
Abstract
The knowledge–practice gap remains a challenge in many fields. Health research has shown that professional networks influence various aspects of patient care, including diffusion of innovative practices. In the current study, we examined the potential utility of professional networks to spread the use of violence-risk-assessment tools in forensic psychiatric settings. A total of 6,664 reports, written by 708 clinicians, were used to examine the effect of clinicians’ use of risk-assessment tools on subsequent reports by other clinicians with whom they share patients. Results show that professional networks serve as an important channel for the spread of assessment practices. Simulation of a continuing education program showed that targeting more influential clinicians in the network could be 3 times more efficient at disseminating best practices than randomly training clinicians. Decision-makers may consider using professional networks to identify and train influential clinicians to maximize diffusion of the use of risk-assessment instruments.
Keywords
Despite the proliferation of empirically established risk-assessment tools over the past 25 years (Fazel, Singh, Doll, & Grann, 2012) and their demonstrated usefulness for violence prediction and treatment planning (de Vries Robbé, de Vogel, Douglas, & Nijman, 2015; Fazel et al., 2012; Singh et al., 2014), the implementation of these tools into clinical practice is incomplete. This is not limited to the field of violence-risk assessment; the “knowledge–practice gap” poses a challenge for scientists and practitioners in many fields (Evensen, Sanson-Fisher, D’Este, & Fitzgerald, 2010; Kazdin, 2008; Lang, Wyer, & Haynes, 2007), with an estimated average lag of 6 to 17 years from research results to uptake and implementation in practice (Morris, Wooding, & Grant, 2011).
A traditional top-down approach is at times insufficiently convincing for practitioners to implement new practices (Freedman, 2002). Health research has shown that professional networks that exist among physicians can influence various aspects of patient care, including diffusion of innovative practices (Barnett, Landon, O’Malley, Keating, & Christakis, 2011; Landon et al., 2012; Landon et al., 2013; Pollack, Soulos, & Gross, 2015; Pollack et al., 2014). Although not without debate (e.g., Lyons, 2011; Shalizi & Thomas, 2011; Thomas, 2013; VanderWeele, Ogburn, & Tchetgen-Tchetgen, 2012), professional networks have been put forward as a novel way of studying and decreasing the knowledge–practice gap (Barnett et al., 2011). The current study examined the possibility of using professional networks to spread the use of violence-risk-assessment practices among clinicians.
Diffusion of Knowledge
Individuals are embedded in and connected through social networks (e.g., social, familial, occupational; Serrat, 2017). These networks may meaningfully influence diffusion of knowledge, practices, habits, and risks (for a review, see Christakis & Fowler, 2013). Clinicians too are embedded in formal (e.g., hospitals, health authorities) and informal professional networks (e.g., via patient sharing; Barnett et al., 2011). Although formal networks are more prescriptive, a growing evidence base suggests that informal networks may be more influential on practices and treatment outcomes (Hayward, Guyatt, Moore, McKibbon, & Carter, 1997; Landon et al., 2012, 2013; Pollack et al., 2015). However, little is known about the potential influence of professional networks in the transfer of professional practices in mental health and even less in the field of forensic mental health.
Risk Assessment in Forensic Mental Health
The field of forensic mental health focuses on individuals with mental health problems who are involved in the criminal-justice system. Forensic mental health professionals often have the challenging task of evaluating the risk of future violence by a specific patient (Carver & Langlois-Klassen, 2006; Mullen, 2000) to support decisions about the appropriate nature of treatment and supervision (Hilton & Simmons, 2001; Wilson, Crocker, Nicholls, Charette, & Seto, 2015). An incorrect assessment or inadequate recommendation may unnecessarily restrict patients’ civil liberties or, conversely, decrease public safety (Guy, Douglas, & Hart, 2015).
To aid in legal and clinical decision-making, researchers have developed a number of structured risk-assessment tools based on empirically established and clinically relevant predictors of future offending (Guy et al., 2015). These tools can predict future violence and other offenses with some accuracy over and above unstructured clinical judgment (Ægisdóttir et al. 2006; Campbell, French, & Gendreau, 2009; Fazel et al., 2012; Guy, 2008; Yang, Wong, & Coid, 2010). Note that predictions based on unstructured clinical judgment have been shown to correctly classify around 62% of cases as recidivists or nonrecidivists, whereas predictions based on structured tools can correctly classify up to 75% of these cases (Gardner, Lidz, Mulvey, & Shaw, 1996). Because of the severity of the potential consequences of these predictions, authors have cogently recommended the continued development and use of structured assessment tools (Otto & Douglas, 2010).
Knowledge–Practice Gaps in the Violence-Risk-Assessment Field
An international survey showed that just approximately 58% of forensic mental health professionals used some type of structured instrument in their violence-risk assessments (Singh et al., 2014). In an analysis of more than 5,000 forensic psychiatric reports, just 17% mentioned using a structured risk-assessment instrument (Crocker, Nicholls, Charette, & Seto, 2014). Considering the implications for patients’ liberties and public safety, this gap is concerning (Guy et al., 2015).
A clearer understanding of factors that influence diffusion of structured risk-assessment practices is needed to develop effective and cost-efficient strategies to promote structured risk assessment in forensic services. Peer influences through informal professional networks may help to reduce that knowledge–practice gap (Barnett et al., 2011; Freedman, 2002; Landon et al., 2012; Landon et al., 2013; Pollack et al., 2014; Pollack et al., 2015).
Given recent findings regarding the proliferation of risk assessments (Fazel et al., 2012) and variation in the use of empirically validated risk-assessment measures (Wilson et al., 2015), we tested the diffusion of structured risk-assessment reporting practices through informal professional networks of forensic clinicians. We hypothesized that clinicians using risk-assessment tools in their reports would influence others’ reporting practices over time by increasing their use of risk-assessment tools as a result of mere exposure through their informal professional networks.
Method
Sample
We used data from a Canadian file-based study of 1,800 forensic patients found not criminally responsible on account of mental disorder (NCRMD) in the three most populous provinces between 2001 and 2005 and followed until 2008 (Crocker, Nicholls, et al., 2015). In Canada, a defendant found NCRMD is deemed to have been unaware of an act or omission or not to have understood the wrongfulness of an act or omission because of mental illness (Criminal Code, R.S.C., 1985, c. C-46). Under Canadian law, an independent tribunal—called a review board—is tasked with the annual review of NCRMD accused. Review boards render one of three dispositions (detention, release to community with conditions, or release to community without conditions) based largely on forensic practitioners’ assessments of each patient’s violence risk and treatment progress (Crocker, Charette, et al., 2015; Hilton & Simmons, 2001; Hilton, Simpson, & Ham, 2016; McKee, Harris, & Rice, 2007).
Although a variety of mental health professionals use structured violence-risk-assessment measures (Singh et al., 2014) and the law states that assessments may be conducted “by a medical practitioner or any other person who has been designated by the Attorney General as being qualified” (Criminal Code, RSC 1985, c. C-46, p. 672.1 (1)), all assessment reports in this sample were conducted by psychiatrists. In the current study, the content of 7,037 reports to review boards was examined. For 94.7% of the reports (N = 6,664), we were able to identify 708 distinct clinicians who submitted reports. These reports constitute the final sample used to examine the use and diffusion of structured risk assessment.
Informal professional networks
Because physicians often refer patients to colleagues they know, patient transfers have been shown to be an adequate proxy for informal professional networks between health professionals (Barnett et al., 2011). During the average 963.2 days (SD = 797.02, Mdn = 783) of follow-up, 999 patients (56%) transitioned, on average twice, between clinicians (M = 1.82 transitions; SD = 1.11). In this sample, 1,417 transfer links were observed among 639 clinicians (69 clinicians had no links). The date of the first transfer between two clinicians was considered as the starting date of the professional link between a set of two clinicians.
Figure 1 shows the network structure of patient transfers across forensic clinicians. The nodes represent clinicians, and the lines represent transferred patients. The size of the node reflects the number of patients assessed by this clinician. The province of Québec provided the largest clinician network with 517 clinicians, followed by Ontario with 156 clinicians, and British Columbia with 35 clinicians. This is an artifact of the number of individuals found NCRMD and how the forensic systems were designed in each province (Crocker, Nicholls, et al., 2015). Forensic patients were spread out over 50 hospitals in Québec, 11 hospitals in Ontario, and a single provincial hospital in British Columbia with six satellite outpatient clinics.
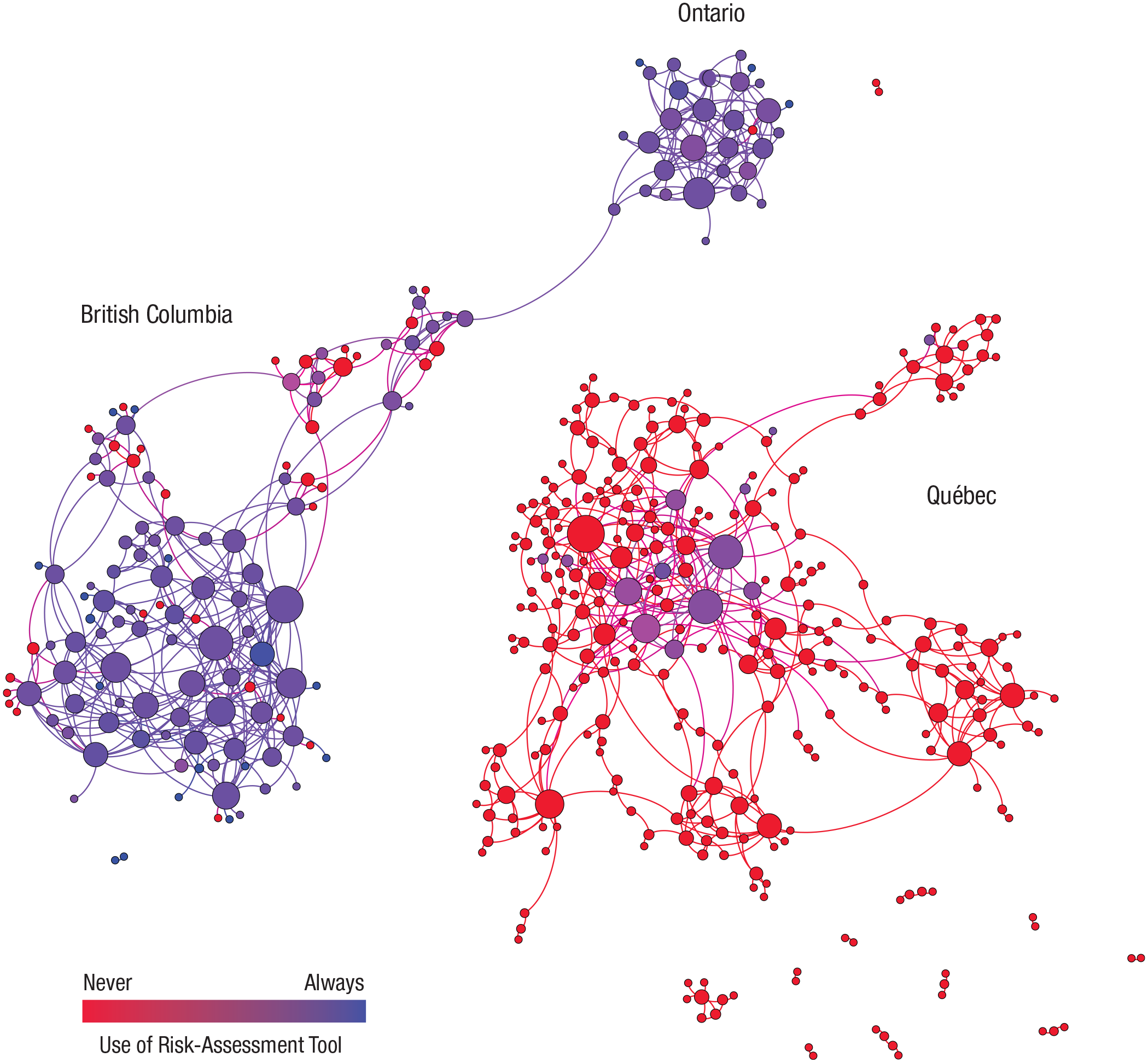
Patient networks shared among clinicians and the use of a risk-assessment tool. The size of the node represents the number of clinician peers.
Risk-assessment practices
In the present study, risk-assessment practice was operationalized as the assessor mentioning the use of a structured risk-assessment tool in the report to review boards. Reports to courts and, by extension, review boards should contain an exhaustive enumeration of the sources of data drawn from to form an opinion, including risk-assessment tools (Melton et al., 2018). Structured risk-assessment approaches involve actuarial or structured professional judgment models. Actuarial models mechanically weigh and combine risk factors according to their unique, empirically established relationships with the outcome and provide probabilistic risk estimates, whereas structured professional judgment models comprise theoretically, clinically, and empirically informed variables that evaluators weigh and integrate (Guy et al., 2015). Six meta-analyses demonstrated the comparable predictive accuracy between these two models in terms of violence-risk assessment (Ægisdóttir et al., 2006; Campbell et al., 2009; Fazel et al., 2012; Grove, Zald, Lebow, Snitz, & Nelson, 2000; Guy, 2008; Yang et al., 2010), and there is no evidence of the relative superiority of one over the other in terms of violence-risk prediction (Heilbrun, Yasuhara, & Shah, 2010). However, this is not to suggest that the models are interchangeable. The selection of a measure should reflect the assessment purpose (Skeem & Monahan, 2011). Consequently, both structured risk-assessment approaches were considered as an appropriate tool in these reports. Alternative analyses using the number of items of the two most popular tools of these two approaches and separate analyses using the Historical and Clinical Risk Management 20 (HCR-20) (Webster, Douglas, Eaves, & Hart, 1997) as a structured professional judgment tool and the Violence Risk Appraisal Guide (VRAG) as an actuarial tool (Quinsey, Harris, Rice, & Cormier, 2006) led to similar results (for statistical models and sensitivity tests, see Table S3 in the Supplemental Material available online).
Approximately 18% (n = 1,218) of the reports analyzed in this study mentioned the use of a risk-assessment tool. The color of the nodes in Figure 1 shows the distribution of the use of structured assessment tools between the clinicians’ networks.
Analysis
Diffusion effects
A simplified example of the diffusion of risk-assessment practices would be that a given clinician (“Dr. Ego”) had not used a risk-assessment tool at Time 1, and we wanted to observe whether exposure to reports from a peer (“Dr. Alter”) that mentioned using a risk assessment tool would influence the mention or use of a risk-assessment tool in Dr. Ego’s report at Time 2.
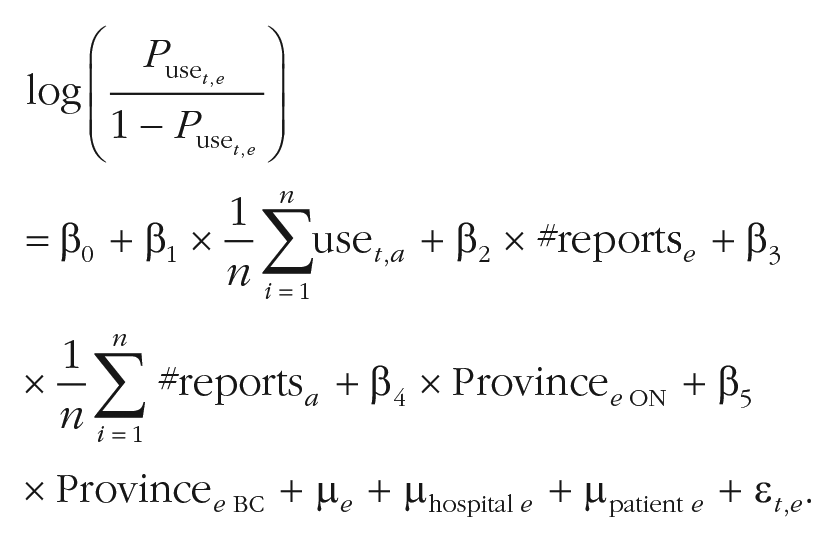
We examined all reports for all 893,069 clinician dyads that were observed in the network between the source (Alter, a) and the target (Ego, e) occurring after the first patient transfer recorded in our study window. Equation 1 presents a logistic regression model predicting the probability that the Ego report uses a risk-assessment tool (Puse t,e ) at one given time (t), with the proportion of risk-assessment tool use of the n Alters’ reports at different time points (use t,a ) as a covariate. To control for clinicians’ report writing experience, the number of reports written by Ego (#reports e ) and the average number of reports written by the Alters (#reports a ) were included in the equation. To account for dependencies of observations (i.e., each Ego can have more than one report), a random effect was included at the node levels (μ e ; Snijders & Kenny, 1999). To account for institutional effects (e.g., hospital policies), a random effect at the hospital level was included in the model (μhospital e). Patient characteristics may also influence the use of a risk-assessment tool. For example, the severity of a patient’s offense may motivate some assessors to include a more rigorous assessment. To account for this, a random effect was included at the patient level (μpatient e). The province where the Ego report was conducted (Provincee ON, Provincee BC) was included to account for provincial differences, using inconsequentially Québec as the reference category. The coefficient β1 tests the diffusion hypothesis and estimates whether an increase of the proportion of Alters’ reports including a risk-assessment tool would increase Egos’ future use of a risk-assessment tool. A positive coefficient indicates that if Alters’ reports included risk-assessment tools, Egos’ reported use of a risk-assessment tool increased as well:
We observed that clinicians using risk-assessment tools were clustered together in the network (for statistical models, see Table S1, Model 1 in the Supplemental Material). If influenced by Alter reports, Ego’s report risk item count would logically increase only after exposure to an Alter report. To ensure that the transfer link between the dyad was formed before the diffusion process, we used only Alter reports written before Ego reports and after the time we observed the first patient transfer between the two clinicians. To ensure that the knowledge transfer did not solely occur because of a reproduction of previous reports, 271,396 reports concerning the shared patients between Ego and Alter were removed from this analysis.
Continued education simulation
First, we examined whether our specific network demonstrated some type of diffusion or spread of risk-assessment practice. Note that diffusion through professional networks could be a medium for both good (i.e., using a risk-assessment tool) and bad (i.e., not using a risk-assessment tool) practices. In a second analysis, we examined whether diffusion could have a positive impact if used for targeting continued-education participants by conducting a clinician training simulation. Training was simulated by artificially making some clinicians in the network systematically use a risk-assessment tool in their reports, as if they had followed best practices after a training session at the beginning of our observation period. Four alternative methods for selecting who would receive training are presented: (a) random selection, (b) targeted selection based on network influence, (c) number of peers, or (d) bad reporting practices. In the first strategy, and to have a distribution of the random process, 100 iterations of the random selection process were carried out, and the average is presented. Targeted selection strategies involved training clinicians who were more influential in their network (i.e., those with more connections and more reports distributed throughout their network; weighted out-degree centrality; Newman, 2004), clinicians with the highest number of clinician peers (degree centrality), and clinicians who have not previously used a risk-assessment tool. Clinicians with more connections were hypothesized to reach more peers in the diffusion process and may thus spread risk-assessment practices more quickly or efficiently. Once targeted nodes were selected, the diffusion of the new information on the other reports was assessed using the coefficient estimates from Model 2 (for statistical models and sensitivity tests, see Table S1 in the Supplemental Material). The use of a risk-assessment tool per report following this simulated training are presented as a function of the number of clinicians trained.
Results
Diffusion effects
As hypothesized, the proportion of Alters’ reports using risk-assessment tools increased the use of these tools in the subsequent report of the Ego clinicians. An increase of 10% in the proportion of Alters reporting risk-assessment tool use increased the likelihood of Ego’s’ subsequent use of risk-assessment tools by 30% (95% confidence interval [CI] = [21%, 42%]; for statistical models, sensitivity tests, and the full description of the model, see Table S1 in the Supplemental Material). Iterated models, considering the effect may decrease over time, found an optimal diffusion effect for reports within a framework of less than 2 years after initial exposure (for statistical models and sensitivity tests for the iterated models, see Fig. S1 in the Supplemental Material). Alters’ total number of reports written did not influence the use of risk-assessment tools in Ego reports. Furthermore, Egos’ total number of reports written did not influence their use of risk-assessment tools: Clinicians who wrote more reports were not necessarily the ones who used the risk-assessment measures the most. Note that the direction of the patient flow did not influence the results, which suggests that the flow of information is bidirectional (for statistical models, sensitivity tests, and the full description of the model, see Table S1 in the Supplemental Material). The diffusion process was also observed using the number of risk items mentioned on the VRAG and the HCR-20 (for statistical models, sensitivity tests, and the full description of the model, see Table S2 in the Supplemental Material). This effect was also observed independently for each of the HCR-20 domains (historical, clinical, and risk management; for statistical models, sensitivity tests, and the full description of the model, see Table S3 in the Supplemental Material).
Continued-education simulation
Figure 2 shows the number of reports that included a risk-assessment tool as a function of the number of clinicians trained through the simulation processes, either (a) randomly, (b) targeted on the basis of the influence on the network (weighted out-degree centrality), (c) as a function of the number of alter clinicians (degree centrality), or (d) by targeting the clinicians who are not using risk-assessment tools. As expected, the more training clinicians received, the higher the overall increase in the use of risk-assessment tools across the network. Furthermore, as hypothesized, providing continuing education to influential clinicians is the most effective and efficient strategy in increasing the use of risk-assessment tools throughout the network. Targeting clinicians with a high number of Alter clinicians had a similar effect.
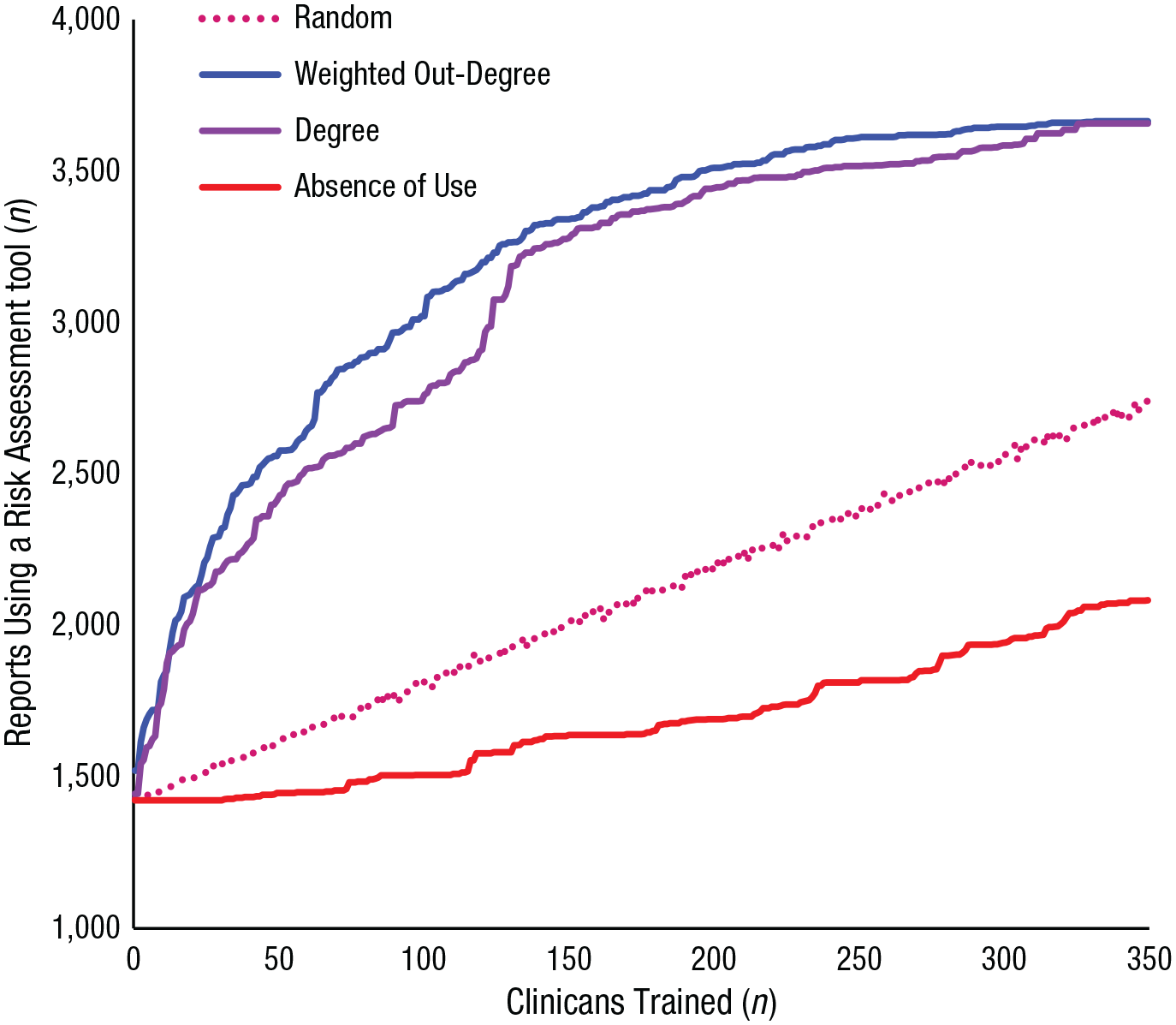
Number of reports using a risk-assessment tool as a function of the number of clinicians trained through a simulation using a random selection process, a targeted selection process based on influence on the network (weighted out-degree centrality), a targeted selection process based on the number of alter clinicians (degree centrality), and a targeted selection process based on the absence of a risk-assessment tool.
For example, if 50 clinicians were assigned to do training via targeted selection based on their network influence (Fig. 2), 2,577 reports would show the use of a risk-assessment tool, whereas just 1,613 reports would do so if 50 clinicians were assigned randomly to training (Fig. 2, dotted line). Because 1,218 reports showed the use of risk-assessment tool before any training, targeted selection improved the use of assessment tools 3.4 times more than random selection [(2,577 – 1,218) / (1,613 – 1,218)]. If no training was offered, just 18% of the reports would mention the use of risk-assessment tools; 50% of the reports would mention the use of a risk-assessment tool with 145 clinicians trained using the targeted method, whereas 497 clinicians would be necessary if trained randomly.
Discussion
Peer exposure to the use of risk-assessment measures was significantly associated with the use of risk-assessment tools in subsequent clinicians’ reports. This is consistent with prior research reporting on the influence of physician networks in the adoption of new medicines (Iyengar, Van den Bulte, & Valente, 2011), cancer treatment (Pollack et al., 2015), the adoption of electronic medical records (Angst, Agarwal, Sambamurthy, & Kelley, 2010; Zheng, Padman, Krackhardt, Johnson, & Diamond, 2010), and evidence-based medicine more generally (Mascia & Cicchetti, 2011). It is important to note, however, that the diffusion effect of Alter reports declined each year after initial exposure. This may speak to the importance of booster sessions and fostering consistent exposure to peers with desired risk-reporting practices.
We have also demonstrated that knowledge diffusion can be accelerated by providing continuing education to the most influential individuals in professional networks. It is yet unclear how effective risk-assessment training is. Previous studies have indicated that even short education sessions are effective in improving risk-assessment practices (Gough, Richardson, & Weeks, 2015; McNiel et al., 2008; Reynolds & Miles, 2009; Sen, Lindsey, Chatterjee, Rama-Iyer, & Picchioni, 2015). For example, a 5-hr workshop on the management of risk of violence and suicide significantly improved psychiatrists’ ability to identify risk and protective factors (McNiel et al., 2008; Teo, Holley, Leary, & McNiel, 2012). The success of further implementation of structured risk-assessment instruments hinges on additional factors such as the perceived complexity and clinical usefulness thereof, users’ lack of confidence, or staff not perceiving a need to update their practice (Levin, Nilsen, Bendtsen, & Bulow, 2016). In practice, it may be that forensic mental health networks can consider factors additional to training network influencers to optimize the diffusion of risk-assessment practices. However, using informal professional networks may be a cost-effective and efficient knowledge diffusion technique deserving further exploration. Perhaps surprisingly, we found that clinicians writing more reports were not necessarily the ones more likely to use risk-assessment tools. A number of factors may explain this finding. For example, experts writing more reports may have a (too) large caseload and may sacrifice rigor for efficiency. The relative sparseness in the use of risk-assessment tools may reflect a difference in framework (e.g., not taught to use structured risk assessment consistently, different reporting practices) or conceptual drift (e.g., over time, risk-assessment practice drifts from what was initially intended/taught). This finding warrants additional research.
The fact that psychiatrists were responsible for all reports mentioned in this study is an artifact of the legal framework in Canada. Psychologists, psychiatrists, and nurses conduct violence-risk assessments globally (e.g., Singh et al., 2014). These mental health professionals are all embedded in informal professional networks, and the same contingencies regarding knowledge diffusion on risk-assessment practices may or may not apply. Moreover, there is preliminary evidence of extrarole knowledge transfer (i.e., knowledge sharing among different professional groups; Tagliaventi & Mattarelli, 2006). Extrarole knowledge transfer and how it affects patient care would be an important avenue for further research in the field of mental health.
Limitations
First and foremost, we cannot infer causality from this study design. Indeed, as noted by other authors (Lyons, 2011; Shalizi & Thomas, 2011; Thomas, 2013; VanderWeele et al., 2012), the apparent causality of the network effect could be influenced by the network structure or simple network autocorrelation through homophily (e.g., association with clinicians who are like-minded) or exogenous processes (e.g., same workplace could indicate shared training, same geographical area could facilitate collaboration). However, to the best of our knowledge, this is the first study of knowledge diffusion in professional psychiatric networks, a promising field that requires further investigation.
Prior research has indicated that a number of clinician-related factors influence risk-assessment use (e.g., training, more exposure to ‘“duty to warn’” clientele, or prior violence-risk-assessment experience; Wong, Morgan, Wilkie, & Barbaree, 2012). Unfortunately, we had access to few variables or characteristics describing the report writers and were unable to include clinician covariates in our analyses. In addition, patient transfers are network proxies. Although patient transfers are consistently used to track and build physician networks (Landon et al., 2012; Landon et al., 2013; Pollack et al., 2014; Pollack et al., 2015), we recognize that other factors may influence network building and the strength of ties (e.g., same alma mater, family ties, same social circles). The influence of the courts and review boards might result in some constraints on patient-sharing networks compared with general psychiatry. In Canada, courts and review boards are responsible for decisions about detention in hospital, including security level, which hospital someone is registered with, and hospital transfers. However, the courts and review boards do not make patient referral decisions directly. Patient transfers might depend in part on security level (e.g., detention vs. community living) but also psychopathology (e.g., generalist vs. specialized and complex mental health needs) and infrastructure (e.g., bed availability, availability of forensic hospitals, and clinics in specific region). In addition, many patient transfers would be within the same hospital, such as from one ward to another or from inpatient to outpatient services. General psychiatry also has systemic constraints, as when health maintenance organizations in the United States define networks of clinicians and transfers out-of-network are difficult or even prohibited. The effect of differences in the overarching networks on knowledge transfer is a topic deserving further research.
Our data are approximately 10 to 15 years old; practices may have changed. Although a recent small-scale study concluded that Canadian forensic practices may have changed for the better (i.e., risk-assessment information was not cited selectively; Hilton et al., 2016), relatively recent international data show that many (> 50%) forensic mental health professionals still do not use structured risk-assessment instruments (Singh et al., 2014). Finally, our estimation of the collaborative ties is likely censored to the left given that past patient sharing (and thus existing informal professional networks) could not be tracked before the study period. Note that these latter two points do not invalidate the diffusion process observed in this study.
Conclusions
Our study indicates that informal professional networks may play a role in the diffusion of risk-reporting practices. Before drawing firm conclusions, our study requires replication in other samples and settings in which violence-risk assessment is used and patients transition between practitioners. Current forensic mental health systems may benefit from this knowledge, specifically to implement or increase attention to structured risk assessment in reports to legal tribunals. It would be worthwhile to explore the impact of informal professional networks on other aspects of forensic mental health as well as other areas in mental health care more generally.
Supplemental Material
sj-pdf-1-cpx-10.1177_2167702620954797 – Supplemental material for Is Knowledge Contagious? Diffusion of Violence-Risk-Reporting Practices Across Clinicians’ Professional Networks
Supplemental material, sj-pdf-1-cpx-10.1177_2167702620954797 for Is Knowledge Contagious? Diffusion of Violence-Risk-Reporting Practices Across Clinicians’ Professional Networks by Yanick Charette, Ilvy Goossens, Michael C. Seto, Tonia L. Nicholls and Anne G. Crocker in Clinical Psychological Science
Footnotes
Transparency
Action Editor: Scott O. Lilienfeld
Editor: Scott O. Lilienfeld
Author Contributions
M. C. Seto, T. L. Nicholls, and A. G. Crocker designed the original study from which the data were taken. Y. Charette and I. Goossens developed the theoretical framework for the current study. Y. Charette performed the statistical analyses. All of the authors drafted the manuscript and approved the final version for submission.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.