
Abstract
Individuals with suicidal thoughts and behaviors experience abnormalities in reward-related processes, yet little is known about specific components or stages of reward processing that are impaired, especially in children. The primary aim of this study was to conduct an investigation of the Initial Response to Reward subconstruct of the National Institute of Mental Health’s Research Domain Criteria in relation to recent suicidal ideation (SI) in children. Participants were 23 children between the ages of 7 and 11 with a history of recent SI and 46 demographically and clinically matched children with no recent SI. Children completed a simple guessing task during which electroencephalographic signals were continuously recorded to isolate the reward positivity (RewP) event-related potential; specifically, we examined change in RewP (∆RewP), quantified as the difference between neural responses to monetary gains and neural responses to monetary losses. Children with recent SI exhibited significantly smaller (i.e., blunted)
There was a 24% increase in suicide rates between 1999 and 2014 in the United States, and those ages 10 to 14 had the greatest increase (National Center for Health Statistics, 2016), highlighting the importance of identifying early correlates of suicide risk. However, despite the efforts of past research, the field’s progress in the understanding (Franklin et al., 2017) and prevention (Zalsman et al., 2016) of suicide remains limited. According to the conclusions of a recent meta-analytic review, this progress has been stunted largely as a result of a failure to identify and examine novel risk factors in a transdiagnostic manner (Glenn et al., 2018). To this end, the Research Domain Criteria (RDoC) project of the National Institute of Mental Health (NIMH; Cuthbert, 2014) has been suggested as a promising framework capable of addressing these important limitations of prior research (Glenn, Cha, Kleiman, & Nock, 2017; Glenn et al., 2018). Indeed, because of its focus on an integrative dimensional understanding of disordered behavior across traditional diagnostic boundaries, the RDoC is well-suited to advancing our understanding of suicide risk.
Most studies to date have focused on correlates and predictors of suicidal thoughts and behaviors (STBs) that fall within the Negative Valence Systems domain of the RDoC, with significantly fewer studies focusing on other RDoC domains, including the Positive Valence Systems domain, which includes a number of subdomains related to reward processing. This represents an important gap in the literature because the predominant focus on only one RDoC domain limits the field’s ability to identify novel correlates and risk factors of STBs. Indeed, a recent meta-analysis demonstrates the presence of a robust link between anhedonia, the most frequently investigated proxy of reward responsiveness in individuals with STBs, and current suicidal ideation (SI; Ducasse et al., 2018). Note that this association was found to be at least partially independent of the presence of psychiatric disorders, including depression (Ducasse et al., 2018), which further highlights the need to focus on suicidal thinking transdiagnostically.
A recent review suggested that numerous reward processing deficits in suicide attempters (including impairments in reward learning and valuation) contribute to impaired decision making in these individuals (Dombrovski & Hallquist, 2017), which may further heighten suicide risk. More specifically, extant evidence suggests that these individuals, particularly those who engage in unplanned suicidal acts, might tend to overvalue their current state, including reward-related information in their environment, in making decisions (Dombrovski & Hallquist, 2017). Further, suicidal individuals might exhibit impairments in the ability to mentally represent the future, including difficulties estimating the expected value of actions and events (Dombrovski & Hallquist, 2017). Consequently, one could argue that suicidal crises stem, at least in part, from the tendency to overvalue current aversive emotional state coupled with the preference for immediate rewards (i.e., escape from such state) and beliefs that the desired outcomes would fail to occur in the future. This argument is in line with extant suicide theories (for reviews, see Abramson et al., 2000; Klonsky & May, 2015) and ample empirical evidence (O’Connor & Nock, 2014) supporting a link between the construct of hopelessness (i.e., a cognitive state that involves a belief that highly expected outcomes will not occur and negative outcomes will occur in the future) and STBs. However, despite the centrality of reward-related disruptions in STBs, additional research is needed to achieve an accurate and theoretically sound understanding of reward functioning abnormalities in individuals with STBs and their specific contributions to suicidal ideation and suicide attempts.
Although numerous studies have attempted to elucidate the link between self-reported anhedonia and STBs, anticipatory and consummatory stages of reward processing are distinct and have separable neural correlates (Liu, Hairston, Schrier, & Fan, 2011). Indeed, the RDoC construct of Reward Responsiveness includes specific subconstructs for Reward Anticipation versus Initial Response to Reward. Because self-reports likely pick up on impairments in multiple subconstructs related to reward responsiveness and do not necessarily provide objective data on these impairments, research is needed that uses tasks specifically designed to assess initial responses to reward if we are to gain a better understanding of how impairments in these processes may be linked to STBs.
The primary aim of the present study was to begin addressing these prominent gaps in the literature by conducting an investigation of initial response to reward in children with recent SI compared with children with no recent history of SI. Event-related potentials (ERPs) are well-suited for the assessment of this subconstruct because of their millisecond-level resolution of cognitive processes. In the current study, we focused on the reward positivity (RewP; also referred to in the literature as feedback-related negativity or feedback negativity), specifically change in RewP (
The
Method
Participants
Participants for this study were drawn from a larger sample of children recruited from the community. Using a 1:2 matching ratio, we had 23 children with a history of recent SI and 46 children with no recent SI. The two groups were equated on (a) age, (b), sex, (c) race, (d) household income, (e) lifetime history of a major depressive disorder (MDD), (f) lifetime history of any anxiety disorder, and (g) mean current depressive, anxious, and externalizing symptoms. To be eligible to participate in the larger study, children had to be between the ages of 7 and 11 and have no learning or developmental disorders that would make it difficult for them to complete the study. The presence of recent (i.e., in the past 2 weeks) SI in children was assessed using questions about SI from the Schedule for Affective Disorders and Schizophrenia for School-Age Children–Present and Lifetime Version (K-SADS-PL; Kaufman et al., 1997) and the Children’s Depression Inventory (CDI; Kovacs, 1981). Specifically, as part of the K-SADS-PL diagnostic interview, both parents and children were asked, “Sometimes children who get upset or feel bad think about dying or even killing themselves. Have you/your child ever had these types of thoughts?” The interrater reliability of the K-SADS-PL item assessing suicidal ideation in our sample was good (κ = .77). On the CDI, which was administered verbally by a research assistant, children were asked From each group of three sentences, pick one that describes you best for the past two weeks: (1) I do not think about killing myself; (2) I think about killing myself but I would not do it; (3) I want to kill myself(Item 9).
The children who endorsed answer 2 or 3 on the CDI and/or the presence of suicidal ideation during the KSADS-PL interview in the past 2 weeks were classified as having had recent SI. We chose to use this multimethod assessment approach to maximize the disclosure of child SI on the basis of previous research suggesting that individuals might vary in their degree of comfort when reporting on their SI depending on the assessment format (“as patients sometimes deny suicidal ideation in interviews but endorse it on self-report questionnaires”; Koplin & Agathen, 2002, p. 715). In our sample, out of 23 children who were classified into the recent-SI group, a total of 15 endorsed recent SI on both the K-SADS-PL and CDI, and 8 children reported recent SI on CDI but not on the K-SADS-PL. 1 The average age of the children in our study was 9.50 years (SD = 1.29), and 49.3% were female. In terms of race, 68.1% of the children were White, 21.7% were African American, 8.7% were biracial, and 1.4% were Asian/Pacific Islander. In terms of ethnicity, 8.7% of the children were Hispanic. The demographic and clinical characteristics of the recent-SI and no-recent-SI groups are presented in Table 1.
Descriptive Statistics for Children in Each of the Two Groups
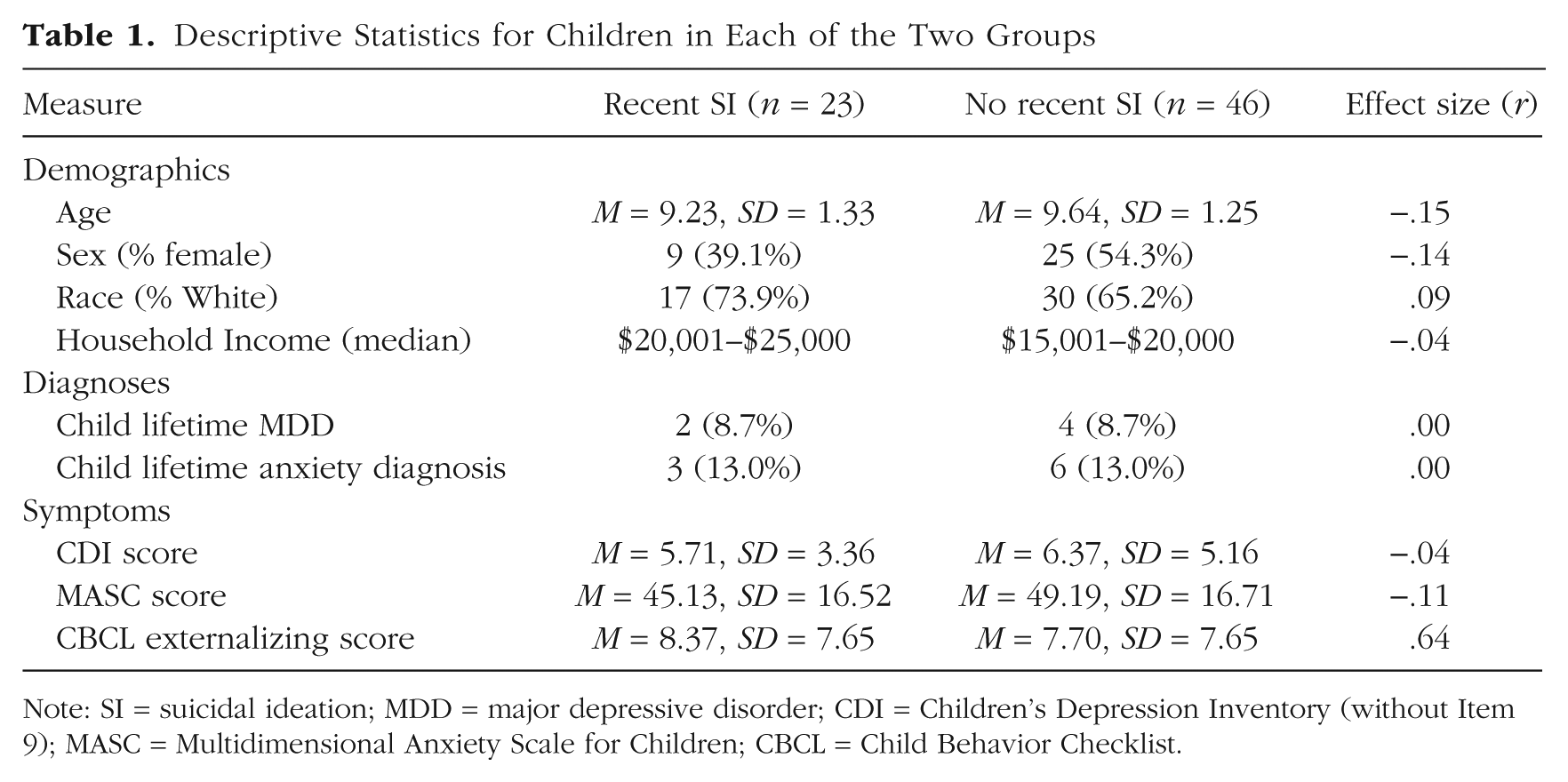
Note: SI = suicidal ideation; MDD = major depressive disorder; CDI = Children’s Depression Inventory (without Item 9); MASC = Multidimensional Anxiety Scale for Children; CBCL = Child Behavior Checklist.
Measures
Diagnoses and symptoms
The K-SADS-PL was also used to assess for current and past MDD and anxiety disorders in children (according to the fourth edition of the Diagnostic and Statistical Manual of Mental Disorders, or DSM–IV; American Psychiatric Association, 1994). In our sample, a total of 6 children (2 girls, 4 boys) met criteria for a lifetime history of MDD, and a total of 9 children (5 girls, 4 boys) met criteria for a lifetime history of an anxiety disorder. To assess interrater reliability, we had a subset of 20 diagnostic interviews from this project coded by a second interviewer, and κ coefficients for diagnoses of MDD and anxiety disorders were good (all κs ≥ .86). In addition to lifetime diagnoses, children’s current symptoms of depression, anxiety, and externalizing problems were assessed using the Children’s Depression Inventory 2 (Kovacs, 1981), the Multidimensional Anxiety Scale for Children (MASC; March, Parker, Sullivan, Stallings, & Conners, 1997), and the Child Behavior Checklist (CBCL; Achenbach & Rescorla, 2000) externalizing subscale, respectively. The internal consistency values for the CDI and MASC scales and the CBCL externalizing subscale were .81, .89, and .91, respectively.
Reward task
The reward task was a simple guessing doors task that is commonly used in studies of reward processing (e.g., Bress et al., 2012, 2015; Foti et al., 2011; Kujawa et al., 2014; Nelson et al., 2016; Tsypes et al., 2017; Weinberg et al., 2015). The task consisted of 50 trials, presented in two blocks of 25 trials. Participants were shown an image of two doors at the beginning of each trial and instructed to guess which door had a monetary prize behind it by pressing either the left or right button on a game controller. They were informed that on each trial, they could either win $0.50, as indicated by a green up arrow, or lose $0.25, as indicated by a red down arrow. Feedback about having chosen correctly or incorrectly was presented for 2,000 ms and then followed by the message “Click for the next round.” This message remained on the screen until the participant responded and the next trial began. Across the task, 25 gain and 25 loss trials were presented in a random order.
EEG data acquisition and processing
During the task, electroencephalographic (EEG) signals were recorded continuously using a custom cap and the ActiveTwo system (BioSemi BV, Amsterdam, The Netherlands). The EEG was digitized at 24-bit resolution with a sampling rate of 512 Hz. Recordings were taken from 34 scalp electrodes based on the 10-20 system. The electrooculogram was recorded from four facial electrodes. Off-line analysis was performed using the extension EEGLAB (Delorme & Makeig, 2004) for MATLAB (The MathWorks, Natick, MA) and the EEGLAB plug-in ERPLAB (Lopez-Calderon & Luck, 2010). All data were rereferenced to the average of the left and right mastoid electrodes and band-pass filtered with cutoffs of 0.1 Hz and 30 Hz. EEG data were processed using both artifact rejection and correction. Large and stereotypical ocular components were identified and removed using independent component analysis (ICA) scalp maps (Jung et al., 2001). Epochs with large artifacts (greater than 100 μV) were excluded from analysis. EEG was segmented for each trial, beginning 200 ms before onset of the feedback stimulus and ending 1,000 ms after onset of the feedback stimulus. On the basis of findings of a recent comprehensive study on internal consistency of functional MRI (fMRI) and EEG measures of reward in late childhood and early adolescence demonstrating that internally consistent measure of response to gain and loss can be obtained using just 14 gain and 14 loss trials of the doors task (Luking, Nelson, Infantolino, Sauder, & Hajcak, 2017), we focused only on children who had at least 14 trials per condition.
In our sample, the average number of gain trials remaining following artifact rejection was 22.54 (SD = 2.42, range = 15–25), and the average number of loss trials was 22.74 (SD = 2.40 range = 14–25). ERPs were separately averaged across gain and loss trials, and the activity 200 ms before feedback onset served as the baseline. These averages were then exported for temporospatial principal component analysis (PCA), which allows for the isolation of the RewP-gain and RewP-loss from the overlapping components. The key strength of PCA, therefore, is that it allows the isolation of the
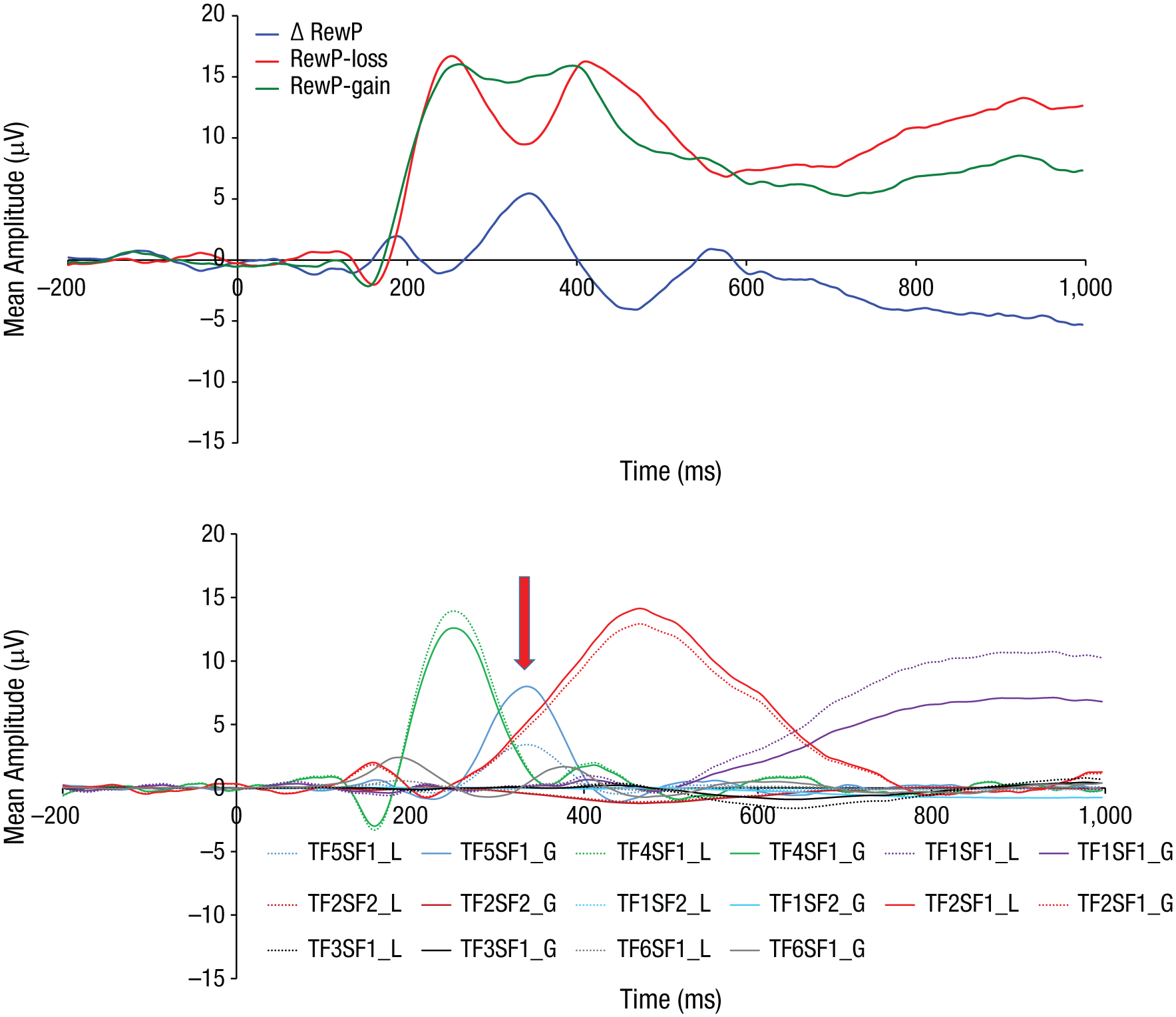
Event-related potentials (ERPs). Top graph shows stimulus-locked mean ERPs at FCz in response to feedback indicating monetary loss (red) and monetary gain (green) as well as the difference waveform (blue) for gain minus loss trials for the full sample. Bottom graph shows eight virtual ERPs (i.e., PCA factor combinations) that accounted for at least 1% of variance each (L = loss condition; G = gain condition, SF = spatial factor; TF = temporal factor). The PCA-derived factor TF5SF1 (indicated by red arrow), which resembled the reward positivity (RewP) in its temporal and spatial distribution, was extracted at FCz and used in the statistical analyses.
To facilitate interpretation of the PCA solutions, after analysis, the ERP PCA Toolkit automatically reproduces the original data, recreating the waveform (in microvolts) of each factor loading by multiplying the correlation factor loadings with the standard deviations of the variables (Dien, 2006). The toolkit then reports the peak channel and peak time point for each factor (Dien, 2010a, 2010b). The PCA-derived factor TF5SF1, which accounted for 3% of total variance and resembled the
Procedure
After arrival at the laboratory, parents were asked to provide informed consent, and children were asked to provide assent to be in the study. Next, the child completed the reward task. During this time, the K-SADS-PL (Kaufman et al., 1997) was administered to the parent by a trained interviewer. Following this, the same interviewer who had administered the K-SADS-PL to the parent also administered it to the child. Self-report questionnaires were also administered to children by a trained interviewer. The institutional review board approved all procedures. Families were compensated a total of $80 for their participation. All children also received a bonus of $5 for completing the reward task.
Results
Focusing first on the
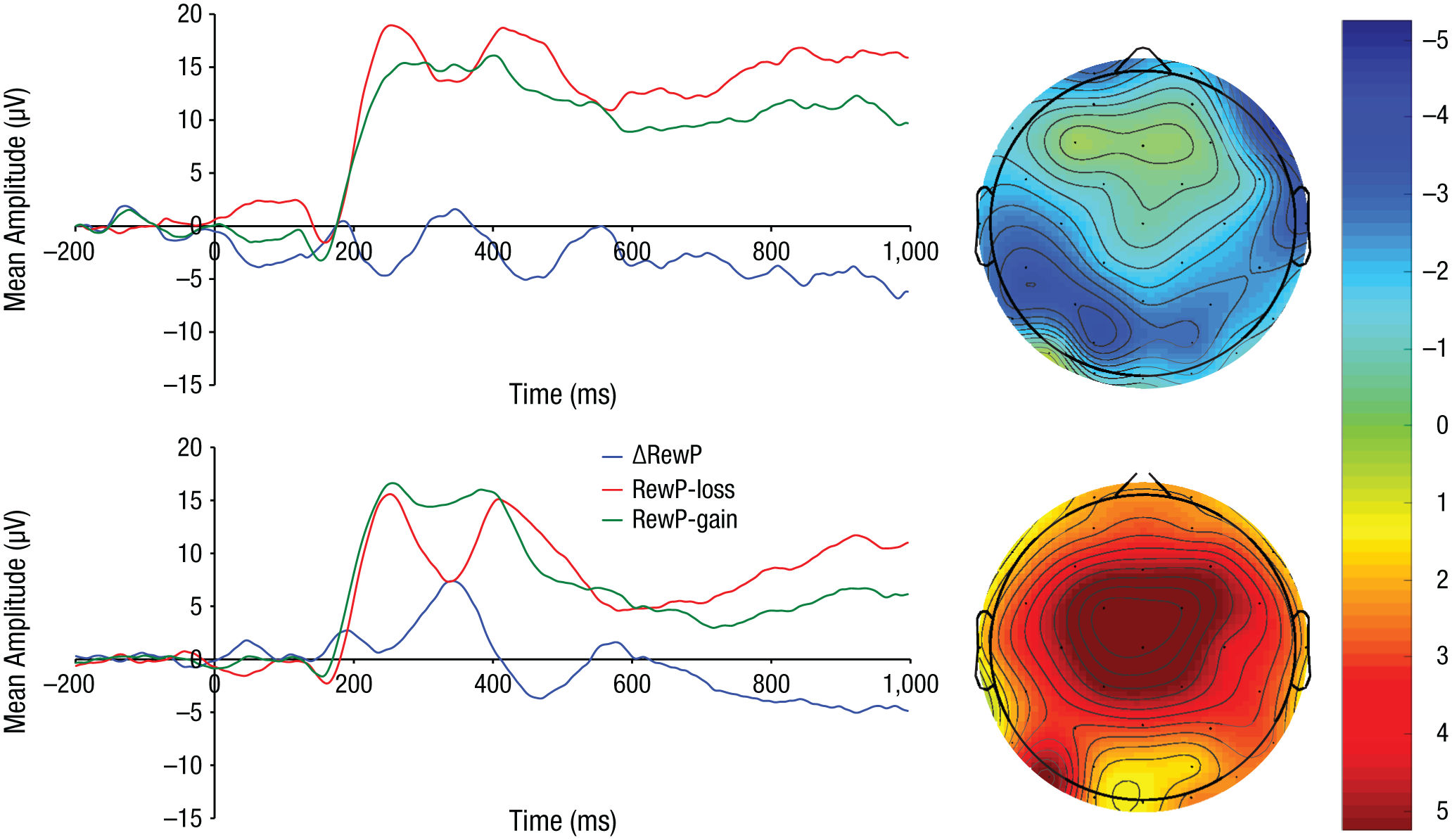
Stimulus-locked mean event-related potentials (ERPs) at FCz in response to feedback indicating monetary loss (red) and monetary gain (green) as well as the difference waveform for gain-minus-loss trials (blue) for children with (top) and children without (bottom) a history of recent suicidal ideation. The topographic scalp maps show the reward positivity (RewP) ERP component 275 to 375 ms after feedback for children with a history of recent suicidal ideation (top right) and those without (bottom right).
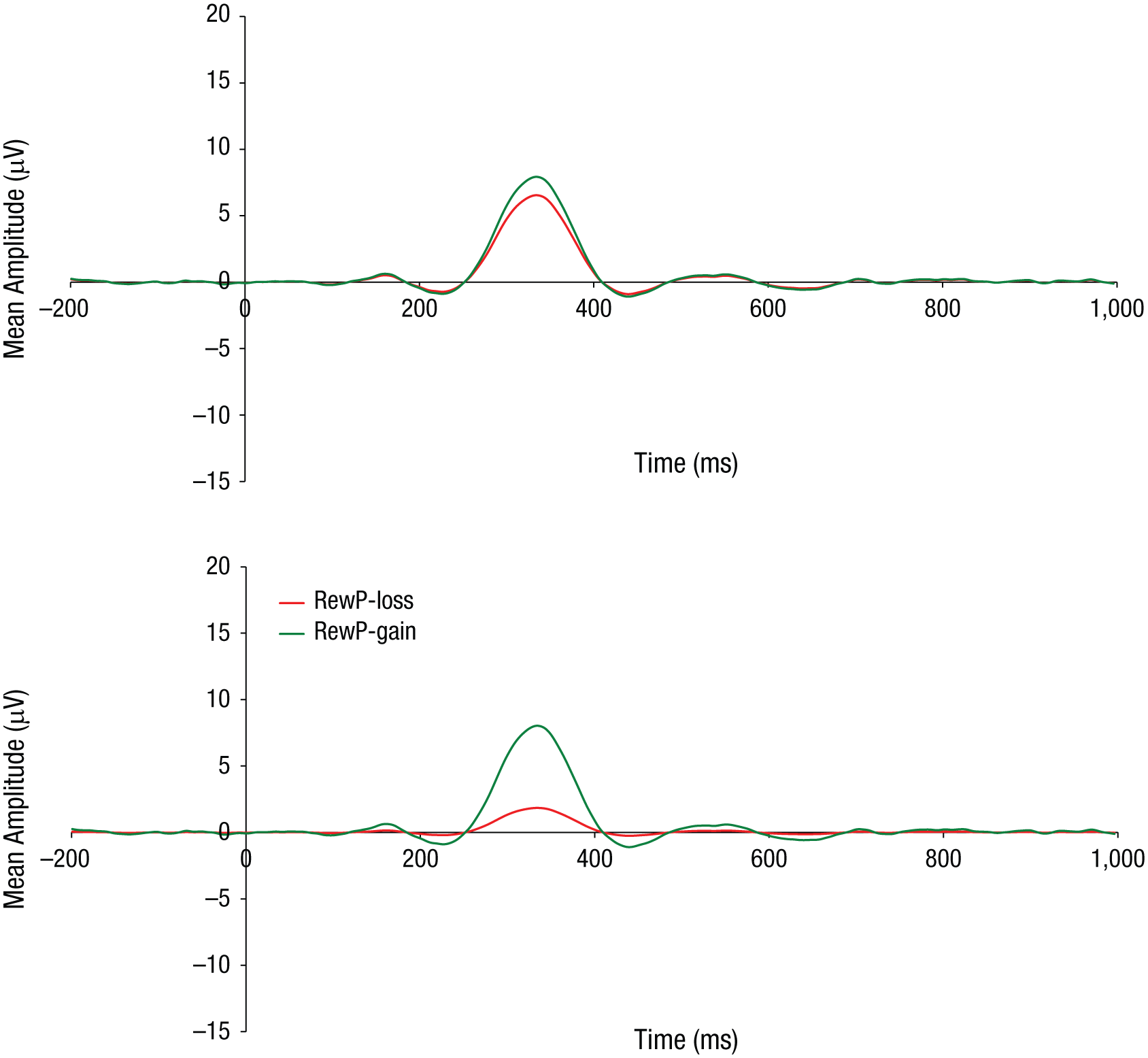
The PCA-derived factor TF5SF1, which resembled the reward positivity (RewP) in response to feedback indicating monetary loss (red) and monetary gain (green) at FCz for children with (top) and children without (bottom) a history of recent suicidal ideation.
Despite the primary focus in this study on the
Discussion
The goal of this study was to examine the RDoC Initial Response to Reward subconstruct in children with a history of recent SI and children with no recent SI. We found that children with a history of recent SI exhibited significantly smaller (i.e., blunted)
Likewise, in the context of depression, anhedonia levels have been shown to affect feedback-related negativity responsiveness to negative feedback (Mueller, Pechtel, Cohen, Douglas, & Pizzagalli, 2015). This suggests some fruitful directions for future studies, such as the potential importance of also examining the characteristics of anhedonia (e.g., recency, severity, chronicity) rather than simply its presence or absence. However, because parental history of a suicide attempt represents a risk factor for a broad range of outcomes in their offspring and not all children of suicide attempters will develop suicidal thoughts themselves, it is possible that heightened neural differentiation between losses versus gains represents one (out of many) pathways of risk for children of suicide attempters. For example, it might be indicative of risk for nonsuicidal self-injury because we also previously found heightened differentiation between gains versus losses in children with a history of NSSI (Tsypes et al., 2018). It is important to note, however, that these conclusions remain speculative until greater advances in the understanding of reward-related abnormalities in relation to different forms of STBs and familial risk for STBs are made.
The present study exhibited a number of strengths and represents an important step in obtaining a more precise understanding of reward-related processes in STBs. Although consistent with ample evidence that links self-reported anhedonia with recent suicidal thinking independently of psychopathology (Ducasse et al., 2018), the present study provides initial evidence that these impairments might also be observed on neural level of analysis. Specifically, this is the first study of which we are aware that specifically examines a neural index of initial response to reward in children with recent SI. Indeed, whereas self-reports are unable to differentiate between different constructs and subconstructs within the Positive Valence Systems domain of the RDoC, the high temporal resolution of ERPs allows for a demonstration of reward-related impairments that are specific to consummatory (i.e., Initial Response to Reward) reward processing. Building on our findings, it will be important for future research to investigate whether similar impairments are observed when other constructs and subconstructs within the Positive Valence Systems domain of the RDoC are examined. In addition, the use of PCA by the present study allowed for the isolation of the
Despite these important contributions of the present study, there were also some limitations that provide directions for future research. First, because of the cross-sectional nature of our study, it will be important for future work to establish whether neural reward responsiveness constitutes an antecedent, consequence, or merely correlate of recent SI and whether our findings generalize to other age groups and other forms of STBs. Relatedly, future research should also examine the potential impact of STB characteristics (e.g., recency, severity, frequency, chronicity) on reward responsiveness. Second, it will also be important for future research to examine the potential moderating effects of participant characteristics (e.g., age, race/ethnicity, sex, sexual orientation, cognitive ability) and types of rewarding stimuli experienced by these individuals (e.g., money, social bonds and interactions, sex, food, music, and art). Third, because of the focus of the present study on the RewP as an index of Initial Response to Reward RDoC subconstruct, it will be important for future research to examine the links between other constructs and subconstructs of reward processing delineated within the RDoC Positive Valence Systems domain in relation to STBs. Finally, despite the focus of the present study on the RewP as a result of the extensive empirical support for the meaning of this component in the context of the doors task, our exploratory analyses showing the presence of between-group differences in the PCA factors that resembled P2 and P3 suggest that it might be fruitful for future work to also examine potential links between these components and STBs.
Taken together, the current study contributes to the literature on the nature of reward processing abnormalities in STBs by providing initial evidence that children with a history of recent SI demonstrate blunted neural responsiveness to gains versus losses. In the current study, we used a demographically and clinically matched sample and we statistically controlled for the potential influence of a range of demographic and clinical variables, which suggests that this pattern of blunted initial response to reward is at least partially independent of children’s history of depression or anxiety disorders and current internalizing and externalizing symptoms. Pending replications and longitudinal investigations, consistent with the precision medicine movement in psychiatry aimed at moving away from the one-size-fits-all approach to more targeted treatment (Cuthbert, 2014; Williams, 2016), these findings might contribute to improved identification, treatment, and prevention of STBs. For example, consistent with the urgent need to identify and examine novel risk factors in a transdiagnostic manner to make significant progress in the field of suicide research (Glenn et al., 2018), neural markers of reward processing might constitute additional variables to be analyzed in machine learning algorithms to more accurately predict suicide risk (Franklin et al., 2017).
Footnotes
Acknowledgements
We thank Katie Burkhouse, Mary Woody, Anastacia Kudinova, Cope Feurer, Sydney Meadows, Michael Van Wie, Devra Alper, Eric Funk, Effua Sosoo, Nathan Hall, Kiera James, Aholibama Lopez, and Kristina Wong for their help in conducting assessments for this project.
Action Editor
Christopher G. Beevers served as action editor for this article.
Author Contributions
A. Tsypes and B. E. Gibb developed the study concept and design. A. Tsypes performed the data analysis and interpretation under the supervision of B. E. Gibb. A. Tsypes drafted the manuscript, and B. E. Gibb and M. Owens provided critical revisions. All the authors approved the final manuscript for submission.
Declaration of Conflicting Interests
The author(s) declared that there were no conflicts of interest with respect to the authorship or the publication of this article.
Funding
The project was supported by National Science Foundation Graduate Research Fellowship Grant DGE1144464 (to A. Tsypes) and National Institute of Mental Health Grant R01-MH098060 (to B. E. Gibb).