
Abstract
We conducted two studies to examine the relationship between social anxiety (n = 134) and social anxiety disorder (SAD; n = 126), social exclusion, and empathic accuracy. Participants were randomly assigned to either a control or an exclusion condition and then observed four videos of targets discussing high school experiences in which they were socially excluded. Participants’ ratings of targets’ emotions while discussing those experiences were compared with targets’ self-ratings. Results of both studies indicated that individuals with social anxiety and SAD displayed greater empathic accuracy than control subjects and that exclusion did not affect that relationship. State measures of participants’ emotional and cognitive reactions to targets mediated the association between SAD and accuracy. When asked to provide advice to targets, SAD participants provided fewer responses overall and fewer suggestions that promoted relationship repair. Thus, they were less able to translate their empathic responses for social pain into prosocial action.
Individuals with social anxiety disorder (SAD) have been shown to have fewer and lower-quality intimate relationships (Cuming & Rapee, 2010; Rodebaugh, 2009). They perceive themselves as having few close friends and relationships and can also be viewed less positively in initial social interactions (e.g., Alden & Wallace, 1995; Blöte, Kint, & Westenberg, 2007; Heerey & Kring, 2007; Voncken, Alden, Bögels, & Roelofs, 2008). Relational theorists propose that a key skill in developing and maintaining close relationships is the ability to experience and express empathy for other people’s emotions. Therefore, we conducted two studies to examine empathic accuracy in individuals with social anxiety (Study 1) and with SAD (Study 2) to determine whether SAD is associated with deficiencies in empathic responding and to begin to delineate the processes that underlie and influence empathic responding in these individuals.
Research on SAD and emotion judgments has produced inconsistent results. Individuals with SAD have been found to have difficulty judging the complex versus basic emotions of others and to perform worse on measures of social cognition (e.g., Hezel & McNally, 2014; Janssen et al., 2014; O’Toole, Hougaard, & Mennin, 2013). However, not all studies found deficits (e.g., Jacobs et al., 2008; Tibi-Elhanany & Shamay-Tsoory, 2011). A recent meta-analysis revealed an association between social anxiety and poor intrapersonal emotion knowledge, in that there was a larger effect size for clinical than for nonclinical socially anxious samples (O’Toole et al., 2013). However, clinical diagnosis did not influence the effect size for interpersonal emotion knowledge. Likewise, a recent study found that a clinical sample of individuals with SAD was less accurate on two theory-of-mind tasks but that the effect was weaker for negative emotions (Washburn, Wilson, Roes, Rnic, & Harkness, 2016). This finding was in contrast to an earlier study in which individuals with SAD performed worse on the same tasks when the stimuli involved negative emotions (Hezel & McNally, 2014). Finally, one study found that socially anxious participants displayed greater accuracy in judging others’ negative emotions (Auyeung & Alden, 2016). Therefore, further research on empathic responding would add to what is known about the way in which SAD affects judgments of complex social emotions.
The construct of empathy contains two elements, a cognitive component involving the ability to comprehend the other person’s thoughts and feelings, essentially placing oneself in their position, and an emotion-driven component involving awareness and partial sharing of another person’s emotions (Davis, 1994; Ickes, 1997; Singer, 2006). Empathy has traditionally been measured using self-report; however, such reports reflect how one perceives oneself and therefore provide little information about the accuracy of emotion judgments (e.g., Ickes, 2001; Michalska, Kinzler, & Decety, 2013). Accordingly, researchers introduced the method of using an objective referent to measure empathic accuracy. In this technique, target individuals are video recorded talking about an experience, and targets and perceivers rate the emotions they experienced at various points of the recording. Empathic accuracy is measured by how closely perceivers’ ratings are to the targets’ ratings (Ickes, 2001).
Accurate empathy has often been viewed as beneficial because it allows individuals to align themselves with others in a way to coordinate and facilitate positive interpersonal outcomes (e.g., Anderson & Keltner, 2002). Empathic accuracy was found to be associated with successful negotiations (Elfenbein, Maw-Der, White, Hwee-Hoon, & Aik, 2007), leadership effectiveness (Rubin, Munz, & Bommer, 2005), more supportive relationships (Verhofstadt, Buysse, Ickes, Davis, & Devoldre, 2008), and general social adjustment (e.g., Gleason, Jensen-Campbell, & Ickes, 2009). However, accurate empathy does not always have positive effects and can even be harmful in situations involving social threat. For example, greater empathic accuracy on the part of perceivers predicted declines in feelings of closeness to their marital partners when discussing relationship-threatening problems (Simpson, Oriña, & Ickes, 2003). Conversely, individuals who underestimated their partner’s emotional reactions to alternate romantic partners experienced greater relationship satisfaction than individuals who were more accurate (e.g., Simpson et al., 2011). Likewise, mothers who were more empathic toward children with depressive symptoms showed heightened immune system inflammatory responses (Manczak, Basu, & Chen, 2015). In addition, greater empathy in individuals whose profession involves “emotion work” (e.g., first responders, health professionals) was found to increase risk of burnout and vicarious trauma (e.g., Alexander & Klein, 2009). Finally, Bloom (2016) argued that empathy can result in biases that impede rational decision making and actions.
The above studies indicate that a certain degree of empathic inaccuracy can be adaptive when individuals are faced with social threat. It is also important to note that individual differences in threat sensitivity were found to moderate the relationship between social threat and empathic accuracy. For example, when discussing relationship-threatening situations in romantic relationships, anxiously attached individuals tended to be more accurate than nonanxious individuals; however, their accuracy predicted lower relationship satisfaction and subsequent relationship breakup (Simpson et al., 2011; Simpson, Ickes, & Grich, 1999). Conversely, individuals who were less sensitive to social threat (i.e., low rejection sensitivity) underestimated the negativity of ratings from potential dating partners when they believed they were being rated as opposed to when another individual was being rated. Thus, although emotion judgments might be accurate, threat sensitivity can lead to unnecessary self-protective behaviors that inhibit adaptive social responses and unintentionally lead to negative reactions from others (e.g., Romero-Canyas & Downey, 2013; Romero-Canyas, Downey, Berenson, Ayduk, & Kang, 2010). In early stages of both romantic and nonromantic relationships, it can be adaptive to underestimate social threats and downplay negative perceptions (e.g., Fletcher & Kerr, 2010; McKay & Dennett, 2009). These findings indicate that the relationship between accurate empathy and interpersonal functioning is more complex than previously conceptualized. Because individuals with SAD display greater rejection sensitivity, they provide another opportunity to address the role of individual differences in empathic responding.
The mixed findings also point to the influence of contextual factors on the effects of empathic responding. Research on physical pain indicates that individuals who are in pain themselves display greater empathy toward others in pain. For example, studies revealed activation in the anterior insula and dorsal anterior cingulate cortex, two areas associated with affective processing, when individuals felt physical pain and when they viewed others experiencing the same pain (Botvinick et al., 2005; Jackson, Meltzoff, & Decety, 2005; Morrison, Lloyd, Di Pellegrino, & Roberts, 2004; Singer, 2006).
The findings raised questions about whether social pain (i.e., distress arising from adverse social events such as exclusion) might have the same effect. Social pain activates many of the same brain circuits and produces many of the same effects on mood and behavior as those involved in physical pain (Eisenberger, 2011). Several studies found that socially excluded individuals rated scenarios of social exclusion to be more painful, recommended more severe punishment for bullies and more support for bullying victims, and felt worse watching others who had been excluded in the same manner they were (Masten, Morelli, & Eisenberger, 2011; Nordgren, MacDonald, & Banas, 2011). Although these findings suggest that social pain might improve empathic responding, empathy was measured on dimensional scales of how “bad” the perceiver felt for the victim rather than as a form of accuracy. Thus, it is not clear whether perceivers’ perceptions were accurate or simply more negative. Studies examining accurate empathy are inconsistent. Nordgren et al. (2011) found that, compared with included individuals, excluded individuals made more accurate estimates of their partner’s social pain when partners were similarly excluded. In contrast, Pickett, Gardner, and Knowles (2004) found that individuals who wrote about a personal experience of rejection were less empathically accurate compared with control participants. Examining how social pain affects empathic accuracy in socially anxious individuals would draw together the literature on individual differences in threat sensitivity and empathic responses to social pain.
Study 1
In Study 1, we used a university sample to examine the relationship between social anxiety and accurate empathy for targets describing socially painful experiences. Video recordings were made of target individuals discussing a high school event in which they had been socially excluded. Targets were filmed speaking directly to the camera and were alone in the frame. Targets rated the emotions they were feeling while discussing the event. After watching the videos, participants rated their impressions of the targets’ self-ratings and also rated their own emotions while watching the targets’ videos. The discrepancy between participants’ ratings of targets and targets’ self-ratings served as a measure of accurate empathy. Before observing the videos, participants were randomly assigned to either a social-exclusion condition or to a control condition to allow us to examine whether a recent socially painful experience influenced the relationship between social anxiety and empathy for emotional reactions to social exclusion. We hypothesized as follows:
Hypothesis 1: Consistent with previous work, social anxiety would predict greater empathic accuracy in judgments of video targets’ negative affect (NA).
Hypothesis 2: Social exclusion would strengthen this relationship.
Method
Participants
Participants were recruited from the undergraduate subject pool in exchange for course credit. A power analysis using G*Power (Version 3; Faul, Erdfelder, Lang, & Buchner, 2007) indicated that a minimum of 119 participants would be sufficient to detect a medium effect size (Cohen’s f = 0.15) at 80% power with an error probability (α) of .05. A total of 146 participants completed the study. Eleven participants were excluded (10 for suspicion about the manipulation, 1 for lack of language fluency), which resulted in a final sample of 134 1 (79.8% female; mean age = 20.47 years, SD = 2.66; mean time at university = 2.37 years, SD = 1.41). Of the sample, 37.2% self-identified as Chinese, 32.6% self-identified as White, and 30.2% self-identified as being from other backgrounds.
Measures
The Social Interaction Anxiety Scale–Straightforward Score (SIAS-S; Rodebaugh, Woods, & Heimberg, 2007), a 17-item version of the original SIAS (Mattick & Clarke, 1998), was used to assess anxiety in social interactions along a continuous dimension. The SIAS-S has been shown to have stronger psychometric characteristics than the original measure (Rodebaugh et al., 2007). SIAS-S items are rated on a 5-point scale ranging from 0 (not at all characteristic or true of me) to 4 (extremely characteristic or true of me). The measure displayed good internal consistency (Cronbach’s α = .94) in the current study.
Empathy
Emotion ratings were made using the Negative Affect subscale from the Positive and Negative Affect Schedule Short Form (I-PANAS-SF; Thompson, 2007) and a modified version of the Positive Affect (PA) subscale using emotions taken from the 60-item expanded PANAS-X (Watson & Clark, 1994). 2 The NA and PA subscales each comprise five adjectives reflecting various types of NA or PA that are rated on 5-point scales ranging from 1 (never) to 5 (always). In this study, the target individuals in the videos rated the NA and PA they experienced while discussing their high school social experiences. After observing each video, research participants rated their judgments of the emotions the target in the video was experiencing. The PANAS has been used to rate others’ affect (e.g., Watson, Hubbard, & Wiese, 2000) and demonstrated good reliability in the current study, αs = .88 and .93 for NA and PA, respectively.
Accurate empathy was calculated by taking the discrepancy between participants’ and targets’ ratings for each individual affect item for each video (e.g., discrepancy = participant ratings – target ratings) and summing these to yield NA and PA discrepancy scores. Positive scores indicated that the participant overestimated the affect experienced by the target, whereas negative scores indicated underestimates of targets’ affect. Scores closer to 0 indicated greater convergence between participant and target’s affect ratings.
Video stimuli
The stimuli comprised four videos in which two women and two men in their mid-20s recounted real social-exclusion experiences they had experienced in high school. All targets were fully informed about the use of the stimuli and instructed to avoid explicitly labeling the emotions they experienced. Targets were filmed alone in the frame. The videos were approximately 1 to 3 min in length.
Social-exclusion manipulation check
After the manipulation, participants completed a questionnaire that included six questions about their impressions of their supposed conversational partner (e.g., “How would you rate your first impression of this individual?”) and their reactions to the situation (“How accepted do you feel by this person?”) on 9-point scales (1 = not at all, 9 = very much so). Following previous research (e.g., Nordgren et al., 2011), participants also completed the Faces Pain Scale–Revised (Bieri, Reeve, Champion, Addicoat, & Ziegler, 1990) to assess social pain intensity. The measure contains six human faces distributed across a 10-point scale that varied in terms of the magnitude of expressed pain. Participants were asked to “indicate how you currently feel by circling the faces that best reflects your feelings on the scale below.” The scale was found to be reliable and valid in previous studies. The first impression and social pain variables were converted to z-scores and summed. The resulting situation appraisal score was found to be internally consistent, α = .83, and was used to evaluate whether the exclusion manipulation was successful. Participants also completed the NA and PA items to assess postexclusion affect. These items were summed to yield NA and PA total scores.
Procedure
All research measures and procedures were approved by the University Behavioral Research Ethics Committee. Participants were informed that the study investigated how perceptions of similarity influence how individuals judge others’ emotions and that they would engage in a brief social interaction. Participants were randomly assigned to either the experimental (social rejection) or control condition using a table of random numbers (http://www.random.org) and were blind to condition.
Social-exclusion manipulation
The experimental manipulation was based on previous research with the intent of creating a naturalistic experience of social exclusion (e.g., Mallot, Maner, DeWall, & Schmidt, 2009). After participants arrived at the lab, the experimenter asked them to complete a questionnaire about themselves (e.g., something they we’re proud of, their pet peeves) and were told that this would be e-mailed to a partner. Participants then received an e-mail with the partner’s questionnaire to read while the experimenter left the room to bring the “partner” to meet the participant. All information on the partner’s questionnaire was the same across participants except that the gender (as indicated by name) of the partner was randomized. After a few minutes, the experimenter returned to the lab alone and told participants either that their partner left the study because they had forgotten about an appointment (control condition) or that their partner appeared uncomfortable after reading the participant’s questionnaire and stated they did not want to meet (experimental condition). No specific reasons were provided for why the partner did not want to meet. The experimenter then stated “Although you never met your partner, you were only going to meet them briefly. We can still probably use your data from this short questionnaire with your first impressions of your partner so far.”
Participants then completed a questionnaire assessing their impressions of the situation and affect (NA and PA). Detailed description of the manipulation is presented in the Supplemental Material available online.
Empathy task
Participants then observed the four videos and rated their perceptions of each video target’s NA and PA.
Debriefing
Participants were debriefed about the true nature of the study. A funnel debriefing was conducted in which participants were asked about suspicion of the manipulation and other procedures.
Results
Preliminary analyses
Descriptive statistics
The mean SIAS-S score (M = 23.53, SD = 13.78) indicated comparability with other undergraduate samples (e.g., Rodebaugh et al., 2011). Analyses of variance (ANOVAs) were conducted and revealed no significant SIAS-S differences between the control (M = 22.79, SD = 13.32) and experimental (M = 24.30, SD = 14.31) participants, t(127) = −0.62, p = .54, for gender or years of university. However, the experimental group was significantly older (M = 21.01 years, SD = 3.09) than the control group (M = 19.93 years, SD = 1.98), t(133) = −2.44, p = .016. Analyses controlling for age yielded the same results; therefore, analyses without age are reported.
Stimuli validation
The internal consistency of participants’ ratings across the four videos was adequate for NA, Cronbach’s α = .80 (αs = .77, .87, .73, and .81), and PA, α = .91 (αs = .84, .94, .96, and .91).
Exclusion-manipulation check
Three multiple linear regression analyses were conducted to evaluate the exclusion manipulation on the situation appraisal and NA and PA scales. In all analyses, social anxiety (SIAS-S), condition, and the interaction were entered as predictors. SIAS-S was mean-centered, and condition was categorically coded with the experimental group as the reference. All variables were converted to z-scores to produce standardized regression coefficients (βs). For the situation appraisal score, the overall model was significant, F(3, 129) = 14.72, p < .001. There was a significant main effect of condition, β = −0.46, t = −5.94, p < .001, indicating that excluded participants felt excluded. The main effect of social anxiety was also significant, β = −0.31, t = −2.73, p = .007, indicating that individuals with social anxiety felt more excluded. The interaction was not significant, β = 0.16, t = 1.42, p = .16. For both NA and PA, the overall models were significant, F(3, 129) = 12.52 and 9.38, ps < .001. Again, there were significant main effects of condition, βs = 0.46 and −0.39, ps < .001. Neither the social anxiety main effects, βs = 0.15 and −0.18, ps = .19 and .12, nor interactions, βs = −0.05 and 0.04, ps = .67 and .73, were significant. Thus, the exclusion manipulation resulted in the expected negative response.
Main analyses
Two multiple linear regression analyses were conducted in which social anxiety (SIAS-S), condition, and their interaction were entered as predictors with NA and PA discrepancy scores as dependent variables. SIAS-S was mean-centered, and condition was categorically coded such that the experimental group was the reference group (i.e., experimental group = 1). All variables were converted to z-scores to produce βs.
The overall model for NA was significant, F(3, 128) = 3.20, p = .026, R2 = .07. There was a significant main effect of social anxiety, b = 0.36, t = 2.98, p = .003. Follow-up analyses were conducted using a mean split for social anxiety (M = 23.20, SD = 13.74). Higher social anxiety predicted greater accuracy in judgments of targets’ NA (M = 1.23, SD = 10.99 vs. M = −3.52, SD = 8.73, for high and low social anxiety, respectively). Neither the main effect of condition, b = −0.06, t = −0.37, p = .71, nor the interaction, b = −0.26, t = −0.50, p = .14, was significant. The overall model for PA was not significant, F(3, 127) = 1.52, p = .21, R2 = .04.
Discussion
Social anxiety predicted greater empathic accuracy for others’ negative emotions in response to social exclusion. The findings were consistent with our hypothesis and with previous research indicating that individuals with anxious attachment patterns and higher rejection sensitivity displayed greater empathy (e.g., Simpson et al., 2011; Simpson et al., 1999). The accuracy of socially anxious individuals’ ratings may be explained by the tendency of socially anxious individuals to selectively attend to negative emotions and social stimuli as a means to avoid rejection or other feared negative social outcomes (e.g., Yang, Yoon, Chong, & Oh, 2013). One consequence of this tendency could be that socially anxious individuals are more accurate at judging the negative emotions of others who are experiencing social pain as well.
Contrary to our hypotheses, a recent experience of social exclusion did not affect the social anxiety–empathy link. Individuals in the exclusion condition reported more negative reactions to the manipulation, which indicates that being told a peer did not want to meet them was effective in producing the desired effect. As expected, greater social anxiety predicted more negative perceptions of the exclusion; however, this did not affect empathic accuracy, suggesting that social pain did not facilitate empathy for either socially anxious or nonanxious individuals.
Study 2
Individuals with SAD are likely to experience more severe symptoms than a university sample and also to display stronger associated features, for example, self-focused attention, which could distract them from attending to others’ emotions. They also are higher on rejection sensitivity, which might render them more vulnerable to the effects of social exclusion. Study 2 was conducted to examine empathic accuracy in a sample of individuals diagnosed with SAD.
As noted earlier, empathy comprises both cognitive and emotional components. Cognitive empathy is the ability to mentally place oneself in others’ positions and take their perspective. Emotional empathy refers to understanding the other person through the automatic and vicarious experience of similar emotions (e.g., Preston & de Waal, 2002). Although the shared experience of negative emotions may serve as a cue that the other person is in need and thereby facilitate understanding, the experience of high negative arousal can lead to self-focused attention and distress in the perceiver that disrupts constructive action (e.g., Eisenberg et al., 1994) and rational judgment (Bloom, 2016). In Study 2, we measured state versions of both the emotional and cognitive components of participants’ empathy to determine whether either or both aspects mediated the link between social anxiety and accuracy in judging targets’ emotions and if so, whether one component was the stronger mediator. Establishing a mediational role for state empathy would strengthen the conclusion that the emotion judgments made by individuals with SAD reflected their responses to targets rather than a general negative view of social events. Assessing the relative importance of the two components would also provide more detailed information on how individuals with SAD may differ from nonsocially anxious control participants in their empathic responses.
Research in nonclinical samples suggested that social anxiety was associated with less adaptive responses to social exclusion (e.g., Mallot et al., 2009; Maner, DeWall, Baumeister, & Schaller, 2007); however, little research has examined clinical SAD samples. A recent Cyberball ostracism study that examined social exclusion found that individuals with SAD reported an increase in self-focused negative emotions, internal negative attributions such as self-blame, and a decrease in feelings of control and intent to engage in pleasant activities compared with non-SAD control participants (Gutz, Roepke, & Renneberg, 2016); however, other studies did not (e.g., Gutz, Renneberg, Roepke, & Niedeggen, 2015). Given these inconsistencies, we examined the effects of exclusion on empathic accuracy in this clinical sample.
Finally, we wanted to address a puzzling issue. Previous studies found that socially anxious participants displayed greater empathic accuracy relative to nonanxious control participants (Auyeung & Alden, 2016; our Study 1). In light of this empathy, why do these individuals not do better socially? As noted earlier, accurate empathy for distressing or threat-related content can lead to worse social outcomes in certain situations (e.g., Manczak et al., 2015; Simpson et al., 2011; Simpson et al., 2003). Studies also indicated that after rejection, most individuals make efforts to reconnect and engage in positive social behaviors to regain feelings of belonging and acceptance (e.g., DeWall et al., 2011; Maner et al., 2007). It is possible that nonanxious individuals, although less empathically accurate, may be better able to engage in positive interpersonal behaviors aimed at regaining a sense of belonging, whereas individuals with SAD may be overwhelmed by the negative affect they experience while watching the videos, which then impedes their ability to generate effective social responses even if they accurately recognize others’ negative emotions. To explore this possibility, we examined the link between empathic accuracy and social responses. When friends talk about difficult topics, it is important for the listener to be able to respond in ways that are empathic and helpful. In Study 2, after viewing the videos, participants were asked to provide open-ended descriptions about the advice they would give to the target individuals in response to targets’ rejection experiences. These descriptions were content analyzed to determine whether participants with SAD and control participants differed in the quality of the social responses they provided.
Study 2 hypotheses
We hypothesized as follows:
Hypothesis 1: Participants with SAD would be more empathically accurate.
Hypothesis 2: The relationship between social anxiety and empathic accuracy would be mediated by participants’ emotional and cognitive empathic reactions while observing the video.
Hypothesis 3: Non-SAD control participants would be more willing to socially reconnect and provide positive advice to targets, whereas individuals with SAD would provide no advice and be less likely to provide advice to socially reconnect.
Given the Study 1 results, we made no predictions about the effects of exclusion on those relationships.
Method
Participants
The standardized regression coefficient (β) from Study 1 was 0.36, representing a large effect size (Cohen’s f = 0.39). A power analysis using G*Power (Faul et al., 2007) was conducted assuming a large effect size and based the analysis on a fixed-effects ANOVA model (two main effects and interaction), an α level of .05, and a false-negative rate of β = 0.95. A sample of 117 subjects was judged to provide 80% power.
Participants were recruited from the community through posters and online advertisements using separate ads for the non-SAD controls and SAD participants. All prospective participants completed a 15- to 25-min telephone screening interview with one of four trained research assistants that assessed SAD and depressive symptoms and the inclusion and exclusion criteria. Eligible applicants participated in the lab portion of the study and were compensated $35 for their participation.
Participants were assessed using the Anxiety Disorders Interview Schedule (ADIS-IV; (Brown, Di Nardo, & Barlow, 1994) for the fourth edition of the Diagnostic and Statistical Manual of Mental Disorders (American Psychiatric Association, 1994), a semistructured interview that has demonstrated high interrater reliability and good concurrent validity (Brown et al., 1994). Diagnostic interviews were conducted by three doctoral-level graduate students who had training and experience administering the ADIS-IV. Inclusion criteria for the SAD group were (a) primary diagnosis of SAD according to the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM–V; American Psychiatric Association, 2013); (b) no current major depressive disorder, psychosis, substance abuse, or severe self-reported suicidal ideation and/or nonsuicidal self-injury; and (c) English fluency. Inclusion criteria for the control group were (a) no diagnosis of SAD, current major depressive disorder, psychosis, substance abuse, or severe self-reported suicidal ideation and/or nonsuicidal self-injury and (b) English fluency. Fifteen percent of the interviews were rated by two research assistants and revealed good agreement on SAD diagnosis (κ = .90, p < .001).
Eleven participants were eliminated from the control applicants because they (a) had SAD (n = 2), (b) were experiencing a current or recent depressive episode (n = 4), and/or (c) met criteria for other disorders (n = 5); 15 SAD participants were eliminated because (a) they failed to meet SAD criteria (n = 6), (b) they had a current or recent depressive episode (n = 6), and/or (c) SAD was not their primary diagnosis (n = 3). During the debriefing, 2 SAD participants were excluded because they were suspicious of the experimental manipulation. Independent samples t tests revealed no significant differences between excluded and included non-SAD control participants for age, t(72) = 0.20, p = .84; gender, t(72) = −0.68, p = .50; or education, t(70) = 1.06, p = .29. Likewise, no significant differences emerged between included and excluded SAD participants for age, t(77) = −1.66, p = .10; gender, t(77) = 0.29, p = .77; education, t(74) = 0.26, p = .80; or SAD symptom severity, t(76) = 0.74, p = .46.
The final sample included 126 participants, 63 in each group. The non-SAD control group was 61.9% female and had a mean age of 29.9 years (SD = 12.51); 26 participants (41.3%) self-identified as White, 17 (27.0%) self-identified as Chinese, and the remaining endorsed a variety of cultural identities. The SAD group was 60.3% female, had a mean age of 29.30 years (SD = 9.19), and had mean time of university/college education of 3.37 years (SD = 2.50); 31 (49.2%) self-identified as White, 11 (17.5%) self-identified as Chinese, and the remaining participants identified a variety of cultural backgrounds.
Measures
Symptom measures
SAD symptom severity was assessed using the SIAS-S (Rodebaugh et al., 2007) as in Study 1. In the current study, internal consistency was adequate, Cronbach’s α = .97.
Given the high comorbidity between SAD and major depressive disorder, we wanted to examine the specificity of any findings to SAD. Therefore, participants also completed the Beck Depression Inventory–Second Edition (BDI-II; Beck, Steer, & Brown, 1996), a 21-item self-report instrument that assesses depressive symptoms over the past 2 weeks. Items are rated on 4-point scales ranging from 0 (symptom not present) to 3 (symptom very intense) and summed. The BDI-II has been validated across multiple samples and demonstrated high internal consistency. In the current study, α = .94
Empathy
As in Study 1, emotion ratings were made using the NA and PA scales. The procedure for making empathy ratings and calculating NA and PA discrepancy was the same as Study 1.
Manipulation checks
After the experimental manipulation, participants completed a questionnaire rating their feelings toward their supposed conversational partners on the same measures as those used in Study 1. In the current study, the internal consistency of the situation appraisal scale and NA and PA scores were adequate, αs = .80, .76, and .76 for situation appraisal, NA, and PA, respectively.
Potential mediators
State emotional and cognitive empathy were assessed as potential mediators.
State emotional empathy
Participants rated how they themselves were feeling while watching each of the videos using the NA and PA subscales.
State cognitive empathy
Participants rated two items that reflected the cognitive component of empathy (e.g., “I imagined how I would feel in this person’s place”; “I was able to imagine how things looked from his/her perspective”). Items were rated on 7-point scales (1 = not at all, 7 = very much so) and summed to yield a total score. In the current study, α = .88
Advice
Participants were provided the opportunity to give open-ended advice to the targets in the videos with the instructions that “this advice would be shared with the targets to help them respond to this or similar situations.” After each video, participants were asked, “What advice would you give this individual? You can write as much or as little as you like. Otherwise, please type ‘no advice.’” The question was open-ended, and there was no limit on word length. Three independent raters conducted content analyses to code the open-ended answers into three categories reflecting the potential relational effects of the advice. Positive advice referred to advice that encouraged positive social behaviors to help restore feelings of inclusion and/or reestablish the target’s relationship with the rejecting party (Sample item: “If it’s still a painful memory, don’t be afraid to share those feelings with your close friends.”). Negative advice referred to advice that was judgmental of the targets’ actions and/or dismissive of the severity of the events discussed (Sample item: “It doesn’t really matter. Move on.”). No advice was assigned to answers in which participants chose not to provide advice to the targets in the videos. The open-ended responses were coded for the type of advice (negative, positive, or no advice), and the number of times each type was provided was tallied for each participant. Interrater agreement was good for both positive advice, α = .78, and negative advice, α = .79.
Procedure
All research measures and procedures were approved by the University Behavioral Research Ethics Committee. Participants were informed that the study investigated how perceptions of similarity influence how individuals judge others’ emotions. Participants were blind to experimental condition. Participants were randomly assigned to either the experimental (social exclusion) or control condition using a table of random numbers (www.random.org) and completed the study tasks below.
Experimental manipulation
The experimental manipulation procedure and manipulation check were the same as those used in Study 1.
Video ratings
After the social-exclusion manipulation, participants rated the same four videos of targets (two male, two female) discussing high school social rejection experiences used in Study 1. As in Study 1, after each video, participants rated their perceptions of the target’s NA and PA and wrote their advice to that target. Participants also completed the state emotional and cognitive empathy measures to assess their reactions to targets.
Debriefing
Participants were debriefed about the true nature of the study and informed about the deception. A funnel debriefing was conducted in which participants were asked about suspicion of the manipulation and other procedures. Eight participants expressed suspicion and were eliminated from data analyses. The experimenter also talked with participants to ensure they were not feeling any significant negative emotions.
Results
Preliminary analyses
Descriptive statistics
The mean level of social anxiety for the SAD group (M = 40.70, SD = 10.32) was similar to that in individuals seeking treatment for SAD (e.g., M = 43.93, SD = 11.84; Rodebaugh et al., 2011). Independent samples t tests indicated that SIAS-S scores were significantly higher for the SAD group than for the non-SAD control group (M = 10.22, SD = 6.39), t(1045) = −19.93, p < .001. The SAD group (M = 18.68, SD = 9.53) also reported significantly higher levels of depression than the non-SAD control group (M = 5.54, SD = 4.54), t(89) = −9.89, p < .001. The main analyses were reconducted using depression as a covariate. Depression did not affect the main results and was not a significant predictor of empathic accuracy. Therefore, the main analyses without depression are reported.
Stimuli validation
The video stimuli were validated as in Study 1. The internal consistency of participants’ ratings across the four videos for the current study was adequate for NA, Cronbach’s α = .68 (αs = .70, .65, .62, and .73), and PA, α = .78 (αs = .77, .81, .76, and .78).
Exclusion manipulation check
For situation appraisal, the overall two-way ANOVA was significant, F(3, 121) = 14.64, p < .001. There was a significant main effect of experimental condition, F(1, 121) = 34.27, p = .001, and group, F(1, 121) = 10.53, p = .002, but the interaction was not significant, F(1, 121) = 0.00, p = .99. The overall two-way ANOVAs for NA and PA were both significant, F(3, 119) = 13.77 and 3.25, ps = .001 and .02 for NA and PA, respectively. There were also significant main effects of experimental condition, F(1, 119) = 3.83 and 8.47, ps = .05 and .004 for PA and NA, respectively. The group main effect of NA was significant, F(1, 119) = 37.79, p < .001; SAD participants reported greater NA than non-SAD control participants. The Group × Condition interaction was not significant, F(1, 119) = .18, p = .68. For PA, neither the group main effect, F(1, 119) = 0.39, p = .53, nor the interaction, F(1, 119) = 1.12, p = .29, was significant. To summarize, participants in the exclusion condition felt greater social rejection and NA and lower PA compared with non-SAD control participants which indicated that the manipulation was effective. SAD participants experienced greater social exclusion and greater NA than control participants. As in Study 1, SAD participants who were excluded did not differ significantly from included control participants.
Main analyses
Two ANOVAS (two way, between subjects) were conducted with group, condition, and the interaction entered as fixed factors and NA and PA discrepancy scores as dependent variables. The overall ANOVA for NA discrepancy was significant, F(3, 122) = 2.98, p = .034, partial η2 = .07. There was a significant main effect of group, F(1, 122) = 8.88, p = .003, partial η2 = .07. The slope indicated that the SAD group was significantly more accurate (M = −5.33, SD = 10.78) compared with the non-SAD control group (M = −10.98, SD = 10.35). Neither the condition main effect, F(1, 122) = .03, p = .87, nor the interaction, F(1, 122) = .04, p = .85, was significant. The overall Group × Condition ANOVA for PA discrepancy was not significant, F(3, 122) = .94, p = .42.
Mediators
Because individuals with SAD tend to experience greater NA in general and we wanted to examine situation-specific reactions, we computed residual change scores (r-NA) by regressing participants’ self-rated NA while observing the videos onto their prior self-rated NA. We conducted a two-way ANOVA with group (i.e., non-SAD control participants = 0, SAD = 1), exclusion condition, and their interaction as predictors and the r-NA scores as the dependent variable. The overall model was significant, F(3, 121) = 5.76, p = .001. A significant main effect emerged for group, F(1, 121) = 13.04, p < .001. The main effect of experimental condition did not reach significance F(1, 121) = 3.85, p = .052, and the interaction was not significant, F(1, 121) = .051, p = .82. The results indicated that individuals with SAD experienced an increase in negative affect while watching the videos, suggesting they were responding to targets’ comments.
We computed a parallel mediation analysis to investigate the relationship between SAD and NA discrepancy (i.e., the difference between participants’ ratings of target NA and targets’ own ratings of NA). Both the cognitive empathy score and the emotional empathy score (i.e., r-NA, change in participants’ own NA from before to after observing the videos) were entered into the model as mediators with group (non-SAD control, SAD) as the independent variable and NA discrepancy as the dependent variable. Analyses were conducted using the IBM SPSS (Version XX) macro PROCESS (Model 4; Hayes, 2013).
Group significantly predicted NA discrepancy (Path c, β = 0.39, SE = 0.13, p = .003) as did both cognitive empathy (Path a1; β = 0.75, SE = 0.17, p < .001) and emotional empathy (Path a2; β = 1.08, SE = 0.15, p < .001). Both cognitive empathy (Path b1; β = 0.15, SE = 0.06, p = .015) and emotional empathy (Path b2; β = 0.38, SE = 0.07, p < .001) significantly predicted NA discrepancy. It is notable that emotion empathy showed a stronger effect. These results are consistent with a mediational hypothesis. To determine whether the indirect (a × b) effect was significant, a bootstrap estimation approach with 5,000 resamples was conducted. The indirect effect was significant (β = 0.53, SE = 0.11, 95% CI = [0.35, 0.76], p < .05). This finding is consistent with the hypothesis that a proportion of the variance in the relationship between group and NA discrepancy was accounted for by perceivers’ empathic responses to targets. To investigate the extent to which state empathy mediated this relationship (i.e., full or partial mediation), we recalculated path c with the state measures in the model (c′ path). Group was no longer a significant predictor of NA discrepancy after controlling for the mediators, β = −0.14, SE = 0.14, p = .32, consistent with full mediation. Approximately 33% of the variance in NA discrepancy was accounted for by the predictors (R2 = .33). See Figure 1.
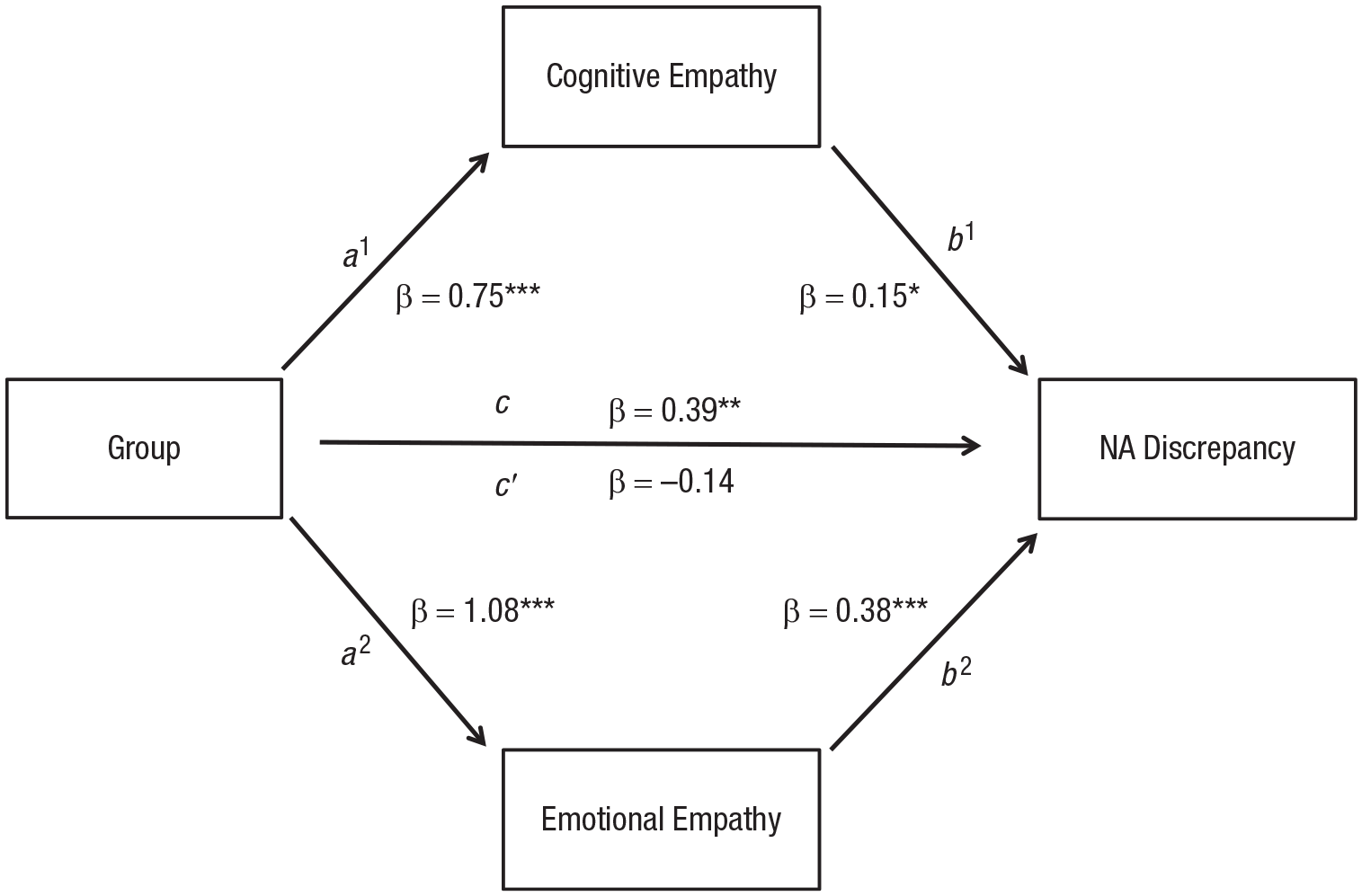
Model of the indirect effect of cognitive empathy and emotional empathy on the relationship between group and negative affect discrepancy. The indirect effect (a × b) was significant at β = 0.53, SE = 0.11, 95% CI = [0.35, 0.76]. NA = negative affect.
Advice analyses
Three Group × Condition ANOVAs were conducted to examine frequency of each type of advice. The overall ANOVA for positive advice was significant, F(3, 121) = 3.07, p = .030, partial η2 = .07. A significant group main effect emerged, F(1, 121) = 7.93, p = .006, partial η2 = .06. The slope indicated that the SAD group (M = 2.08, SD = 0.16) provided positive advice to targets less often than non-SAD control participants (M = 2.70, SD = 0.16). Neither the main effect of experimental condition, F(1, 121) = 0.57, p = .45, nor the interaction, F(1, 121) = 0.04, p = .84, was significant. The overall ANOVA for negative advice did not reach significance, F(3, 121) = 2.41, p = .070, partial η2 = .06.
The overall ANOVA for no advice was significant, F(3, 121) = 3.42, p = .024, partial η2 = .08, with a significant main effect of group, F(1, 121) = 8.31, p = .005, partial η2 = .06. The slope indicated that, overall, individuals with SAD (M = 1.29, SD = 0.15) more often provided no advice to the targets compared with non-SAD control participants (M = 0.67, SD = 0.15). Neither the main effect of experimental condition, F(1, 121) = 0.42, p = .52, nor the interaction, F(1, 121) = 1.69, p = .20, was significant.
General Discussion
Across two studies, participants with SAD and participants with social anxiety displayed greater accuracy in their judgments of others’ negative emotions arising from social exclusion relative to individuals without SAD. The mediation analyses provided support for the conclusion that these judgments reflected genuine empathic accuracy in that participants with SAD had higher scores on state empathy, which in turn predicted greater accuracy in their judgments of others. Relative to non-SAD control participants, individuals with SAD saw themselves as more similar to targets and were better able to take their perspective, possibly because they too had experienced socially painful events. They were also significantly more likely to share targets’ distress. Moreover, the increase in negative affect when watching the videos indicated that their emotion judgments reflected use of target-related information and were not simply a function of preexisting negative affect.
The findings are in line with cognitive models of social anxiety that suggest that socially anxious individuals may have attentional and perceptual biases toward signs of social threat (e.g., Clark & Wells, 1995; Hofmann, 2007; Rapee & Heimberg, 1997). Numerous studies have found that social anxiety was associated with faster processing of threat-relevant information, such as angry faces or words related to social threat (e.g., Mogg, Philippot, & Bradley, 2004). The results of these studies suggested that the attentional biases found in social anxiety might actually facilitate the accurate perception of others’ negative emotions by increasing sensitivity to others’ signs of distress.
To assess potential responses to empathy, we offered participants the option to provide written advice to the video targets. Individuals with SAD were more likely to give no advice, and the advice they did offer was less likely to suggest engaging in behaviors that might facilitate relationship repair. These findings may help to consolidate the counterintuitive findings that socially anxious individuals were more accurate at judging others’ negative emotions. Despite their accuracy, socially anxious individuals may not be able to use this information to facilitate positive social behavior. Providing written advice is a narrow measure of the domain of prosocial behavior; however, the pattern observed here is consistent with a large body of literature indicating that individuals with SAD engage in social avoidance, withdrawal, and constraint. They display lower self-disclosure, even with friends or romantic partners, relative to nonanxious individuals (Sparrevohn & Rapee, 2009; Stoltenberg, Christ, and Carlo, 2013). In addition, they are constrained in displaying warm or prosocial behaviors (e.g., Rodebaugh et al., 2013). As a result, they can be perceived by others to be less warm and friendly (Inderbitzen-Nolan, Andersen, & Johnson, 2007). To take the current situation as an example, if individuals with SAD fail to respond to a peer’s disclosure of a painful event, one would expect that the relationship would be weakened. These avoidant tendencies might be expected to impede the ability of socially anxious individuals to generate effective social responses even if they detect others’ negative emotions (e.g., Bloom, 2016).
Across both studies, individuals with low social anxiety were less empathically accurate and underestimated the negative emotions of others. As previously discussed, a certain level of inaccuracy may be beneficial for the perceiver, particularly in the presence of distress and negative emotions (e.g., Manczak et al., 2015; Simpson et al., 2011). Consistent with theories of exclusion, individuals without SAD may have turned their attention away from negative information and toward positive social information, which is theorized to help individuals recover from the effects of social exclusion and facilitate the restoration of feelings of social inclusion (e.g., engaging in positive social behaviors; Powers & Heatherton, 2013). Another factor may be that these individuals were less likely to have the painful exclusion experiences that might facilitate empathy.
One question that remains to be answered is whether the empathic accuracy displayed by participants with SAD was specific to exclusion and negative affect or whether it would extend to other types of social situations and other emotions. For example, Morrison and colleagues (2016) showed that socially anxious individuals were less able to empathize with others’ positive emotions. Individuals with SAD report having adverse social developmental experiences (e.g., Blöte & Westenberg, 2007), which may render them particularly sensitive to negative social events and less able to detect or take pleasure in others’ positive experiences. Further work is needed to determine whether the empathic accuracy found here is confined to socially painful experiences or extends to nonsocial pain and other emotions. In addition, there was variability in empathy within both groups. It would be informative to determine the factors that predicted greater empathic accuracy. For example, it may be that individuals who themselves experienced significant social exclusion, criticism, or bullying were better able to detect the targets’ affect.
A recent experience of social exclusion did not influence how individuals empathized with others. It is worth noting that participants with SAD felt greater distress even in the control condition, which may have obscured reactions to the exclusion manipulation. This finding is in line with previous research that found socially anxious individuals interpreted neutral and ambiguous stimuli as more threatening than nonanxious individuals did and showed more neurological reactivity in the amygdala, which suggests that they experienced more fear in response to neutral stimuli (e.g., Cooney, Atlas, Joormann, Eugene, & Gotlib, 2006; Yoon & Zinbarg, 2008). Furthermore, studies also found that socially anxious individuals fail to show the positive interpretation of ambiguous events found in nonanxious individuals (Hirsch & Mathews, 2000). An alternative explanation is that social anxiety may not influence initial reactions to social rejection but rather prolongs the recovery process; however, support for this idea is tenuous (see Hartgerink, van Beest, Wicherts, & Williams, 2015). Nonetheless, the results of these two studies come down on the side of earlier findings indicating that social pain does not facilitate empathy, even for emotionally vulnerable people.
Several limitations should be acknowledged concerning the current research. The video stimuli used here did not involve the type of back-and-forth interaction and potential for negative outcomes found during genuine social events that might create self-focused attention and distract from noticing others’ emotions. These stimuli offer the advantage of consistency in targets’ expressions and depicted genuinely moving social rejection experiences; however, they were video presentations. Likewise, the laboratory social-exclusion manipulation may have lacked real-life validity. Given that this was a novel question regarding the intersection between social anxiety, social exclusion, and empathic accuracy, we considered it useful to first investigate the findings in a laboratory setting so that rejection was consistent across participants. In addition, laboratory studies allow for prospective examination of the effects of exclusion on empathy. Much of the extant research on social exclusion has used retrospective designs to determine how exclusion is related to current behaviors (i.e., asking participants about how often they have been excluded in the past). These designs, although representing real experiences of social exclusion, do not allow for the direct examination of the relationship between these events and current behaviors. Other studies used manipulations in which individuals were asked to write about a particular and/or recent social-exclusion experience. In these designs, there is no way to equate the severity or frequency of previous exclusion experiences across participants. Nonetheless, the next step in this research would be to address these questions using more ecologically valid social events.
Another issue is that the measure of prosocial behavior used here captures only a limited part of the prosocial bonding spectrum. Moreover, giving advice is an assertive behavior and can be viewed by recipients as directive and intrusive. Individuals with SAD may find it particularly difficult to provide social advice given their own self-perceived deficiencies. It would be informative for future work to determine whether they can offer other kinds of supportive responses. Finally, participants made ratings of targets’ emotions at the end of the video. Future studies could use Ickes’s (2001) empathic accuracy paradigm of having targets and participants make ratings at multiple points throughout the videos to get a more nuanced measure of empathic accuracy. It is possible that the off-line ratings made in the current study provided less interference or were less overwhelming compared with on-line ratings (e.g., Morrison et al., 2016).
These limitations notwithstanding, the research offers a novel contribution by bringing together the literatures on social anxiety, empathy, social exclusion, and positive interpersonal behavior with a goal of understanding the interpersonal difficulties associated with SAD. If replicated, the finding that individuals with SAD were less able to provide relationship building advice may have treatment implications. These individuals often report being unsure of how to properly respond to others. Given that they may indeed be more accurate in their judgments of others’ negative social emotions, therapeutic work could focus on validating these initial judgments and devising ways to act appropriately on these judgments. It could be useful to role-play ways to respond empathically to others, such as providing validation and positive encouragement and potentially engaging in self-disclosure. Many therapeutic interventions for SAD focus on helping individuals to turn attention away from one’s own internal sensations and negative thoughts and focus on external stimuli. This approach could be combined with training to practice ways to express that they are feeling empathy for that person’s experience. These steps may help individuals with SAD capitalize on their empathic sensitivity.
Supplemental Material
Alden_Supplemental_Material – Supplemental material for Accurate Empathy, Social Rejection, and Social Anxiety Disorder
Supplemental material, Alden_Supplemental_Material for Accurate Empathy, Social Rejection, and Social Anxiety Disorder by Karen Auyeung and Lynn E. Alden in Clinical Psychological Science
Footnotes
Transparency
Action Editor: Erin B. Tone
Editor: Scott O. Lilienfeld
Author Contributions
Both of the authors contributed to the research design, methodology, and data interpretation. K. Auyeung conducted the research procedure, data collection, and analysis. The authors cowrote the manuscript. Both of the authors approved the order of authorship. Both of the authors approved the final manuscript for submission.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.