seeman, 2002; Stone & Wilson, 2016).
Parents with chronic pain catastrophize about their child’s pain more, subsequently communicating high-threat information about pain; this can, and does, influence their child’s beliefs about experiencing pain (Langer, Romano, Levy, Walker, & Whitehead, 2009; Stone & Wilson, 2016). This also leads to communication that rapid pain amelioration through administration of analgesics is the best method to negotiate pain. Moreover, evidence supports a relationship between maternal medicating behavior and administration of over-the-counter analgesics to their children (Jensen et al., 2014). This transmission of information, modeling of pain experience, and connection of pain to impaired function leads to higher child-reported pain and activity restriction (Stone & Wilson, 2016).
Parent behaviors
There are numerous routes whereby parent factors exacerbate substance use risk. Family substance use history can contribute to differential brain processing in the context of substance use and rewarding positive experience of substance use, subsequently increasing adolescent likelihood of use (Cservenka, Alarcón, Jones, & Nagel, 2015). Similarly, parent substance use at home, including norms of use around the house and approval of recreational substance use, impacts adolescents’ perception of when, where, and how substances should be used (Epstein et al., 2015; Gilligan & Kypri, 2012).
In turn, one of the most modifiable parental behaviors around substance use includes parental monitoring (Karoly, Callahan, Schmiege, & Feldstein Ewing, 2015). Less monitored youth have more opportunities to experiment with illicit substances without consequence. They also tend to maintain social ties with peers who use substances, which, in turn, increases likelihood of substance use. Low parental monitoring predicts positive attitudes toward substance use and ties to social environments and peers in which substance use is tolerated or viewed positively, factors associated specifically with opioid misuse (Donaldson et al., 2015). Similarly, parental involvement is a protective factor against opioid misuse in youth (Sung, Richter, Vaughan, Johnson, & Thom, 2005). Parent history, parenting style, and disruptive home environments can impact development of pain and use of analgesic medication in children (Skarstein, Lagerlov, Kvarme, & Helseth, 2016). Finally, the majority of parents who have addictive prescription drugs in the home do not take recommended precautions (e.g., use of a safe) to keep teens from accessing these drugs (Friese et al., 2013), providing easy access to the substance and opportunity to use, particularly among less monitored youth.
Postprescription risk factors
Parents’ perceived risk of opioids
Parents are an influential factor in modeling their children’s pain responses. Social Learning Theory posits that children’s responses to pain may be learned through observation of their parents’ responses to pain (Bandura, 1977). When children are younger, they are strongly influenced by their parents, rendering parental behavioral modeling of medication use highly impactful during early developmental stages. Thus, parent beliefs and behaviors around pain, pain medication, and medical treatment influence children’s beliefs through this observational learning (Bandura, 1977; Levy et al., 2004; Van Tilburg et al., 2015) and are a contributing factor to adolescents’ attitudes about analgesic medication (Holmstrom, Bastholm-Rahmner, Bernsten, Roing, & Bjorkman, 2014). Parents model pain medication use (routine use or with increased pain), which is influenced by their own perceptions of opioid risk (Kosterman et al., 2016). Particularly in younger age groups, parental beliefs about medication, its dangers, and its utility influence children’s medication compliance (Kankkunen, Vehviläinen-Julkunen, Pietilä, Kokki, & Halonen, 2003). For parents of children undergoing elective outpatient surgery, (mis)information about pain medication predicted dose of analgesic medication (Rony, Fortier, Chorney, Perret, & Kain, 2010), resulting in poor control of their child’s pain and a surplus of opioid analgesic medication in the home (Porucznik et al., 2010; Voepel-Lewis et al., 2015).
Household opioid availability, storage, and monitoring
Prescription opioid availability in the home is also a critical contributing factor, particularly for youth experiencing pain. Many parents, particularly those of younger children, may very carefully administer medication such that they are left with a large amount of leftover medication (Mazer-Amirshahi, Mullins, Rasooly, van den Anker, & Pines, 2014; Rony et al., 2010). Ultimately, 79% of families have enough leftover medication to treat pain for 2 to 3 additional weeks after initial symptom resolution (Voepel-Lewis et al., 2015). Similarly, parents are frequently prescribed more opioids than they need or use and keep the remainder at home (Porucznik et al., 2010). Given the high cost of many medications, it is not surprising that many parents often do not dispose of leftover medication and report intent to keep the medications in the home for future use (Abou-Karam et al., 2015). Furthermore, parents infrequently lock prescription medications, and over 50% of teens report easy access to medication in their parent’s medicine cabinet (Friese et al., 2013). These factors result in a cache of opioids around the house that can be easily misused or overtaken by children and adolescents (Burghardt et al., 2013). Given the connection between availability and transition to abuse (Gillespie, Neale, & Kendler, 2009), household availability can serve as a context for opioid prescription misuse, particularly among youth whose pain has been undertreated (McCabe & Cranford, 2012). In fact, 40% of high school seniors report sourcing misused opioids from accessing their own previous prescription (Johnston et al., 2008), and a significant portion report being given prescription opioids by family members or simply taking them without permission (McCabe et al., 2013a). Additionally, household availability is a significant risk factor for youth who experience and remember positive pain resolution and emotional outcomes from opioids (Casey et al., 2010; Conrod & Nikolaou, 2016; Hollenstein & Lougheed, 2013).
Parents also influence adolescent opioid use via medication monitoring. A majority of adolescents report no parental supervision of their opioid medication (Ross-Durow, McCabe, & Boyd, 2013). This can set the stage for difficulties knowing when or how to discontinue legitimate use after pain abatement as well as exacerbate misuse following medical use (Johnston et al., 2008; Miech et al., 2015). There are limited data on how medication is managed within the family (i.e., parent monitoring of pain and medication) and which youth continue to experience pain symptoms and pain-related anxiety when they stop opioids or seek continued medication despite resolution of pain.
Parent pain catastrophizing
Adolescents with chronic pain conditions are able to accurately observe and report on parental pain behaviors, indicating that pain-specific social learning is an influential factor in the development of chronic pain conditions (Bandura, 1977; Stone & Wilson, 2016). Parental catastrophizing of a child’s pain is associated with greater pain and pain-related disability in the child (Rabbitts, Zhou, Groenewald, Durkin, & Palermo, 2015; Wilson, Moss, Palermo, & Fales, 2014). Thus, parents can model maladaptive pain responses and reinforce these behaviors in their children (Stone & Wilson, 2016). Given that pain experience is linked to licit and illicit opioid use, parents can indirectly impact their child’s opioid use behavior through pain catastrophizing. Furthermore, parents who are highly fearful of and/or reactive to pain may increase their child’s vulnerability to pain through teaching pain responses, such as overprotecting children from the threat of bodily pain via use of analgesic medication at the expense of normalizing the experience of pain, communicating appropriate levels of pain tolerance, and modeling nonpharmacological approaches to coping with it.
Risks and Adverse Outcomes Associated With Opioid Treatment for Pain
Chronic pain, disability, and hyperalgesia
Among adults, there is evidence for an iatrogenic relationship between opioids and pain, wherein continued use of opioids increases pain sensitivity (Edwards et al., 2016). In adults, chronic opioid use increases risk for persistent pain, disability, and opioid-induced hyperalgesia (Roeckel et al., 2016; Yi & Pryzbylkowski, 2015). In both VA and other health care system patients, adults prescribed the highest doses of opioids are most likely to have comorbid pain-related diagnoses, comorbid psychiatric and substance use disorders, and higher pain intensity (Kobus et al., 2012; Morasco, Duckart, Carr, Deyo, & Dobscha, 2010; Morasco et al., 2017). Continued opioid prescriptions are also associated with less sustained improvement in adults (Dobscha et al., 2016). While these poorer outcomes could be due to chronic opioid therapy patients being more likely to evidence severe or unremitting pain conditions, adult initiates of long-term opioid therapy for chronic pain have poorer pain and activity interference outcomes than do patients with minimal or no opioid use, even within comparable pain types (Turner et al., 2016). Given the observed trajectories for adults administered prescription opioids in medical settings, it is plausible that children and adolescents with similar pain and opioid treatment experiences are also at increased risk for poorer outcomes in terms of pain and disability and opioid misuse trajectories. It is important to note that the directionality and causality of chronic opioid use and these adverse outcomes are unclear, as there is a lack of long-term (i.e., over 1 year) research directly comparing opioid therapy as compared to no treatment. Thus, those patients who received long-term opioid therapy (beyond 3 months) and/or high doses may be at risk for adverse outcomes simply by the nature of their pain condition.
Continued use of opioid prescription, refills, and dosage
One highly relevant risk factor for which data are lacking regards which adolescents are likely to obtain a refill and how refills impact later opioid misuse. Even less is known about which adolescents are able to terminate opioid use. Physician instruction to discontinue use within a certain timeframe does influence opioid cessation after injury, but it is not standard practice to provide specific instructions about how and when to stop (Holman et al., 2014). Prescriptions are dispensed with limited label instructions (e.g., “take 1–2 tablets as needed every 4 hours”), and written instructions are often inadequate, poorly comprehended, and misplaced by patients (Osborne & Bryant, 2003; Spandorfer, Karras, Hughes, & Caputo, 1995). Thus, decisions about when and how to discontinue use is often left up to youth and their parents.
While the majority of longitudinal research exists in adult populations, emerging evidence with adolescents suggests that that legitimate use of prescription opioids in adolescence increases risk of long-term opioid use for pain management (McCabe, Veliz, & Schulenberg, 2016; Miech et al., 2015). Clearly, the pain experience necessarily predicates receipt of an opioid prescription. However, the initial utilization of opioids for acute pain increases risk for continued use of opioids as a primary method of analgesia (Shah, 2017), potentially at the expense of other less risky methods of treatment. Furthermore, continued use of opioids to treat chronic pain is associated with increased sensitivity to pain, physiological tolerance to opioids, and opioid use disorder (Blanco et al., 2016; Roeckel et al., 2016), further perpetuating opioid use and its cyclical relationship with poor pain outcomes.
Opioid-related substance abuse problems
Among adolescents and young adults who use heroin, easy access to prescription opioids through personal prescriptions, home availability, and access through friends were key factors in transitioning from oral use of prescription opioids (Lankenau et al., 2012). Both accidental and intentional opioid overdose and poisoning have also become increasingly common among both younger children and adolescents (Burghardt et al., 2013). These phenomena are more consistently established in adult research: Among adults, opioid misuse has been connected to the transition into heroin use, opioid overdose, and death (Banerjee et al., 2015; Bartels et al., 2016; Martins et al., 2017).
Nonpharmacologic approaches to pain treatment
Little is known about the role of nonpharmacologic, self-management, or complementary and integrative medicine (CIM) pain treatments that may reduce the need for opioid refills in the context of acute pain or opioid prescription in youth (Ali, Drendel, Kircher, & Beno, 2010; Le May et al., 2016). Nonpharmacologic approaches are recommended as part of acute pain management guidelines for children and adolescents (Committee on Psychosocial Aspects of Child and Family Health, 2001). CIM for youth involves specific techniques to optimize pain management, including the PRICE method (protection, rest, ice, compression, and elevation). It also includes broader nonmedication approaches, including short-term immobilization via splint or cast as well as distraction and breathing. Thermal regulation and massage can also mitigate chronic pain (Ali et al., 2010).
In adults, CIM approaches show promise for helping phase out opioid use and misuse (Garland et al., 2017; Mehl-Madrona, Mainguy, & Plummer, 2016). Prior pediatric work shows that youth with chronic pain prefer noninvasive CIM approaches (Groenewald, Wright, & Palermo, 2015; Toliver-Sokol, Murray, Wilson, Lewandowski, & Palermo, 2011; Tsao, Meldrum, Kim, Jacob, & Zeltzer, 2007). Family income has been associated with increased utilization of these approaches (Toliver-Sokol et al., 2011). Preliminary data suggest the promise of intensive interdisciplinary approaches to obviate the need for opioid medications in youth with chronic pain (Bruce et al., 2017).
In addition to CIM, there are a number of behavioral treatments for chronic pain that psychologists, particularly those working in hospital settings, are well poised to implement. There is evidence for behavioral (Block, Kremer, & Gaylor, 1980; Fordyce, Roberts, & Sternbach, 1985; McCracken & Turk, 2002; van Tulder et al., 2000), cognitive behavioral (McCracken & Turk, 2002), and mindfulness-based approaches (Morone, Greco, & Weiner, 2008; Veehof, Oskam, Schreurs, & Bohlmeijer, 2011; Veehof, Trompetter, Bohlmeijer, & Schreurs, 2016) for coping with pain. These approaches contribute to successful chronic pain management in the absence of opioid-based pharmacologic interventions, particularly in reducing pain, distress, and improving daily functioning. The greatest benefit has been observed for adult patients with mild to moderate, rather than severe, pain (McCracken & Turk, 2002). These strategies are also showing true promise in pediatric patients (Eccleston et al., 2014).
Diathesis-Stress Model of Peer and Parent Influences on Pain Outcomes and Opioid Use
While opioid prescriptions are made in response to a patient’s pain presentation, adolescent addiction models typically do not consider the role of pain characteristics, including pain chronicity and expected pain recovery (McCabe et al., 2016). Summarizing the paths of review, the proposed integrated theoretical model (see Fig. 1) draws from diathesis-stress models in which children with high genetic loading for addiction are predisposed to develop substance abuse in the context of exposure to substances (Lorenzetti et al., 2016), developmental models of adolescent substance abuse (e.g., Conrod & Nikolaou, 2016; Prado et al., 2009), and intergenerational models of pain (e.g., Palermo et al., 2014; Stone & Wilson, 2016), with unique consideration for factors relevant to opioid prescriptions and pain. This expanded model posits risk and protective factors at several levels, both pre- and postprescription, including bidirectional and interactive effects, and expands consideration across individual, parental, and peer influences on pain and opioid outcomes. Further, paths are suggested wherein which inherited and environmental individual risks for adverse outcomes lead to lowered resilience in the face of pain experiences, increased availability of prescription opioids, and higher susceptibility to opioid misuse, particularly in risky peer and family contexts.
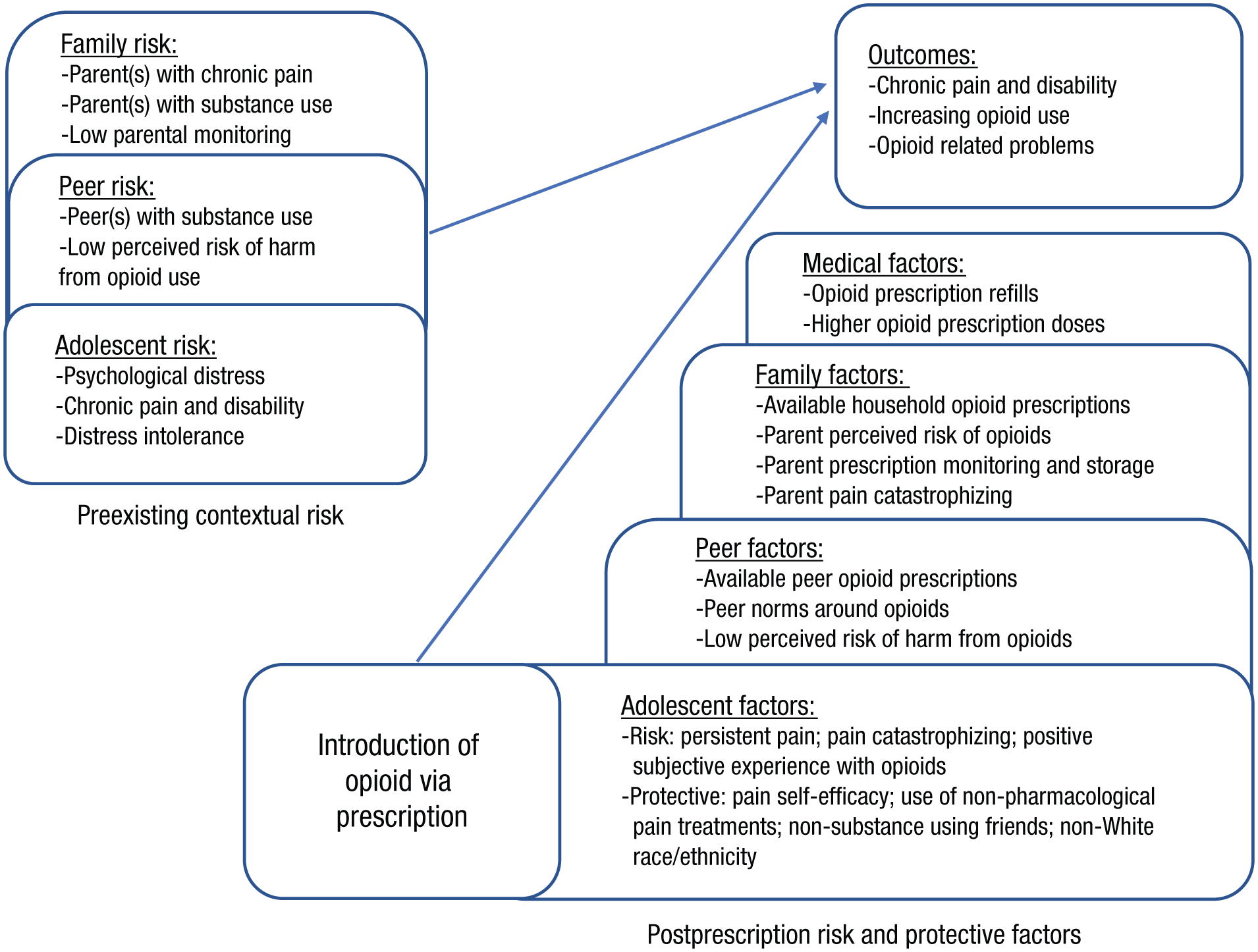
Integrated theoretical model of risk and protective factors for pain and opioid use outcomes among youth receiving an opioid prescription.
Limitations and future directions
While the presented model identifies individual, peer, and familial risks that heighten risk for misuse both before and after prescription receipt, future longitudinal research will help unravel the long-term trajectory of youth experiencing pain who receive opioid prescriptions, including differential use and sequelae for youth with various and distinct motives for their use. Initial steps are being taken in this direction; data regarding refill rates, increasing dosage, and increased pain sensitivity in youth receiving legitimate prescriptions will improve with future studies in this area.
Particularly important to consider in the context of opioid access to children and adolescents with chronic pain is the legal provision of a substance with abuse potential via a medical system accessed for the purpose of treatment. Thus, while models of substance abuse and addiction in youth often integrate the notion that rules and norms are violated in order to engage in such behavior (Conrod & Nikolaou, 2016), the provision of opioids to children and adolescents in a medical setting exposes youth who may not seek out these kinds of illicit experiences to potentially addictive substances. While many youth may express high disapproval of substance use, they are receiving legitimate prescriptions from doctors and are susceptible to increased risk of opioid use disorder even if taking their medication as prescribed (Hah, 2016; McCabe et al., 2016; Miech et al., 2015). Facilitating this effect is the lack of physician-provided information regarding use and discontinuation of use of prescription opiates (Holman et al., 2014), particularly among youth (Dowell et al., 2016; Schechter & Walco, 2016), leaving much of the decision-making regarding adolescent opioid administration up to youth and their parents.
Conclusion
This model offers one initial perspective to inform future development of effective prevention programs for children and adolescents experiencing pain who may be at increased risk for opioid-related problems. Many of the proposed risk and protective factors can be identified and targeted in medical settings, which could lead to the development of prevention programs designed to reduce opioid misuse and abuse. For instance, prevention efforts designed to reduce pain catastrophizing, increase utilization of nonopioid approaches to treating and reducing pain, and provide detailed information on tapering off of opioids might be provided as a means of mitigating the potential risks for opioid misuse. Psychologists working in medical settings are in a unique position to provide input on policies and guidelines that can reduce risk for misuse and abuse among youth prescribed opioids for pain.
Supplemental Material
Dash_Open_Practices_Disclosure – Supplemental material for A Model of the Intersection of Pain and Opioid Misuse in Children and Adolescents
Supplemental material, Dash_Open_Practices_Disclosure for A Model of the Intersection of Pain and Opioid Misuse in Children and Adolescents by Genevieve F. Dash, Anna C. Wilson, Benjamin J. Morasco and Sarah W. Feldstein Ewing in Clinical Psychological Science
Footnotes
Action Editor
John J. Curtin served as action editor for this article.
Author Contributions
G. F. Dash, A. C. Wilson, and S. W. Feldstein Ewing contributed to conceptualization and development of review topic, scope, and content. G. F. Dash drafted the manuscript, and A. C. Wilson, B. J. Morasco, and S. W. Feldstein Ewing provided critical contributions to sections of relative expertise as well as revisions to the manuscript in its entirety. All the authors approved the final version of the manuscript for submission.
Declaration of Conflicting Interests
The author(s) declared that there were no conflicts of interest with respect to the authorship or the publication of this article.
Funding
This work was supported by National Institute on Alcohol Abuse and Alcoholism Grant 1R01-AA023658-01 (to S. W. Feldstein Ewing), Eunice Kennedy Shriver National Institute of Child Health and Human Development Grant R01-HD082200-01 (to A. C. Wilson), National Institute on Drug Abuse Grant R01-DA034083 (to B. J. Morasco), and National Institute on Drug Abuse Grant 1R01-DA044778-01A1 (to A. C. Wilson and S. W. Feldstein Ewing).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.